Embed Size (px)
Citation preview
Strategies for Young Children with Dual Sensory Disabilities The Sooner the Better
For Families and Service Providers – Birth-to-Three and Preschool
Section 5: A Few Handy Forms
• Checklist: B-3 Content on Deaf-Blindness
• Communication Consistency
• Communication Dictionary [template and example]
• Deaf-Blind Census Form
• Likes/Dislikes [template]
• Release of Information (WSDS ROI)
• Routines [template]
• Use of Sensory Channels [template]

B-3 and Preschool Content Checklist: Deaf-Blindness
Child’s Name Date of Birth
Assessment Date Comment Update Comment
Likes/Dislikes Form
Communication Matrix
Preferred Sensory Channels
Home Talk
Home/School Inventory of Problem-Solving Skills
Other:
Building a Foundation Date Comment Update Comment
Access to People, Objects, Activities
Bonding/Relationships
Importance of Routines
Likes/Dislikes
Sensory Channels
Touch
Strategy Introduced Date Comment Update Comment
Active Learning
Choice Making
Co-Active Movement
Cues
1. Touch Cues
2. Object Cues
Greeting/Leaving Rituals
Hand-Under-Hand
Name Cues/Identifiers
Wait Time and Pacing
Other Forms Date Comment Update Comment
Release of Information
Deaf-Blind Census Form

COMMUNICATION CONSISTENCY FORM
Child: ________________________ Date: __________________
Activity Spoken Message Signed Message Object Cue Touch Cue
Communication Consistency/FORMS [Rev. 03/2006]

Communication Dictionary
What she does What we think it means How we respond

Communication Dictionary (Example)
What he does What we think it means How we respond
Head turn, make eye contact, over- exaggerated blink
• In response to “Are you ready?”: he is indicating “yes”
• When initiated it means: “I want to connect.”
In response: you initiate the activity you’ve asked if he is ready for.
When he initiated: initiate interaction.
Look and rapid blink • Typically questioning something: o It may be for reassurance in
unfamiliar settings/situations, “What’s going on?”
o It also might be asking “What’s that?”
o Can also be excitement
Respond to him by describing what’s going on.
Tickling hand with finger when you present your hand to him
Initiation for interaction, might mean: “I’m ready to engage.”
Signing with him and initiating play.
Lifts shoulders, without lifting hands (jerky movements typically-- you might see muscle effort)
“I want to continue this interaction.” Continue interaction using sign and verbal language.
Lifting one hand up Again, this might be inquiry, he might be checking in about a new experience, shows he’s engaged.
Give information about the experience.
Lifting both hands and shoulders up from elbows—hands end in air, curled up
This is a seizure. Provide some verbal reassurance:
“It’s almost done.”
“You’re back.”
Turn toward a person “I’m thinking about you and want to connect with you”—showing he’s engaged.
Give wait time for him to fully turn, then respond with verbal and sign to initiate interaction.
His eyes are almost closed, sneaky peeks
• “I’m tired” or
• “Not yet fully engaged” or
• “I’m not sure about this” or
• “I don’t want to interact”
Be big about engagement (increase volume, big hand movements, motherese—lots of intonation).
Cue him by saying, “Big boy eyes” with gesture.
Use tactile contact with him.
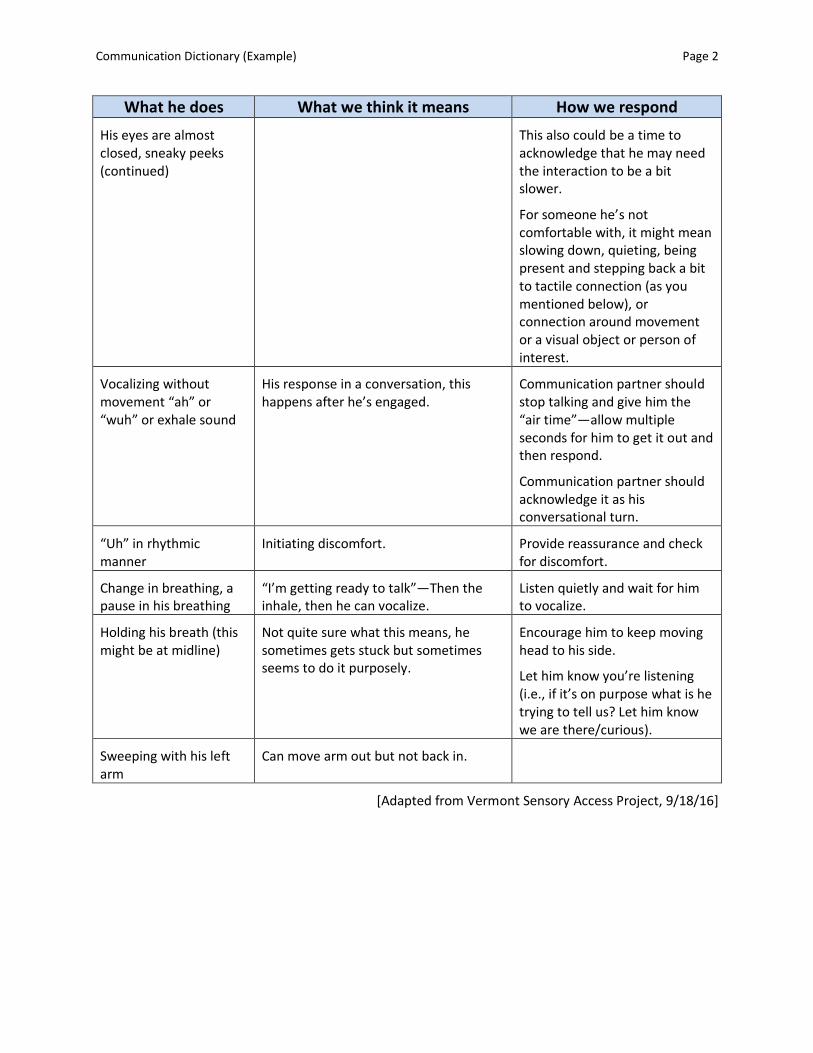
Communication Dictionary (Example) Page 2
What he does What we think it means How we respond
His eyes are almost closed, sneaky peeks (continued)
This also could be a time to acknowledge that he may need the interaction to be a bit slower.
For someone he’s not comfortable with, it might mean slowing down, quieting, being present and stepping back a bit to tactile connection (as you mentioned below), or connection around movement or a visual object or person of interest.
Vocalizing without movement “ah” or “wuh” or exhale sound
His response in a conversation, this happens after he’s engaged.
Communication partner should stop talking and give him the “air time”—allow multiple seconds for him to get it out and then respond.
Communication partner should acknowledge it as his conversational turn.
“Uh” in rhythmic manner
Initiating discomfort. Provide reassurance and check for discomfort.
Change in breathing, a pause in his breathing
“I’m getting ready to talk”—Then the inhale, then he can vocalize.
Listen quietly and wait for him to vocalize.
Holding his breath (this might be at midline)
Not quite sure what this means, he sometimes gets stuck but sometimes seems to do it purposely.
Encourage him to keep moving head to his side.
Let him know you’re listening (i.e., if it’s on purpose what is he trying to tell us? Let him know we are there/curious).
Sweeping with his left arm
Can move arm out but not back in.
[Adapted from Vermont Sensory Access Project, 9/18/16]

⃝New ⃝ Male
⃝ Update
⃝ No change ⃝ Female
FORM TO BE COMPLETED BY THE STUDENT'S TEACHER OR TEAM MEMBER
⃝No longer in district. Moved to: Student’s Last Name Student’s First Name School District _______________________________
⃝SSID#_______________________ Address (10 digit student ID#)
Date of Birth:
City State Zip Code / /
Month Day Year
Parent(s)/Guardian Phone
PRIMARY IDENTIFIED ETIOLOGY: Select ONE from the list below that best describes
the etiology of the individual’s primary disability.
Hereditary/Chromosomal Syndromes and Disorders
101 Aicardi syndrome
102 Alport syndrome
103 Alstrom syndrome
104 Apert syndrome (Acrocephalosyndactyly, Type 1)
105 Bardet-Biedl syndrome (Laurence Moon-Biedl)
106 Batten disease
107 CHARGE association
108 Chromosome 18, Ring 18
109 Cockayne syndrome
110 Cogan Syndrome
111 Cornelia de Lange
112 Cri du chat syndrome (Chromosome 5p-syndrome)
113 Crigler-Najjar syndrome
114 Crouzon syndrome (Craniofacial Dysotosis)
115 Dandy Walker syndrome
116 Down syndrome (Trisomy 21 syndrome)
117 Goldenhar syndrome
118 Hand-Schuller-Christian (Histiocytosis X)
119 Hallgren syndrome
120 Herpes-Zoster (or Hunt)
121 Hunter Syndrome (MPS II)
122 Hurler syndrome (MPS I-H)
123 Kearns-Sayre syndrome
124 Klippel-Feil sequence
125 Klippel-Trenaunay-Weber syndrome
126 Kniest Dysplasia
127 Leber congenital amaurosis
128 Leigh disease
129 Marfan syndrome
130 Marshall syndrome
131 Maroteaux-Lamy syndrome (MPS VI)
132 Moebius syndrome
133 Monosomy 10p
134 Morquio syndrome (MPS IV-B)
135 NF1 - Neurofibromatosis (von Recklinghausen disease)
136 NF2 - Bilateral Acoustic Neurofibromatosis
137 Norrie disease
138 Optico-Cochleo-Dentate Degeneration
139 Pfeiffer syndrome
140 Prader-Willi
141 Pierre-Robin syndrome
142 Refsum syndrome
143 Scheie syndrome (MPS I-S)
144 Smith-Lemli-Opitz (SLO) syndrome
145 Stickler syndrome
146 Sturge-Weber syndrome
147 Treacher Collins syndrome
148 Trisomy 13 (Patau syndrome, Trisomy 13-15)
149 Trisomy 18 (Edwards syndrome)
150 Turner syndrome
151 Usher I syndrome
152 Usher II syndrome
153 Usher III syndrome
154 Vogt-Koyanagi-Harada syndrome
155 Waardenburg syndrome
156 Wildervanck syndrome
157 Wolf-Hirschhorn syndrome (Trisomy 4p)
199 Other __________________________
Pre-Natal/Congenital Complications Post-Natal/Non-Congenital Complications
201 Congenital Rubella Syndrome
202 Congenital Syphilis
203 Congenital Toxoplasmosis
204 Cytomegalovirus (CMV)
205 Fetal Alcohol Syndrome
206 Hydrocephaly
207 Maternal Drug Use
208 Microcephaly
209 Neonatal Herpes Simplex (HSV)
299 Other_______________________
301 Asphyxia
302 Direct Trauma (to the eye and/or ear)
303 Encephalitis
304 Infections
305 Meningitis
306 Severe Head Injury
307 Stroke
308 Tumors
309 Chemically Induced
399 Other _______________________
Related to Prematurity Undiagnosed
401 Complications of Prematurity 501 No Determination of Etiology
National Deaf-Blind Census: Individual Entry Form

RACE ETHNICITY: CHECK ONE BOX ONLY
⃝1. American Indian or Alaska Native ⃝ 3. Black or African American ⃝ 5. White ⃝ 7. Two or more races
⃝2. Asian ⃝ 4. Hispanic/Latino ⃝ 6. Native Hawaiian or Pacific Islander
VISUAL IMPAIRMENT: PRIMARY CLASSIFICATION OF VISUAL IMPAIRMENT
CHECK ONE BOX ONLY
⃝1. Low Vision (visual acuity of 20/70 to 20/200 or more in the better eye with correction.)
⃝2. Legally Blind (visual acuity of 20/200 or less or field restriction of 20 degrees or less in the
better eye with correction.)
⃝3. Light Perception Only
⃝4. Totally Blind
⃝6. Diagnosed Progressive Loss
⃝7. Further Testing Needed to Determine Visual Impairment
⃝9. Documented Functional Vision Loss
CHECK IF APPLICABLE
Cortical Vision Impairment
⃝ 1. Yes
⃝ 0. No
⃝ 2. Unknown
HEARING IMPAIRMENT: PRIMARY CLASSIFICATION OF HEARING IMPAIRMENT
CHECK ONE BOX ONLY
⃝1. Mild (26-40 dB loss)
⃝2. Moderate (41-55 dB loss)
⃝3. Moderately Severe (56-70 dB loss)
⃝4. Severe (71-90 dB loss)
⃝5. Profound (91+ dB loss)
⃝6. Diagnosed Progressive Loss
⃝7. Further Testing Needed to Determine Hearing Impairment
⃝9. Documented Functional Hearing Loss
CHECK EITHER “NO,” “YES,” OR “UNKNOWN”
Central Auditory Processing Disorder
⃝1. Yes ⃝ 0. No ⃝ 2. Unknown
Auditory Neuropathy
⃝ 1. Yes ⃝ 0. No ⃝ 2. Unknown
Cochlear Implant
⃝ 1. Yes ⃝ 0. No ⃝ 2. Unknown
Other Impairments: Indicate impairments, in addition to the individual’s hearing and visual impairments, that have a
significant impact on the individual’s development or educational progress.
CHECK ALL CATEGORIES AS EITHER “NO” OR “YES”
1. Orthopedic/Physical Impairments ⃝ 1. Yes ⃝ 0. No
2. Cognitive Impairments ⃝ 1. Yes ⃝ 0. No
3. Behavioral Disorders ⃝ 1. Yes ⃝ 0. No
4. Complex Health Care Needs ⃝ 1. Yes ⃝ 0. No
5. Communication, Speech and/or Language ⃝ 1. Yes ⃝ 0. No
6. Other Impairment(s) ⃝ 1. Yes ⃝ 0. No (Specify)
PART C (BIRTH THROUGH 2 YRS.) CATEGORY CODES: CHECK ONE BOX ONLY
⃝ 1.At-risk for developmental delays (as defined by the state’s Part C Lead Agency)
⃝ 2. Developmentally Delayed
⃝ 888. Not Reported under Part C of IDEA
PART B (3 THROUGH 21 YRS.) CATEGORY CODES*: CHECK ONE BOX ONLY
⃝1. Intellectual Disability
⃝2. Hearing Impaired/Deaf
⃝3. Speech or Language Impairment
⃝4. Visually Impaired/Blind
⃝5. Emotional/Behavioral
⃝6. Orthopedic Impairment
⃝7. Other Health Impairment
⃝8. Specific Learning Disability
⃝9. Deaf-Blindness
⃝10. Multiple Disabilities
⃝11. Autism
⃝12. Traumatic Brain Injury
⃝13. Developmentally Delayed (age 3 to 9)
⃝14. Non-Categorical
⃝888. Not Reported under Part B of IDEA
*As child was reported on December 1 Child Count

EDUCATIONAL SETTING: CHECK ONE BOX ONLY
Birth through Age 2
⃝1. Home ⃝2. Community-based settings ⃝3. Other settings (specify): Ages 3 - 5
⃝1. Attending a regular early childhood program at least 80% of the time
⃝2. Attending a regular early childhood program 40% to 79% of the time
⃝3. Attending a regular early childhood program less than 40% of the
time
⃝4. Attending a separate class
⃝5. Attending a separate school
⃝6. Attending a residential facility
⃝7. Service provider location
⃝8. Home
Ages 6 – 21 ⃝9. Inside the regular class 80% or more of day
⃝10. Inside the regular class 40% to 79% of the day
⃝11. Inside the regular class less than 40% of the day
⃝12. Separate School
⃝13. Residential facility
⃝14. Homebound/Hospital
⃝15. Correctional facilities
⃝16. Parentally placed in private schools, including home
schooled
PARTICIPATION IN STATEWIDE ASSESSMENTS: CHECK ONE BOX ONLY ~ TAKEN FROM THE LAST STATEWIDE ASSESSMENT ⃝1. Regular grade-level state assessment
⃝2. Regular grade-level state assessment with
accommodations
⃝3. Alternate assessments aligned with grade-level
achievement standards
⃝4. Not Used
⃝5. Not Used
⃝6. Not yet required
⃝7. Parent Opt Out
PART C (BIRTH THROUGH 2 YRS.) EXITING: CHECK ONE BOX ONLY
NOTE: CHILDREN WHO HAVE TURNED AGE 3 AND TRANSITIONED FROM PART C TO PART B DURING THE REPORTING PERIOD MAY BE
REPORTED UNDER BOTH PART C AND PART B.
⃝ 0. In a Part C early intervention program
⃝ 1. Completion of IFSP prior to reaching maximum age for Part C
⃝ 2. Eligible for IDEA, Part B
⃝ 3. Not eligible for Part B, exit with referrals to other programs
⃝ 4. Not eligible for Part B, exit with no referrals
⃝ 5. Part B eligibility not determined
⃝ 6. Deceased
⃝ 7. Moved out of state
⃝ 8. Withdrawal by parent (or guardian)
⃝ 9.Attempts to contact parent and/or child were unsuccessful
PART B (3 YRS. THROUGH 21 YRS.) EXITING: CHECK ONE BOX ONLY
NOTE: CHILDREN WHO HAVE TURNED AGE 3 AND TRANSITIONED FROM PART C TO PART B DURING THE REPORTING PERIOD MAY BE
REPORTED UNDER BOTH PART C AND PART B.
⃝0. In ECSE or school-aged special education program
⃝1. Transferred to regular education
⃝2. Graduated with regular diploma
⃝3. Received a certificate
⃝ 4. Reached maximum age
⃝ 5. Deceased ⃝ 6. Moved, known to be continuing.
School district moved to:
⃝ 8. Dropped out
DEAF-BLIND PROJECT EXITING STATUS: CHECK ONE BOX ONLY
⃝ 1. Eligible to receive services from the deaf-blind project ⃝ 2. No longer eligible to receive services from the deaf-blind project
LIVING SETTING: CHECK ONE BOX ONLY
⃝1. Home: Birth/Adoptive Parents
⃝2. Home: Extended Family
⃝3. Home: Foster Parents
⃝4. State Residential Facility
⃝5. Private Residential Facility
⃝6. Group Home (less than 6 residents)
⃝7. Group Home (6 or more residents)
⃝8. Apartment (with non-family person(s))
⃝9. Pediatric Nursing Home
⃝555. Other (Specify)
ASSISTIVE DEVICES: CHECK EITHER “NO,” “YES,” OR “UNKNOWN”
Glasses or contact lenses used:
⃝1. Yes ⃝ 0. No ⃝ 2. Unknown
Hearing aids, FM system or other listening device used:
⃝1. Yes ⃝ 0. No ⃝ 2. Unknown
Additional assistive technology other than corrective lenses or
assistive listening devices:
⃝ 1. Yes ⃝ 0. No ⃝ 2. Unknown

Student’s Name: Date Completed:
*Intervener services are provided by an individual, typically a paraeducator, who has received specialized
training in deaf-blindness and the process intervention.
Person Completing Form: (Please fill out #1 and #2 below.)
1. Your Name: Title:
Agency Name:
Address: City: Zip:
Phone: ( ) Email:
District: ESD:
Home School District (if different from serving district):
2. Teacher’s Name: Title:
School Name:
School Address: City: Zip:
Teacher’s Phone: ( ) Email:
District: ESD:
Home School District (if different from serving district): Revised 01/15/2016
RETURN FORM TO:
WA State Services for Children with Deaf-Blindness
Puget Sound ESD/WSDS
800 Oakesdale Avenue SW
Renton, WA 98057-5221
Phone: (800) 572-7000 (in-state); (425) 917-7827
- OR –
FAX to: (425) 917-7838
EMAIL to: [email protected]
Intervener*: 0. No ⃝ 1. Yes ⃝ 2. Unknown
Intervener Services: Check either “NO,” “YES,” or “UNKNOWN”

WEB Rev 12/12
“LIKES” INFORMATION
Child: Date:
FOODS
taste/ texture
SMELLS
TOUCH
texture/ hugs/ fabrics light - heavy
MOVEMENT
rock/ bounce swing
VIBRATION
car ride toys/ appliances
SIGHTS
lights/colors
SOUNDS voices/ music
pitch/ loudness environmental
MUSCLES
push - pull bear weight
PEOPLE PLACES ACTIVITIES TOYS SELF STIMULATION BEHAVIORS
OTHER
Page 1 of 2

WEB Rev 12/12
“DISLIKES” INFORMATION
Child: Date:
FOODS
taste/ texture
SMELLS
TOUCH
texture/ hugs/ fabrics light - heavy
MOVEMENT
rock/ bounce swing
VIBRATION
car ride toys/ appliances
SIGHTS
lights/colors
SOUNDS voices/ music
pitch/ loudness environmental
MUSCLES
push - pull bear weight
PEOPLE PLACES ACTIVITIES TOYS SELF STIMULATION BEHAVIORS
OTHER
Page 2 of 2

Washington Sensory Disabilities Services 9/28/2015
Authorization for Release of Records
PURPOSE: As a parent, guardian or student (aged 18 or older), you have the right to give, or not give, permission for the release of your child’s records to other persons or agencies. This request provides you with the opportunity to approve or not approve such a request, unless release of records is allowed under one of the exceptions under the rules implementing the Family Education Rights and Privacy Act, FERPA.
CHILD’s NAME Male Female CHILD’S DOB
SCHOOL DISTRICT/AGENCY STATE STUDENT ID # (10 digits)
I HEREBY AUTHORIZE THE EXCHANGE OF INFORMATION VERBALLY, IN WRITING, OR ELECTRONICALLY BETWEEN WSDS PROJECT STAFF AND THE AGENCIES/PERSONS LISTED BELOW FOR THE FOLLOWING PURPOSE(S):
Check one or more:
☐ Determining eligibility for WSDS project services ☐ Sharing evaluation/assessment results, progress notes
☐ Developing an appropriate IFSP/IEP ☐ Other (specify)
Washington Sensory Disabilities Services (WSDS) and Name of agency/person Name of agency/person
800 Oakesdale Ave. SW
Street address Street address
Renton, Washington 98057
City, State, Zip City, State, Zip
(425) 917-7827 or (800) 572-7000 (425 ) 917-7838 ( ) ( )
Phone # Fax # Phone # Fax #
and
Name of agency/person
Street address
City, State, Zip
( ) ( )
Phone # Fax #
and
Name of agency/person
Street address
City, State, Zip
( ) ( )
Phone # Fax #
and
Name of agency/person
Street address
City, State, Zip
( ) ( )
Phone # Fax #
THE RECORDS TO BE EXCHANGED INCLUDE:
(check all that apply)
☐ Reports/Assessment for:
Vision Hearing
☐ IFSP/IEP
☐ Relevant medical records
☐ Other (specify)
FOR QUESTIONS, CONTACT WSDS STAFF:
Puget Sound ESD:
800-572-7000 (or) 425-917-7827
North Central ESD:
509-665-2619
Central Washington University:
509-963-1131
www.wsdsonline.org

Washington Sensory Disabilities Services 9/28/2015
I understand that this information obtained will be treated in a confidential manner by Washington Sensory
Disabilities Services project staff under the provisions of the Family Education Rights and Privacy Act (FERPA).
FERPA prohibits disclosure of personally identifiable information without consent except in limited circumstances.
Neither treatment nor payment is dependent on a signed authorization.
Information disclosed may be subject to re-disclosure by an authorized recipient and privacy laws may no longer
protect your information.
The following information is protected via HIPPA. Check each item below that you wish to be released:
☐ HIV (AIDS virus) ☐ Sexually transmitted diseases
☐ Drug or alcohol abuse ☐ Psychiatric disorder or mental health
☐ This authorization is valid for one year. Specify end date:
☐ If less than one year, this authorization is valid from: to
Date Date
Requesting Records: From: To:
Date Date
I understand that my consent for the release of records is voluntary and I can withdraw my consent at any time in
writing. Should I withdraw my consent, it does not apply to information that has already been provided under the
prior consent for release.
Parent Signature Date Relationship to Child
Father’s Name (if appropriate) Mother’s Name (if appropriate)
Parent/Guardian Address Child’s Address (if different)
City, State, Zip City, State, Zip
( ) ( )
Phone(s) Phone(s)
Email Email

Adapted from Donta, N. & Purvis, B. (2005). NTAC Handout.
Routine
INITIATION:
1.
2.
3.
PREPARATION:
1.
2.
3.
CORE:
1.
2.
3.
TERMINATION:
1.
2.
3.
Other Comments:
________

USE OF SENSORY CHANNELS
Student: Has glasses/contacts? Yes No Has hearing aids? R L Wearing them now? Yes No Wearing aids now? R L
Setting/Activity:____________________________________________________________________
Date: ___________________________ Observer:_______________________________________
Observed Behavior Sensory Channel V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V V T A O/G P/V
V T A O/G P/V
V T A O/G P/V
V T A O/G P/V
V T A O/G P/V
V T A O/G P/V
Totals
Probable Primary Channel:
Secondary Sensory Channel(s):
KEY: V = Visual
T = Tactual
A = Auditory
O/G = Olfactory/Gustatory
P/V = Proprioceptive/Vestibular
Adapted from Koenig & Holbrook/TSBVI (1993) in collaboration with Arizona Schools for the Deaf & Blind. [Rev. 8/2005]