Embed Size (px)
Citation preview

Screening
Principles of Epidemiology
Lecture 12
Dona Schneider, PhD, MPH, FACE

Principles Underlying Screening Programs
Validity – the ability to predict who has the disease and who does not
Sensitivity – the ability of a test to correctly identify those who have the disease
A test with high sensitivity will have few false negatives
Specificity – the ability of a test to correctly identify those who do not have the disease
A test that has high specificity will have few false positives

Principles Underlying Screening Programs (cont.)
An ideal screening test would be 100% sensitive and 100% specific – that is there would be no false positives and no false negatives
In practice these are usually inversely related
It is possible to vary the sensitivity and specificity by varying the level at which the test is considered positive

Calculating Measures of Validity
a+b+c+db+da+cTotal
c+ddcNegative
a+bbaPositive
TotalNo DiseaseDiseaseTest Result
True Diagnosis

Note the Following Screening Relationships Specificity + false positive rate = 1
d/(b+d) + b/(b+d) = 1 If the specificity is increased, the false positive rate is decreased
If the specificity is decreased, the false positive rate is increased
Sensitivity + false negative rate = 1
a/(a+c) + c/(a+c) = 1 If the sensitivity is increased, the false negative rate is decreased
If the sensitivity is decreased, the false negative rate is increased

Probability of Disease
Pre-test probability of disease = disease prevalence
Post-test probability of disease =
If normal, c/(c+d)
If negative, a/(a+b)

Interrelationship Between Sensitivity and Specificity

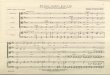
Sensitivity and Specificity of a Blood Glucose Level
100.0100.0
48.4
(true negatives)
7.1
(false negatives)
All those with level under 110 mg/100 ml are
classified as nondiabetics
51.6
(false positives)
92.9
(true positives)
All those with level over 110 mg/100 ml are
classified as diabetics
Nondiabetics
(Percent)
Diabetics
(Percent)
Blood Glucose Level
(mg/100 ml)
Sensitivity and Specificity of a Blood Glucose Level of 110 mg/100 ml for Presumptive Determination of Diabetes Status

Adjusting Sensitivity and Specificity by Adjusting Cut Points

Which is Preferred: High Sensitivity orHigh Specificity?
If you have a fatal disease with no treatment (such as for early cases of AIDS), optimize specificity
If you are screening to prevent transmission of a preventable disease (such as screening for HIV in blood donors), optimize sensitivity

Remember….
Sensitivity and specificity are functions of the screening test
If you use a given screening test on a low prevalence population, you will have a low positive predictive value and potentially many false positives

Translated into Real Life…..
Another 68,950 are frightened into believing they have the disease and require more testing
But, 10,500 people who are HIV+ think they are disease free
Efficiency of test = (TP + TN)/Total tested = 98.9%
7 million6,895,000105,000Total
6,836,5506,826,05010,500Test -163,45068,95094,500Test +
TotalDisease NoDisease Yes
99.8%58%1.5%NJ (7 million)
PV-PV+Prevalence of HIVPopulation
Elisa is about 90% sensitive and 99% specific

If You Change To a High Risk Population, You Get Better Results….
But only 35 are frightened into believing they have the disease and require more testing
Now 350 people who are HIV+ think they are disease free
Efficiency of test = (TP + TN)/Total tested = 94.5%
7,0003,5003,500Total
3,1853,465350Test -
3,185353,150Test +
TotalDisease NoDisease Yes
90.8%98.9%50%IV Drug UserPV-PV+Prevalence of HIVPopulation

Suppose You Have a Very High Prevalence?
HIV seropositivity is 90% among IV drug users in Newark
PV+ = 99.9%
PV- = 52%
But, why bother to screen?

Example: Breast Cancer Screening
64,81064,633177Total
63,69563,65045Negative
1,115983132Positive
TotalNo DiseaseDiseaseMammogram
Results
Breast Cancer

Example: Disease X (prevalence = 2%)
100098020Total
9339312Negative
674918Positive
TotalNo DiseaseDiseaseTest Results
True Diagnosis of Disease X

Example: Disease X (prevalence = 1%)
100098010Total
941.5940.51Negative
58.549.59Positive
TotalNo DiseaseDiseaseTest Results
True Diagnosis of Disease X
To increase positive predictive value increase prevalence by screening high risk populations

Importance of Prevalence in Screening
100,00099.99010Total
99,98599,9850Negative
15510Positive
TotalNo DiseaseDiseaseTest Results
True Diagnosis of HIVFemale Donors
Assume we have a test for AIDS which has a sensitivity of 100% and a specificity of 99.995%. We wish to apply it to female blood donors who have an HIV prevalence of 0.01% and we wish to apply it to male homosexuals in San Francisco, in whom the prevalence is 50%. For every 100,000 screened we find:
100,00050,00050,000Total
49,99749,9970Negative
50,003350,000Positive
TotalNo DiseaseDiseaseMale Homosexuals
True Diagnosis of HIV
PV+ = 0.66667
PV+ = 0.99994

Relationship of Specificity to Predictive Value
Prev = 20%, Sens = 50%, Spec = 90%,
PV = 100/180 = 56%
1,000800200
820100- 720Test
18080100+
-+
Disease
400
Prev = 20%, Sens = 50%, Spec = 50%,
PV = 100/500 = 20%
1,000800200
500100-
Test
500400100+
-+Disease
- 40020
Prev = 20%, Sens = 90%, Spec = 50%,
PV = 180/520 = 31%
1,000800200
420
Test
580400
180+
-+
Disease
500250
Prev = 50%, Sens = 50%, Spec = 50%,
PV = 250/500 = 50%
1,000500500
250-
Test500250250+
-+
Disease

Suppose You Are Faced With the Following Brain Teaser
In a given population of 1,000 persons, the prevalence of Disease X is 10%. You have a screening test that is 95% sensitive and 90% specific.
What is the positive predictive value?
What is the efficiency of the test?

Suppose You Are Faced With the Following Brain Teaser (cont.)
1) Set up a 2x2 table
1000900100Total
True NegativeFalse Negative Negative
False PositiveTrue PositivePositive
TotalNo DiseaseDiseaseTest Results
True Diagnosis of Disease X

Suppose You Are Faced With the Following Brain Teaser (cont.)
1000900100Total
8158105Negative
1859095Positive
TotalNo DiseaseDiseaseTest Results
True Diagnosis of Disease X

Principles Underlying Screening Programs Reliability – the ability of a test to give consistent results when
performed more than once on the same individual under the same conditions Variation in the method due to variability of test chemicals or fluctuation
in the item measured (e.g., diurnal variation in body temperature or in relation to meals) Standardize fluctuating variables Use standards in laboratory tests, run multiple samples whenever possible
Observer variation Train observers Use more than one observer and have them check each other

Principles Underlying Screening Programs Yield – the amount of previously unrecognized disease that is diagnosed and
brought to treatment as a result of the screening program
Sensitivity You must detect a sufficient population of disease to be useful
Prevalence of unrecognized disease Screen high risk populations
Frequency of screening Screening on a one time basis does not allow for the natural history of the disease, differences in
individual risk, or differences in onset Diseases have lead time
Participation and follow-up Tests unacceptable to those targeted for screening will not be utilized

The condition should be an important health problem
There should be an accepted treatment for patients with recognized disease
If there is no treatment, it is premature to institute screening
Facilities for diagnosis and treatment should be available
It is unethical to screen without providing possibilities for follow-up
There should be a recognizable latent or early symptomatic stage
If early detection does not improve survival, there is no benefit from screening
Conditions for Establishing Screening Programs

There should be a suitable test for examination, with sufficient sensitivity and specificity to be of use in identifying new cases
The test should be acceptable to the population
The natural history of the condition, including development from latent to declared disease, should be adequately understood
There should be an agreed-upon policy concerning whom to treat as patients
Conditions for Establishing Screening Programs (cont.)

Conditions for Establishing Screening Programs (cont.)
The cost of case-finding should be economically balanced in relation to possible expenditure on medical care as a whole
Case-finding should be in a continuing process and not a one-time project

Biases in Screening
Referral Bias (volunteer bias)
Length Bias
Screening selectively identifies those with a long preclinical and clinical phase (i.e., those who would have a better prognosis regardless of the screening program)

Biases in Screening (cont.)
Lead Time Bias
The apparently better survival that is observed for those screened is not because these patients are actually living longer, but instead because diagnosis is being made at an earlier point in the natural history of the disease

Biases in Screening (cont.)
Overdiagnosis Bias (a misclassification bias)
Enthusiasm for a new screening program may result in a higher rate of false positives and give false impression of increased rates of diagnosis and detection
Also, false positives would result in unrealistically favorable outcomes in persons thought to have the disease