Embed Size (px)
Citation preview

Seclusion and Restraints A Failure Not a Treatment
Protecting Mental Health Patients from Abuses
California Senate Office of Research
March 2002
Seclusion and Restraints A Failure Not a Treatment
Protecting Mental Health Patients from Abuses
Prepared by Laurel Mildred
California Senate Office of Research Elisabeth Kersten Director
Edited by Rebecca LaVally
This report can be found online at wwwsencagovsor under ldquoReportsrdquo
March 2002
Contents
Executive Summary 1
Part I Seclusion and Restraints Issues and Actions 5
Part II Federal Reforms and State Impacts 12
Part III Pennsylvania ndash A Model for Reform 20
Part IV Conclusion 24
Endnotes 27
Figures
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities 16
Figure 2 Pennsylvania Reduces Incidents of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96 21
Figure 3 Pennsylvania Seclusion and Restraints Reduction Initiative 23
Appendices 31
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between March 2000 and October 1998
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000
Seclusion and Restraints A Failure Not a Treatment
Executive Summary
Overview
Seclusion and restraint of psychiatric patients are known to be dangerous practices that can result in serious injury trauma and even death1 The Harvard Center for Risk Analysis estimates that 50 to 150 deaths occur nationally each year because of psychiatric seclusion and restraints2 Here in California at least 14 people have died and at least one has become permanently comatose while being subjected to these practices since July of 19993 This does not reflect those who are injured or traumatized ndash California does not keep track of those data
We do know however that at a very conservative estimate over 100000 Californians are involuntarily committed to psychiatric facilities each year4 and that along with voluntary patients they are at risk of being subjected to seclusion and restraints (SR)
Accounts of serious injuries and deaths resulting from SR were reported in the Hartford Courant and other sources during 1998 and gained wide national attention These reports found that patients became comatose suffered broken bones were hit in the face bruised needed stitches or were bleeding as a result of being placed in SR5 In the worst cases patients died of causes that included asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdoses or interactions and choking6
These revelations led Congress to adopt significant federal reforms in 1999 and again in 2000 The Joint Commission on the Accreditation of Healthcare Organizations also adopted new policies that affect about 80 percent of the nationrsquos health care facilities However federal reforms have not by themselves prevented harm to our most vulnerable citizens held in psychiatric
Seclusion and Restraints A Failure Not a Treatment
facilities against their will for what is supposedly their own well-being
Californiarsquos oversight of SR in psychiatric facilities is a regulatory maze that impedes accountability and progress In addition statewide standards on SR are piecemeal depending upon the type of facility and we lack a comprehensive and mandatory statewide reporting system Consequently the only meaningful measure of seclusion and restraints in California is when people die
The California Office of Patient Rights is vested with responsibility for collecting and reporting information about use of SR However it must rely on data supplied by counties and facilities In 2000 the Office of Patient Rights documented a high rate of noncompliance with reporting requirements 56 facilities or 22 percent submitted either an incomplete report or no report at all7
Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement8
The Office of Patient Rights cites these limitations in Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements9
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements10
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements11
For these reasons the Office of Patient Rights has concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo12 In addition the California Department of Health Services reports that it does not consider data on seclusion and restraints from the Office of Patient Rights when deciding whether to conduct inspections on facilities
- 2 -
Seclusion and Restraints A Failure Not a Treatment
Other states have imposed new restrictions in their SR policies Most notably Pennsylvania has developed an award-winning model that reduced overall incidents of seclusion and restraint by 74 percent and reduced the hours that patients spent in SR by 96 percent over a three-year period13
The Pennsylvania reforms were accomplished with no additional staff or funds and no increase in injuries to staff14 Charles Curie then deputy secretary of Pennsylvaniarsquos mental health and substance abuse services15 articulated a new philosophy of care that became the basis for a comprehensive change of culture in Pennsylvaniarsquos state hospital system ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo16
Pennsylvaniarsquos first step was to institute a mandated and publicly accountable system of tracking seclusion and restraints The state developed system-wide policies that required training diffusion of conflict accountability for using SR awards and recognition for reducing its use cultural competence a prohibition on all chemical restraints a prohibition on using SR on voluntary patients and debriefings with patients families and staff after each incident Central to these reforms was the core concept that seclusion and restraints are not treatment ndash they reflect a treatment failure and should be handled as such to prevent the escalation of violence This commitment has radically changed the longstanding culture environment and level of violence in Pennsylvaniarsquos nine state hospitals
This analysis determines that Californiarsquos piecemeal regulatory system could benefit from practices similar to those developed in Pennsylvania
Findings and Options
The new federal reforms that govern SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to accountability in the use of SR in California facilities
diams A lack of uniform statewide standards across various types of facilities and
diams A lack of mandatory consistent and publicly accessible reporting on the use and consequences of SR These include deaths serious injuries frequency and duration of SR and
- 3 -
Seclusion and Restraints A Failure Not a Treatment
related conditions and situations such as airway obstructions patient falls staff injuries and medication errors
Private psychiatric hospitals may be the most difficult to regulate The US inspector general found in August 2000 that private facilities may be the least likely to comply with the 1999 federal SR regulations and therefore may be the most in need of uniform state standards and enforcement17
There is compelling evidence in the Pennsylvania experience that SR can be dramatically reduced with a change of organizational values and culture
The following steps could be taken with a goal of reducing SR practices and the injuries deaths and traumas that can result from them
diams California could develop uniform seclusion and restraint standards that match if not exceed the highest federal regulations to cover all facilities ndash private as well as public ndash that treat people with psychiatric disabilities Federal standards vary based on licensing and accreditation while state standards vary based on type of facility The experience of other states has shown that a high uniform state standard improves the quality of enforcement and compliance
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to safely and cost-effectively reduce the use of SR in California
- 4 -
Seclusion and Restraints A Failure Not a Treatment
Part I
Seclusion and Restraints Issues and Actions
The issue of seclusion and restraint of psychiatric and substance-abuse patients gained national notoriety in October of 1998 when the Hartford Courant published a five-part investigative series entitled ldquoDeadly Restraintrdquo The Courant conducted a national survey that documented 142 deaths in the past decade that were directly connected to the use of seclusion or physical restraints (Appendix 1)
Seclusion refers to isolating a person in a locked room Restraints are human or mechanical measures that use force or the threat of force to control someonersquos actions ldquoTake downsrdquolowast holding someone face-down in a prone position strait jackets or tying someone by hands and feet are all examples of restraints Chemical restraints are medications that are not otherwise necessary and that are used to control someonersquos behavior
The Harvard Center for Risk Analysis has estimated that deaths and injuries from seclusion and restraints are significantly under-reported Its study of the prevalence of seclusion and restraint-related deaths statistically estimated that between 50 and 150 deaths occur nationally each year because of SR use on psychiatric and substance-abuse patients18
A national impetus for reform was triggered by incidents reported by the Courant and other sources
lowast A ldquotake downrdquo is a technique to force an uncooperative person to the floor to place him or her in restraints At least five staff surround the patient each taking the head an arm or leg and force him or her down Injury to the patient often occurs if staff sit on the person while restraints are secured This technique is frequently violent causing significant patient and staff injuries
- 5 -
Seclusion and Restraints A Failure Not a Treatment
diams Gloria Huntley 31 years old died in Central State Hospital in Petersburg Virginia after having been kept in restraints for 558 hours during the last two months of her life Although she had been diagnosed with asthma and epilepsy she was nevertheless restrained over and over again because of angry outbursts at hospital staff (Hartford Courant 1998)
diams Sixteen-year-old Tristan Sovern died in Charter Greensboro in North Carolina in 1998 after he was placed in restraints as ldquopunishmentrdquo for leaving a group-therapy session In response to his screams of ldquoYoursquore choking me I canrsquot breatherdquo a towel was shoved over Tristanrsquos mouth (60 Minutes II 1999)
diams Here in California Kristal Mayon-Ceniceros age 16 died of respiratory arrest in New Alternatives a private Chula Visa residential-care facility She died after being restrained face-down on the floor by four staff members (Associated Press 1999)
diams Also in California Rick Griffin 36 of Stockton died of cardio-respiratory failure and extreme agitation in the San Joaquin County Psychiatric Health Facility He had been wrestled to the floor by eight staff members and bound in leather restraints (The Stockton Record 1998)
diams Andrew McClain was 11 years old and weighed 96 pounds when two aides at the Elmcrest psychiatric hospital in Portland Connecticut sat on his back and crushed him to death His offense Refusing to move to another breakfast table (Lieberman Dodd and De Lauro 1999)
diams Edith Campos 15 suffocated while being held face-down after resisting an aide at the Desert Hills Center for Youth and Families in Tucson Arizona She was subjected to restraints after refusing to hand over an ldquounauthorizedrdquo personal item The item was a family photograph (Lieberman Dodd and De Lauro 1999)
Initial Response
The Courant series sparked congressional hearings into SR policies and how people have been traumatized injured and killed as a result of these practices Congressional leaders responded with federal reform proposals In a series of high-profile hearings
- 6 -
Seclusion and Restraints A Failure Not a Treatment
deaths injuries and abuses resulting from seclusion and restraints were exposed
Unfortunately these are not isolated incidents They are but a few of scores of cases in which mental health patients ndash a disproportionate number of them children ndash died barbaric deaths more suited to medieval torture chambers than to late 20th century America They died because of the improper use of seclusion and physical or chemical restraints They died at the hands of the very people who were supposed to protect them
- Senator Lieberman Senator Dodd and Representative DeLauro July 16 1999
The National Alliance for the Mentally Ill (NAMI) also has tracked reports of recent and past SR abuses (Appendix 2) NAMI reported over 25 new incidents nationwide of deaths injuries and traumas caused by seclusion and restraints after the Courant survey Currently there is no official tracking of injury or trauma to patients or to staff in California NAMI however reported numerous incidents of serious injury ndash patients who became comatose who suffered broken bones were hit in the face bruised needed stitches or were bleeding as a result of restraints19
Equally troubling is the humiliation and trauma NAMI documents such as its many reports of patients unable to use the bathroom and left for hours in their own bodily wastes One patient was restrained for rejecting medication because she still hoped to nurse her young child another was placed in restraints because he couldnrsquot stop crying A 12-year-old was placed in a straightjacket in the middle of the floor where everyone could watch her ndash and staff called this a ldquoburritordquo A patient who voluntarily admitted herself to a hospital found herself reliving former traumatic experiences
Suddenly the guard had a huge pair of leather cuffs with padlocks on them All I knew was that I was being strapped down to a bed by a strange man with a gun This is not good therapy for a rape victim All I could do was close my eyes and pretend this wasnrsquot happening to me20
The US General Accounting Office (GAO) in an October 1999 report on improper seclusion and restraints validated the notion that patients may be severely traumatized while being restrained
- 7 -
Seclusion and Restraints A Failure Not a Treatment
even if no physical injuries are sustained ldquo Research indicates that at least half of all women treated in psychiatric settings have a history of physical or sexual abuserdquo21
Citing a Massachusetts state task force on the topic the GAO stated that the use of restraints on patients who have been abused often results in their re-experiencing their traumas and contributes to a setback in the course of treatment
Congress adopted reforms to federal policies administered by the US Centers for Medicare and Medicaid Services (CMS formerly HCFA) in 1999 In addition the Joint Commission on Accreditation of Healthcare Organizations has adopted new policies The recently enacted Childrenrsquos Healthcare Act of 2000 was the third major federal reform Explained more fully in Part II of this report these new policies are intended to restrict and reduce SR practices
Despite these reforms the federally mandated advocate organization Protection and Advocacy reports that 14 Californians have died and one has beenen permanently injured (in a persistent coma) while in seclusion or behavioral restraints since the new CMS rules were put into place in July 1999 Since there is no official requirement for reporting nonfatal injuries we cannot officially confirm the types of injuries documented by NAMI the news media and the GAO
Californiarsquos standards governing SR practice are different for each kind of facility State hospitals general acute care hospitals psychiatric health facilities skilled nursing facilities ndash all are facilities that utilize SR However each type of facility is governed by a different set of state regulations For example
General Acute Care Hospitals ndash In a case of emergency SR can be initiated at the discretion of a registered nurse and a verbal or written order obtained from a physician afterwards If a verbal order is obtained it shall be signed by the physician on his next visit Orders for SR may be for longer than 24 hours
Psychiatric Health Facilities ndash In an emergency a physicianrsquos order can be received over the telephone within one hour of initiating SR and must be signed in person within 24 hours Orders for SR may be in force for no longer than 24 hours
Skilled Nursing Facilities with Special Treatment Programs ndash A physician may give the order for SR by telephone and sign it in
- 8 -
Seclusion and Restraints A Failure Not a Treatment
person within five days The order expires and must be renewed each 24 hours to keep a person in SR
Each facilityrsquos standards differ from the others and on this particular issue none is as stringent as the federal standard Californiarsquos regulatory standards and some of the problems associated with them are discussed more fully under ldquoPatchwork Oversightrdquo on page 15
Scope of Report
This report focuses on issues of psychiatric seclusion and restraints It does not address issues of medical restraints such as immobilizing a person for a surgical procedure or placing a personrsquos arm in a ldquosleeverdquo to prevent removing an intravenous needle Nor does it address the important issues of SR policies in schools or facilities for the developmentally disabled or in correctional facilities for youths or adults It is limited in scope to policies of psychiatric seclusion and restraints in mental health facilities
The Pennsylvania Experience
Seclusion and restraints have been used to control the behavior of psychiatric patients since the Middle Ages22 However these techniques have also involved high risk of patient injury and death Pennsylvania has been a leader in trying to change this culture and working to reduce and ultimately eliminate the use of seclusion and restraints in its nine state hospitals
The Pennsylvania Office of Mental Health and Substance Abuse Services implemented its program because
hellipthese measures [SR] do not alleviate human suffering or psychiatric symptoms do not alter behavior and have frequently resulted in patient and staff injury emotional trauma and patient death23
Expert testimony at hearings of the Joint Commission on Accreditation of Healthcare Organizations also called attention to the counter-therapeutic aspects of SR
The attempt to impose ldquotreatmentrdquo by force is always counterproductive ndash creating humiliation resentment and resistance to further treatment that might be more helpful24
- 9 -
Seclusion and Restraints A Failure Not a Treatment
In practice seclusion and restraints are sometimes imposed on psychiatric patients for reasons that are not therapeutic These uses of SR have been discredited and are illegal under current law however they persist SR practices are sometimes used to
diams Control the environment ndash To curtail a patientrsquos movement to compensate for having inadequate staff on the ward or to avoid providing appropriate clinical interventions
diams Coerce ndash To force a patient to comply with the staffrsquos wishes or
diams Punish ndash To impose penalties on patient behaviors
NAMI has been a leader in the effort to end SR on these terms Its position is that restraints and seclusion have no therapeutic value and therefore they are not a ldquotreatmentrdquo NAMI asserts that SR are dangerous interventions and should be used only in cases of extreme emergency when someonersquos physical safety is in jeopardy and then only with careful safeguards25
The idea that psychiatric patients are treated with brutality are seriously injured or even killed in this day and age may be difficult to believe But the Courant investigation the Harvard Center for Risk Analysis and NAMIrsquos report all demonstrate that these practices continue to exist placing psychiatric patients at risk of trauma injury and even death In the most egregious cases where someone has died the causes of death are frequently violent asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdose drug interactions and choking26
These are our most vulnerable citizens Since they are often held against their will supposedly for their own well being it would be incumbent upon the state to protect them from being injured traumatized and abused
To address that responsibility this paper examines three critical issues
1) Seclusion and restraints policies have received national attention and have been the focus of three successive initiatives of federal reform Is that enough
2) Californiarsquos oversight of seclusion and restraints is a patchwork quilt of confusing bureaucracy that impedes accountability and progress Can it be improved
- 10 -
Seclusion and Restraints A Failure Not a Treatment
3) Other states have taken action to improve seclusion and restraints policies on the state level Most notably Pennsylvania has developed a model that garnered the Harvard Innovations in American Government Award and reduced hours of seclusion and restraints by 96 percent in its state hospitals Can California benefit from model practices developed in Pennsylvania
- 11 -
Seclusion and Restraints A Failure Not a Treatment
Part II
Federal Reforms and State Impacts
New Federal Regulations Three Layers of Reform
In response to the Hartford Courant series and the vigorous lobbying of NAMI federal actions to revise national policy on seclusion and restraints were proposed and implemented Reform came in three successive initiatives
diams First the US Centers for Medicare and Medicaid Services (CMS) issued new interim rules for Medicare and Medicaid hospitals in July of 1999
diams Next the Joint Commission on Accreditation of Healthcare Organizations released revised seclusion and restraints standards that took effect January 1 2001
diams Most recently on May 22 last year CMS issued Interim Final Rules under the Childrenrsquos Health Act of 2000 setting forth new regulations for psychiatric facilities that receive federal funds and for ldquononmedical community-based facilities for children and youthrdquo
First Reform CMS Breaks New Ground
CMS set forth interim final rules as of July 1999 that revised seclusion and restraints standards in any hospital that receives Medicare or Medicaid financing
The preamble to the rules broke new ground by declaring ldquoThe patientrsquos right to be free from restraints is paramountrdquo27 The rules stated that SR may only be used in emergency situations if needed to ensure the patientrsquos physical safety and when less-restrictive alternatives have been determined ineffective and that
- 12 -
Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
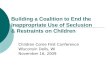
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
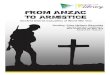
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
Protecting Mental Health Patients from Abuses
Prepared by Laurel Mildred
California Senate Office of Research Elisabeth Kersten Director
Edited by Rebecca LaVally
This report can be found online at wwwsencagovsor under ldquoReportsrdquo
March 2002
Contents
Executive Summary 1
Part I Seclusion and Restraints Issues and Actions 5
Part II Federal Reforms and State Impacts 12
Part III Pennsylvania ndash A Model for Reform 20
Part IV Conclusion 24
Endnotes 27
Figures
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities 16
Figure 2 Pennsylvania Reduces Incidents of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96 21
Figure 3 Pennsylvania Seclusion and Restraints Reduction Initiative 23
Appendices 31
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between March 2000 and October 1998
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000
Seclusion and Restraints A Failure Not a Treatment
Executive Summary
Overview
Seclusion and restraint of psychiatric patients are known to be dangerous practices that can result in serious injury trauma and even death1 The Harvard Center for Risk Analysis estimates that 50 to 150 deaths occur nationally each year because of psychiatric seclusion and restraints2 Here in California at least 14 people have died and at least one has become permanently comatose while being subjected to these practices since July of 19993 This does not reflect those who are injured or traumatized ndash California does not keep track of those data
We do know however that at a very conservative estimate over 100000 Californians are involuntarily committed to psychiatric facilities each year4 and that along with voluntary patients they are at risk of being subjected to seclusion and restraints (SR)
Accounts of serious injuries and deaths resulting from SR were reported in the Hartford Courant and other sources during 1998 and gained wide national attention These reports found that patients became comatose suffered broken bones were hit in the face bruised needed stitches or were bleeding as a result of being placed in SR5 In the worst cases patients died of causes that included asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdoses or interactions and choking6
These revelations led Congress to adopt significant federal reforms in 1999 and again in 2000 The Joint Commission on the Accreditation of Healthcare Organizations also adopted new policies that affect about 80 percent of the nationrsquos health care facilities However federal reforms have not by themselves prevented harm to our most vulnerable citizens held in psychiatric
Seclusion and Restraints A Failure Not a Treatment
facilities against their will for what is supposedly their own well-being
Californiarsquos oversight of SR in psychiatric facilities is a regulatory maze that impedes accountability and progress In addition statewide standards on SR are piecemeal depending upon the type of facility and we lack a comprehensive and mandatory statewide reporting system Consequently the only meaningful measure of seclusion and restraints in California is when people die
The California Office of Patient Rights is vested with responsibility for collecting and reporting information about use of SR However it must rely on data supplied by counties and facilities In 2000 the Office of Patient Rights documented a high rate of noncompliance with reporting requirements 56 facilities or 22 percent submitted either an incomplete report or no report at all7
Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement8
The Office of Patient Rights cites these limitations in Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements9
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements10
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements11
For these reasons the Office of Patient Rights has concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo12 In addition the California Department of Health Services reports that it does not consider data on seclusion and restraints from the Office of Patient Rights when deciding whether to conduct inspections on facilities
- 2 -
Seclusion and Restraints A Failure Not a Treatment
Other states have imposed new restrictions in their SR policies Most notably Pennsylvania has developed an award-winning model that reduced overall incidents of seclusion and restraint by 74 percent and reduced the hours that patients spent in SR by 96 percent over a three-year period13
The Pennsylvania reforms were accomplished with no additional staff or funds and no increase in injuries to staff14 Charles Curie then deputy secretary of Pennsylvaniarsquos mental health and substance abuse services15 articulated a new philosophy of care that became the basis for a comprehensive change of culture in Pennsylvaniarsquos state hospital system ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo16
Pennsylvaniarsquos first step was to institute a mandated and publicly accountable system of tracking seclusion and restraints The state developed system-wide policies that required training diffusion of conflict accountability for using SR awards and recognition for reducing its use cultural competence a prohibition on all chemical restraints a prohibition on using SR on voluntary patients and debriefings with patients families and staff after each incident Central to these reforms was the core concept that seclusion and restraints are not treatment ndash they reflect a treatment failure and should be handled as such to prevent the escalation of violence This commitment has radically changed the longstanding culture environment and level of violence in Pennsylvaniarsquos nine state hospitals
This analysis determines that Californiarsquos piecemeal regulatory system could benefit from practices similar to those developed in Pennsylvania
Findings and Options
The new federal reforms that govern SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to accountability in the use of SR in California facilities
diams A lack of uniform statewide standards across various types of facilities and
diams A lack of mandatory consistent and publicly accessible reporting on the use and consequences of SR These include deaths serious injuries frequency and duration of SR and
- 3 -
Seclusion and Restraints A Failure Not a Treatment
related conditions and situations such as airway obstructions patient falls staff injuries and medication errors
Private psychiatric hospitals may be the most difficult to regulate The US inspector general found in August 2000 that private facilities may be the least likely to comply with the 1999 federal SR regulations and therefore may be the most in need of uniform state standards and enforcement17
There is compelling evidence in the Pennsylvania experience that SR can be dramatically reduced with a change of organizational values and culture
The following steps could be taken with a goal of reducing SR practices and the injuries deaths and traumas that can result from them
diams California could develop uniform seclusion and restraint standards that match if not exceed the highest federal regulations to cover all facilities ndash private as well as public ndash that treat people with psychiatric disabilities Federal standards vary based on licensing and accreditation while state standards vary based on type of facility The experience of other states has shown that a high uniform state standard improves the quality of enforcement and compliance
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to safely and cost-effectively reduce the use of SR in California
- 4 -
Seclusion and Restraints A Failure Not a Treatment
Part I
Seclusion and Restraints Issues and Actions
The issue of seclusion and restraint of psychiatric and substance-abuse patients gained national notoriety in October of 1998 when the Hartford Courant published a five-part investigative series entitled ldquoDeadly Restraintrdquo The Courant conducted a national survey that documented 142 deaths in the past decade that were directly connected to the use of seclusion or physical restraints (Appendix 1)
Seclusion refers to isolating a person in a locked room Restraints are human or mechanical measures that use force or the threat of force to control someonersquos actions ldquoTake downsrdquolowast holding someone face-down in a prone position strait jackets or tying someone by hands and feet are all examples of restraints Chemical restraints are medications that are not otherwise necessary and that are used to control someonersquos behavior
The Harvard Center for Risk Analysis has estimated that deaths and injuries from seclusion and restraints are significantly under-reported Its study of the prevalence of seclusion and restraint-related deaths statistically estimated that between 50 and 150 deaths occur nationally each year because of SR use on psychiatric and substance-abuse patients18
A national impetus for reform was triggered by incidents reported by the Courant and other sources
lowast A ldquotake downrdquo is a technique to force an uncooperative person to the floor to place him or her in restraints At least five staff surround the patient each taking the head an arm or leg and force him or her down Injury to the patient often occurs if staff sit on the person while restraints are secured This technique is frequently violent causing significant patient and staff injuries
- 5 -
Seclusion and Restraints A Failure Not a Treatment
diams Gloria Huntley 31 years old died in Central State Hospital in Petersburg Virginia after having been kept in restraints for 558 hours during the last two months of her life Although she had been diagnosed with asthma and epilepsy she was nevertheless restrained over and over again because of angry outbursts at hospital staff (Hartford Courant 1998)
diams Sixteen-year-old Tristan Sovern died in Charter Greensboro in North Carolina in 1998 after he was placed in restraints as ldquopunishmentrdquo for leaving a group-therapy session In response to his screams of ldquoYoursquore choking me I canrsquot breatherdquo a towel was shoved over Tristanrsquos mouth (60 Minutes II 1999)
diams Here in California Kristal Mayon-Ceniceros age 16 died of respiratory arrest in New Alternatives a private Chula Visa residential-care facility She died after being restrained face-down on the floor by four staff members (Associated Press 1999)
diams Also in California Rick Griffin 36 of Stockton died of cardio-respiratory failure and extreme agitation in the San Joaquin County Psychiatric Health Facility He had been wrestled to the floor by eight staff members and bound in leather restraints (The Stockton Record 1998)
diams Andrew McClain was 11 years old and weighed 96 pounds when two aides at the Elmcrest psychiatric hospital in Portland Connecticut sat on his back and crushed him to death His offense Refusing to move to another breakfast table (Lieberman Dodd and De Lauro 1999)
diams Edith Campos 15 suffocated while being held face-down after resisting an aide at the Desert Hills Center for Youth and Families in Tucson Arizona She was subjected to restraints after refusing to hand over an ldquounauthorizedrdquo personal item The item was a family photograph (Lieberman Dodd and De Lauro 1999)
Initial Response
The Courant series sparked congressional hearings into SR policies and how people have been traumatized injured and killed as a result of these practices Congressional leaders responded with federal reform proposals In a series of high-profile hearings
- 6 -
Seclusion and Restraints A Failure Not a Treatment
deaths injuries and abuses resulting from seclusion and restraints were exposed
Unfortunately these are not isolated incidents They are but a few of scores of cases in which mental health patients ndash a disproportionate number of them children ndash died barbaric deaths more suited to medieval torture chambers than to late 20th century America They died because of the improper use of seclusion and physical or chemical restraints They died at the hands of the very people who were supposed to protect them
- Senator Lieberman Senator Dodd and Representative DeLauro July 16 1999
The National Alliance for the Mentally Ill (NAMI) also has tracked reports of recent and past SR abuses (Appendix 2) NAMI reported over 25 new incidents nationwide of deaths injuries and traumas caused by seclusion and restraints after the Courant survey Currently there is no official tracking of injury or trauma to patients or to staff in California NAMI however reported numerous incidents of serious injury ndash patients who became comatose who suffered broken bones were hit in the face bruised needed stitches or were bleeding as a result of restraints19
Equally troubling is the humiliation and trauma NAMI documents such as its many reports of patients unable to use the bathroom and left for hours in their own bodily wastes One patient was restrained for rejecting medication because she still hoped to nurse her young child another was placed in restraints because he couldnrsquot stop crying A 12-year-old was placed in a straightjacket in the middle of the floor where everyone could watch her ndash and staff called this a ldquoburritordquo A patient who voluntarily admitted herself to a hospital found herself reliving former traumatic experiences
Suddenly the guard had a huge pair of leather cuffs with padlocks on them All I knew was that I was being strapped down to a bed by a strange man with a gun This is not good therapy for a rape victim All I could do was close my eyes and pretend this wasnrsquot happening to me20
The US General Accounting Office (GAO) in an October 1999 report on improper seclusion and restraints validated the notion that patients may be severely traumatized while being restrained
- 7 -
Seclusion and Restraints A Failure Not a Treatment
even if no physical injuries are sustained ldquo Research indicates that at least half of all women treated in psychiatric settings have a history of physical or sexual abuserdquo21
Citing a Massachusetts state task force on the topic the GAO stated that the use of restraints on patients who have been abused often results in their re-experiencing their traumas and contributes to a setback in the course of treatment
Congress adopted reforms to federal policies administered by the US Centers for Medicare and Medicaid Services (CMS formerly HCFA) in 1999 In addition the Joint Commission on Accreditation of Healthcare Organizations has adopted new policies The recently enacted Childrenrsquos Healthcare Act of 2000 was the third major federal reform Explained more fully in Part II of this report these new policies are intended to restrict and reduce SR practices
Despite these reforms the federally mandated advocate organization Protection and Advocacy reports that 14 Californians have died and one has beenen permanently injured (in a persistent coma) while in seclusion or behavioral restraints since the new CMS rules were put into place in July 1999 Since there is no official requirement for reporting nonfatal injuries we cannot officially confirm the types of injuries documented by NAMI the news media and the GAO
Californiarsquos standards governing SR practice are different for each kind of facility State hospitals general acute care hospitals psychiatric health facilities skilled nursing facilities ndash all are facilities that utilize SR However each type of facility is governed by a different set of state regulations For example
General Acute Care Hospitals ndash In a case of emergency SR can be initiated at the discretion of a registered nurse and a verbal or written order obtained from a physician afterwards If a verbal order is obtained it shall be signed by the physician on his next visit Orders for SR may be for longer than 24 hours
Psychiatric Health Facilities ndash In an emergency a physicianrsquos order can be received over the telephone within one hour of initiating SR and must be signed in person within 24 hours Orders for SR may be in force for no longer than 24 hours
Skilled Nursing Facilities with Special Treatment Programs ndash A physician may give the order for SR by telephone and sign it in
- 8 -
Seclusion and Restraints A Failure Not a Treatment
person within five days The order expires and must be renewed each 24 hours to keep a person in SR
Each facilityrsquos standards differ from the others and on this particular issue none is as stringent as the federal standard Californiarsquos regulatory standards and some of the problems associated with them are discussed more fully under ldquoPatchwork Oversightrdquo on page 15
Scope of Report
This report focuses on issues of psychiatric seclusion and restraints It does not address issues of medical restraints such as immobilizing a person for a surgical procedure or placing a personrsquos arm in a ldquosleeverdquo to prevent removing an intravenous needle Nor does it address the important issues of SR policies in schools or facilities for the developmentally disabled or in correctional facilities for youths or adults It is limited in scope to policies of psychiatric seclusion and restraints in mental health facilities
The Pennsylvania Experience
Seclusion and restraints have been used to control the behavior of psychiatric patients since the Middle Ages22 However these techniques have also involved high risk of patient injury and death Pennsylvania has been a leader in trying to change this culture and working to reduce and ultimately eliminate the use of seclusion and restraints in its nine state hospitals
The Pennsylvania Office of Mental Health and Substance Abuse Services implemented its program because
hellipthese measures [SR] do not alleviate human suffering or psychiatric symptoms do not alter behavior and have frequently resulted in patient and staff injury emotional trauma and patient death23
Expert testimony at hearings of the Joint Commission on Accreditation of Healthcare Organizations also called attention to the counter-therapeutic aspects of SR
The attempt to impose ldquotreatmentrdquo by force is always counterproductive ndash creating humiliation resentment and resistance to further treatment that might be more helpful24
- 9 -
Seclusion and Restraints A Failure Not a Treatment
In practice seclusion and restraints are sometimes imposed on psychiatric patients for reasons that are not therapeutic These uses of SR have been discredited and are illegal under current law however they persist SR practices are sometimes used to
diams Control the environment ndash To curtail a patientrsquos movement to compensate for having inadequate staff on the ward or to avoid providing appropriate clinical interventions
diams Coerce ndash To force a patient to comply with the staffrsquos wishes or
diams Punish ndash To impose penalties on patient behaviors
NAMI has been a leader in the effort to end SR on these terms Its position is that restraints and seclusion have no therapeutic value and therefore they are not a ldquotreatmentrdquo NAMI asserts that SR are dangerous interventions and should be used only in cases of extreme emergency when someonersquos physical safety is in jeopardy and then only with careful safeguards25
The idea that psychiatric patients are treated with brutality are seriously injured or even killed in this day and age may be difficult to believe But the Courant investigation the Harvard Center for Risk Analysis and NAMIrsquos report all demonstrate that these practices continue to exist placing psychiatric patients at risk of trauma injury and even death In the most egregious cases where someone has died the causes of death are frequently violent asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdose drug interactions and choking26
These are our most vulnerable citizens Since they are often held against their will supposedly for their own well being it would be incumbent upon the state to protect them from being injured traumatized and abused
To address that responsibility this paper examines three critical issues
1) Seclusion and restraints policies have received national attention and have been the focus of three successive initiatives of federal reform Is that enough
2) Californiarsquos oversight of seclusion and restraints is a patchwork quilt of confusing bureaucracy that impedes accountability and progress Can it be improved
- 10 -
Seclusion and Restraints A Failure Not a Treatment
3) Other states have taken action to improve seclusion and restraints policies on the state level Most notably Pennsylvania has developed a model that garnered the Harvard Innovations in American Government Award and reduced hours of seclusion and restraints by 96 percent in its state hospitals Can California benefit from model practices developed in Pennsylvania
- 11 -
Seclusion and Restraints A Failure Not a Treatment
Part II
Federal Reforms and State Impacts
New Federal Regulations Three Layers of Reform
In response to the Hartford Courant series and the vigorous lobbying of NAMI federal actions to revise national policy on seclusion and restraints were proposed and implemented Reform came in three successive initiatives
diams First the US Centers for Medicare and Medicaid Services (CMS) issued new interim rules for Medicare and Medicaid hospitals in July of 1999
diams Next the Joint Commission on Accreditation of Healthcare Organizations released revised seclusion and restraints standards that took effect January 1 2001
diams Most recently on May 22 last year CMS issued Interim Final Rules under the Childrenrsquos Health Act of 2000 setting forth new regulations for psychiatric facilities that receive federal funds and for ldquononmedical community-based facilities for children and youthrdquo
First Reform CMS Breaks New Ground
CMS set forth interim final rules as of July 1999 that revised seclusion and restraints standards in any hospital that receives Medicare or Medicaid financing
The preamble to the rules broke new ground by declaring ldquoThe patientrsquos right to be free from restraints is paramountrdquo27 The rules stated that SR may only be used in emergency situations if needed to ensure the patientrsquos physical safety and when less-restrictive alternatives have been determined ineffective and that
- 12 -
Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Contents
Executive Summary 1
Part I Seclusion and Restraints Issues and Actions 5
Part II Federal Reforms and State Impacts 12
Part III Pennsylvania ndash A Model for Reform 20
Part IV Conclusion 24
Endnotes 27
Figures
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities 16
Figure 2 Pennsylvania Reduces Incidents of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96 21
Figure 3 Pennsylvania Seclusion and Restraints Reduction Initiative 23
Appendices 31
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between March 2000 and October 1998
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000
Seclusion and Restraints A Failure Not a Treatment
Executive Summary
Overview
Seclusion and restraint of psychiatric patients are known to be dangerous practices that can result in serious injury trauma and even death1 The Harvard Center for Risk Analysis estimates that 50 to 150 deaths occur nationally each year because of psychiatric seclusion and restraints2 Here in California at least 14 people have died and at least one has become permanently comatose while being subjected to these practices since July of 19993 This does not reflect those who are injured or traumatized ndash California does not keep track of those data
We do know however that at a very conservative estimate over 100000 Californians are involuntarily committed to psychiatric facilities each year4 and that along with voluntary patients they are at risk of being subjected to seclusion and restraints (SR)
Accounts of serious injuries and deaths resulting from SR were reported in the Hartford Courant and other sources during 1998 and gained wide national attention These reports found that patients became comatose suffered broken bones were hit in the face bruised needed stitches or were bleeding as a result of being placed in SR5 In the worst cases patients died of causes that included asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdoses or interactions and choking6
These revelations led Congress to adopt significant federal reforms in 1999 and again in 2000 The Joint Commission on the Accreditation of Healthcare Organizations also adopted new policies that affect about 80 percent of the nationrsquos health care facilities However federal reforms have not by themselves prevented harm to our most vulnerable citizens held in psychiatric
Seclusion and Restraints A Failure Not a Treatment
facilities against their will for what is supposedly their own well-being
Californiarsquos oversight of SR in psychiatric facilities is a regulatory maze that impedes accountability and progress In addition statewide standards on SR are piecemeal depending upon the type of facility and we lack a comprehensive and mandatory statewide reporting system Consequently the only meaningful measure of seclusion and restraints in California is when people die
The California Office of Patient Rights is vested with responsibility for collecting and reporting information about use of SR However it must rely on data supplied by counties and facilities In 2000 the Office of Patient Rights documented a high rate of noncompliance with reporting requirements 56 facilities or 22 percent submitted either an incomplete report or no report at all7
Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement8
The Office of Patient Rights cites these limitations in Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements9
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements10
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements11
For these reasons the Office of Patient Rights has concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo12 In addition the California Department of Health Services reports that it does not consider data on seclusion and restraints from the Office of Patient Rights when deciding whether to conduct inspections on facilities
- 2 -
Seclusion and Restraints A Failure Not a Treatment
Other states have imposed new restrictions in their SR policies Most notably Pennsylvania has developed an award-winning model that reduced overall incidents of seclusion and restraint by 74 percent and reduced the hours that patients spent in SR by 96 percent over a three-year period13
The Pennsylvania reforms were accomplished with no additional staff or funds and no increase in injuries to staff14 Charles Curie then deputy secretary of Pennsylvaniarsquos mental health and substance abuse services15 articulated a new philosophy of care that became the basis for a comprehensive change of culture in Pennsylvaniarsquos state hospital system ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo16
Pennsylvaniarsquos first step was to institute a mandated and publicly accountable system of tracking seclusion and restraints The state developed system-wide policies that required training diffusion of conflict accountability for using SR awards and recognition for reducing its use cultural competence a prohibition on all chemical restraints a prohibition on using SR on voluntary patients and debriefings with patients families and staff after each incident Central to these reforms was the core concept that seclusion and restraints are not treatment ndash they reflect a treatment failure and should be handled as such to prevent the escalation of violence This commitment has radically changed the longstanding culture environment and level of violence in Pennsylvaniarsquos nine state hospitals
This analysis determines that Californiarsquos piecemeal regulatory system could benefit from practices similar to those developed in Pennsylvania
Findings and Options
The new federal reforms that govern SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to accountability in the use of SR in California facilities
diams A lack of uniform statewide standards across various types of facilities and
diams A lack of mandatory consistent and publicly accessible reporting on the use and consequences of SR These include deaths serious injuries frequency and duration of SR and
- 3 -
Seclusion and Restraints A Failure Not a Treatment
related conditions and situations such as airway obstructions patient falls staff injuries and medication errors
Private psychiatric hospitals may be the most difficult to regulate The US inspector general found in August 2000 that private facilities may be the least likely to comply with the 1999 federal SR regulations and therefore may be the most in need of uniform state standards and enforcement17
There is compelling evidence in the Pennsylvania experience that SR can be dramatically reduced with a change of organizational values and culture
The following steps could be taken with a goal of reducing SR practices and the injuries deaths and traumas that can result from them
diams California could develop uniform seclusion and restraint standards that match if not exceed the highest federal regulations to cover all facilities ndash private as well as public ndash that treat people with psychiatric disabilities Federal standards vary based on licensing and accreditation while state standards vary based on type of facility The experience of other states has shown that a high uniform state standard improves the quality of enforcement and compliance
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to safely and cost-effectively reduce the use of SR in California
- 4 -
Seclusion and Restraints A Failure Not a Treatment
Part I
Seclusion and Restraints Issues and Actions
The issue of seclusion and restraint of psychiatric and substance-abuse patients gained national notoriety in October of 1998 when the Hartford Courant published a five-part investigative series entitled ldquoDeadly Restraintrdquo The Courant conducted a national survey that documented 142 deaths in the past decade that were directly connected to the use of seclusion or physical restraints (Appendix 1)
Seclusion refers to isolating a person in a locked room Restraints are human or mechanical measures that use force or the threat of force to control someonersquos actions ldquoTake downsrdquolowast holding someone face-down in a prone position strait jackets or tying someone by hands and feet are all examples of restraints Chemical restraints are medications that are not otherwise necessary and that are used to control someonersquos behavior
The Harvard Center for Risk Analysis has estimated that deaths and injuries from seclusion and restraints are significantly under-reported Its study of the prevalence of seclusion and restraint-related deaths statistically estimated that between 50 and 150 deaths occur nationally each year because of SR use on psychiatric and substance-abuse patients18
A national impetus for reform was triggered by incidents reported by the Courant and other sources
lowast A ldquotake downrdquo is a technique to force an uncooperative person to the floor to place him or her in restraints At least five staff surround the patient each taking the head an arm or leg and force him or her down Injury to the patient often occurs if staff sit on the person while restraints are secured This technique is frequently violent causing significant patient and staff injuries
- 5 -
Seclusion and Restraints A Failure Not a Treatment
diams Gloria Huntley 31 years old died in Central State Hospital in Petersburg Virginia after having been kept in restraints for 558 hours during the last two months of her life Although she had been diagnosed with asthma and epilepsy she was nevertheless restrained over and over again because of angry outbursts at hospital staff (Hartford Courant 1998)
diams Sixteen-year-old Tristan Sovern died in Charter Greensboro in North Carolina in 1998 after he was placed in restraints as ldquopunishmentrdquo for leaving a group-therapy session In response to his screams of ldquoYoursquore choking me I canrsquot breatherdquo a towel was shoved over Tristanrsquos mouth (60 Minutes II 1999)
diams Here in California Kristal Mayon-Ceniceros age 16 died of respiratory arrest in New Alternatives a private Chula Visa residential-care facility She died after being restrained face-down on the floor by four staff members (Associated Press 1999)
diams Also in California Rick Griffin 36 of Stockton died of cardio-respiratory failure and extreme agitation in the San Joaquin County Psychiatric Health Facility He had been wrestled to the floor by eight staff members and bound in leather restraints (The Stockton Record 1998)
diams Andrew McClain was 11 years old and weighed 96 pounds when two aides at the Elmcrest psychiatric hospital in Portland Connecticut sat on his back and crushed him to death His offense Refusing to move to another breakfast table (Lieberman Dodd and De Lauro 1999)
diams Edith Campos 15 suffocated while being held face-down after resisting an aide at the Desert Hills Center for Youth and Families in Tucson Arizona She was subjected to restraints after refusing to hand over an ldquounauthorizedrdquo personal item The item was a family photograph (Lieberman Dodd and De Lauro 1999)
Initial Response
The Courant series sparked congressional hearings into SR policies and how people have been traumatized injured and killed as a result of these practices Congressional leaders responded with federal reform proposals In a series of high-profile hearings
- 6 -
Seclusion and Restraints A Failure Not a Treatment
deaths injuries and abuses resulting from seclusion and restraints were exposed
Unfortunately these are not isolated incidents They are but a few of scores of cases in which mental health patients ndash a disproportionate number of them children ndash died barbaric deaths more suited to medieval torture chambers than to late 20th century America They died because of the improper use of seclusion and physical or chemical restraints They died at the hands of the very people who were supposed to protect them
- Senator Lieberman Senator Dodd and Representative DeLauro July 16 1999
The National Alliance for the Mentally Ill (NAMI) also has tracked reports of recent and past SR abuses (Appendix 2) NAMI reported over 25 new incidents nationwide of deaths injuries and traumas caused by seclusion and restraints after the Courant survey Currently there is no official tracking of injury or trauma to patients or to staff in California NAMI however reported numerous incidents of serious injury ndash patients who became comatose who suffered broken bones were hit in the face bruised needed stitches or were bleeding as a result of restraints19
Equally troubling is the humiliation and trauma NAMI documents such as its many reports of patients unable to use the bathroom and left for hours in their own bodily wastes One patient was restrained for rejecting medication because she still hoped to nurse her young child another was placed in restraints because he couldnrsquot stop crying A 12-year-old was placed in a straightjacket in the middle of the floor where everyone could watch her ndash and staff called this a ldquoburritordquo A patient who voluntarily admitted herself to a hospital found herself reliving former traumatic experiences
Suddenly the guard had a huge pair of leather cuffs with padlocks on them All I knew was that I was being strapped down to a bed by a strange man with a gun This is not good therapy for a rape victim All I could do was close my eyes and pretend this wasnrsquot happening to me20
The US General Accounting Office (GAO) in an October 1999 report on improper seclusion and restraints validated the notion that patients may be severely traumatized while being restrained
- 7 -
Seclusion and Restraints A Failure Not a Treatment
even if no physical injuries are sustained ldquo Research indicates that at least half of all women treated in psychiatric settings have a history of physical or sexual abuserdquo21
Citing a Massachusetts state task force on the topic the GAO stated that the use of restraints on patients who have been abused often results in their re-experiencing their traumas and contributes to a setback in the course of treatment
Congress adopted reforms to federal policies administered by the US Centers for Medicare and Medicaid Services (CMS formerly HCFA) in 1999 In addition the Joint Commission on Accreditation of Healthcare Organizations has adopted new policies The recently enacted Childrenrsquos Healthcare Act of 2000 was the third major federal reform Explained more fully in Part II of this report these new policies are intended to restrict and reduce SR practices
Despite these reforms the federally mandated advocate organization Protection and Advocacy reports that 14 Californians have died and one has beenen permanently injured (in a persistent coma) while in seclusion or behavioral restraints since the new CMS rules were put into place in July 1999 Since there is no official requirement for reporting nonfatal injuries we cannot officially confirm the types of injuries documented by NAMI the news media and the GAO
Californiarsquos standards governing SR practice are different for each kind of facility State hospitals general acute care hospitals psychiatric health facilities skilled nursing facilities ndash all are facilities that utilize SR However each type of facility is governed by a different set of state regulations For example
General Acute Care Hospitals ndash In a case of emergency SR can be initiated at the discretion of a registered nurse and a verbal or written order obtained from a physician afterwards If a verbal order is obtained it shall be signed by the physician on his next visit Orders for SR may be for longer than 24 hours
Psychiatric Health Facilities ndash In an emergency a physicianrsquos order can be received over the telephone within one hour of initiating SR and must be signed in person within 24 hours Orders for SR may be in force for no longer than 24 hours
Skilled Nursing Facilities with Special Treatment Programs ndash A physician may give the order for SR by telephone and sign it in
- 8 -
Seclusion and Restraints A Failure Not a Treatment
person within five days The order expires and must be renewed each 24 hours to keep a person in SR
Each facilityrsquos standards differ from the others and on this particular issue none is as stringent as the federal standard Californiarsquos regulatory standards and some of the problems associated with them are discussed more fully under ldquoPatchwork Oversightrdquo on page 15
Scope of Report
This report focuses on issues of psychiatric seclusion and restraints It does not address issues of medical restraints such as immobilizing a person for a surgical procedure or placing a personrsquos arm in a ldquosleeverdquo to prevent removing an intravenous needle Nor does it address the important issues of SR policies in schools or facilities for the developmentally disabled or in correctional facilities for youths or adults It is limited in scope to policies of psychiatric seclusion and restraints in mental health facilities
The Pennsylvania Experience
Seclusion and restraints have been used to control the behavior of psychiatric patients since the Middle Ages22 However these techniques have also involved high risk of patient injury and death Pennsylvania has been a leader in trying to change this culture and working to reduce and ultimately eliminate the use of seclusion and restraints in its nine state hospitals
The Pennsylvania Office of Mental Health and Substance Abuse Services implemented its program because
hellipthese measures [SR] do not alleviate human suffering or psychiatric symptoms do not alter behavior and have frequently resulted in patient and staff injury emotional trauma and patient death23
Expert testimony at hearings of the Joint Commission on Accreditation of Healthcare Organizations also called attention to the counter-therapeutic aspects of SR
The attempt to impose ldquotreatmentrdquo by force is always counterproductive ndash creating humiliation resentment and resistance to further treatment that might be more helpful24
- 9 -
Seclusion and Restraints A Failure Not a Treatment
In practice seclusion and restraints are sometimes imposed on psychiatric patients for reasons that are not therapeutic These uses of SR have been discredited and are illegal under current law however they persist SR practices are sometimes used to
diams Control the environment ndash To curtail a patientrsquos movement to compensate for having inadequate staff on the ward or to avoid providing appropriate clinical interventions
diams Coerce ndash To force a patient to comply with the staffrsquos wishes or
diams Punish ndash To impose penalties on patient behaviors
NAMI has been a leader in the effort to end SR on these terms Its position is that restraints and seclusion have no therapeutic value and therefore they are not a ldquotreatmentrdquo NAMI asserts that SR are dangerous interventions and should be used only in cases of extreme emergency when someonersquos physical safety is in jeopardy and then only with careful safeguards25
The idea that psychiatric patients are treated with brutality are seriously injured or even killed in this day and age may be difficult to believe But the Courant investigation the Harvard Center for Risk Analysis and NAMIrsquos report all demonstrate that these practices continue to exist placing psychiatric patients at risk of trauma injury and even death In the most egregious cases where someone has died the causes of death are frequently violent asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdose drug interactions and choking26
These are our most vulnerable citizens Since they are often held against their will supposedly for their own well being it would be incumbent upon the state to protect them from being injured traumatized and abused
To address that responsibility this paper examines three critical issues
1) Seclusion and restraints policies have received national attention and have been the focus of three successive initiatives of federal reform Is that enough
2) Californiarsquos oversight of seclusion and restraints is a patchwork quilt of confusing bureaucracy that impedes accountability and progress Can it be improved
- 10 -
Seclusion and Restraints A Failure Not a Treatment
3) Other states have taken action to improve seclusion and restraints policies on the state level Most notably Pennsylvania has developed a model that garnered the Harvard Innovations in American Government Award and reduced hours of seclusion and restraints by 96 percent in its state hospitals Can California benefit from model practices developed in Pennsylvania
- 11 -
Seclusion and Restraints A Failure Not a Treatment
Part II
Federal Reforms and State Impacts
New Federal Regulations Three Layers of Reform
In response to the Hartford Courant series and the vigorous lobbying of NAMI federal actions to revise national policy on seclusion and restraints were proposed and implemented Reform came in three successive initiatives
diams First the US Centers for Medicare and Medicaid Services (CMS) issued new interim rules for Medicare and Medicaid hospitals in July of 1999
diams Next the Joint Commission on Accreditation of Healthcare Organizations released revised seclusion and restraints standards that took effect January 1 2001
diams Most recently on May 22 last year CMS issued Interim Final Rules under the Childrenrsquos Health Act of 2000 setting forth new regulations for psychiatric facilities that receive federal funds and for ldquononmedical community-based facilities for children and youthrdquo
First Reform CMS Breaks New Ground
CMS set forth interim final rules as of July 1999 that revised seclusion and restraints standards in any hospital that receives Medicare or Medicaid financing
The preamble to the rules broke new ground by declaring ldquoThe patientrsquos right to be free from restraints is paramountrdquo27 The rules stated that SR may only be used in emergency situations if needed to ensure the patientrsquos physical safety and when less-restrictive alternatives have been determined ineffective and that
- 12 -
Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
Executive Summary
Overview
Seclusion and restraint of psychiatric patients are known to be dangerous practices that can result in serious injury trauma and even death1 The Harvard Center for Risk Analysis estimates that 50 to 150 deaths occur nationally each year because of psychiatric seclusion and restraints2 Here in California at least 14 people have died and at least one has become permanently comatose while being subjected to these practices since July of 19993 This does not reflect those who are injured or traumatized ndash California does not keep track of those data
We do know however that at a very conservative estimate over 100000 Californians are involuntarily committed to psychiatric facilities each year4 and that along with voluntary patients they are at risk of being subjected to seclusion and restraints (SR)
Accounts of serious injuries and deaths resulting from SR were reported in the Hartford Courant and other sources during 1998 and gained wide national attention These reports found that patients became comatose suffered broken bones were hit in the face bruised needed stitches or were bleeding as a result of being placed in SR5 In the worst cases patients died of causes that included asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdoses or interactions and choking6
These revelations led Congress to adopt significant federal reforms in 1999 and again in 2000 The Joint Commission on the Accreditation of Healthcare Organizations also adopted new policies that affect about 80 percent of the nationrsquos health care facilities However federal reforms have not by themselves prevented harm to our most vulnerable citizens held in psychiatric
Seclusion and Restraints A Failure Not a Treatment
facilities against their will for what is supposedly their own well-being
Californiarsquos oversight of SR in psychiatric facilities is a regulatory maze that impedes accountability and progress In addition statewide standards on SR are piecemeal depending upon the type of facility and we lack a comprehensive and mandatory statewide reporting system Consequently the only meaningful measure of seclusion and restraints in California is when people die
The California Office of Patient Rights is vested with responsibility for collecting and reporting information about use of SR However it must rely on data supplied by counties and facilities In 2000 the Office of Patient Rights documented a high rate of noncompliance with reporting requirements 56 facilities or 22 percent submitted either an incomplete report or no report at all7
Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement8
The Office of Patient Rights cites these limitations in Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements9
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements10
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements11
For these reasons the Office of Patient Rights has concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo12 In addition the California Department of Health Services reports that it does not consider data on seclusion and restraints from the Office of Patient Rights when deciding whether to conduct inspections on facilities
- 2 -
Seclusion and Restraints A Failure Not a Treatment
Other states have imposed new restrictions in their SR policies Most notably Pennsylvania has developed an award-winning model that reduced overall incidents of seclusion and restraint by 74 percent and reduced the hours that patients spent in SR by 96 percent over a three-year period13
The Pennsylvania reforms were accomplished with no additional staff or funds and no increase in injuries to staff14 Charles Curie then deputy secretary of Pennsylvaniarsquos mental health and substance abuse services15 articulated a new philosophy of care that became the basis for a comprehensive change of culture in Pennsylvaniarsquos state hospital system ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo16
Pennsylvaniarsquos first step was to institute a mandated and publicly accountable system of tracking seclusion and restraints The state developed system-wide policies that required training diffusion of conflict accountability for using SR awards and recognition for reducing its use cultural competence a prohibition on all chemical restraints a prohibition on using SR on voluntary patients and debriefings with patients families and staff after each incident Central to these reforms was the core concept that seclusion and restraints are not treatment ndash they reflect a treatment failure and should be handled as such to prevent the escalation of violence This commitment has radically changed the longstanding culture environment and level of violence in Pennsylvaniarsquos nine state hospitals
This analysis determines that Californiarsquos piecemeal regulatory system could benefit from practices similar to those developed in Pennsylvania
Findings and Options
The new federal reforms that govern SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to accountability in the use of SR in California facilities
diams A lack of uniform statewide standards across various types of facilities and
diams A lack of mandatory consistent and publicly accessible reporting on the use and consequences of SR These include deaths serious injuries frequency and duration of SR and
- 3 -
Seclusion and Restraints A Failure Not a Treatment
related conditions and situations such as airway obstructions patient falls staff injuries and medication errors
Private psychiatric hospitals may be the most difficult to regulate The US inspector general found in August 2000 that private facilities may be the least likely to comply with the 1999 federal SR regulations and therefore may be the most in need of uniform state standards and enforcement17
There is compelling evidence in the Pennsylvania experience that SR can be dramatically reduced with a change of organizational values and culture
The following steps could be taken with a goal of reducing SR practices and the injuries deaths and traumas that can result from them
diams California could develop uniform seclusion and restraint standards that match if not exceed the highest federal regulations to cover all facilities ndash private as well as public ndash that treat people with psychiatric disabilities Federal standards vary based on licensing and accreditation while state standards vary based on type of facility The experience of other states has shown that a high uniform state standard improves the quality of enforcement and compliance
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to safely and cost-effectively reduce the use of SR in California
- 4 -
Seclusion and Restraints A Failure Not a Treatment
Part I
Seclusion and Restraints Issues and Actions
The issue of seclusion and restraint of psychiatric and substance-abuse patients gained national notoriety in October of 1998 when the Hartford Courant published a five-part investigative series entitled ldquoDeadly Restraintrdquo The Courant conducted a national survey that documented 142 deaths in the past decade that were directly connected to the use of seclusion or physical restraints (Appendix 1)
Seclusion refers to isolating a person in a locked room Restraints are human or mechanical measures that use force or the threat of force to control someonersquos actions ldquoTake downsrdquolowast holding someone face-down in a prone position strait jackets or tying someone by hands and feet are all examples of restraints Chemical restraints are medications that are not otherwise necessary and that are used to control someonersquos behavior
The Harvard Center for Risk Analysis has estimated that deaths and injuries from seclusion and restraints are significantly under-reported Its study of the prevalence of seclusion and restraint-related deaths statistically estimated that between 50 and 150 deaths occur nationally each year because of SR use on psychiatric and substance-abuse patients18
A national impetus for reform was triggered by incidents reported by the Courant and other sources
lowast A ldquotake downrdquo is a technique to force an uncooperative person to the floor to place him or her in restraints At least five staff surround the patient each taking the head an arm or leg and force him or her down Injury to the patient often occurs if staff sit on the person while restraints are secured This technique is frequently violent causing significant patient and staff injuries
- 5 -
Seclusion and Restraints A Failure Not a Treatment
diams Gloria Huntley 31 years old died in Central State Hospital in Petersburg Virginia after having been kept in restraints for 558 hours during the last two months of her life Although she had been diagnosed with asthma and epilepsy she was nevertheless restrained over and over again because of angry outbursts at hospital staff (Hartford Courant 1998)
diams Sixteen-year-old Tristan Sovern died in Charter Greensboro in North Carolina in 1998 after he was placed in restraints as ldquopunishmentrdquo for leaving a group-therapy session In response to his screams of ldquoYoursquore choking me I canrsquot breatherdquo a towel was shoved over Tristanrsquos mouth (60 Minutes II 1999)
diams Here in California Kristal Mayon-Ceniceros age 16 died of respiratory arrest in New Alternatives a private Chula Visa residential-care facility She died after being restrained face-down on the floor by four staff members (Associated Press 1999)
diams Also in California Rick Griffin 36 of Stockton died of cardio-respiratory failure and extreme agitation in the San Joaquin County Psychiatric Health Facility He had been wrestled to the floor by eight staff members and bound in leather restraints (The Stockton Record 1998)
diams Andrew McClain was 11 years old and weighed 96 pounds when two aides at the Elmcrest psychiatric hospital in Portland Connecticut sat on his back and crushed him to death His offense Refusing to move to another breakfast table (Lieberman Dodd and De Lauro 1999)
diams Edith Campos 15 suffocated while being held face-down after resisting an aide at the Desert Hills Center for Youth and Families in Tucson Arizona She was subjected to restraints after refusing to hand over an ldquounauthorizedrdquo personal item The item was a family photograph (Lieberman Dodd and De Lauro 1999)
Initial Response
The Courant series sparked congressional hearings into SR policies and how people have been traumatized injured and killed as a result of these practices Congressional leaders responded with federal reform proposals In a series of high-profile hearings
- 6 -
Seclusion and Restraints A Failure Not a Treatment
deaths injuries and abuses resulting from seclusion and restraints were exposed
Unfortunately these are not isolated incidents They are but a few of scores of cases in which mental health patients ndash a disproportionate number of them children ndash died barbaric deaths more suited to medieval torture chambers than to late 20th century America They died because of the improper use of seclusion and physical or chemical restraints They died at the hands of the very people who were supposed to protect them
- Senator Lieberman Senator Dodd and Representative DeLauro July 16 1999
The National Alliance for the Mentally Ill (NAMI) also has tracked reports of recent and past SR abuses (Appendix 2) NAMI reported over 25 new incidents nationwide of deaths injuries and traumas caused by seclusion and restraints after the Courant survey Currently there is no official tracking of injury or trauma to patients or to staff in California NAMI however reported numerous incidents of serious injury ndash patients who became comatose who suffered broken bones were hit in the face bruised needed stitches or were bleeding as a result of restraints19
Equally troubling is the humiliation and trauma NAMI documents such as its many reports of patients unable to use the bathroom and left for hours in their own bodily wastes One patient was restrained for rejecting medication because she still hoped to nurse her young child another was placed in restraints because he couldnrsquot stop crying A 12-year-old was placed in a straightjacket in the middle of the floor where everyone could watch her ndash and staff called this a ldquoburritordquo A patient who voluntarily admitted herself to a hospital found herself reliving former traumatic experiences
Suddenly the guard had a huge pair of leather cuffs with padlocks on them All I knew was that I was being strapped down to a bed by a strange man with a gun This is not good therapy for a rape victim All I could do was close my eyes and pretend this wasnrsquot happening to me20
The US General Accounting Office (GAO) in an October 1999 report on improper seclusion and restraints validated the notion that patients may be severely traumatized while being restrained
- 7 -
Seclusion and Restraints A Failure Not a Treatment
even if no physical injuries are sustained ldquo Research indicates that at least half of all women treated in psychiatric settings have a history of physical or sexual abuserdquo21
Citing a Massachusetts state task force on the topic the GAO stated that the use of restraints on patients who have been abused often results in their re-experiencing their traumas and contributes to a setback in the course of treatment
Congress adopted reforms to federal policies administered by the US Centers for Medicare and Medicaid Services (CMS formerly HCFA) in 1999 In addition the Joint Commission on Accreditation of Healthcare Organizations has adopted new policies The recently enacted Childrenrsquos Healthcare Act of 2000 was the third major federal reform Explained more fully in Part II of this report these new policies are intended to restrict and reduce SR practices
Despite these reforms the federally mandated advocate organization Protection and Advocacy reports that 14 Californians have died and one has beenen permanently injured (in a persistent coma) while in seclusion or behavioral restraints since the new CMS rules were put into place in July 1999 Since there is no official requirement for reporting nonfatal injuries we cannot officially confirm the types of injuries documented by NAMI the news media and the GAO
Californiarsquos standards governing SR practice are different for each kind of facility State hospitals general acute care hospitals psychiatric health facilities skilled nursing facilities ndash all are facilities that utilize SR However each type of facility is governed by a different set of state regulations For example
General Acute Care Hospitals ndash In a case of emergency SR can be initiated at the discretion of a registered nurse and a verbal or written order obtained from a physician afterwards If a verbal order is obtained it shall be signed by the physician on his next visit Orders for SR may be for longer than 24 hours
Psychiatric Health Facilities ndash In an emergency a physicianrsquos order can be received over the telephone within one hour of initiating SR and must be signed in person within 24 hours Orders for SR may be in force for no longer than 24 hours
Skilled Nursing Facilities with Special Treatment Programs ndash A physician may give the order for SR by telephone and sign it in
- 8 -
Seclusion and Restraints A Failure Not a Treatment
person within five days The order expires and must be renewed each 24 hours to keep a person in SR
Each facilityrsquos standards differ from the others and on this particular issue none is as stringent as the federal standard Californiarsquos regulatory standards and some of the problems associated with them are discussed more fully under ldquoPatchwork Oversightrdquo on page 15
Scope of Report
This report focuses on issues of psychiatric seclusion and restraints It does not address issues of medical restraints such as immobilizing a person for a surgical procedure or placing a personrsquos arm in a ldquosleeverdquo to prevent removing an intravenous needle Nor does it address the important issues of SR policies in schools or facilities for the developmentally disabled or in correctional facilities for youths or adults It is limited in scope to policies of psychiatric seclusion and restraints in mental health facilities
The Pennsylvania Experience
Seclusion and restraints have been used to control the behavior of psychiatric patients since the Middle Ages22 However these techniques have also involved high risk of patient injury and death Pennsylvania has been a leader in trying to change this culture and working to reduce and ultimately eliminate the use of seclusion and restraints in its nine state hospitals
The Pennsylvania Office of Mental Health and Substance Abuse Services implemented its program because
hellipthese measures [SR] do not alleviate human suffering or psychiatric symptoms do not alter behavior and have frequently resulted in patient and staff injury emotional trauma and patient death23
Expert testimony at hearings of the Joint Commission on Accreditation of Healthcare Organizations also called attention to the counter-therapeutic aspects of SR
The attempt to impose ldquotreatmentrdquo by force is always counterproductive ndash creating humiliation resentment and resistance to further treatment that might be more helpful24
- 9 -
Seclusion and Restraints A Failure Not a Treatment
In practice seclusion and restraints are sometimes imposed on psychiatric patients for reasons that are not therapeutic These uses of SR have been discredited and are illegal under current law however they persist SR practices are sometimes used to
diams Control the environment ndash To curtail a patientrsquos movement to compensate for having inadequate staff on the ward or to avoid providing appropriate clinical interventions
diams Coerce ndash To force a patient to comply with the staffrsquos wishes or
diams Punish ndash To impose penalties on patient behaviors
NAMI has been a leader in the effort to end SR on these terms Its position is that restraints and seclusion have no therapeutic value and therefore they are not a ldquotreatmentrdquo NAMI asserts that SR are dangerous interventions and should be used only in cases of extreme emergency when someonersquos physical safety is in jeopardy and then only with careful safeguards25
The idea that psychiatric patients are treated with brutality are seriously injured or even killed in this day and age may be difficult to believe But the Courant investigation the Harvard Center for Risk Analysis and NAMIrsquos report all demonstrate that these practices continue to exist placing psychiatric patients at risk of trauma injury and even death In the most egregious cases where someone has died the causes of death are frequently violent asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdose drug interactions and choking26
These are our most vulnerable citizens Since they are often held against their will supposedly for their own well being it would be incumbent upon the state to protect them from being injured traumatized and abused
To address that responsibility this paper examines three critical issues
1) Seclusion and restraints policies have received national attention and have been the focus of three successive initiatives of federal reform Is that enough
2) Californiarsquos oversight of seclusion and restraints is a patchwork quilt of confusing bureaucracy that impedes accountability and progress Can it be improved
- 10 -
Seclusion and Restraints A Failure Not a Treatment
3) Other states have taken action to improve seclusion and restraints policies on the state level Most notably Pennsylvania has developed a model that garnered the Harvard Innovations in American Government Award and reduced hours of seclusion and restraints by 96 percent in its state hospitals Can California benefit from model practices developed in Pennsylvania
- 11 -
Seclusion and Restraints A Failure Not a Treatment
Part II
Federal Reforms and State Impacts
New Federal Regulations Three Layers of Reform
In response to the Hartford Courant series and the vigorous lobbying of NAMI federal actions to revise national policy on seclusion and restraints were proposed and implemented Reform came in three successive initiatives
diams First the US Centers for Medicare and Medicaid Services (CMS) issued new interim rules for Medicare and Medicaid hospitals in July of 1999
diams Next the Joint Commission on Accreditation of Healthcare Organizations released revised seclusion and restraints standards that took effect January 1 2001
diams Most recently on May 22 last year CMS issued Interim Final Rules under the Childrenrsquos Health Act of 2000 setting forth new regulations for psychiatric facilities that receive federal funds and for ldquononmedical community-based facilities for children and youthrdquo
First Reform CMS Breaks New Ground
CMS set forth interim final rules as of July 1999 that revised seclusion and restraints standards in any hospital that receives Medicare or Medicaid financing
The preamble to the rules broke new ground by declaring ldquoThe patientrsquos right to be free from restraints is paramountrdquo27 The rules stated that SR may only be used in emergency situations if needed to ensure the patientrsquos physical safety and when less-restrictive alternatives have been determined ineffective and that
- 12 -
Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
facilities against their will for what is supposedly their own well-being
Californiarsquos oversight of SR in psychiatric facilities is a regulatory maze that impedes accountability and progress In addition statewide standards on SR are piecemeal depending upon the type of facility and we lack a comprehensive and mandatory statewide reporting system Consequently the only meaningful measure of seclusion and restraints in California is when people die
The California Office of Patient Rights is vested with responsibility for collecting and reporting information about use of SR However it must rely on data supplied by counties and facilities In 2000 the Office of Patient Rights documented a high rate of noncompliance with reporting requirements 56 facilities or 22 percent submitted either an incomplete report or no report at all7
Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement8
The Office of Patient Rights cites these limitations in Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements9
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements10
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements11
For these reasons the Office of Patient Rights has concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo12 In addition the California Department of Health Services reports that it does not consider data on seclusion and restraints from the Office of Patient Rights when deciding whether to conduct inspections on facilities
- 2 -
Seclusion and Restraints A Failure Not a Treatment
Other states have imposed new restrictions in their SR policies Most notably Pennsylvania has developed an award-winning model that reduced overall incidents of seclusion and restraint by 74 percent and reduced the hours that patients spent in SR by 96 percent over a three-year period13
The Pennsylvania reforms were accomplished with no additional staff or funds and no increase in injuries to staff14 Charles Curie then deputy secretary of Pennsylvaniarsquos mental health and substance abuse services15 articulated a new philosophy of care that became the basis for a comprehensive change of culture in Pennsylvaniarsquos state hospital system ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo16
Pennsylvaniarsquos first step was to institute a mandated and publicly accountable system of tracking seclusion and restraints The state developed system-wide policies that required training diffusion of conflict accountability for using SR awards and recognition for reducing its use cultural competence a prohibition on all chemical restraints a prohibition on using SR on voluntary patients and debriefings with patients families and staff after each incident Central to these reforms was the core concept that seclusion and restraints are not treatment ndash they reflect a treatment failure and should be handled as such to prevent the escalation of violence This commitment has radically changed the longstanding culture environment and level of violence in Pennsylvaniarsquos nine state hospitals
This analysis determines that Californiarsquos piecemeal regulatory system could benefit from practices similar to those developed in Pennsylvania
Findings and Options
The new federal reforms that govern SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to accountability in the use of SR in California facilities
diams A lack of uniform statewide standards across various types of facilities and
diams A lack of mandatory consistent and publicly accessible reporting on the use and consequences of SR These include deaths serious injuries frequency and duration of SR and
- 3 -
Seclusion and Restraints A Failure Not a Treatment
related conditions and situations such as airway obstructions patient falls staff injuries and medication errors
Private psychiatric hospitals may be the most difficult to regulate The US inspector general found in August 2000 that private facilities may be the least likely to comply with the 1999 federal SR regulations and therefore may be the most in need of uniform state standards and enforcement17
There is compelling evidence in the Pennsylvania experience that SR can be dramatically reduced with a change of organizational values and culture
The following steps could be taken with a goal of reducing SR practices and the injuries deaths and traumas that can result from them
diams California could develop uniform seclusion and restraint standards that match if not exceed the highest federal regulations to cover all facilities ndash private as well as public ndash that treat people with psychiatric disabilities Federal standards vary based on licensing and accreditation while state standards vary based on type of facility The experience of other states has shown that a high uniform state standard improves the quality of enforcement and compliance
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to safely and cost-effectively reduce the use of SR in California
- 4 -
Seclusion and Restraints A Failure Not a Treatment
Part I
Seclusion and Restraints Issues and Actions
The issue of seclusion and restraint of psychiatric and substance-abuse patients gained national notoriety in October of 1998 when the Hartford Courant published a five-part investigative series entitled ldquoDeadly Restraintrdquo The Courant conducted a national survey that documented 142 deaths in the past decade that were directly connected to the use of seclusion or physical restraints (Appendix 1)
Seclusion refers to isolating a person in a locked room Restraints are human or mechanical measures that use force or the threat of force to control someonersquos actions ldquoTake downsrdquolowast holding someone face-down in a prone position strait jackets or tying someone by hands and feet are all examples of restraints Chemical restraints are medications that are not otherwise necessary and that are used to control someonersquos behavior
The Harvard Center for Risk Analysis has estimated that deaths and injuries from seclusion and restraints are significantly under-reported Its study of the prevalence of seclusion and restraint-related deaths statistically estimated that between 50 and 150 deaths occur nationally each year because of SR use on psychiatric and substance-abuse patients18
A national impetus for reform was triggered by incidents reported by the Courant and other sources
lowast A ldquotake downrdquo is a technique to force an uncooperative person to the floor to place him or her in restraints At least five staff surround the patient each taking the head an arm or leg and force him or her down Injury to the patient often occurs if staff sit on the person while restraints are secured This technique is frequently violent causing significant patient and staff injuries
- 5 -
Seclusion and Restraints A Failure Not a Treatment
diams Gloria Huntley 31 years old died in Central State Hospital in Petersburg Virginia after having been kept in restraints for 558 hours during the last two months of her life Although she had been diagnosed with asthma and epilepsy she was nevertheless restrained over and over again because of angry outbursts at hospital staff (Hartford Courant 1998)
diams Sixteen-year-old Tristan Sovern died in Charter Greensboro in North Carolina in 1998 after he was placed in restraints as ldquopunishmentrdquo for leaving a group-therapy session In response to his screams of ldquoYoursquore choking me I canrsquot breatherdquo a towel was shoved over Tristanrsquos mouth (60 Minutes II 1999)
diams Here in California Kristal Mayon-Ceniceros age 16 died of respiratory arrest in New Alternatives a private Chula Visa residential-care facility She died after being restrained face-down on the floor by four staff members (Associated Press 1999)
diams Also in California Rick Griffin 36 of Stockton died of cardio-respiratory failure and extreme agitation in the San Joaquin County Psychiatric Health Facility He had been wrestled to the floor by eight staff members and bound in leather restraints (The Stockton Record 1998)
diams Andrew McClain was 11 years old and weighed 96 pounds when two aides at the Elmcrest psychiatric hospital in Portland Connecticut sat on his back and crushed him to death His offense Refusing to move to another breakfast table (Lieberman Dodd and De Lauro 1999)
diams Edith Campos 15 suffocated while being held face-down after resisting an aide at the Desert Hills Center for Youth and Families in Tucson Arizona She was subjected to restraints after refusing to hand over an ldquounauthorizedrdquo personal item The item was a family photograph (Lieberman Dodd and De Lauro 1999)
Initial Response
The Courant series sparked congressional hearings into SR policies and how people have been traumatized injured and killed as a result of these practices Congressional leaders responded with federal reform proposals In a series of high-profile hearings
- 6 -
Seclusion and Restraints A Failure Not a Treatment
deaths injuries and abuses resulting from seclusion and restraints were exposed
Unfortunately these are not isolated incidents They are but a few of scores of cases in which mental health patients ndash a disproportionate number of them children ndash died barbaric deaths more suited to medieval torture chambers than to late 20th century America They died because of the improper use of seclusion and physical or chemical restraints They died at the hands of the very people who were supposed to protect them
- Senator Lieberman Senator Dodd and Representative DeLauro July 16 1999
The National Alliance for the Mentally Ill (NAMI) also has tracked reports of recent and past SR abuses (Appendix 2) NAMI reported over 25 new incidents nationwide of deaths injuries and traumas caused by seclusion and restraints after the Courant survey Currently there is no official tracking of injury or trauma to patients or to staff in California NAMI however reported numerous incidents of serious injury ndash patients who became comatose who suffered broken bones were hit in the face bruised needed stitches or were bleeding as a result of restraints19
Equally troubling is the humiliation and trauma NAMI documents such as its many reports of patients unable to use the bathroom and left for hours in their own bodily wastes One patient was restrained for rejecting medication because she still hoped to nurse her young child another was placed in restraints because he couldnrsquot stop crying A 12-year-old was placed in a straightjacket in the middle of the floor where everyone could watch her ndash and staff called this a ldquoburritordquo A patient who voluntarily admitted herself to a hospital found herself reliving former traumatic experiences
Suddenly the guard had a huge pair of leather cuffs with padlocks on them All I knew was that I was being strapped down to a bed by a strange man with a gun This is not good therapy for a rape victim All I could do was close my eyes and pretend this wasnrsquot happening to me20
The US General Accounting Office (GAO) in an October 1999 report on improper seclusion and restraints validated the notion that patients may be severely traumatized while being restrained
- 7 -
Seclusion and Restraints A Failure Not a Treatment
even if no physical injuries are sustained ldquo Research indicates that at least half of all women treated in psychiatric settings have a history of physical or sexual abuserdquo21
Citing a Massachusetts state task force on the topic the GAO stated that the use of restraints on patients who have been abused often results in their re-experiencing their traumas and contributes to a setback in the course of treatment
Congress adopted reforms to federal policies administered by the US Centers for Medicare and Medicaid Services (CMS formerly HCFA) in 1999 In addition the Joint Commission on Accreditation of Healthcare Organizations has adopted new policies The recently enacted Childrenrsquos Healthcare Act of 2000 was the third major federal reform Explained more fully in Part II of this report these new policies are intended to restrict and reduce SR practices
Despite these reforms the federally mandated advocate organization Protection and Advocacy reports that 14 Californians have died and one has beenen permanently injured (in a persistent coma) while in seclusion or behavioral restraints since the new CMS rules were put into place in July 1999 Since there is no official requirement for reporting nonfatal injuries we cannot officially confirm the types of injuries documented by NAMI the news media and the GAO
Californiarsquos standards governing SR practice are different for each kind of facility State hospitals general acute care hospitals psychiatric health facilities skilled nursing facilities ndash all are facilities that utilize SR However each type of facility is governed by a different set of state regulations For example
General Acute Care Hospitals ndash In a case of emergency SR can be initiated at the discretion of a registered nurse and a verbal or written order obtained from a physician afterwards If a verbal order is obtained it shall be signed by the physician on his next visit Orders for SR may be for longer than 24 hours
Psychiatric Health Facilities ndash In an emergency a physicianrsquos order can be received over the telephone within one hour of initiating SR and must be signed in person within 24 hours Orders for SR may be in force for no longer than 24 hours
Skilled Nursing Facilities with Special Treatment Programs ndash A physician may give the order for SR by telephone and sign it in
- 8 -
Seclusion and Restraints A Failure Not a Treatment
person within five days The order expires and must be renewed each 24 hours to keep a person in SR
Each facilityrsquos standards differ from the others and on this particular issue none is as stringent as the federal standard Californiarsquos regulatory standards and some of the problems associated with them are discussed more fully under ldquoPatchwork Oversightrdquo on page 15
Scope of Report
This report focuses on issues of psychiatric seclusion and restraints It does not address issues of medical restraints such as immobilizing a person for a surgical procedure or placing a personrsquos arm in a ldquosleeverdquo to prevent removing an intravenous needle Nor does it address the important issues of SR policies in schools or facilities for the developmentally disabled or in correctional facilities for youths or adults It is limited in scope to policies of psychiatric seclusion and restraints in mental health facilities
The Pennsylvania Experience
Seclusion and restraints have been used to control the behavior of psychiatric patients since the Middle Ages22 However these techniques have also involved high risk of patient injury and death Pennsylvania has been a leader in trying to change this culture and working to reduce and ultimately eliminate the use of seclusion and restraints in its nine state hospitals
The Pennsylvania Office of Mental Health and Substance Abuse Services implemented its program because
hellipthese measures [SR] do not alleviate human suffering or psychiatric symptoms do not alter behavior and have frequently resulted in patient and staff injury emotional trauma and patient death23
Expert testimony at hearings of the Joint Commission on Accreditation of Healthcare Organizations also called attention to the counter-therapeutic aspects of SR
The attempt to impose ldquotreatmentrdquo by force is always counterproductive ndash creating humiliation resentment and resistance to further treatment that might be more helpful24
- 9 -
Seclusion and Restraints A Failure Not a Treatment
In practice seclusion and restraints are sometimes imposed on psychiatric patients for reasons that are not therapeutic These uses of SR have been discredited and are illegal under current law however they persist SR practices are sometimes used to
diams Control the environment ndash To curtail a patientrsquos movement to compensate for having inadequate staff on the ward or to avoid providing appropriate clinical interventions
diams Coerce ndash To force a patient to comply with the staffrsquos wishes or
diams Punish ndash To impose penalties on patient behaviors
NAMI has been a leader in the effort to end SR on these terms Its position is that restraints and seclusion have no therapeutic value and therefore they are not a ldquotreatmentrdquo NAMI asserts that SR are dangerous interventions and should be used only in cases of extreme emergency when someonersquos physical safety is in jeopardy and then only with careful safeguards25
The idea that psychiatric patients are treated with brutality are seriously injured or even killed in this day and age may be difficult to believe But the Courant investigation the Harvard Center for Risk Analysis and NAMIrsquos report all demonstrate that these practices continue to exist placing psychiatric patients at risk of trauma injury and even death In the most egregious cases where someone has died the causes of death are frequently violent asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdose drug interactions and choking26
These are our most vulnerable citizens Since they are often held against their will supposedly for their own well being it would be incumbent upon the state to protect them from being injured traumatized and abused
To address that responsibility this paper examines three critical issues
1) Seclusion and restraints policies have received national attention and have been the focus of three successive initiatives of federal reform Is that enough
2) Californiarsquos oversight of seclusion and restraints is a patchwork quilt of confusing bureaucracy that impedes accountability and progress Can it be improved
- 10 -
Seclusion and Restraints A Failure Not a Treatment
3) Other states have taken action to improve seclusion and restraints policies on the state level Most notably Pennsylvania has developed a model that garnered the Harvard Innovations in American Government Award and reduced hours of seclusion and restraints by 96 percent in its state hospitals Can California benefit from model practices developed in Pennsylvania
- 11 -
Seclusion and Restraints A Failure Not a Treatment
Part II
Federal Reforms and State Impacts
New Federal Regulations Three Layers of Reform
In response to the Hartford Courant series and the vigorous lobbying of NAMI federal actions to revise national policy on seclusion and restraints were proposed and implemented Reform came in three successive initiatives
diams First the US Centers for Medicare and Medicaid Services (CMS) issued new interim rules for Medicare and Medicaid hospitals in July of 1999
diams Next the Joint Commission on Accreditation of Healthcare Organizations released revised seclusion and restraints standards that took effect January 1 2001
diams Most recently on May 22 last year CMS issued Interim Final Rules under the Childrenrsquos Health Act of 2000 setting forth new regulations for psychiatric facilities that receive federal funds and for ldquononmedical community-based facilities for children and youthrdquo
First Reform CMS Breaks New Ground
CMS set forth interim final rules as of July 1999 that revised seclusion and restraints standards in any hospital that receives Medicare or Medicaid financing
The preamble to the rules broke new ground by declaring ldquoThe patientrsquos right to be free from restraints is paramountrdquo27 The rules stated that SR may only be used in emergency situations if needed to ensure the patientrsquos physical safety and when less-restrictive alternatives have been determined ineffective and that
- 12 -
Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
Other states have imposed new restrictions in their SR policies Most notably Pennsylvania has developed an award-winning model that reduced overall incidents of seclusion and restraint by 74 percent and reduced the hours that patients spent in SR by 96 percent over a three-year period13
The Pennsylvania reforms were accomplished with no additional staff or funds and no increase in injuries to staff14 Charles Curie then deputy secretary of Pennsylvaniarsquos mental health and substance abuse services15 articulated a new philosophy of care that became the basis for a comprehensive change of culture in Pennsylvaniarsquos state hospital system ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo16
Pennsylvaniarsquos first step was to institute a mandated and publicly accountable system of tracking seclusion and restraints The state developed system-wide policies that required training diffusion of conflict accountability for using SR awards and recognition for reducing its use cultural competence a prohibition on all chemical restraints a prohibition on using SR on voluntary patients and debriefings with patients families and staff after each incident Central to these reforms was the core concept that seclusion and restraints are not treatment ndash they reflect a treatment failure and should be handled as such to prevent the escalation of violence This commitment has radically changed the longstanding culture environment and level of violence in Pennsylvaniarsquos nine state hospitals
This analysis determines that Californiarsquos piecemeal regulatory system could benefit from practices similar to those developed in Pennsylvania
Findings and Options
The new federal reforms that govern SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to accountability in the use of SR in California facilities
diams A lack of uniform statewide standards across various types of facilities and
diams A lack of mandatory consistent and publicly accessible reporting on the use and consequences of SR These include deaths serious injuries frequency and duration of SR and
- 3 -
Seclusion and Restraints A Failure Not a Treatment
related conditions and situations such as airway obstructions patient falls staff injuries and medication errors
Private psychiatric hospitals may be the most difficult to regulate The US inspector general found in August 2000 that private facilities may be the least likely to comply with the 1999 federal SR regulations and therefore may be the most in need of uniform state standards and enforcement17
There is compelling evidence in the Pennsylvania experience that SR can be dramatically reduced with a change of organizational values and culture
The following steps could be taken with a goal of reducing SR practices and the injuries deaths and traumas that can result from them
diams California could develop uniform seclusion and restraint standards that match if not exceed the highest federal regulations to cover all facilities ndash private as well as public ndash that treat people with psychiatric disabilities Federal standards vary based on licensing and accreditation while state standards vary based on type of facility The experience of other states has shown that a high uniform state standard improves the quality of enforcement and compliance
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to safely and cost-effectively reduce the use of SR in California
- 4 -
Seclusion and Restraints A Failure Not a Treatment
Part I
Seclusion and Restraints Issues and Actions
The issue of seclusion and restraint of psychiatric and substance-abuse patients gained national notoriety in October of 1998 when the Hartford Courant published a five-part investigative series entitled ldquoDeadly Restraintrdquo The Courant conducted a national survey that documented 142 deaths in the past decade that were directly connected to the use of seclusion or physical restraints (Appendix 1)
Seclusion refers to isolating a person in a locked room Restraints are human or mechanical measures that use force or the threat of force to control someonersquos actions ldquoTake downsrdquolowast holding someone face-down in a prone position strait jackets or tying someone by hands and feet are all examples of restraints Chemical restraints are medications that are not otherwise necessary and that are used to control someonersquos behavior
The Harvard Center for Risk Analysis has estimated that deaths and injuries from seclusion and restraints are significantly under-reported Its study of the prevalence of seclusion and restraint-related deaths statistically estimated that between 50 and 150 deaths occur nationally each year because of SR use on psychiatric and substance-abuse patients18
A national impetus for reform was triggered by incidents reported by the Courant and other sources
lowast A ldquotake downrdquo is a technique to force an uncooperative person to the floor to place him or her in restraints At least five staff surround the patient each taking the head an arm or leg and force him or her down Injury to the patient often occurs if staff sit on the person while restraints are secured This technique is frequently violent causing significant patient and staff injuries
- 5 -
Seclusion and Restraints A Failure Not a Treatment
diams Gloria Huntley 31 years old died in Central State Hospital in Petersburg Virginia after having been kept in restraints for 558 hours during the last two months of her life Although she had been diagnosed with asthma and epilepsy she was nevertheless restrained over and over again because of angry outbursts at hospital staff (Hartford Courant 1998)
diams Sixteen-year-old Tristan Sovern died in Charter Greensboro in North Carolina in 1998 after he was placed in restraints as ldquopunishmentrdquo for leaving a group-therapy session In response to his screams of ldquoYoursquore choking me I canrsquot breatherdquo a towel was shoved over Tristanrsquos mouth (60 Minutes II 1999)
diams Here in California Kristal Mayon-Ceniceros age 16 died of respiratory arrest in New Alternatives a private Chula Visa residential-care facility She died after being restrained face-down on the floor by four staff members (Associated Press 1999)
diams Also in California Rick Griffin 36 of Stockton died of cardio-respiratory failure and extreme agitation in the San Joaquin County Psychiatric Health Facility He had been wrestled to the floor by eight staff members and bound in leather restraints (The Stockton Record 1998)
diams Andrew McClain was 11 years old and weighed 96 pounds when two aides at the Elmcrest psychiatric hospital in Portland Connecticut sat on his back and crushed him to death His offense Refusing to move to another breakfast table (Lieberman Dodd and De Lauro 1999)
diams Edith Campos 15 suffocated while being held face-down after resisting an aide at the Desert Hills Center for Youth and Families in Tucson Arizona She was subjected to restraints after refusing to hand over an ldquounauthorizedrdquo personal item The item was a family photograph (Lieberman Dodd and De Lauro 1999)
Initial Response
The Courant series sparked congressional hearings into SR policies and how people have been traumatized injured and killed as a result of these practices Congressional leaders responded with federal reform proposals In a series of high-profile hearings
- 6 -
Seclusion and Restraints A Failure Not a Treatment
deaths injuries and abuses resulting from seclusion and restraints were exposed
Unfortunately these are not isolated incidents They are but a few of scores of cases in which mental health patients ndash a disproportionate number of them children ndash died barbaric deaths more suited to medieval torture chambers than to late 20th century America They died because of the improper use of seclusion and physical or chemical restraints They died at the hands of the very people who were supposed to protect them
- Senator Lieberman Senator Dodd and Representative DeLauro July 16 1999
The National Alliance for the Mentally Ill (NAMI) also has tracked reports of recent and past SR abuses (Appendix 2) NAMI reported over 25 new incidents nationwide of deaths injuries and traumas caused by seclusion and restraints after the Courant survey Currently there is no official tracking of injury or trauma to patients or to staff in California NAMI however reported numerous incidents of serious injury ndash patients who became comatose who suffered broken bones were hit in the face bruised needed stitches or were bleeding as a result of restraints19
Equally troubling is the humiliation and trauma NAMI documents such as its many reports of patients unable to use the bathroom and left for hours in their own bodily wastes One patient was restrained for rejecting medication because she still hoped to nurse her young child another was placed in restraints because he couldnrsquot stop crying A 12-year-old was placed in a straightjacket in the middle of the floor where everyone could watch her ndash and staff called this a ldquoburritordquo A patient who voluntarily admitted herself to a hospital found herself reliving former traumatic experiences
Suddenly the guard had a huge pair of leather cuffs with padlocks on them All I knew was that I was being strapped down to a bed by a strange man with a gun This is not good therapy for a rape victim All I could do was close my eyes and pretend this wasnrsquot happening to me20
The US General Accounting Office (GAO) in an October 1999 report on improper seclusion and restraints validated the notion that patients may be severely traumatized while being restrained
- 7 -
Seclusion and Restraints A Failure Not a Treatment
even if no physical injuries are sustained ldquo Research indicates that at least half of all women treated in psychiatric settings have a history of physical or sexual abuserdquo21
Citing a Massachusetts state task force on the topic the GAO stated that the use of restraints on patients who have been abused often results in their re-experiencing their traumas and contributes to a setback in the course of treatment
Congress adopted reforms to federal policies administered by the US Centers for Medicare and Medicaid Services (CMS formerly HCFA) in 1999 In addition the Joint Commission on Accreditation of Healthcare Organizations has adopted new policies The recently enacted Childrenrsquos Healthcare Act of 2000 was the third major federal reform Explained more fully in Part II of this report these new policies are intended to restrict and reduce SR practices
Despite these reforms the federally mandated advocate organization Protection and Advocacy reports that 14 Californians have died and one has beenen permanently injured (in a persistent coma) while in seclusion or behavioral restraints since the new CMS rules were put into place in July 1999 Since there is no official requirement for reporting nonfatal injuries we cannot officially confirm the types of injuries documented by NAMI the news media and the GAO
Californiarsquos standards governing SR practice are different for each kind of facility State hospitals general acute care hospitals psychiatric health facilities skilled nursing facilities ndash all are facilities that utilize SR However each type of facility is governed by a different set of state regulations For example
General Acute Care Hospitals ndash In a case of emergency SR can be initiated at the discretion of a registered nurse and a verbal or written order obtained from a physician afterwards If a verbal order is obtained it shall be signed by the physician on his next visit Orders for SR may be for longer than 24 hours
Psychiatric Health Facilities ndash In an emergency a physicianrsquos order can be received over the telephone within one hour of initiating SR and must be signed in person within 24 hours Orders for SR may be in force for no longer than 24 hours
Skilled Nursing Facilities with Special Treatment Programs ndash A physician may give the order for SR by telephone and sign it in
- 8 -
Seclusion and Restraints A Failure Not a Treatment
person within five days The order expires and must be renewed each 24 hours to keep a person in SR
Each facilityrsquos standards differ from the others and on this particular issue none is as stringent as the federal standard Californiarsquos regulatory standards and some of the problems associated with them are discussed more fully under ldquoPatchwork Oversightrdquo on page 15
Scope of Report
This report focuses on issues of psychiatric seclusion and restraints It does not address issues of medical restraints such as immobilizing a person for a surgical procedure or placing a personrsquos arm in a ldquosleeverdquo to prevent removing an intravenous needle Nor does it address the important issues of SR policies in schools or facilities for the developmentally disabled or in correctional facilities for youths or adults It is limited in scope to policies of psychiatric seclusion and restraints in mental health facilities
The Pennsylvania Experience
Seclusion and restraints have been used to control the behavior of psychiatric patients since the Middle Ages22 However these techniques have also involved high risk of patient injury and death Pennsylvania has been a leader in trying to change this culture and working to reduce and ultimately eliminate the use of seclusion and restraints in its nine state hospitals
The Pennsylvania Office of Mental Health and Substance Abuse Services implemented its program because
hellipthese measures [SR] do not alleviate human suffering or psychiatric symptoms do not alter behavior and have frequently resulted in patient and staff injury emotional trauma and patient death23
Expert testimony at hearings of the Joint Commission on Accreditation of Healthcare Organizations also called attention to the counter-therapeutic aspects of SR
The attempt to impose ldquotreatmentrdquo by force is always counterproductive ndash creating humiliation resentment and resistance to further treatment that might be more helpful24
- 9 -
Seclusion and Restraints A Failure Not a Treatment
In practice seclusion and restraints are sometimes imposed on psychiatric patients for reasons that are not therapeutic These uses of SR have been discredited and are illegal under current law however they persist SR practices are sometimes used to
diams Control the environment ndash To curtail a patientrsquos movement to compensate for having inadequate staff on the ward or to avoid providing appropriate clinical interventions
diams Coerce ndash To force a patient to comply with the staffrsquos wishes or
diams Punish ndash To impose penalties on patient behaviors
NAMI has been a leader in the effort to end SR on these terms Its position is that restraints and seclusion have no therapeutic value and therefore they are not a ldquotreatmentrdquo NAMI asserts that SR are dangerous interventions and should be used only in cases of extreme emergency when someonersquos physical safety is in jeopardy and then only with careful safeguards25
The idea that psychiatric patients are treated with brutality are seriously injured or even killed in this day and age may be difficult to believe But the Courant investigation the Harvard Center for Risk Analysis and NAMIrsquos report all demonstrate that these practices continue to exist placing psychiatric patients at risk of trauma injury and even death In the most egregious cases where someone has died the causes of death are frequently violent asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdose drug interactions and choking26
These are our most vulnerable citizens Since they are often held against their will supposedly for their own well being it would be incumbent upon the state to protect them from being injured traumatized and abused
To address that responsibility this paper examines three critical issues
1) Seclusion and restraints policies have received national attention and have been the focus of three successive initiatives of federal reform Is that enough
2) Californiarsquos oversight of seclusion and restraints is a patchwork quilt of confusing bureaucracy that impedes accountability and progress Can it be improved
- 10 -
Seclusion and Restraints A Failure Not a Treatment
3) Other states have taken action to improve seclusion and restraints policies on the state level Most notably Pennsylvania has developed a model that garnered the Harvard Innovations in American Government Award and reduced hours of seclusion and restraints by 96 percent in its state hospitals Can California benefit from model practices developed in Pennsylvania
- 11 -
Seclusion and Restraints A Failure Not a Treatment
Part II
Federal Reforms and State Impacts
New Federal Regulations Three Layers of Reform
In response to the Hartford Courant series and the vigorous lobbying of NAMI federal actions to revise national policy on seclusion and restraints were proposed and implemented Reform came in three successive initiatives
diams First the US Centers for Medicare and Medicaid Services (CMS) issued new interim rules for Medicare and Medicaid hospitals in July of 1999
diams Next the Joint Commission on Accreditation of Healthcare Organizations released revised seclusion and restraints standards that took effect January 1 2001
diams Most recently on May 22 last year CMS issued Interim Final Rules under the Childrenrsquos Health Act of 2000 setting forth new regulations for psychiatric facilities that receive federal funds and for ldquononmedical community-based facilities for children and youthrdquo
First Reform CMS Breaks New Ground
CMS set forth interim final rules as of July 1999 that revised seclusion and restraints standards in any hospital that receives Medicare or Medicaid financing
The preamble to the rules broke new ground by declaring ldquoThe patientrsquos right to be free from restraints is paramountrdquo27 The rules stated that SR may only be used in emergency situations if needed to ensure the patientrsquos physical safety and when less-restrictive alternatives have been determined ineffective and that
- 12 -
Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
related conditions and situations such as airway obstructions patient falls staff injuries and medication errors
Private psychiatric hospitals may be the most difficult to regulate The US inspector general found in August 2000 that private facilities may be the least likely to comply with the 1999 federal SR regulations and therefore may be the most in need of uniform state standards and enforcement17
There is compelling evidence in the Pennsylvania experience that SR can be dramatically reduced with a change of organizational values and culture
The following steps could be taken with a goal of reducing SR practices and the injuries deaths and traumas that can result from them
diams California could develop uniform seclusion and restraint standards that match if not exceed the highest federal regulations to cover all facilities ndash private as well as public ndash that treat people with psychiatric disabilities Federal standards vary based on licensing and accreditation while state standards vary based on type of facility The experience of other states has shown that a high uniform state standard improves the quality of enforcement and compliance
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to safely and cost-effectively reduce the use of SR in California
- 4 -
Seclusion and Restraints A Failure Not a Treatment
Part I
Seclusion and Restraints Issues and Actions
The issue of seclusion and restraint of psychiatric and substance-abuse patients gained national notoriety in October of 1998 when the Hartford Courant published a five-part investigative series entitled ldquoDeadly Restraintrdquo The Courant conducted a national survey that documented 142 deaths in the past decade that were directly connected to the use of seclusion or physical restraints (Appendix 1)
Seclusion refers to isolating a person in a locked room Restraints are human or mechanical measures that use force or the threat of force to control someonersquos actions ldquoTake downsrdquolowast holding someone face-down in a prone position strait jackets or tying someone by hands and feet are all examples of restraints Chemical restraints are medications that are not otherwise necessary and that are used to control someonersquos behavior
The Harvard Center for Risk Analysis has estimated that deaths and injuries from seclusion and restraints are significantly under-reported Its study of the prevalence of seclusion and restraint-related deaths statistically estimated that between 50 and 150 deaths occur nationally each year because of SR use on psychiatric and substance-abuse patients18
A national impetus for reform was triggered by incidents reported by the Courant and other sources
lowast A ldquotake downrdquo is a technique to force an uncooperative person to the floor to place him or her in restraints At least five staff surround the patient each taking the head an arm or leg and force him or her down Injury to the patient often occurs if staff sit on the person while restraints are secured This technique is frequently violent causing significant patient and staff injuries
- 5 -
Seclusion and Restraints A Failure Not a Treatment
diams Gloria Huntley 31 years old died in Central State Hospital in Petersburg Virginia after having been kept in restraints for 558 hours during the last two months of her life Although she had been diagnosed with asthma and epilepsy she was nevertheless restrained over and over again because of angry outbursts at hospital staff (Hartford Courant 1998)
diams Sixteen-year-old Tristan Sovern died in Charter Greensboro in North Carolina in 1998 after he was placed in restraints as ldquopunishmentrdquo for leaving a group-therapy session In response to his screams of ldquoYoursquore choking me I canrsquot breatherdquo a towel was shoved over Tristanrsquos mouth (60 Minutes II 1999)
diams Here in California Kristal Mayon-Ceniceros age 16 died of respiratory arrest in New Alternatives a private Chula Visa residential-care facility She died after being restrained face-down on the floor by four staff members (Associated Press 1999)
diams Also in California Rick Griffin 36 of Stockton died of cardio-respiratory failure and extreme agitation in the San Joaquin County Psychiatric Health Facility He had been wrestled to the floor by eight staff members and bound in leather restraints (The Stockton Record 1998)
diams Andrew McClain was 11 years old and weighed 96 pounds when two aides at the Elmcrest psychiatric hospital in Portland Connecticut sat on his back and crushed him to death His offense Refusing to move to another breakfast table (Lieberman Dodd and De Lauro 1999)
diams Edith Campos 15 suffocated while being held face-down after resisting an aide at the Desert Hills Center for Youth and Families in Tucson Arizona She was subjected to restraints after refusing to hand over an ldquounauthorizedrdquo personal item The item was a family photograph (Lieberman Dodd and De Lauro 1999)
Initial Response
The Courant series sparked congressional hearings into SR policies and how people have been traumatized injured and killed as a result of these practices Congressional leaders responded with federal reform proposals In a series of high-profile hearings
- 6 -
Seclusion and Restraints A Failure Not a Treatment
deaths injuries and abuses resulting from seclusion and restraints were exposed
Unfortunately these are not isolated incidents They are but a few of scores of cases in which mental health patients ndash a disproportionate number of them children ndash died barbaric deaths more suited to medieval torture chambers than to late 20th century America They died because of the improper use of seclusion and physical or chemical restraints They died at the hands of the very people who were supposed to protect them
- Senator Lieberman Senator Dodd and Representative DeLauro July 16 1999
The National Alliance for the Mentally Ill (NAMI) also has tracked reports of recent and past SR abuses (Appendix 2) NAMI reported over 25 new incidents nationwide of deaths injuries and traumas caused by seclusion and restraints after the Courant survey Currently there is no official tracking of injury or trauma to patients or to staff in California NAMI however reported numerous incidents of serious injury ndash patients who became comatose who suffered broken bones were hit in the face bruised needed stitches or were bleeding as a result of restraints19
Equally troubling is the humiliation and trauma NAMI documents such as its many reports of patients unable to use the bathroom and left for hours in their own bodily wastes One patient was restrained for rejecting medication because she still hoped to nurse her young child another was placed in restraints because he couldnrsquot stop crying A 12-year-old was placed in a straightjacket in the middle of the floor where everyone could watch her ndash and staff called this a ldquoburritordquo A patient who voluntarily admitted herself to a hospital found herself reliving former traumatic experiences
Suddenly the guard had a huge pair of leather cuffs with padlocks on them All I knew was that I was being strapped down to a bed by a strange man with a gun This is not good therapy for a rape victim All I could do was close my eyes and pretend this wasnrsquot happening to me20
The US General Accounting Office (GAO) in an October 1999 report on improper seclusion and restraints validated the notion that patients may be severely traumatized while being restrained
- 7 -
Seclusion and Restraints A Failure Not a Treatment
even if no physical injuries are sustained ldquo Research indicates that at least half of all women treated in psychiatric settings have a history of physical or sexual abuserdquo21
Citing a Massachusetts state task force on the topic the GAO stated that the use of restraints on patients who have been abused often results in their re-experiencing their traumas and contributes to a setback in the course of treatment
Congress adopted reforms to federal policies administered by the US Centers for Medicare and Medicaid Services (CMS formerly HCFA) in 1999 In addition the Joint Commission on Accreditation of Healthcare Organizations has adopted new policies The recently enacted Childrenrsquos Healthcare Act of 2000 was the third major federal reform Explained more fully in Part II of this report these new policies are intended to restrict and reduce SR practices
Despite these reforms the federally mandated advocate organization Protection and Advocacy reports that 14 Californians have died and one has beenen permanently injured (in a persistent coma) while in seclusion or behavioral restraints since the new CMS rules were put into place in July 1999 Since there is no official requirement for reporting nonfatal injuries we cannot officially confirm the types of injuries documented by NAMI the news media and the GAO
Californiarsquos standards governing SR practice are different for each kind of facility State hospitals general acute care hospitals psychiatric health facilities skilled nursing facilities ndash all are facilities that utilize SR However each type of facility is governed by a different set of state regulations For example
General Acute Care Hospitals ndash In a case of emergency SR can be initiated at the discretion of a registered nurse and a verbal or written order obtained from a physician afterwards If a verbal order is obtained it shall be signed by the physician on his next visit Orders for SR may be for longer than 24 hours
Psychiatric Health Facilities ndash In an emergency a physicianrsquos order can be received over the telephone within one hour of initiating SR and must be signed in person within 24 hours Orders for SR may be in force for no longer than 24 hours
Skilled Nursing Facilities with Special Treatment Programs ndash A physician may give the order for SR by telephone and sign it in
- 8 -
Seclusion and Restraints A Failure Not a Treatment
person within five days The order expires and must be renewed each 24 hours to keep a person in SR
Each facilityrsquos standards differ from the others and on this particular issue none is as stringent as the federal standard Californiarsquos regulatory standards and some of the problems associated with them are discussed more fully under ldquoPatchwork Oversightrdquo on page 15
Scope of Report
This report focuses on issues of psychiatric seclusion and restraints It does not address issues of medical restraints such as immobilizing a person for a surgical procedure or placing a personrsquos arm in a ldquosleeverdquo to prevent removing an intravenous needle Nor does it address the important issues of SR policies in schools or facilities for the developmentally disabled or in correctional facilities for youths or adults It is limited in scope to policies of psychiatric seclusion and restraints in mental health facilities
The Pennsylvania Experience
Seclusion and restraints have been used to control the behavior of psychiatric patients since the Middle Ages22 However these techniques have also involved high risk of patient injury and death Pennsylvania has been a leader in trying to change this culture and working to reduce and ultimately eliminate the use of seclusion and restraints in its nine state hospitals
The Pennsylvania Office of Mental Health and Substance Abuse Services implemented its program because
hellipthese measures [SR] do not alleviate human suffering or psychiatric symptoms do not alter behavior and have frequently resulted in patient and staff injury emotional trauma and patient death23
Expert testimony at hearings of the Joint Commission on Accreditation of Healthcare Organizations also called attention to the counter-therapeutic aspects of SR
The attempt to impose ldquotreatmentrdquo by force is always counterproductive ndash creating humiliation resentment and resistance to further treatment that might be more helpful24
- 9 -
Seclusion and Restraints A Failure Not a Treatment
In practice seclusion and restraints are sometimes imposed on psychiatric patients for reasons that are not therapeutic These uses of SR have been discredited and are illegal under current law however they persist SR practices are sometimes used to
diams Control the environment ndash To curtail a patientrsquos movement to compensate for having inadequate staff on the ward or to avoid providing appropriate clinical interventions
diams Coerce ndash To force a patient to comply with the staffrsquos wishes or
diams Punish ndash To impose penalties on patient behaviors
NAMI has been a leader in the effort to end SR on these terms Its position is that restraints and seclusion have no therapeutic value and therefore they are not a ldquotreatmentrdquo NAMI asserts that SR are dangerous interventions and should be used only in cases of extreme emergency when someonersquos physical safety is in jeopardy and then only with careful safeguards25
The idea that psychiatric patients are treated with brutality are seriously injured or even killed in this day and age may be difficult to believe But the Courant investigation the Harvard Center for Risk Analysis and NAMIrsquos report all demonstrate that these practices continue to exist placing psychiatric patients at risk of trauma injury and even death In the most egregious cases where someone has died the causes of death are frequently violent asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdose drug interactions and choking26
These are our most vulnerable citizens Since they are often held against their will supposedly for their own well being it would be incumbent upon the state to protect them from being injured traumatized and abused
To address that responsibility this paper examines three critical issues
1) Seclusion and restraints policies have received national attention and have been the focus of three successive initiatives of federal reform Is that enough
2) Californiarsquos oversight of seclusion and restraints is a patchwork quilt of confusing bureaucracy that impedes accountability and progress Can it be improved
- 10 -
Seclusion and Restraints A Failure Not a Treatment
3) Other states have taken action to improve seclusion and restraints policies on the state level Most notably Pennsylvania has developed a model that garnered the Harvard Innovations in American Government Award and reduced hours of seclusion and restraints by 96 percent in its state hospitals Can California benefit from model practices developed in Pennsylvania
- 11 -
Seclusion and Restraints A Failure Not a Treatment
Part II
Federal Reforms and State Impacts
New Federal Regulations Three Layers of Reform
In response to the Hartford Courant series and the vigorous lobbying of NAMI federal actions to revise national policy on seclusion and restraints were proposed and implemented Reform came in three successive initiatives
diams First the US Centers for Medicare and Medicaid Services (CMS) issued new interim rules for Medicare and Medicaid hospitals in July of 1999
diams Next the Joint Commission on Accreditation of Healthcare Organizations released revised seclusion and restraints standards that took effect January 1 2001
diams Most recently on May 22 last year CMS issued Interim Final Rules under the Childrenrsquos Health Act of 2000 setting forth new regulations for psychiatric facilities that receive federal funds and for ldquononmedical community-based facilities for children and youthrdquo
First Reform CMS Breaks New Ground
CMS set forth interim final rules as of July 1999 that revised seclusion and restraints standards in any hospital that receives Medicare or Medicaid financing
The preamble to the rules broke new ground by declaring ldquoThe patientrsquos right to be free from restraints is paramountrdquo27 The rules stated that SR may only be used in emergency situations if needed to ensure the patientrsquos physical safety and when less-restrictive alternatives have been determined ineffective and that
- 12 -
Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
Part I
Seclusion and Restraints Issues and Actions
The issue of seclusion and restraint of psychiatric and substance-abuse patients gained national notoriety in October of 1998 when the Hartford Courant published a five-part investigative series entitled ldquoDeadly Restraintrdquo The Courant conducted a national survey that documented 142 deaths in the past decade that were directly connected to the use of seclusion or physical restraints (Appendix 1)
Seclusion refers to isolating a person in a locked room Restraints are human or mechanical measures that use force or the threat of force to control someonersquos actions ldquoTake downsrdquolowast holding someone face-down in a prone position strait jackets or tying someone by hands and feet are all examples of restraints Chemical restraints are medications that are not otherwise necessary and that are used to control someonersquos behavior
The Harvard Center for Risk Analysis has estimated that deaths and injuries from seclusion and restraints are significantly under-reported Its study of the prevalence of seclusion and restraint-related deaths statistically estimated that between 50 and 150 deaths occur nationally each year because of SR use on psychiatric and substance-abuse patients18
A national impetus for reform was triggered by incidents reported by the Courant and other sources
lowast A ldquotake downrdquo is a technique to force an uncooperative person to the floor to place him or her in restraints At least five staff surround the patient each taking the head an arm or leg and force him or her down Injury to the patient often occurs if staff sit on the person while restraints are secured This technique is frequently violent causing significant patient and staff injuries
- 5 -
Seclusion and Restraints A Failure Not a Treatment
diams Gloria Huntley 31 years old died in Central State Hospital in Petersburg Virginia after having been kept in restraints for 558 hours during the last two months of her life Although she had been diagnosed with asthma and epilepsy she was nevertheless restrained over and over again because of angry outbursts at hospital staff (Hartford Courant 1998)
diams Sixteen-year-old Tristan Sovern died in Charter Greensboro in North Carolina in 1998 after he was placed in restraints as ldquopunishmentrdquo for leaving a group-therapy session In response to his screams of ldquoYoursquore choking me I canrsquot breatherdquo a towel was shoved over Tristanrsquos mouth (60 Minutes II 1999)
diams Here in California Kristal Mayon-Ceniceros age 16 died of respiratory arrest in New Alternatives a private Chula Visa residential-care facility She died after being restrained face-down on the floor by four staff members (Associated Press 1999)
diams Also in California Rick Griffin 36 of Stockton died of cardio-respiratory failure and extreme agitation in the San Joaquin County Psychiatric Health Facility He had been wrestled to the floor by eight staff members and bound in leather restraints (The Stockton Record 1998)
diams Andrew McClain was 11 years old and weighed 96 pounds when two aides at the Elmcrest psychiatric hospital in Portland Connecticut sat on his back and crushed him to death His offense Refusing to move to another breakfast table (Lieberman Dodd and De Lauro 1999)
diams Edith Campos 15 suffocated while being held face-down after resisting an aide at the Desert Hills Center for Youth and Families in Tucson Arizona She was subjected to restraints after refusing to hand over an ldquounauthorizedrdquo personal item The item was a family photograph (Lieberman Dodd and De Lauro 1999)
Initial Response
The Courant series sparked congressional hearings into SR policies and how people have been traumatized injured and killed as a result of these practices Congressional leaders responded with federal reform proposals In a series of high-profile hearings
- 6 -
Seclusion and Restraints A Failure Not a Treatment
deaths injuries and abuses resulting from seclusion and restraints were exposed
Unfortunately these are not isolated incidents They are but a few of scores of cases in which mental health patients ndash a disproportionate number of them children ndash died barbaric deaths more suited to medieval torture chambers than to late 20th century America They died because of the improper use of seclusion and physical or chemical restraints They died at the hands of the very people who were supposed to protect them
- Senator Lieberman Senator Dodd and Representative DeLauro July 16 1999
The National Alliance for the Mentally Ill (NAMI) also has tracked reports of recent and past SR abuses (Appendix 2) NAMI reported over 25 new incidents nationwide of deaths injuries and traumas caused by seclusion and restraints after the Courant survey Currently there is no official tracking of injury or trauma to patients or to staff in California NAMI however reported numerous incidents of serious injury ndash patients who became comatose who suffered broken bones were hit in the face bruised needed stitches or were bleeding as a result of restraints19
Equally troubling is the humiliation and trauma NAMI documents such as its many reports of patients unable to use the bathroom and left for hours in their own bodily wastes One patient was restrained for rejecting medication because she still hoped to nurse her young child another was placed in restraints because he couldnrsquot stop crying A 12-year-old was placed in a straightjacket in the middle of the floor where everyone could watch her ndash and staff called this a ldquoburritordquo A patient who voluntarily admitted herself to a hospital found herself reliving former traumatic experiences
Suddenly the guard had a huge pair of leather cuffs with padlocks on them All I knew was that I was being strapped down to a bed by a strange man with a gun This is not good therapy for a rape victim All I could do was close my eyes and pretend this wasnrsquot happening to me20
The US General Accounting Office (GAO) in an October 1999 report on improper seclusion and restraints validated the notion that patients may be severely traumatized while being restrained
- 7 -
Seclusion and Restraints A Failure Not a Treatment
even if no physical injuries are sustained ldquo Research indicates that at least half of all women treated in psychiatric settings have a history of physical or sexual abuserdquo21
Citing a Massachusetts state task force on the topic the GAO stated that the use of restraints on patients who have been abused often results in their re-experiencing their traumas and contributes to a setback in the course of treatment
Congress adopted reforms to federal policies administered by the US Centers for Medicare and Medicaid Services (CMS formerly HCFA) in 1999 In addition the Joint Commission on Accreditation of Healthcare Organizations has adopted new policies The recently enacted Childrenrsquos Healthcare Act of 2000 was the third major federal reform Explained more fully in Part II of this report these new policies are intended to restrict and reduce SR practices
Despite these reforms the federally mandated advocate organization Protection and Advocacy reports that 14 Californians have died and one has beenen permanently injured (in a persistent coma) while in seclusion or behavioral restraints since the new CMS rules were put into place in July 1999 Since there is no official requirement for reporting nonfatal injuries we cannot officially confirm the types of injuries documented by NAMI the news media and the GAO
Californiarsquos standards governing SR practice are different for each kind of facility State hospitals general acute care hospitals psychiatric health facilities skilled nursing facilities ndash all are facilities that utilize SR However each type of facility is governed by a different set of state regulations For example
General Acute Care Hospitals ndash In a case of emergency SR can be initiated at the discretion of a registered nurse and a verbal or written order obtained from a physician afterwards If a verbal order is obtained it shall be signed by the physician on his next visit Orders for SR may be for longer than 24 hours
Psychiatric Health Facilities ndash In an emergency a physicianrsquos order can be received over the telephone within one hour of initiating SR and must be signed in person within 24 hours Orders for SR may be in force for no longer than 24 hours
Skilled Nursing Facilities with Special Treatment Programs ndash A physician may give the order for SR by telephone and sign it in
- 8 -
Seclusion and Restraints A Failure Not a Treatment
person within five days The order expires and must be renewed each 24 hours to keep a person in SR
Each facilityrsquos standards differ from the others and on this particular issue none is as stringent as the federal standard Californiarsquos regulatory standards and some of the problems associated with them are discussed more fully under ldquoPatchwork Oversightrdquo on page 15
Scope of Report
This report focuses on issues of psychiatric seclusion and restraints It does not address issues of medical restraints such as immobilizing a person for a surgical procedure or placing a personrsquos arm in a ldquosleeverdquo to prevent removing an intravenous needle Nor does it address the important issues of SR policies in schools or facilities for the developmentally disabled or in correctional facilities for youths or adults It is limited in scope to policies of psychiatric seclusion and restraints in mental health facilities
The Pennsylvania Experience
Seclusion and restraints have been used to control the behavior of psychiatric patients since the Middle Ages22 However these techniques have also involved high risk of patient injury and death Pennsylvania has been a leader in trying to change this culture and working to reduce and ultimately eliminate the use of seclusion and restraints in its nine state hospitals
The Pennsylvania Office of Mental Health and Substance Abuse Services implemented its program because
hellipthese measures [SR] do not alleviate human suffering or psychiatric symptoms do not alter behavior and have frequently resulted in patient and staff injury emotional trauma and patient death23
Expert testimony at hearings of the Joint Commission on Accreditation of Healthcare Organizations also called attention to the counter-therapeutic aspects of SR
The attempt to impose ldquotreatmentrdquo by force is always counterproductive ndash creating humiliation resentment and resistance to further treatment that might be more helpful24
- 9 -
Seclusion and Restraints A Failure Not a Treatment
In practice seclusion and restraints are sometimes imposed on psychiatric patients for reasons that are not therapeutic These uses of SR have been discredited and are illegal under current law however they persist SR practices are sometimes used to
diams Control the environment ndash To curtail a patientrsquos movement to compensate for having inadequate staff on the ward or to avoid providing appropriate clinical interventions
diams Coerce ndash To force a patient to comply with the staffrsquos wishes or
diams Punish ndash To impose penalties on patient behaviors
NAMI has been a leader in the effort to end SR on these terms Its position is that restraints and seclusion have no therapeutic value and therefore they are not a ldquotreatmentrdquo NAMI asserts that SR are dangerous interventions and should be used only in cases of extreme emergency when someonersquos physical safety is in jeopardy and then only with careful safeguards25
The idea that psychiatric patients are treated with brutality are seriously injured or even killed in this day and age may be difficult to believe But the Courant investigation the Harvard Center for Risk Analysis and NAMIrsquos report all demonstrate that these practices continue to exist placing psychiatric patients at risk of trauma injury and even death In the most egregious cases where someone has died the causes of death are frequently violent asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdose drug interactions and choking26
These are our most vulnerable citizens Since they are often held against their will supposedly for their own well being it would be incumbent upon the state to protect them from being injured traumatized and abused
To address that responsibility this paper examines three critical issues
1) Seclusion and restraints policies have received national attention and have been the focus of three successive initiatives of federal reform Is that enough
2) Californiarsquos oversight of seclusion and restraints is a patchwork quilt of confusing bureaucracy that impedes accountability and progress Can it be improved
- 10 -
Seclusion and Restraints A Failure Not a Treatment
3) Other states have taken action to improve seclusion and restraints policies on the state level Most notably Pennsylvania has developed a model that garnered the Harvard Innovations in American Government Award and reduced hours of seclusion and restraints by 96 percent in its state hospitals Can California benefit from model practices developed in Pennsylvania
- 11 -
Seclusion and Restraints A Failure Not a Treatment
Part II
Federal Reforms and State Impacts
New Federal Regulations Three Layers of Reform
In response to the Hartford Courant series and the vigorous lobbying of NAMI federal actions to revise national policy on seclusion and restraints were proposed and implemented Reform came in three successive initiatives
diams First the US Centers for Medicare and Medicaid Services (CMS) issued new interim rules for Medicare and Medicaid hospitals in July of 1999
diams Next the Joint Commission on Accreditation of Healthcare Organizations released revised seclusion and restraints standards that took effect January 1 2001
diams Most recently on May 22 last year CMS issued Interim Final Rules under the Childrenrsquos Health Act of 2000 setting forth new regulations for psychiatric facilities that receive federal funds and for ldquononmedical community-based facilities for children and youthrdquo
First Reform CMS Breaks New Ground
CMS set forth interim final rules as of July 1999 that revised seclusion and restraints standards in any hospital that receives Medicare or Medicaid financing
The preamble to the rules broke new ground by declaring ldquoThe patientrsquos right to be free from restraints is paramountrdquo27 The rules stated that SR may only be used in emergency situations if needed to ensure the patientrsquos physical safety and when less-restrictive alternatives have been determined ineffective and that
- 12 -
Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
diams Gloria Huntley 31 years old died in Central State Hospital in Petersburg Virginia after having been kept in restraints for 558 hours during the last two months of her life Although she had been diagnosed with asthma and epilepsy she was nevertheless restrained over and over again because of angry outbursts at hospital staff (Hartford Courant 1998)
diams Sixteen-year-old Tristan Sovern died in Charter Greensboro in North Carolina in 1998 after he was placed in restraints as ldquopunishmentrdquo for leaving a group-therapy session In response to his screams of ldquoYoursquore choking me I canrsquot breatherdquo a towel was shoved over Tristanrsquos mouth (60 Minutes II 1999)
diams Here in California Kristal Mayon-Ceniceros age 16 died of respiratory arrest in New Alternatives a private Chula Visa residential-care facility She died after being restrained face-down on the floor by four staff members (Associated Press 1999)
diams Also in California Rick Griffin 36 of Stockton died of cardio-respiratory failure and extreme agitation in the San Joaquin County Psychiatric Health Facility He had been wrestled to the floor by eight staff members and bound in leather restraints (The Stockton Record 1998)
diams Andrew McClain was 11 years old and weighed 96 pounds when two aides at the Elmcrest psychiatric hospital in Portland Connecticut sat on his back and crushed him to death His offense Refusing to move to another breakfast table (Lieberman Dodd and De Lauro 1999)
diams Edith Campos 15 suffocated while being held face-down after resisting an aide at the Desert Hills Center for Youth and Families in Tucson Arizona She was subjected to restraints after refusing to hand over an ldquounauthorizedrdquo personal item The item was a family photograph (Lieberman Dodd and De Lauro 1999)
Initial Response
The Courant series sparked congressional hearings into SR policies and how people have been traumatized injured and killed as a result of these practices Congressional leaders responded with federal reform proposals In a series of high-profile hearings
- 6 -
Seclusion and Restraints A Failure Not a Treatment
deaths injuries and abuses resulting from seclusion and restraints were exposed
Unfortunately these are not isolated incidents They are but a few of scores of cases in which mental health patients ndash a disproportionate number of them children ndash died barbaric deaths more suited to medieval torture chambers than to late 20th century America They died because of the improper use of seclusion and physical or chemical restraints They died at the hands of the very people who were supposed to protect them
- Senator Lieberman Senator Dodd and Representative DeLauro July 16 1999
The National Alliance for the Mentally Ill (NAMI) also has tracked reports of recent and past SR abuses (Appendix 2) NAMI reported over 25 new incidents nationwide of deaths injuries and traumas caused by seclusion and restraints after the Courant survey Currently there is no official tracking of injury or trauma to patients or to staff in California NAMI however reported numerous incidents of serious injury ndash patients who became comatose who suffered broken bones were hit in the face bruised needed stitches or were bleeding as a result of restraints19
Equally troubling is the humiliation and trauma NAMI documents such as its many reports of patients unable to use the bathroom and left for hours in their own bodily wastes One patient was restrained for rejecting medication because she still hoped to nurse her young child another was placed in restraints because he couldnrsquot stop crying A 12-year-old was placed in a straightjacket in the middle of the floor where everyone could watch her ndash and staff called this a ldquoburritordquo A patient who voluntarily admitted herself to a hospital found herself reliving former traumatic experiences
Suddenly the guard had a huge pair of leather cuffs with padlocks on them All I knew was that I was being strapped down to a bed by a strange man with a gun This is not good therapy for a rape victim All I could do was close my eyes and pretend this wasnrsquot happening to me20
The US General Accounting Office (GAO) in an October 1999 report on improper seclusion and restraints validated the notion that patients may be severely traumatized while being restrained
- 7 -
Seclusion and Restraints A Failure Not a Treatment
even if no physical injuries are sustained ldquo Research indicates that at least half of all women treated in psychiatric settings have a history of physical or sexual abuserdquo21
Citing a Massachusetts state task force on the topic the GAO stated that the use of restraints on patients who have been abused often results in their re-experiencing their traumas and contributes to a setback in the course of treatment
Congress adopted reforms to federal policies administered by the US Centers for Medicare and Medicaid Services (CMS formerly HCFA) in 1999 In addition the Joint Commission on Accreditation of Healthcare Organizations has adopted new policies The recently enacted Childrenrsquos Healthcare Act of 2000 was the third major federal reform Explained more fully in Part II of this report these new policies are intended to restrict and reduce SR practices
Despite these reforms the federally mandated advocate organization Protection and Advocacy reports that 14 Californians have died and one has beenen permanently injured (in a persistent coma) while in seclusion or behavioral restraints since the new CMS rules were put into place in July 1999 Since there is no official requirement for reporting nonfatal injuries we cannot officially confirm the types of injuries documented by NAMI the news media and the GAO
Californiarsquos standards governing SR practice are different for each kind of facility State hospitals general acute care hospitals psychiatric health facilities skilled nursing facilities ndash all are facilities that utilize SR However each type of facility is governed by a different set of state regulations For example
General Acute Care Hospitals ndash In a case of emergency SR can be initiated at the discretion of a registered nurse and a verbal or written order obtained from a physician afterwards If a verbal order is obtained it shall be signed by the physician on his next visit Orders for SR may be for longer than 24 hours
Psychiatric Health Facilities ndash In an emergency a physicianrsquos order can be received over the telephone within one hour of initiating SR and must be signed in person within 24 hours Orders for SR may be in force for no longer than 24 hours
Skilled Nursing Facilities with Special Treatment Programs ndash A physician may give the order for SR by telephone and sign it in
- 8 -
Seclusion and Restraints A Failure Not a Treatment
person within five days The order expires and must be renewed each 24 hours to keep a person in SR
Each facilityrsquos standards differ from the others and on this particular issue none is as stringent as the federal standard Californiarsquos regulatory standards and some of the problems associated with them are discussed more fully under ldquoPatchwork Oversightrdquo on page 15
Scope of Report
This report focuses on issues of psychiatric seclusion and restraints It does not address issues of medical restraints such as immobilizing a person for a surgical procedure or placing a personrsquos arm in a ldquosleeverdquo to prevent removing an intravenous needle Nor does it address the important issues of SR policies in schools or facilities for the developmentally disabled or in correctional facilities for youths or adults It is limited in scope to policies of psychiatric seclusion and restraints in mental health facilities
The Pennsylvania Experience
Seclusion and restraints have been used to control the behavior of psychiatric patients since the Middle Ages22 However these techniques have also involved high risk of patient injury and death Pennsylvania has been a leader in trying to change this culture and working to reduce and ultimately eliminate the use of seclusion and restraints in its nine state hospitals
The Pennsylvania Office of Mental Health and Substance Abuse Services implemented its program because
hellipthese measures [SR] do not alleviate human suffering or psychiatric symptoms do not alter behavior and have frequently resulted in patient and staff injury emotional trauma and patient death23
Expert testimony at hearings of the Joint Commission on Accreditation of Healthcare Organizations also called attention to the counter-therapeutic aspects of SR
The attempt to impose ldquotreatmentrdquo by force is always counterproductive ndash creating humiliation resentment and resistance to further treatment that might be more helpful24
- 9 -
Seclusion and Restraints A Failure Not a Treatment
In practice seclusion and restraints are sometimes imposed on psychiatric patients for reasons that are not therapeutic These uses of SR have been discredited and are illegal under current law however they persist SR practices are sometimes used to
diams Control the environment ndash To curtail a patientrsquos movement to compensate for having inadequate staff on the ward or to avoid providing appropriate clinical interventions
diams Coerce ndash To force a patient to comply with the staffrsquos wishes or
diams Punish ndash To impose penalties on patient behaviors
NAMI has been a leader in the effort to end SR on these terms Its position is that restraints and seclusion have no therapeutic value and therefore they are not a ldquotreatmentrdquo NAMI asserts that SR are dangerous interventions and should be used only in cases of extreme emergency when someonersquos physical safety is in jeopardy and then only with careful safeguards25
The idea that psychiatric patients are treated with brutality are seriously injured or even killed in this day and age may be difficult to believe But the Courant investigation the Harvard Center for Risk Analysis and NAMIrsquos report all demonstrate that these practices continue to exist placing psychiatric patients at risk of trauma injury and even death In the most egregious cases where someone has died the causes of death are frequently violent asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdose drug interactions and choking26
These are our most vulnerable citizens Since they are often held against their will supposedly for their own well being it would be incumbent upon the state to protect them from being injured traumatized and abused
To address that responsibility this paper examines three critical issues
1) Seclusion and restraints policies have received national attention and have been the focus of three successive initiatives of federal reform Is that enough
2) Californiarsquos oversight of seclusion and restraints is a patchwork quilt of confusing bureaucracy that impedes accountability and progress Can it be improved
- 10 -
Seclusion and Restraints A Failure Not a Treatment
3) Other states have taken action to improve seclusion and restraints policies on the state level Most notably Pennsylvania has developed a model that garnered the Harvard Innovations in American Government Award and reduced hours of seclusion and restraints by 96 percent in its state hospitals Can California benefit from model practices developed in Pennsylvania
- 11 -
Seclusion and Restraints A Failure Not a Treatment
Part II
Federal Reforms and State Impacts
New Federal Regulations Three Layers of Reform
In response to the Hartford Courant series and the vigorous lobbying of NAMI federal actions to revise national policy on seclusion and restraints were proposed and implemented Reform came in three successive initiatives
diams First the US Centers for Medicare and Medicaid Services (CMS) issued new interim rules for Medicare and Medicaid hospitals in July of 1999
diams Next the Joint Commission on Accreditation of Healthcare Organizations released revised seclusion and restraints standards that took effect January 1 2001
diams Most recently on May 22 last year CMS issued Interim Final Rules under the Childrenrsquos Health Act of 2000 setting forth new regulations for psychiatric facilities that receive federal funds and for ldquononmedical community-based facilities for children and youthrdquo
First Reform CMS Breaks New Ground
CMS set forth interim final rules as of July 1999 that revised seclusion and restraints standards in any hospital that receives Medicare or Medicaid financing
The preamble to the rules broke new ground by declaring ldquoThe patientrsquos right to be free from restraints is paramountrdquo27 The rules stated that SR may only be used in emergency situations if needed to ensure the patientrsquos physical safety and when less-restrictive alternatives have been determined ineffective and that
- 12 -
Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
deaths injuries and abuses resulting from seclusion and restraints were exposed
Unfortunately these are not isolated incidents They are but a few of scores of cases in which mental health patients ndash a disproportionate number of them children ndash died barbaric deaths more suited to medieval torture chambers than to late 20th century America They died because of the improper use of seclusion and physical or chemical restraints They died at the hands of the very people who were supposed to protect them
- Senator Lieberman Senator Dodd and Representative DeLauro July 16 1999
The National Alliance for the Mentally Ill (NAMI) also has tracked reports of recent and past SR abuses (Appendix 2) NAMI reported over 25 new incidents nationwide of deaths injuries and traumas caused by seclusion and restraints after the Courant survey Currently there is no official tracking of injury or trauma to patients or to staff in California NAMI however reported numerous incidents of serious injury ndash patients who became comatose who suffered broken bones were hit in the face bruised needed stitches or were bleeding as a result of restraints19
Equally troubling is the humiliation and trauma NAMI documents such as its many reports of patients unable to use the bathroom and left for hours in their own bodily wastes One patient was restrained for rejecting medication because she still hoped to nurse her young child another was placed in restraints because he couldnrsquot stop crying A 12-year-old was placed in a straightjacket in the middle of the floor where everyone could watch her ndash and staff called this a ldquoburritordquo A patient who voluntarily admitted herself to a hospital found herself reliving former traumatic experiences
Suddenly the guard had a huge pair of leather cuffs with padlocks on them All I knew was that I was being strapped down to a bed by a strange man with a gun This is not good therapy for a rape victim All I could do was close my eyes and pretend this wasnrsquot happening to me20
The US General Accounting Office (GAO) in an October 1999 report on improper seclusion and restraints validated the notion that patients may be severely traumatized while being restrained
- 7 -
Seclusion and Restraints A Failure Not a Treatment
even if no physical injuries are sustained ldquo Research indicates that at least half of all women treated in psychiatric settings have a history of physical or sexual abuserdquo21
Citing a Massachusetts state task force on the topic the GAO stated that the use of restraints on patients who have been abused often results in their re-experiencing their traumas and contributes to a setback in the course of treatment
Congress adopted reforms to federal policies administered by the US Centers for Medicare and Medicaid Services (CMS formerly HCFA) in 1999 In addition the Joint Commission on Accreditation of Healthcare Organizations has adopted new policies The recently enacted Childrenrsquos Healthcare Act of 2000 was the third major federal reform Explained more fully in Part II of this report these new policies are intended to restrict and reduce SR practices
Despite these reforms the federally mandated advocate organization Protection and Advocacy reports that 14 Californians have died and one has beenen permanently injured (in a persistent coma) while in seclusion or behavioral restraints since the new CMS rules were put into place in July 1999 Since there is no official requirement for reporting nonfatal injuries we cannot officially confirm the types of injuries documented by NAMI the news media and the GAO
Californiarsquos standards governing SR practice are different for each kind of facility State hospitals general acute care hospitals psychiatric health facilities skilled nursing facilities ndash all are facilities that utilize SR However each type of facility is governed by a different set of state regulations For example
General Acute Care Hospitals ndash In a case of emergency SR can be initiated at the discretion of a registered nurse and a verbal or written order obtained from a physician afterwards If a verbal order is obtained it shall be signed by the physician on his next visit Orders for SR may be for longer than 24 hours
Psychiatric Health Facilities ndash In an emergency a physicianrsquos order can be received over the telephone within one hour of initiating SR and must be signed in person within 24 hours Orders for SR may be in force for no longer than 24 hours
Skilled Nursing Facilities with Special Treatment Programs ndash A physician may give the order for SR by telephone and sign it in
- 8 -
Seclusion and Restraints A Failure Not a Treatment
person within five days The order expires and must be renewed each 24 hours to keep a person in SR
Each facilityrsquos standards differ from the others and on this particular issue none is as stringent as the federal standard Californiarsquos regulatory standards and some of the problems associated with them are discussed more fully under ldquoPatchwork Oversightrdquo on page 15
Scope of Report
This report focuses on issues of psychiatric seclusion and restraints It does not address issues of medical restraints such as immobilizing a person for a surgical procedure or placing a personrsquos arm in a ldquosleeverdquo to prevent removing an intravenous needle Nor does it address the important issues of SR policies in schools or facilities for the developmentally disabled or in correctional facilities for youths or adults It is limited in scope to policies of psychiatric seclusion and restraints in mental health facilities
The Pennsylvania Experience
Seclusion and restraints have been used to control the behavior of psychiatric patients since the Middle Ages22 However these techniques have also involved high risk of patient injury and death Pennsylvania has been a leader in trying to change this culture and working to reduce and ultimately eliminate the use of seclusion and restraints in its nine state hospitals
The Pennsylvania Office of Mental Health and Substance Abuse Services implemented its program because
hellipthese measures [SR] do not alleviate human suffering or psychiatric symptoms do not alter behavior and have frequently resulted in patient and staff injury emotional trauma and patient death23
Expert testimony at hearings of the Joint Commission on Accreditation of Healthcare Organizations also called attention to the counter-therapeutic aspects of SR
The attempt to impose ldquotreatmentrdquo by force is always counterproductive ndash creating humiliation resentment and resistance to further treatment that might be more helpful24
- 9 -
Seclusion and Restraints A Failure Not a Treatment
In practice seclusion and restraints are sometimes imposed on psychiatric patients for reasons that are not therapeutic These uses of SR have been discredited and are illegal under current law however they persist SR practices are sometimes used to
diams Control the environment ndash To curtail a patientrsquos movement to compensate for having inadequate staff on the ward or to avoid providing appropriate clinical interventions
diams Coerce ndash To force a patient to comply with the staffrsquos wishes or
diams Punish ndash To impose penalties on patient behaviors
NAMI has been a leader in the effort to end SR on these terms Its position is that restraints and seclusion have no therapeutic value and therefore they are not a ldquotreatmentrdquo NAMI asserts that SR are dangerous interventions and should be used only in cases of extreme emergency when someonersquos physical safety is in jeopardy and then only with careful safeguards25
The idea that psychiatric patients are treated with brutality are seriously injured or even killed in this day and age may be difficult to believe But the Courant investigation the Harvard Center for Risk Analysis and NAMIrsquos report all demonstrate that these practices continue to exist placing psychiatric patients at risk of trauma injury and even death In the most egregious cases where someone has died the causes of death are frequently violent asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdose drug interactions and choking26
These are our most vulnerable citizens Since they are often held against their will supposedly for their own well being it would be incumbent upon the state to protect them from being injured traumatized and abused
To address that responsibility this paper examines three critical issues
1) Seclusion and restraints policies have received national attention and have been the focus of three successive initiatives of federal reform Is that enough
2) Californiarsquos oversight of seclusion and restraints is a patchwork quilt of confusing bureaucracy that impedes accountability and progress Can it be improved
- 10 -
Seclusion and Restraints A Failure Not a Treatment
3) Other states have taken action to improve seclusion and restraints policies on the state level Most notably Pennsylvania has developed a model that garnered the Harvard Innovations in American Government Award and reduced hours of seclusion and restraints by 96 percent in its state hospitals Can California benefit from model practices developed in Pennsylvania
- 11 -
Seclusion and Restraints A Failure Not a Treatment
Part II
Federal Reforms and State Impacts
New Federal Regulations Three Layers of Reform
In response to the Hartford Courant series and the vigorous lobbying of NAMI federal actions to revise national policy on seclusion and restraints were proposed and implemented Reform came in three successive initiatives
diams First the US Centers for Medicare and Medicaid Services (CMS) issued new interim rules for Medicare and Medicaid hospitals in July of 1999
diams Next the Joint Commission on Accreditation of Healthcare Organizations released revised seclusion and restraints standards that took effect January 1 2001
diams Most recently on May 22 last year CMS issued Interim Final Rules under the Childrenrsquos Health Act of 2000 setting forth new regulations for psychiatric facilities that receive federal funds and for ldquononmedical community-based facilities for children and youthrdquo
First Reform CMS Breaks New Ground
CMS set forth interim final rules as of July 1999 that revised seclusion and restraints standards in any hospital that receives Medicare or Medicaid financing
The preamble to the rules broke new ground by declaring ldquoThe patientrsquos right to be free from restraints is paramountrdquo27 The rules stated that SR may only be used in emergency situations if needed to ensure the patientrsquos physical safety and when less-restrictive alternatives have been determined ineffective and that
- 12 -
Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
even if no physical injuries are sustained ldquo Research indicates that at least half of all women treated in psychiatric settings have a history of physical or sexual abuserdquo21
Citing a Massachusetts state task force on the topic the GAO stated that the use of restraints on patients who have been abused often results in their re-experiencing their traumas and contributes to a setback in the course of treatment
Congress adopted reforms to federal policies administered by the US Centers for Medicare and Medicaid Services (CMS formerly HCFA) in 1999 In addition the Joint Commission on Accreditation of Healthcare Organizations has adopted new policies The recently enacted Childrenrsquos Healthcare Act of 2000 was the third major federal reform Explained more fully in Part II of this report these new policies are intended to restrict and reduce SR practices
Despite these reforms the federally mandated advocate organization Protection and Advocacy reports that 14 Californians have died and one has beenen permanently injured (in a persistent coma) while in seclusion or behavioral restraints since the new CMS rules were put into place in July 1999 Since there is no official requirement for reporting nonfatal injuries we cannot officially confirm the types of injuries documented by NAMI the news media and the GAO
Californiarsquos standards governing SR practice are different for each kind of facility State hospitals general acute care hospitals psychiatric health facilities skilled nursing facilities ndash all are facilities that utilize SR However each type of facility is governed by a different set of state regulations For example
General Acute Care Hospitals ndash In a case of emergency SR can be initiated at the discretion of a registered nurse and a verbal or written order obtained from a physician afterwards If a verbal order is obtained it shall be signed by the physician on his next visit Orders for SR may be for longer than 24 hours
Psychiatric Health Facilities ndash In an emergency a physicianrsquos order can be received over the telephone within one hour of initiating SR and must be signed in person within 24 hours Orders for SR may be in force for no longer than 24 hours
Skilled Nursing Facilities with Special Treatment Programs ndash A physician may give the order for SR by telephone and sign it in
- 8 -
Seclusion and Restraints A Failure Not a Treatment
person within five days The order expires and must be renewed each 24 hours to keep a person in SR
Each facilityrsquos standards differ from the others and on this particular issue none is as stringent as the federal standard Californiarsquos regulatory standards and some of the problems associated with them are discussed more fully under ldquoPatchwork Oversightrdquo on page 15
Scope of Report
This report focuses on issues of psychiatric seclusion and restraints It does not address issues of medical restraints such as immobilizing a person for a surgical procedure or placing a personrsquos arm in a ldquosleeverdquo to prevent removing an intravenous needle Nor does it address the important issues of SR policies in schools or facilities for the developmentally disabled or in correctional facilities for youths or adults It is limited in scope to policies of psychiatric seclusion and restraints in mental health facilities
The Pennsylvania Experience
Seclusion and restraints have been used to control the behavior of psychiatric patients since the Middle Ages22 However these techniques have also involved high risk of patient injury and death Pennsylvania has been a leader in trying to change this culture and working to reduce and ultimately eliminate the use of seclusion and restraints in its nine state hospitals
The Pennsylvania Office of Mental Health and Substance Abuse Services implemented its program because
hellipthese measures [SR] do not alleviate human suffering or psychiatric symptoms do not alter behavior and have frequently resulted in patient and staff injury emotional trauma and patient death23
Expert testimony at hearings of the Joint Commission on Accreditation of Healthcare Organizations also called attention to the counter-therapeutic aspects of SR
The attempt to impose ldquotreatmentrdquo by force is always counterproductive ndash creating humiliation resentment and resistance to further treatment that might be more helpful24
- 9 -
Seclusion and Restraints A Failure Not a Treatment
In practice seclusion and restraints are sometimes imposed on psychiatric patients for reasons that are not therapeutic These uses of SR have been discredited and are illegal under current law however they persist SR practices are sometimes used to
diams Control the environment ndash To curtail a patientrsquos movement to compensate for having inadequate staff on the ward or to avoid providing appropriate clinical interventions
diams Coerce ndash To force a patient to comply with the staffrsquos wishes or
diams Punish ndash To impose penalties on patient behaviors
NAMI has been a leader in the effort to end SR on these terms Its position is that restraints and seclusion have no therapeutic value and therefore they are not a ldquotreatmentrdquo NAMI asserts that SR are dangerous interventions and should be used only in cases of extreme emergency when someonersquos physical safety is in jeopardy and then only with careful safeguards25
The idea that psychiatric patients are treated with brutality are seriously injured or even killed in this day and age may be difficult to believe But the Courant investigation the Harvard Center for Risk Analysis and NAMIrsquos report all demonstrate that these practices continue to exist placing psychiatric patients at risk of trauma injury and even death In the most egregious cases where someone has died the causes of death are frequently violent asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdose drug interactions and choking26
These are our most vulnerable citizens Since they are often held against their will supposedly for their own well being it would be incumbent upon the state to protect them from being injured traumatized and abused
To address that responsibility this paper examines three critical issues
1) Seclusion and restraints policies have received national attention and have been the focus of three successive initiatives of federal reform Is that enough
2) Californiarsquos oversight of seclusion and restraints is a patchwork quilt of confusing bureaucracy that impedes accountability and progress Can it be improved
- 10 -
Seclusion and Restraints A Failure Not a Treatment
3) Other states have taken action to improve seclusion and restraints policies on the state level Most notably Pennsylvania has developed a model that garnered the Harvard Innovations in American Government Award and reduced hours of seclusion and restraints by 96 percent in its state hospitals Can California benefit from model practices developed in Pennsylvania
- 11 -
Seclusion and Restraints A Failure Not a Treatment
Part II
Federal Reforms and State Impacts
New Federal Regulations Three Layers of Reform
In response to the Hartford Courant series and the vigorous lobbying of NAMI federal actions to revise national policy on seclusion and restraints were proposed and implemented Reform came in three successive initiatives
diams First the US Centers for Medicare and Medicaid Services (CMS) issued new interim rules for Medicare and Medicaid hospitals in July of 1999
diams Next the Joint Commission on Accreditation of Healthcare Organizations released revised seclusion and restraints standards that took effect January 1 2001
diams Most recently on May 22 last year CMS issued Interim Final Rules under the Childrenrsquos Health Act of 2000 setting forth new regulations for psychiatric facilities that receive federal funds and for ldquononmedical community-based facilities for children and youthrdquo
First Reform CMS Breaks New Ground
CMS set forth interim final rules as of July 1999 that revised seclusion and restraints standards in any hospital that receives Medicare or Medicaid financing
The preamble to the rules broke new ground by declaring ldquoThe patientrsquos right to be free from restraints is paramountrdquo27 The rules stated that SR may only be used in emergency situations if needed to ensure the patientrsquos physical safety and when less-restrictive alternatives have been determined ineffective and that
- 12 -
Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
person within five days The order expires and must be renewed each 24 hours to keep a person in SR
Each facilityrsquos standards differ from the others and on this particular issue none is as stringent as the federal standard Californiarsquos regulatory standards and some of the problems associated with them are discussed more fully under ldquoPatchwork Oversightrdquo on page 15
Scope of Report
This report focuses on issues of psychiatric seclusion and restraints It does not address issues of medical restraints such as immobilizing a person for a surgical procedure or placing a personrsquos arm in a ldquosleeverdquo to prevent removing an intravenous needle Nor does it address the important issues of SR policies in schools or facilities for the developmentally disabled or in correctional facilities for youths or adults It is limited in scope to policies of psychiatric seclusion and restraints in mental health facilities
The Pennsylvania Experience
Seclusion and restraints have been used to control the behavior of psychiatric patients since the Middle Ages22 However these techniques have also involved high risk of patient injury and death Pennsylvania has been a leader in trying to change this culture and working to reduce and ultimately eliminate the use of seclusion and restraints in its nine state hospitals
The Pennsylvania Office of Mental Health and Substance Abuse Services implemented its program because
hellipthese measures [SR] do not alleviate human suffering or psychiatric symptoms do not alter behavior and have frequently resulted in patient and staff injury emotional trauma and patient death23
Expert testimony at hearings of the Joint Commission on Accreditation of Healthcare Organizations also called attention to the counter-therapeutic aspects of SR
The attempt to impose ldquotreatmentrdquo by force is always counterproductive ndash creating humiliation resentment and resistance to further treatment that might be more helpful24
- 9 -
Seclusion and Restraints A Failure Not a Treatment
In practice seclusion and restraints are sometimes imposed on psychiatric patients for reasons that are not therapeutic These uses of SR have been discredited and are illegal under current law however they persist SR practices are sometimes used to
diams Control the environment ndash To curtail a patientrsquos movement to compensate for having inadequate staff on the ward or to avoid providing appropriate clinical interventions
diams Coerce ndash To force a patient to comply with the staffrsquos wishes or
diams Punish ndash To impose penalties on patient behaviors
NAMI has been a leader in the effort to end SR on these terms Its position is that restraints and seclusion have no therapeutic value and therefore they are not a ldquotreatmentrdquo NAMI asserts that SR are dangerous interventions and should be used only in cases of extreme emergency when someonersquos physical safety is in jeopardy and then only with careful safeguards25
The idea that psychiatric patients are treated with brutality are seriously injured or even killed in this day and age may be difficult to believe But the Courant investigation the Harvard Center for Risk Analysis and NAMIrsquos report all demonstrate that these practices continue to exist placing psychiatric patients at risk of trauma injury and even death In the most egregious cases where someone has died the causes of death are frequently violent asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdose drug interactions and choking26
These are our most vulnerable citizens Since they are often held against their will supposedly for their own well being it would be incumbent upon the state to protect them from being injured traumatized and abused
To address that responsibility this paper examines three critical issues
1) Seclusion and restraints policies have received national attention and have been the focus of three successive initiatives of federal reform Is that enough
2) Californiarsquos oversight of seclusion and restraints is a patchwork quilt of confusing bureaucracy that impedes accountability and progress Can it be improved
- 10 -
Seclusion and Restraints A Failure Not a Treatment
3) Other states have taken action to improve seclusion and restraints policies on the state level Most notably Pennsylvania has developed a model that garnered the Harvard Innovations in American Government Award and reduced hours of seclusion and restraints by 96 percent in its state hospitals Can California benefit from model practices developed in Pennsylvania
- 11 -
Seclusion and Restraints A Failure Not a Treatment
Part II
Federal Reforms and State Impacts
New Federal Regulations Three Layers of Reform
In response to the Hartford Courant series and the vigorous lobbying of NAMI federal actions to revise national policy on seclusion and restraints were proposed and implemented Reform came in three successive initiatives
diams First the US Centers for Medicare and Medicaid Services (CMS) issued new interim rules for Medicare and Medicaid hospitals in July of 1999
diams Next the Joint Commission on Accreditation of Healthcare Organizations released revised seclusion and restraints standards that took effect January 1 2001
diams Most recently on May 22 last year CMS issued Interim Final Rules under the Childrenrsquos Health Act of 2000 setting forth new regulations for psychiatric facilities that receive federal funds and for ldquononmedical community-based facilities for children and youthrdquo
First Reform CMS Breaks New Ground
CMS set forth interim final rules as of July 1999 that revised seclusion and restraints standards in any hospital that receives Medicare or Medicaid financing
The preamble to the rules broke new ground by declaring ldquoThe patientrsquos right to be free from restraints is paramountrdquo27 The rules stated that SR may only be used in emergency situations if needed to ensure the patientrsquos physical safety and when less-restrictive alternatives have been determined ineffective and that
- 12 -
Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
In practice seclusion and restraints are sometimes imposed on psychiatric patients for reasons that are not therapeutic These uses of SR have been discredited and are illegal under current law however they persist SR practices are sometimes used to
diams Control the environment ndash To curtail a patientrsquos movement to compensate for having inadequate staff on the ward or to avoid providing appropriate clinical interventions
diams Coerce ndash To force a patient to comply with the staffrsquos wishes or
diams Punish ndash To impose penalties on patient behaviors
NAMI has been a leader in the effort to end SR on these terms Its position is that restraints and seclusion have no therapeutic value and therefore they are not a ldquotreatmentrdquo NAMI asserts that SR are dangerous interventions and should be used only in cases of extreme emergency when someonersquos physical safety is in jeopardy and then only with careful safeguards25
The idea that psychiatric patients are treated with brutality are seriously injured or even killed in this day and age may be difficult to believe But the Courant investigation the Harvard Center for Risk Analysis and NAMIrsquos report all demonstrate that these practices continue to exist placing psychiatric patients at risk of trauma injury and even death In the most egregious cases where someone has died the causes of death are frequently violent asphyxiation strangulation cardiac arrest fire or smoke inhalation blunt trauma drug overdose drug interactions and choking26
These are our most vulnerable citizens Since they are often held against their will supposedly for their own well being it would be incumbent upon the state to protect them from being injured traumatized and abused
To address that responsibility this paper examines three critical issues
1) Seclusion and restraints policies have received national attention and have been the focus of three successive initiatives of federal reform Is that enough
2) Californiarsquos oversight of seclusion and restraints is a patchwork quilt of confusing bureaucracy that impedes accountability and progress Can it be improved
- 10 -
Seclusion and Restraints A Failure Not a Treatment
3) Other states have taken action to improve seclusion and restraints policies on the state level Most notably Pennsylvania has developed a model that garnered the Harvard Innovations in American Government Award and reduced hours of seclusion and restraints by 96 percent in its state hospitals Can California benefit from model practices developed in Pennsylvania
- 11 -
Seclusion and Restraints A Failure Not a Treatment
Part II
Federal Reforms and State Impacts
New Federal Regulations Three Layers of Reform
In response to the Hartford Courant series and the vigorous lobbying of NAMI federal actions to revise national policy on seclusion and restraints were proposed and implemented Reform came in three successive initiatives
diams First the US Centers for Medicare and Medicaid Services (CMS) issued new interim rules for Medicare and Medicaid hospitals in July of 1999
diams Next the Joint Commission on Accreditation of Healthcare Organizations released revised seclusion and restraints standards that took effect January 1 2001
diams Most recently on May 22 last year CMS issued Interim Final Rules under the Childrenrsquos Health Act of 2000 setting forth new regulations for psychiatric facilities that receive federal funds and for ldquononmedical community-based facilities for children and youthrdquo
First Reform CMS Breaks New Ground
CMS set forth interim final rules as of July 1999 that revised seclusion and restraints standards in any hospital that receives Medicare or Medicaid financing
The preamble to the rules broke new ground by declaring ldquoThe patientrsquos right to be free from restraints is paramountrdquo27 The rules stated that SR may only be used in emergency situations if needed to ensure the patientrsquos physical safety and when less-restrictive alternatives have been determined ineffective and that
- 12 -
Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
3) Other states have taken action to improve seclusion and restraints policies on the state level Most notably Pennsylvania has developed a model that garnered the Harvard Innovations in American Government Award and reduced hours of seclusion and restraints by 96 percent in its state hospitals Can California benefit from model practices developed in Pennsylvania
- 11 -
Seclusion and Restraints A Failure Not a Treatment
Part II
Federal Reforms and State Impacts
New Federal Regulations Three Layers of Reform
In response to the Hartford Courant series and the vigorous lobbying of NAMI federal actions to revise national policy on seclusion and restraints were proposed and implemented Reform came in three successive initiatives
diams First the US Centers for Medicare and Medicaid Services (CMS) issued new interim rules for Medicare and Medicaid hospitals in July of 1999
diams Next the Joint Commission on Accreditation of Healthcare Organizations released revised seclusion and restraints standards that took effect January 1 2001
diams Most recently on May 22 last year CMS issued Interim Final Rules under the Childrenrsquos Health Act of 2000 setting forth new regulations for psychiatric facilities that receive federal funds and for ldquononmedical community-based facilities for children and youthrdquo
First Reform CMS Breaks New Ground
CMS set forth interim final rules as of July 1999 that revised seclusion and restraints standards in any hospital that receives Medicare or Medicaid financing
The preamble to the rules broke new ground by declaring ldquoThe patientrsquos right to be free from restraints is paramountrdquo27 The rules stated that SR may only be used in emergency situations if needed to ensure the patientrsquos physical safety and when less-restrictive alternatives have been determined ineffective and that
- 12 -
Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
Part II
Federal Reforms and State Impacts
New Federal Regulations Three Layers of Reform
In response to the Hartford Courant series and the vigorous lobbying of NAMI federal actions to revise national policy on seclusion and restraints were proposed and implemented Reform came in three successive initiatives
diams First the US Centers for Medicare and Medicaid Services (CMS) issued new interim rules for Medicare and Medicaid hospitals in July of 1999
diams Next the Joint Commission on Accreditation of Healthcare Organizations released revised seclusion and restraints standards that took effect January 1 2001
diams Most recently on May 22 last year CMS issued Interim Final Rules under the Childrenrsquos Health Act of 2000 setting forth new regulations for psychiatric facilities that receive federal funds and for ldquononmedical community-based facilities for children and youthrdquo
First Reform CMS Breaks New Ground
CMS set forth interim final rules as of July 1999 that revised seclusion and restraints standards in any hospital that receives Medicare or Medicaid financing
The preamble to the rules broke new ground by declaring ldquoThe patientrsquos right to be free from restraints is paramountrdquo27 The rules stated that SR may only be used in emergency situations if needed to ensure the patientrsquos physical safety and when less-restrictive alternatives have been determined ineffective and that
- 12 -
Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
coercion discipline convenience of the staff or retaliation are unacceptable reasons for placing a patient in restraints
The interim standards also required training for staff involved in SR and most significantly implemented a ldquoone-hour rulerdquo This required a patient placed in restraints to receive a face-to-face evaluation by a licensed professional practitioner within one hour The new regulations also required reporting all deaths associated with seclusion and restraints in CMS facilities28
These changes in federal policy were significant although advocacy groups argued that they did not go far enough Some providers however countered that reform was unnecessary and prohibitively expensive There was a contentious debate over whether the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) should adopt lesser standards or conform to CMSrsquos new interim rules
Second Reform JCAHO is Lobbied to Concur with CMS Rules
JCAHOrsquos standards are important because it gives accreditation to approximately 80 percent of the health care facilities in the country JCAHO is a legal agency of the federal government If a health care facility is accredited by JCAHO and meets all of JCAHOrsquos standards it also is deemed to have met all of CMSrsquos standards and is eligible to receive Medicare and Medicaid financing
In a protracted battle advocates persuaded JCAHO not to adopt lesser standards than those in the CMS reforms Some of JCAHOrsquos new rules (Appendix 3) are stronger than CMSrsquos but they meet all of the CMS minimal standards including the hotly debated one-hour rule
In releasing JCAHOrsquos new standards on seclusion and restraints JCAHO President Dennis OrsquoLeary MD stated ldquoThese standards underscore the importance of applying great care in using interventions that can harm or even kill patientsrdquo29
Third Reform Childrenrsquos Health Act of 2000 Sets Strongest Rules Yet
The third and most comprehensive set of reforms were included in the federal Childrenrsquos Health Act of 2000 This act which had 36 legislative titles30 included national standards that restricted the use of restraints and seclusion in psychiatric facilities and
- 13 -
Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
ldquononmedical community-based facilities for children and youthrdquo that receive federal funds (Appendix 4) Nonmedical community childrenrsquos programs had not previously been covered by SR standards
Key provisions of the new federal standards
diams SR may be imposed solely to ensure physical safety ndash never as punishment or for staff convenience
diams SR may be imposed only with a written order from a physician or licensed practitioner and must specify duration and circumstances
diams These standards should not be construed to offset or impede any federal or state regulations with greater protections thus affirming the CMS one-hour rule
diams Facilities must report every death that occurs within 24 hours after a patient has been removed from SR
diams CMS must set standards for adequate staffing and appropriate training for the use of SR and alternatives
How Does Reform Affect California
How many people are at risk of being put into seclusion or restraints Any person in a psychiatric facility may be at risk Those confined involuntarily in mental health facilities in California may number more than 100000 each year
The RAND Corporationrsquos 2001 analysis of the California Client Data System (CDS) estimated that in fiscal 1997-98 nearly 52000 people were admitted to psychiatric facilities on 72-hour involuntary holds in the state But RAND stated that the California Department of Mental Health believes this represents only half of the true number of involuntary inpatient admissions31 Thatrsquos because ldquomental health services paid for by private insurers and services delivered through Medi-Cal Inpatient Consolidation are not included in the CDS systemrdquo RAND said
An estimate of roughly 100000 does not include people in long-term psychiatric facilities since there is no comprehensive system for counting those patients Nor does it include people who voluntarily commit themselves to mental health facilities Those patients also are vulnerable to seclusion or restraints
- 14 -
Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
Patchwork Oversight
Regulatory systems that govern SR use are extremely complicated There are state standards which differ by type of facility For example the standards are different for state hospitals than for private acute care hospitals The federal standards cited earlier also vary by facility depending upon whether a facility is accredited by JCAHO
Enforcement of the rules is equally complex JCAHO conducts inspections once every three years A representative from the California Department of Health Services (DHS) accompanies JCAHO on these inspections making sure that state standards are being followed DHS also conducts random ldquosample validationsrdquo of 5 percent of JCAHO facilities to make sure they are following CMS standards and remain eligible to receive federal funds
DHS inspects non-JCAHO facilities every two years to enforce both federal and state standards In other types of facilities the process is different still Skilled nursing facilities for example have their own standards and are inspected once a year by DHS But psychiatric health facilities and mental health rehabilitation centers are governed by different rules and inspected by a different department ndash the Department of Mental Health (DMH)
This table illustrates the complexity of the system There are at least six categories of facility two types of federal standards depending upon the accreditation the various state standards depending on facility type and enforcement by JCAHO DHS or DMH
The practical result of this complex system this SOR report finds is confusion lack of accountability and inadequate protection of mental health patients from injury and death
- 15 -
Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
Figure 1 Regulatory Authority over Seclusion and Restraints in California Psychiatric Facilities
No No Beds Licensed JCAHO- Facilities Accredited Acute Care Facilities State Hospitals 4 4828 DHS 4
Acute Psychiatric Hospitals 41 2846 DHS 15
Psychiatric Health Facilities 16 354 DMH 1
General Acute Care Hospitals 124 4421 DHS 47 with Acute Psychiatric Program
Long-Term Care Facilities
Mental Health Rehab Ctrs 18 1301 DMH 0
Skilled Nursing Facilities 34 3240 DHS 1 with Special Psychiatric Treatment Programs
Source California Department of Health Services and Department of Mental Health
Official SR Reporting is Deficient
Californiarsquos system for tracking and documenting the use of SR is fragmentary at best Although reporting these incidents is required by state lawlowast the information collected is incomplete and compliance is poor
The California Office of Patient Rights is vested with responsibility for collecting and reporting this information However it must rely on data supplied by counties and facilities In the year 2000 the Office of Patient Rights documented a high rate of noncompliance 56 facilities or 22 percent submitted either an incomplete report or no report at all32 Even two of the state hospitals ndash Atascadero and Metropolitan ndash did not comply with the requirement33
lowast California Welfare and Institutions Code Section 53261
- 16 -
Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
The Office of Patient Rights points out the limitations of Californiarsquos reporting system
diams There are no specific statutory or regulatory provisions or other mechanisms for enforcing facility andor county compliance with the regulatory requirements
diams There are no standard procedures or guidelines for counties to establish and maintain a list of facilities that are required to comply with these reporting requirements
diams Consequently absent any routine monitoring of the Department of Health Servicesrsquo licensing and certification records of licensed facilities we cannot assert that this report reflects or contains information from all California facilities falling within reporting requirements34
For these reasons the Office of Patient Rights concluded that ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo35
In addition DHS reports that it does not consider SR data from the Office of Patient Rights when deciding whether to conduct inspections on facilities
Even when the legally required information is submitted the process lacks teeth In 1999 the Office of Patient Rights wrote ldquoJohn George Pavilion in Alameda County reports an astronomical use of seclusion and restraint (1641 incidents)rdquo36 Yet in 2000 the John George Pavilion did not report at all
Since California lacks a meaningful statewide tracking system there is no way to measure SR practices except to measure when a person dies That information is also incomplete but what we do know about deaths and grave injuries comes from Protection and Advocacy Inc (PAI)
The PAI system was established by federal mandate in 1975 to protect the rights of people with disabilities thus mental health patients may look to Protection and Advocacy for legal representation and other advocacy services if their rights are violated Until 1999 PAI had no systematic way to track deaths from SR and generally heard about instances of abuse only when it received formal complaints
- 17 -
Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
Hospital deaths or permanently disabling injuries (such as comatose conditions) that are related to seclusion and behavioral restraints must be reported to PAI under the 1999 CMS hospital regulations PAI stresses that these numbers do not reflect the extent of the problem The GAO which calls the reporting ldquopiecemealrdquo concurs that the system under-represents these incidents37
Since the new rules went into effect in July 1999 PAI says that 12 deaths or serious injuries have been officially reported by CMS PAI also says it is aware of three additional cases that were not reported to CMS By its count at least 14 people have died and at least one became persistently comatose while in seclusion or behavioral restraints in California in the past 31 months
Removing Barriers to Accountability
Accreditation Offers No Guarantees
NAMI cites these ldquoinadequaciesrdquo inrelying exclusively on JCAHO for SR oversight
diams JCAHOrsquos governing board is controlled by physicians andhospitals
diams Information collected byJCAHO is confidential and unavailable to the public
diams JCAHO does not investigate individual complaints and generally conducts site visitson a preannounced three-yearcycle
diams JCAHO accreditation has not ended SR deaths GloriaHuntley died in the CentralState Hospital in Virginia after 558 hours in restraints over two months NAMI reports that she died the day after JCAHO inspected her hospital and awarded it with accreditation and a special
d ti
There are several significant barriers to improving outcomes and reducing the dangers of injury for patients and staff in mental health settings Key among these is that California has no uniform standards covering all facilities The use of SR is governed by differing federal regulations and the GAO cites differing standards as contributing to difficulties in obtaining accountability38
None of the new federal regulations prohibits states from setting standards that are higher than those of the federal government Some states ndash Delaware Pennsylvania Massachusetts New York ndash have reduced SR by implementing their own more stringent standards39
- 18 -
Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
Also there is no mandatory consistent and publicly accessible system of reporting on SR uses serious injuries or deaths Among states that have succeeded in lowering their use of SR mandatory reporting has been a critical tool for improving outcomes Such reporting ideally should include ndash in addition to patient deaths and serious injuries ndash the number of SR incidents the duration of the use of seclusion or restraints medication errors falls staff injuries and airway obstructions
- 19 -
Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
Part III
Pennsylvania ndash A Model for Reform
In 1997 the Pennsylvania Department of Public Welfare instituted an aggressive program to reduce and ultimately eliminate seclusion and restraints in its nine state hospitals Charles Curie deputy secretary of mental health and substance abuse services articulated the philosophy behind the change in policy ldquoMost of our patients are already the victims of trauma There is no need to reinforce that trauma or to re-traumatizerdquo40
Three years later Pennsylvania had reduced incidents of seclusion and restraint in its nine state hospitals by 74 percent and reduced the number of hours patients spent in seclusion and restraints by 96 percent Its program which includes both forensic and civil commitments has the highest standards for SR in the nation Pennsylvaniarsquos hospitals experienced no increase in staff injuries In addition its changes were implemented without any additional funds using only existing staff and resources41
By July of 2000 Pennsylvania reported that one state mental hospital had not used seclusion for over 20 months Another had used neither seclusion nor restraints for eight of the last 12 months Three hospitals had been seclusion- and restraint-free for one or more consecutive months and others were approaching zero use42
In October 2000 Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative received the prestigious Harvard University Innovations in American Government Award
Figure 2 illustrates the reduction in seclusion and restraints that Pennsylvania achieved over the course of its three-year reform project as measured by the Pennsylvania Office of Mental Health and Substance Abuse Services
- 20 -
Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
Figure 2
Pennsylvania Reduces Incidence of Seclusion and Restraints by 74 and Duration of Seclusion and Restraints by 96
Restraint Usage per 1000 Patient Days 70
60
50
40
30
20
10
0
6058
398
3996
376
4616
256
186
219 134
259 216
068
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Restraint Hours Restraint Incidents
Seclusion Usage per 1000 Patient Days 35
30
25
20
15
10
5
0
3283
302
3252
323
443
139 288
134 071
051 046
033
FY 199293 CY 1994 CY 1997 CY 1998 CY 1999 CY 2000
Seclusion Hours Seclusion Incidents
- 21 -
Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
Elements of Reform
Pennsylvania began its reform project by carefully tracking the use of SR and then used that 1997 data as its baseline to measure improvements A workgroup of practicing hospital clinicians set about developing new policies and procedures goals strategies and monitoring systems to design and implement the new approach Key among these goals was developing a new philosophy of care ndash one that identified SR as treatment failure and restricted it to emergency use only
Mental health officials cite a number of innovations as critical to the success of the program Among them
diams Computerized data collection and analysis
diams Strategies for organizational change
diams Staff training in crisis prevention and intervention
diams Risk-assessment and treatment-planning tools
diams Patient debriefing methods
diams Recovery-based treatment models and
diams Adequate numbers of staff
Also critical was changing the culture of state hospitals Pennsylvania did this by requiring open public access to SR data by creating competition among hospitals to reduce SR and by giving awards and acknowledgments for improvement
Figure 3 shows the key elements of Pennsylvaniarsquos SR reduction policy
- 22 -
__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

__________________________________________________________________
Seclusion and Restraints A Failure Not a Treatment
Figure 3
Pennsylvania Seclusion and Restraints Reduction Initiative43
Seclusion and restraints must be the intervention of last resort
SR are exceptional and extreme practices for any patient They are not to be used as a substitute for treatment nor as punishment or for the convenience of the staff
SR are safety measures not therapeutic techniques which should be implemented in a careful manner
Staff shall include patient strengths and cultural competence to prevent incidents of SR
Staff must work with the patient to end SR as quickly as possible
A physician must order SR
Orders are limited to one hour and require direct physician contact with the client within 30 minutes
The patient and family are considered part of the treatment team
The patient advocate is the spokesperson for the patient (if the patient desires it) and is involved in care and treatment
Patients being restrained cannot be left alone
Chemical restraints are prohibited
The treatment plan includes specific interventions to avoid SR
Patients and staff must be debriefed after every incident and treatment plans must be revised
Staff must be trained in de-escalation techniques
Patient status must be reviewed prior to utilizing SR Voluntary patients who did not agree to these procedures must be involuntarily committed before these procedures may be initiated
Leaders of the hospital clinical department heads and ward leaders are accountable at all times for every phase of an SR procedure Accountability is demonstrated as a component of the hospitalrsquos ldquoperformance improvementrdquo index and in staff competency evaluations
Data regarding the use of SR are made available to consumer and family organizations and government officials
- 23 -
Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
Part IV
Conclusion
The crude and ancient practices of secluding and restraining mental health patients are antiquated traumatizing and potentially dangerous If from 50 to 150 patients die nationally each year as a result of seclusion and restraint as the Harvard Center for Risk Analysis has estimated deaths in California could number between six and 18 annually because the state represents 12 percent of the US population In addition there is no official tracking of SR injuries to patients or to staff
The federal government in July 1999 instituted reforms aimed at increasing oversight of SR and reducing its use However Protection and Advocacy Inc reports that 15 Californians have been killed or disabled while in SR since then PAI knows of 14 cases of death and one comatose victim
An estimated 100000 Californians are committed involuntarily each year in mental health facilities and countless more voluntarily enter as inpatients Any one of them is at risk of seclusion or restraint under todayrsquos patchwork of state and federal standards that vary by type of facility
This confusion contributes to a lack of accountability and a dearth of protections against SR abuses In California the Office of Patient Rights concludes ldquothere is no way to accurately track or report countywide or statewide trends regarding the denial of patientsrsquo rights or the use of seclusion and restraintrdquo44
Yet Pennsylvania after officially determining that SR is a failure rather than a treatment cut use of seclusion and restraint in its state hospitals by 74 percent in three years without increasing staff costs or injuries
- 24 -
Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
Federal reforms governing SR policies are only as effective as the oversight mechanisms that enforce them There are at least two significant barriers to adequate oversight in California
diams Lack of uniform statewide standards over SR use affecting all types of facilities and
diams Lack of mandatory consistent and publicly accessible reporting on serious injuries and deaths caused by SR the frequency and duration of SR and other issues related to its use
Although private psychiatric hospitals may be the most difficult to regulate they may also be the most out-of-compliance with federal standards In 1999 the US inspector general issued a report titled Restraints and Seclusion ndash State Policies for Psychiatric Hospitals that evaluated state compliance with the new federal SR standards The report found that many state policies had already met some of the new requirements while other state policies for both public and private facilities did not45 The inspector general reported that state policies for the use of restraints and seclusion in private psychiatric hospitals more frequently failed to meet the new regulations46 The report concluded
We recommend that HCFA [now CMS] work aggressively to quickly raise psychiatric hospital compliance with the new Patientsrsquo Rights Condition of Participation where necessary Particular attention should be given to policies for private psychiatric hospitals47
Options
diams California could develop uniform standards that at least match if not exceed the highest federal regulations across all facility types that treat people with psychiatric disabilities
diams California could develop mandatory comprehensive and publicly accessible data-reporting requirements on the use of seclusion and restraints with meaningful consequences for noncompliance
diams A working group could be directed to review practices policies and facilities in Pennsylvania with the goal of developing proposals to similarly reduce the use of SR in California Its members could include representatives of the state Department of Mental Health the Legislature county mental health
- 25 -
Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
departments patient advocacy groups and consumers families and providers
Hubert Humphrey believed that a just society may be measured by the way it treats its most vulnerable citizens48 Protecting Californians from injuries trauma and abuse caused by isolating and restraining them is a fundamental responsibility and a measure of our society Given the known harms that seclusion and restraints have inflicted on vulnerable Californians policymakers may want to give serious consideration to comprehensive safe and cost-effective ways to reduce their use
- 26 -
Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
ENDNOTES
1 Leslie G Aronovitz Extent of Risk From Improper Restraint or Seclusion is Unknown (Washington DC US General Accounting Office 1999) pp 1-2
2 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) p 1
3 Leslie B Morrison Supervising Attorney Investigations Unit Protection andAdvocacy Inc Based on official reporting from CMS and completed PAI investigations February 26 2002
4 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
5 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
6 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
7 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
8 Ibid pp 2 10
9 Ibid p 2
10 Ibid
11 Ibid
12 Ibid
13 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative
- 27 -
Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
(Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
14 Ibid
15 In November 2001 Mr Curie was appointed administrator of the Substance Abuse and Mental Health Services Administration of the US Department ofHealth and Human Services
16 Harvard University Innovations in American Government Mental Hospital Seclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
17 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) pp 1 and 3
18 National Alliance for the Mentally Ill The National Regulation of Restraint Use in HCFA Funded Treatment Facilities Some Questions and Answers (ArlingtonNAMI Website 1999) p 1
19 National Alliance for the Mentally Ill A Summary of Reports of Restraints and Seclusion Abuse Received Since the October 1998 Investigation by The Hartford Courant (Arlington NAMI Website 2000) pp 1-22
20 Ibid p 12
21 Ibid
22 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) p 1
23 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Application Essay (Boston Harvard University Website 2000) p 2
24 Peter R Breggin MD Principles for the Elimination of Restraint Testimony for the Joint Commission on Accreditation of Healthcare Organizations (Bethesda Center for Study of Psychiatry and Psychology April 25 1999) p 1
25 National Alliance for the Mentally Ill Use of Restraints and Seclusion (ArlingtonNAMI Website 1999) p 1
26 Eric M Weiss Dave Altimari Dwight F Blint Kathleen Megan et al Deadly Restraint (Hartford The Hartford Courant 1998) pp 1-16
27 Health Care Financing Administration Medicare and Medicaid Programs Hospital Conditions of Participation Patientsrsquo Rights Interim Final Rules (64 Fed Reg 36078 [July 2 1999])
- 28 -
Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
28 Ibid p 36085
29 Deborah Flapan Medscape Wire Joint Commission Releases Revised Restraints Standards for Behavioral Healthcare (Medscape Website 2000) p 1
30 Including re-authorization of the Substance Abuse and Mental Health Services Administration
31 Susan M Ridgely Randy Borum and John Petrila The Effectiveness of Involuntary Outpatient Treatment Empirical Evidence and the Experience of Eight States (Santa Monica RAND 2001) p 85
32 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
33 Ibid
34 Ibid
35 Ibid
36 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 1999 (Sacramento 1999) p 4
37 Leslie G Aronovitz Extent of Risk from Improper Restraint or Seclusion is Unknown (Washington DC United States General Accounting Office 1999) p 5
38 Ibid p 8
39 Ibid p 11
40 Harvard University Innovations in American Government Mental HospitalSeclusion and Restraint Reduction ndash 2000 Winner (Boston Harvard University Website 2000) p 1
41 The Pennsylvania Department of Public Welfare Office of Mental Health and Substance Abuse Services Leading the Way Toward a Seclusion and Restraint-Free Environment ndash Pennsylvaniarsquos Seclusion and Restraint Reduction Initiative (Harrisburg Office of Mental Health and Substance Abuse Services 2000) pp 1-3
42 Ibid
43 Ibid
44 California Office of Patient Rights Annual Report of Denial of Rights and SeclusionRestraint 2000 (Sacramento 2000) p 2
45 Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 1
- 29 -
Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
46 Ibid
47Jesse J Flowers et al Restraints and Seclusion ndash State Policies for Psychiatric Hospitals (Atlanta United States Department of Health and Human Services Office of Inspector General 2000) p 3
48 Senator Hubert H Humphrey remarks at the dedication of the Hubert H Humphrey Building November 1 1977 Congressional Record November 4 1977 vol 128 p 87287
- 30 -
Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Seclusion and Restraints A Failure Not a Treatment
Appendices
Appendix 1 Deadly Restraint A Hartford Courant Investigative Report httpwwwcourantclassifiedscomprojectsrestraintdeath_datastm
Appendix 2 California cases excerpted from National Alliance for the Mentally Ill (NAMI) summary of nationwide reports of restraint and seclusion abuses received between October 1998 and March 2000 (Attached)
Appendix 3 Summary of key changes in the Joint Commission on the Accreditation of Healthcare Organizationsrsquo Seclusion and Restraints Standards (Attached)
Appendix 4 Summary of key changes in nonmedical Community Childrenrsquos Programs under the Federal Childrenrsquos Health Act of 2000 (Attached)
- 31 -
APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

APPENDIX 2
California cases excerpted fromNational Alliance for the Mentally Ill (NAMI) summary of reports of restraint and seclusion abuses received between
October 1998 and March 2000
After The Hartford Courant published its ldquoDeadly Restraintrdquo investigative series inOctober 1998 NAMI reported receiving ldquoa steady stream of reportsrdquo of recent or past abuses of restraints and seclusion including more deaths The California incidents reported below are taken from NAMIrsquos Web site athttpwwwnamiorgupdatehartfordhtml
ldquoUnless otherwise indicated the source of each report is the person actually involved in the incidentrdquo NAMI says on its Web site ldquoNAMI has not independently investigated each incident but will provide assistance to government authorities ornews reporters who wish additional details about specific incidents or to talk with sources directlyrdquo
Locale Facility Details of Incident DateSource Berkeley Hospital A man who asked for something to help
him sleep was placed in seclusion Without a bathroom he was left to defecate in his clothing
Occurred in 1993 reportedby parents299
Chula New Kristal Mayon-Ceniceros 16 died of 2599Vista Alternative
s (privatefacility)
respiratory arrest after she was put face-down on the floor with arms and legs restrained by four staff members
Associated Press
Green- County A 6-foot-7 man was admitted to the Occurred 399 brae hospital psychiatric ward involuntarily after
calling 911 for help He was given anti-psychotic drugs without his consent denied prescribed sleep medication became agitated and struck a wall signStaff told him to go into a seclusion room to avoid restraints he cooperated and was put into restraints in seclusion for 12-14 hours Charts showed he initiallywas cooperative ldquoyet they did not let him uphellip he started thrashing around Then they shot him full of drugshellip He was treated inhumane denied all dignity had to urinate on himselfrdquo
reported bymother on 32999
Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

Los Altos Described by thepatient asldquoa veryreputablewell-runrdquo hospital
A 29-year-old woman had her hands andfeet restrained to a bed and was isolated in a room for an estimated 18 hours Nurses entered only twice and left waterout of reach She was not informed of the nature of her illness throughout her hospitalization
Occurred in 1995 reported299
Oakland Hospital A newly widowed mother of three wasrestrained for four hours after she refused medication because she hoped to nurse her youngest child She consideredit a punishment ldquoRestraints are used tobreak your spirit and the humiliationputs one into a major depressionhellip I donrsquot think Irsquove ever recovered the confidence and self-esteem I used to haverdquo
Occurred in 1989 reported299
San Inpatient Son was put into a coma as a result of Occurred 1299 Francisco mental
health center
being placed in restraints and reportedby father
San Luis General A woman placed in seclusion all night Occurred in Obispo hospital defecated in her clothes and drank her
urine to quench a thirst caused bylithium carbonate
1997 reportedby parents299
Stockton San JoaquinCountypsychiatrichealth facility
Rick Griffin 36 6-foot-3 and 340 pounds died from cardio-respiratory failure and extreme agitation after he was wrestled to the floor by eight staff members and bound in leather restraints
Occurred in 1198 reported by sister and Stockton Record
____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

____________________________________________________________________
APPENDIX 3
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
New Standards For Seclusion And Restraint ndash Key Changes
bull Restricts use of SR to emergencies in which there is an imminent risk of harm to self or others
bull Requires communication throughout a facility on the philosophy of using SR only in extraordinary situations and only for the safety of the patient
bull Requires staff education to understand de-escalation techniques medication self-protection and to recognize signs of physical distress
bull Restricts time of an SR incident initially to one hour for children under age 7 and four hours for adults Subsequent renewals are limited to one hour for children under 9 and four hours for adults
bull Stipulates that only licensed independent practitioners can place orders for SR
bull Requires continuous monitoring of individuals while under SR
bull Requires patients under 18 to be evaluated in person by a licensed independent practitioner within two hours and adults within four hours of initiation of an SR order [However JCAHO in practice has agreed torequire the stricter CMS ldquoone hourrdquo rule] If the patient continues in SR he or she must be re-evaluated by a licensed independent practitioner every eight hours if age 18 and over and every four hours if under 18 If the person is released before being evaluated a licensed independent practitioner must do a face-to-face evaluation within 24-hours
bull Requires staff to try to contact a restrained or isolated patientrsquos family if she or he requests it
bull Requires criteria to be established and communicated for discontinuing use of SR
bull Requires a de-briefing within 24 hours of SR use among the patient staff and family of the patient (if the patient desires family participation)
_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons

_____________________________________________________________
APPENDIX 4
Childrenrsquos Health Act Of 2000
Nonmedical Community Childrenrsquos Programs ndash Key Changes
bull SR may be used only in emergencies and to ensure immediate physical safety
bull Mechanical restraints are prohibited
bull Seclusion is allowed only when a staff member continuously monitors the patient face-to-face (ldquoTime outsrdquo are not considered seclusion)
bull Only staff trained and certified by a state-recognized body may impose SR (Until a certification process is in place only a supervisory or senior staff person with specified skills and competencies may initiate SR or assess patients as required within a one-hour timeframe)
bull Skills and competencies required of such staff include relationship-building avoiding power struggles methods for de-escalating conflict alternatives to seclusion or restraints use of time limits monitoring signs of physical distress knowledge of asphyxia from body positioning knowing when and how to obtain medical assistance and legal issues
bull States must develop licensing and monitoring rules for such facilities and the US Department of Health and Human Services will develop national staffing standards and guidelines
These standards address only psychiatric treatment facilities ndash they do not affect schools wilderness camps jails or prisons