-
8/3/2019 script #9 gas transportation
1/18
1
In this lecture, we will talk about gas transportation in the
blood and we will also
give you an idea about regulation in the respiratory system.
Gas Transportation
The composition of air that you inspire will have the pressure
of 150 mmHg by the
end of inspiration which is different than the end of
expiration. It will give you an
alveolar composition in that space, so youll have the
atmospheric composition
that will be a little bit different, because of the water
vapor.
We did talk previously about the major force principle for gas
diffusion which is
thepartial gradient pressure. According to this principle, O2
will have the pressure
of 140 mmHg in the lungs area and the same pressure in the
tissue. The O2 will go
from the lungs to the tissue, as the carbon dioxide CO2 is
higher in the tissue than
in the pulmonary arteries.
Carbon Dioxide
Lets start with CO2 because its easier to discuss. CO2
transports in the blood in
differentforms:
60 % of CO2 is in form of H2CO3
30 % of CO2 is a compound with hemoglobin
10 % of CO2 dissolved in the plasma
CO2 as carbonic acid (H2CO3), which is not a stable compound,
can be dissociated
to hydrogen & CO2 , CO2 can bind to hydrogen to form H2CO3.
Thats why the
majority of CO2 in the blood is in the form of H2CO3.
Now the most important gas is not CO2 but O2. after diffusion,
O2 will be in the
blood and it will cross the cytoplasm membrane of RBCs. 97% -
98% of that O2
will bind to the hemoglobin molecule, each hemoglobin molecule
has 4 sites to
bind with O2.
-
8/3/2019 script #9 gas transportation
2/18
2
Hemoglobin is a protein with a long polypeptide structure of
amino acids. And as
we remember from biochemistry it has 4 subunits, 2 of them is
called alpha and 2
of them is called beta. The functional one for oxygen binding is
thebeta.
Forms of hemoglobin
Hemoglobin has 2 forms :
1- Liking O2 (exposed sites)
2- Disliking O2 (released sites)
The benefit of this is that when the hemoglobin is in the area
of the lungs (the
pulmonary arteries, capillaries and alveolar structure) where
thePulmonary
Circulation occurs. The hemoglobin will be in the liking form,
because the function
there is to catch the O2 from the lungs down to the tissue. Then
(in the tissue) it
changes to its disliking form so the hemoglobin will start to
release the oxygen in
the tissue.
Factors that can change the hemoglobin form
Different factors can change the form of the hemoglobin.
Changing here is not
about being exposed or closing the sites, but its about
increasing or decreasing
the power or force of the hemoglobin to catch the O2, which is
calledaffinity
(meaning strength). So the affinityof the hemoglobin describes
its capability of
holding O2. Hemoglobin with high affinity catches O2 well and
that with low
affinity releases O2 somehow, easily.
So, what are the factors that change the affinity of the
hemoglobin?
-CO2, Hydrogen concentration,Temperature and BPG
(2,3-bisphosphoglcerate).
The increase of one of these factors or more than one will
decrease the affinity of
Hb (Inverse relationship).
-
8/3/2019 script #9 gas transportation
3/18
3
Note: In the pulmonary circulation we have continuous
ventilation -O2 supply,
CO2 deplete. if one site of the Hb binds one oxygen the other 3
sites will have
more affinity to bind with the remaining oxygens, and when it
binds to the second
oxygen the other 2 sites will have more and more affinity to
bind to the remaining
2 oxygens.
1- CO2
Depleting of CO2 means decreasing its concentration in the blood
, and according
to the ventilation concept we mentioned earlier, it will
increase the affinity of Hb.
2- Hydrogen Concentration :
From studying PH we found that by reducing the CO2
concentration, the
Hydrogen concentration will be reduced as well because CO2 is a
volatile acid. So
when you leave out CO2, the hydrogen will be less and the PH
will be alkali. Thus,
increasing PH will give us higher affinity, and decreasing PH
lowers the affinity
because its similar to the increase and decrease of hydrogen
concentration.
H+ , CO2 , PH , affinity
3- Temperature :
Continuous ventilation happens when the blood comes to the
lungs. It will cool
the blood vessels and the blood itself like when you open the
door and the
windows of the room so youll have an airway that cools the room
due to the low
temperature of the air itself. This continuous ventilation will
decrease the
temperature in the pulmonary circulation in your body.
Note: we can conclude so far that those 3 factors are not
favorable in the
pulmonary circulation.
4- BPG (2,3-bisphosphoglcerate).
we still dont know the way it works in physiology but its
important in pathology.
-
8/3/2019 script #9 gas transportation
4/18
4
Fig. 12-23, p. 389
Alveoli
Pulmonary
capillary
blood
= O2 molecule
= Partially saturated hemoglobin molecules
= Fully saturated hemoglobin molecules
Fig. 12-25, p. 392
Tissue cell Alveolus
Plasma
From systemiccirculation
to pulmonary
circulation
-
8/3/2019 script #9 gas transportation
5/18
5
In the tissue :
The metabolic reaction occur in the cell , produce energy ,
produce heat , so the
Temp will be closer to the tissue , and higher the Temp .
If we are talking about nerve or muscle cell ( the places where
we need more O2 (
, the Temp is more higher , so that will decrease the affinity
that will cause the
release of oxygen . metabolic reaction in the cell will produce
CO2 always.
Nutrients + O2 + H2O + Enzyme CO2
So CO2 level will be more in the tissue that will decrease the
affinity .
Increasing CO2 will cause it bind to H from H2O to produce H2CO3
( with the help
of Enzyme or carbonic anhydrase in the tissue ,
and the H2CO3 will disassociate to H2 and CO2
CO2 + H2O
>
H2CO3 H2 + CO2
SO we have more CO2 >>> more H >>> Less PH
So these Factor will increase the affinity of the Hb to bind to
oxygen
So whenever Hb move to pulmonary circulation >> higher
affinity to catch O2
whenever it is in the tissue >>it release oxygen
AND THIS IS THE GOALS OF RESPIRATION( take the O2 from atm ,
release the O2
in the tissue )
Carbonic anhydrase
Enzyme
-
8/3/2019 script #9 gas transportation
6/18
6
How fast that reaction occur ?
This is a capillary which we divide it into 3 thirds
>>>
1/3 1/3 1/3
When Hb moves on the first part ( first third distance )it is
more than enough time
to have 100% saturation of Hb , So when Hb is move to the
pulmonary circulation
doesnt take long time to have 100% saturation .
What is 100% saturation ??
When the 4 sites of the Hb are fully occupied by O2
Now the Qs is : How many molecule of Hb in each RBC ?
Answer : It is 250-300 thousand molecule
( according to some calculation the Dr did )
FIGURE 12-22 / SLIDE 34
97% bound with Hb
3% swimming in the plasma
Very fastHb
-
8/3/2019 script #9 gas transportation
7/18
7
Fig. 12-22, p. 388
Average resting
PO2 at systemiccapillaries
Normal PO2 at
pulmonarycapillaries
1 g Hb 1.34 ml of O2 ( total weight of the 4 oxygen molecule
that binds to 1 g
Hb
So
1 g Hb 1.34 ml O2 / dL
50 g Hb 12 ml O2 / dL
So , at 1/3 distance the blood cell will be fully saturated
before it reach the second
third or the third third ( last part of capillary ) , so what is
the need of this parts
without binding to O1 ???
Bcz GOD knows that sometimes when u r running or stressful the
heart will pumpur blood much faster , so the blood flow instead of
X it might be 2X more , So , in
this case GOD doesnt want this blood cell to leave the lungs
without oxygen
{ ABNORMALITIES IN BINDING OXYGEN }
** CARBON MONOXIDE POISONING
It is very common especially in poor countries bcz they dont
have a central
heating > when we are in winter people try to warm themselves
, one way of
warming is burning wood or kerosene , the result of that fire is
producing the CO2
-
8/3/2019 script #9 gas transportation
8/18
8
and CO ( carbon monoxide ) . This CO Loves this site of oxygen
more than O2
Loves the sites ( higher attraction )
Bcz of that > in the presence of CO the O2 lose its affinity
to bind to the sites
For example : if there are 250 O2 and 1 CO the 1 CO will win the
250 , and O2
will lose the site of binding
CO binding affinity to Hb is stronger 250 times more than O2
affinity
Now let me give you what will happen after CO poisoning , people
die peacefully ,
they dont feel pain , dont shout , dont cry , they just sleepy
and it is the end of
their life !
Study the following figures well :
Fig. 12-24, p. 391
Arterial PCO2 and acidity,
normal body temperature
(as at pulmonary level)
PCO2
Acid (H+)
Temperatureor
2,3-Bisphosphoglycerate
(as at
tissue
level)
-
8/3/2019 script #9 gas transportation
9/18
9
pO2
% saturation
9 ml O2 / dL
20 ml O2 / dL
100 mmHg40 mmHg
16 ml O2 / dL
19 ml O2 / dL
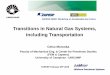
About the last figure:
1) The partial pressure of O2 in the blood could be zero when we
have heavyexercise m when all the O2 are consumed
2) The pressure at artery part, at full saturation is = 100 mmHg
and theamount of O2 at that time is 20 ml
3) The pressure at veins part is = 40 mmHg and the amount of O2
at thattime is 16 ml
NOW the Qs is :
( What is the amount of O2 that is released , and we usually
need
It ?)
**The Answer >>
Artery part
= saturated blood
= Artery blood
= Oxygenated blood
= 100 mmHg
Veins part
= unsaturated blood
= vein blood
=deoxygenated blood
= 40 mmHg
Capillary
-
8/3/2019 script #9 gas transportation
10/18
10
the amount Of realized O2=
the amount that inter the amount that leave
So , here >> the amount of realized O2 = 20 16 = 4 ml
Now
Lets assume that the affinity of Hb is higher or lower than
normal
The amount of
realized O2
The curve
Higher affinity 20-19 = 1 ml Shift to the left
Normal affinity 20-16 = 4 ml normal
Lower affinity 20-9 = 11 ml Shift to the right
Lets say a normal person has 15g of Hb, after a CO poisoning he
inhaled a certain
amount of CO (not much). Lets assume that half of Hb was bound
to CO
(0.5*15=7.5 g/Hb). We have only 7.5g/Hb available for oxygen and
the other half
it appears as it is absent because they come to the lungs they
dont take O2, and
the go to the tissue and they dont release oxygen (thats why we
use the term
absent).
So, we have half the amount of the Hb available, so the full
saturation will actually
be half the normal one: not 20 mL but 10 mL as the full
saturation.
So again: why this curve got changed and reduced to the
half?
-
8/3/2019 script #9 gas transportation
11/18
11
-because half Hb are available for the oxygen and the other half
will be lost.
one half is lost by CO binding the other half, affinity is
decresed. The other half
has a higher affinity because of CO binding so the curve will
shift to the left.
Now lets ask ourselves this question: with carbon monoxide
poisoning, how
much oxygen in the arterial blood coming to the tissue and how
much oxygen
released to the tissue..??
The same simple question..
In here arterial blood have the partial pressure of 100 mmHg so
the amount of
oxygen is 10 mL, when the blood comes to the tissue it carries
10 mL because its
fully saturated condition means only half the amount of the
hemoglobin is
saturated. Now we want to take some of that oxygen to the
tissue..
when we take that, the partial pressure of oxygen here is 40
mmHg so the
amount which matches this point on the figure is another 10 mL.
So when you
subtract them you get zero mL of oxygen released. So in carbon
monoxidepoisoning because 1) the affinity of the curve is shifted
to the left, 2) the amount
of the Hb is less the other half is carried by CO, we will not
have any oxygen
released to the tissue . And this is whats going on while people
are sleeping
peacefully inhaling the carbon monoxide from the stove and when
the carbon
monoxide concentration increase and increase, reaching that
point so theres no
O2 to the nerve cells.. the point here.. Nerve cells
we have a center for respiration, and this center is capable of
sensing how much
oxygen is present in your tissues. If it is low, it will
increase your ventelation tosupply the tissue with more oxygen. But
there is a cut of point limit when we have
zero oxygen to the supply the respiratory center itself, in this
case, the respiratory
center got killed and its work is stopped. We dont do more
ventilation, we
stop it.
at the same time, we lose our conscious. So these people, when
they reach that
-
8/3/2019 script #9 gas transportation
12/18
12
level of No oxygen and the carbon monoxide is full they will
lose their conscious
which is good for not feeling the pain of dyeing.
This the best way to commit suicide, (please believe the doctor
in this). People
who want to die peacefully set in the garage and turn on the
cars and inhale the
smoke thats coming out of the car which is full of carbon
monoxide.
Carbon monoxide, what it does??
It will bind ., very strong, and it will increase the non bound
for
oxygen, it will increase the affinity. So that increased
affinity will shift the curve to
the left and so, people die.
we hear a lot of stories about whole families die because of
this. Securing all the
windows and the doors and sleeping while the stove is turned on.
This is the
carbon monoxide poisoning.
Another case is Anemia. Therere different types of the anemia
but well talk
about the common one, which is the iron deficiency anemia. The
normal amount
of oxygen is 20 mL of oxygen in arteries and 60 mLs in veins and
4 mLs was
utilized. Lets assume this child has anemia.
in other words when we major the Hb content of that child it
will be lower than
the normal. The normal Hb is said to be 50 % g/dl just for the
simple discussion
we repeat it again in front of you, lets assume we major that Hb
in the patient is
7.5 so half of his Hb is lost, not lost because of carbon
monoxide bound because
its not there! Iron deficiency they are not able to produce and
synthesize enough
Hb so the amount is half , because its half so we will have 10
ml of the full
saturation this is the curve for this patient.
-
8/3/2019 script #9 gas transportation
13/18
13
Now the problem is the same when we calculate the utilization.
This is 10 ml and
this is 8 ml so 10 8 = 2 ml from each dl, this is bad, normally
this child needs
more than 4 ml from each dk. What he gets only half of it. Now
if you ask mepractically all these anemic patients especially
children they are not bad in their
feeding and sign and symptoms, theyre playing theyre normal but
when you
major the Hb itll be lower, you discover them by screening or
majoring that. Why
they dont feel bad? Because somehow when the HB is lower and the
other half is
absent completely, the remaining Hb decreases its affinity. In
the CO poising the
opposite; the remaining half increase their affinity, here the
existing Hb as
homeostatic function or reaction it will decrease the affinity
of Hb, because its
decreased that means the curve shifted to the right (left
strongerright weaker)so that curve will be this on but the
saturation will will stay 10 ml (full) of
oxygen now because this shift to the right lets calculate the
oxygen utilization
in the artery the amount of oxygen is 10 ml when it comes to the
tissue
When it leaves the tissue its 40 mm Hg. So the amount of oxygen
in this curve
will be about 6. So if you see there is compensation by shifting
the curve to the
right youll get better amount of oxygen released even the
absolute total amount
to oxygen is half instead of 20 we have 10 so the patients are
good becausesomehow the curve is shifted to the right, after a
while it will go back to the
normal affinity and that will cause a reduction of oxygen
utilization. So this is the
other case of oxygen Hb dissociation curve.
-
8/3/2019 script #9 gas transportation
14/18
14
Fig. 12-26, p. 396
Pons
Pneumotaxic center
Apneustic center
Pre-Btzingercomplex
Dorsal respiratorygroup
Ventral respiratory
group Medulla
Ponsrespiratory
centers
Medullaryrespiratory
center
Respiratory
controlcenters in
brain stem
Lets go to the last topic of respiration:
We already know how the first step, ventilation, is
physiologically conducted, and
how diffusion occurs between the glands and blood vessels, and
between blood
and tissues as the second step to the process. We also know how
gas is
transported in the blood by carbonation, where CO2 either binds
to hemoglobin,
or it dissolves. 98% of O2 can also bind to hemoglobin, and the
2% binds to the
plasma.
-
8/3/2019 script #9 gas transportation
15/18
15
Table 12-5, p. 397
Now lets see how we can control and regulate the three steps of
respiration:
Since we are talking about regulation, we must mention both the
central nervous
system and chemical regulation. Let me start with the central
nervous system.
The regulation of human breathing has to major parts: the first
one is your will to
stop breathing. If you want to stop breathing you can. If you
ask yourself to hyper
ventilate, you will. For how long does this go on for? It goes
on until your nervous
system tells you to stop.
The second part which is involuntary is located in the medullar
open gate bone in
the central nervous system. We will explain this in brief, I
will give you the main
idea of regulation but not in detail.
We have a collection of nerve cells, they are special in
respiration which means
they send a signal to the inspiratory muscle, and then the
muscle will contract.
There is another collection of nerve cells, the expiratory
nerves, but the benefit is
that when the inspiratory neurons are firing, the expiratory are
inhibited, and
when the the expiratory are firing, the inspiratory are
inhibitedbecause you cant
-
8/3/2019 script #9 gas transportation
16/18
16
do both opposing actions together, I was talking about forcible
breathing but in
normal breathing I discussed before in the diaphragm contraction
and relaxation,
just inspiratory neurons fire with that muscle to contract the
diaphragm then a
release of diaphragm, what causes the expiration recalling
tendency elastic
tissues and the intra-pleural pressure which becomes less
negative.
There is no brain control for normal quiet expiration at all,
the only control for
normal inspiration its an on and off signal and if we cut all
the neurons up and
down, this center for normal quite breathing it will fire on and
off ,on and off. In
physiology we call this circadian rhythm, the same thing applied
to your eyes
when they are closed and opened or like when you sleep and wake
up. We need
to balance this rhythm to make our health proper, if we dont
balance those 2
facts inhibition and estimation (on & off) we will die, so
the respiratory central(inspiratory neuron and expiratory neurons),
are the major neurons but they are
not enough, another thing is needed, like sometimes we need hypo
and hyper
ventilate and sometimes we need to stop a little bit, this is
not coming from the
brain but from the outside the brain.
Fig. 12-27, p. 397
Sensory
nerve fiber
Carotid sinus
Carotid artery
Aortic arch
Sensory
nerve fiber
Carotid bodies
Aortic bodies
Heart
-
8/3/2019 script #9 gas transportation
17/18
17
We have different receptors that are located in the most
beautiful area of our
bodies: the aorta and carotid artery. These receptors have one
ultimate goal: to
sense the amount of oxygen and the amount of CO2 in the area. If
this is the case,
let us assume that these receptors were found on the muscle
fiber.
In the muscle fiber, oxygen will be 100, 40. If the muscle is
moving it will be 100,
10 and 100, 0 if the muscle is running, meaning they cant
control the normal
situation. In the normal situation, the muscle moving will have
zero oxygen, while
a still muscle will have 40 mm mercury of oxygen. So the normal
range is between
0 40 mm.
If they were located there, they would send a wrong message to
the brain. Notice
the aorta and carotid artery. The blood flow is very fast and
this is one of the
factors. The second factor is the fact that we dont have an
excitable membrane
in the carotid artery. In other words, we dont utilize and
produce much oxygen
there. This would be the same case if the receptors were
sensitive to CO2 and we
put them on any tissue, at times we will have a lot of CO2 (the
metabolic reaction
is high), and times were metabolism is low, meaning that the
normal range will be
high. So the receptors shouldnt be in wrong places, they should
be here where
the oxygen content is 100 and the CO2 content is 40 mm.
When the oxygen content is low and CO2 is high, then there is
something wrong in
our respire system. When we dont have enough oxygen to breathe,
the aorta and
carotid artery will have lower oxygen. This makes them sense the
low content of
oxygen, meaning they should interact.
Back to the tissue, it was normal to have zero oxygen and
abnormal to have
60mm mercury, because we dont utilize oxygen here. At the same
time, when we
have more than 50 mm mercury of CO2 here and here, it means
something is
wrong in the metabolic action which will increase the amount of
CO2 which isbeyond the capacity of the respire system to expel out.
A message to the brains
center will be sent telling the brain to interact, where low O2
and high CO2 will
cause hyper ventilation, where we will expel CO2 and get more
O2, then change
the normal concentration of O2 and CO2 in the blood to the norm,
these
receptors will quiet down.
-
8/3/2019 script #9 gas transportation
18/18
18
This is the function of our respire center in the brain. They
are working day and
night in the normal case, and receptors here to sense the
reduction of O2 or the
increasing of CO2 to interact. So we have the regulation of the
respite center and
the peripheral which are the respire receptors. There are other
factors too such
as pain. So when you sense pain you will hyper ventilate so the
pain will affect the
respiratory regulation. Sudden cold temperatures will also stop
the breathing.
Drugs such as sleeping pills or pain killers in large
concentrations will also cause
hypo ventilation. Under anesthesia will also cause the control
of respiration to
stop. That is what happens when people are anesthetized under
operations and
we do artificial breathing, because the respire center does not
send signals.
Paraphrased by : Marwa Al-Halalmeh & Eman Nazzal
Thanx A lot for : Malak joudeh & Noha Ghazal
. Good luck