Embed Size (px)
DESCRIPTION
Overzicht van stand van zaken 2011 en blik op de toekomst
Citation preview

NATURE REVIEWS | GASTROENTEROLOGY & HEPATOLOGY ADVANCE ONLINE PUBLICATION | 1
Department of Biological Sciences, University of Essex, Wivenhoe Park, Colchester CO4 3SQ, UK (N. Pawa, J. D. Norton). ICENI Centre, Department of Surgery, Colchester Hospital University NHS Foundation Trust, Turner Road, Colchester CO4 5JL, UK (T. Arulampalam).
Correspondence to: J. D. Norton [email protected]
Screening for colorectal cancer: established and emerging modalitiesNikhil Pawa, Tan Arulampalam and John D. Norton
Abstract | It has been estimated that >95% of cases of colorectal cancer (CRC) would benefit from curative surgery if diagnosis was made at an early or premalignant polyp stage of disease. Over the past 10 years, most developed nation states have implemented mass population screening programs, which are typically targeted at the older (at-risk) age group (>50–60 years old). Conventional screening largely relies on periodic patient-centric investigation, particularly involving colonoscopy and flexible sigmoidoscopy, or else on the fecal occult blood test. These methods are compromised by either low cost-effectiveness or limited diagnostic accuracy. Advances in the development of diagnostic molecular markers for CRC have yielded an expanding list of potential new screening modalities based on investigations of patient stool (for colonocyte DNA mutations, epigenetic changes or microRNA expression) or blood specimens (for plasma DNA mutations, epigenetic changes, heteroplasmic mitochondrial DNA mutations, leukocyte transcriptome profile, plasma microRNA expression or protein and autoantibody expression). In this Review, we present a critical evaluation of the performance data and relative merits of these various new potential methods. None of these molecular diagnostic methods have yet been evaluated beyond the proof-of-principle and pilot-scale study stage and it could be some years before they replace existing methods for population screening in CRC.
Pawa, N. et al. Nat. Rev. Gastroenterol. Hepatol. advance online publication 1 November 2011; doi:10.1038/nrgastro.2011.205
IntroductionColorectal cancer (CRC) is one of the most prevalent forms of malignancy worldwide with approximately 1 million new cases diagnosed each year, accounting for 500,000 deaths.1 The pathogenesis of CRC involves the progressive accumulation of gene mutations over a time-scale of years as the disease advances.1 Most cases of early stage disease are clinically silent and, as a result, approximately 55% of patients in the UK present with lymph node or distant metastases.2 The stage of disease at diagnosis is the single most important predictor of prognosis and disease-free survival.3 The overall 5-year age-standardized survival rate for CRC in Europe ranges from only 52% to 62%.2,4
It has been estimated that over 95% of cases of CRC would benefit from curative surgery if diagnosis was made at an early or premalignant polyp stage, and several large-scale studies have demonstrated a statisti-cally signifi cant reduction in mortality with implementa-tion of mass CRC screening programs.5,6 It is perhaps relevant that during their lifetime, an estimated 40–50% of the population in developed nations will develop one or more polyps, although the majority of these polyps will remain benign.7
Broadly speaking, screening strategies are of two types: those that involve direct investigation of the patient, often with an invasive procedure, and those based on laboratory analysis of patient specimens (typically feces
or peripheral blood) to detect disease biomarkers. Both strategies target the higher-risk older-aged population (>50–60 years old). An ideal screening strategy needs to fulfill four important criteria: acceptable performance in terms of positive and negative predictive value for the target population; a reduction in mortality from the disease; acceptable levels of patient compliance; and low enough cost to be affordable within the context of the specific health-care system. No such ideal diag-nostic screening procedure for CRC currently exists, and the main screening modalities that have so far been adopted (invasive diagnosis of the patient and the fecal occult blood test [FOBT]) represent a trade-off between the above four criteria. Several authors have recently reviewed the current state of practice and investigation in this field.5,6,8,9 The purpose of this Review is to sum-marize the different diagnostic screening strategies that have been or are being investigated (Table 1; Box 1), and to explore the potential of emerging technologies in the application of molecular markers for population screening for CRC.
Established screening modalities Direct investigation of the patientColonoscopyColonoscopy is regarded as the gold standard for the diagnosis of colorectal polyps and malignancy, and has gained increased popularity in the USA and Canada over the past 10–20 years; however, Poland is currently the only European country utilizing colonoscopy as the sole
Competing interestsThe authors declare no competing interests.
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

2 | ADVANCE ONLINE PUBLICATION www.nature.com/nrgastro
screening method for individuals aged 55–66 years.10 Although its use is clearly associated with a decrease in CRC-related deaths, no direct evidence from random-ized controlled trials has demonstrated the effectiveness of colonoscopy in reducing mortality from CRC, and therefore inferences are drawn from indirect evidence. In a prospective observational study of asymptom-atic average-risk individuals, Kahi et al.11 reported a 65% reduction in CRC mortality and 67% reduc-tion in disease incidence with colonoscopy screen-ing. Similarly, Rabenck and colleagues12 identified an
Key points
■ Approximately 1 million new cases of colorectal cancer are diagnosed each year
■ Population screening for detection of disease at an early stage has demonstrated a significant reduction in mortality
■ The fecal occult blood test is the most widely adopted screening method, but is compromised by poor reliability and patient compliance
■ Although flexible sigmoidoscopy is cost-effective, more definitive direct investigative procedures (such as colonoscopy) are prohibitively expensive for most national screening programs
■ An expanding list of potential new screening methods based on the detection of DNA, RNA or protein molecular markers in patient stool or blood specimens is currently being evaluated
■ The introduction of screening based on molecular markers is likely to be an incremental process; established screening modalities are likely to remain in widespread use for some years
inverse association between mortality and increased rate of complete colonoscopy. A large population-based, case– controlled study demonstrated a marked mortality reduction for left-sided lesions, but with very little reduc-tion for right-sided tumors in patients who underwent colonoscopy.13 This observation concurs with similar findings from a cross-sectional study of the German population.14 Despite some confounding issues in these studies, such as variability in procedural performance at different centers, they do question the presumed supe-riority of colonoscopy as a screening tool, especially for tumors of the proximal colon. Under the auspices of the Northern-European Initiative on Colorectal Cancer (NordICC), a large multicenter randomized trial is currently underway that aims to establish the clinical impact of colonoscopy screening on CRC incidence and mortality, with the final results expected in 2026.15
Another area of concern with colonoscopy is that it is a very operator-dependent procedure; a ‘miss rate’ of between 6% and 12% has been identified for larger polyps and 5% for cancers.16 As an invasive procedure, it is also not without some attendant risk of complications, such as bowel perforation. The rate of major complications has been reported at 0.2%, a figure representing approxi-mately 10 times that of any other cancer screening test.17 However, the main disadvantage of colonoscopy is its high cost, making it unaffordable as a population screening method for most of the global health-care sector.18
Table 1 | Current CRC screening guidelines
Risk European Union Guidelines 2010125 American Cancer Society Guidelines 2011126
Average risk Screening age: 50–74 yearsScreening options: fecal occult blood test (2 yearly)
Screening age: 50 years (45 years for African Americans)Screening options: fecal occult blood test (yearly)*CT colonography (5 yearly)*Flexible sigmoidoscopy (5 yearly)*Double contrast barium enema (5 yearly)*Colonoscopy (10 yearly)
Increased risk (history of polyps or other risk factors)
Low risk (1–2 adenomas [<10 mm])
Routine screening: fecal occult blood test after polyps removed
Colonoscopy 5–10 years after polyps removed
Intermediate risk (3–4 small adenomas or 1 ≥10 mm)
Colonoscopy 3 years after polyps removed. 1 negative colonoscopy, extend interval to 5 years; 2 consecutive normal exams, return to routine screening
Colonoscopy 3 years after polyps removed
High risk (5 or more adenomas or 1 ≥20 mm)
Colonoscopy within 1 year of removal of polyps, followed by 3 yearly surveillance
Colonoscopy within 3 years of removal of polyps. Consider genetic condition
History of cancer (resected)
pT1 lesions: surveillance as high-risk adenomas
Colonoscopy within 1 year of surgery
Family history (1st degree relative)
Not to be excluded from screening program (commence at 40 years‡)
Commence 5 yearly colonoscopy at age 40
IBD Specific colonoscopy surveillance programs at shorter intervals
Colonoscopy every 1–2 years with biopsies for dysplasia
Hereditary risk
Familial adenomatous polyposis
Specific colonoscopy surveillance programs at shorter intervals with genetic testing clinic
Commence yearly flexible sigmoidoscopy at age 10. Consider colectomy if genetic test positive
Hereditary nonpolyposis CRC
Specific colonoscopy surveillance programs at shorter intervals with genetic testing clinic
Colonoscopy every 1–2 years from age 20. Genetic testing including 1st degree relatives
*Colonoscopy if positive. ‡Barcelona declaration. Abbreviation: CRC, colorectal cancer.
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | GASTROENTEROLOGY & HEPATOLOGY ADVANCE ONLINE PUBLICATION | 3
Barium enemaThe double-contrast barium enema examination has a reported sensitivity of between 85% and 97% for CRCs and 73% for adenomas >7 mm when used as a screening tool.16 However, the bowel preparation involved in this labor-intensive procedure, together with its high cost, has limited its popularity.16 Additionally, a lack of well-designed studies assessing its effectiveness as a screening tool has led to further skepticism, particularly with the introduction of CT colonography. Glick and colleagues19 generated a model of 16 different screening strategies to analyze the cost-effectiveness of the barium enema examination. The model illustrated the cost-effectiveness of the examination every 5 years, but only assuming the reported high sensitivity of early studies.16 However, in a population-based study, Toma and colleagues20 reported the chance of missing a cancer at barium enema examina tion to be one in five.
CT colonographyCT colonography has been recommended by the American College of Gastroenterology as a screening method at an interval of 5 years. Studies have shown sensitivities and specificities for the detection of lesions that are comparable to other screening methods. To date, the effectiveness of this screening tool in reduc-ing CRC mortality and incidence has not been estab-lished, although meta-analyses have confirmed a high sensitivity and specificity for the identification of large polyps (≥10 mm), but not so high for smaller polyps.21,22 An additional disadvantage of CT colonography as a screening tool is the extracolonic findings described in up to 66% of cases, with 16% of individuals requiring further evaluation.23 Reports on the cost- effectiveness of this method as a screening tool in comparison with colonoscopy have been encouraging, although the additional costs associated with investigation and reporting of extra-colonic findings must also be con-sidered.24,25 On the other hand, CT colonography could offer some additional benefits with the opportunistic identification of aortic aneurysm and other specific intra-abdominal conditions.
Flexible sigmoidoscopyFlexible sigmoidoscopy has the advantage that is requires less bowel preparation and usually does not require seda-tion for the patient, but has the disadvantage of only detecting carcinomas or adenomas in the distal colon. The Norwegian Colorectal Cancer Prevention group found no reduction in the incidence of CRC or mortal-ity with flexible sigmoidoscopy screening after 7 years follow up.26 By contrast, a larger-scale study in the UK reported a 33% reduction in CRC incidence and a 43% reduction in mortality in a randomized population of 57,237 individuals undergoing sigmoidoscopy with a median follow-up time of 11 years.27 A similar reduc-tion in both the incidence and mortality of CRC was reported by the Italian randomized controlled SCORE trial, in which individuals aged 55–64 years were ran-domly allocated to receive either flexible sigmoidoscopy
(n = 17,136) or no intervention (n = 17,136).28 On the basis of the UK and Italian studies, a single flexible sigmoido-scopy at age 55 would outperform the FOBT (see below) by a considerable margin. Furthermore, a cost-analysis model demonstrated flexible sigmoidoscopy to be cost saving, with or without the FOBT, whilst acknowledging the considerable investment involved when introducing a new screening option.29
Fecal hemoglobinTable 2 presents a snap-shot view of currently estab-lished diagnostic procedures utilizing molecular markers for CRC. As an inexpensive, noninvasive method, the FOBT is the most widely used screening method for CRC worldwide. In a number of independent studies, screening by FOBT has been shown to be associated with a statistically significant reduction in disease-related mortal ity. For example, a meta-analysis of six trials using the Hemoccult® (Beckman Coulter, Inc., Brea, CA) test reported a 16% reduction in CRC mortality in the popula tions offered screening.30 The traditional FOBT is based upon guaiac detection of peroxidise activ-ity of the heme moiety in fecal specimens and is, there-fore, susceptible to interference from bleeding of both upper and lower gastrointestinal origin. Similarly, inges-tion of certain foods and drugs can yield false-positive results, necessitating a strict 3-day diet that eliminates meats, aspirin and other NSAIDs before sampling. The protocol consists of collecting two samples from three consecutive bowel movements. Positive results require a follow-up colonoscopy for definitive diagnosis. Patient compliance remains an important issue, with up-take rates of only 53.4–66.8% being reported. This problem is exacerbated by the annual or biannual testing required in many screening protocols. Nevertheless, this method is the most popular screening tool to date in Europe. As of 2007, 12 countries are basing their population screening
Box 1 | Challenges of CRC screening practices
Direct investigation of the patient
■ Colonoscopy is an operator-dependent procedure with variable miss rates and a low risk of perforation
■ High costs associated with colonoscopy limit its use in a mass screening program
■ The barium enema examination has a low sensitivity, particularly for small adenomas
■ CT colonography can be associated with a high rate of extracolonic findings requiring further investigation
Investigation of patient specimens
■ The fecal occult blood test (FOBT) is associated with a high false-positive rate, necessitating a strict diet before sampling
■ Poor patient compliance rates are reported with the FOBT
■ Immunochemical FOBT has better sensitivity and specificity although variable sample storage conditions can cause false-negative results
■ The fecal DNA marker examination offers a more robust screening tool; however, cost-effectiveness remains an issue
■ Established serum antigens CEA and CA19-9 show low sensitivity for diagnosis, with CEA offering benefit in disease monitoring
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

4 | ADVANCE ONLINE PUBLICATION www.nature.com/nrgastro
programs on the FOBT, the majority of which organize colonoscopy for positive results.31,32
The immunochemical FOBT relies on specific detec-tion of human hemoglobin in stools, making it more selective for bleeding of colorectal origin. An increase in patient compliance is also expected as no dietary restrictions are required, and sample collection is easier. A more recent version of the immunochemical test determines quantitative levels of hemoglobin in stools. With a threshold of 100 ng hemoglobin per ml, this test has a sensitivity of 76.5% and a specificity of 95.3%, which is similar to colonscopic findings (for adenomas and cancers).33 However, suboptimal conditions of sample storage, particularly increased temperature, can lead to a higher rate of false-negative results with the immunochemical FOBT.34
Results from a French CRC screening program demon strated that immunochemical testing identified twice as many advanced cancers in comparison with the Hemoccult II® FOBT, albeit with a similar specifi-city.35 Van Rossum et al.36 conducted a random popula-tion-based comparative study between the guaiac and immunochemical FOBT and reported a notably higher participation rate for the immunochemical test. The guaiac-based test also substantially underestimated the prevalence of advanced adenomas and cancers. A Spanish study also concluded that the immunochemical test is markedly superior to the guaiac test in detecting advanced adenomas and CRC.37
At present, the immunochemical FOBT remains the preferred option as a FOBT screening tool with its improved patient compliance, better performance and automated quantitative measurement; the test is also probably less costly compared with the traditional guaiac FOBT.38,39 As discussed by Ward et al.,18 the various national screening programs using the FOBT do incur substantial hidden extra costs associated with large
numbers of follow-up colonoscopy investigations. To date, only one randomized controlled trial has assessed the efficacy of the FOBT as a screening method. With a follow-up time of 8 years, and using flexible sigmoido-scopy as a follow-up for positive results, a 32% reduc-tion in rectal cancer mortality was reported, but with no reduction in mortality for colon cancer nor incidence of CRC.40
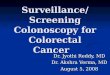
Fecal DNA markersCells shed from the colonic mucosa into the feces can be examined to detect the gene mutations or epi-genetic markers that are the hallmarks of adenomas and carcinomas.41 In contrast to mucosal bleeding, the shedding of colonocytes is believed to be a continuous process; stool-derived DNA markers therefore facili-tate a more robust screening strategy. A panel of DNA markers can be assessed for mutations that arise in the adenoma→carcinoma sequence, typically, APC, KRAS and p53 (Figure 1). This approach requires a larger sample of stool than the FOBT. Recommendations for a 5-year screening interval have been made;41 however, at present, insufficient evidence exists to support this strategy. Imperiale et al.42 conducted a large population-based study that compared fecal DNA testing with the FOBT. The study utilized a DNA marker panel consist-ing of 21 mutations and demonstrated a sensitivity of 52% for invasive cancers and 41% for invasive cancers plus adenomas. These results compare with a sensitiv-ity of 13% (invasive cancers) and 14% (invasive cancers plus adenomas) obtained using the FOBT for the same popula tion. Screening using fecal DNA markers thus demonstrated a higher sensitivity than the FOBT, although the two tests yielded similar specificities.42
Subsequent improvements to fecal DNA testing have led to three distinct changes in this technology: the addition of a DNA stabilization buffer; altering the
Table 2 | Established screening methods for CRC using molecular markers
Marker Sensitivity (%) Specificity (%) Status
Fecal hemoglobin: guaiac fecal occult blood test127,128 15–30, 14.3 95, 79.2 In use
Immunohistochemistry129 94.1 87.5 In use
Serum carcinoembryonic antigen (CEA)130 56 95 In use
Serum CA 19-9131 26 98 In use
Fecal DNA markers (KRAS, APC, L-DNA, p53)132–134 91, 74, 87.5 93, 97, 82 Clinical validation
Cytological assay: circulating tumor cells50,51,135 32, 62, 94 ND, ND, 94 Clinical validation
Abbreviation: ND, not determined.
Normalepithelium
Aberrantcrypts foci
Loss or mutationof APC/β-catenin/
axin genes
Otheralterations
Loss or mutationof p53
Loss or mutationof DCC
Genomicinstability
Mutation of KRAS/BRAF
Earlyadenoma
Intermediateadenoma
Lateadenoma Carcinoma Metastatic
disease
Figure 1 | Temporal sequence of major genetic changes involved in the pathogenesis of colorectal cancer.
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | GASTROENTEROLOGY & HEPATOLOGY ADVANCE ONLINE PUBLICATION | 5
DNA capture assay; and adding a promoter methylation marker for the vimentin gene.23 In a study that compared this second-generation fecal DNA assay with Hemoccult® and Hemoccult SENSA® FOBT, Ahlquist et al.43 reported a 46% detection rate of advanced adenoma and CRC lesions using the DNA test compared with 16% for Hemoccult® and 24% with Hemoccult SENSA®. The inclusion of additional methylation-based gene markers in fecal DNA testing offers the prospect of further improvements in performance.44
Although fecal DNA testing is gaining wider accept-ance as a screening tool, concerns still exist regarding its cost. Song et al.45 used a Markov model to compare cost- effectiveness of various screening methods. The analysis found the FOBT and colonoscopy to be more cost- effective than fecal DNA testing.45 It has been suggested that by using the second-generation fecal DNA testing platform, fewer markers will be necessary, which could potentially reduce the overall cost.46 Further larger-scale studies involving the screening of average-risk popula-tion groups are necessary to validate the cost-benefits of fecal DNA testing.
Cytological assaysThe presence of low levels of circulating tumor cells in the peripheral blood of patients with carcinomas of epithelial origin has been well documented.47–49 In patients with CRC, the detection of such circulat-ing tumor cells is usually associated with progressive or metastatic disease and in some centers is used rou-tinely as a marker of progressive disease and to monitor therapeutic response.48,50–55 Cytological detection of occult peripheral blood tumor cells relies on antibodies to epithelial antigens (typically epithelial cell adhesion molecule [EpCAM] or cyto keratin) that are expressed by cancers of epi thelial origin but are absent from hematopoietic cells.47–49,56 However, the poor sensitiv-ity of commercial cell counting instruments that are based on immuno magnetic bead purifica tion (such as CellSearch® [Johnson and Johnson, New Brunswick, NJ]) precludes their use in population-screening applica-tions; circulating tumor cells are detected in only around 20–60% of patients with metastatic disease using these instruments.53 Combining immunomagnetic purifica-tion with immunocyto chemistry for microscopic detec-tion of gastrointestinal-specific cytokeratin-20- positive cells reportedly detects circulating tumor cells in 62% of patients with CRC.51
A higher sensitivity can be achieved for detecting low cell numbers of circulating occult tumor cells by direct immunofluorescence microscopy of peripheral blood cells using automated image capture and analysis systems.57–59 The development of an automated micro-fluidic ‘lab-on-a-chip’ device for capturing, quanti-tating and analyzing circulating tumor cells directly from a peripheral blood sample should afford an even higher sensitivity and diagnostic accuracy.60,61 Such an instrument would readily lend itself to use in a routine diagnostic laboratory. However, although cytological assays of circulating tumor cells are undeniably of value
in stratifying patients with progressive or metastatic disease and in monitoring therapeutic response,48,50–55 the current level of sensitivity attainable is too low for applications in popula tion screening, particularly for early-stage disease.
Established serum antigen markersThe high molecular weight glycoprotein, carcino-embryonic antigen (CEA), is found in embryonic tissue and colorectal malignancies; it has a half-life of 2 weeks.62 High CEA levels are associated with cancer progression, and levels decrease after resection. However, high levels of CEA can also occur in other malignancies (such as breast, stomach and pancreatic cancer), not to mention IBD, liver disease and pancrea-titis.2,63,64 Its role in screening is limited because levels of this antigen typically do not increase until the tumor has penetrated the serosa, and although levels rise with metastatic liver disease they rarely increase with perito-neal involvement. Fletcher et al.65 demonstrated that by using a cut-off value of 2.5 μg/l, screening of a normal population would result in a sensitivity of 30–40%. In a systematic review by Hundt and colleagues,66 19 studies were included reporting on the performance of CEA for early CRC detection. The overall sensitivity varied between 43% and 69%. A clear increase in the sensitiv-ity was identified with tumor stage; 8% for Stage I up to 89% for Stage IV. A specificity of >90% was reported in 11 studies.66 On the basis of these results, the clinical value of CEA lies more in monitoring disease progres-sion and as a prognostic marker after diagnosis rather than for screening.
The CA19-9 antigen is the second most investigated gastrointestinal tumor marker. Although it is the best available marker for the detection of pancreatic carci-noma, it remains less sensitive for the detection of CRC. A review of 13 studies evaluating its role in the early detection of CRC, using a common cut-off of 37 units/ml, reported overall sensitivities ranging from 18% to 65%, with specificities of >90% in most studies. Unfortunately, comparing sensitivity by tumor stage revealed 0% for Stage I and up to 67% for Stage IV, making it inappropriate as a population screening tool.66
Emerging screening modalitiesProtein markers in serum and plasmaOver the past 10 years, a variety of proteomics-based strategies have been pursued in the quest for serum biomarkers of CRC (Table 3).67 With the limited applic-ability of CEA and CA19-9 antigens, a number of alterna-tive candidate diagnostic protein markers have emerged from studies of the tumor tissue proteome. These include nuclear matrix proteins, CCSA-2, CCSA-3, CCSA-4, matrix metalloproteinase 9, S100A8 and S100A9.68–71 Although the individual sensitivities and specificities of these markers in pilot studies fall short of accept-able performance for population screening, their rela-tive ease of quantitation by immunoassay lends itself to develop ment as part of an extended panel of serum protein biomarkers.
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

6 | ADVANCE ONLINE PUBLICATION www.nature.com/nrgastro
The existence of circulating tumor-associated auto-antigens in patients with cancer has been known for some time. However, only since 2010 have tumor- associated serum autoantibodies been systematically evaluated as potential disease markers.72,73 At least in part, this renewed interest has been facilitated by the availability of high-density protein microarray technologies, based on either commercial protein arrays or phage display expression libraries. Preliminary studies in lung, ovarian and pancreatic cancer illustrate how extended panels of arrayed antigens afford both high sensitivity and speci-ficity in distinguishing patients with cancer from healthy individuals.74,75 In CRC, Badel et al.76 used a commercial protein microarray platform representing 8,000 proteins to identify 43 proteins that are differentially recognized by tumoral and reference sera. In 2009, a diagnostic ELISA based on a combination of two of these proteins (MAPKAPK3 and ACVR2B) yielded specificity and sensi tivity values of 73.9% and 83.3%, respectively, in dis-tinguishing patients with CRC from healthy individuals.76 More recently, the same laboratory identified two further markers from a phage display screen, MST1/STK4 and SULF1, that improve the diagnostic performance of the
assay.77 These studies highlight the potential of serologi-cal analysis of arrays displaying the complete human pro-teome (seromics) for the comprehensive identification of circulating autoantibodies that could be used to develop robust immunoassay screening methods for CRC. This concept is a fairly new area of investigation in the quest for serum markers that could be used as a multiplexed panel in ELISA or other solid phase assay platforms in population screening for CRC. Although considerable development work remains to be done, the approach is particularly attractive because it would ultimately utilize immunoassay-type methodology with its inherent low cost, robustness and established use.
The most intensively investigated field in serum pro-teomics over the past 10 years has been in the applica-tion of surface-enhanced laser desorption–ionization time-of-flight mass spectrometry (SELDI-TOF MS) and matrix-assisted laser desorption–ionization time-of-flight mass spectrometry (MALDI-TOF MS).78 In SELDI-TOF MS, serum or plasma samples are applied directly to protein chip surfaces that differentially retain proteins on the basis of their physicochemical prop-erties. In MALDI-TOF MS, protein samples are first
Table 3 | Emerging molecular marker strategies for CRC screening
Marker Cases Controls Sensitivity (%) Specificity (%)
Serum peptide markers
CCSA-3, CCSA-468 28 107 91 82–91
CCSA-269 27 40 89 84
MMP-970 90 46 78 77
S100A8, S100A971 88 21 41–44 95
MAPKAPK3, ACVR2B76 52 42 83 74
SELDI-TOF136 55 92 91 93
SELDI-TOF137 55 92 89 92
SELDI-TOF85 37 31 65–90 65–90
SELDI-TOF138 62 31 95 91
SELDI-TOF139 55 92 91 93
MALDI-TOF87 66 50 95 90
MALDI-TOF140 66 50 98 96
DNA markers
TMEF2, NGFR, SEPT9107 135 185 30–52 95
SEPT9108 90 155 55–71 86–95
SEPT9141 183 126 72 90
APC, KRAS, p53142 104 50 13-34 100
APC, MLH1, HLTF143 49 41 6–57 90–100
RNA markers
5-gene panel: CDA, MGC20553, BANK1, BCNP1, MS4A1112 43 49 88 64
7-gene panel: ANXA3, CLEC4D, LMNB1, PRRG4, TNFAIP6, VNN1, IL2RB113
202 208 72 70
7-gene panel: ANXA3, CLEC4D, TNFAIP6, LMNB1, PRRG4, VNN1, IL2RB114
99 111 61 77
Fecal microRNA122 10 8 74 79
mRNA-L6144 187 45 79 100
MicroRNA145 90 50 89 70
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | GASTROENTEROLOGY & HEPATOLOGY ADVANCE ONLINE PUBLICATION | 7
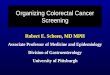
co-crystallized with an energy-absorbing matrix, usually with prior ‘off-line’ purification, before laser irradiation in the mass spectrometer. In both techniques, the laser desorbs the complex mixture of proteins, which are then detected by their mass-to-charge ratio in the time-of-flight analyzer to generate a spectral profile ‘fingerprint’ representing numerous proteins and/or peptides in the sample (Figure 2). In numerous published studies, serum spectral profiles that distinguish between healthy indivi-duals and patients with cancer have been reported.79–82 Similarly, in CRC, both SELDI-TOF MS and MALDI-TOF MS profiling has yielded impressive results in terms of sensitivity and specificity (Table 3).67,83,84 Engwegen
and colleagues85 conducted one of the first studies using SELDI-TOF MS to detect and validate biomarker pro-teins for CRC in serum. Two sets of serum samples were analyzed, the first containing samples from healthy con-trols or patients with stage IV cancer, and the second comprising samples from controls or patients with cancer of all stages. The CRC profiles were then compared with other cancer serum samples. The results identified five biomarker proteins able to reliably distinguish between healthy controls and patients with CRC. Sensitivities and specificities of between 65% and 90% were reported. However, a comparison with other cancer serum samples revealed that these biomarkers were not solely specific for
Acquired spectra
Normal sera
Normalized expressionlevels of discriminatingpeaks
Normalized expressionvalues of matched peaks
Samples
Detector
High voltage
Laser pulse
Positively charged ions
Dataset spreadsheet
MALDI plate
TOF mass spectrometer
45058.0
36082.6
27107.2
18131.8
9158.4
181.01200.05 3159.94 5119.84 7079.74 9039.63 10999.53
a
c d
e
b
CRC seraPredictive model (heat map)
Test sera
Peak massvalues
Serum proteinsamples spotted onplate with matrix
MALDI plate
Sample
Figure 2 | Schematic outline of serum or plasma protein expression profiling by MALDI-TOF mass spectrometry. a | Serum or plasma protein samples from matched healthy controls and from patients with a confirmed diagnosis of CRC are crystallized with a matrix compound as spots on the stainless steel MALDI plate. Test serum samples for screening can also be included. b | In the mass spectrometer, individual sample spots are pulsed with a high energy laser to ionize the complex mixture of proteins and peptides. Under the influence of an electric field, positively charged protein and peptide ions are accelerated down the ‘flight tube’. The speed of flight, and hence time taken to impact the detector is determined by the charge-to-mass (m/z) ratio of the protein. For uniformly charged species, this time interval is proportional mass. c | Detector output time data from multiple laser pulses is converted to a Da mass scale (strictly speaking m/z) that together with recorded amplitude data is represented as a spectrum. d | The spectral graph data is exported as a simple digital text file so that matching peaks and their normalized ion intensities across all samples can be identified. e | Various algorithms can be used to identify ‘diagnostic’ marker peaks whose amplitude discriminates between CRC and normal serum. A diagnosis of test sera is then made by determining whether the amplitude of marker peaks most closely resembles normal or CRC serum. Abbreviations: CRC, colorectal cancer; MALDI-TOF, matrix-assisted laser desorption–ionization time-of-flight.
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

8 | ADVANCE ONLINE PUBLICATION www.nature.com/nrgastro
CRC.85 This apparent lack of specificity for CRC has sub-sequently been confirmed in other studies.86 In another study, De Noo and colleagues87 used MALDI-TOF MS to compare 66 preoperative serum samples from patients who had CRC with 50 samples from healthy controls. 34 of 37 patients with early-stage disease, and all the patients with late-stage disease, were correctly classified as having cancer.87 So far, only one study has investigated the use of SELDI-TOF MS and MALDI-TOF MS profil-ing of proteins in urine from patients with CRC; Ward et al.88 reported a sensitivity of 78% and a specificity of 87% when comparing 67 patients with CRC and 72 non-cancer control patients.
Smith and colleagues89 used SELDI-TOF MS to assess the ability of proteomics in predicting and monitoring the response of patients with locally advanced rectal cancer to neoadjuvant chemoradiotherapy. Sequential serum samples were taken from 20 patients; these samples identi fied a total of 14 protein peaks that collectively differ entiated between good (9) and poor (11) responders with a sensitivity of 87.5% and a specificity of 80%. The study supports the analysis of dynamic tumor responses as an alternative predictive tool.89 A pilot study utilizing MALDI-TOF MS profiling of preoperative and post-operative serum from patients with CRC suggests that this technique might also be useful in monitoring disease course in patients after surgery.90
As discussed by Petricoin et al.,91 the ‘tumor-specific’ proteins (as detected by MALDI-TOF MS and SELDI-TOF MS) do not, in most cases, represent genuine biomarkers. In the few cases in which the identities of discriminating protein peaks have been determined, they have been found to comprise degradation products of larger, usually abundant serum proteins. The origin of the tumor- specific ‘peptidome/degradome’ in cancer sera seems to arise from the actions of specific proteases, most likely released from tumor-associated stromal cells. Although this finding does not invalidate their value as diagnostic markers, the reliability and reproducibil-ity of SELDI-TOF MS and, to a lesser extent, MALDI-TOF MS platforms has, however, attracted consider able criticism. As discussed elsewhere, these concerns arise from considera tions of sample storage and processing, instrumenta tion (particularly with older SELDI-TOF instruments) and in bio informatics data analysis culmi-nating in statistical ‘overfitting’ of predictive models.78,92,93 In addition, such studies in CRC have so far been limited to relatively small-scale patient cohorts, sometimes without appropriate matched controls. Although the technique is low-cost in terms of reagents and lends itself to high-throughput semi- automated sample pro-cessing, it suffers the drawback of being inherently semi- quantitative at best. In addition, a high level of technical skill is required in quality control and data analysis and interpretation. Hence, most authorities would not envisage SELDI-TOF MS or MALDI-TOF MS instru-mentation platforms, at least in their present form, being used in routine (population) screening of serum samples. Despite these reservations, the technique still represents a worthwhile approach for the discovery and
identification of serum markers for CRC that can subse-quently be utilized in population screening using more robust immuno sorbent assays.
Under the auspices of the Human Plasma Proteome Project (HUPO), the efforts of numerous collaborating laboratories are being facilitated by advances in instru-mentation of tandem mass spectrometers to elucidate the complete protein composition of human plasma. To date, around 10,000 proteins have been identified.94 Given that accurate quantitation of protein abundance is now routinely achievable using this type of mass spectro-meter, it seems highly likely that this resource will have a major effect on the identification of diagnostic plasma protein markers for many cancer types.95 The resolution capabilities of advanced tandem mass spectrometers, when coupled with upstream purification, far exceeds that of conventional MALDI-TOF MS or SELDI-TOF MS, and is particularly suited to high throughput, multi plexed detection and quantitation of discriminat-ing protein and peptide biomarkers that are likely to be of low abundance.96 Translating such biomarker discov-ery into an inexpensive ‘lab-on-a-chip’ test kit will be greatly facilitated by technologies for multiplexed analy-sis using integrated barcode chips, detecting proteins in the subfemtomolar concentration range by using single- molecule ELISA and magnetic nanosensor platforms with resolution down to attomolar concentrations and extensive linear dynamic range.97–99
DNA markers in serum and plasmaAs with circulating tumor cells, free plasma nucleic acid of tumor cell origin has been well documented to occur in patients with a number of cancer types, although its representation is very low compared with DNA and RNA of non-tumor origin.100,101 Nonetheless, it does rep-resent a potential source of tumor biomarkers.102 With the advent of massively parallel sequencing combined with accurate quantitation by PCR amplification, Diehl et al.103 were able to precisely quantitate levels of plasma DNA of tumor origin in patients with CRC by using a panel of somatic mutations in genes that are commonly mutated in this disease (TP53, KRAS, APC and PIK3CA) (Figure 1). This method enabled the tumor dynamics in individual patients to be monitored after surgery or chemotherapy. Leary et al.104 used a different approach to identify tumor-specific translocations that were then used as markers for monitoring levels of circulating tumor-specific DNA in a small cohort of patients with CRC or breast cancer. Finally, He et al.105 showed that heteroplasmic mutations in mitochondrial DNA occur in CRC tumor cells and, by virtue of the high copy number of mitochondrial DNA (relative to nuclear DNA), can be readily detected and quantified in patient’s plasma. However, how useful these approaches would be for population screening in CRC is not clear; apart from the prohibitive cost, a priori knowledge of the target muta-tions in individual patient’s tumor cells is required. This methodology is likely to be most useful for ‘personal-ized’ monitoring of treatment response and for stratify-ing patients using markers such as KRAS mutations that
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | GASTROENTEROLOGY & HEPATOLOGY ADVANCE ONLINE PUBLICATION | 9
are predictive of poor response to therapies targeting the epidermal growth factor receptor.106
As an alternative to using gene mutations as markers, several studies have exploited tumor-associated epi-genetic methylation changes as markers to detect cir-culating plasma DNA of tumor origin.107 A simple PCR-based assay of plasma to detect methylation of SEPT9 reportedly identifies patients with CRC with a sensitivity of 70% and a specificity of 90%.108,109 This performance compares favorably with both the FOBT and PCR screening of fecal DNA. The assay can also be automated and is now commercially available as the Epi proColon Early Detection Assay kit® (Epigenomics, Berlin, Germany).109 The addition of further markers to this blood screen test might further improve its perform-ance in the future.110 However, its high cost does not compare favorably with an inexpensive annual FOBT and decadal colonoscopy.109
RNA markers in blood cells, plasma and fecesThe peripheral blood transcriptome is a potential source of discriminating diagnostic markers for a number of diseases.111 By microarray gene expression profiling of leukocyte mRNA, Han et al.112 generated a five-gene discriminating marker panel (CDA, MGC20553, BANK1, BCNP1 and MS4A1) from genes that were differ entially expressed between blood cells of patients with CRC and healthy individuals. The reported sensitivity was 88% with a specificity of 64% on an independent test set of normal and CRC samples.112 In a subsequent study, a seven-gene marker panel (ANXA3, CLEC4D, LMNB1, PRRG4, TNFAIP6, VNN1 and IL2RB) had a sensitivity of 82% and a specificity of 64%.113 Although the diag-nostic performance in both studies was comparable, the absence of any overlap between the two diagnostic marker panels highlights the well-recognized ‘instabil-ity’ problem that afflicts classification based on gene markers obtained from differential expression profil-ing. The seven-gene marker panel has been validated in an independent popula tion study with a reported perform ance of 61% and 77% for sensitivity and specificity, respectively.114
MicroRNAs (miRNAs) have attracted considerable attention as diagnostic or prognostic markers when applied to tumor tissue from many cancers, includ-ing CRC,115,116 and circulating miRNAs are emerging as potential biomarkers for population screening.117,118 One study has shown that circulating plasma miRNA levels in patients with gastric cancers largely reflect those in matched tumor tissue; two miRNAs in particular (miR-106b and miR-106a/let-7a) discriminate between normal and gastric cancer plasma with high sensitivity and specificity (receiver-operating characteristic curve: 0.721 for miR-106b and 0.879 for miR-106a/let-7a).119 Studies in CRC have shown that circulating levels of miRNA-29a, miRNA-92a and miRNA-17 display a statisti cally significant increase in CRC plasma com-pared with controls.120,121 Quantitation of plasma miRNA markers thus offers a worthwhile avenue for future investigation as an approach for CRC screening. Finally,
miRNA seems to be remarkably well-preserved in exfoli-ated colonocytes from feces. The stools of patients with CRC reportedly display unique and identifiable patterns of miRNA expression. In a preliminary study, miRNA expression profiling gave an overall sensitivity and specificity of 74.1% and 79.0%, respectively.122
ConclusionsDespite major investment and important scientific advancements over the past 15 years, very few new bio-markers for cancer diagnosis have so far been approved for clinical use.123,124 For CRC screening, established pro-grams with proven, albeit less-than-ideal efficacy, such as the FOBT and patient-centric investigative procedures, are likely to remain in place for some years to come. Indeed, the potential of low-cost flexible sigmoidoscopy for statistically significant reduction in the incidence and mortality of CRC27,28 illustrates how evidence-based approaches in conventional screening programs can have a remarkable effect without the need for major investment in basic science and subsequent clinical validation, with its attendant less-than-certain outcome. Nonetheless, on the basis of the numerous precedents of the paradigm shift of conventional diagnostics towards molecular diagnostics in the health-care sector, it seems likely that population screening for CRC using molecular markers will eventually replace conventional methods. Herein lies a dilemma—of the plethora of different strategies that are currently being developed and evaluated, there is no obvious clear ‘winner’ at the present time; none of methods have been evaluated beyond proof-of-principle and pilot-scale study.
This field is rapidly progressing, however, with major new advances being made every year. From the view-point of patient compliance, a blood-sampling-based test is clearly preferable to a stool test. Markers based on nucleic acid are usually more readily translatable into a test-kit platform but, together with cytological detection, might have theoretical limits of predictive accuracy. Nucleic acid detection is also quite costly, particularly when it involves a PCR procedure. Plasma protein markers, on the other hand, offer considerably more potential, at least in the longer term, for two main reasons. First, only a small fraction of the total human ‘plasmasome’ has so far been explored, and therefore an enormous untapped reservoir of potential disease markers is waiting to be discovered. These potential disease markers include not only the individual plasma proteins and peptides themselves but also a vast diver-sity of their post-translationally modified derivatives. Second, diagnostic immunoassay test kits for proteins have been in widespread use for many years in a variety of health-care settings. They are generally robust and inexpensive to mass-produce. In addition, the technol-ogy for more sensitive, second-generation protein assay platforms already exists.97–99 It seems likely that the introduction of molecular marker screening methods will be an incremental process over the next few years. Moreover, national health-care programs are unlikely to divert resources away from conventional screening
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

10 | ADVANCE ONLINE PUBLICATION www.nature.com/nrgastro
methods that have taken many years of planning and infrastructure investment to establish. It is therefore probable that the implementation of new technology for popula tion screening in CRC will rely heavily on the activities of the commercial biopharmceutical sector rather than on publicly funded ventures, particularly during a period of global economic austerity.
Review criteria
Published original articles (full-text in English) on which this review is based were identified by PubMed and MEDLINE searches using the keywords “colorectal cancer ‘AND’ screening”. Additional articles were retrieved by citation searches in Web-of-Science (Thomson Reuters).
1. Weitz, J. et al. Colorectal cancer. Lancet 365, 153–165 (2005).
2. Cancer Research UK. Bowel cancer statistics—UK. Cancer Research UK [online], http://info.cancerresearchuk.org/cancerstats/types/bowel/symptomsandtreatment/ (2011).
3. Kim, H. J., Yu, M. H., Kim, H., Byun, J. & Lee, C. Noninvasive molecular biomarkers for the detection of colorectal cancer. BMB Rep. 41, 685–692 (2008).
4. Verdecchia, A. et al. Recent cancer survival in Europe: a 2000–2002 period analysis of EUROCARE-4data. Lancet Oncol. 8, 784–796 (2007).
5. Gupta, A. K., Brenner, D. E. & Turgeon, D. K. Early detection of colon cancer: new tests on the horizon. Mol. Diag. Ther. 12, 77–85 (2008).
6. Burt, R. W. Colorectal cancer screening. Curr. Opin. Gastroenterol. 26, 466–470 (2010).
7. Hofstad, B. in Colonoscopy: Principles and Practice 1st edn (eds Waye, J. D., Rex, D. K., Williams, C. B.) 358–376 (Wiley-Blackwell, Oxford, 2003).
8. Ahlquist, D. A. Molecular detection of colorectal neoplasia. Gastroenterology 138, 2127–2139 (2010).
9. Lieberman, D. Progress and challenges in colorectal cancer screening and surveillance. Gastroenterology 138, 2115–2126 (2010).
10. Regula, J. et al. Colonoscopy in colorectal cancer screening for detection of advanced neoplasia. N. Engl. J. Med. 355, 1863–1872 (2006).
11. Kahi, C. J., Imperiale, T. F., Juliar, B. E. & Rex, D. K. Effect of screening colonoscopy on colorectal cancer incidence and mortality. Clin. Gastroenterol. Hepatol. 7, 770–775 (2009).
12. Rabeneck, L., Paszat, L. F., Saskin, R. & Stukel, T. A. Association between colonoscopy rates and colorectal cancer mortality. Am. J. Gastroenterol. 105, 1627–1632 (2010).
13. Baxter, N. N. et al. Association of colonoscopy and death from colorectal cancer. Ann. Intern. Med. 150, 1–8 (2009).
14. Brenner, H. et al. Protection from right- and left-sided colorectal neoplasms after colonoscopy: population-based study. J. Natl Cancer Inst. 102, 89–95 (2010).
15. The Northern-European Initiative on Colorectal Cancer (NordICC). ClinicalTrials.gov [online], http://clinicaltrials.gov/ct2/show/NCT00883792 (2011).
16. Nelson, S. R. & Thorson, A. G. Colorectal cancer screening. Curr. Oncol. Rep. 11, 482–489 (2009).
17. Ransohoff, A. F. How much does colonoscopy reduce colon cancer mortality? Ann. Intern. Med. 150, 50–52 (2009).
18. Ward, N., Wright, J., Marsh, S. & Norton, J. Fast track referrals for colorectal cancer: impact of the faecal occult blood test screening programme. Colorectal Dis. 9, 258–261 (2007).
19. Glick, S., Wagner, J. L. & Johnson, C. D. Cost-effectiveness of double contrast barium enema in screening for colorectal cancer. AJR Am. J. Roentgenol. 170, 629–636 (1998).
20. Toma, J., Paszat, L. F., Gunraj, N. & Rabeneck, L. Rates of new or missed colorectal cancer after
barium enema and their risk factors: a population based study. Am. J. Gastroenterol. 103, 3142–3148 (2008).
21. Sosna, J. et al. CT colonography of colorectal polyps: a metaanalysis. AJR Am. J. Roentgenol. 181, 1593–1598 (2003).
22. Rosman, A. S. & Korsten, M. A. Meta-analysis comparing CT colonography, air contrast barium enema, and colonoscopy. Am. J. Med. 120, 203–210 (2007).
23. Vu, H. T. & Burke, C. A. Advances in colorectal cancer screening. Curr. Gastroenterol. Rep. 11, 406–412 (2009).
24. Knudsen, A. B. et al. Cost-effectiveness of computed tomographic colonography screening for colorectal cancer in the medicare population. J. Natl Cancer Inst. 102, 1238–1252 (2010).
25. Sweet, A. et al. The impact of CT colonography for colorectal cancer screening on the UK NHS: costs, healthcare resources and health outcomes. Appl. Health Econ. Health Policy 9, 51–64 (2011).
26. Hoff, G., Grotmol, T., Skovlund, E. & Bretthauer, M. & Norwegian Colorectal Cancer Prevention Study Group. Risk of colorectal cancer seven years after flexible sigmoidoscopy screening: randomised controlled trial. BMJ 338, b1846 (2009).
27. Atkin, W. S. et al. Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicentre randomised controlled trial. Lancet 375, 1624–1633 (2010).
28. Segnan, N. et al. Once-only sigmoidoscopy in colorectal cancer screening: follow-up findings of the Italian randomized controlled trial—SCORE. J. Natl Cancer Inst. 103, 1310–1322 (2011).
29. Tappenden, P. et al. Option appraisal of population-based colorectal cancer screening programmes in England. Gut 56, 677–684 (2007).
30. Towler, B. et al. A systematic review of the effects of screening for colorectal cancer using the faecal occult blood test, hemoccult. BMJ 317, 559–565 (1998).
31. Zavoral, M. et al. Colorectal cancer screening in Europe. World J. Gastroenterol. 15, 5907–5915 (2009).
32. West, N. J., Boustiere, C., Fischbach, W., Parente, F. & Leicester, R. Colorectal cancer screening in Europe: differences in approach; similar barriers to overcome. Int. J. Colorectal Dis. 24, 731–740 (2009).
33. Vilkin, A. et al. Performance characteristics and evaluation of an automated-developed and quantitative, immunochemical, fecal occult blood screening test. Am. J. Gastroenterol. 100, 2519–2525 (2005).
34. Grazzini, G. et al. Influence of seasonal variations in ambient temperature on performance of immunochemical faecal occult blood test for colorectal cancer: observational study from the Florence district. Gut 59, 1511–1515 (2010).
35. Guittet, L. et al. Comparison of a guaiac based and an immunochemical faecal occult blood test in screening for colorectal cancer in a general average risk population. Gut 56, 210–214 (2007).
36. Van Rossum, L. G. et al. Random comparison of guaiac and immunochemical fecal occult blood tests for colorectal cancer in a screening population. Gastroenterology 135, 82–90 (2008).
37. Parra-Blanco, A. et al. Diagnostic accuracy of immunochemical versus guaiac faecal occult blood tests for colorectal cancer. J. Gastroenterol. 45, 703–712 (2010).
38. Li, S. et al. New immunochemical fecal occult blood test with two-consecutive stool sample testing is a cost-effective approach for colon cancer screening: results of a prospective multicenter study in Chinese patients. Int. J. Cancer 118, 3078–3083 (2006).
39. Parekh, M., Fendrick, A. M. & Ladabaum, U. As tests evolve and costs of cancer care rise: reappraising stool-based screening for colorectal neoplasia. Aliment. Pharmacol. Ther. 27, 697–712 (2008).
40. Zheng, S. et al. Cluster randomization trial of sequence mass screening for colorectal cancer. Dis. Colon Rectum 46, 51–58 (2003).
41. Potack, J. & Itzkowitz, S. H. Practical advances in stool screening for colorectal cancer. J. Natl Comp. Canc. Netw. 8, 81–92 (2010).
42. Imperiale, T. F. et al. Fecal DNA versus fecal occult blood for colorectal cancer screening in an average risk population. N. Engl. J. Med. 351, 2704–2714 (2004).
43. Ahlquist, D. A. et al. Stool DNA and occult blood testing for screen detection of colorectal neoplasia. Ann. Intern. Med. 149, 441–450 (2008).
44. Goel, A. DNA methylation-based fecal biomarkers for non-invasive screening of GI cancers. Future Oncol. 6, 333–336 (2010).
45. Song, K., Fendrick, A. M. & Ladabaum, U. Fecal DNA testing compared with conventional colorectal cancer screening methods: a decision analysis. Gastroenterology 126, 1270–1279 (2004).
46. Itzkowitz, S. et al. A simplified, noninvasive stool DNA test for colorectal cancer detection. Am. J. Gastroenterol. 103, 2862–2870 (2008).
47. Paterlini-Brechot, P. & Benali, N. L. Circulating tumor cells (CTC): detection, clinical impact and future directions. Cancer Lett. 253, 180–204 (2007).
48. Sleijfer, S. et al. Circulating tumour cell detection on its way to routine diagnostic implementation. Eur. J. Cancer 43, 2645–2650 (2007).
49. Pantel, K., Brakenhoff, R. H. & Brandt, B. Detection, clinical relevance and specific biological properties of disseminating tumour cells. Nat. Rev. Cancer 8, 329–340 (2008).
50. Sastre, J. et al. Circulating tumor cells in colorectal cancer: correlation with clinical and pathological variables. Ann. Oncol. 19, 935–938 (2008).
51. Wong, S. C. et al. Clinical significance of cytokeratin 20-positive circulating tumor cells detected by a refined immunomagnetic enrichment assay in colorectal cancer patients. Clin. Cancer Res. 15, 1005–1012 (2009).
52. Negin, B. P. & Cohen, S. J. Circulating tumor cells in colorectal cancer: past, present and future
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | GASTROENTEROLOGY & HEPATOLOGY ADVANCE ONLINE PUBLICATION | 11
challenges. Curr. Treat. Options Oncol. 11, 1–13 (2010).
53. Allen, J. E. & El-Deiry, W. S. Circulating tumor cells and colorectal cancer. Curr. Colorectal Cancer Rep. 6, 212–220 (2010).
54. Cohen, S. J. et al. Relationship of circulating tumor cells to tumor response, progression-free survival and overall survival in patients with metastatic colorectal cancer. J. Clin. Oncol. 26, 3213–3221 (2008).
55. Tol, J. et al. Circulating tumour cells early predict progression-free and overall survival in advanced colorectal cancer patients treated with chemotherapy and targeted agents. Ann. Oncol. 21, 1006–1012 (2010).
56. Antolovic, D. et al. Heterogenous detection of circulating tumor cells in patients with colorectal cancer by immunomagnetic enrichment using different EpCAM-specific antibodies. BMC Biotechnol. 10, 35 (2010).
57. Krivacic, R. T. et al. A rare-cell detector for cancer. Proc. Natl Acad. Sci. USA 101, 10501–10504 (2004).
58. Kraeft, S. K. et al. Reliable and sensitive identification of occult tumor cells using the improved rare event imaging system. Clin. Cancer Res. 10, 3020–3028 (2004).
59. Marrinucci, D. et al. Cytomorphology of circulating colorectal tumor cells: a small case series. J. Oncol. 861341 (2010).
60. Nagrath, S. et al. Isolation of rare circulating tumour cells in cancer patients by microchip technology. Nature 450, 1235–1239 (2007).
61. Stott, S. L. et al. Isolation and characterization of circulating tumor cells from patients with localized and metastatic prostate cancer. Sci. Transl. Med. 2, 25ra23 (2010).
62. Huerta, S. Recent advances in the molecular diagnosis and prognosis of colorectal cancer. Expert Rev. Mol. Diagn. 8, 277–288 (2008).
63. Wanebo, H. J. et al. Preoperative carcinoembryonic antigen level as a prognostic indicator in colorectal cancer. N. Engl. J. Med. 299, 448–451 (1978).
64. Posner, M. R. & Mayer, R. J. The use of serologic tumor markers in gastrointestinal malignancies. Hematol. Oncol. Clin. North Am. 8, 533–553 (1994).
65. Fletcher, R. H. Carcinoembryonic antigen. Ann. Intern. Med. 104, 66–73 (1986).
66. Hundt, S., Haug, U. & Brenner, H. Blood markers for early detection of colorectal cancer: a systematic review. Cancer Epidemiol. Biomarkers Prev. 16, 1935–1953 (2007).
67. Tjalsma, H. Identification of biomarkers for colorectal cancer through proteomics-based approaches. Expert Rev. Proteomics 7, 879–895 (2010).
68. Leman, E. S. et al. Initial analysis of colon cancer-specific antigen CCSA-3 and CCSA-4 as colorectal cancer-associated serum markers. Cancer Res. 67, 5600–5605 (2007).
69. Walgenbach-Brunagel, G. et al. The use of a colon cancer associated nuclear antigen CCSA-2 for the blood-based detection of colon cancer. J. Cell. Biochem. 104, 286–294 (2008).
70. Hurst, N. G. et al. Elevated serum matrix metalloproteinase 9 (MMP-9) concentration predicts the presence of colorectal cancer in symptomatic patients. Br. J. Cancer 97, 971–977 (2007).
71. Kim, H. J. et al. Identification of S100A8 and S100A9 as serological markers for colorectal cancer. J. Proteome Res. 8, 1368–1379 (2009).
72. Kobold, S., Luetkens, T., Cao, Y., Bokemeyer, C. & Atanackovic, D. Prognostic and diagnostic value of spontaneous tumor-related antibodies. Clin. Dev. Immunol. 721531 (2010).
73. Casal, J. I. & Barderas, R. Identification of cancer autoantigens in serum: toward diagnostic/prognostic testing? Mol. Diagn. Ther. 14, 149–154 (2010).
74. Leidinger, P. et al. Identification of lung cancer with high sensitivity and specificity by blood testing. Respir. Res. 11, 18 (2010).
75. Gnjatic, S. et al. Seromic profiling of ovarian and pancreatic cancer. Proc. Natl Acad. Sci. USA 107, 5088–5093 (2010).
76. Babel, I. et al. Identification of tumor-associated autoantigens for the diagnosis of colorectal cancer in serum using high density protein microarrays. Mol. Cell. Proteomics 8, 2382–2395 (2009).
77. Babel, I. et al. Identification of MST1/STK4 and SULF1 proteins as autoantibody targets for the diagnosis of colorectal cancer by using phage microarrays. Mol. Cell. Proteomics 10, M110.001784 (2011).
78. De Bock, M. et al. Challenges for biomarker discovery in body fluids using SELDI-TOF MS. J. Biomed. Biotechnol. 2010, 9606082 (2010).
79. Adam, B. L. et al. Serum protein fingerprinting coupled with a pattern-matching algorithm distinguishes prostate cancer from benign prostate hyperplasia and healthy men. Cancer Res. 62, 3609–3614 (2002).
80. Petricoin, E. F. et al. Use of proteomic patterns in serum to identify ovarian cancer. Lancet 359, 572–575 (2002).
81. Li, J., Zhang, Z., Rosenzweig, J., Wang, Y. Y. & Chan, D. W. Proteomics and bioinformatics approaches for identification of serum biomarkers to detect breast cancer. Clin. Chem. 48, 1296–1304 (2002).
82. Honda, K. et al. Possible detection of pancreatic cancer by plasma protein profiling. Cancer Res. 65, 10613–10622 (2005).
83. McHugh, S. M., O’Donnell, J. & Gillen, P. Genomic and oncoproteomic advances in detection and treatment of colorectal cancer. World J. Surg. Oncol. 7, 36 (2009).
84. Huijbers, A. et al. Proteomic serum biomarkers and their potential application in cancer Screening Programs. Int. J. Mol. Sci. 11, 4175–4193 (2010).
85. Engwegen, J. Y. et al. Identification of serum proteins discriminating colorectal cancer patients and healthy controls using surface-enhanced laser desorption ionisation-time of flight mass spectrometry. World J. Gastroenterol. 12, 1536–1544 (2006).
86. Wang, Q. et al. Limitations in SELDI-TOF MS whole serum proteomic profiling with IMAC surface to specifically detect colorectal cancer. BMC Cancer 9, 287 (2009).
87. De Noo, M. E. et al. Detection of colorectal cancer using MALDI-TOF serum protein profiling. Eur. J. Cancer 42, 1068–1076 (2006).
88. Ward, D. G. et al. Proteomic profiling of urine for the detection of colon cancer. Proteome Sci. 6, 19 (2008).
89. Smith, F. M. et al. Combination of SELDI-TOF MS and data mining provides early-stage response prediction for rectal tumors undergoing multimodal neoadjuvant therapy. Ann. Surg. 245, 259–266 (2007).
90. Liao, C. C. et al. Analysis of post-operative changes in serum protein expression profiles from colorectal cancer patients by MALDI-TOF mass spectrometry: a pilot methodological study. World J. Surg. Oncol. 8, 33 (2010).
91. Petricoin, E. F., Belluco, C., Araujo, R. P. & Liotta, L. A. The blood peptidome: a higher dimension of information content for cancer biomarker discovery. Nat. Rev. Cancer 6, 961–967 (2006).
92. Albrethsen, J. Reproducibility in protein profiling by MALDI-TOF mass spectrometry. Clin. Chem. 53, 852–858 (2007).
93. Karsan, A. et al. Analytical and pre-analytical biases in serum proteomic pattern analysis for breast cancer diagnosis. Clin. Chem. 51, 1525–1528 (2005).
94. Omenn, G. S., Aebersold, R. & Paik, Y. K. 7(th) HUPO World Congress of Proteomics: launching the second phase of the HUPOPlasma Proteome Project (PPP-2) 16–20 August 2008, Amsterdam, The Netherlands. Proteomics 9, 4–6 (2009).
95. Vogel, C. & Marcotte, E. M. Absolute abundance for the masses. Nat. Biotechnol. 27, 825–826 (2009).
96. Whiteaker, J. R. et al. A targeted proteomics-based pipeline for verification of biomarkers in plasma. Nat. Biotechnol. 29, 625–634 (2011).
97. Fan, R. et al. Integrated barcode chips for rapid, multiplexed analysis of proteins in microliter quantities of blood. Nat. Biotechnol. 26, 1373–1378 (2008).
98. Rissin, D. M. et al. Single-molecule enzyme-linked immunosorbent assay detects serum proteins at subfemtomolar concentrations. Nat. Biotechnol. 28, 595–599 (2010).
99. Gaster, R. S. et al. Matrix-insensitive protein assays push the limits of biosensors in medicine. Nat. Med. 15, 1327–1332 (2009).
100. Fleischhacker, M. & Schmidt, B. Circulating nucleic acids (CNAs) and cancer—a survey. Biochim. Biophys. Acta 1775, 181–232 (2007).
101. Vlassov, V. V., Laktionov, P. P. & Rykova, E. Y. Circulating nucleic acids as a potential source for cancer biomarkers. Curr. Mol. Med. 10, 142–165 (2010).
102. Schwarzenbach, H., Hoon, D. S. & Pantel, K. Cell-free nucleic acids as biomarkers in cancer patients. Nat. Rev. Cancer 11, 426–437 (2011).
103. Diehl, F. et al. Circulating mutant DNA to assess tumor dynamics. Nat. Med. 14, 985–990 (2008).
104. Leary, R. J. et al. Development of personalized tumor biomarkers using massively parallel sequencing. Sci. Transl. Med. 2, 20ra14 (2010).
105. He, Y. et al. Heteroplasmic mitochondrial DNA mutations in normal and tumour cells. Nature 464, 610–614 (2010).
106. Holdhoff, M., Schmidt, K., Donehower, R. & Diaz, L. A. Jr. Analysis of circulating tumor DNA to confirm somatic KRAS mutations. J. Natl Cancer Inst. 101, 1284–1285 (2009).
107. Lofton-Day, C. et al. DNA methylation biomarkers for blood-based colorectal cancer screening. Clin. Chem. 54, 414–423 (2008).
108. deVos, T. et al. Circulating methylated SEPT9 DNA in plasma is a biomarker for colorectal cancer. Clin. Chem. 55, 1337–1346 (2009).
109. Mullard, A. Epigenomic colon cancer kit. Nat. Biotechnol. 27, 1066 (2009).
110. Tänzer, M. et al. Performance of epigenetic markers, SEPT9 and ALX4 in plasma for detection of colorectal precancerous lesions. PLoS ONE 5, e9061 (2010).
111. Liew, C. C., Ma, J., Tang, H. C., Zheng, R. & Dempsey, A. A. The peripheral blood transcriptome dynamically reflects system wide biology: a potential diagnostic tool. J. Lab. Clin. Med. 147, 126–132 (2006).
112. Han, M. et al. Novel blood-based five gene biomarker set for the detection of colorectal cancer. Clin. Cancer Res. 14, 455–460 (2008).
113. Marshall, K. W. et al. A blood-based biomarker panel for stratifying current risk for colorectal cancer. Int. J. Cancer 126, 1177–1186 (2010).
114. Yip, K. T. et al. A case-controlled validation study of a blood-based seven-gene biomarker panel for
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

12 | ADVANCE ONLINE PUBLICATION www.nature.com/nrgastro
colorectal cancer in Malaysia. J. Exp. Clin. Cancer Res. 29, 128 (2010).
115. Song, B. & Ju, J. Impact of miRNAs in gastrointestinal cancer diagnosis and prognosis. Expert Rev. Mol. Med. 12, e33 (2010).
116. Dong, Y. et al. MicroRNA dysregulation in colorectal cancer: a clinical perspective. Br. J. Cancer 104, 893–898 (2011).
117. Aslam, M. I., Taylor, K., Pringle, J. H. & Jameson, J. S. MicroRNAs are novel biomarkers for colorectal cancer. Br. J. Surg. 96, 702–710 (2009).
118. Mostert, B., Sieuwerts, A. M., Martens, J. W. & Sleijer, S. Diagnostic applications of cell-free and circulating tumor cell-associated miRNAs in cancer patients. Expert Rev. Mol. Diagn. 11, 259–275 (2011).
119. Tsujiura, M. et al. Circulating microRNAs in plasma of patients with gastric cancers. Br. J. Cancer 102, 1174–1179 (2010).
120. Huang, Z. et al. Plasma microRNAs are promising novel biomarkers for early detection of colorectal cancer. Int. J. Cancer 127, 118–126 (2010).
121. Ng, E. K. et al. Differential expression of microRNAs in plasma of patients with colorectal cancer: a potential marker for colorectal cancer screening. Gut 58, 1375–1381 (2009).
122. Link, A. et al. Fecal MicroRNAs as novel biomarkers for colon cancer screening. Cancer Epidemiol. Biomarkers Prev. 19, 1766–1774 (2010).
123. Diamandis, E. P. Cancer biomarkers: can we turn recent failures into success? J. Natl Cancer Inst. 102, 1462–1467 (2010).
124. Hanash, S. M., Baik, C. S. & Kallioniemi, O. Emerging molecular biomarkers—blood-based strategies to detect and monitor cancer. Nat. Rev. Clin. Oncol. 8, 142–150 (2011).
125. European Commission. European guidelines for quality assurance in colorectal cancer screening and diagnosis 1st edition. UEGF [online], http://www.uegf.org/eu_affairs/eu_news/CRC_guidelines_publication%20EU_2011.pdf (2010).
126. American Cancer Society. American Cancer Society recommendations for colorectal cancer early detection (People at increased or high risk). American Cancer Society [online], http://
www.cancer.org/Cancer/ColonandRectumCancer/MoreInformation/ColonandRectumCancerEarlyDetection/colorectal-cancer-early-detection-acs-recommendations (2011).
127. Pignone, M., Rich, M., Teutsch, S. M., Berg, A. O. & Lohr, K. N. Screening for colorectal cancer in adults at average risk: a summary of the evidence for the US preventative services task force. Ann. Intern. Med. 137, 132–141 (2002).
128. Sung, J. J. et al. Screening for colorectal cancer in Chinese: comparison of fecal occult blood test, flexible sigmoidoscopy, and colonoscopy. Gastroenterology 124, 608–614 (2003).
129. Levi, Z. et al. A quantitative immunochemical fecal occult blood test for colorectal neoplasia. Ann. Intern. Med. 146, 244–255 (2007).
130. Fernandes, L. C., Kim, S. B. & Matos, D. Cytokeratins and carcinoembryonic antigen in diagnosis, staging and prognosis of colorectal adenocarcinoma. World J. Gastroenterol. 11, 645–648 (2005).
131. Carpelan-Holmstrom, M. et al. Estimating the probability of cancer with several tumor markers in patients with colorectal disease. Oncology 66, 296–302 (2004).
132. Ahlquist, D. A. et al. Colorectal cancer screening by detection of altered human DNA in stool: feasibility of a multitarget assay panel. Gastroenterology 119, 1219–1227 (2000).
133. Calistri, D. et al. Fecal multiple molecular tests to detect colorectal cancer in stool. Clin. Gastroenterol. Hepatol. 1, 377–383 (2003).
134. Itzkowitz, S. H. et al. Improved fecal DNA test for colorectal cancer screening. Clin. Gastroenterol. Hepatol. 5, 111–117 (2007).
135. Wang, J. Y. et al. Development and evaluation of a colorimetric membrane-array method for the detection of circulating tumor cells in the peripheral blood of Taiwanese patients with colorectal cancer. Int. J. Mol. Med. 17, 737–747 (2006).
136. Chen, Y. D., Zheng, S., Yu, J. K. & Hu, X. Artificial neural networks analysis of surface enhanced laser desorption/ionisation mass spectra of serum protein pattern distinguishes colorectal cancer from healthy population. Clin. Cancer Res. 10, 8380–8385 (2004).
137. Yu, J. K., Chen, Y. D. & Zheng, S. An integrated approach to the detection of colorectal cancer utilizing proteomics and bioinformatics. World J. Gastroenterol. 10, 3127–3131 (2004).
138. Ward, D. G. et al. Identification of serum biomarkers for colon cancer by proteomic analysis. Br. J. Cancer 94, 1898–1905 (2006).
139. Chen, Y. D., Xie, P. P., Yu, J. W., Zhou, J. & Zheng, S. Classification and diagnostic prediction of colorectal cancer using protein profiling of serum and bioinformatics [Chinese]. Zhejiang Da Xue Xue Bao Yi Xue Ban 38, 470–477 (2009).
140. Alexandrov, T. et al. Biomarker discovery in MALDI-TOF serum protein profiles using discrete wavelet transformation. Bioinformatics 25, 643–649 (2009).
141. Grutzmann, R. et al. Sensitive detection of colorectal cancer in peripheral blood by septin 9 DNA methylation assay. PLoS ONE 3, e3759 (2008).
142. Wang, J. Y. et al. Molecular detection of APC, K-ras and p53 mutations in the serum of colorectal cancer patients as circulating biomarkers. World J. Surg. 28, 721–726 (2004).
143. Leung, W. K. et al. Quantitative detection of promoter hypermethylation in multiple genes in the serum of patients with colorectal cancer. Am. J. Gastroenterol. 100, 2274–2279 (2005).
144. Schiedeck, T. H., Wellm, C., Roblick, U. J., Broll, R. & Bruch, H. P. Diagnosis and monitoring of colorectal cancer by L6 blood serum polymerase chain reaction is superior to carcinoembryonic antigen-enzyme-linked immunosorbent assay. Dis. Colon Rectum 46, 818–825 (2003).
145. Ng, E. K. et al. Differential expression of microRNAs in plasma of patients with colorectal cancer: a potential marker for colorectal cancer screening. Gut 58, 1375–1381 (2009).
Author contributionsN. Pawa and J. D. Norton contributed to the research, discussion, writing and editing of this manuscript. T. Arulampalam contributed to the discussion of content and editing.
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved