Embed Size (px)
Citation preview
OHSU Parkinson Center www.ohsubrain.com/pco
OHSU TEAM-PD RESOURCE MANUAL
SECTION 3: HELPFUL RESOURCES & HANDOUTS
1. Area Agencies on Aging Contact Information (pg 2-4) 2. Parkinson’s Disease Local & National Resources (pg 5) 3. OHSU PCO Newly Diagnosed Education Session Information (pg 6) 4. Aware in Care – Fact Sheet (pg 7-8) 5. Patient Instructional Handouts:
a. Members you should have on your health care team (pg 9) b. What is Parkinson’s disease? (pg 10-11) c. Constipation in PD (pg 12) d. Driving when you have PD (pg 13) e. Low blood pressure in PD (pg 14) f. Urinary Problems in PD (pg 15) g. Fatigue and PD (pg 16) h. Sleep Hygiene: Good Habits for Better Sleep (pg 17) i. Depression & Anxiety in PD (pg 18) j. Dealing with Hallucinations, Delusions in PD (pg 19) k. LSVT Information (pg 20) l. Clinical Pathway for Speech Communication Changes with PD (pg 21-22) m. Swallowing Tips for the Person with PD (pg 23) n. Making Your Meds Work Better / Pill Management Tools (pg 24)
6. PT/exercise Web Resources List (pg 25-26) 7. Information Sheets on Cueing for PD (pg 27-48) 8. Speech to Speech Relay Service (pg 49-51) 9. ChatterVox – Voice Amplifier (pg 52) 10. U-Step Walker and Sample letter of medical necessity (pg 53-55) 11. Allied Health Team Questions: Have you ever experienced…? (pg 56)
OHSU Parkinson Center www.ohsubrain.com/pco
OHSU TEAM-PD RESOURCE MANUAL
Area Agencies on Aging http://www.oregon.gov/DHS/SENIORS-DISABILITIES
3:2
Area Agency on Aging
-----------Find Locations & Community Services----------
Area Agencies on Aging office locator: http://www.n4a.org Eldercare Locator (search for local community services): http://www.eldercare.gov./Eldercare.NET/Public/Index.aspx
-----------Services----------
ADVOCACY - The Council on Aging or local Area Agency on Aging (AAA) is charged by the Federal Government with the role of providing advocacy services for seniors in their communities and at the State and Federal level. Advocacy involves representing seniors by preserving and developing services and supporting senior rights. FAMILY CAREGIVER SUPPORT PROGRAM - Respite Care The AAA provides specially trained relief caregivers to family members and those who care for seniors on a 24 hour 7 days a week basis, to afford these round-the-clock family caregivers a short term break to rest and renew, making them better family caregivers. For more information contact the local Council on Aging case manager listed on this site in the community nearest to where you live. HEALTH INSURANCE COUNSELING - SHIBA (Senior Health Insurance Benefits Assistance) The Council on Aging offers counseling to resolve problems with supplemental insurance, medicare claims or bills, doctor's bills, and problems with insurance companies regarding the payment of bills. Are you having trouble with your insurance company or are you unclear about your bills? Call for an appointment and we will be glad to help you. HEALTH AND WELLNESS - Fitness, social and volunteer opportunities are provided throughout the year through senior groups and centers. Contact us for possible programming for your members. Keep your body fit, keep your spirit happy with a variety of on-going activities sponsored by the Council on Aging and senior groups. INFORMATION AND REFERRAL - For information about the many community services and benefits available to senior citizens, call the local AAA office. LEGAL SERVICES - The Council on Aging provides tri-county residents ages 60 and older with referrals to free legal advice and representation pertaining to, but not limited to: - Medicare and Medicaid - Social Security and Supplemental Security Income - Landlord/Tenant Relations - Consumer Complaints - Hospital Patient Rights - Adult and Nursing Home Residents Rights
- Other Entitlements and Benefits - Powers of Attorney - Health Care Proxy - Living Wills
Legal Services are not available to cover wills, criminal cases, negligence actions or other cases for which a private attorney may be obtained on a contingency basis. LONG TERM CARE OMBUDSMAN PROGRAM - Ombudsman Program recruits and trains local volunteers and Ombudsman (advocates) to receive, investigate and resolve a wide range of concerns and complaints made by or on behalf of residents of adult and nursing homes. Ombudsmen visit the facilities regularly to: monitor the quality of care, help residents understand and exercise their rights, assure care with dignity and respect, and encourage residents to express their opinions. OREGON PROJECT INDEPENDENCE (OPI) - The OPI program provides help with housekeeping and personal care services for people age 60+ who could not remain in their own homes without assistance. Services are provided under contract through licensed home care agencies and/or the Client Employed Provider Program to those 60 and over, on a sliding fee scale, based upon income of the recipient. OUTREACH - The Council on Aging offers outreach to seniors who are unable to understand or access the information or services that they need. We visit homes and refer seniors to as many programs as they need. Please call and let us know who needs our information or services.
3:3

VOLUNTEER OPPORTUNITIES - "Volunteering is a 'win/win' opportunity for the volunteers as well as for the human service organizations that rely on volunteers to provide services and staff support". Senior Centers have a variety of volunteer opportunities including home-delivered meal drivers, mealsite assistants, information and referral and office help. Contact the Council on Aging or your local senior center. HOME DELIVERED MEALS - Home delivered meals are provided to homebound persons who, based on an assessment, are unable to meet their daily nutritional needs. Home delivered meals provide one hot noon meal and frozen weekend meals. NUTRITION EDUCATION AND COUNSELING - Referral to a Registered Dietitian is available for counseling and assistance with special diet problems, restrictions, food/nutrition related questions, and nutrition education.
3:4
PARKINSON’S DISEASE LOCAL & NATIONAL RESOURCES
---------------- Specialists ----------------
OHSU’s Parkinson Center (PCO) • 503-494-7230; www.ohsubrain.com/pco
VA PADRECC (Parkinson Disease Research, Education, & Clinical Care Center) – Medical & Research Experts for eligible Veterans with PD
• www.visn20.med.va.gov/portland/PADRECC • 800-949-1004 x51091
Other movement disorders experts;
• Providence – Portland, OR • Legacy – Portland, OR • Oregon Neurology – Eugene, OR • Booth Gardner Parkinson Center – Evergreen, WA • University of Washington – Seattle, WA
----------------Support Groups----------------
Northwest Parkinson Foundation
• Support groups and educational forums throughout the NW o 877-980-7500; www.nwpf.org
Parkinson’s Resources of Oregon (PRO) • Support groups and educational forums throughout Oregon & Southern Washington
o 800-426-6806; www.parkinsonsresources.org
APDA Washington Chapter • Support groups and educational forums throughout WA
o 425-243-2732; http://www.waparkinsons.org/
Parkinson’s Resource Center of Spokane • Support groups and educational forums throughout the NW
o 509-473-2490; http://www.spokaneparkinsons.org/
----------------National Organizations----------------
NPF (National Parkinson Foundation) – National Organization • NPF Rainbow Books & NPF Progress Report and more…
o Free – order online at www.parkinson.org or by calling 800-327-4545
PDF (Parkinson Disease Foundation) – National Organization • Web Resources for People with Parkinson’s
o Free – order online at www.pdf.org
APDA (American Parkinson Disease Association) – National Organization • Check out their Young Onset PD website at www.youngparkinsons.org and their national
website at www.apdaparkinson.org
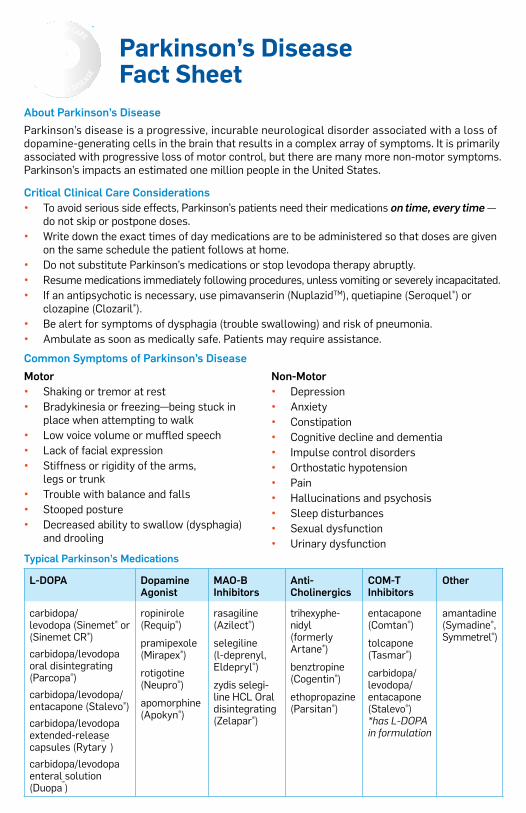
Parkinson’s Disease Fact Sheet
About Parkinson’s DiseaseParkinson’s disease is a progressive, incurable neurological disorder associated with a loss of dopamine-generating cells in the brain that results in a complex array of symptoms. It is primarily associated with progressive loss of motor control, but there are many more non-motor symptoms. Parkinson’s impacts an estimated one million people in the United States.
Critical Clinical Care Considerations• To avoid serious side effects, Parkinson’s patients need their medications on time, every time —
do not skip or postpone doses.• Write down the exact times of day medications are to be administered so that doses are given
on the same schedule the patient follows at home.• Do not substitute Parkinson’s medications or stop levodopa therapy abruptly.• Resume medications immediately following procedures, unless vomiting or severely incapacitated.• If an antipsychotic is necessary, use pimavanserin (NuplazidTM), quetiapine (Seroquel®) or
clozapine (Clozaril®).• Be alert for symptoms of dysphagia (trouble swallowing) and risk of pneumonia.• Ambulate as soon as medically safe. Patients may require assistance.
Common Symptoms of Parkinson’s DiseaseMotor• Shaking or tremor at rest• Bradykinesia or freezing—being stuck in
place when attempting to walk• Low voice volume or muffled speech• Lack of facial expression• Stiffness or rigidity of the arms,
legs or trunk• Trouble with balance and falls• Stooped posture• Decreased ability to swallow (dysphagia)
and drooling
Non-Motor• Depression• Anxiety• Constipation• Cognitive decline and dementia• Impulse control disorders• Orthostatic hypotension• Pain• Hallucinations and psychosis• Sleep disturbances• Sexual dysfunction• Urinary dysfunction
Typical Parkinson’s Medications
L-DOPA Dopamine Agonist
MAO-B Inhibitors
Anti- Cholinergics
COM-T Inhibitors
Other
carbidopa/ levodopa (Sinemet® or (Sinemet CR®)
carbidopa/levodopa oral disintegrating (Parcopa®)
carbidopa/levodopa/entacapone (Stalevo®)
carbidopa/levodopa extended-release capsules (Rytary )
carbidopa/levodopa enteral solution (Duopa )
ropinirole (Requip®)
pramipexole (Mirapex®)
rotigotine (Neupro®)
apomorphine (Apokyn®)
rasagiline (Azilect®)
selegiline (l-deprenyl, Eldepryl®)
zydis selegi-line HCL Oral disintegrating (Zelapar®)
trihexyphe-nidyl (formerly Artane®)
benztropine (Cogentin®)
ethopropazine (Parsitan®)
entacapone (Comtan®)
tolcapone (Tasmar®)
carbidopa/levodopa/ entacapone (Stalevo®) *has L-DOPA in formulation
amantadine (Symadine®, Symmetrel®)
TM
TM
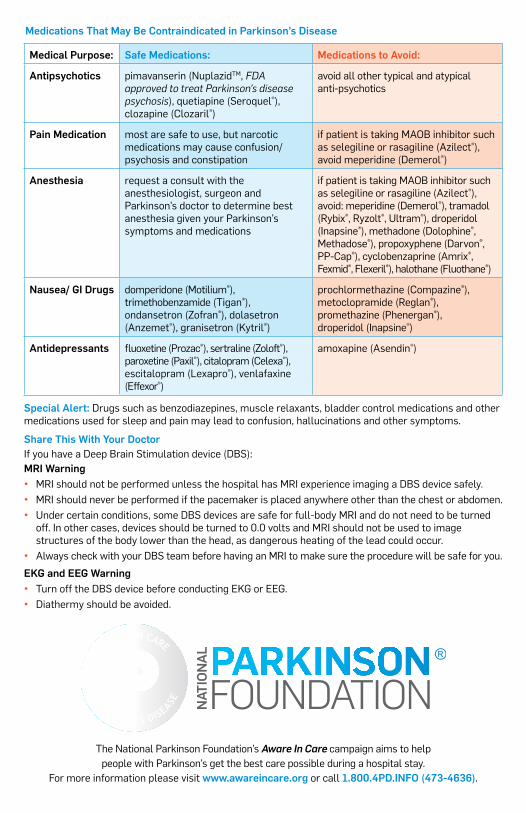
Medical Purpose: Safe Medications: Medications to Avoid:
Antipsychotics pimavanserin (NuplazidTM, FDA approved to treat Parkinson’s disease psychosis), quetiapine (Seroquel®), clozapine (Clozaril®)
avoid all other typical and atypical anti-psychotics
Pain Medication most are safe to use, but narcotic medications may cause confusion/ psychosis and constipation
if patient is taking MAOB inhibitor such as selegiline or rasagiline (Azilect®), avoid meperidine (Demerol®)
Anesthesia request a consult with the anesthesiologist, surgeon and Parkinson’s doctor to determine best anesthesia given your Parkinson’s symptoms and medications
if patient is taking MAOB inhibitor such as selegiline or rasagiline (Azilect®), avoid: meperidine (Demerol®), tramadol (Rybix®, Ryzolt®, Ultram®), droperidol (Inapsine®), methadone (Dolophine®, Methadose®), propoxyphene (Darvon®, PP-Cap®), cyclobenzaprine (Amrix®, Fexmid®, Flexeril®), halothane (Fluothane®)
Nausea/ GI Drugs domperidone (Motilium®), trimethobenzamide (Tigan®), ondansetron (Zofran®), dolasetron (Anzemet®), granisetron (Kytril®)
prochlormethazine (Compazine®), metoclopramide (Reglan®), promethazine (Phenergan®), droperidol (Inapsine®)
Antidepressants fluoxetine (Prozac®), sertraline (Zoloft®), paroxetine (Paxil®), citalopram (Celexa®), escitalopram (Lexapro®), venlafaxine (Effexor®)
amoxapine (Asendin®)
Special Alert: Drugs such as benzodiazepines, muscle relaxants, bladder control medications and other medications used for sleep and pain may lead to confusion, hallucinations and other symptoms.
Share This With Your Doctor If you have a Deep Brain Stimulation device (DBS): MRI Warning• MRI should not be performed unless the hospital has MRI experience imaging a DBS device safely.• MRI should never be performed if the pacemaker is placed anywhere other than the chest or abdomen.• Under certain conditions, some DBS devices are safe for full-body MRI and do not need to be turned
off. In other cases, devices should be turned to 0.0 volts and MRI should not be used to image structures of the body lower than the head, as dangerous heating of the lead could occur.
• Always check with your DBS team before having an MRI to make sure the procedure will be safe for you.
EKG and EEG Warning• Turn off the DBS device before conducting EKG or EEG.• Diathermy should be avoided.
Medications That May Be Contraindicated in Parkinson’s Disease
The National Parkinson Foundation’s Aware In Care campaign aims to help people with Parkinson’s get the best care possible during a hospital stay.
For more information please visit www.awareincare.org or call 1.800.4PD.INFO (473-4636).
Oregon Health & Science University Parkinson Center
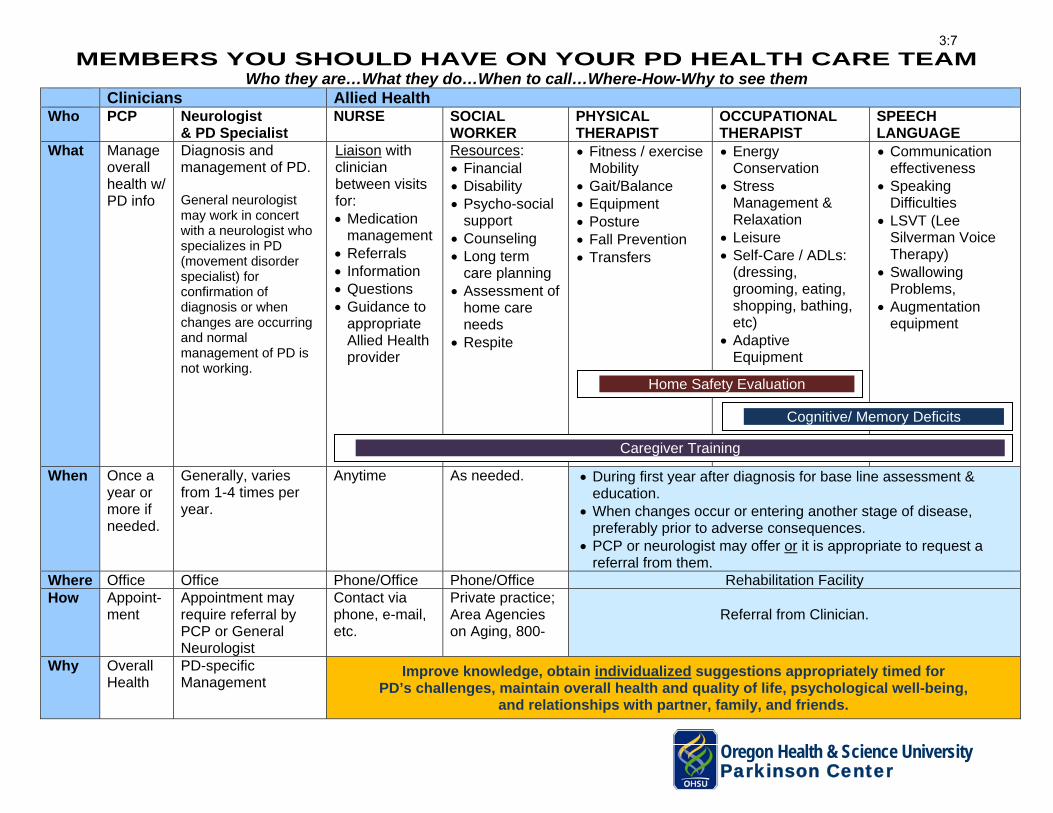
MEMBERS YOU SHOULD HAVE ON YOUR PD HEALTH CARE TEAM Who they are…What they do…When to call…Where-How-Why to see them
Clinicians Allied Health Who PCP Neurologist
& PD Specialist NURSE SOCIAL
WORKER PHYSICAL THERAPIST
OCCUPATIONAL THERAPIST
SPEECH LANGUAGE
What Manage overall health w/ PD info
Diagnosis and management of PD.
General neurologist may work in concert with a neurologist who specializes in PD (movement disorder specialist) for confirmation of diagnosis or when changes are occurring and normal management of PD is not working.
Liaison with clinician between visits for: • Medication
management• Referrals• Information• Questions• Guidance to
appropriateAllied Healthprovider
Resources: • Financial• Disability• Psycho-social
support• Counseling• Long term
care planning• Assessment of
home careneeds
• Respite
• Fitness / exerciseMobility
• Gait/Balance• Equipment• Posture• Fall Prevention• Transfers
• EnergyConservation
• StressManagement &Relaxation
• Leisure• Self-Care / ADLs:
(dressing,grooming, eating,shopping, bathing,etc)
• AdaptiveEquipment
• Communicationeffectiveness
• SpeakingDifficulties
• LSVT (LeeSilverman VoiceTherapy)
• SwallowingProblems,
• Augmentationequipment
When Once a year or more if needed.
Generally, varies from 1-4 times per year.
Anytime As needed. • During first year after diagnosis for base line assessment &education.
• When changes occur or entering another stage of disease,preferably prior to adverse consequences.
• PCP or neurologist may offer or it is appropriate to request areferral from them.
Where Office Office Phone/Office Phone/Office Rehabilitation Facility How Appoint-
ment Appointment may require referral by PCP or General Neurologist
Contact via phone, e-mail, etc.
Private practice; Area Agencies on Aging, 800-
Referral from Clinician.
Why Overall Health
PD-specific Management
Improve knowledge, obtain individualized suggestions appropriately timed for PD’s challenges, maintain overall health and quality of life, psychological well-being,
and relationships with partner, family, and friends.
Cognitive/ Memory Deficits
Caregiver Training
Home Safety Evaluation
3:7
What is Parkinson’s Disease?
What is Parkinson’s disease (PD)? PD is a progressive brain disorder. PD occurs when certain nerve cells (neurons) in a part of the brain called the substantia nigra die or become impaired. Normally, these cells produce a vital chemical known as dopamine. Dopamine allows smooth, coordinated function of the body’s muscles and movement. When approximately 80 percent of the dopamine-producing cells are damaged, the symptoms of PD appear.
What are the signs and symptoms of PD? The loss of dopamine production in the brain causes the primary symptoms of PD. The key signs of PD are:
• Tremor (shaking)• Slowness of movement• Rigidity (stiffness)• Difficulty with balance
Other signs of PD may include: • Small, cramped handwriting• Stiff facial expression• Shuffling walk• Muffled speech• Depression
What causes PD? Nobody knows what causes dopamine-producing nerve cells to die. Parkinson’s is not contagious. It is not hereditary, but sometimes occurs in families.
Who gets PD? PD affects both men and women in almost equal numbers. It shows no social, ethnic, economic or geographic boundaries. In the United States, it is estimated that 60,000 new cases are diagnosed each year, joining the 1.5 million Americans who currently have PD. While the condition usually develops after the age of 65, 15 percent of those diagnosed are under the age 50.
How is PD diagnosed? The process of making a PD diagnosis can be difficult. There is no X-ray or blood test that can confirm PD. A physician arrives at the diagnosis only after a thorough examination. Blood tests and brain scans known a magnetic resonance imaging (MRI) may be performed to rule out other conditions that have similar symptoms. People suspected of having PD should consider seeking the care of a neurologist who specializes in PD.
OHSU PARKINSON CENTE
National Parkinson Foundation Center of
Excellence
3:8
What is the treatment for PD? There are a number of effective medicines that help to ease the symptoms of PD. Most symptoms are caused by lack of dopamine. The medicines most commonly used will attempt to either replace or mimic dopamine, which improves the tremor, rigidity and slowness associated with PD. Several new medicines are being studied that may slow the progression. Many promise to improve the lives of people with PD.
Can surgery help PD? Surgery can ease the symptoms of PD, but it is not a cure. Because of the risks associated with brain surgery, it is usually not considered unless all appropriate medications have been tried unsuccessfully. When considering surgery, it is important to see both a neurologist and brain surgeon who specialize in the treatment of PD.
Can I live well with PD? Exercise, good nutrition and the support of your health care team can help you live well. Learning as much as possible about PD will also help. Support groups are an excellent source of information and practical advice.
Is there a cure for PD? There is no cure for PD. In order to find the cure, researchers must determine what causes PD. Top scientists around the world are working to find the cause and a cure. Many believe that it could be cured within the next decade. The Parkinson Center of Oregon at OHSU is proud to be part of this effort.
Where can I get help? If you or a loved one has Parkinson’s disease (PD) and would like to consult a specialist in PD, please contact our clinic referral line at 503-494-7772 or visit our website at www.ohsu.edu/pco.
How can I help? Donations provided to the Parkinson Center of Oregon at OHSU will assist researchers in finding treatments, the cause, and, eventually, a cure for PD.
Donations can be sent to: OHSU Foundation / OHSU Parkinson CenterAttn: Diana Potts 3181 Sam Jackson Park Rd, OP-32 Portland, OR 97239
OHSU PARKINSON CENTERNational Parkinson
Foundation Center of Excellence
3:9
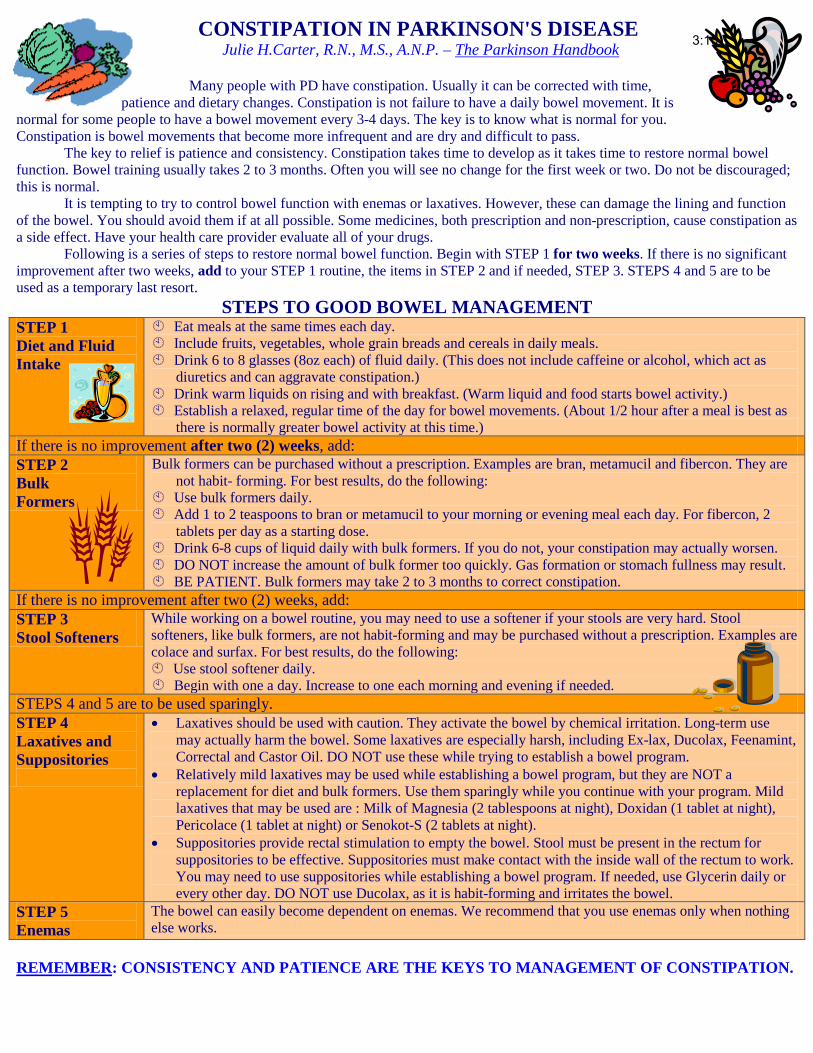
CONSTIPATION IN PARKINSON'S DISEASE Julie H.Carter, R.N., M.S., A.N.P. – The Parkinson Handbook
Many people with PD have constipation. Usually it can be corrected with time, patience and dietary changes. Constipation is not failure to have a daily bowel movement. It is
normal for some people to have a bowel movement every 3-4 days. The key is to know what is normal for you. Constipation is bowel movements that become more infrequent and are dry and difficult to pass.
The key to relief is patience and consistency. Constipation takes time to develop as it takes time to restore normal bowel function. Bowel training usually takes 2 to 3 months. Often you will see no change for the first week or two. Do not be discouraged; this is normal.
It is tempting to try to control bowel function with enemas or laxatives. However, these can damage the lining and function of the bowel. You should avoid them if at all possible. Some medicines, both prescription and non-prescription, cause constipation as a side effect. Have your health care provider evaluate all of your drugs.
Following is a series of steps to restore normal bowel function. Begin with STEP 1 for two weeks. If there is no significant improvement after two weeks, add to your STEP 1 routine, the items in STEP 2 and if needed, STEP 3. STEPS 4 and 5 are to be used as a temporary last resort.
STEPS TO GOOD BOWEL MANAGEMENT STEP 1 Diet and Fluid Intake
Eat meals at the same times each day. Include fruits, vegetables, whole grain breads and cereals in daily meals. Drink 6 to 8 glasses (8oz each) of fluid daily. (This does not include caffeine or alcohol, which act as
diuretics and can aggravate constipation.) Drink warm liquids on rising and with breakfast. (Warm liquid and food starts bowel activity.) Establish a relaxed, regular time of the day for bowel movements. (About 1/2 hour after a meal is best as
there is normally greater bowel activity at this time.) If there is no improvement after two (2) weeks, add: STEP 2 Bulk Formers
Bulk formers can be purchased without a prescription. Examples are bran, metamucil and fibercon. They are not habit- forming. For best results, do the following:
Use bulk formers daily. Add 1 to 2 teaspoons to bran or metamucil to your morning or evening meal each day. For fibercon, 2
tablets per day as a starting dose. Drink 6-8 cups of liquid daily with bulk formers. If you do not, your constipation may actually worsen. DO NOT increase the amount of bulk former too quickly. Gas formation or stomach fullness may result. BE PATIENT. Bulk formers may take 2 to 3 months to correct constipation.
If there is no improvement after two (2) weeks, add: STEP 3 Stool Softeners
While working on a bowel routine, you may need to use a softener if your stools are very hard. Stool softeners, like bulk formers, are not habit-forming and may be purchased without a prescription. Examples are colace and surfax. For best results, do the following: Use stool softener daily. Begin with one a day. Increase to one each morning and evening if needed.
STEPS 4 and 5 are to be used sparingly. STEP 4 Laxatives and Suppositories
• Laxatives should be used with caution. They activate the bowel by chemical irritation. Long-term usemay actually harm the bowel. Some laxatives are especially harsh, including Ex-lax, Ducolax, Feenamint,Correctal and Castor Oil. DO NOT use these while trying to establish a bowel program.
• Relatively mild laxatives may be used while establishing a bowel program, but they are NOT areplacement for diet and bulk formers. Use them sparingly while you continue with your program. Mildlaxatives that may be used are : Milk of Magnesia (2 tablespoons at night), Doxidan (1 tablet at night),Pericolace (1 tablet at night) or Senokot-S (2 tablets at night).
• Suppositories provide rectal stimulation to empty the bowel. Stool must be present in the rectum forsuppositories to be effective. Suppositories must make contact with the inside wall of the rectum to work.You may need to use suppositories while establishing a bowel program. If needed, use Glycerin daily orevery other day. DO NOT use Ducolax, as it is habit-forming and irritates the bowel.
STEP 5 Enemas
The bowel can easily become dependent on enemas. We recommend that you use enemas only when nothing else works.
REMEMBER: CONSISTENCY AND PATIENCE ARE THE KEYS TO MANAGEMENT OF CONSTIPATION.
3:10
Driving when you have Parkinson's Disease For most people, driving represents freedom, control and competence. Driving enables most people to get to the places they want or need to go. For many people, driving is important economically – some drive as part of their job or to get to and from work.
Driving is a complex skill. Our ability to drive safely can be affected by changes in our physical, emotional and mental condition. The goal of this brochure is to help you and your health care professional talk about how Parkinson’s disease (PD) may affect your ability to drive safely. How can PD affect my driving?
Parkinson’s disease can cause your arms, hands, or legs to shake – even when you are relaxed. It also can make it harder for you to keep your balance, or start to move when you have been still. If you have Parkinson’s and you try to drive, you may not be able to: react quickly to a road hazard; turn the steering wheel; or use the gas pedal or push down the brake.
Can I still drive with PD?
Most likely, yes, in the early stages of the disease, and if you take medicines that control your symptoms. But realistically there may come a time when you can no longer drive safely and you need to plan ahead for this possibility.
What can I do when PD affects my driving?
Ask your doctor about medicines and surgeries that could help treat your symptoms of Parkinson’s disease. Ask about the affect medicines may have on your continued ability to drive safely.
Staying fit and active will help maintain your muscle strength that you need to drive. This will help keep you safely behind the wheel and on the road.
Your doctor also can refer you to a center or a specialist who can give you on and off-road tests to see if, and how, your Parkinson’s is affecting your driving. The specialist also may offer training to improve your driving skills if your Parkinson’s still allows you to drive safely.
Improving your skills could help keep you and others around you safe. To find a specialist near you, call the Association of Driver Rehabilitation Specialists at 1-800-290-2344 or go to their website at www.aded.net. You also can call your local hospital and rehabilitation facility to find an occupational therapist who can help with the driving skills assessment.
What if I have to cut back or give up driving?
You can keep your independence even if you have to cut back or give up on your driving. It may take planning ahead on your part, but planning will get you to the places you want to go and the people you want to see.
Consider: * rides with family and friends * taxi cabs * shuttle buses or vans * public buses, trains and subways Senior centers, and religious and other local service groups often offer transportation services for older adults in your community.
Who can I call for help with transportation?
Call the ElderCare Locator at 1-800-677-1116 and ask for your local Office on Aging, or go to their website at www.eldercare.gov.
Contact your regional transit authority to find out which bus or train to take: www.trimet.org Call Easter Seals Project ACTION (Accessible Community Transportation In Our Nation) at
1-800-659-6428 or go to their website at www.projectaction.org. You also can get a copy of “Age Page On Older Drivers” from the National Institute on Aging by calling 1-800-222-2225, or by going to their website at www.nia.nih.gov/health/agepages/ drivers.htm.
Wear your safety belt and make sure everyone with you does to! Source: U.S. Department of Transportation, NHTSA (National Hwy Traffic Safety Administration, APDA (American Parkinson Disease Association), NPF (National Parkinson Foundation); DOT HS 809 687; 11/2003; additional comments by OHSU-PCO.
3:11

LOW BLOOD PRESSURE (hypotension) in PARKINSON’S DISEASE
Individuals with Parkinson’s disease (PD) may experience low blood pressure
(hypotension) at some point during their treatment course. This occurs because PD can impair the body’s natural reflex mechanism which causes automatic adjustments of your blood pressure when you change position, exercise, eat, or are out in warm or cold weather. Also, anti-parkinson’s medications (and many other drugs as well) can lower blood pressure.
When it does occur, the
patient may recognize and report sensations such as dizziness, lightheaded-ness, or weakness. If severe, hypotension can lead to fainting and/or falling. Individuals have also used terms such as giddiness, sleepiness, tiredness, mental or visual blurring to describe what has actually turned out to be low blood pressure.
Blood pressure decreases when blood vessels relax or lose their ability to constrict.
If there is less fluid in the body, the circulating blood volume is decreased and blood pressure drops. Normal blood pressure range is usually 100/60 to 140/90. Drops in blood pressure below 100/60 may result in the sensations mentioned below and a few individuals may not experience any warning signals.
These sensations will often intensify upon standing or after walking. Although
any time of day is possible, many report the occurrence more in the early morning hours and/or 1-2 hours after receiving a dose(s) of medication.
The emphasis is to seek the cause and treat the problem before an episode of fainting or falling occurs based on each person’s symptoms and associated conditions. Monitoring blood pressure should be routine.
It is advisable that patients have their blood pressure taken in the sitting and standing positions periodically. Here are a number of simple measures which can be employed to restore normal blood pressure regulation.
Evaluate Medications
Re-evaluate the patient's complete medication list. Adjustments of the medications themselves or the timing sequence might be all that is needed.
Increase Fluids & Salty Foods
Interventions such as increasing fluids and salt in the diet can be very effective. Drinking eight glasses of water per day and eating salty foods are commonly recommended. With more fluid in the body , circulating blood volume is enhanced and blood pressure increases.
Caffeine Drinking caffeinated coffee, in addition to adding fluid enhances blood vessel constriction, thus increasing blood pressure.
Frequent, Small Meals
Eat frequent, small meals as blood pressure is often lowered after a large meal. Alcohol should be avoided as it has a tendency to dilate blood vessels, contributing to lower blood pressure.
Environment Warm weather, hot baths, or any activities that cause blood vessels to relax should be avoided.
Clothing Waist-high compression/support hose (i.e. Jobst® stockings or Sigvars® pantyhose) can be helpful in maintaining blood pressure.
Slow Position Change
When rising from a lying position, sit on the edge of the bed for a few minutes; then stand up slowly, holding on to a secure support.
Bed Position Raise the head of the bed 30-40 degrees as lying flat for a prolonged period of time can contribute to lower blood pressure.
Medication Occasionally, salt tablets or medications such as fludrocortisone (Florinef®) and Pro-Amatine (Midodrine®) are prescribed. By increasing blood volume and promoting vascular constriction, these drugs help raise blood pressure. The risks associated with using these drugs can be controlled with close medical supervision. Some patients respond better using a combination of treatments.
Always consult with your healthcare provider if you experience the sensations described herein and especially before altering your medication schedule.
Source: Linda P. Miller, R.N., MEd – The Parkinson Handbook
3:12
URINARY PROBLEMS IN PARKINSON'S DISEASE
Julie H.Carter, R.N., M.S., A.N.P. – The Parkinson Handbook
Urinary incontinence (involuntary loss of urine) is a common symptom in Parkinson's disease.
WHY DO PROBLEMS OCCUR IN PD? The bladder is a muscle which gradually expands as urine collects. At the opening there is a muscle called the sphincter which is closed except when urinating. Both muscles are controlled by the brain. When 1-2 cups of urine have collected in the bladder, the bladder may begin to have small contractions that signal the brain that the bladder is filling up. The brain can suppress the contractions until it is convenient for the person to go to the bathroom. At that time the brain allows the bladder to contract while the sphincter relaxes, thereby allowing the urine to leave the bladder.
Difficulty holding urine is the most common problem. In PD, normal control from the brain is disturbed; the bladder becomes overactive, wanting to empty even when there is just a small amount of urine present. This results in symptoms of urgency frequency, incontinence and repeated nighttime urination.
Drugs are available (e.g. Ditropan®, Detrol®, Vesicare®, Hytrin®, Probanthine®) which help by relaxing the bladder muscle.
Difficulty eliminating urine can be caused by a sphincter which wants to close when the bladder is ready to empty, or by a bladder muscle which is too weak to expel the urine. The concern is that with incomplete bladder emptying, urine will accumulate, bacteria will grow, and infections will result. The symptoms of difficulty eliminating urine are weak urinary stream dribbling or leaking feeling that the bladder is not completely
emptied.These problems must be carefully evaluated by a urologist to determine their cause. If the symptoms are PD-related, the most successful management is intermittent catheterization.
DOCUMENT: The following signs of bladder problems should be reported to your health care provider:
1. Leakage of urine significant to causeembarrassment.
2. Inability to urinate when bladder is full -requires immediate attention.
3. Unusually frequent urination without a provenbladder infection.
4. Needing to rush to the bathroom or losing urineif you do not "arrive in time" (urgency).
5. Pain related to urination.6. Progressive weakness of the urinary stream
which may be accompanied by a feeling thatthe bladder is not emptying completely.
Also, note how often you urinate in 24 hours, how often you are incontinent, how many times you urinate at night, and over what period of time these changes have occurred.
MANAGEMENT may include… • Medication for urinary urgency and
frequency• Urological evaluation• Intermittent self catheterization for urinary
retention• Incontinence aids: Although urinary
incontinence can often be treated, there aretimes when incontinence aids are needed.Knowing which aids work best for you andwhere to get them can restore your freedom andconfidence. Incontinence aids are primarilychosen by the degree of absorbency required andthe ease of use. During the night, highabsorbency pads are usually required. Briefswith elastic around the legs and sticky tabs onthe side are the most absorbent. Gel briefs aremore absorbent than cellulose and can hold 2-3voidings. For daytime use, "undergarments"which button at the hip or underwear shieldsmay be sufficient and are easy to pull up anddown.
• N.A.F.C. (National Associate for Continence) isan organization which provides a resource guidefor a nominal fee as well a other self-helpinformation: phone: 1-800-BLADDER (252-3337) or www.nafc.org.
3:13
FATIGUE & PARKINSON'S DISEASE Cathi A.Thomas, R.N., M.S. – The Parkinson Handbook
For people with Parkinson's disease, fatigue can seem as much a state of mind as of the body. We do not know everything about this common symptom, but we do know that fatigue can have both mental and physical causes. In Parkinson's disease, the feeling of fatigue is hard to describe and even harder to measure. Many symptoms of PD can cause a feeling of weariness and can make it difficult to finish an activity. Fatigue can mean slow movement, muscle stiffness, depression or even changes in being able to move or sleep. It can be experienced throughout the day or only when medications are wearing off.
Fatigue Due to Akinesia
Akinesia, or trouble starting a movement, often feels like fatigue. A person with this symptom must move slowly and will find it hard to finish a task in a regular amount of time. Everyday tasks such as getting dressed can take a lot of effort. Keep track of times during the day when akinesia is better and medications are working well. Energy consuming tasks can then be done at these times when movement is easier.
Muscle Fatigue
Parkinson's symptoms like muscle stiffness, cramping, tremor (shaking) and difficulty initiating a movement put stress on a person's muscles. To move with these symptoms, muscles have to work very hard and often against each other. With tremor, the constant shaking can quickly fatigue muscles. Muscles that do not move enough become deconditioned and reduced in size (atrophied). Loss of muscle strength decreases stamina and endurance and for many people, this decrease feels like fatigue Antiparkinson medications can be used to treat symptoms that can fatigue, but they must be carefully monitored to avoid a common side effect called dyskinesia (fidgety, involuntary movements), because this side effect will also cause fatigue. The only treatment for deconditioned muscles is a regular exercise program. People who have included exercise as a part of their daily routine have less fatigue.
Fluctuations in Mobility
Many people with Parkinson's disease have fluctuations in their mobility throughout the day. Typically these fluctuations follow the dosing cycle, with an increase in symptoms at the end of a dose. It is also common to have the best relief from symptoms in the morning, when people feel well rested. Often, people try to get everything done in the orning when they feel well, but over activity can lead to fatigue. Time your periods of activity for maximum mobility, but also pace yourself and allow for rest periods.
Fatigue due to Depression
Depression is common in people with Parkinson's disease, occurring in about 40% of the patients. Fatigue is a typical symptom of depression and is often reported as a lack of motivation or a loss of energy. Antidepressants are used to treat this problem. When successful, people begin to feel less tired and are more willing to participate fully in a day's activities.
Fatigue due to Sleep Disturbance
Parkinson's disease is often associated with sleep disturbance. Causes vary but may be due to sleep cycle changes, inability to get comfortable, or side effects of medications. Sleep disruption contributes to daytime sleepiness and people often have a strong desire to nap throughout the day. A short nap after lunch is healthy and refreshing, but frequent naps throughout the day will only make sleeping at night more difficult. Sleep problems should be evaluated because it is well-known that a poorly rested person will perform poorly during the day. It is also important to note that some medications used to treat sleep disturbance may cause daytime fatigue.
Fatigue due to Medications
Dopamine agonistis, such as Mirapex® and Requip®, can cause fatigue and daytime sleepiness. Reducing the medication may help; however, it can come at the cost of increased symptoms. Medications such as Provigil® and Ritalin® are being studied for combating fatigue in PD.
WORKING WITH YOUR CLINICIAN TO MANAGE FATIGUE: It is clear that fatigue is a problem for many people with Parkinson's disease. To get help, a complete health history and physical exam is first necessary to rule out non-Parkinson causes. Sometimes problems not associated with PD, such as anemia, are found. When giving their history, people should note: when they feel fatigued how long the feeling lasts
how fatigue fluctuates with their symptoms and medications how badly they feel when it happens
The answers will help identify the reason for the problem necessary, Parkinson’s medications can be adjusted. SOME STEPS PEOPLE WITH PD CAN TAKE TO AVOID FATIGUE
1. Eat well; getting the right food is necessary for feeling strong.
2. Participate in an exercise program with both aerobic and stretching exercises.
3. Practice good sleep habits; establish a regular bedtime, avoid frequent napping or stimulation at bedtime, and decrease caffeine and alcohol intake.
4. Keep mentally active. Boredom often leads to fatigue.
5. Eat a lot of fiber and drink plenty of fluids to avoid constipation.
6. Do more difficult daily tasks when movement is easier and medications are working well.
7. Know your limitations and seek assistance when necessary. Forcing too many activities into one time period will cause fatigue.
3:14
Sleep Hygiene: Good Habits for Better Sleep Source: NPF’s “Mind, Mood, & Memory”
Daytime Tips
1. Wake up the same time everyday. Setan alarm if you have to.
2. Get out of bed right after you wakeup. Too much time spent in bed canlead to more waking up at night.
3. Limit daytime naps. They can makesleep at night more difficult.
4. Eat regular, healthy meals. Eat at thesame time every day. Three to foursmall meals are better than 1-2 largemeals.
5. Do not drink coffee, tea, sodas orcocoa after noon. They containcaffeine and can interfere withnormal sleep.
6. Do not drink alcohol after dinner. Itmay help you fall asleep faster, butmakes sleep shallower later in thenight. Alcohol can also make snoringand sleep apnea worse.
7. Use caution when taking headacheand cold medicines. Some containstimulants that can affect sleep.
8. Stop smoking. Cigarette smokingstimulates the body and makes sleepdifficult.
9. Increase or start doing daily exercise.Regular exercise helps to deepensleep. The best time to exercise isearly in the morning. Avoid heavyexercise 2 hours before bedtime.
Nighttime Tips
1. Get into bed only when you are sleepy.2. Do not use over-the-counter sleeping medications.
They may help you to fall asleep faster, but they donot help you to get deeper sleep. They can also makesnoring and sleep apnea worse.
3. Develop a sleep ritual. Do something relaxing beforebed such as reading or listening to music. This tellsyour body that it is time to settle down.
4. A warm shower or bath an hour before bedtime canhelp you to fall asleep.
5. If you tend to worry about things while lying in bed,make an effort to do your worrying outside of bed.Before going to the bedroom, make a list of things todeal with tomorrow.
6. If you are hungry at bedtime, eat a small snack ordrink a glass of milk. Do not eat sugary snacks orchocolate or drink tea or coffee. Large meals beforebedtime can worsen sleep.
7. Use your bed only for sleep or sexual activity. Do notdo anything else in bed such as reading, watching TV,arguing, catching up on work, smoking, etc.
8. Keep the bedroom dark and the temperaturecomfortable.
9. Block out noise as much as possible. Occasional loudnoises disturb sleep even in people who cannotremember them in the morning. The hum of a fan canhelp cover up some noise.
10. Do not watch the clock and worry about lost sleep.Turn the clock face away.
Do not try to force sleep. If you cannot fall asleep… • Get out of bed.• Move to another room and watch TV, read, or listen to soothing music
until you are sleepy• Go back to bed.• If you are still unable to sleep, get out of bed again and repeat the cycle
until you are able to sleep.
3:15
Depression & Anxiety in Parkinson’s Disease Source: Wientraub, Dan, MD. “Emotional Changes in Parkinson’s Disease”
in NPF’s Mind, Mood, & Memory; 2005 During the course of PD, it is estimated that up to 50% of people with Parkinson’s (PWP) will experience depression and/or anxiety. Both can be considered symptoms of PD caused by chemical imbalances in the brain. SYMPTOMS: Depression can present differently in PWP, and each patient is unique. Some commonly reported symptoms of depression and anxiety are: • feelings of guilt • thoughts of death or suicide • decreased interest or pleasure
• poor attention and concentration • sleep problems • feeling slowed down or restless inside
• self-blame or worthlessness • excessive worry in public • anxiety during “off” periods
CAUSES: Depression & anxiety can be caused by psychological and biological factors. • Psychological factors:
o Sadness & hopelessness in facing a chronic illness o Isolation to avoid being in public o Anxiety over other people noticing PD symptoms or medication wearing off
• Biological Factors: o People with PD are more likely to have experienced depression or anxiety earlier in life o Regions of the brain affected by PD are the same as those affected by depression and anxiety o Certain brain chemicals (dopamine, serotonin, norepinephrine, and GABA) change in both PD and
depression/anxiety. DIAGNOSIS: Diagnosing depression in PD can be difficult, as some of the symptoms of depression can also occur in PD without depression. A patient with major depression would have, most of the time over a two week period: depressed mood and loss of interest or pleasure. In addition, some of the following symptoms must be present: • changes in sleep or appetite • decreased concentration or attention • increased fatigue
• feeling slowed down or restless • feeling worthless and guilty • suicide ideas or a wish for death.
Generalized anxiety is a feeling of nervousness and thoughts of worry most of the time. The worrying is in excess of what patients would normally expect and often feels out of control. Physical symptoms are also common, including• butterflies in the stomach • trouble breathing or swallowing • racing of the heart
• sweating • increased tremors
TREATMENT:
Anti-depressants such as Zoloft®, Paxil®, Celexa®, Effexor®, Remeron®, and Wellbutrin® (to name a few) have been used to treat people with PD who have depression. All anti-depressants take 4-6 weeks before benefits are evident and dosage adjustment may be necessary. PWP may not receive adequate treatment for their depression. It may be necessary to treat the first episode of depression for 6-12 months. But continuing depression needs consistent treatment
with periodic review of the effectiveness of anti-depressant medication. Psychotherapy and regular exercise are also beneficial. Anxiety medications are available and the newer anti-depressants can be effective for anxiety as well. However, clinician assessment and monitoring is important to find the most appropriate medication given the individual’s symptoms.
Seek help and talk openly to your healthcare provider.
3:16
Dealing with Hallucinations, Delusions in Parkinson’s DiseaseFrom NPF’s: “How to React and Respond to Psychosis in Parkinson’s Disease”’
[Psychosis is a loss of sense of reality, which may exhibit in hallucinations, delusions, or delirium.]
* Practical Tips for Caregivers *
Talk to your loved one about their experiences with psychosis. They may be reluctant to introduce the subject on their own due to social stigmas related to mental illness. Openly discuss their thoughts, feeling and symptoms in a non-threatening environment. This can ease their anxiety and will allow you to have a better understanding of the situation.
Try to stay calm and patient. Caring for an individual who is experiencing psychosis can be very challenging and frustrating. Remember that the patient cannot control these symptoms. If you become angry, aggravated or demanding, the patient’s own aggression and agitation can worsen.
Be prepared and know how to handle the situation if your loved one should become agitated or aggressive: 1. Provide space without crowding.2. Talk calmly and evenly. Do not raise your voice.3. Provide reassurance. (“Everything is fine. You are safe.”)4. Keep your hands in view and your movements to a minimum.5. Inquire about their feelings and their reason for being upset.6. Listen to their responses and comments.
Examine the environment and make necessary adjustments. Below are several examples: • Visual hallucinations: Lighting at night can help reduce shadows and the risk for visual illusions.• Delusions and confusion: Keep dangerous objects in secure locations. Make sure furniture is arranged so
that a confused patient cannot trip and/or fall.• Agitation or aggression: Make sure that the environment is quiet and calm without disturbing noises or
distractions.
Do not challenge hallucinations or delusions by saying “They are not real”. Alternatively, do not reinforce psychosis by endorsing the illogical behaviors or ideas. Try generic phrases instead, such as: “I understand that the children appear real to you but I cannot see them I wonder if they might be a hallucination.”
Educate others who are frequently around your loved one about psychosis and mental health issues in PD. This will allow them to better understand the odd or unusual behaviors that they may observe. It can also relieve their fears and inhibitions while interacting with the patient. These individuals can be helpful in many situations, especially when you need immediate help.
Allow others to help. Caring for someone with Parkinson disease can be challenging enough. Psychosis can make it significantly more difficult. You cannot properly care for your loved one if you do not care for yourself. Do not be afraid to ask for assistance from family or friends or seek assistance from social services or home health agencies.
Safety must be a priority. Always ensure your own safety as well as the safety of your loved one. A patient who is experiencing psychosis can be confused, agitated, aggressive, suspicious and argumentative. If the situation becomes out-of-control and/or unsafe, leave the room and get help either from a family member, friend or neighbor. You can also call your local police department or 911. They can help gain control of the situation and will be understanding of the circumstances.
Explore available resources and options. In rare cases, psychosis may progress despite treatment. This can make home-based care extremely difficult. It is appropriate to consider placement in a facility that can provide constant supervision to ensure that the patient is not a threat to himself or others. This can either be on a short-term or long-term basis. Social workers can be excellent resources when considering alternative care options.
Source: Martine, Rebecca, APRN, CS, BC. “Psychosis in Parkinson’s Disease,” NPF’s Mind, Mood, & Memory. 2005
3:17
NW Clinic for Voice & Swallowing 3181 SW Sam Jackson Park Rd, Portland, OR 97239-3098 Tel: 503-494-5947
LEE SILVERMAN VOICE TREATMENT
LSVT is an effective treatment to improve speech in people with Parkinson disease.
Nearly every person (89%) with Parkinson disease will have problems with speech that start early in the disease process and progressively diminish quality of life.
o Soft voice o Mumbled speech o Monotone speech o Hoarse voice
LSVT is an intense 1 hour a day, 4-week course of therapy that teaches people with Parkinson disease to develop the strength required to speak at a normal vocal loudness. The strong research base behind LSVT has demonstrated substantive results:
o Improved vocal loudness o Improved intelligibility o More facial expression o Improved ability to swallow
LSVT teaches self-empowerment by improving the ability to communicate and in turn enhancing quality of life. Tips to Maximize Communication
o TALK LOUD – Your speech will become slower, clearer and more intelligible o Don’t trust your brain to tell you when you are loud enough – PD causes it to give
you bad feedback o Unless you think you are speaking too loudly, you are probably not loud enough
Clinicians at the Northwest Clinic for Voice and Swallowing are certified in the LSVT approach and are qualified to evaluate and treat people with the LSVT method. If you are interested in an evaluation of your speech and to learn more about LSVT:
o Ask your physician for a referral for a speech/voice evaluation o Contact the Northwest Clinic for Voice and Swallowing at OHSU at
503.494.5947
3:18
)
PATIENT'S CLINICALPATHWAY FOR SPEECHCOMMUNICATIONCHANGES WITHPARKINSON'S DISEASE
Melanie Fried-Oken, Ph.D., CCC/SpOHSU Augmentative Communication Clinic(503) 494-7587
Linda Bryans, M.A., CCC/SpOHSU Northwest Center for Voice andSwallowing(503) 494-2421
NOTES:
) )
This clinical pathway is a guide to help you with speechcommunication changes secondary to Parkinson's disease.Everyone experiences different symptoms and. differenttimelines in their disease. The changes you may experience aredivided into stages for you to understand what help is availablewhen these changes occur. This pathway identifies your team,assessment, treatment and intervention specific to speechandpatient education that you may receive. Speech-languagetherapies provided should be offered in conjunction withmedical management to help you compensate for the changesand/or improve your speech and voice. Early assessment andintervention for voice and speech problems will maximize yourcommunication skills. This clinical pathway is only a guide.Your plan may be changed to meet your individual needs.Please let us know if you have any special requirements.
We hope to make your care and visits a positive experience.We encourage you to ask your team members any questionsabout speech changes, options to make communication easier,or ways to enhance your communication.
Your team includes:Speech-language pathologistsOccupational therapistsPhysical therapistsSocial WorkersAssistive Technology (AAC) specialistsNurse/nurse practitionerPhysician
. Patient, family and friendsVendorsInsurance case managerPCO or PRO representative
3:19
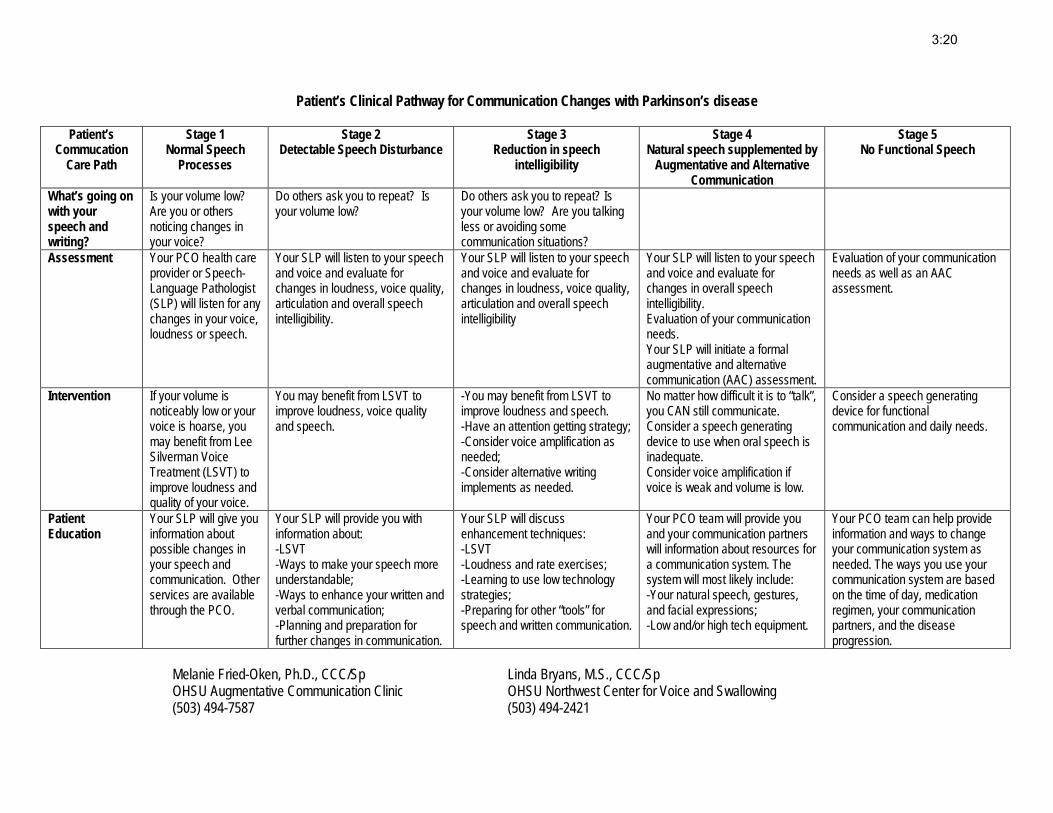
Patient’s Clinical Pathway for Communication Changes with Parkinson’s disease
Patient’s Commucation
Care Path
Stage 1 Normal Speech
Processes
Stage 2 Detectable Speech Disturbance
Stage 3 Reduction in speech
intelligibility
Stage 4 Natural speech supplemented by
Augmentative and Alternative Communication
Stage 5 No Functional Speech
What’s going on with your speech and writing?
Is your volume low? Are you or others noticing changes in your voice?
Do others ask you to repeat? Is your volume low?
Do others ask you to repeat? Is your volume low? Are you talking less or avoiding some communication situations?
Assessment Your PCO health care provider or Speech-Language Pathologist (SLP) will listen for any changes in your voice, loudness or speech.
Your SLP will listen to your speech and voice and evaluate for changes in loudness, voice quality, articulation and overall speech intelligibility.
Your SLP will listen to your speech and voice and evaluate for changes in loudness, voice quality, articulation and overall speech intelligibility
Your SLP will listen to your speech and voice and evaluate for changes in overall speech intelligibility. Evaluation of your communication needs. Your SLP will initiate a formal augmentative and alternative communication (AAC) assessment.
Evaluation of your communication needs as well as an AAC assessment.
Intervention If your volume is noticeably low or your voice is hoarse, you may benefit from Lee Silverman Voice Treatment (LSVT) to improve loudness and quality of your voice.
You may benefit from LSVT to improve loudness, voice quality and speech.
-You may benefit from LSVT to improve loudness and speech. -Have an attention getting strategy; -Consider voice amplification as needed; -Consider alternative writing implements as needed.
No matter how difficult it is to “talk”, you CAN still communicate. Consider a speech generating device to use when oral speech is inadequate. Consider voice amplification if voice is weak and volume is low.
Consider a speech generating device for functional communication and daily needs.
Patient Education
Your SLP will give you information about possible changes in your speech and communication. Other services are available through the PCO.
Your SLP will provide you with information about: -LSVT -Ways to make your speech more understandable; -Ways to enhance your written and verbal communication; -Planning and preparation for further changes in communication.
Your SLP will discuss enhancement techniques: -LSVT -Loudness and rate exercises; -Learning to use low technology strategies; -Preparing for other “tools” for speech and written communication.
Your PCO team will provide you and your communication partners will information about resources for a communication system. The system will most likely include: -Your natural speech, gestures, and facial expressions; -Low and/or high tech equipment.
Your PCO team can help provide information and ways to change your communication system as needed. The ways you use your communication system are based on the time of day, medication regimen, your communication partners, and the disease progression.
Melanie Fried-Oken, Ph.D., CCC/Sp Linda Bryans, M.S., CCC/Sp OHSU Augmentative Communication Clinic OHSU Northwest Center for Voice and Swallowing (503) 494-7587 (503) 494-2421
3:20
SWALLOWING AND PARKINSON DISEASE Swallowing is a complex process that begins with the sight of food. After the food is chewed and prepared into a ball or bolus it is moved back in the mouth. This first part of the swallowing process is called the oral stage. Parkinson disease can cause rigidity, tremors or dyskinesias in the muscles in the tongue, jaw, lips and face which can impact the oral stage of the swallow. The following symptoms can be signs of problems in the oral stage of swallowing:
• Reduced or effortful chewing• Drooling• Repetitive or excessive tongue movement• Difficulty moving the food to the back of the mouth• Food left in the mouth after the food is swallowed
The second stage of swallowing begins when the food or liquid is propelled from the tongue into the throat. This is called the pharyngeal stage. During this stage, the airway is closed and protected and then the food passes into the esophagus. Parkinson disease can cause the swallow to be delayed, reduce the contraction of the muscles in the throat, and reduce the sensation in the throat. The following symptoms can be signs of problems in the pharyngeal stage of swallowing:
• Choking or coughing while eating or drinking• Wet sounding voice after eating or drinking• Frequent throat clearing while eating or drinking• Avoidance of certain foods/textures or liquids• A sensation of food sticking in the throat• Unexplained weight loss• Unexplained fever or pneumonia
The esophageal stage is the final stage in swallowing. Here the food is squeezed down the esophagus and into the stomach. Parkinson disease can cause tightness in the sphincter at the top of the esophagus, reduced squeezing of the food down the esophagus and esophageal reflux. The following symptoms can be signs of problems in the pharyngeal stage of swallowing:
• Heartburn• Food coming back up into the throat or mouth after swallowing• Coughing after eating• Frequent coughing or throat clearing
Each of these stages occurs fairly quickly without our giving them much thought. For people with Parkinson disease, there can be disruption in each of these phases of the swallow. These problems can range from mild to fairly severe at the end stages of the disease process. A referral to a Speech-Language Pathologist and Dietician can be useful to establish dietary modifications and swallowing recommendations to facilitate safer swallowing with less effort.
*Information compiled by Linda Bryans, MA, CCC-SLPNorthwest Clinic for Voice and Swallowing
3:21
SWALLOWING TIPS FOR THE PERSON WITH PARKINSON DISEASE
The following is a list of suggestions that can improve swallowing safety and reduce the risk of aspiration (food or liquid entering the airway). It is important to note that not all swallowing suggestions work for every individual. A comprehensive swallowing evaluation is necessary to provide individualized recommendations to maximize safety and eating ability.
• Sit as upright as possible when eating or drinking• Tilt the chin slightly down when swallowing (never tilt the
had backward)• Completely swallow each bite or sip before taking another• Eat slowly – Don’t rush through your meal• Don’t talk while you are eating or drinking• Minimize distractions; turn off the TV, turn off the radio,
avoid conversation while eating• Take smaller bites/sips and chew your food well• Do not inhibit coughing; coughing clears the airway of
food/liquid• Do not continue eating if you are coughing a lot• Maximize sensory input; check dentures for placement/fit,
wear hearing aids and glasses at meal time as needed, andmaximize flavor and temperature to increase sensation
• Contact your physician if you notice swallowing problems todetermine if a swallowing evaluation is appropriate
• Have “easy to swallow” snacks on hand• Monitor hydration – make sure you are getting enough fluids
*Information compiled by Linda Bryans, MA, CCC-SLPNorthwest Clinic for Voice and Swallowing
3:22
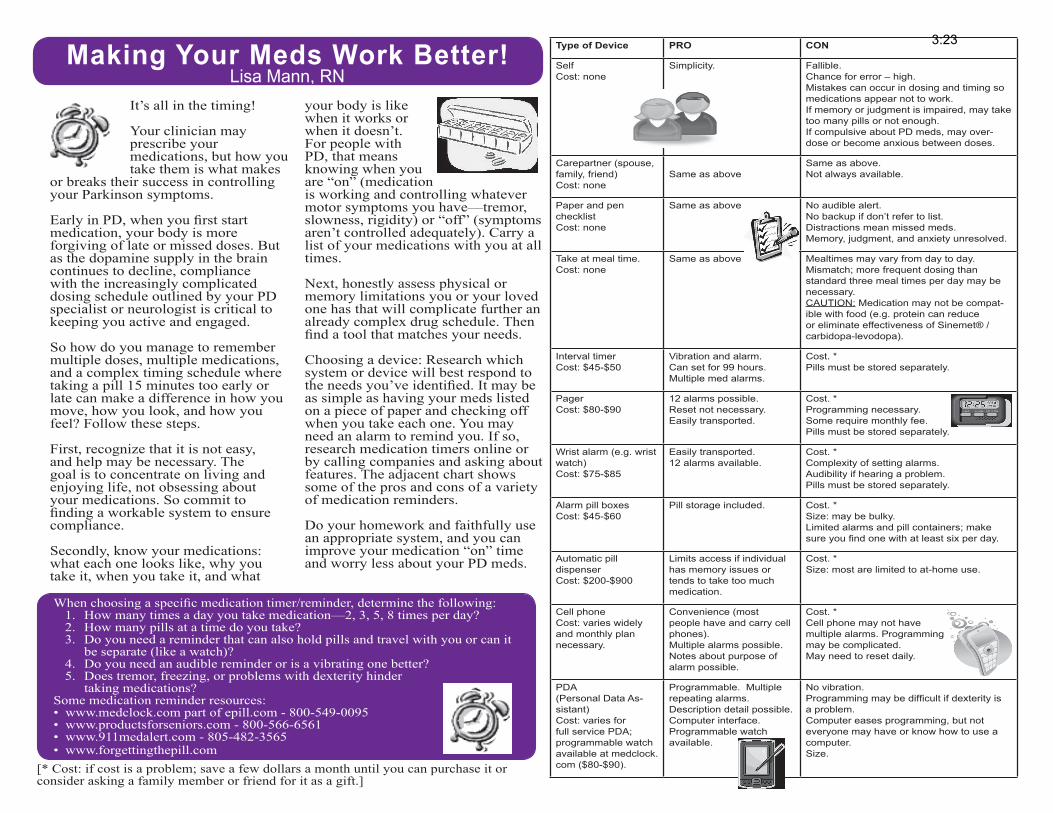
Making Your Meds Work Better!Lisa Mann, RN
Type of Device PRO CON
SelfCost: none
Simplicity. Fallible.Chance for error – high.Mistakes can occur in dosing and timing so medications appear not to work.If memory or judgment is impaired, may take too many pills or not enough.If compulsive about PD meds, may over-dose or become anxious between doses.
Carepartner (spouse, family, friend)Cost: none
Same as aboveSame as above.Not always available.
Paper and pen checklistCost: none
Same as above No audible alert.No backup if don’t refer to list.Distractions mean missed meds.Memory, judgment, and anxiety unresolved.
Take at meal time.Cost: none
Same as above Mealtimes may vary from day to day.Mismatch; more frequent dosing than standard three meal times per day may be necessary.CAUTION: Medication may not be compat-ible with food (e.g. protein can reduce or eliminate effectiveness of Sinemet® / carbidopa-levodopa).
Interval timerCost: $45-$50
Vibration and alarm.Can set for 99 hours. Multiple med alarms.
Cost. * Pills must be stored separately.
PagerCost: $80-$90
12 alarms possible.Reset not necessary.Easily transported.
Cost. * Programming necessary.Some require monthly fee.Pills must be stored separately.
Wrist alarm (e.g. wrist watch)Cost: $75-$85
Easily transported.12 alarms available.
Cost. * Complexity of setting alarms. Audibility if hearing a problem.Pills must be stored separately.
Alarm pill boxesCost: $45-$60
Pill storage included. Cost. *Size: may be bulky.Limited alarms and pill containers; make sure you find one with at least six per day.
Automatic pill dispenserCost: $200-$900
Limits access if individual has memory issues or tends to take too much medication.
Cost. * Size: most are limited to at-home use.
Cell phoneCost: varies widely and monthly plan necessary.
Convenience (most people have and carry cell phones).Multiple alarms possible.Notes about purpose of alarm possible.
Cost. *Cell phone may not have multiple alarms. Programming may be complicated.May need to reset daily.
PDA(Personal Data As-sistant)Cost: varies for full service PDA; programmable watch available at medclock.com ($80-$90).
Programmable. Multiple repeating alarms.Description detail possible. Computer interface.Programmable watch available.
No vibration.Programming may be difficult if dexterity is a problem.Computer eases programming, but not everyone may have or know how to use a computer.Size.
[* Cost: if cost is a problem; save a few dollars a month until you can purchase it or consider asking a family member or friend for it as a gift.]
When choosing a specific medication timer/reminder, determine the following:1. How many times a day you take medication—2, 3, 5, 8 times per day?2. How many pills at a time do you take?3. Do you need a reminder that can also hold pills and travel with you or can it
be separate (like a watch)?4. Do you need an audible reminder or is a vibrating one better?5. Does tremor, freezing, or problems with dexterity hinder
taking medications?Some medication reminder resources:• www.medclock.com part of epill.com - 800-549-0095• www.productsforseniors.com - 800-566-6561• www.911medalert.com - 805-482-3565• www.forgettingthepill.com
It’s all in the timing!
Your clinician may prescribe your medications, but how you take them is what makes
or breaks their success in controlling your Parkinson symptoms.
Early in PD, when you first start medication, your body is more forgiving of late or missed doses. But as the dopamine supply in the brain continues to decline, compliance with the increasingly complicated dosing schedule outlined by your PD specialist or neurologist is critical to keeping you active and engaged.
So how do you manage to remember multiple doses, multiple medications, and a complex timing schedule where taking a pill 15 minutes too early or late can make a difference in how you move, how you look, and how you feel? Follow these steps.
First, recognize that it is not easy, and help may be necessary. The goal is to concentrate on living and enjoying life, not obsessing about your medications. So commit to finding a workable system to ensure compliance.
Secondly, know your medications: what each one looks like, why you take it, when you take it, and what
your body is like when it works or when it doesn’t. For people with PD, that means knowing when you are “on” (medication is working and controlling whatever motor symptoms you have—tremor, slowness, rigidity) or “off” (symptoms aren’t controlled adequately). Carry a list of your medications with you at all times.
Next, honestly assess physical or memory limitations you or your loved one has that will complicate further an already complex drug schedule. Then find a tool that matches your needs.
Choosing a device: Research which system or device will best respond to the needs you’ve identified. It may be as simple as having your meds listed on a piece of paper and checking off when you take each one. You may need an alarm to remind you. If so, research medication timers online or by calling companies and asking about features. The adjacent chart shows some of the pros and cons of a variety of medication reminders.
Do your homework and faithfully use an appropriate system, and you can improve your medication “on” time and worry less about your PD meds.
3:23
ATTP II: Additional Physical Therapy/Exercise Resources
• www.ahta.orgWebsite of the American horticultural Therapy AssociationA good resource for those considering horticulture therapy as part of their program
• www.delaythedisease.comExercise program for Parkinson's designed by personal trainer David lidAvailable as a book: $19.95and in DVD format: $24.95
• www.deltasociety.orgWebsite with resources for animal assisted activities and therapy programs
• www.evolution.caEvolution Walkers2530 Davies Ave. Port Coquitlam, B.C. V3C 2J9, CanadaToll free: (800) 556-2558
• www.hipsavers.comAdaptive clothing offering joint protection for frequent fallers
• www.lsvtglobal.comWebsite for LSVT Big information, resources and training certification workshops
• www.motivatingmoves.com"Motivating Moves for people with Parkinson's" by Janet HamburgDistributed by the Parkinson Disease Foundation
1359 Broadway Suite 1509New York, NY 10018
Video (VHS, PAL or SECAM formats) or DVD $14.95
• www.nia.nih.govThe National Institute on Aging offers free publications on a variety of topics pertinent toseniors. These brochures may be useful for general patient education, when speaking tosupport groups, etc
• www.johnargue.com"Parkinson's disease and the Art of Moving" by John ArgueBook: $19.95 (in bookstore or online)Video/DVD companion (online only) $47.00"Parkinson's Disease and Activities of Daily Living (ADL)" $27.00
• www.rescueproject.orgWebsite of the multi-center European study "The Rescue Project" includes patient educationmaterials for downloading
3:24
• www.parkinsonspyramid.orgInformation from David Heydrick's model for Parkinson's management
• www.parknicollet.com/MethodistlparkinsonsStruthers Parkinson's Center website
• www.ustep.comInstep MobilityFor Ustep Walkers and Laser Canes(800) 558-7837
3:25

PROJECT PUBLICATIONS AND ABSTRACTSPublic Deliverables
Conference Abstracts
Peer Reviewed Papers
Information Sheets on Cueingfor People with Parkinson's Disease
Rescue Project CD Rom for Therapists
Information Sheets on Cueing for People with Parkinson's Disease
Background information on Cueing
Distractions can make it difficulty to concentrate on walking and distract your attention. When this happens your steps may become smaller, your walking slower and you may find you begin to shuffle or freeze on the spot. People find this can occur whilst turning around, moving in tight spaces, through doorways or in crowded environments. Cues can be used to help you focus your attention on walking so that it is easier to keep your feet moving while you walk around your home and community. Cues allow you to use other areas of the brain that are not affected by Parkinson’s disease, making movement faster and easier for short periods of time. Cues are used to give information about the number of steps taken while you walk and the size of your steps. Different types of cue can be used to provide this information.
Visual cues such as lines on the ground that a person steps over can be helpful where someone has difficulty with freezing, such as in a doorway at home. Putting a piece of tape across the doorway and stepping over it can be useful. It helps to focus attention on stepping and enables you to keep your feet moving. Other examples of visual cues can be lines or patterns on the carpet that you step your feet on or over, or stepping on the cracks between tiles or paving stones. This helps to keep the size of your steps regular and to focus attention on the quality of your walking.
Rhythmical cues such as tones given at a steady beat are also useful. These can be given with a metronome or alternatively by using music with the appropriate rhythm to step in time to. The rhythm should be set to a comfortable pace that you try to step each foot in time to. As you hear the beat you should think about stepping your feet in time to it. You can also try to associate taking a big step in time to the beat, try saying this in your head to begin with and withpractise this will become easier. Do not try to set the rhythm to high, start with it slower and see how your walking changes. You are aiming to take larger steps and practise at different speeds that are suited to the different surroundings. For example you will walk at a slower pace in your house compared to in an open space outside.
Attentional strategies can also be useful. This is where you rehearse movements in your mind (such as taking big steps) or count a rhythm in your head that you try to step in time to. As you walk youtry to focus your attention on those aspects of your walking that are difficult. For example, people report that they focus on putting their heels down firmly on the ground. It may be more difficult to use attentional strategies and keep concentrating without an external cue or reminder present.
Some more specific examples are given in the information sheets in relation to individual problems experienced by people.
No. 1 - Why walking becomes difficult in Parkinson's Disease No. 2 - What are cues and why can cues help? No. 3 - I walk more slowly now No. 4 - I tend to shuffle No. 5 - My feet stick to the ground (I freeze) No. 6 - The first step is the most difficult No. 7 - I'm alright in a straight line but changing direction is difficult No. 8 - I get stuck in the chair No. 9 - I can feel myself stooping No. 10 - I feel as if I am going to fall No. 11 - My walking is fine as long as no one talks to me No. 12 - I can't walk as far or as fast as I did No. 13 - I feel stiff generally No. 14 - Carers can cue too No. 15 - Involuntary movements (dyskinesia) affect my walking
Disclaimer: The RESCUE project cannot be held responsible for any of the information contained in the above Information Sheets. Therefore, if you are in doubt, please contact your doctor for further advice.
TOP
© Rescue Consortium, 2004. All Rights Reserved. Funded by the EC Fifth Framework Programme. Contact us: [email protected]. Site guide.
Page 1 of 1RESCUE
3/23/2012http://hces‐online.net/websites/rescue/pubs/info_sheets.htm
3:26
Information sheet 1
Why walking becomes difficult in Parkinson’s disease
It is important to remember that the basic walking pattern remains in tact in Parkinson’s disease, but new ways must be found to:
• Activate walking.
• Adjust the size and timing of the steps.
What causes walking to become difficult?
The basal ganglia is the part of the brain responsible for automatic movements (the ones we don’t usually think about) and is affected in Parkinson’s disease.
Due to loss of cells in the substantia nigra in the brain stem, a key chemical messenger – dopamine - responsible for automatic movement is depleted.
This automatic pilot is responsible for guiding our walking and other complex movements such as getting in and out of a chair or bed.
Changes in muscle tone (rigidity) can cause stiffness. Changes in balance mechanisms and involuntary movements (e.g. dyskinesia) can make people feel unsteady.
What sorts of difficulties are experienced?
• The length of steps becomes smaller.• The rhythm of walking is affected.• Starting and maintaining the walking pattern is a
problem.• Concentrating on other things while walking is
difficult.• Falling is more frequent.
This information was prepared by members of the Rescue
project
Last updated: August 2005
This project was funded by the European Commission under the Fifth Framework Quality of Life Programme, Contract Number
QLK6-2001-00120
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
3:27
Information sheet 2
What are cues and why can cues help?
3:28
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
What are cues?
Cues are prompts that give information on when and how an action should be carried out. In relation to walking this information can be about the timing of movement or the size of movements.
Types of cues
Cues can be –
Attention – thinking about your movement.
Auditory – a beat from a metronome or music.
Visual – a marker e.g. on the floor or wall.
Why can cues help?
Cues make movement less dependent on the automatic pilot, which is situated in the part of the brain affected by Parkinson’s disease.
Cues use a different route through the brain to activate and maintain movement.
This information was prepared by members of the Rescue
project
Last updated: March 2005
This project was funded by the uropean Commission under theFifth Framework Quality of Life
rogramme, Contract NumbeQLK6-2001-00120
E
P r
Information sheet 3
I walk more slowly now
3:29
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
Why do I walk more slowly?
• The rhythm of walking can be affected and thesteps do not follow each other as quickly.
• Walking is more effortful and stiff joints mayslow you down.
• If you have to concentrate on your walking it isdifficult to speed up.
• Because your steps become shorter you coverless distance in a given time.
When might this happen most?
• When you are tired.• When your medication does not work well.• When you are distracted.• When you have not been very active.
What can I do about it?
You can increase your speed of walking by using a faster rhythm than you normally use. You can increase your rhythm by counting in your head or by using a metronome beat.
You can think about taking bigger steps, making them long and even. You can use stripes in floor patterns, or on paving stones, as visual cues for this purpose.
You should never increase your speed if the quality of your walking suffers. This information was prepared
by members of the Rescue project
Last updated: March 2005
This project was funded by the uropean Commission under theFifth Framework Quality of Life
rogramme, Contract NumbeQLK6-2001-00120
E
P r
Information sheet 4
I tend to shuffle
3:30
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
Why do my steps become smaller?
• The automatic pilot in the brain is not sending a strong enough signal and the movement that results is therefore smaller.
• It can be more effortful to walk with bigger steps.
• Stiff muscles and joints can cause small steps. When might this happen most?
• When you have been walking for a while. • When you are distracted by another task such
as carrying something or talking. • If you have been inactive and are stiff, e.g. first
thing in the morning. • When your medication does not work well.
What can I do about it? Concentrate on keeping your steps long and even. This may be easier if you use a prompt such as counting or instructing yourself to ‘heel – toe’. This is more difficult in busy areas when you might be distracted so you might want to use an alternative cue.
Visual cues – using stripes in floor patterns, on paving stones. Auditory cues – use a rhythm from a metronome or a piece of music with a definite beat. This information was
prepared by members of the Rescue project
Last updated: March 2005
This project was funded by the European Commission under the Fifth Framework Quality of Life Programme, Contract Number QLK6-
2001-00120
You may have to reduce your normal number of steps to make them longer. It is better to take fewer, longer steps than lots of fast, shuffling ones.
Information sheet 5
My feet stick to the ground (I freeze)
3:31
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
Why do my feet stick to the ground?
• The automatic pilot in the brain stops givingthe instruction to step.
• Walking is a complex series of movements(steps) strung together in a sequence; if onepart of the sequence is interrupted the wholemovement can come to a stop.
When might this happen most?
• When you are approaching doorways, chairsor obstacles.
• When you are taking turns or changingdirection.
• When you are distracted by another task andstop focusing on your walking.
• In places that are crowded or cluttered andtherefore more difficult to negotiate.
• When the ‘flow’ of your walking is interruptedand you cannot keep a rhythm going.
• When your medication does not work well.
What can I do about it?
If you feel yourself sticking, S T O P . Think about standing tall with your feet apart. Shift your weight from side to side to unlock. Try making a very definite large step, and continue this pattern for the first few steps until you feel you’ve got going.
This information was prepared by members of
the Rescue project
Last updated: March 2005
This project was funded by the European Commission under the Fifth Framework Quality of Life Programme, Contract Number QLK6-
2001-00120
If there are areas where you stick often, you might want to use cues, e.g. a stripe on the floor to step over or stepping in time to a metronome beat.
Start to count or use the beat as you approach where you stick.
Information sheet 5 continued
Keep stepping during a turn or when opening a door.
3:32
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
If you need an extra prompt to keep stepping, start to stamp your feet on the floor. Stamping also works when you are turning.
This information was prepared by members of the Rescue
project
Last updated: March 2005
This project was funded by the uropean Commission under theFifth Framework Quality of Life
rogramme, Contract NumbeQLK6-2001-00120
E
P r
Information sheet 6
The first step is the most difficult
3:33
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
Why can’t I get going?
• The automatic pilot in the brain does not givethe instruction to step.
• The first step you take when walking is thestart of a complex sequence of movements, ifthis is not triggered correctly, the rest of thesequence can’t follow.
When might this happen most?
• After rising from a chair or bed.• Moving away from an obstacle such as a
kitchen bench when your first step is a turn.• In crowded or cluttered places.• When your medication is not working, early in
the morning or at night.
What can I do about it?
If you feel you can’t make a first step, try slowly rocking your weight from left to right, and then command yourself to step, and keep stepping. It might help to count when rocking and stepping.
You could take a step backwards or to the side to unlock the sticking if stepping forwards is difficult.
You could use a stripe on the floor to step over.
You could set a metronome rhythm to rock and step to. The rhythm should be slow and steady to allow you to make your first step large.
If you have got a choice, step into an open space rather than towards furniture or other obstacles.
This information was prepared by members of the Rescue
project
Last updated: March 2005
This project was funded by the uropean Commission under theFifth Framework Quality of Life
rogramme, Contract NumbeQLK6-2001-00120
E
P r
Information sheet 7
I’m alright in a straight line but changing direction is difficult
3:34
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
Why do I find turning difficult?
• Turning requires each leg to do somethingslightly different which is a much morecomplicated movement than walking in astraight line.
• Your walking rhythm that is generated whenwalking in a straight line is interrupted.
• Interruption of rhythm may make you freeze,i.e. your feet stick to the floor.
• Turning requires more balance and control.
When might this happen most?
• Sudden changes of direction, e.g. to avoidsomeone who has stepped in front of you, canbe difficult as this requires a fast response.
• When the path you are trying to negotiate iscomplicated, e.g. narrow walkways, obstaclesetc, requiring lots of changes of direction.
• When you have to turn after standing still, e.g.to move away from a bench you have beenstanding at.
• When your medication is not working well.
What can I do about it?
When needing to turn start to count before the turn and concentrate on not allowing your steps to get shorter as you turn. This information was
prepared by members of the Rescue project
Last updated: March 2005
This project was funded by the European Commission under the Fifth Framework Quality of Life Programme, Contract Number QLK6-
2001-00120
Avoid shuffling around on the spot. Instead use a wide arc with large definite steps.
You could place visual markers on the floor anywhere that turning is regularly difficult to encourage large steps.
Information sheet 7 continued
Stepping to a slow, steady beat will encourage larger steps and allow your feet to keep moving through the turn.
3:35
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
You may find Information sheet 5 helpful if you freeze.
This information was prepared by members of the Rescue
project
Last updated: March 2005
This project was funded by the uropean Commission under theFifth Framework Quality of Life
rogramme, Contract NumbeQLK6-2001-00120
E
P r
Information sheet 8
I get stuck in the chair
3:36
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
Why do I get stuck in the chair?
• It is often the first part of a movement that ismost difficult.
• Moving from one position (sitting) to a verydifferent position (standing) requires lots ofeffort from your muscles.
• Moving from one position to another requires acomplicated series of movements to happen ina specific order.
What can I do about it?
Rehearse the movement in your head. Have a set of simple commands for each part of the movement.
Front of chair Hands on chair arms Feet flat on floor Nose over toes (feel your weight move on to your feet)
Head up Stand tall
If you are sitting far back in a soft chair, rock from side to side to travel to the front of the chair. Counting may help this sideways movement. Once at the front of the chair, you can count whilst rocking gently forwards and backwards to give yourself some momentum to push up. This information was prepared
by members of the Rescue project
Last updated: March 2005
This project was funded by theuropean Commission undere Fifth Framework Quality oLife Programme, Contract
Number QLK6-2001-00120
E th f
As an alternative to counting, you can use a metronome beat or music.
You can use a visual target on the wall opposite to help you straighten as you stand.
Information sheet 9
I can feel myself stooping
3:37
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
Why do I tend to stoop?
• Your brain will not automatically remind you tostraighten up.
• Stiffness in your trunk can make it difficult tostraighten up.
• It is difficult to concentrate on your posturewhen you are thinking about your walking orother movements.
When might this happen most?
• If you have been in one position for a longtime, e.g. sitting watching television.
• When you are tired.• When you have to concentrate particularly
hard on another activity.• When your medication is not working well.
What can I do about it?
Try to be aware of your posture in sitting, standing and walking.
Have a checklist for good posture in sitting –
Am I sitting at the back of the seat? Am I using the headrest? Am I sitting centrally, not leaning over to one side?
Establish a prompt to revisit your checklist regularly, e.g. checking your posture each time the advertisements are shown on the television.
This information was prepared by members of the Rescue
project
Last updated: March 2005
This project was funded by theuropean Commission undere Fifth Framework Quality oLife Programme, Contract
Number QLK6-2001-00120
E th f
Use a visual target to help lift your gaze from the floor to aid good alignment, e.g. a clock on the wall.
Information sheet 10
I feel as if I am going to fall
3:38
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
Why do I feel as if I am going to fall?
• Walking with smaller steps makes it morelikely that you will catch your feet on the floor.(see Information sheet 4).
• If your feet stick you may feel like you areunable to correct yourself if you fall (seeInformation sheet 5).
• If you can’t take an initial step you may feelunsteady (see Information sheet 6).
• If you find it difficult to turn you might find thisis when you feel most unsteady (seeInformation sheet 7).
When might this happen most?
• In crowded or cluttered places.• On uneven or unpredictable terrain.• When distracted.• If you reach too far or too quickly, e.g. for a
door.• When your medication is not working well.
What can I do about it?
If you feel you are going to fall, try to stop with your feet apart and stand tall. Concentrate on your standing rather than reaching for support, which can make you overbalance.
To avoid feeling unsteady concentrate on making sure your heel hits the ground first, which will help your feet clear the floor. You could use stripes on the floor or paving stones to help your stepping.
This information was prepared by members of the Rescue
project
Last updated: March 2005
This project was funded by the uropean Commission under theFifth Framework Quality of Life
rogramme, Contract NumbeQLK6-2001-00120
E
P r
Take wide rather than sharp turns.
Information sheet 10 continued Stand close to anything you want to reach for and avoid stretching too far.
3:39
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
Have a well-rehearsed strategy to help you get going when you stick and tend to fall. Identify areas where you often feel unsteady so you are more aware of where you are at risk.
This information was prepared by members of the Rescue
project
Last updated: March 2005
This project was funded by the uropean Commission under theFifth Framework Quality of Life
rogramme, Contract NumbeQLK6-2001-00120
E
P r
Information sheet 11
My walking is fine as long as no one talks to me
3:40
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
Why do I find it difficult to walk when distracted?
• The other activity such as talking takes yourfocus away from your walking.
• The automatic pilot in the brain does not takeover the control of your walking.
• While your attention is distracted by the othertask your walking may suffer.
When might this happen most?
• When there are other people around who willdistract you.
• When you are doing something else as well aswalking such as housework or shopping.
• When you are unable to focus on your walking.
What can I do about it?
Identify which activities are difficult to perform, e.g. walking and carrying an item, walking and talking. If possible do one element of a task at a time, e.g. stop to read a list then continue to shop.
Concentrating on your walking – taking large steps, making wide turns – can help keep you safe when there are distractions around.
This information was prepared by members of the Rescue
project Use a metronome beat is a way of focusing your attention on to your stepping. Last updated: March 2005
This project was funded by the uropean Commission under theFifth Framework Quality of Life
rogramme, Contract NumbeQLK6-2001-00120
E
P r
Information sheet 11 continued
If you are at risk of falling when doing two things at once,
3:41
avoid the situation. Consider finding an alternative way of performing the activity. An occupational therapist is likely to be able to offer advice.
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
This information was prepared by members of the Rescue
project
Last updated: March 2005
This project was funded by the uropean Commission under theFifth Framework Quality of Life
rogramme, Contract NumbeQLK6-2001-00120
E
P r
Information sheet 12
I can’t walk as far or as fast as I did
3:42
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
Why can’t I walk as far and as fast as before?
• Walking is more effortful than usual because you have to think about what you are doing.
• Muscles and joints that are stiff are more difficult to move and tire more easily.
• If you are generally doing less your level of fitness will suffer.
What can I do about it? It is important to maintain your fitness level to allow you to walk to the best of your ability. Walking at a slightly increased speed in time to a beat is a good way of improving your cardiovascular fitness. Using a slightly slower rhythm allows you to maintain the quality of your walking pattern over a greater distance to improve your endurance. You may find with regular practise, e.g. walking for half an hour a day, you can walk further and faster.
This information was prepared by members of the Rescue
project
Last updated: March 2005
This project was funded by the uropean Commission under theFifth Framework Quality of Life
rogramme, Contract NumbeQLK6-2001-00120
E
P r
Information sheet 13
I feel stiff generally
Why do I feel stiff all over?
3:43
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
• If movements are more difficult the tendencycan be to avoid doing them which leads tomore stiffness.
• Poor posture can lead to stiff joints.• If you are walking with shorter steps you are
not stretching the leg muscles as much asusual.
Where might I feel most stiff?
• The joints of your spine and shoulders areparticularly prone to stiffness.
• Your legs will feel stiff if you are less mobile.• You may have stiffness in your hands and
arms if coordination is difficult.• When your medication is not working well,
especially early in the morning.
What can I do about it?
Moving well will allow you to be more active and will reduce your level of stiffness.
Working on the quality of your walking and your posture will be beneficial.
Regularly moving all the major joints in your body through their full range of movement will prevent stiffness. Using a rhythm or music will help you to make the movements bigger.
This information was prepared by members of the Rescue
project
Last updated: March 2005
This project was funded by theuropean Commission undere Fifth Framework Quality oLife Programme, Contract
Number QLK6-2001-00120
E th f
If you have a specific area of stiffness, a physiotherapist may show you stretches or exercises to help. They may suggest a general exercise group in the community.
Information sheet 14
Carers can cue too
Using cues is about providing prompts not physical
3:44
assistance. People with Parkinson’s disease may need instructions and you should not feel guilty about giving them. You are aiming to help the person you are caring for improve the quality of their movement and therefore do as much as possible for themselves.
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
What can I do when the person I am caring for … ? … walks slowly or with shuffling steps Walk beside them at a steady pace and encourage them to match their footsteps to yours. Count in a steady rhythm to encourage regular longer steps. … has difficulty initiating the first step or freezes Encourage the person to stand tall with feet wide. A steady count to sway to can help to unlock. Give a target to step over, e.g. point to a pattern on the carpet. Encourage big steps. Often if you can avoid shuffling you can avoid freezing. Give them prior warning of something that can cause freezing. Use a strategy such as counting out loud to enable stepping to continue.
This information was prepared by members of the Rescue
project
Last updated: March 2005
This project was funded by theuropean Commission undere Fifth Framework Quality oLife Programme, Contract
Number QLK6-2001-00120
E th f
… has difficulty turning Give as much room as possible, do not stand too close to someone. Ensure you turn together in an arc, not sharply.
Information sheet 14 continued
… gets stuck in the chair
Give short, clear commands for each stage of the movement, e.g. come to the front of the chair, etc.
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
… has a stooped posture
Give feedback about how straight they are sitting or standing.
Provide a target ahead to focus on to encourage straightening.
… has a tendency to feel unsteady
Avoid distracting with too much talking whilst walking as they may need to concentrate on their steps.
Bring deterioration in walking to their attention and encourage larger steps by example or by counting.
Encourage them to walk tall rather than leaning on you.
… has difficulty doing two things at once
Help them to break tasks down so that one element is completed at a time as far as possible.
If you notice they walk poorly when they are distracted, draw their attention back to their stepping.
… can’t walk as far or as fast
This information was prepared by members of the Rescue
project
Last updated: March 2005
This project was funded by theuropean Commission undere Fifth Framework Quality oLife Programme, Contract
Number QLK6-2001-00120
E th f
Think about a realistic target distance to walk, and try to gradually increase it over time.
Providing a steady pace will prevent them from walking with short, shuffling steps which is tiring.
3:45
Information sheet 14 continued … feels stiff
3:46
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
Performing simple exercises together, perhaps to music, will benefit you both. Encourage large, full range movements.
This information was prepared by members of the Rescue
project
Last updated: March 2005
This project was funded by the uropean Commission under theFifth Framework Quality of Life
rogramme, Contract NumbeQLK6-2001-00120
E
P r
Information sheet 15
Involuntary movements (dyskinesia) affect my walking
Why do I find it difficult to walk with dyskinesia?
• Involuntary movements are unpredictable – mostly you do not know when they will occur, for how long or the type or size of movement they might be.
• Walking is made up of a number of sub-movements that occur in sequence. Involuntary movements disrupt the flow of the sequence, affecting balance and safety.
When might this happen most?
• Both increasing and decreasing the dosage of Parkinson’s disease medication may cause involuntary movements.
• Over time the response to medication can become shortened and unpredictable and involuntary movements may appear. They can occur in the period before and after dosage.
• In advanced Parkinson’s disease the benefits of the ‘on’ phase between two doses of medication can be affected by involuntary movements.
What can I do about it? Close monitoring of medication response is needed to maximise drug therapy and minimise side effects. Find a pattern on the floor, e.g. tiles on the pavement, to guide your feet while walking. This can help you to both walk in a straight line and avoid drifting to the side. Walking at a slightly increased speed in time to a beat may help as this restricts the time available for the involuntary movements to disrupt stepping.
Rehabilitation in Parkinson’s Disease: Strategies for Cueing
This information was prepared by members of the Rescue
project
Last updated: August 2005
This project was funded by the European Commission under the Fifth Framework Quality of
Life Programme, Contract Number QLK6-2001-00120
3:47
Published on FCC.gov (http://www.fcc.gov)
Home > Printer-friendly > Printer-friendly
Speech-To-Speech Relay ServiceBackground
Speech-to-Speech (STS) is one form of Telecommunications Relay Service (TRS). TRS is a service that allows persons with hearing and speech disabilities to access the telephone system to place and receive telephone calls. STS enables persons with a speech disability to make telephone calls using their own voice (or an assistive voice device). Like all forms of TRS, STS uses specially trained operators – called Communications Assistants (CAs) – to relay the conversation back and forth between the person with the speech disability and the other party to the call. STS CAs are specially trained in understanding a variety of speech disorders, which enables them to repeat what the caller says in a manner that makes the caller’s words clear and understandable to the called party.
Who Uses STS
Often people with speech disabilities cannot communicate by telephone because the parties they are calling cannot understand their speech. People with cerebral palsy, multiple sclerosis, muscular dystrophy, Parkinson's disease and those who are coping with limitations from a stroke or traumatic brain injury may have speech disabilities. People who stutter or have had a laryngectomy may also have difficulty being understood. In general, anyone with a speech disability or anyone who wishes to call someone with a speech disability can use STS.
Using STS
A special phone is not needed for STS. You simply call the relay center by dialing 711, and indicate you wish to make an STS call. You are then connected to an STS CA who will repeat your spoken words, making the spoken words clear to the other party. Persons with speech disabilities may also receive STS calls. The calling party calls the relay center by dialing 711 and asks the CA to call the person with a speech disability.
Alternatives
Persons with speech disabilities may use a TTY to make a TRS call, but many such people have some type of physical limitation that makes typing into a text input device difficult. STS offers an alternative to a TTY or other text input device when the only other option would be not to communicate via telephone at all. Some STS providers also offer STS service for Spanish to Spanish callers.
Page 1 of 3Speech‐To‐Speech Relay Service
3/23/2012http://www.fcc.gov/print/node/32092
3:48
Mandatory Minimum Standards for STS
The FCC imposes mandatory minimum standards on providers of all forms of TRS, such as ensuring user confidentiality, making service available 24 hours a day, seven days a week, and answering 85 percent of calls within 10 seconds. The FCC also imposes certain additional requirements on STS providers. For example, STS CAs must remain with a call for a minimum of 15 minutes. In addition:
An STS CA may, at the request of the user, retain information from a particular call in order to facilitate the completion of consecutive calls. The user may ask the TRS CA to retain such information, or the CA may ask the user if he or she wants the CA to repeat the same information during subsequent calls. The STS CA may retain the information only for as long as it takes to complete the subsequent calls.
•
STS providers must offer STS users the option to maintain at the relay center a list of names and telephone numbers that the STS user commonly calls. When the STS user requests one of these names, the CA must repeat the name and state the telephone number to the STS user. This information must be transferred to any new STS provider.
•
STS has emergency call procedures in case an STS user calls 911.•
For further information on the TRS mandatory minimum standards, and other types of TRS in addition to STS, go to www.fcc.gov/guides/telecommunications-relay-service-trs [1].
Filing a Complaint with the FCC
If you have a problem with STS Relay Service, first try to resolve it with the provider. If you are unable to resolve it directly, you can file a complaint with the FCC. There is no charge for filing a complaint. You can file your complaint using an online complaint form [2]. You can also file your complaint with the FCC’s Consumer Center by calling 1-888-CALL-FCC (1-888-225-5322) voice or 1-888-TELL-FCC (1-888-835-5322) TTY; faxing 1-866-418-0232; or writing to:
Federal Communications Commission Consumer & Governmental Affairs Bureau
Consumer Inquiries and Complaints Division 445 12th Street, SW
Washington, D.C. 20554.
What to Include in Your Complaint
The best way to provide all the information the FCC needs to process your complaint is to thoroughly complete the online complaint form. When you open the online complaint form, you will be asked a series of questions that will take you to the particular section of the form you need to complete. If you do not use the online complaint form, your complaint, at a minimum, should indicate:
your name, address, email address and phone number where you can be reached;•whether you are filing a complaint on behalf of another party, and if so, the party’sname, address, email address, day time phone number and your relationship to theparty;
•
Page 2 of 3Speech‐To‐Speech Relay Service
3/23/2012http://www.fcc.gov/print/node/32092
3:49
preferred format or method of response (letter, fax, voice phone call, email, TRS, TTY, ASCII text, audio recording or Braille);
•
that your complaint is about TRS;•the name, address and telephone number (if known) of the company or companies involved with your complaint; and
•
a brief description of your complaint and the resolution you are seeking, and a full description of the equipment or service you are complaining about, including date of purchase, use or attempt to use.
•
For More Information
For more information about STS Relay Service or TRS, or to learn more about FCC programs to promote access to telecommunications services for people with disabilities, visit the FCC’s Disability Rights Office website [3]. For information about other telecommunications issues, visit the FCC’s Consumer & Governmental Affairs Bureau website [4], or contact the FCC’s Consumer Center using the information provided for filing a complaint.
Print Out
Speech-To-Speech Relay Service Guide [5] (pdf)
Consumer & Governmental Affairs [6]
Consumer & Governmental Affairs
Source URL: http://www.fcc.gov/guides/speech-speech-relay-service
Links: [1] http://www.fcc.gov/guides/telecommunications-relay-service-trs [2] http://www.fcc.gov/complaints [3] http://www.fcc.gov/cgb/dro [4] http://www.fcc.gov/consumer-governmental-affairs-bureau [5] http://www.fcc.gov/cgb/consumerfacts/speechtospeech.pdf [6] http://www.fcc.gov/category/bureau-office/consumer-governmental-affairs
Page 3 of 3Speech‐To‐Speech Relay Service
3/23/2012http://www.fcc.gov/print/node/32092
3:50
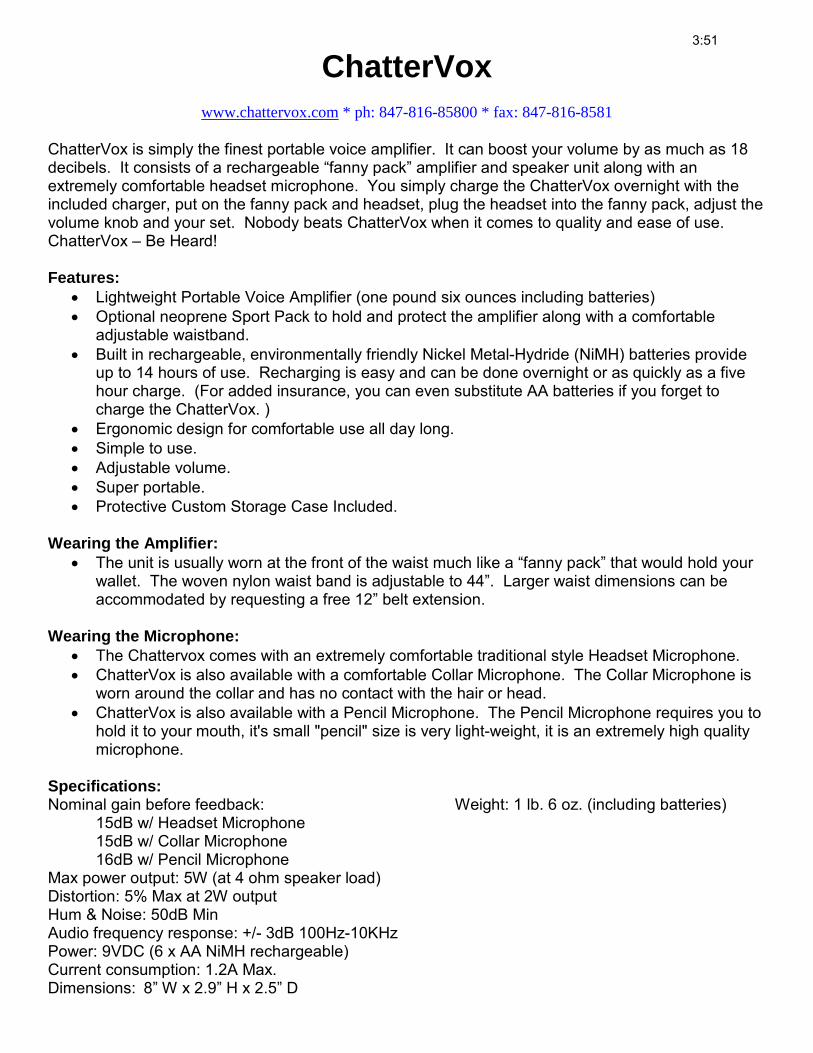
ChatterVox www.chattervox.com * ph: 847-816-85800 * fax: 847-816-8581
ChatterVox is simply the finest portable voice amplifier. It can boost your volume by as much as 18 decibels. It consists of a rechargeable “fanny pack” amplifier and speaker unit along with an extremely comfortable headset microphone. You simply charge the ChatterVox overnight with the included charger, put on the fanny pack and headset, plug the headset into the fanny pack, adjust the volume knob and your set. Nobody beats ChatterVox when it comes to quality and ease of use. ChatterVox – Be Heard! Features:
• Lightweight Portable Voice Amplifier (one pound six ounces including batteries) • Optional neoprene Sport Pack to hold and protect the amplifier along with a comfortable
adjustable waistband. • Built in rechargeable, environmentally friendly Nickel Metal-Hydride (NiMH) batteries provide
up to 14 hours of use. Recharging is easy and can be done overnight or as quickly as a five hour charge. (For added insurance, you can even substitute AA batteries if you forget to charge the ChatterVox. )
• Ergonomic design for comfortable use all day long. • Simple to use. • Adjustable volume. • Super portable. • Protective Custom Storage Case Included.
Wearing the Amplifier:
• The unit is usually worn at the front of the waist much like a “fanny pack” that would hold your wallet. The woven nylon waist band is adjustable to 44”. Larger waist dimensions can be accommodated by requesting a free 12” belt extension.
Wearing the Microphone:
• The Chattervox comes with an extremely comfortable traditional style Headset Microphone. • ChatterVox is also available with a comfortable Collar Microphone. The Collar Microphone is
worn around the collar and has no contact with the hair or head. • ChatterVox is also available with a Pencil Microphone. The Pencil Microphone requires you to
hold it to your mouth, it's small "pencil" size is very light-weight, it is an extremely high quality microphone.
Specifications: Nominal gain before feedback: 15dB w/ Headset Microphone 15dB w/ Collar Microphone 16dB w/ Pencil Microphone Max power output: 5W (at 4 ohm speaker load) Distortion: 5% Max at 2W output Hum & Noise: 50dB Min Audio frequency response: +/- 3dB 100Hz-10KHz Power: 9VDC (6 x AA NiMH rechargeable) Current consumption: 1.2A Max. Dimensions: 8” W x 2.9” H x 2.5” D
Weight: 1 lb. 6 oz. (including batteries)
3:51
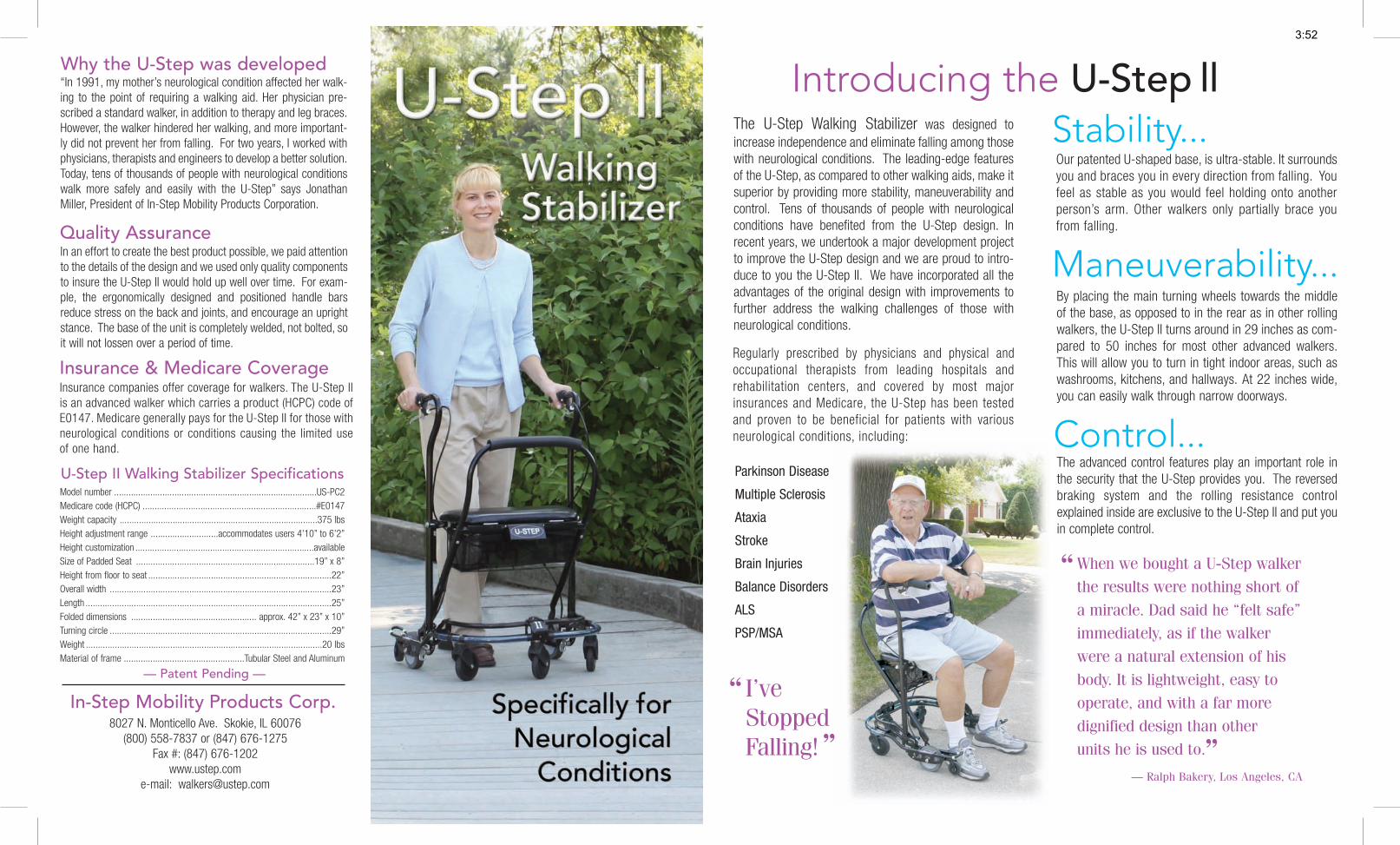
Parkinson Disease
Multiple Sclerosis
Ataxia
Stroke
Brain Injuries
Balance Disorders
ALS
PSP/MSA
The advanced control features play an important role inthe security that the U-Step provides you. The reversedbraking system and the rolling resistance controlexplained inside are exclusive to the U-Step II and put youin complete control.
“In 1991, my mother’s neurological condition affected her walk-ing to the point of requiring a walking aid. Her physician pre-scribed a standard walker, in addition to therapy and leg braces.However, the walker hindered her walking, and more important-ly did not prevent her from falling. For two years, I worked withphysicians, therapists and engineers to develop a better solution.Today, tens of thousands of people with neurological conditionswalk more safely and easily with the U-Step” says JonathanMiller, President of In-Step Mobility Products Corporation.
Model number ....................................................................................US-PC2Medicare code (HCPC) ........................................................................#E0147Weight capacity ..................................................................................375 lbsHeight adjustment range ............................accommodates users 4’10” to 6’2”Height customization ..........................................................................availableSize of Padded Seat ..........................................................................19” x 8”Height from floor to seat ............................................................................22”Overall width ............................................................................................23”Length ......................................................................................................25”Folded dimensions .................................................... approx. 42” x 23” x 10”Turning circle ............................................................................................29”Weight ..................................................................................................20 lbsMaterial of frame ..................................................Tubular Steel and Aluminum
— Patent Pending —
By placing the main turning wheels towards the middleof the base, as opposed to in the rear as in other rollingwalkers, the U-Step II turns around in 29 inches as com-pared to 50 inches for most other advanced walkers.This will allow you to turn in tight indoor areas, such aswashrooms, kitchens, and hallways. At 22 inches wide,you can easily walk through narrow doorways.
Our patented U-shaped base, is ultra-stable. It surroundsyou and braces you in every direction from falling. Youfeel as stable as you would feel holding onto anotherperson’s arm. Other walkers only partially brace youfrom falling.
I’veStoppedFalling!
Regularly prescribed by physicians and physical andoccupational therapists from leading hospitals andrehabilitation centers, and covered by most majorinsurances and Medicare, the U-Step has been testedand proven to be beneficial for patients with variousneurological conditions, including:
Introducing the U-Step llStability...
Control...
Maneuverability...
The U-Step Walking Stabilizer was designed toincrease independence and eliminate falling among thosewith neurological conditions. The leading-edge featuresof the U-Step, as compared to other walking aids, make itsuperior by providing more stability, maneuverability andcontrol. Tens of thousands of people with neurologicalconditions have benefited from the U-Step design. Inrecent years, we undertook a major development projectto improve the U-Step design and we are proud to intro-duce to you the U-Step II. We have incorporated all theadvantages of the original design with improvements tofurther address the walking challenges of those withneurological conditions.
When we bought a U-Step walkerthe results were nothing short ofa miracle. Dad said he “felt safe”immediately, as if the walkerwere a natural extension of hisbody. It is lightweight, easy tooperate, and with a far moredignified design than otherunits he is used to.
Why the U-Step was developed
In an effort to create the best product possible, we paid attentionto the details of the design and we used only quality componentsto insure the U-Step II would hold up well over time. For exam-ple, the ergonomically designed and positioned handle barsreduce stress on the back and joints, and encourage an uprightstance. The base of the unit is completely welded, not bolted, soit will not lossen over a period of time.
Quality Assurance
In-Step Mobility Products Corp.
Insurance companies offer coverage for walkers. The U-Step IIis an advanced walker which carries a product (HCPC) code ofE0147. Medicare generally pays for the U-Step II for those withneurological conditions or conditions causing the limited useof one hand.
8027 N. Monticello Ave. Skokie, IL 60076(800) 558-7837 or (847) 676-1275
Fax #: (847) 676-1202www.ustep.com
e-mail: [email protected]
Insurance & Medicare Coverage
U-Step II Walking Stabilizer Specifications
— Ralph Bakery, Los Angeles, CA””
“
“
3:52

U-Step II Advanced features to address your walking needs...Reversed Braking System
Laser & Sound Cueing Module
Easily Transported
4-inch non-markingcasters
Paddedseat
Tension control
Heightadjustable
Adjustablebackrest
Spring-loadedfront wheel Place to step for
going up curbs
Glow-in-the-Dark tabs
Lasermodule(Optional)
Laser projectedred line
ErgonomicallyPositionedHandlebars
Comfort grips
Removablebasket
Included with the U-Step II is an Alternative Brake Accessory that allows you to hold onto a middle bar to walk, rather than hand grips on each side. The accessory is not commonly used.
The innovative braking system is easyto use and puts you in complete con-trol. The U-Step will not roll until youlightly squeeze either hand brake.Once you release the hand brake, theunit will stop immediately. This featureis particularly helpful when standingup from a chair because the unit willnot roll away from you.
Lifting a walker to go up a curb orsmall stair can be dangerous. Thisinnovative feature is designed to helpyou safely and easily go up a curb orone step. Either by stepping down onthe back of the base or just by pullingback on the handlebars, you can raisethe front of the walker to go up a curbor small step.
Folding the U-Step II is as easy as one, two,three! Lift the release lever by the seat, pull upon the seat support tofold the U-Step II andput it in the car; nobending down to pickit up. The U-Step IIis four pounds lighterthan the original U-Step, making it easierto lift and transport.
Handling Curbs
Optional Weights Alternative Brake Accessory
Rolling Resistance Control
Spring-Loaded Front Wheel
Primarily used by those with Parkinson’sfreezing but can be used by anyone with anirregular gait pattern. The Laser and SoundCueing Module can help get you started,normalize your walking and increase yourstride. Press the red button on the moduleto project a bright red laser line on the floorto guide your step. You can also turn on thesound feature to set a beat pattern forwalking speed.
The patented spring-loadedfront caster system glideseasily over uneven surfaces,such as indoor moldingstrips and cracks in the side-walk. This avoids suddenjolts as well as the need tolift the walker over smallobstacles.
Unlike other rollingwalkers, you can adjustthe rolling speed of theU-Step II. Many peoplefind wheeled walkersroll too fast for them.That is why we engi-neered a control forsetting the rolling
resistance. Loosen the set screw and rotate the adjustment lever tothe desired amount of resistance, then re-tighten the set screw.
Although the U-Step is very stable, we do offer weights as an accessory to increase the stabilityof the walker. These weights easily secure to the base of the U-Step II using Velco straps.
3:53
U-STEP Supporting Documentation Letter SAMPLE
To Whom It May Concern:
My patient, [NAME], has a severe neurological condition-Parkinson's disease (PD), that is progressive in nature (ICD-9 code 332.0). I am prescribing the U-Step walking stabilizer (DMERC Model # US-PC) Medicare code EO147, produced by In-Step Mobility.
My patient's gait has been severely affected by this condition. Therefore, after trying a standard wheeled walker, it is apparent that due to the severity of [HER/HIS] neurological condition my patient requires an advanced walking aid with multiple braking system and variable wheel resistance to ambulate.
[NAME]'s PD is fairly advanced, and [S/HE] experiences fluctuations to [HER/HIS] medications, which also impact [HER/HIS] mobility. These reactions can range from [HER/HIS] being dyskinetic to freezing. [HER/HIS] posture is flexed forward and can cause postural imbalance related to a shift of [HER/HIS] center of gravity and may also contribute to falling. Fatigue and freezing (sudden inability to move) are also problems for this patient.
[NAME]'s Parkinson's disease is progressive and chronic; so, it will continue to impair safe mobility. Therefore, I feel the U-Step walker would enhance [HER/HIS] safety more than a normal walker given its unique braking reverse braking design, wheel resistance, laser-cuing ability, and special U-shaped framing all of which help correct the mobility problems inherent in PD patients generally, and specifically for [NAME]'s case as described.
The recommended walker for this patient would include: > U-Step walking stabilizer (DMERC Model # US-PC; Medicare code EO147) > Laser-line attachment to counter freezing > Seat for the walking stabilizer (Medicare code EO156) for fatigue
3:54
TEAM QUESTIONS: Have you ever experienced….?
Occupational Therapy Questions:
Trouble “getting started” in the morning?
Trouble with zippers or buttons?
Not able to stand up from the toilet?
Trouble figuring out which way a shirt goes on?
Difficulty telling how far down a step is from your foot?
Problems writing out a check because your handwriting has changed?
Not enough energy to get through the day?
Physical Therapy Questions:
A fall, near falls or stumbling?
Problems going up or down stairs?
Difficulty turning around or turning corners while walking?
Difficulty standing up from a chair or getting out of bed?
Stiffness and you don’t know how to stretch?
Need new equipment (walker or wheelchair) and don’t know where to start?
Increased stress and unable to relax?
Pain in your back or shoulders?
Speech-Language Pathology Questions:
People having difficulty understanding you?
Have the word on the ‘tip of your tongue’ without being able to find it?
Difficulty remembering details of daily routine, conversations, etc?
Easily distracted; Short attention span, etc?
Interdisciplinary Questions
Concerns with maintaining employment?
Questions about care-partner safety or burn-out?
Questions about changes in your home for safety?
If you answered yes to any of these questions, you should consider asking your physician for an order for OT, PT or SLP.
3:55