Embed Size (px)
Citation preview
Chapter 43An Approach to Children With Suspected Congenital Heart Disease . . . . 418
Chapter 44Echocardiography in Congenital Heart Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . 429
Chapter 45Cardiac Catheter Interventions for Congenital Heart Disease . . . . . . . . . . . . . . . . . 443
Chapter 46Surgical Interventions for Congenital Heart Disease . . . . . . . . . . . . . . . . . 456
Chapter 47Arrhythmias in Congenital Heart Disease . . . . 467
Chapter 48Cardiopulmonary Exercise Testingin Children With Congenital Heart Disease . . . 479
Chapter 49Kawasaki Disease . . . . . . . . . . . . . . . . . . . . . . . . 484
Chapter 50Congenital Coronary Anomalies . . . . . . . . . . . . 491
Section VIIICCONGENITONGENITAL HEARAL HEART DISEASET DISEASE

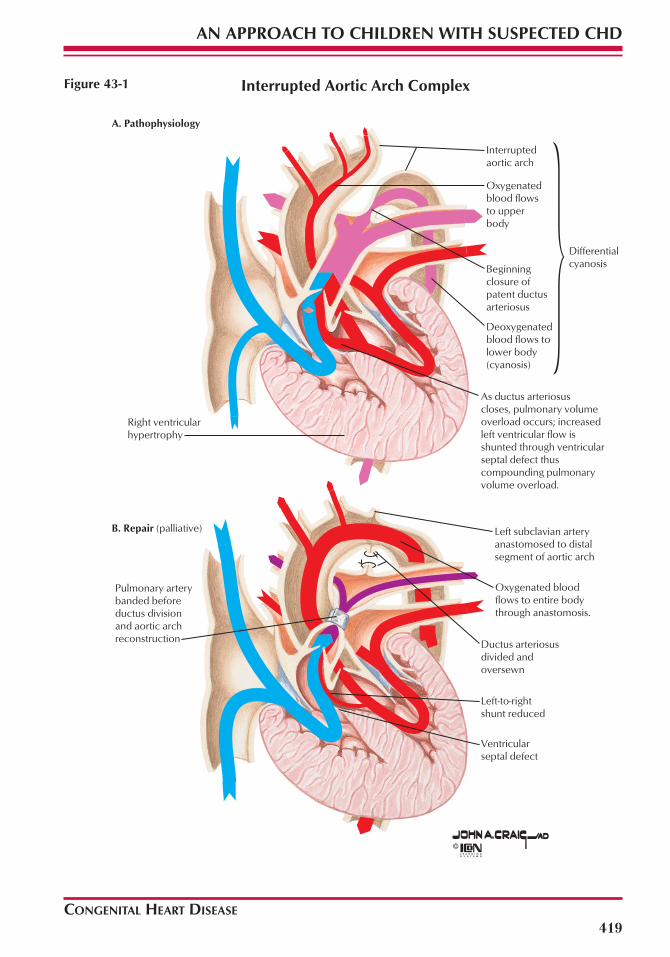
Congenital heart defects can be classified intothose that result in cyanosis and those that donot. Acyanotic defects include those with a left-to-right shunt and increased pulmonary blood flowand obstructive defects without associated shunt-ing. Left-to-right shunts occur at various anatomiclevels: atrial (e.g., atrial septal defect), ventricular(e.g., ventricular septal defect [part of the com-plex defect depicted in Fig. 43-1]), or arterial (e.g.,patent arterial duct). Obstructive lesions withoutany associated shunts include pulmonary steno-sis, aortic stenosis, and coarctation of the aorta.
Cyanotic defects are generally characterizedby a right-to-left shunt and may be classified intotwo broad categories. In the first group, withintracardiac defects and obstruction to pul-monary flow, cyanosis results from decreasedpulmonary blood flow and the intracardiac mix-ing of oxygenated and desaturated blood. In thesecond group, cyanosis results from the admix-ture of pulmonary and systemic venous returnsdespite normal or increased pulmonary bloodflow. In most cardiac malformations classified inthis group, a single chamber receives the total sys-temic and pulmonary venous returns. The admix-ture lesion can occur at any intracardiac level:venous (e.g., total anomalous pulmonary venousconnection), atrial (e.g., single atrium), ventricu-lar (e.g., single ventricle), and great vessel (e.g.,persistent truncus arteriosus). Near-uniform mix-ing of the venous returns usually occurs. Com-plete transposition of the great arteries (Fig. 43-2)can be included in this group, although only par-tial admixture of the two venous returns occurs,leading to severe hypoxemia.
CONGENITAL HEART DISEASE
CLINICAL INDICATIONS FOR MEDICAL OR SURGICALINTERVENTION
The interdisciplinary approach that is neededclinically to optimally care for children with con-genital heart disease includes accurate assess-ment of anatomic defects and their physiologicconsequences and effective communication ofthese findings. The consequences of alteredblood flow induced by congenital heart diseaseand the effects of therapeutic interventionsinvariably influence the pulmonary circulationby increasing pulmonary blood flow (e.g., left-to-right shunting through intracardiac septaldefects), decreasing pulmonary blood flow(e.g., right-sided obstructive heart lesions, suchas tetralogy of Fallot) (Fig. 43-3), altering the path-way of pulmonary blood flow (e.g., Fontan-Kreutzer repair), or altering the hemodynamicsto which pulmonary blood flow (e.g., pulmonaryhypertension) is subjected. Successful manage-ment can often depend on the ability of the clini-cian to monitor pulmonary hemodynamics andassess pulmonary vascular impairment.
Critically important to an understanding of thephysiologic consequences of these defects arethe maturational differences that occur in car-diopulmonary function. For example, cardiacfunction is subject to maturational changes occur-ring at the cellular level in a variety of processes,including those in the neurocardiac functionalunit: changes in neurotransmitter content, thereceptor system, innervation, the effector/trans-ducer systems, and the cellular componentsaffected by autonomic stimulation (Fig. 43-4).
418
Birth defects occur in approximately 2% of all births. Congenital heart disease comprises almosthalf of such defects, occurring in approximately 8 in 1000 newborn infants. Many classifications existfor congenital heart disease, and two variations based on a simple physiologic approach follow.
G. William Henry
Chapter 43
An Approach to Children With Suspected Congenital Heart Disease
CONGENITAL HEART DISEASE
AN APPROACH TO CHILDREN WITH SUSPECTED CHD
Interrupted Aortic Arch Complex
A. Pathophysiology
B. Repair (palliative)
Right ventricularhypertrophy
Interruptedaortic arch
Oxygenatedblood flows to upperbody
Beginningclosure ofpatent ductusarteriosus
Deoxygenatedblood flows tolower body(cyanosis)
Differentialcyanosis
As ductus arteriosuscloses, pulmonary volumeoverload occurs; increasedleft ventricular flow isshunted through ventricularseptal defect thuscompounding pulmonaryvolume overload.
Left subclavian arteryanastomosed to distalsegment of aortic arch
Oxygenated bloodflows to entire bodythrough anastomosis.
Ductus arteriosusdivided andoversewn
Left-to-rightshunt reduced
Ventricularseptal defect
Pulmonary artery banded before ductus division and aortic archreconstruction
419
Figure 43-1

4. Common atrium produced by septostomyallows mixing of oxygenated anddeoxygenated blood
1. Balloon-tipped catheter introduced intoleft atrium through patent foramen ovale
2. Balloon inflated
3. Balloon withdrawn producing largeseptal defect
Balloon Atrial Septostomy (Technique)
Transposition of Great Arteries
CONGENITAL HEART DISEASE
AN APPROACH TO CHILDREN WITH SUSPECTED CHD
420
Figure 43-2
Regardless of the anatomic defects, the physi-ologic consequences necessitating medicalintervention, surgical intervention, or both fallinto three broad categories—heart failure,hypoxemia/hypoxia, and risk of pulmonary vas-
cular disease—and represent a second approachto children with suspected congenital heart dis-ease (by risk stratification).
Heart failure is defined as the inability of theheart to supply an adequate cardiac output

CONGENITAL HEART DISEASE
AN APPROACH TO CHILDREN WITH SUSPECTED CHD
Tetralogy of Fallot
Pathophysiology
Blalock-Taussig Operation
Right ventricular outflow obstruction
Right-to-left shunt through ventricular septal defect
Right ventricular hypertrophy
Intense cyanosis caused by high proportion of deoxygenated blood
Decreased pulmonary flow
Small pulmonary trunk
Aorta shifted to right and overrides defect
Ventricular septal defect
(palliative)
Anastomosis of subclavian artery to pulmonary artery
Right ventricular outflow obstruction
Right-to-left shunt through ventricular septal defect
Left-to-right shunt through anastomosis of subclavian artery to pulmonary artery
Cyanosis reduced or eliminated by increased proprtion of oxygenated blood
Increased pulmonary flow distal to right ventricular outflow obstruction
Increased pulmonary pressure enlarges pulmonary arterial tree
Aorta shifted to right and overrides defect
Ventricular septal defect
421
Figure 43-3
(CO) to meet the aerobic metabolic demands ofthe body, including those incurred by growth;inefficiency of the heart to meet the metabolic
demands can also be included in a more liberaldefinition of heart failure. An alteration in one ormore physiologic determinants of ventricular

CONGENITAL HEART DISEASE
AN APPROACH TO CHILDREN WITH SUSPECTED CHD
422
Sympathetic presynaptic
Sympathetic postsynaptic
Parasympathetic presynaptic
Parasympathetic postsynaptic
Visceral afferentaccompanying sympathetic fibers
Visceral afferent accompanyingparasympathetic fibers
Cardiacplexus
Nucleus ofsolitary tract
Posterior nucleusof vagus nerve
Medullaoblongata
Vagus nerves
Superior cervical(vagal) cardiac nerves
Inferior cervical(vagal) cardiac nerves
Ascendingconnections
T1
T2
T3
T4
Superior cervicalsympathetic ganglion
Superior cervical(sympathetic) cardiac nerve
Middle cervicalsympathetic ganglion
Middle cervical(sympathetic) cardiac nerve
Vertebral ganglion (variation)
Ansa subclavia
Cervicothoracic(stellate) ganglion
Inferior cervical (sympathetic) cardiac nerve
Thoracic cardiacbranch of vagus nerve
2nd thoracicsympathetic ganglion
White ramus communicans
Gray ramus communicans
Thoracic (sympathetic)cardiac branches
4th thoracic sympathetic ganglion
1st intercostalnerve
Innervation of Heart: Schema Figure 43-4

CONGENITAL HEART DISEASE
AN APPROACH TO CHILDREN WITH SUSPECTED CHD
423
function—preload, afterload, contractility, andHR or rhythm—can adversely affect cardiac per-formance beyond the compensatory mecha-nisms, particularly in fetuses or newborn infants,where cardiac function occurs much higher(and hence less efficiently) on the Frank-Starlingcurve because of maturational aspects. As aphysiologic consequence, fetuses and infantsare more dependent on mechanisms thatincrease HR rather than those that increasestroke volume to increase CO in response toincreased metabolic demands.
The etiology of hypoxemia (abnormal reduc-tion in the arterial oxygen tension) must beestablished to determine whether therapeuticintervention is necessary immediately. Hypoxia(inadequate tissue perfusion) is always a med-ical emergency because high morbidity andmortality are associated with uncorrected meta-bolic acidosis. Hypoxemia is most often associ-ated with defects characterized by right-to-leftintracardiac shunting in which effective pul-monary blood flow is reduced. Pulmonaryblood flow may be entirely dependent on thepatency of the arterial duct. The arterial ductbegins to close shortly after birth, at which timethe hypoxemic (and hypoxic) consequences ofductal dependency manifest. Since the 1970s,pharmacologic manipulation of the arterial ductto maintain or reestablish patency by constantintravenous infusion of prostaglandin E1 or E2has dramatically improved the care of affectedchildren by diminishing hypoxia during trans-port to a center where diagnostic and therapeu-tic interventions can more safely take place.
Defining the pathophysiology of pulmonaryvascular disease remains a fertile area forresearch. The primary approach is to study ther-apeutic interventions to eliminate the risk fac-tors for pulmonary vascular disease (Fig. 43-5) inall children identified at high risk because knowl-edge of the pathogenesis of these arteriolarchanges remains incomplete. Three principalrisk factors should be characterized by noninva-sive and invasive techniques described subse-quently: increased pulmonary blood flow fromleft-to-right, intracardiac or extracardiac shunt-ing or an abnormal cardiac connection (e.g.,septal defect, patent arterial duct, arteriovenousfistula, transposition of the great arteries);
increased pulmonary artery pressure fromincreased pulmonary blood flow or increasedpulmonary venous pressure; and hyperviscosityas a consequence of hypoxemia from de-creased pulmonary blood flow in right-sidedobstructive heart lesions (e.g., tetralogy of Fallot,tricuspid atresia, pulmonary atresia) or hypox-emia from inadequate mixing (e.g., transpositionof the great arteries).
Increased pulmonary blood flow can be dis-tinguished physiologically with the concept ofindependent or obligatory flow, where depend-ency is defined relative to pulmonary vascularresistance (or impedance). For example, in chil-dren with unrestricted ventricular septal defects,the magnitude of the left-to-right shunting, andtherefore pulmonary blood flow, depends onthe relative difference between pulmonary andsystemic vascular resistances (or impedances).As physiologic influences change this relativedifference, the ratio of pulmonary to systemicflow changes proportionally. Therefore, this typeof shunting depends on the status of the pul-monary vascular bed. In contrast, in childrenwith atrioventricular (AV) septal defects withunrestricted left ventricular (LV)–right atrial (RA)shunting via the abnormal left AV valve, a signif-icant difference in the resistances determiningthis flow (e.g., LV systolic pressure comparedwith simultaneous RA pressure) always exists.Therefore, increased flow occurs across the tri-cuspid and pulmonary valves, independent ofthe pulmonary vascular resistance. The magni-tude of such a shunt is modulated more by ven-tricular function. Commonly in this clinical set-ting, pulmonary hemodynamics are furtherimpaired by pulmonary hypertension, increas-ing the burden on ventricular function and sub-jecting the child to higher risks of heart failureand accelerated development of pulmonary vas-cular disease.
Timing for medical or surgical interventionbecomes more evident by examining the actu-arial consequences of these three risk factors forpulmonary vascular disease: increased pul-monary blood flow, pulmonary hypertension,and hyperviscosity. Increased pulmonary bloodflow alone contributes to the risk of develop-ment of pulmonary vascular disease, but thetime course for irreversible pulmonary vascular

Pulmonary arteriole showing intimal and medial changes secondary to pulmonary volume overload
Medial hypertrophy
Intimal proliferation
Pulmonary Vessel Complications of Left-to-Right Shunts
CONGENITAL HEART DISEASE
AN APPROACH TO CHILDREN WITH SUSPECTED CHD
424
Figure 43-5
changes is measured in years. In contrast, pul-monary hypertension is a more significant risk,with irreversible changes observed in months to1 to 2 years. Severe hyperviscosity states andpulmonary hypertension in children with cyan-otic heart disease contribute to an extremelyhigh risk of irreversible changes as early as 3months of age. An optimal time for interventionto decrease the risk associated with the naturalhistory can be determined by overlaying theactuarial experience for specific medical andsurgical interventions.
INITIAL NONINVASIVE ASSESSMENTOF CHILDREN WITH CONGENITALHEART DISEASEHistory
The history is critically important for childrenwith suspected congenital heart disease.Because congenital heart disease is most oftendiagnosed in early infancy, a chronologicapproach is simple but effective. The history ofpregnancy, labor, and delivery is often helpful(e.g., perinatal asphyxia) with age and develop-mentally appropriate attention to expectedactivity. For example, inquiry into the feedinghistory may be disproportionately important ininfants, whereas inappropriate fatigue or exer-cise tolerance may be important in older chil-dren. One issue that cannot be overemphasizedin the pediatric age group is growth. Growth is a
cardiovascular stress, and absence of growthmay be the only manifestation of heart failure.
The family history is often benign but mayalert the clinician to relevant issues, such as theincidence of and the genetic predisposition tocongenital heart disease. Information aboutgene-specific etiologies of specific defects (orrisk of such expression) will increase the impor-tance of family history and inquiry into geneticpredisposition in the near future.
Physical ExaminationThe physiologic features associated with
altered pulmonary artery hemodynamics thatare discernible by physical examination can begenerally ascribed to features associated withpulmonary hypertension and decreased orincreased pulmonary blood flow. Cardiac situsmust first be established by means of palpation.
Children with decreased pulmonary bloodflow secondary to congenital heart disease pres-ent clinically with cyanosis. Cyanosis necessi-tates approximately 5 g of circulating deoxy-genated hemoglobin; therefore, in children withrelative anemia, cyanosis may not be as obviousas expected, even in cyanotic congenital heartdisease. Despite cyanosis, children with congen-ital heart disease often seem comfortable, with-out evidence of respiratory distress—an impor-tant distinction to differentiate hypoxemia as aconsequence of a parenchymal disorder (leading

CONGENITAL HEART DISEASE
AN APPROACH TO CHILDREN WITH SUSPECTED CHD
to a ventilation/perfusion defect of perfused butunderventilated portions of the lungs). Childrenwith congenital heart disease who are cyanoticbecause of obstruction to pulmonary blood flowhave alterations in the second heart sound with adiminished or absent pulmonary componentresulting from diminished or absent flow acrossthe pulmonary valve. Despite the most astuteclinical efforts, the diagnosis of specific congeni-tal heart defects by means of physical examina-tion is often disappointing and can only beregarded as an initial screening procedure.
The physical diagnosis of pulmonary hyper-tension is rarely difficult. The cardiac examina-tion predictably consists of a prominent rightventricular (RV) impulse that is either visible oreasily palpable at the lower left sternal border orin the subxiphoid area (when present with nor-mal cardiac situs). On auscultation, a single,loud or narrowly split second heart sound with aloud pulmonary component is present. Pul-monary systolic ejection clicks are also commonin severe pulmonary hypertension, arising froma dilated, hypertensive proximal main pul-monary artery. Systolic murmurs at the lower leftsternal border consistent with tricuspid insuffi-ciency are sometimes present, although tricus-pid insufficiency is common and usually pres-ents without a murmur being noted onauscultation. In severe, long-standing pul-monary hypertension, a decrescendo, high-pitched, early diastolic murmur of pulmonaryinsufficiency may be present along the mid leftsternal border. When pulmonary hypertensionis accompanied by RV failure, findings of sys-temic venous engorgement are present, includ-ing hepatosplenomegaly and peripheral edema.Abnormal v and a waves may be found duringexamination of the neck veins.
Features associated with increased pulmonaryartery flow are typically related to auscultatoryfindings from excessive flow crossing normalheart valves (Fig. 43-6). Because the semilunarvalves have approximately one half the cross--sectional area of the AV valves, early diastolicmurmurs associated with increased flow acrossthe AV valves require more flow than midsystolicflow murmurs associated with flow across thesemilunar valves. This point can be a distinguish-ing feature in quantifying a left-to-right shunt with
normal ventricular function because flow acrossthe AV valves must be approximately doubled toauscultate such diastolic murmurs.
Chest RadiographyAlthough more sophisticated imaging modali-
ties exist to provide anatomic and physiologicinformation regarding the pulmonary circulation,chest radiography is still used routinely as ascreening method to determine the status of thepulmonary vasculature, pulmonary parenchyma,and cardiac situs, size, and morphology.Although its role in cardiopulmonary assessmentwhen compared with cross-sectional echocar-diographic techniques is challenged, its availabil-ity, speed, and usefulness in providing informa-tion about pulmonary features suggest that itsfuture as an imaging modality remains secure.
Evaluation of pulmonary hemodynamics bychest radiography includes assessment of pul-monary ventilation and perfusion. Evaluation ofperfusion by pulmonary vasculature assessmentin chest radiographs is useful to distinguish thepathophysiology of altered pulmonary hemody-namics in children with congenital heart disease.For example, specific diagnostic entities can beconsidered by evaluating the pulmonary vascu-larity. Pulmonary vascularity on a posteroanteri-or chest radiograph can be classified as normal,increased (Fig. 43-7), decreased (Fig. 43-8), orabnormally redistributed and for which eachlung field must be compared with the otherfields. For pulmonary arterial vasculature to beidentified as increased by chest radiography, anincrease in pulmonary blood flow of approxi-mately 100% is required. This helps to evaluatechildren with left-to-right shunting and correlatephysical examination findings. An increase inCO of a similar amount (approximately 100%) isnecessary to auscultate an early diastolic ven-tricular filling murmur across either AV valve.
Diminished pulmonary vasculature typicallyrepresents obstruction of blood flow to thelungs and is an ominous radiographic finding innewborns. Central dilation and peripheral prun-ing of pulmonary arterial vessels is noted inmore advanced pulmonary vascular diseaseand is found with evidence for RV hypertrophyas defined by retrosternal filling on the lateralchest radiograph with the cardiac silhouette.
425

Perspiration and tense, anxious facies
Flared nostrils
Sternal retraction
Intercostal retractions
Infant with respiratory distress (including orthopnea and tachypnea) caused by pulmonary volume overload
Clinical Characteristics of Too Much Pulmonary Flow(Pulmonary Volume Overload)
CONGENITAL HEART DISEASE
AN APPROACH TO CHILDREN WITH SUSPECTED CHD
426
Figure 43-6
Pulmonary edema presents a more distinctivepattern of haziness in the lung fields that war-rants immediate investigation about etiologybecause significantly increased morbidity andmortality are associated with this finding. Specif-ic assessment of the size of the main pulmonaryartery is possible by means of the chest radi-
ograph. Because the pulmonary artery is thinwalled, it dilates readily when exposed toincreased flow or pressure. Dilation of the mainpulmonary artery is readily visible on the chestradiograph, and differentiating radiographic fea-tures are then sought to determine the physio-logic etiology.

CONGENITAL HEART DISEASE
AN APPROACH TO CHILDREN WITH SUSPECTED CHD
Anomalies of the Ventricular Septum
VentricularseptaldefectECG
X-ray: Ventricular septal defect in a 5-year-old boy
L. ventricular angiocardiogram: AO, aorta; PT, pulmonary trunk; LV, left ventricle; RV, right ventricle; VSD, ventricular septal defect
AOPT
LV
VSD
RV
1 2 3 aVLaVR aVF V1 V2 V3 V4 V5 V6
427
Figure 43-7
Anomalies of the Right Ventricular Outflow Tract1 2 3 aVLaVR aVF V1 V2 V3 V4 V5 V6
X-ray: Tetralogy of Fallot in a 6-year-old boy R. ventricular angiocardiogram: AO, aorta; PV, pulmonary valve; RV, right ventricle; Infund, infundibulum
Tetralogy of Fallot ECG
AO
PV
RV
Infund
Figure 43-8
Evaluation of lung ventilation by assessment ofconducting airways and lung parenchyma,including lobar and lung volumes, providesinformation about pulmonary physiology. Evalu-ation of the cardiac situs and chamber enlarge-
ment by cardiac contour evaluation can greatlyaid in the assessment of altered pulmonaryhemodynamics. Because the right ventricle isaffected by altered pulmonary hemodynamics,attention must be given to changes in shape and

size. However, defining changes in RV functionby means of chest radiography is less sensitiveand specific than by means of evaluation of pul-monary perfusion.
Additional noninvasive assessment of childrenwith congenital heart disease includes applica-tion of echocardiographic techniques (chapter44). Less frequently, an invasive approach,involving cardiac catheterization, is required(chapter 45).
FUTURE DIRECTIONS Clinical emphasis has focused on optimizing
diagnosis and treatment of children with con-genital heart disease and including fetuses aspatients. In the future, the clinical focus willinclude the prevention of congenital heart dis-ease through a more complete understanding ofthe influence of cardiac development. Comple-tion of the initial mapping phase of the HumanGenome Project in 2003 will result in accelerat-ed investigations into the control and modula-tion of gene expression in the development ofthe human heart. This expanded understandingof cardiac development may allow interventions
CONGENITAL HEART DISEASE
AN APPROACH TO CHILDREN WITH SUSPECTED CHD
to augment specific structural and functionaldeficiencies and to prevent maldevelopment ofthe human heart.
REFERENCESDenfield S, Henry GW. Postoperative cardiac intensive care.
In: Long WA, ed. Neonatal and Fetal Cardiology. Philadel-phia: WB Saunders; 1990:812–829.
Ha B, Henry W, Lucas C, et al. Pulmonary artery blood flowand hemodynamics. In: Advances in Hemodynamics andHemorheology. Vol 1. Greenwich, CT: Jai Press;1996:230–324.
Henry GW. Perioperative management of the child with pul-monary hypertension and congenital heart disease. In:Harned HS Jr, ed. Pediatric Pulmonary Heart Disease.Boston: Little Brown; 1990:355–375.
Hoffman JIE. Incidence, mortality and natural history. In:Anderson RH, Baker EJ, Macartney FJ, et al., eds. Paedi-atric Cardiology. 2nd ed. London: Churchill Livingstone;2002:111–139.
Keith JD. History and physical examination. In: Keith JD,Rowe RD, Vlad P. Heart Disease in Infancy and Childhood.3rd ed. New York: Macmillan; 1987:14–15.
Long WA, Henry GW. Autonomic and central neuroregula-tion of fetal cardiovascular function. In: Polin RA, FoxWW, eds. Fetal and Neonatal Physiology. 2nd ed. Philadel-phia: WB Saunders; 1998:943–961.
Rudolph AM. Congenital Disease of the Heart. Chicago:Yearbook Medical Publishers; 1974:29–48.
428