Embed Size (px)
Citation preview

Scottsdale, ArizonaScottsdale, Arizona Rochester, MinnesotaRochester, Minnesota Jacksonville, FloridaJacksonville, Florida
Treatment For Newly Diagnosed Myeloma
A. Keith Stewart

Risk Adapted Therapy
AgeRenal
functionCo morbidconditions
Geography Access PatientPreference
RiskProfile

mSMART 2.0: Classification of Active MM
FISH Del 17p t(14;16) t(14;20)
GEP High risk
signature
All others including: Hyperdiploid t(11;14)*** t(6;14)
FISH t(4;14)*
Cytogenetic Deletion 13 or hypodiploidy
PCLI >3%
High-Risk 20% Intermediate-Risk 20% Standard-Risk 60% **
* Prognosis is worse when associated with high beta 2 M and anemia** LDH >ULN and beta 2 M > 5.5 in standard risk may indicate worse prognosis*** t(11;14) is associated with plasma cell leukemia

Clearly not a transplant candidate
Can include melphalan-based combinations
Potential transplant candidate
Non-alkylator based induction
Stem cell harvest
Initial Approach to Treatment

Therapy Options: NonTransplant Candidate
• Melphalan + Prednisone (MP)
• Melphalan + Prednisone + Thalidomide (MPT)
• Melphalan + Prednisone + Bortezomib (MPV)
• Dexamethasone (Dex)
• Thalidomide + Dexamethasone (Thal/Dex)
• Lenalidomide + Dexamethasone (Rev/Dex)
NCCN Practice Guideline-v.2.2008NCCN Practice Guideline-v.2.2008

Figure 2
0
10
20
30
40
50
60
70
80
90
100
VAD TD RD PAD VTD CVD RVD CVRD VTD andTandem
Induction Regimen
Percent Response
ORRVGPRCR/nCR
Therapies for younger patients

Figure 2
0
10
20
30
40
50
60
70
80
90
100
VAD TD RD PAD VTD CVD RVD CVRD VTD andTandem
Induction Regimen
Percent Response
ORRVGPRCR/nCR
Transplant ?

What About Maintenance
N Thalidomide CR rate PFS (year) OS (year)
Barlogie 668 400 mgTaper
62% vs. 43%5-year
56% vs. 44%
6-yearSuperior for Thal in CA abnormal
Attal 597400 mg
Until progression or adverse event
67% vs. 55%4-year
52% vs. 36%4-year
87% vs. 77%
Spencer 243 200 mg12 months
63% vs. 40%3-year
63% vs. 36%3-year
90% vs. 81%
Barlogie, Tricot, et al, 2006; Attal et al, 2003; Spencer et al, 2009.

IFM 2005-02: Study design
Arm A=
Placebo
(N=307)
until relapse
Arm A=
Placebo
(N=307)
until relapse
Patients < 65 years, with non-progressive disease, 6 months after ASCT in first line
Arm B=
Lenalidomide
(N=307)
10-15 mg/d until relapse
Arm B=
Lenalidomide
(N=307)
10-15 mg/d until relapse
Primary end-point: PFS.Secondary end-points: CR rate, TTP, OS, feasibility of long-term lenalidomide….
Phase III randomized, placebo-controlled trialN= 614 patients, from 78 centers, enrolled between 7/2006 and 8/2008
Consolidation:Lenalidomide alone 25 mg/day p.o.
days 1-21 of every 28 days for 2 months
Consolidation:Lenalidomide alone 25 mg/day p.o.
days 1-21 of every 28 days for 2 months
Randomization: stratified according to Beta-2m, del13, VGPRRandomization: stratified according to Beta-2m, del13, VGPR

PFS according to Response Pre-Consolidation
HR= 0.37 - CI 95% [0.25-0.58] HR= 0.54 - CI 95% [0.37-0.78]
PR or SD VGPR or CR
0.00
0.25
0.50
0.75
1.00
0 6 12 18 24 30 36
Placebo Revlimid
0.00
0.25
0.50
0.75
1.00
0 6 12 18 24 30 36
Placebo Revlimid
p<10-5 p=0.001

Lenalidomide Maintenance: TTP
Median Follow up from randomization is 12 months
Median TTP: Not yet reached
Median TTP 25.5 mos
CALGB 100104, Nov 2009

Palumbo et al, 2009
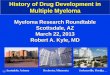
MPR-R vs. MPRMPR-R vs. MPR
Progression-Free SurvivalProgression-Free Survival
MPR-R
MPR
Median PFS
Not reached13.2 months
HR 0.530
100
75
50
25
0
0 5
PFS Time (months)
10 15 20 25 30
Pat
ient
s w
ithou
t E
vent
(%
)

How to treat standard risk disease
Standard-Risk1. OS is 80% at 5 years (before routine maintenance adopted)
2. No difference in induction regimens (needs further study)
3. A drug regimen which results in high overall response rates and which avoids extremes of toxicity (Rd, weekly bortezomib, MPT)
4. Transplant indicated in younger but may be deferred
5. Maintenance likely helps
All others including: Hyperdiploid t(11;14)*** t(6;14)

How to Treat Standard Risk Disease
All others including: Hyperdiploid t(11;14)*** t(6;14)
Standard-Risk**
150 transplant eligible standard risk patients treated with RD, CRD or CBD +/- HDM.

How to treat Intermediate Risk Disease
FISH t(4;14)
Cytogenetic Deletion 13 or hypodiploidy
PCLI >3%
Intermediate-Risk
Vel/Dex
VADp=.0004
Bortezomib-Dex better than VADPre transplant

Short remission post transplant despite high response rates
0
20
40
60
80
100
0 5 10 15 20 25 30 35
Time (months)
%A
live a
nd
Pro
gre
ssio
n F
ree
del17 or t(4;14) all others
Del 17
t(4;14)
All others
4 cycles of CyborD induction and high dose melphalan

FISH t(4;14)*
Cytogenetic Deletion 13 or hypodiploidy
PCLI >3%
Intermediate-Risk
VMP standard risk (N=142): not reached (16 events)VMP high risk (N=26): not reached (3 events)
Prolonged use of Bortezomib may help overcome intermediate risk

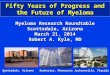
IFM2005: Len maintenance improves PFS even with elevated ß2-m
0.00
0.25
0.50
0.75
1.00
0 6 12 18 24 30 36
Placebo Revlimid
ß2-m 3 mg/l ß2-m > 3 mg/l
0.00
0.25
0.50
0.75
1.00
0 6 12 18 24 30 36
Placebo Revlimid
p=0,0002 p<10-5
Attal et al. 2010

How to treat Intermediate Risk Disease
Intermediate-Risk
FISH t(4;14)*
Cytogenetic Deletion 13 or hypodiploidy
PCLI >3%
1. A bortezomib based multi-agent chemotherapy (CyborD, VRD, VTD, MPV) which maximizes CR
2. Longer duration of bortezomib
3. Autologous transplant
4. Consider Consolidation if not in CR
5. IMID based Maintenance
6. Consider targeted therapy approach on trials

High Risk Disease: Not very effective
• Velcade Dex
• Tandem Autologous Transplant
• Allogeneic Transplant
• Maintenance Thalidomide

POSSIBLY HELPFUL
• Chemotherapy targeting proliferation ?
• Longer duration bortezomib ?
• Lenalidomide maintenance ?

How to treat High risk disease
FISH Del 17p t(14;16) t(14;20)
GEP High risk
signature
High-Risk 1.This population needs novel ideas and therapeutic concepts
2. A multi drug regimen incorporating all available drugs which emphasizes durable CR and uses longer duration of therapy may improve outcomes for p53 deletion
3. Transplant contribution is however of dubious benefit and IMID based maintenance still uncertain

mSMART 2.0: Treatment of Active MM
Novel approaches
New drugs
“TT3 like” approach for p53 deletion ?
Regimen which provides a high ORR and which minimizes early toxicity
HDM could be delayed in patients achieving CR
Lenalidomide maintenance
Prolonged Bortezomib based combination
HDM +/- consolidation
Lenalidomide maintenance
Targeted therapy
High-Risk Intermediate-Risk Standard-Risk

While risk adapted therapy is appealing, randomized trial data is largely lacking:
Minimize toxicity argument: High risk patients do less well even with very aggressive therapy so quality of life more important. Lower risk patients should be treated with focus on lower toxicity as survival long anyway.
Maximize therapy argument: Although less aggressive therapy for standard risk disease may result in good outcomes most patients still relapse so all deserve the most intensive therapy
The Debate Will Continue