Embed Size (px)
DESCRIPTION
endocrine lecture for anatomy & physiology
Citation preview
Section 3, Chapter 13
The Peripheral Endocrine Glands
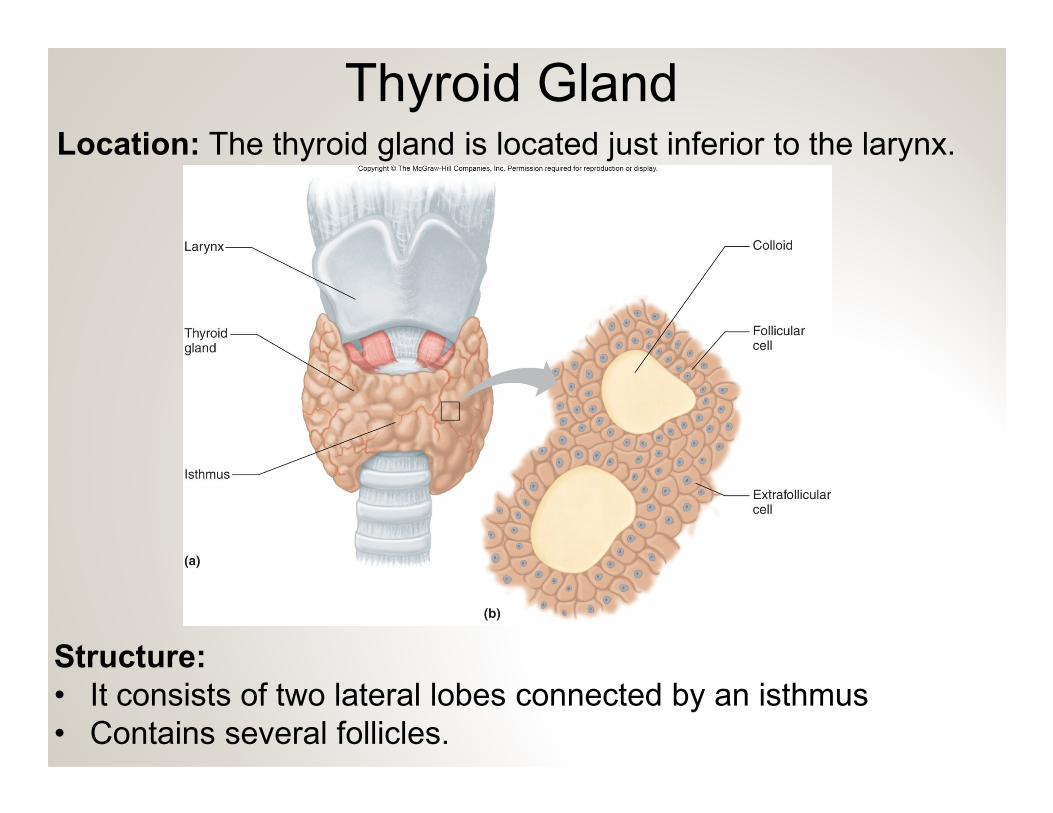
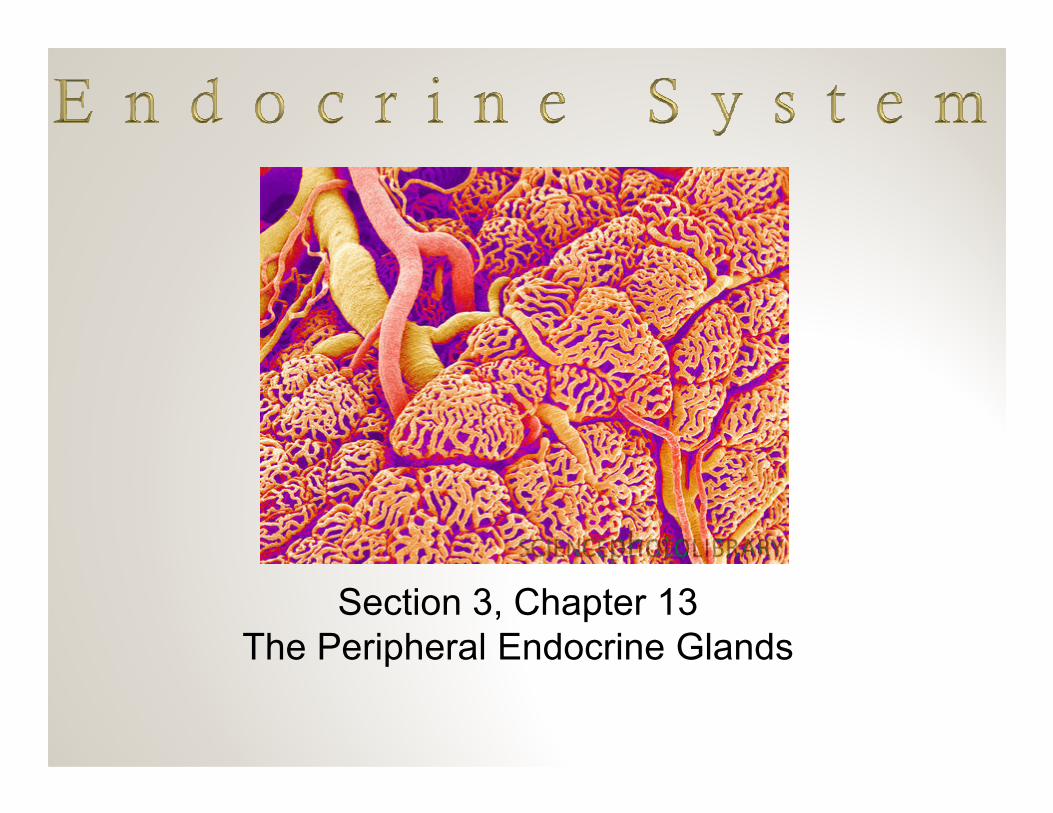
Thyroid GlandLocation: The thyroid gland is located just inferior to the larynx.
Structure:
• It consists of two lateral lobes connected by an isthmus
• Contains several follicles.
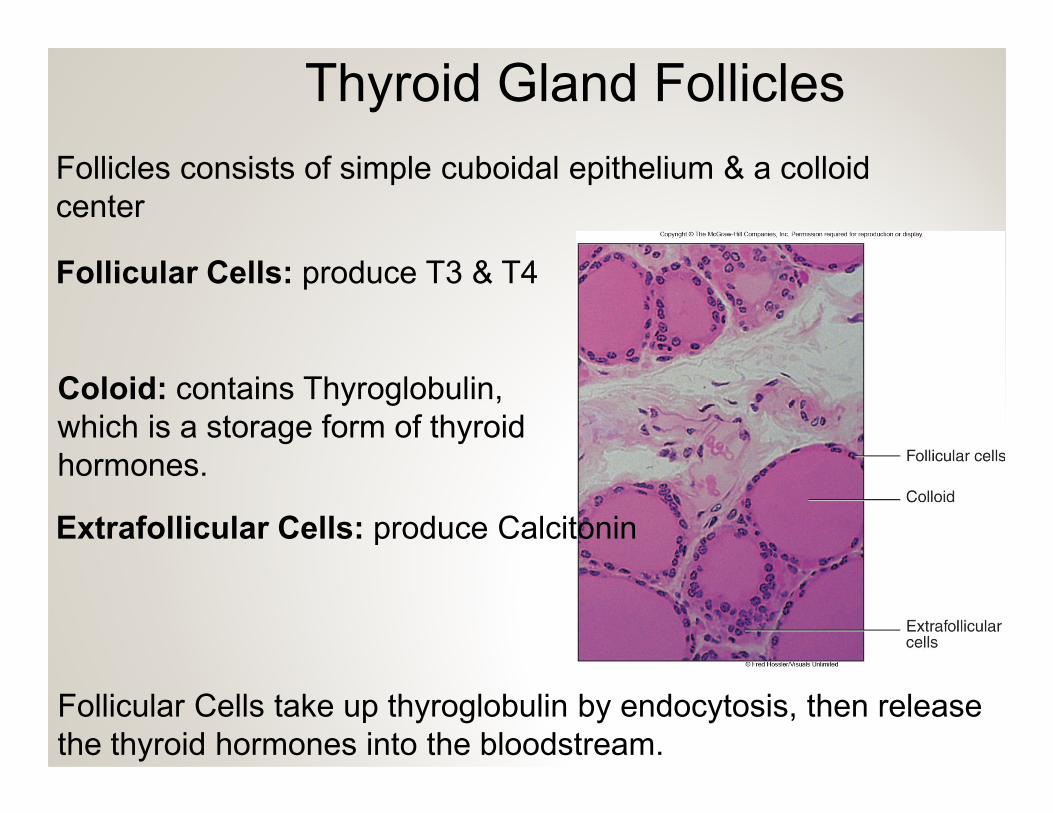
Thyroid Gland Follicles
Follicles consists of simple cuboidal epithelium & a colloid
center
Follicular Cells: produce T3 & T4
Coloid: contains Thyroglobulin,
which is a storage form of thyroid
hormones.
Follicular Cells take up thyroglobulin by endocytosis, then release
the thyroid hormones into the bloodstream.
Extrafollicular Cells: produce Calcitonin
Thyroid Hormones
Target Cells: T3 & T4 affect many cells throughout the body.
Actions of T3 & T4: Raise Metabolic Rate
• Increase rate of carbohydrate catabolism
• Enhance protein synthesis
• Promotes the breakdown and use of lipids
T3 & T4 are major factors in determining the basal metabolic rate T3 & T4 are major factors in determining the basal metabolic rate
(BMR)
BMR = calories required to sustain life
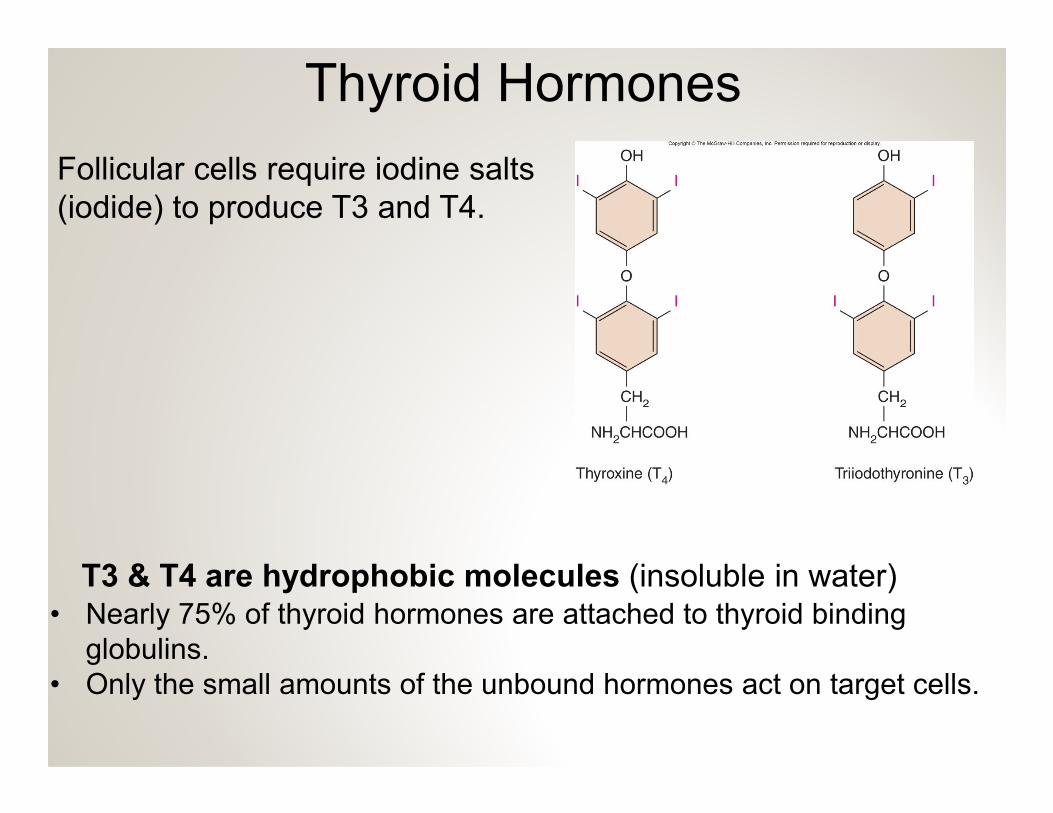
Thyroid Hormones
Follicular cells require iodine salts
(iodide) to produce T3 and T4.
• Nearly 75% of thyroid hormones are attached to thyroid binding
globulins.
• Only the small amounts of the unbound hormones act on target cells.
T3 & T4 are hydrophobic molecules (insoluble in water)
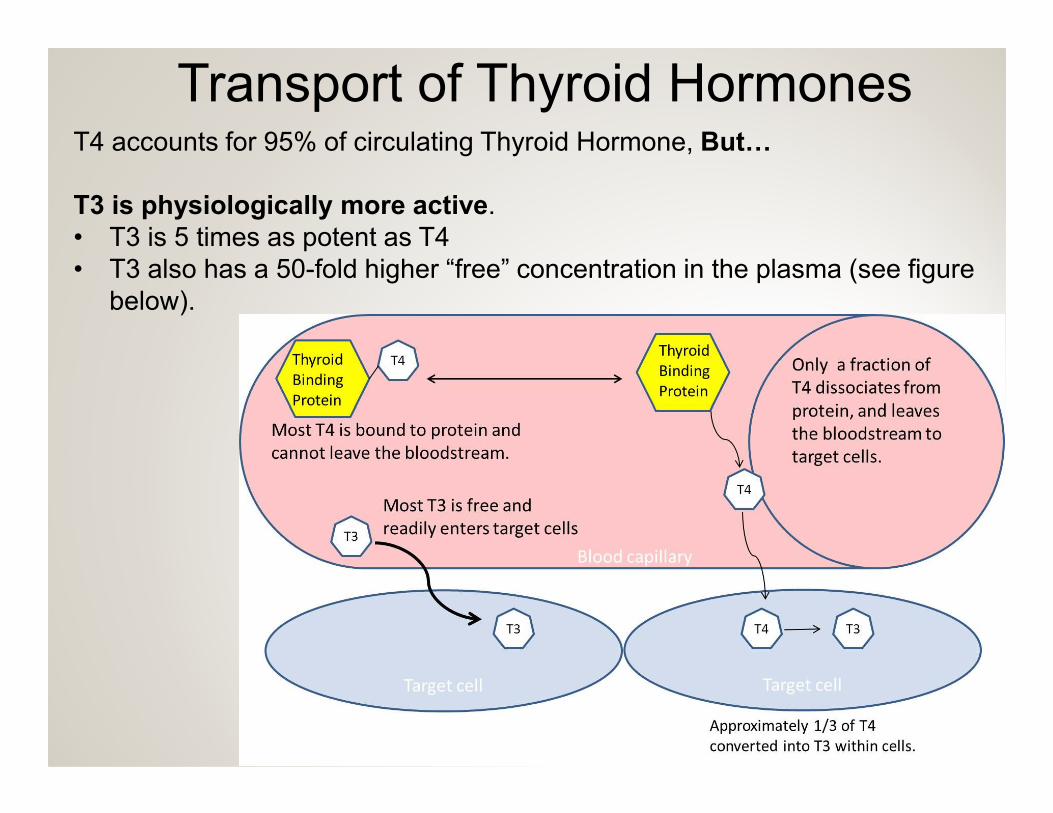
T4 accounts for 95% of circulating Thyroid Hormone, But$
Transport of Thyroid Hormones
T3 is physiologically more active.
• T3 is 5 times as potent as T4
• T3 also has a 50-fold higher “free” concentration in the plasma (see figure
below).
Thyroid Disorders
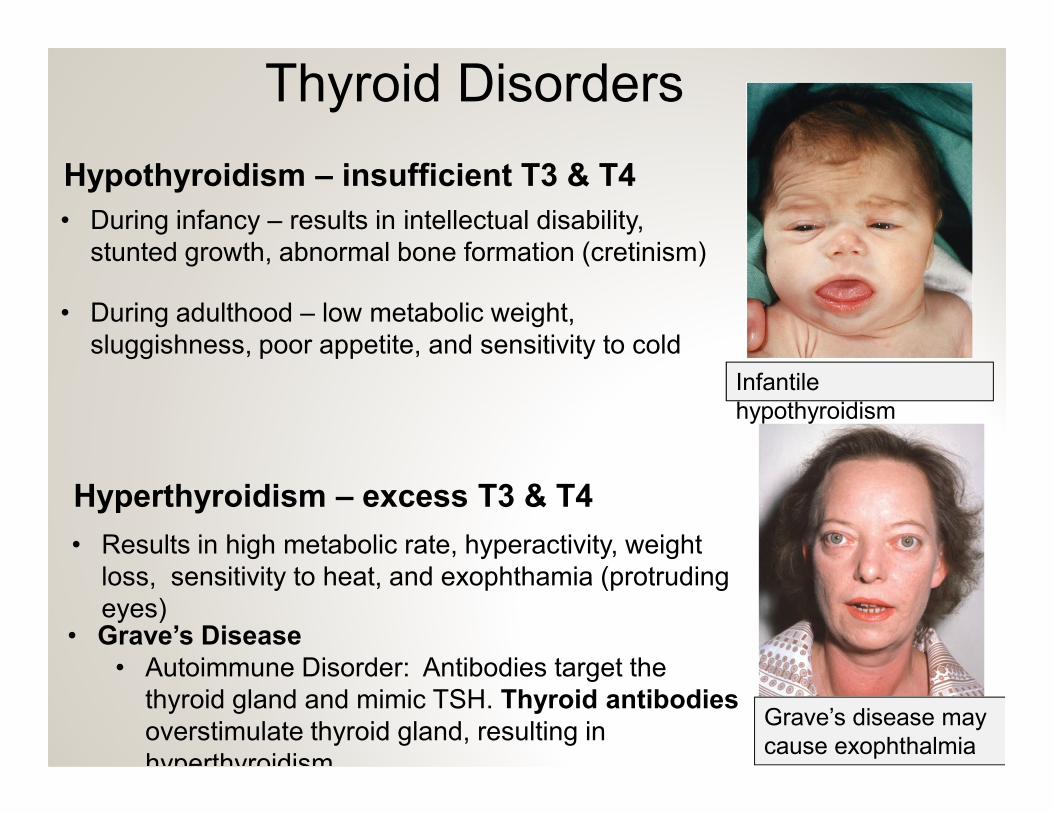
Hypothyroidism – insufficient T3 & T4
• During infancy – results in intellectual disability,
stunted growth, abnormal bone formation (cretinism)
• During adulthood – low metabolic weight,
sluggishness, poor appetite, and sensitivity to cold
Infantile
hypothyroidism
Hyperthyroidism – excess T3 & T4
• Results in high metabolic rate, hyperactivity, weight
loss, sensitivity to heat, and exophthamia (protruding
eyes)• Grave’s Disease
• Autoimmune Disorder: Antibodies target the
thyroid gland and mimic TSH. Thyroid antibodies
overstimulate thyroid gland, resulting in
hyperthyroidism.
Grave’s disease may
cause exophthalmia
hypothyroidism
Calcitonin
Extrafollicular cells (C-cells) secrete Calcitonin
Calcitonin lowers blood calcium concentrations.
• Stimulates Osteoblast activity – increases bone deposition
Actions of Calcitonin
• Stimulates Osteoblast activity – increases bone deposition
Major Source of Control: elevated blood calcium ion concentration
• Inhibits osteoclast activity – reduces bone resorption
• Promotes the excreting of calcium from the
kidneys
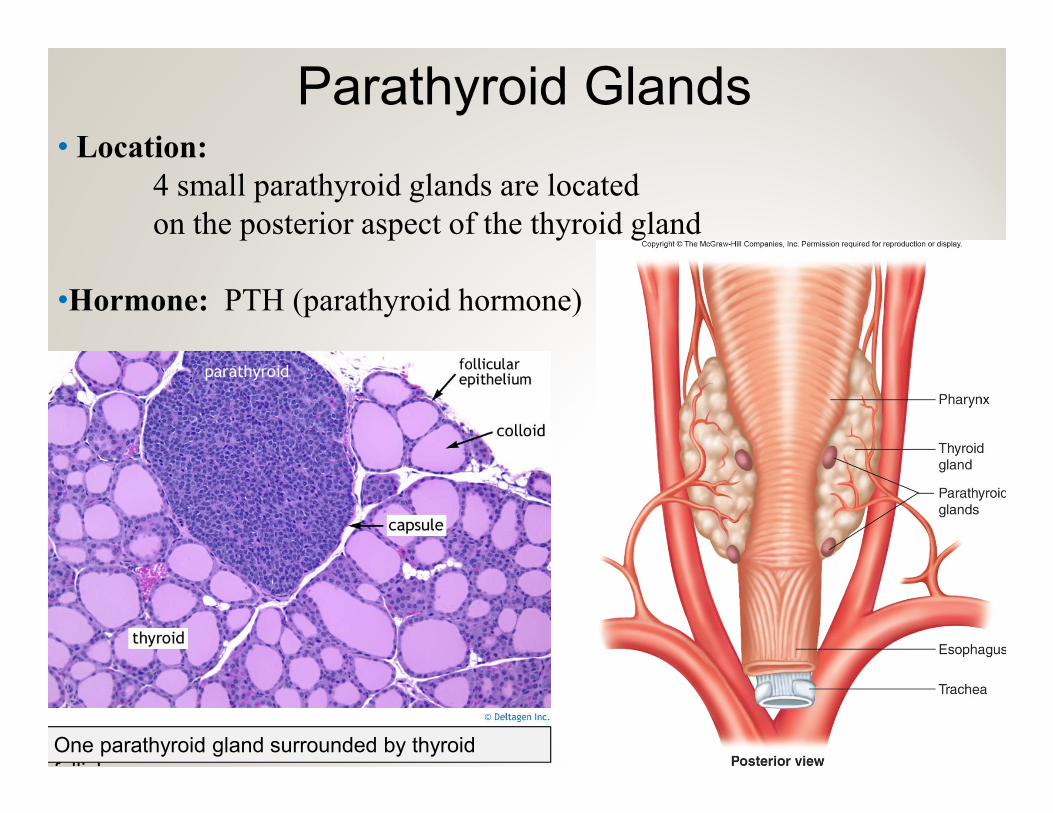
Parathyroid Glands• Location:
4 small parathyroid glands are located
on the posterior aspect of the thyroid gland
•Hormone: PTH (parathyroid hormone)
One parathyroid gland surrounded by thyroid
follicles.
Parathyroid Hormone elevates blood calcium levels.
Parathyroid Hormone (PTH)
• Stimulates Osteoclast activity – increases bone resorption
• Inhibits osteoblast activity – reduces bone
Actions of PTH:
• PTH also promotes the activation of Vitamin D, which
enhances calcium absorption from the small intestine.
• Inhibits osteoblast activity – reduces bone
deposition• Promotes calcium reabsorption from the kidneys.
Major Source of Control: Inadequate blood calcium ion concentration
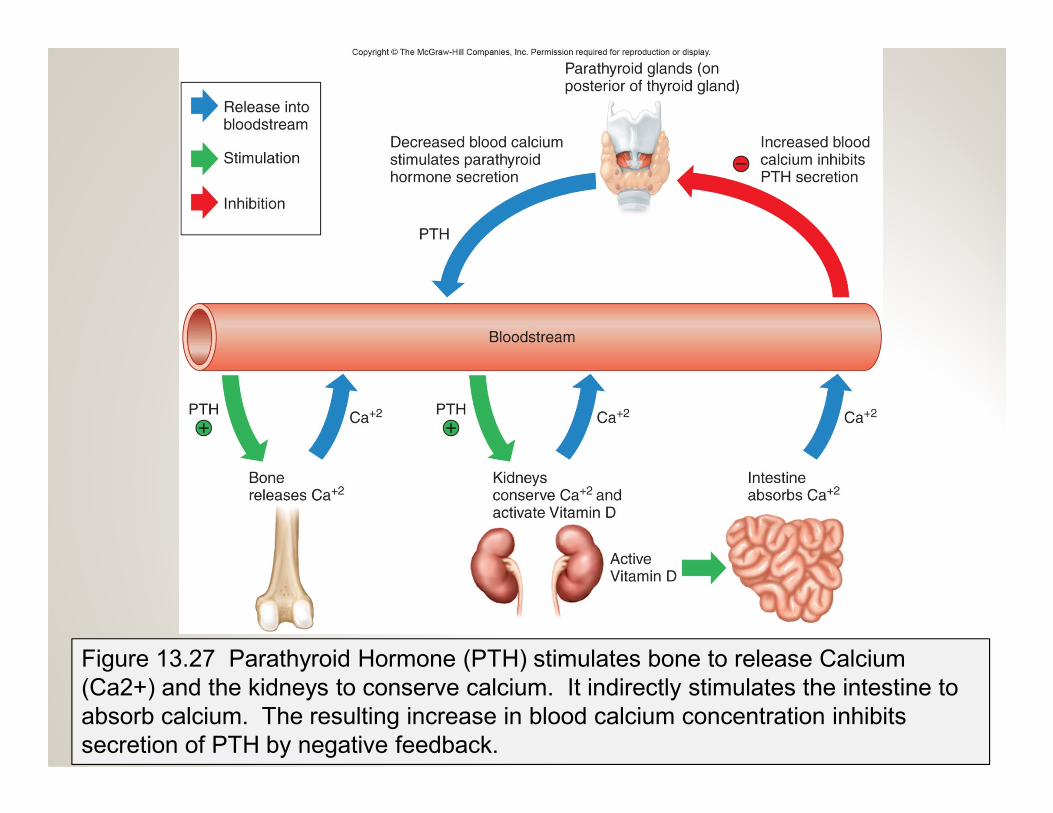
Figure 13.27 Parathyroid Hormone (PTH) stimulates bone to release Calcium
(Ca2+) and the kidneys to conserve calcium. It indirectly stimulates the intestine to
absorb calcium. The resulting increase in blood calcium concentration inhibits
secretion of PTH by negative feedback.
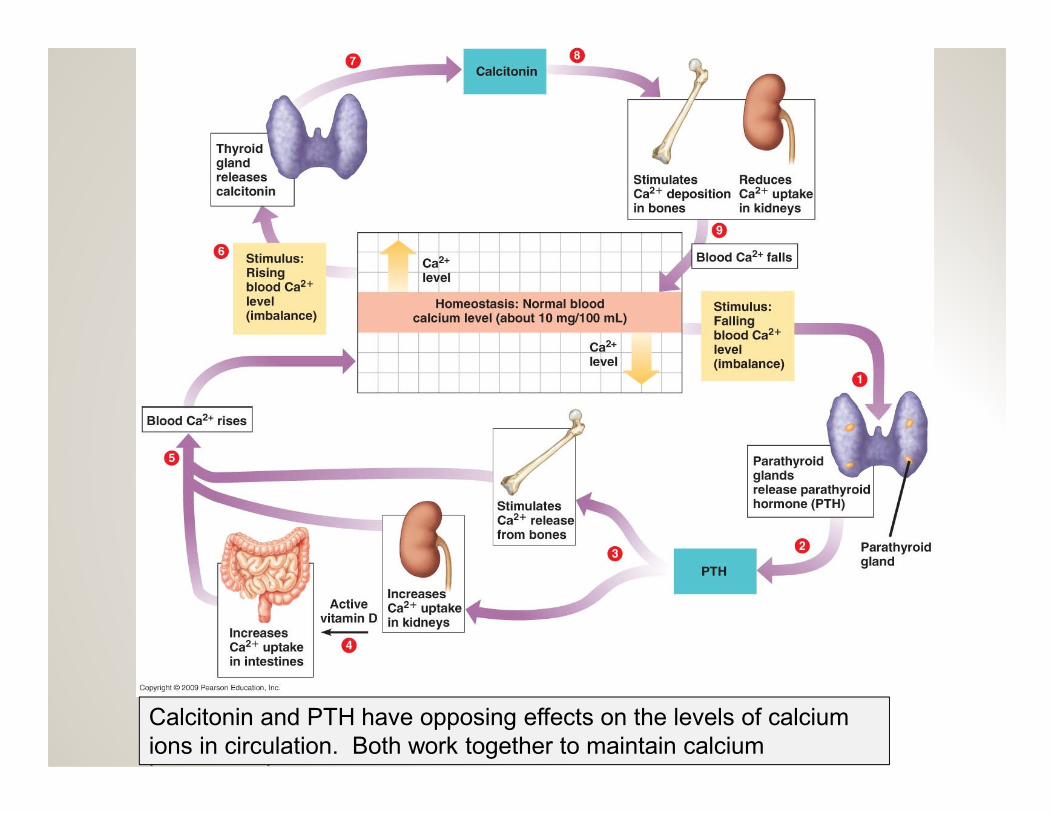
Calcitonin and PTH have opposing effects on the levels of calcium
ions in circulation. Both work together to maintain calcium
homeostasis.
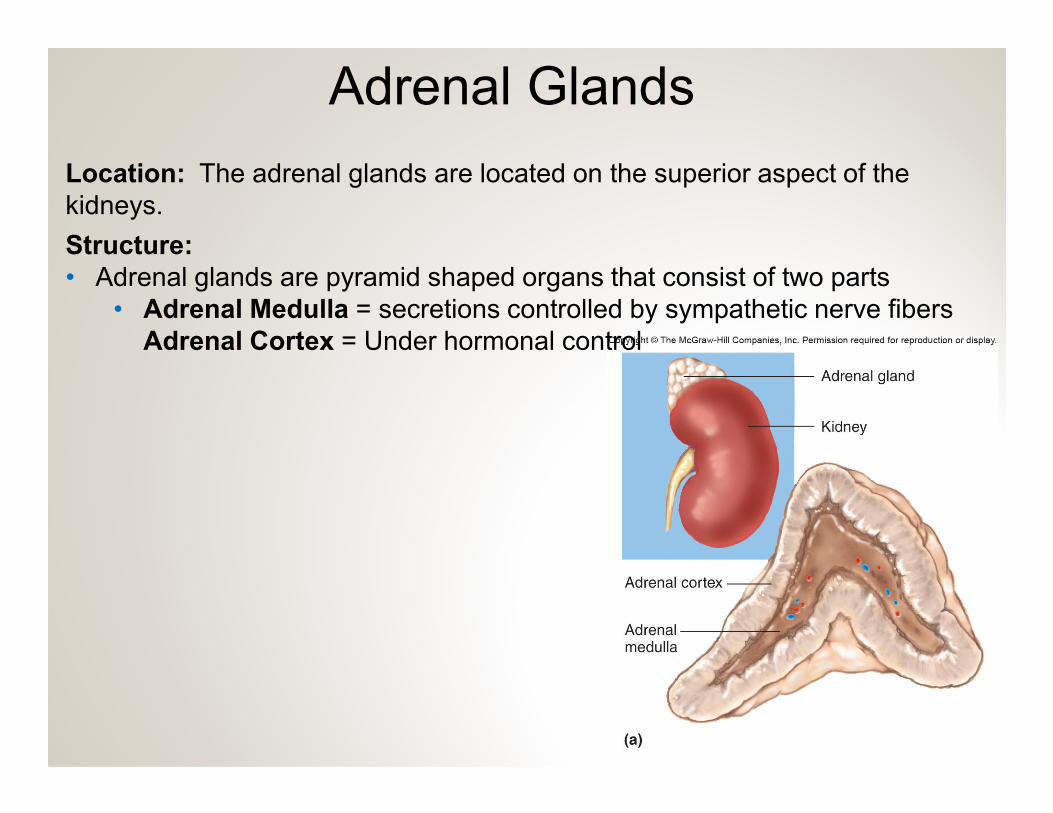
Adrenal Glands
Location: The adrenal glands are located on the superior aspect of the
kidneys.
Structure:
• Adrenal glands are pyramid shaped organs that consist of two parts
• Adrenal Medulla = secretions controlled by sympathetic nerve fibers
Adrenal Cortex = Under hormonal control
Hormones of the Adrenal Medulla
Hormones: Norepinephrine (noradrenalin) & Epinephrine (adrenalin)
• Both are classified as catecholamines.
Nerve fibers control secretions: Hormones of the adrenal medulla are
under control by the sympathetic division (fight or flight) of the ANS.
Actions: Effects are similar to sympathetic nerve fibers, but longer lasting.
• Increases heart rate and force of contraction
• Increases blood pressure
• Increases metabolic rate
• Increases blood glucose levels (primarily epinephrine)
• Decreases digestion
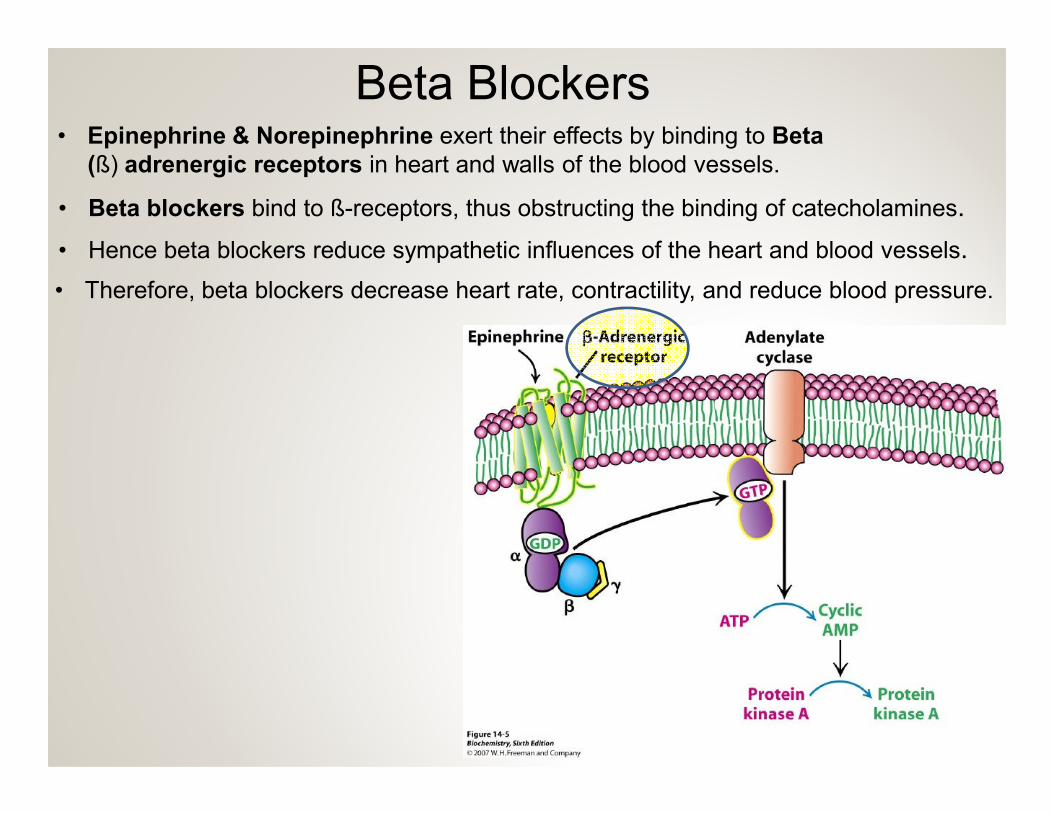
Beta Blockers• Epinephrine & Norepinephrine exert their effects by binding to Beta
(ß) adrenergic receptors in heart and walls of the blood vessels.
• Beta blockers bind to ß-receptors, thus obstructing the binding of catecholamines.
• Hence beta blockers reduce sympathetic influences of the heart and blood vessels.
• Therefore, beta blockers decrease heart rate, contractility, and reduce blood pressure.
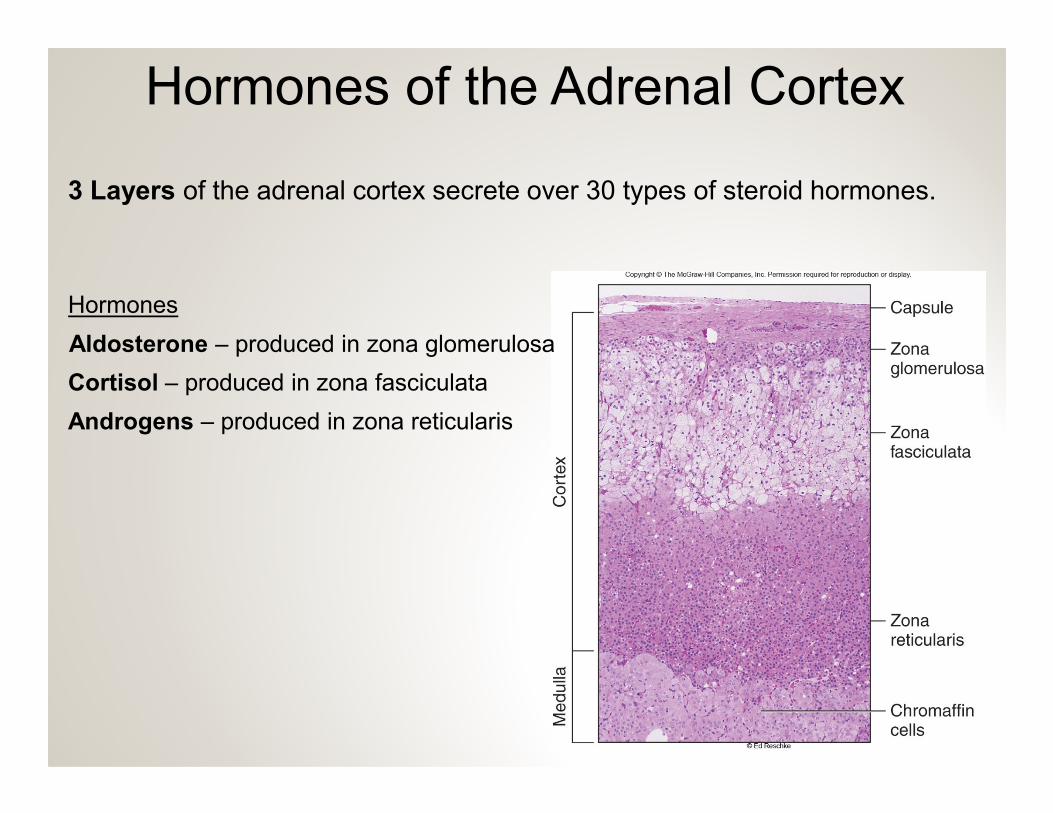
Hormones of the Adrenal Cortex
3 Layers of the adrenal cortex secrete over 30 types of steroid hormones.
Hormones
Aldosterone – produced in zona glomerulosa
Cortisol – produced in zona fasciculata
Androgens – produced in zona reticularis
Hormones of the Adrenal Cortex
1. Aldosterone (mineralocorticoid)
• regulates Na+ and K+ concentrations
• regulates blood pressure
Actions
• Aldosterone causes the kidneys to reabsorb Na+ and to excrete K+
• Aldosterone indirectly raises blood pressure:
Increased Na+ reabsorption increases water reabsorption by osmosis. Increased Na+ reabsorption increases water reabsorption by osmosis.
Controls of Aldosterone Secretion
• Low blood pressure stimulates aldosterone secretion
(renin-angiotensin-aldosterone pathway)
• Elevated blood K+ concentration promotes aldosterone secretion
• Low Na+ has only a slight effect on aldosterone secretion.
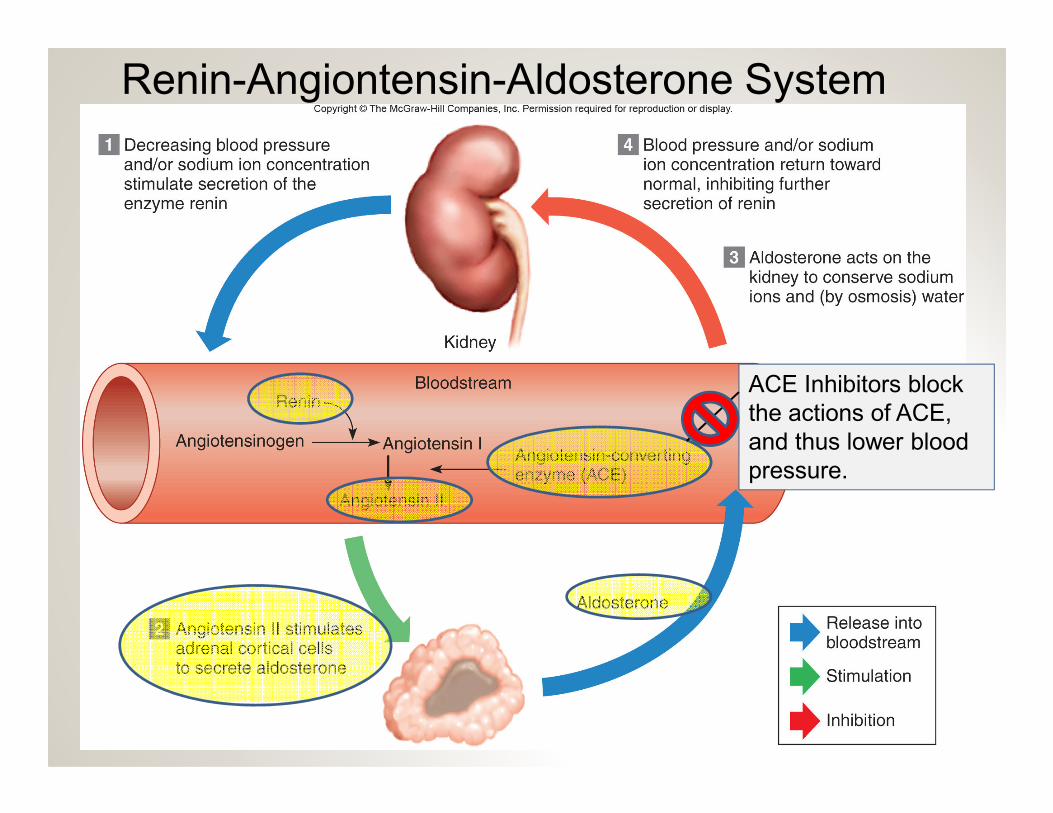
Renin-Angiontensin-Aldosterone System
ACE Inhibitors block
the actions of ACE, the actions of ACE,
and thus lower blood
pressure.
Hormones of the Adrenal Cortex
2. Cortisol (glucocorticoid)
• Its primary effect is to build up and conserve blood glucose supplies
• Its actions keep blood glucose levels constant between meals.
Actions
• Promotes gluconeogenesis in the liver
gluconeogenesis = glucose synthesis from non-carbohydrates
• Inhibits protein synthesis: amino acids used in gluconeogenesis
• Promotes the release and used of fatty acids from adipose for energy.
Using fatty acids for energy allows glucose to be conserved.
Hormones of the Adrenal Cortex
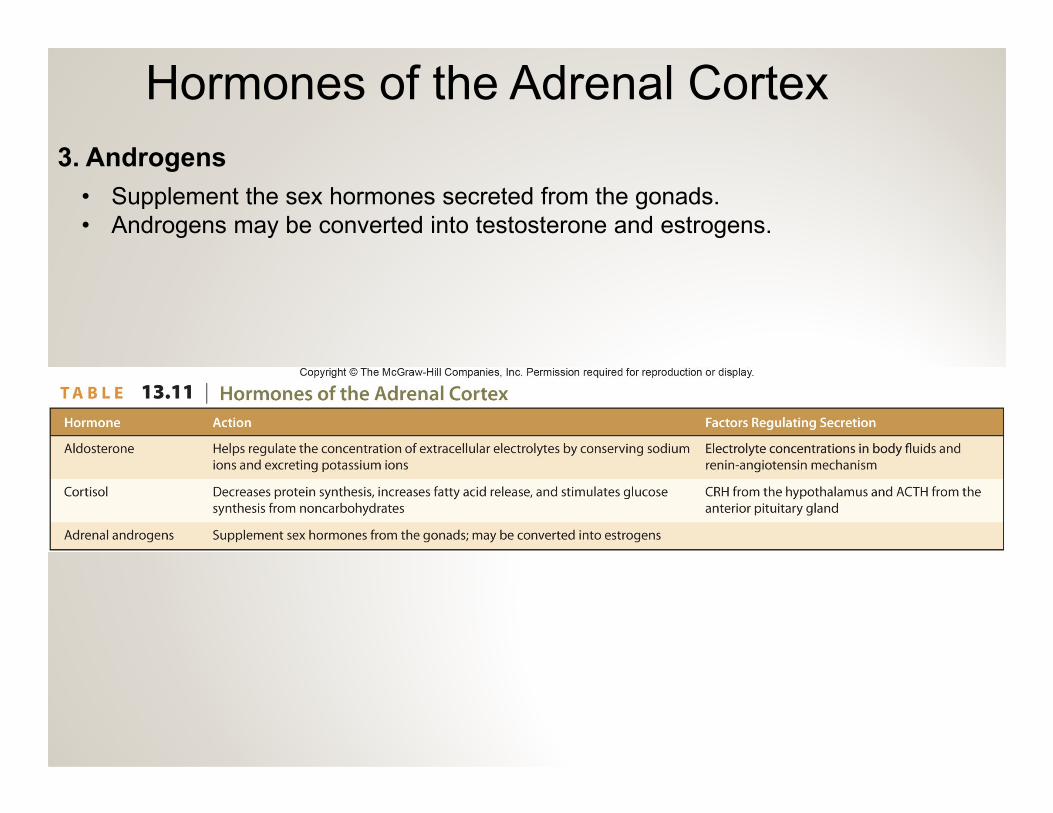
3. Androgens
• Supplement the sex hormones secreted from the gonads.
• Androgens may be converted into testosterone and estrogens.
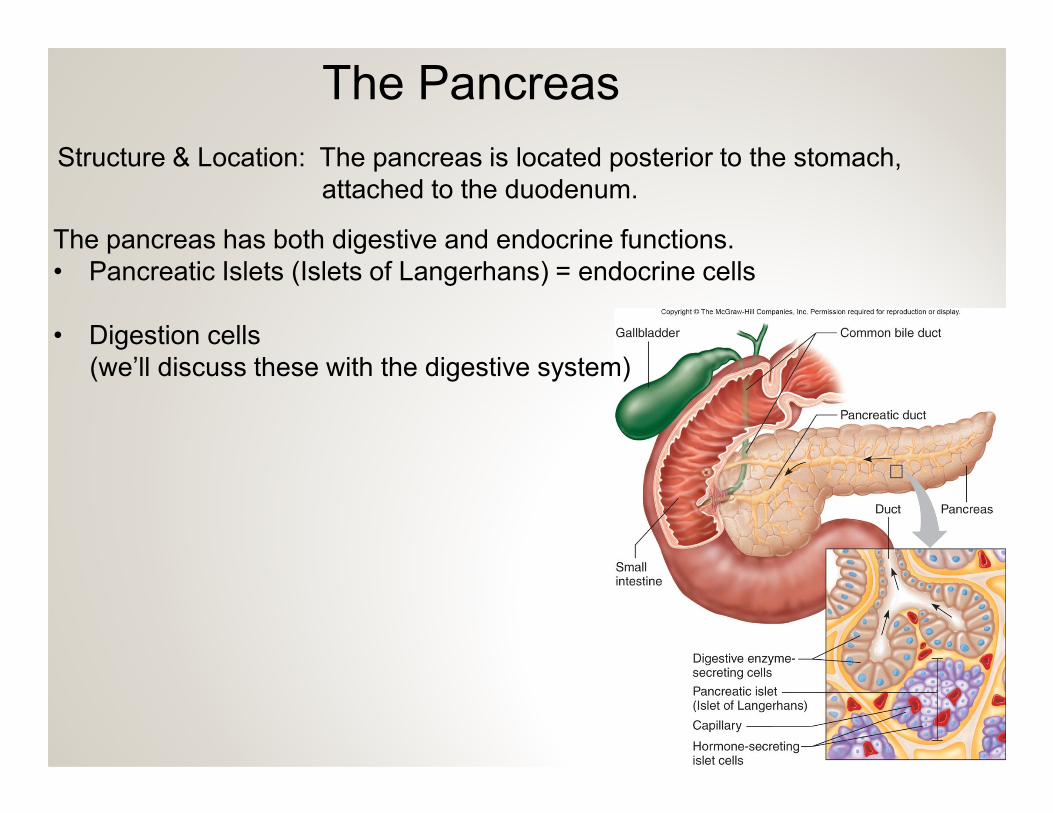
The Pancreas
Structure & Location: The pancreas is located posterior to the stomach,
attached to the duodenum.
The pancreas has both digestive and endocrine functions.
• Pancreatic Islets (Islets of Langerhans) = endocrine cells
• Digestion cells
(we’ll discuss these with the digestive system)
Cells of the Pancreatic Islets
3 distinct type of cells secrete 3 hormones:
• Alpha Cells – secrete glucagon
• Beta Cells – secrete insulin
• Delta Cells – secrete somatostatin
Pancreatic hormones regulate
the storage, use, and release of the storage, use, and release of
fuels (glucose).
Pancreatic Hormones
1. Glucagon
Overall Effect: During fasting, when blood glucose levels drop,
glucagon elevates blood glucose levels
Actions of Glucagon:
• Stimulates glycogenolysis in the liver (breakdown of glycogen into glucose)• Stimulates glycogenolysis in the liver (breakdown of glycogen into glucose)
• Glucagon also promotes gluconeogenesis
• Glucagon also stimulates the breakdown of fats into glycerol and fatty acids.
• Glycerol is used in gluconeogenesis
• Fatty Acids are metabolized for energy
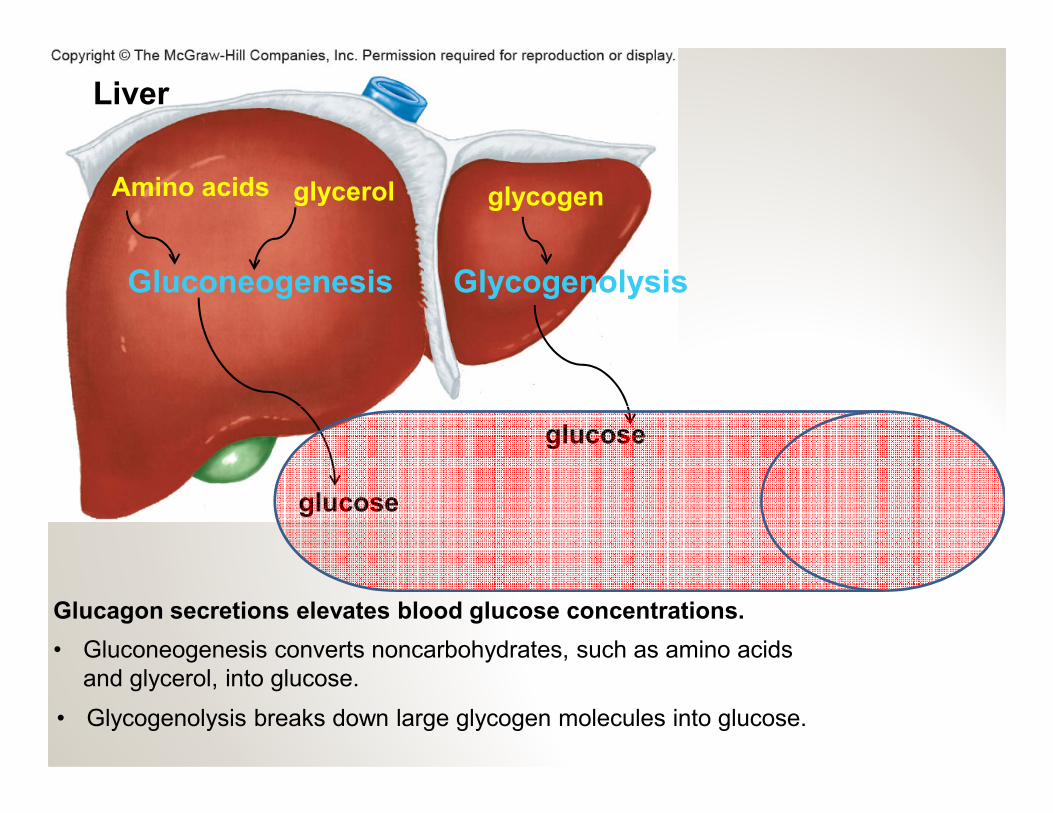
glycogen
Gluconeogenesis
Amino acids glycerol
Glycogenolysis
Liver
glucose
glucose
Glucagon secretions elevates blood glucose concentrations.
• Gluconeogenesis converts noncarbohydrates, such as amino acids
and glycerol, into glucose.
• Glycogenolysis breaks down large glycogen molecules into glucose.
2. Insulin
Pancreatic Hormones
Overall Effect: Following a meal, when blood carbohydrate levels
are high, insulin removes excess glucose from the blood.
Actions of Insulin:
• Stimulates glycogenesis in the liver (formation of glycogen from glucose). • Stimulates glycogenesis in the liver (formation of glycogen from glucose).
• It inhibits gluconeogenesis.
• Insulin promotes glucose uptake in adipose tissue, skeletal muscles, and
cardiac muscle.
3. Somatostatin
Overall Effect: Helps regulate glucose metabolism by inhibiting the
secretion of glucagon and insulin.
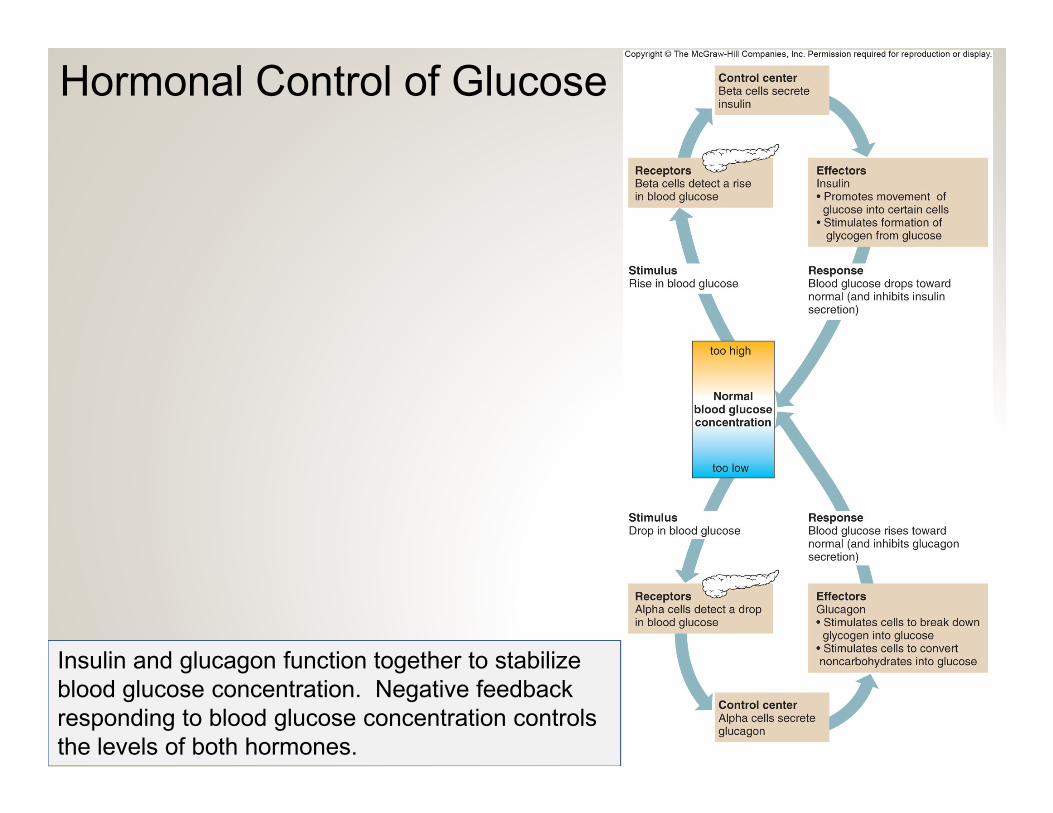
Hormonal Control of Glucose
Insulin and glucagon function together to stabilize
blood glucose concentration. Negative feedback
responding to blood glucose concentration controls
the levels of both hormones.
Diabetes Mellitus
Type I Diabetes Mellitus (juvenile)
• Autoimmune disease – immune system destroys beta cells, resulting in the
loss of insulin production.
• Without insulin, blood glucose cannot be taken up and used for energy.
• Glucose accumulates in the blood and urine = hyperglycemia.
Type II Diabetes Mellitus (adult onset)
• Receptors on target cells wear down and become insensitive to insulin.
• Target cells resist glucose uptake, even in the presence of insulin.
• Insulin levels must be higher than normal just to maintain
normal glucose concentrations.
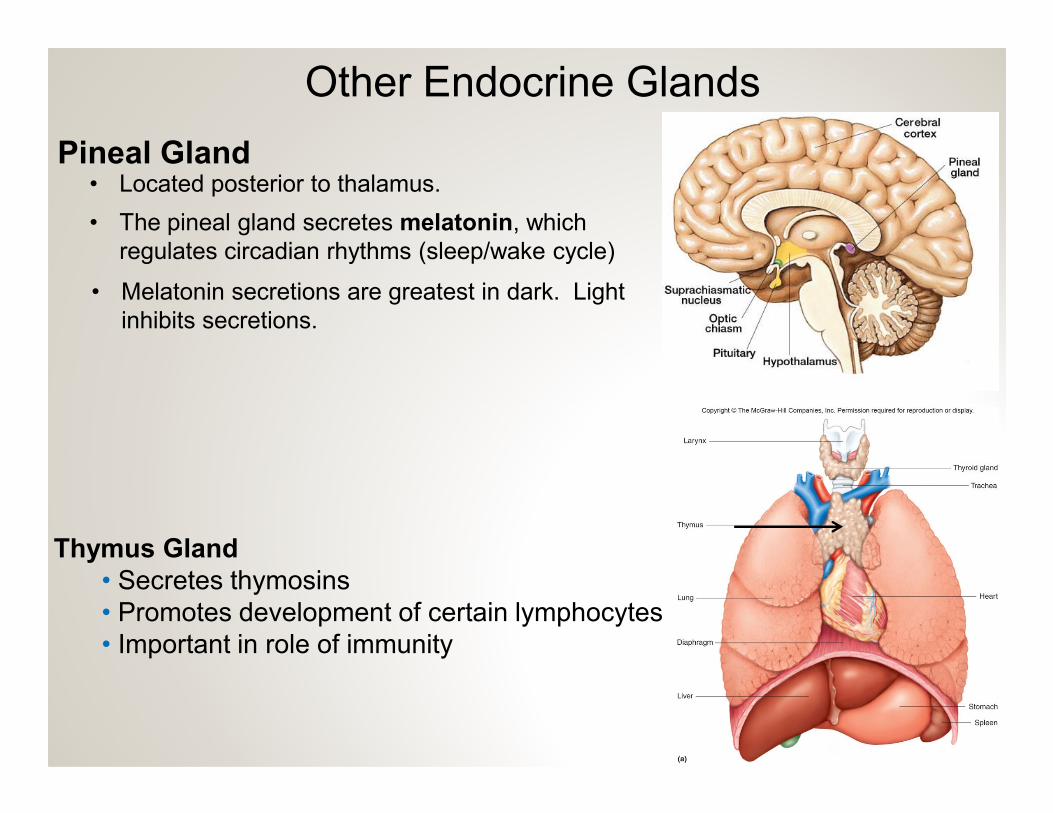
Other Endocrine Glands
Pineal Gland
• The pineal gland secretes melatonin, which
regulates circadian rhythms (sleep/wake cycle)
• Located posterior to thalamus.
• Melatonin secretions are greatest in dark. Light
inhibits secretions.
Thymus Gland
• Secretes thymosins
• Promotes development of certain lymphocytes
• Important in role of immunity
Reproductive Organs
• Ovaries produce estrogens and progesterone
• Testes produce testosterone
• Placenta produces estrogens, progesterone, and gonadotropin
Other organs: digestive glands, heart, and kidney
Other Endocrine Glands
End of Section 3, Chapter 13