Embed Size (px)
Citation preview
SECTION: Toxicological Emergencies REVISED: 06/2017
Section
7 T
OX
ICO
LO
GIC
AL
EM
ER
GE
NC
IES
1. Medical – Overdose/Poisoning – Opioid Protocol 7 - 1
2. Medical – Overdose/Poisoning – Stimulant Protocol 7 - 2
3. Medical – Overdose/Poisoning – Tricyclic Anti-depressant
Protocol 7 - 3
4. Exposure – Organophosphate Protocol 7 - 4
5. Medical – Overdose/Poisoning – Calcium Channel Blocker
Protocol 7 - 5
6. Medical – Overdose/Poisoning – Beta Blocker
Protocol 7 - 6
Section
7 Continued
TO
XIC
OL
OG
ICA
L E
ME
RG
EN
CIE
S
This page intentionally left blank.
SECTION: Toxicological Emergencies PROTOCOL TITLE: Medical – Overdose/Poisoning – Opioid REVISED: 06/2017
Protocol
7-1 O
PIA
TE
OV
ER
DO
SE
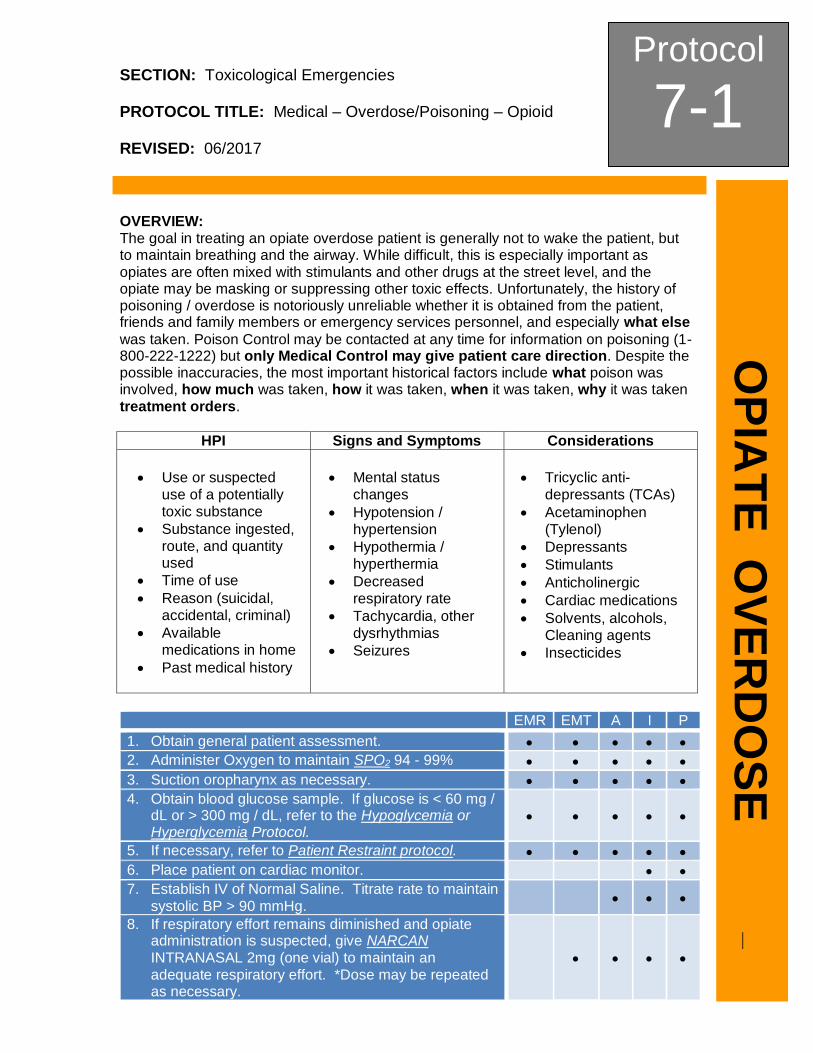
OVERVIEW: The goal in treating an opiate overdose patient is generally not to wake the patient, but to maintain breathing and the airway. While difficult, this is especially important as opiates are often mixed with stimulants and other drugs at the street level, and the opiate may be masking or suppressing other toxic effects. Unfortunately, the history of poisoning / overdose is notoriously unreliable whether it is obtained from the patient, friends and family members or emergency services personnel, and especially what else
was taken. Poison Control may be contacted at any time for information on poisoning (1-800-222-1222) but only Medical Control may give patient care direction. Despite the possible inaccuracies, the most important historical factors include what poison was involved, how much was taken, how it was taken, when it was taken, why it was taken treatment orders.
HPI Signs and Symptoms Considerations
Use or suspected use of a potentially toxic substance
Substance ingested, route, and quantity used
Time of use
Reason (suicidal, accidental, criminal)
Available medications in home
Past medical history
Mental status changes
Hypotension / hypertension
Hypothermia / hyperthermia
Decreased respiratory rate
Tachycardia, other dysrhythmias
Seizures
Tricyclic anti-depressants (TCAs)
Acetaminophen (Tylenol)
Depressants
Stimulants
Anticholinergic
Cardiac medications
Solvents, alcohols, Cleaning agents
Insecticides
EMR EMT A I P
1. Obtain general patient assessment.
2. Administer Oxygen to maintain SPO2 94 - 99%
3. Suction oropharynx as necessary.
4. Obtain blood glucose sample. If glucose is < 60 mg / dL or > 300 mg / dL, refer to the Hypoglycemia or Hyperglycemia Protocol.
5. If necessary, refer to Patient Restraint protocol.
6. Place patient on cardiac monitor.
7. Establish IV of Normal Saline. Titrate rate to maintain systolic BP > 90 mmHg.
8. If respiratory effort remains diminished and opiate administration is suspected, give NARCAN INTRANASAL 2mg (one vial) to maintain an adequate respiratory effort. *Dose may be repeated as necessary.

Protocol
7-1 Continued
OP
IAT
E
OV
ER
DO
SE
EMR EMT A I P
a. If respiratory effort remains diminished and opiate administration is suspected, give NARCAN 0.4 - 2.0 mg slow IVP/IM (ALS levels only) to maintain an adequate respiratory effort. Dose may be repeated as necessary.
9. Transport promptly in position of comfort. Reassess VS as indicated.
Opiate Toxidrome
Altered Mental Status
Miosis
Unresponsiveness
Shallow Respirations
Slow Respiratory Rate
Decreased Bowel Sounds
Hypothermia
Hypotension
PEARLS: 1. If patient is a suspected opiate addict, the administration of Naloxone should be titrated to increase
respirations to normal levels without fully awakening patient to prevent hostile and confrontational episodes and withdrawal symptoms.
2. Any patient receiving Naloxone should be transported for continued monitoring. Many opiates have a longer bioavailability than Naloxone, therefore re-sedation may occur.
3. Do not rely on patient history of ingestion, especially in suicide attempts. 4. The administration of Naloxone should be titrated to increase respirations to normal levels without fully
awakening patient to prevent hostile and confrontational episodes and withdrawal symptoms. 5. Any patient receiving Naloxone should be transported for continued monitoring. Some opiates may
have a longer bioavailability than Naloxone, therefore re-sedation may occur. 6. Some opiates may require significant Naloxone dosing. 7. Do not rely completely on patient history of ingestion (route, dose, substance), especially in suicide
attempts. 8. Providers who may encounter fentanyl or fentanyl analogs should be trained to recognize the symptoms
and objective signs of opioid intoxication, have naloxone readily available, and trained to administer naloxone.
9. For opioid toxicity to occur the drug must enter the blood and brain from the environment. Toxicity cannot occur from simply being in proximity to the drug.
10. Toxicity may occur in canines utilized to detect drug. The risks are not equivalent to those in humans given the distinct contact that dogs, and not humans, have with the local environment.
11. Nitrile gloves provide sufficient protection against dermal absorption. In situations where an enclosed space is heavily contaminated with a potential highly potent opioid, water resistant coveralls should be worn.
12. Incidental dermal exposures should immediately be washed with copious amounts of water. 13. Alcohol based hand sanitizers should not be used for decontamination as they do not wash opioids off
the skin and may increase dermal drug absorption. 14. In the unusual circumstance of significant airborne suspension of powdered opioids, a properly fitted
N95 respirator is likely to provide reasonable respiratory protection. 15. OSHA-approved protection for eyes and face should be used during tasks where there exists possibility
of splash to the face.
SECTION: Toxicological Emergencies PROTOCOL TITLE: Medical – Overdose/Poisoning – Stimulant REVISED: 06/2017
Protocol
7-2 S
TIM
UL
AN
T O
VE
RD
OS
E
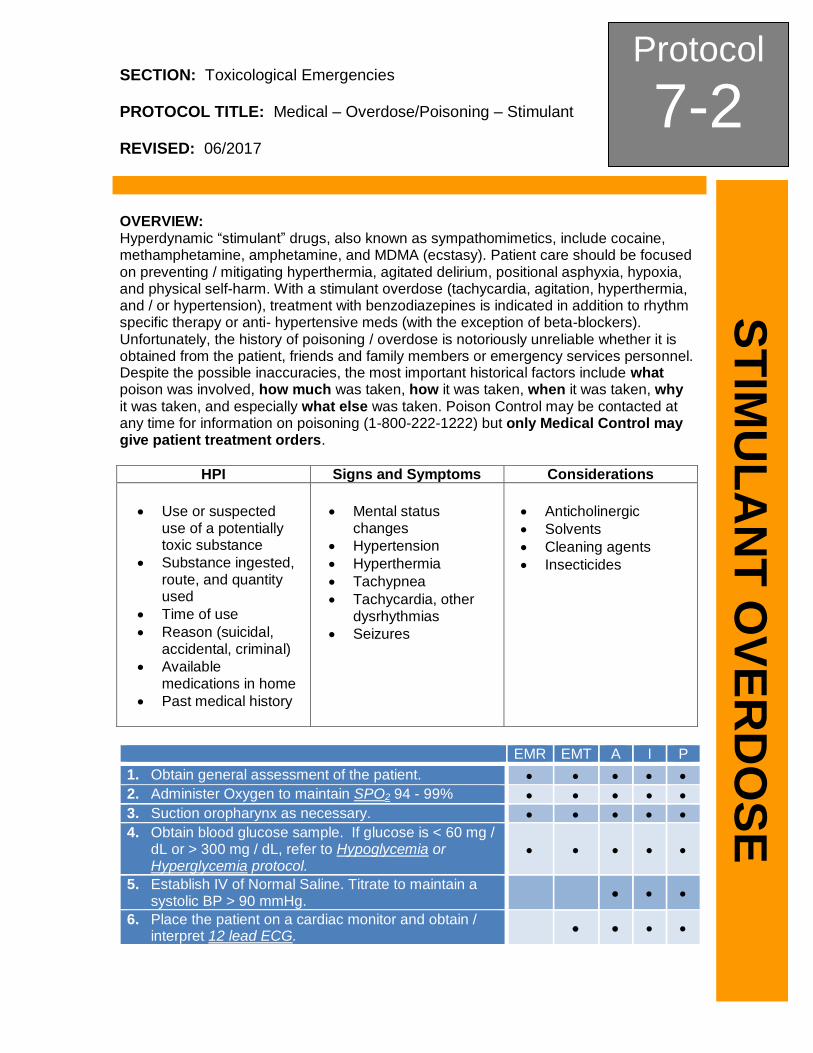
OVERVIEW: Hyperdynamic “stimulant” drugs, also known as sympathomimetics, include cocaine, methamphetamine, amphetamine, and MDMA (ecstasy). Patient care should be focused on preventing / mitigating hyperthermia, agitated delirium, positional asphyxia, hypoxia, and physical self-harm. With a stimulant overdose (tachycardia, agitation, hyperthermia, and / or hypertension), treatment with benzodiazepines is indicated in addition to rhythm specific therapy or anti- hypertensive meds (with the exception of beta-blockers). Unfortunately, the history of poisoning / overdose is notoriously unreliable whether it is obtained from the patient, friends and family members or emergency services personnel. Despite the possible inaccuracies, the most important historical factors include what poison was involved, how much was taken, how it was taken, when it was taken, why it was taken, and especially what else was taken. Poison Control may be contacted at any time for information on poisoning (1-800-222-1222) but only Medical Control may give patient treatment orders.
HPI Signs and Symptoms Considerations
Use or suspected use of a potentially toxic substance
Substance ingested, route, and quantity used
Time of use
Reason (suicidal, accidental, criminal)
Available medications in home
Past medical history
Mental status changes
Hypertension
Hyperthermia
Tachypnea
Tachycardia, other dysrhythmias
Seizures
Anticholinergic
Solvents
Cleaning agents
Insecticides
EMR EMT A I P
1. Obtain general assessment of the patient.
2. Administer Oxygen to maintain SPO2 94 - 99%
3. Suction oropharynx as necessary.
4. Obtain blood glucose sample. If glucose is < 60 mg / dL or > 300 mg / dL, refer to Hypoglycemia or Hyperglycemia protocol.
5. Establish IV of Normal Saline. Titrate to maintain a systolic BP > 90 mmHg.
6. Place the patient on a cardiac monitor and obtain / interpret 12 lead ECG.
Protocol
7-2 Continued
ST
IMU
LA
NT
OV
ER
DO
SE
EMR EMT A I P
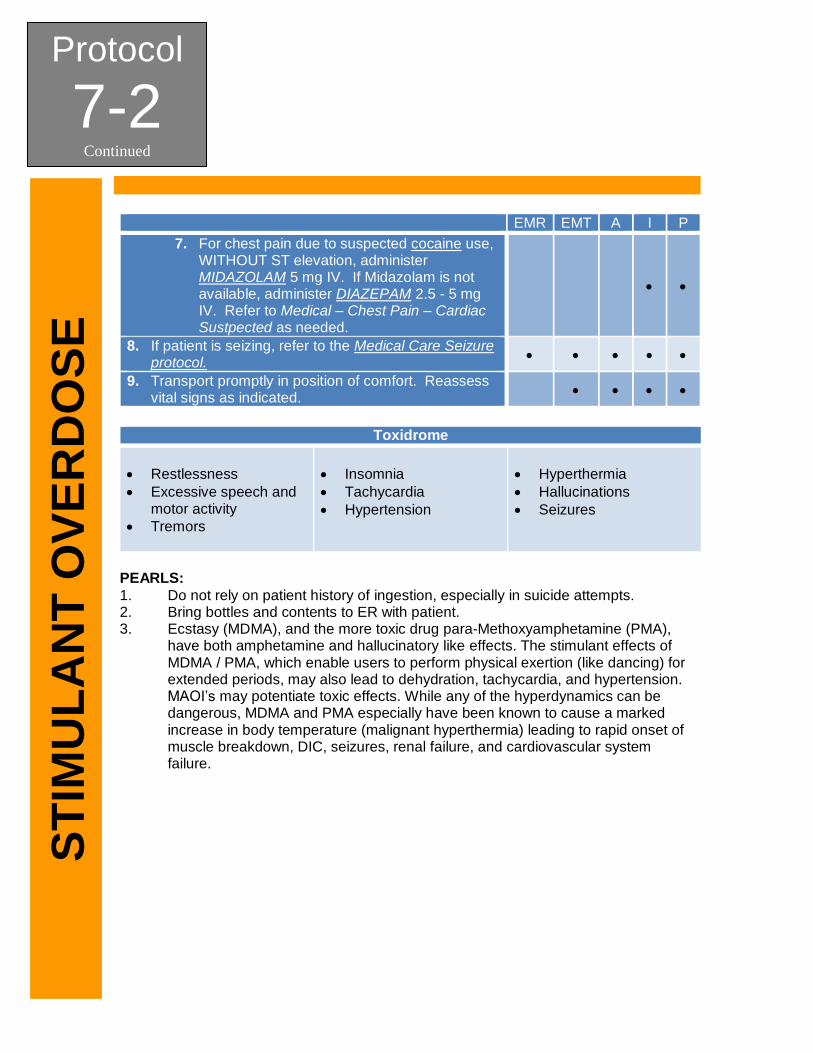
7. For chest pain due to suspected cocaine use, WITHOUT ST elevation, administer MIDAZOLAM 5 mg IV. If Midazolam is not available, administer DIAZEPAM 2.5 - 5 mg IV. Refer to Medical – Chest Pain – Cardiac Sustpected as needed.
8. If patient is seizing, refer to the Medical Care Seizure protocol.
9. Transport promptly in position of comfort. Reassess vital signs as indicated.
PEARLS:
1. Do not rely on patient history of ingestion, especially in suicide attempts. 2. Bring bottles and contents to ER with patient. 3. Ecstasy (MDMA), and the more toxic drug para-Methoxyamphetamine (PMA),
have both amphetamine and hallucinatory like effects. The stimulant effects of MDMA / PMA, which enable users to perform physical exertion (like dancing) for extended periods, may also lead to dehydration, tachycardia, and hypertension. MAOI’s may potentiate toxic effects. While any of the hyperdynamics can be dangerous, MDMA and PMA especially have been known to cause a marked increase in body temperature (malignant hyperthermia) leading to rapid onset of muscle breakdown, DIC, seizures, renal failure, and cardiovascular system failure.
Toxidrome
Restlessness
Excessive speech and motor activity
Tremors
Insomnia
Tachycardia
Hypertension
Hyperthermia
Hallucinations
Seizures
SECTION: Toxicological Emergencies PROTOCOL TITLE: Medical – Overdose/Poisoning – Tricyclic Anti-depressant REVISED: 06/2017
Protocol
7-3 T
RIC
YC
LIC
AN
TID
EP
RE
SS
AN
T
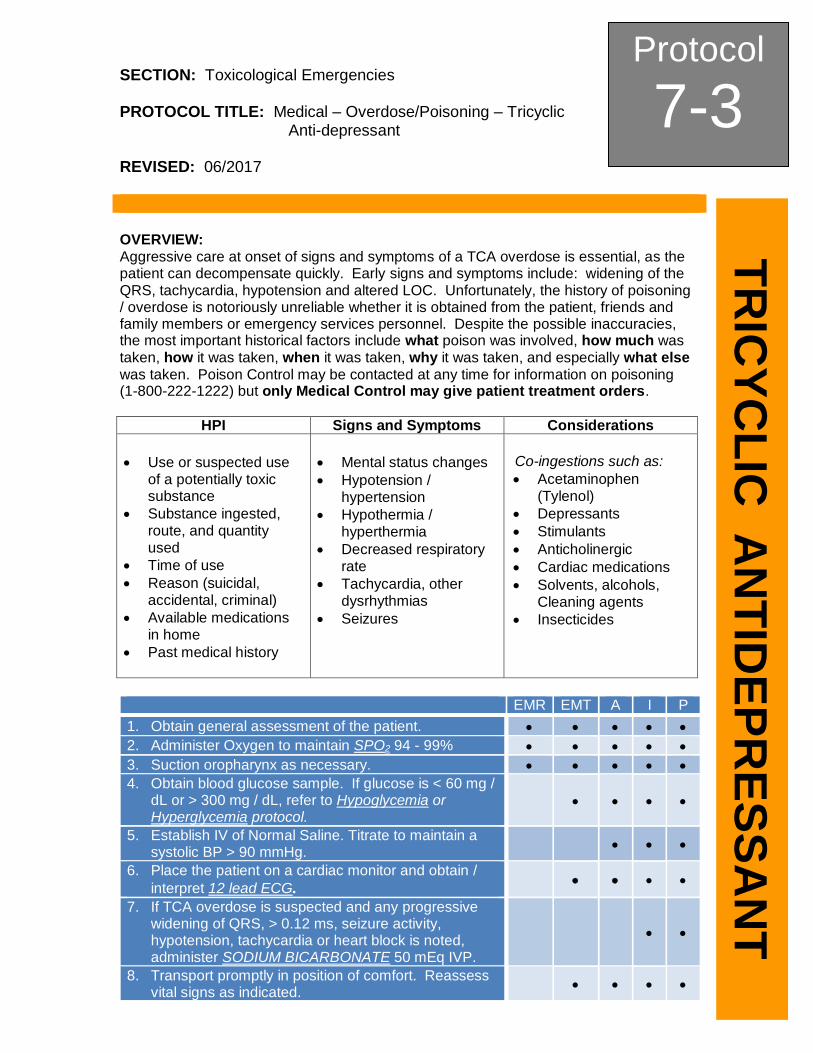
OVERVIEW: Aggressive care at onset of signs and symptoms of a TCA overdose is essential, as the patient can decompensate quickly. Early signs and symptoms include: widening of the QRS, tachycardia, hypotension and altered LOC. Unfortunately, the history of poisoning / overdose is notoriously unreliable whether it is obtained from the patient, friends and family members or emergency services personnel. Despite the possible inaccuracies, the most important historical factors include what poison was involved, how much was taken, how it was taken, when it was taken, why it was taken, and especially what else was taken. Poison Control may be contacted at any time for information on poisoning (1-800-222-1222) but only Medical Control may give patient treatment orders.
HPI Signs and Symptoms Considerations
Use or suspected use of a potentially toxic substance
Substance ingested, route, and quantity used
Time of use
Reason (suicidal, accidental, criminal)
Available medications in home
Past medical history
Mental status changes
Hypotension / hypertension
Hypothermia / hyperthermia
Decreased respiratory rate
Tachycardia, other dysrhythmias
Seizures
Co-ingestions such as:
Acetaminophen (Tylenol)
Depressants
Stimulants
Anticholinergic
Cardiac medications
Solvents, alcohols, Cleaning agents
Insecticides
EMR EMT A I P
1. Obtain general assessment of the patient.
2. Administer Oxygen to maintain SPO2 94 - 99%
3. Suction oropharynx as necessary.
4. Obtain blood glucose sample. If glucose is < 60 mg / dL or > 300 mg / dL, refer to Hypoglycemia or Hyperglycemia protocol.
5. Establish IV of Normal Saline. Titrate to maintain a systolic BP > 90 mmHg.
6. Place the patient on a cardiac monitor and obtain /
interpret 12 lead ECG.
7. If TCA overdose is suspected and any progressive widening of QRS, > 0.12 ms, seizure activity, hypotension, tachycardia or heart block is noted, administer SODIUM BICARBONATE 50 mEq IVP.
8. Transport promptly in position of comfort. Reassess vital signs as indicated.
Protocol
7-3 Continued
TR
ICY
CL
IC A
NT
IDE
PR
ES
SA
NT
PEARLS: 1. Amiodarone is contraindicated, as are other drugs that widen the QRS. 2. Common TCA’s include but are not limited to: Elavil, Triavil, Etrafon, and
Amitriptyline. 3. Flexeril (cyclobenzaprine) can mimic TCA overdose. 4. Do not rely on patient history of ingestion, especially in suicide attempts. 5. Bring bottles and contents to ER with patient.
SECTION: Toxicological Emergencies PROTOCOL TITLE: Exposure – Organophosphate REVISED: 06/2017
Protocol
7-4 O
RG
AN
OP
HO
SP
HA
TE
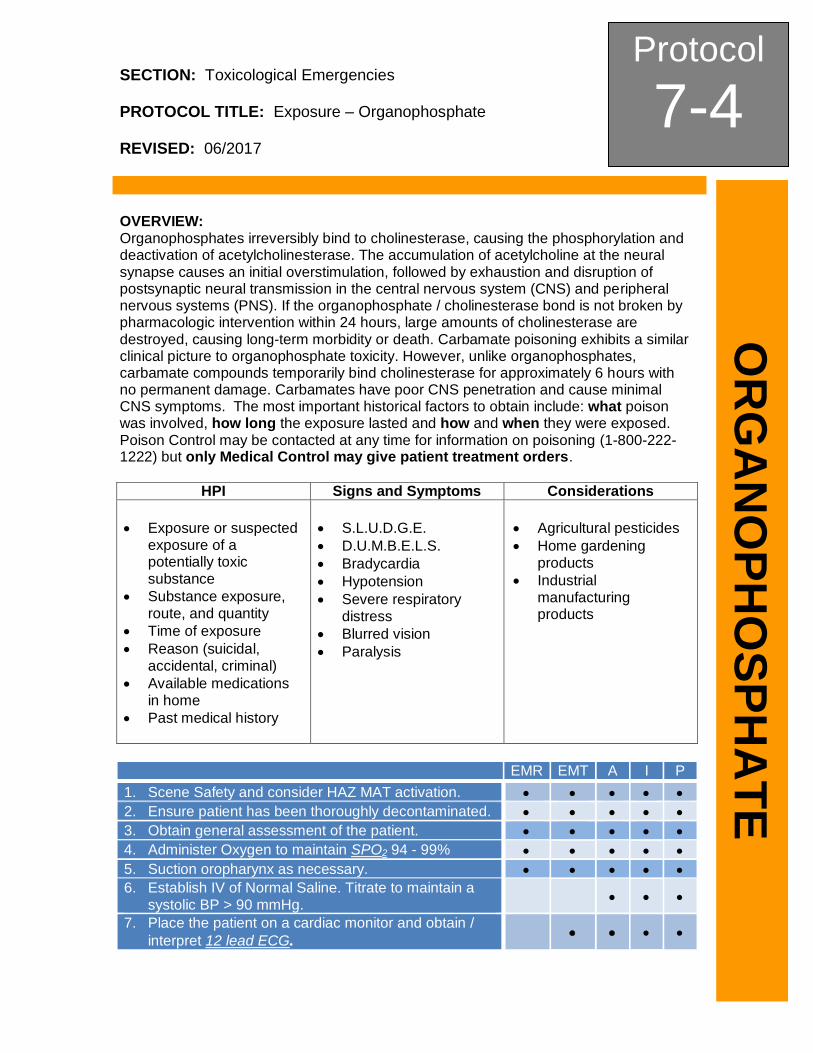
OVERVIEW: Organophosphates irreversibly bind to cholinesterase, causing the phosphorylation and deactivation of acetylcholinesterase. The accumulation of acetylcholine at the neural synapse causes an initial overstimulation, followed by exhaustion and disruption of postsynaptic neural transmission in the central nervous system (CNS) and peripheral nervous systems (PNS). If the organophosphate / cholinesterase bond is not broken by pharmacologic intervention within 24 hours, large amounts of cholinesterase are destroyed, causing long-term morbidity or death. Carbamate poisoning exhibits a similar clinical picture to organophosphate toxicity. However, unlike organophosphates, carbamate compounds temporarily bind cholinesterase for approximately 6 hours with no permanent damage. Carbamates have poor CNS penetration and cause minimal CNS symptoms. The most important historical factors to obtain include: what poison was involved, how long the exposure lasted and how and when they were exposed. Poison Control may be contacted at any time for information on poisoning (1-800-222-1222) but only Medical Control may give patient treatment orders.
HPI Signs and Symptoms Considerations
Exposure or suspected exposure of a potentially toxic substance
Substance exposure, route, and quantity
Time of exposure
Reason (suicidal, accidental, criminal)
Available medications in home
Past medical history
S.L.U.D.G.E.
D.U.M.B.E.L.S.
Bradycardia
Hypotension
Severe respiratory distress
Blurred vision
Paralysis
Agricultural pesticides
Home gardening products
Industrial manufacturing products
EMR EMT A I P
1. Scene Safety and consider HAZ MAT activation.
2. Ensure patient has been thoroughly decontaminated.
3. Obtain general assessment of the patient.
4. Administer Oxygen to maintain SPO2 94 - 99%
5. Suction oropharynx as necessary.
6. Establish IV of Normal Saline. Titrate to maintain a systolic BP > 90 mmHg.
7. Place the patient on a cardiac monitor and obtain /
interpret 12 lead ECG.
Protocol
7-4 Continued
OR
GA
NO
PH
OS
PH
AT
E
EMR EMT A I P
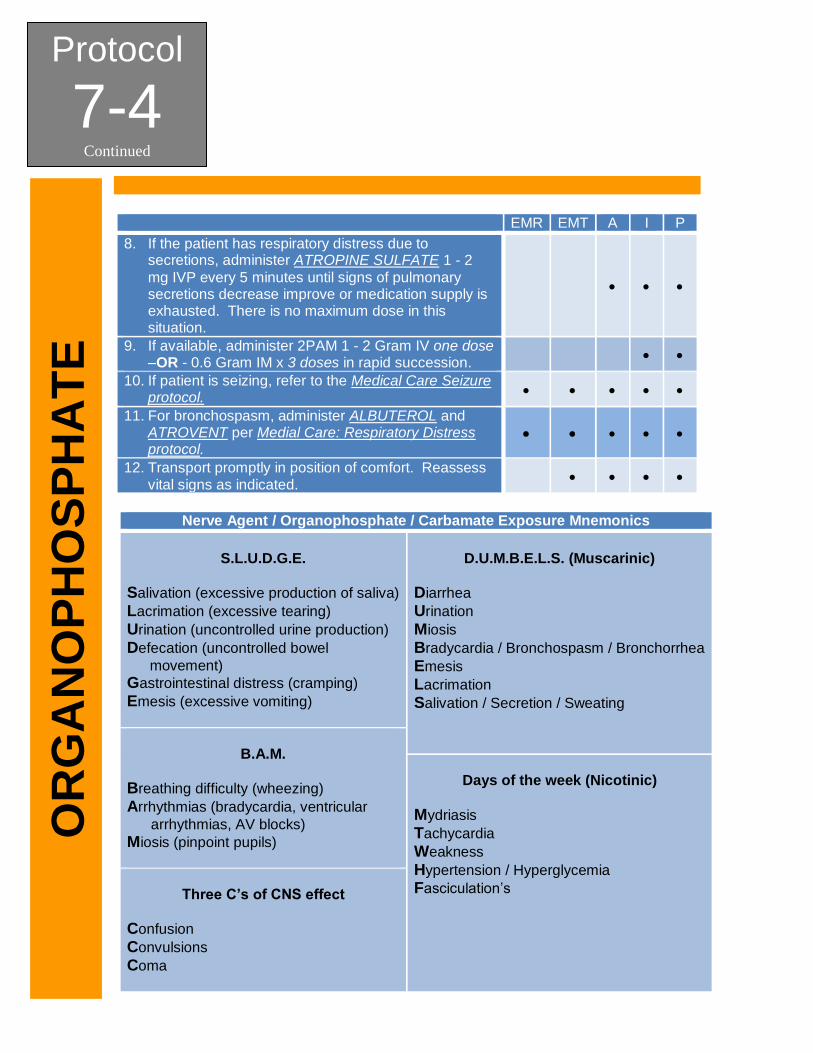
8. If the patient has respiratory distress due to secretions, administer ATROPINE SULFATE 1 - 2
mg IVP every 5 minutes until signs of pulmonary secretions decrease improve or medication supply is exhausted. There is no maximum dose in this situation.
9. If available, administer 2PAM 1 - 2 Gram IV one dose –OR - 0.6 Gram IM x 3 doses in rapid succession.
10. If patient is seizing, refer to the Medical Care Seizure protocol.
11. For bronchospasm, administer ALBUTEROL and ATROVENT per Medial Care: Respiratory Distress protocol.
12. Transport promptly in position of comfort. Reassess vital signs as indicated.
Nerve Agent / Organophosphate / Carbamate Exposure Mnemonics
S.L.U.D.G.E.
Salivation (excessive production of saliva)
Lacrimation (excessive tearing)
Urination (uncontrolled urine production)
Defecation (uncontrolled bowel
movement)
Gastrointestinal distress (cramping)
Emesis (excessive vomiting)
D.U.M.B.E.L.S. (Muscarinic)
Diarrhea
Urination
Miosis
Bradycardia / Bronchospasm / Bronchorrhea
Emesis
Lacrimation
Salivation / Secretion / Sweating
B.A.M.
Breathing difficulty (wheezing)
Arrhythmias (bradycardia, ventricular
arrhythmias, AV blocks)
Miosis (pinpoint pupils)
Days of the week (Nicotinic)
Mydriasis
Tachycardia
Weakness
Hypertension / Hyperglycemia
Fasciculation’s
Three C’s of CNS effect
Confusion
Convulsions
Coma
Protocol
7-4 Continued
OR
GA
NO
PH
OS
PH
AT
E
***Decontamination MUST be completed prior to transport***
PEARLS: 1. Decontamination should be initiated and completed by qualified personnel. 2. Decontamination takes precedence over ALS interventions. 3. Consider calling for additional drug kits for additional atropine. 4. Separate patient from causative agent. Most exposures are to liquid solutions. 5. Clothes should be removed on scene, bagged and sealed by personnel wearing
appropriate PPE, and left for appropriate disposal. DO NOT transport clothes in ambulance or to hospital where they may spread contamination.
6. DO NOT use personal antidote kit, if issued, to provide patient care.

Protocol
7-4 Continued
OR
GA
NO
PH
OS
PH
AT
E
This page intentionally left blank.
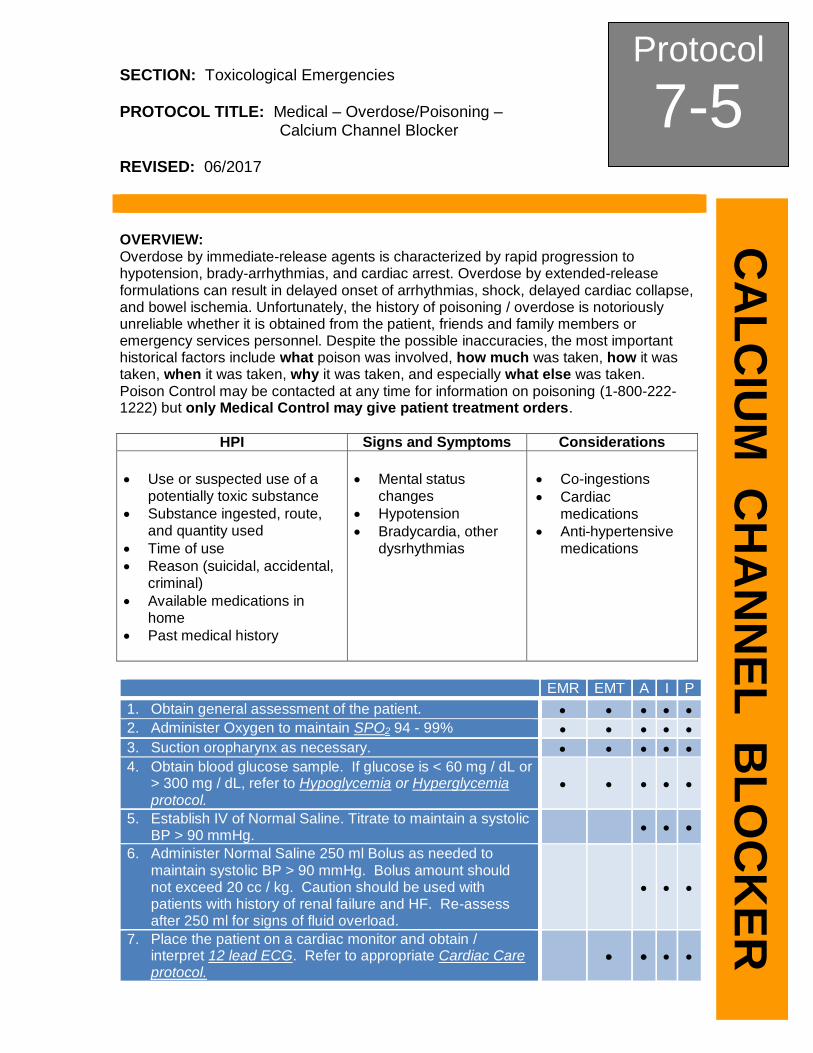
SECTION: Toxicological Emergencies PROTOCOL TITLE: Medical – Overdose/Poisoning – Calcium Channel Blocker REVISED: 06/2017
Protocol
7-5 C
AL
CIU
M C
HA
NN
EL
BL
OC
KE
R
OVERVIEW: Overdose by immediate-release agents is characterized by rapid progression to hypotension, brady-arrhythmias, and cardiac arrest. Overdose by extended-release formulations can result in delayed onset of arrhythmias, shock, delayed cardiac collapse, and bowel ischemia. Unfortunately, the history of poisoning / overdose is notoriously unreliable whether it is obtained from the patient, friends and family members or emergency services personnel. Despite the possible inaccuracies, the most important historical factors include what poison was involved, how much was taken, how it was taken, when it was taken, why it was taken, and especially what else was taken. Poison Control may be contacted at any time for information on poisoning (1-800-222-1222) but only Medical Control may give patient treatment orders.
HPI Signs and Symptoms Considerations
Use or suspected use of a potentially toxic substance
Substance ingested, route, and quantity used
Time of use
Reason (suicidal, accidental, criminal)
Available medications in home
Past medical history
Mental status changes
Hypotension
Bradycardia, other dysrhythmias
Co-ingestions
Cardiac medications
Anti-hypertensive medications
EMR EMT A I P
1. Obtain general assessment of the patient.
2. Administer Oxygen to maintain SPO2 94 - 99%
3. Suction oropharynx as necessary.
4. Obtain blood glucose sample. If glucose is < 60 mg / dL or > 300 mg / dL, refer to Hypoglycemia or Hyperglycemia protocol.
5. Establish IV of Normal Saline. Titrate to maintain a systolic BP > 90 mmHg.
6. Administer Normal Saline 250 ml Bolus as needed to maintain systolic BP > 90 mmHg. Bolus amount should not exceed 20 cc / kg. Caution should be used with patients with history of renal failure and HF. Re-assess after 250 ml for signs of fluid overload.
7. Place the patient on a cardiac monitor and obtain / interpret 12 lead ECG. Refer to appropriate Cardiac Care protocol.
Protocol
7-5 Continued
CA
LC
IUM
C
HA
NN
EL
B
LO
CK
ER
EMR EMT A I P
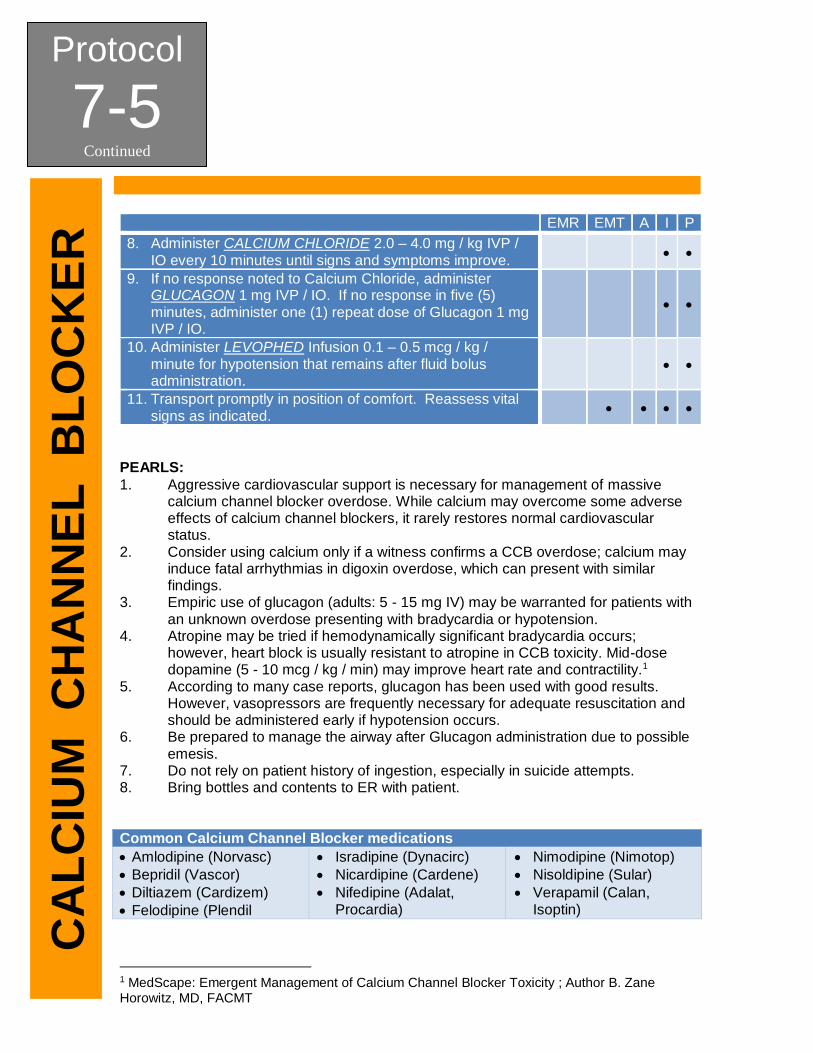
8. Administer CALCIUM CHLORIDE 2.0 – 4.0 mg / kg IVP / IO every 10 minutes until signs and symptoms improve.
9. If no response noted to Calcium Chloride, administer GLUCAGON 1 mg IVP / IO. If no response in five (5) minutes, administer one (1) repeat dose of Glucagon 1 mg IVP / IO.
10. Administer LEVOPHED Infusion 0.1 – 0.5 mcg / kg / minute for hypotension that remains after fluid bolus administration.
11. Transport promptly in position of comfort. Reassess vital signs as indicated.
PEARLS:
1. Aggressive cardiovascular support is necessary for management of massive calcium channel blocker overdose. While calcium may overcome some adverse effects of calcium channel blockers, it rarely restores normal cardiovascular status.
2. Consider using calcium only if a witness confirms a CCB overdose; calcium may induce fatal arrhythmias in digoxin overdose, which can present with similar findings.
3. Empiric use of glucagon (adults: 5 - 15 mg IV) may be warranted for patients with an unknown overdose presenting with bradycardia or hypotension.
4. Atropine may be tried if hemodynamically significant bradycardia occurs; however, heart block is usually resistant to atropine in CCB toxicity. Mid-dose dopamine (5 - 10 mcg / kg / min) may improve heart rate and contractility.1
5. According to many case reports, glucagon has been used with good results. However, vasopressors are frequently necessary for adequate resuscitation and should be administered early if hypotension occurs.
6. Be prepared to manage the airway after Glucagon administration due to possible emesis.
7. Do not rely on patient history of ingestion, especially in suicide attempts. 8. Bring bottles and contents to ER with patient. Common Calcium Channel Blocker medications
Amlodipine (Norvasc)
Bepridil (Vascor)
Diltiazem (Cardizem)
Felodipine (Plendil
Isradipine (Dynacirc)
Nicardipine (Cardene)
Nifedipine (Adalat, Procardia)
Nimodipine (Nimotop)
Nisoldipine (Sular)
Verapamil (Calan, Isoptin)
1 MedScape: Emergent Management of Calcium Channel Blocker Toxicity ; Author B. Zane Horowitz, MD, FACMT
SECTION: Toxicological Emergencies PROTOCOL TITLE: Medical – Overdose/Poisoning – Beta Blocker REVISED: 06/2017
Protocol
7-6 B
ET
A B
LO
CK
ER
OV
ER
DO
SE
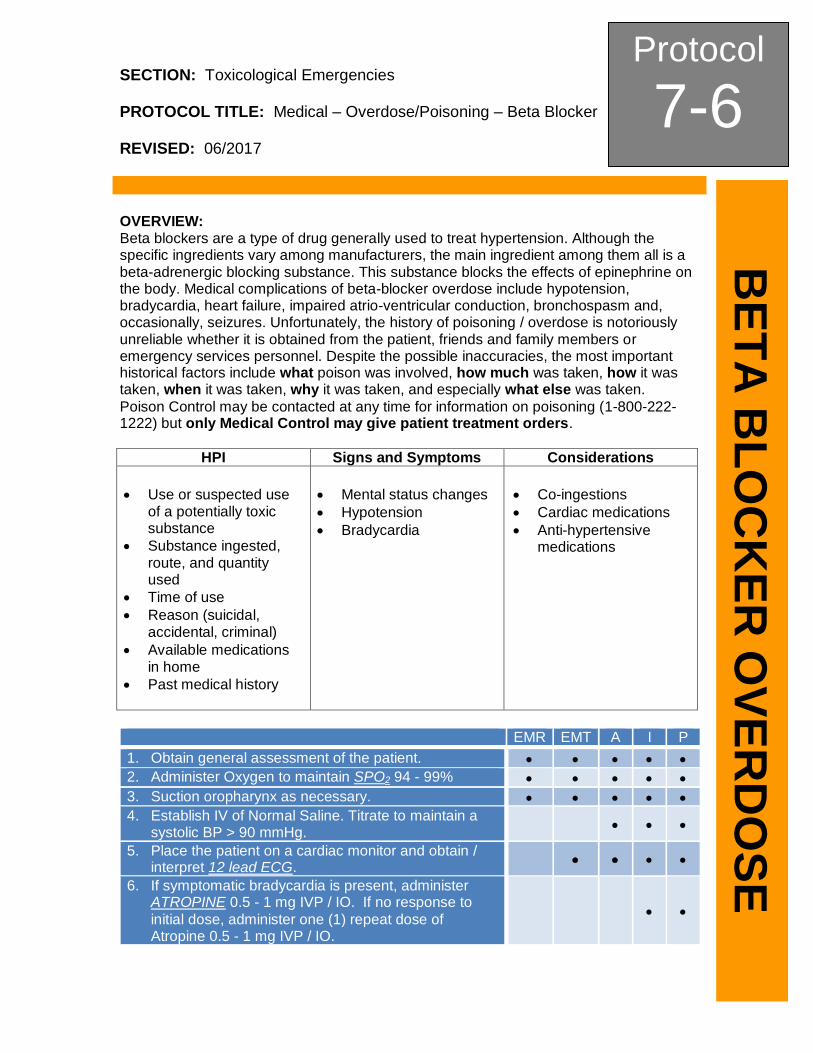
OVERVIEW: Beta blockers are a type of drug generally used to treat hypertension. Although the specific ingredients vary among manufacturers, the main ingredient among them all is a beta-adrenergic blocking substance. This substance blocks the effects of epinephrine on the body. Medical complications of beta-blocker overdose include hypotension, bradycardia, heart failure, impaired atrio-ventricular conduction, bronchospasm and, occasionally, seizures. Unfortunately, the history of poisoning / overdose is notoriously unreliable whether it is obtained from the patient, friends and family members or emergency services personnel. Despite the possible inaccuracies, the most important historical factors include what poison was involved, how much was taken, how it was taken, when it was taken, why it was taken, and especially what else was taken.
Poison Control may be contacted at any time for information on poisoning (1-800-222-1222) but only Medical Control may give patient treatment orders.
HPI Signs and Symptoms Considerations
Use or suspected use of a potentially toxic substance
Substance ingested, route, and quantity used
Time of use
Reason (suicidal, accidental, criminal)
Available medications in home
Past medical history
Mental status changes
Hypotension
Bradycardia
Co-ingestions
Cardiac medications
Anti-hypertensive medications
EMR EMT A I P
1. Obtain general assessment of the patient.
2. Administer Oxygen to maintain SPO2 94 - 99%
3. Suction oropharynx as necessary.
4. Establish IV of Normal Saline. Titrate to maintain a systolic BP > 90 mmHg.
5. Place the patient on a cardiac monitor and obtain / interpret 12 lead ECG.
6. If symptomatic bradycardia is present, administer ATROPINE 0.5 - 1 mg IVP / IO. If no response to
initial dose, administer one (1) repeat dose of Atropine 0.5 - 1 mg IVP / IO.
Protocol
7-6 Continued
BE
TA
BL
OC
KE
R O
VE
RD
OS
E
EMR EMT A I P
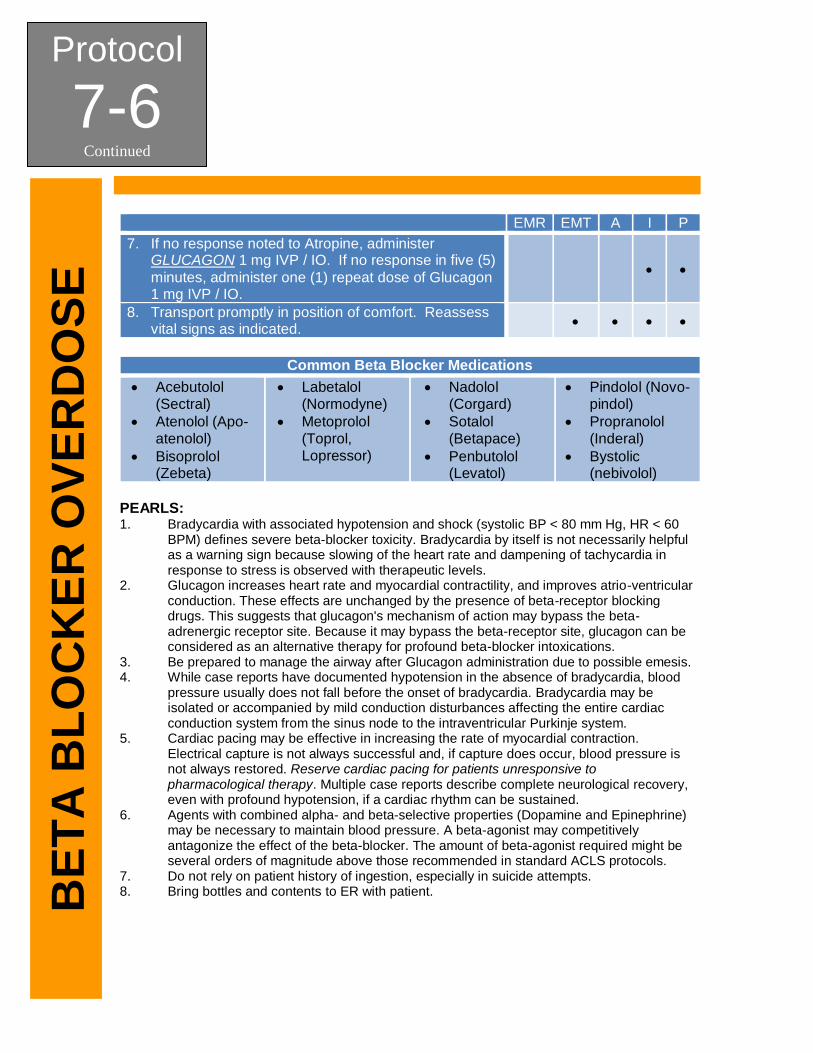
7. If no response noted to Atropine, administer GLUCAGON 1 mg IVP / IO. If no response in five (5)
minutes, administer one (1) repeat dose of Glucagon 1 mg IVP / IO.
8. Transport promptly in position of comfort. Reassess vital signs as indicated.
Common Beta Blocker Medications
Acebutolol (Sectral)
Atenolol (Apo-atenolol)
Bisoprolol (Zebeta)
Labetalol (Normodyne)
Metoprolol (Toprol, Lopressor)
Nadolol (Corgard)
Sotalol (Betapace)
Penbutolol (Levatol)
Pindolol (Novo-pindol)
Propranolol (Inderal)
Bystolic (nebivolol)
PEARLS: 1. Bradycardia with associated hypotension and shock (systolic BP < 80 mm Hg, HR < 60
BPM) defines severe beta-blocker toxicity. Bradycardia by itself is not necessarily helpful as a warning sign because slowing of the heart rate and dampening of tachycardia in response to stress is observed with therapeutic levels.
2. Glucagon increases heart rate and myocardial contractility, and improves atrio-ventricular conduction. These effects are unchanged by the presence of beta-receptor blocking drugs. This suggests that glucagon's mechanism of action may bypass the beta-adrenergic receptor site. Because it may bypass the beta-receptor site, glucagon can be considered as an alternative therapy for profound beta-blocker intoxications.
3. Be prepared to manage the airway after Glucagon administration due to possible emesis. 4. While case reports have documented hypotension in the absence of bradycardia, blood
pressure usually does not fall before the onset of bradycardia. Bradycardia may be isolated or accompanied by mild conduction disturbances affecting the entire cardiac conduction system from the sinus node to the intraventricular Purkinje system.
5. Cardiac pacing may be effective in increasing the rate of myocardial contraction. Electrical capture is not always successful and, if capture does occur, blood pressure is not always restored. Reserve cardiac pacing for patients unresponsive to pharmacological therapy. Multiple case reports describe complete neurological recovery, even with profound hypotension, if a cardiac rhythm can be sustained.
6. Agents with combined alpha- and beta-selective properties (Dopamine and Epinephrine) may be necessary to maintain blood pressure. A beta-agonist may competitively antagonize the effect of the beta-blocker. The amount of beta-agonist required might be several orders of magnitude above those recommended in standard ACLS protocols.
7. Do not rely on patient history of ingestion, especially in suicide attempts. 8. Bring bottles and contents to ER with patient.





























