Embed Size (px)
Citation preview

Specialist Healthcare Commissioning
Quality Strategy
Scottish Pathology Network
February 2019
2
Contents
Approval .............................................................................................................................. 3 1. Introduction ....................................................................................................................... 4 2. Network Vision .................................................................................................................. 6 3. Quick Wins ........................................................................................................................ 7 4. QI Projects...........................................................................................................................8 5. Data and Measurement ..................................................................................................... 8
6. Annexes........ ......................................................................................................................9
3
Document control Key personnel
Title: Scottish Pathology Network Quality Strategy
Authors: Liz Blackman, Lisa Stewart, Dawn Currie
Approver: National Network Management Service
Owners: Scottish Pathology Network Steering Group
Version history
Version Date of revision Summary of changes Changes marked
Distribution
Name Organisation
Approval
Date Approved by Next Review Date
27.02.2018 Network Steering Group
27.02.2018 Information Management Service
27.02.2018 NNMS
13.02.2019 SPAN Core Team 31.03.2021
4
Section 1: Introduction
National Managed Clinical and Diagnostic Networks (NMCNs and NMDNs) are recognised vehicles for improving the quality of the services they support. The key responsibility of networks in delivering quality improvement is clearly articulated in the most recent published guidance, CEL 2012 (29), which states, “The role of MCNs in improving the quality and efficiency of services across complex whole systems has become even more important in the current financial climate. MCNs achieve their results through consensus and collaboration, by enabling clinicians, patients and service managers to work together across boundaries to deliver safe, effective and person-centred care.... MCNs are integral to achieving the three Quality Ambitions. They epitomise the ethos of co-operation and collaboration that distinguishes the whole of NHSScotland.”1 Scottish Government’s core principles of managed networks identify the requirement for:-
Continuous quality improvement, articulated through an annual workplan to demonstrate intended improvements year on year, quantified from the perspective of the service user
Expansion of the evidence base through continuous quality improvement and ongoing audit
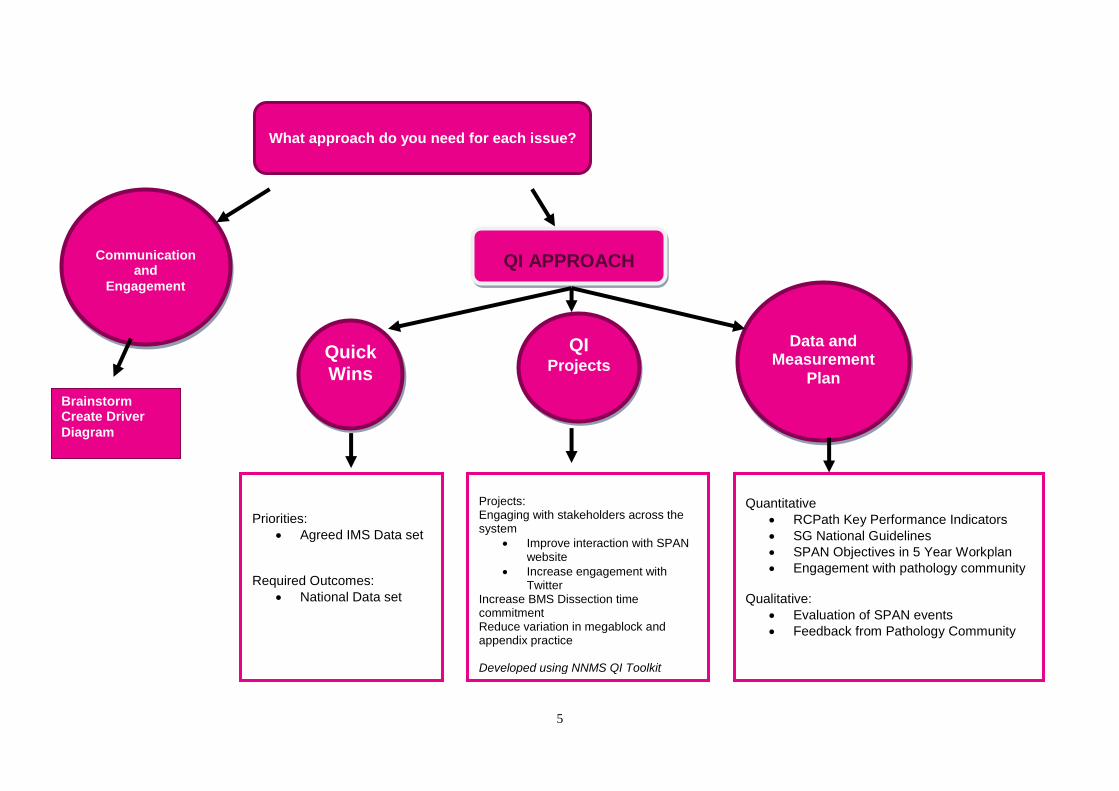
Diagnostics, whether primary care, community or secondary care delivered, have an important role to play in supporting much of the quality strategy and its ambitions by contributing to early, accurate and cost effective diagnosis, monitoring and self-management. This strategy outlines the approach the Scottish Pathology Network (SPAN) will take to improving quality in diagnostic pathology services. This strategy complements the strategic vision for the network, which can be found in its five year plan (Annexe 1). 1.2 Network approach Networks develop five year and annual workplans, based on policy drivers, horizon scanning and identified need for service improvement. From the development of workplans an understanding of the issues to be addressed is developed. How these issues are addressed is contained within this strategy. The network’s identified approach to quality improvement can be illustrated as follows:-
1 http://www.sehd.scot.nhs.uk/mels/CEL2012_29.pdf
5
Communication
and
Engagement
Brainstorm Create Driver
Diagram
What approach do you need for each issue?
Quick Wins
QI Projects
Data and
Measurement
Plan
QI APPROACH
Priorities:
Agreed IMS Data set
Required Outcomes:
National Data set
Projects: Engaging with stakeholders across the system
Improve interaction with SPAN website
Increase engagement with Twitter
Increase BMS Dissection time commitment Reduce variation in megablock and appendix practice Developed using NNMS QI Toolkit
Quantitative
RCPath Key Performance Indicators
SG National Guidelines
SPAN Objectives in 5 Year Workplan
Engagement with pathology community
Qualitative:
Evaluation of SPAN events
Feedback from Pathology Community
6
2. Network Vision
SPAN aims to ensure the provision of an innovative, equitable, patient centred, high quality, and clinically effective Pathology service.
Managed Diagnostic Networks are defined as coordinated groups of health professionals that support diagnostic services to continuously improve service delivery, in order to ensure equitable provision of high quality, clinically effective services. The Scottish Government2/3 has identified that diagnostics are central to whole systems service redesign of the NHS in Scotland. Diagnostic Networks drive forward a number of key pieces of national strategic work, including:
Shared Services
National Delivery Plan for Healthcare Scientists
National Clinical Strategy During 2016-17, in line with NHS Scotland’s national commissioning policy, SPAN became the first NMDN to undergo an external review. The purpose of this was to inform a decision on continuing central funding; based on the extent to which SPAN was meeting the needs of its stakeholders, including NHS Scotland’s vision for diagnostic services. This provided the Network with the opportunity to refresh and revitalise its workplan. The review acknowledged that SPAN has added considerable value to services since inception, highlighting the following as successes:
information sharing between Pathology services
conduit of essential communications
contribution to a number of service redesign initiatives
collection of a sizable data set, providing comparisons on performance and staffing
profiles across Scotland and also comparisons with previous years
tangible engagement and participation from each of the centres, with excellent
attendance at meetings and good buy-in throughout.
Areas for improvement have been identified through the SPAN Review 2017. The following key areas could be targeted for quality improvement initiatives:
Improving turnaround times (productivity) for cellular laboratories
Testing of Digital Pathology
Improving stakeholder engagement across the whole system
Using data to make quality improvements
2 A National Clinical Strategy for Scotland 2016
3 Realistic Medicine Chief Medical Officer’s Annual Report 2014-2015
7
The review highlighted some areas of concern in the Network’s performance, most notably engaging with a range of stakeholders, including at a strategic and operational level, to improve SPAN’s ability to effect change. The review identified that SPAN should improve its communication and engagement within the Pathology community and with its external stakeholders such as service users. Therefore, in December 2016, SPAN issued its first quarterly newsletter. A communication and engagement strategy was produced, which was endorsed by the SPAN steering group. The Communication Strategy was reviewed in December 2017 to measure progress against objectives.
Priorities are reflected through the following activities in the five year plan for years 2017-2022 (Annex 1).
3. Quick Wins
Quick Wins are improvements that have high value to the network but are manageable and inexpensive to implement. The Quick Wins should motivate the network and be communicated to stakeholders about the improvements that are producing results.
The point is to:
Show results and success quickly and communicate this widely
Motivate the network by doing something early
Demonstrate to stakeholders that the network is going to make improvements
Support the overall improvement targets – the five year workplan
Choose Quick Wins that will be visible
Look for Quick Wins that can be easily solved with current resources
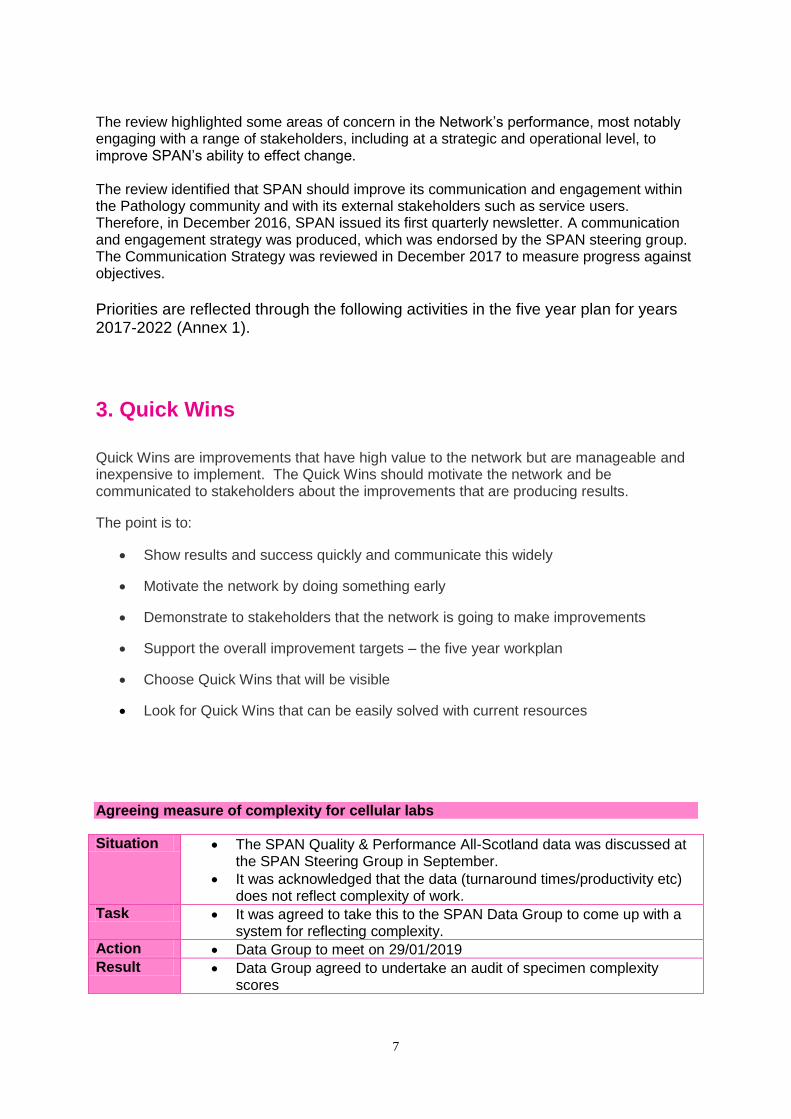
Agreeing measure of complexity for cellular labs
Situation The SPAN Quality & Performance All-Scotland data was discussed at the SPAN Steering Group in September.
It was acknowledged that the data (turnaround times/productivity etc) does not reflect complexity of work.
Task It was agreed to take this to the SPAN Data Group to come up with a system for reflecting complexity.
Action Data Group to meet on 29/01/2019
Result Data Group agreed to undertake an audit of specimen complexity scores
8
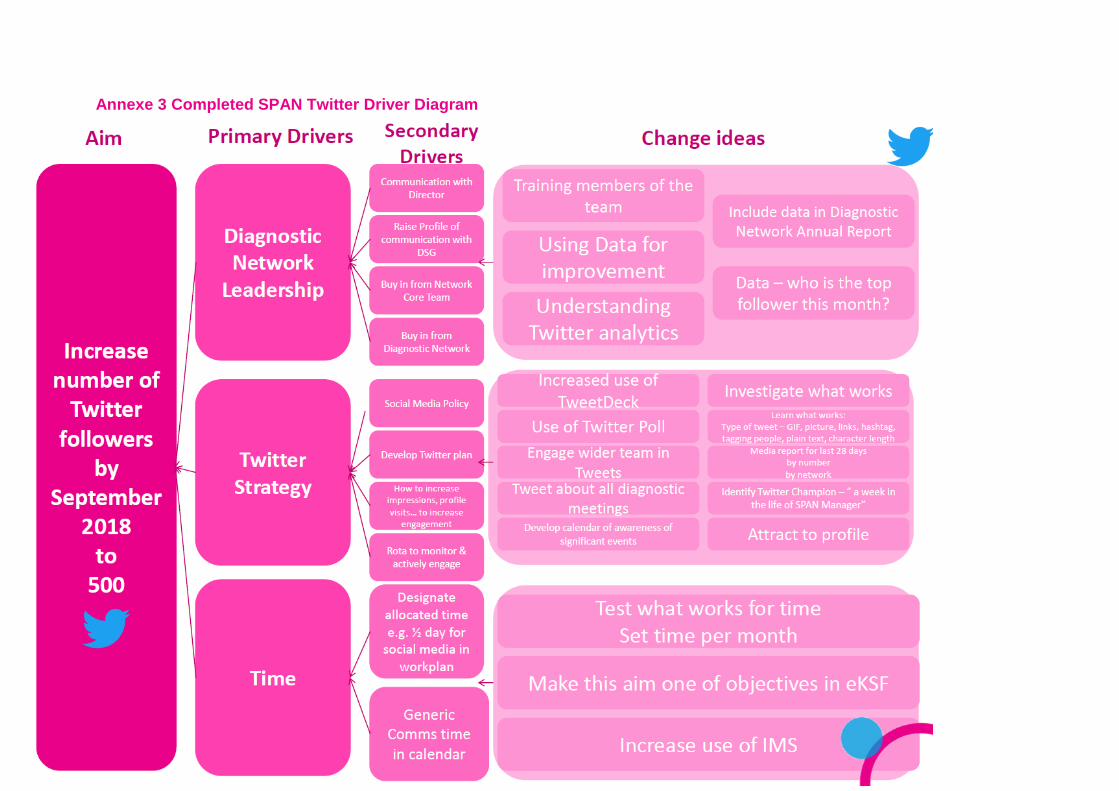
4. QI Projects One of the key areas identified in the review included improving stakeholder engagement across the whole system. Following the development of a Communication Strategy, two QI projects were identified, which were to improve interaction with the SPAN website and to promote the SPAN network and its workplan through Twitter. Attached as Annexe 2 and 3 are the completed QI Projects on Website Engagement and the Driver Diagram on use of Twitter to engage with the Pathology community. SPAN undertook a QI project to improve interaction with the website by 10%. At the beginning of the project, 600 people used the website on a monthly basis. By the end of December 2018, this had increased to 1,005 users per month, an increase of 67.5%. SPAN also undertook a QI project to improve the number of Twitter followers of the @NMDNScot account used by all of the Diagnostic Networks. The aim was to increase the number of followers to 500. By September 2018, Twitter followers had increased to 520. In 2019, SPAN plan to undertake a number of QI projects. These include increasing the time commitment for BMS dissection by 10% and understanding what variation exists between Scottish laboratories in appendix and megablock practice. This includes repeating a data collection exercise of current practice and undertaking an audit of appendix practice at an identified laboratory that previously had high number of blocks taken from appendix to decrease this. Attached as Annex 4, 5 and 6 are QI plans for these projects.
5. Data and Measurement Plan
A Data and Measurement plan has been developed to measure progress against the SPAN workplan. The plan includes process measures (aiming to improve reliability), outcome measures (improving the patient experience) and balancing measures (how improvements in one area may have unintended consequences for another area). (Annexe 4). Measures include:
Quantitative data e.g. quality and performance data generated by NHS Boards and managed through IMS
Quantitative data relating to time commitment for pathological dissection
Quantitative data relating to engagement with the pathology community
Qualitative data work e.g. stakeholder feedback, evaluation of SPAN events
Quality Indicators/RCPath Key Performance Indicators relating to Biopsy Turnaround Times, Reporting Times
Relevant national guidelines including Scottish Government recommendations for mortuary services, post-mortem reporting
Identification of local QI projects e.g. appendix dissection practice
9
Annexes
1. SPAN Five Year Workplan
2. QI Project on Website Engagement
3. Diagram on Use of Twitter
4. QI Project on increasing time commitment for BMS Dissection in Scotland
5. QI Project on understanding variation in megablock and appendix practice
6. SPAN Data and Measurement Plan
10
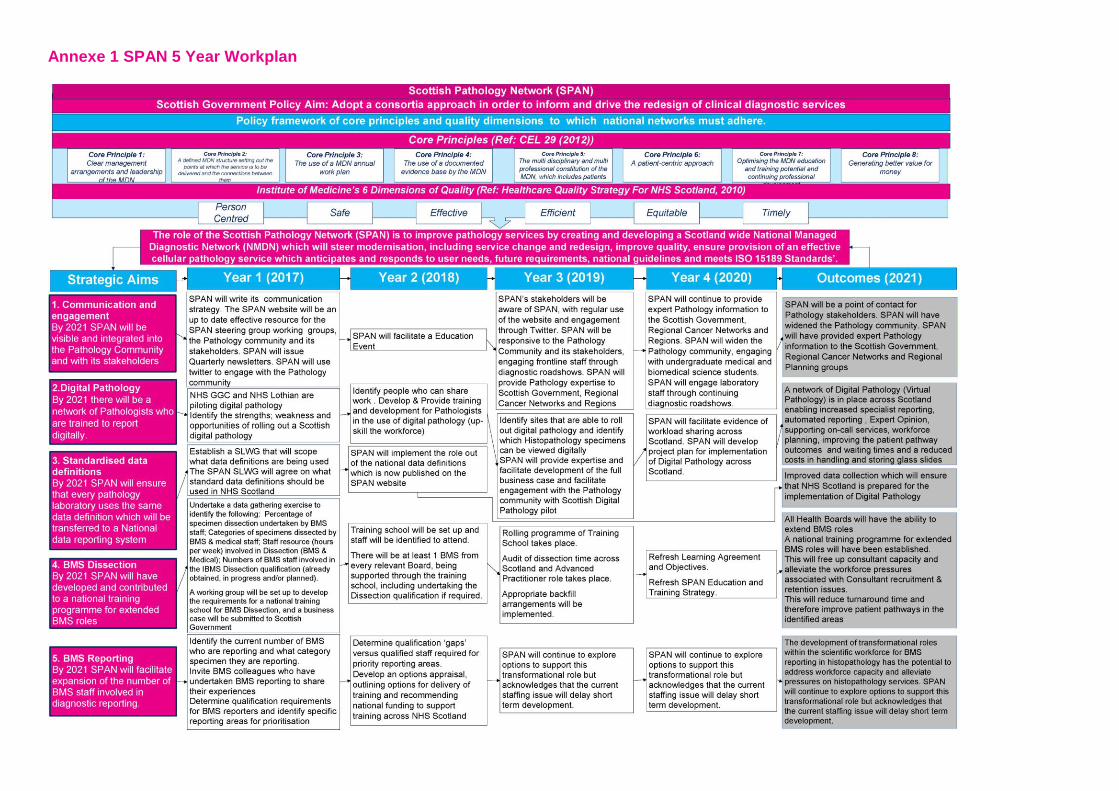
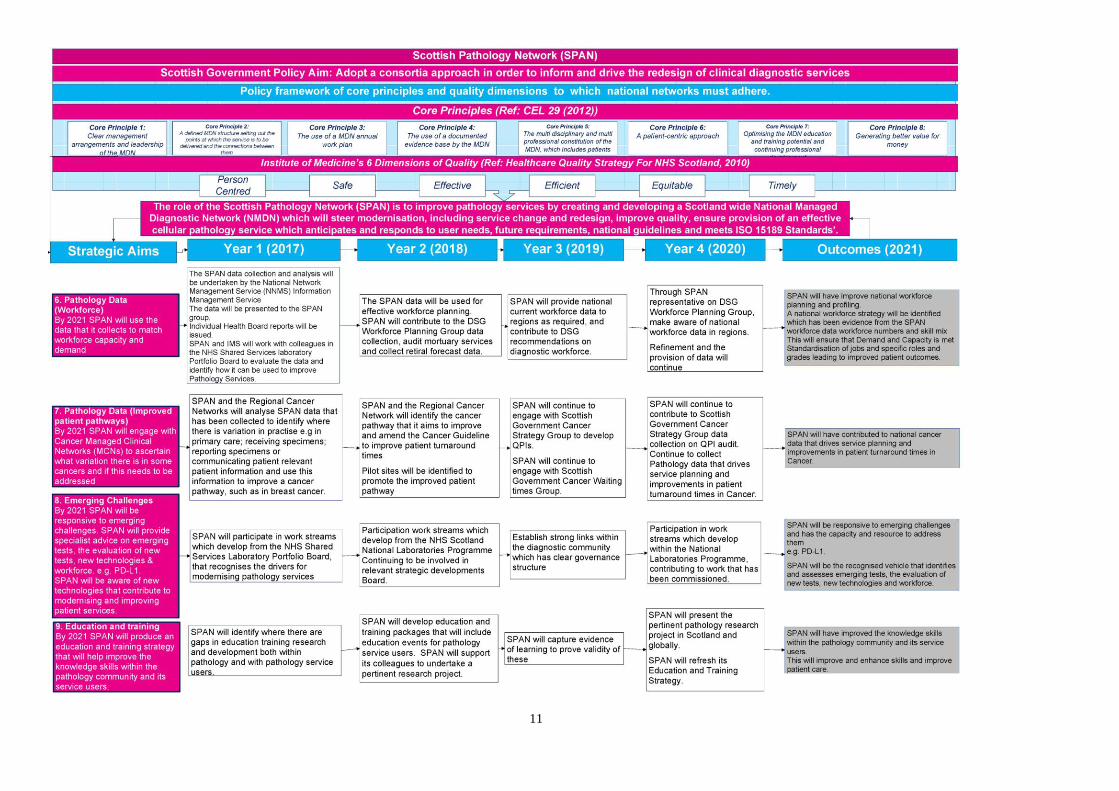
Annexe 1 SPAN 5 Year Workplan
11
12
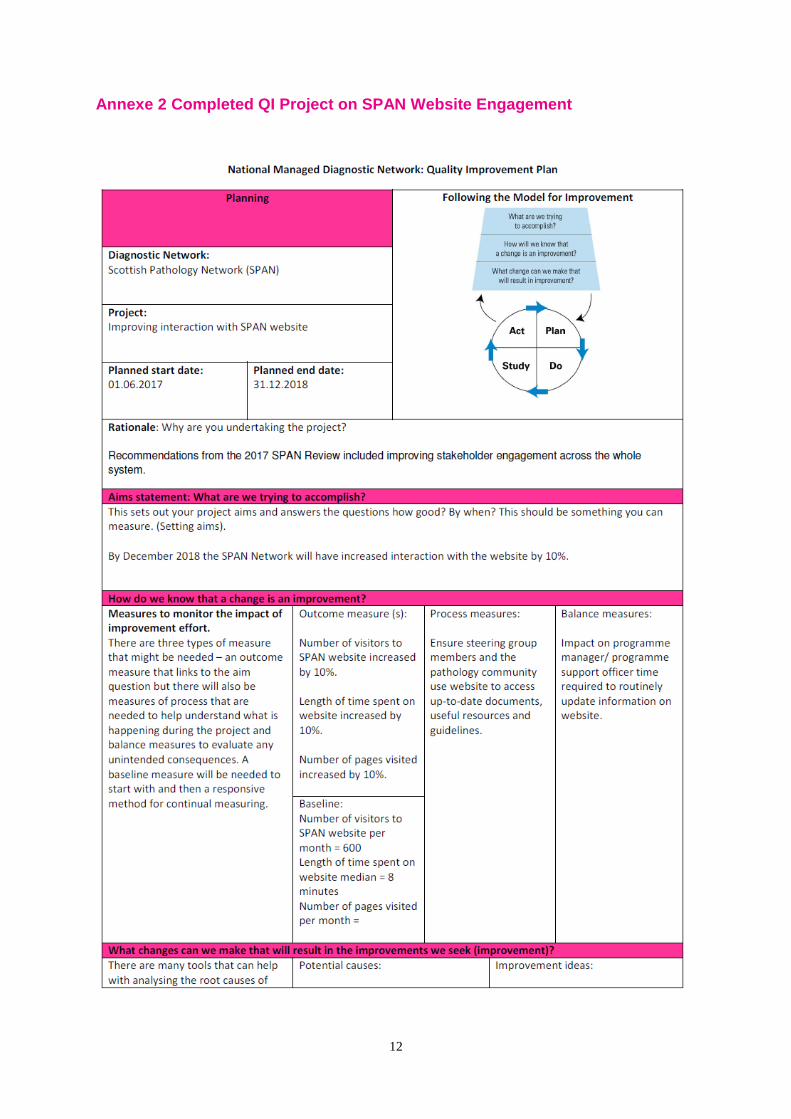
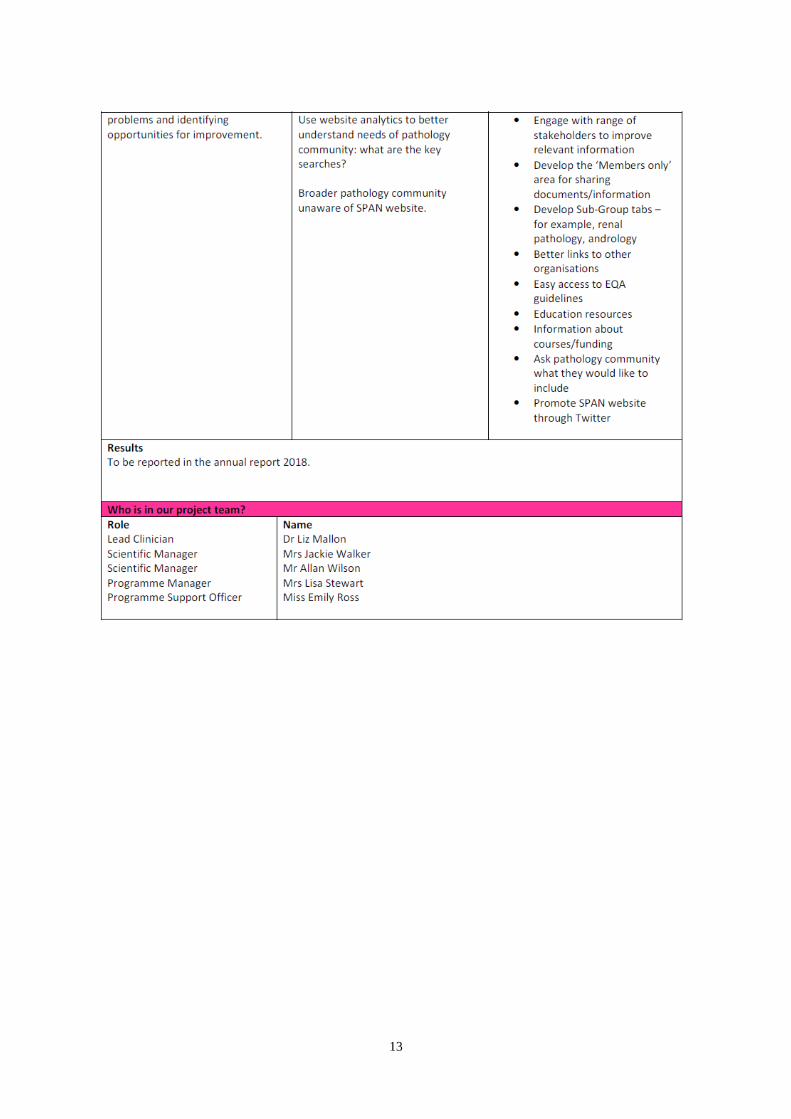
Annexe 2 Completed QI Project on SPAN Website Engagement
13
14
Annexe 3 Completed SPAN Twitter Driver Diagram
15
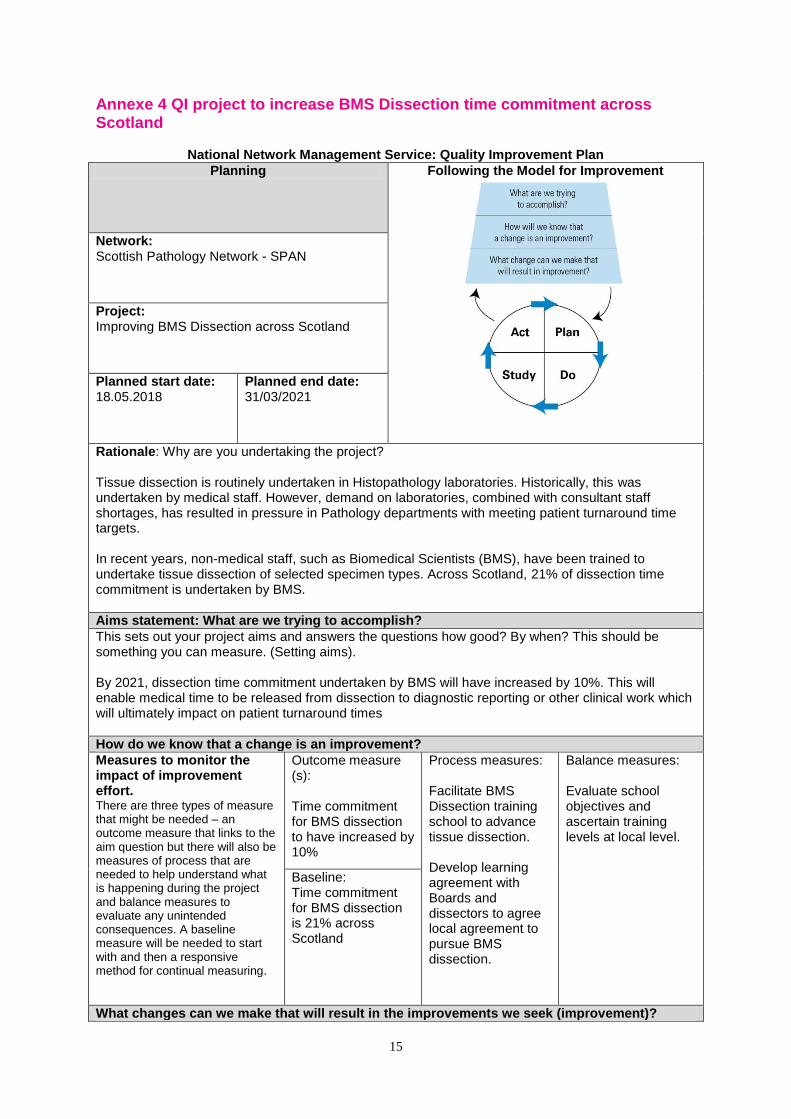
Annexe 4 QI project to increase BMS Dissection time commitment across Scotland
National Network Management Service: Quality Improvement Plan
Planning Following the Model for Improvement
Network: Scottish Pathology Network - SPAN
Project: Improving BMS Dissection across Scotland
Planned start date: 18.05.2018
Planned end date: 31/03/2021
Rationale: Why are you undertaking the project? Tissue dissection is routinely undertaken in Histopathology laboratories. Historically, this was undertaken by medical staff. However, demand on laboratories, combined with consultant staff shortages, has resulted in pressure in Pathology departments with meeting patient turnaround time targets. In recent years, non-medical staff, such as Biomedical Scientists (BMS), have been trained to undertake tissue dissection of selected specimen types. Across Scotland, 21% of dissection time commitment is undertaken by BMS.
Aims statement: What are we trying to accomplish?
This sets out your project aims and answers the questions how good? By when? This should be something you can measure. (Setting aims). By 2021, dissection time commitment undertaken by BMS will have increased by 10%. This will enable medical time to be released from dissection to diagnostic reporting or other clinical work which will ultimately impact on patient turnaround times
How do we know that a change is an improvement?
Measures to monitor the impact of improvement effort. There are three types of measure that might be needed – an outcome measure that links to the aim question but there will also be measures of process that are needed to help understand what is happening during the project and balance measures to evaluate any unintended consequences. A baseline measure will be needed to start with and then a responsive method for continual measuring.
Outcome measure (s): Time commitment for BMS dissection to have increased by 10%
Process measures: Facilitate BMS Dissection training school to advance tissue dissection. Develop learning agreement with Boards and dissectors to agree local agreement to pursue BMS dissection.
Balance measures: Evaluate school objectives and ascertain training levels at local level.
Baseline: Time commitment for BMS dissection is 21% across Scotland
What changes can we make that will result in the improvements we seek (improvement)?
16
There are many tools that can help with analysing the root causes of problems and identifying opportunities for improvement.
Potential causes: Not enough BMS trained to dissect less complex specimens at Board level. Not enough medical time to be released from dissection to diagnostic reporting or other clinical work.
Improvement ideas: Facilitate BMS Dissection training school to advance tissue dissection. BMS dissection to be progressed at local Board levels, upon signed agreement between SPAN and Boards.
Results To be reported midyear October 2019
Who is in our project team?
Role Network Scientific Manager Programme Manager Programme Support Officer BMS Dissection Implementation Group
Name Jackie Walker Dawn Currie Emily Ross
17
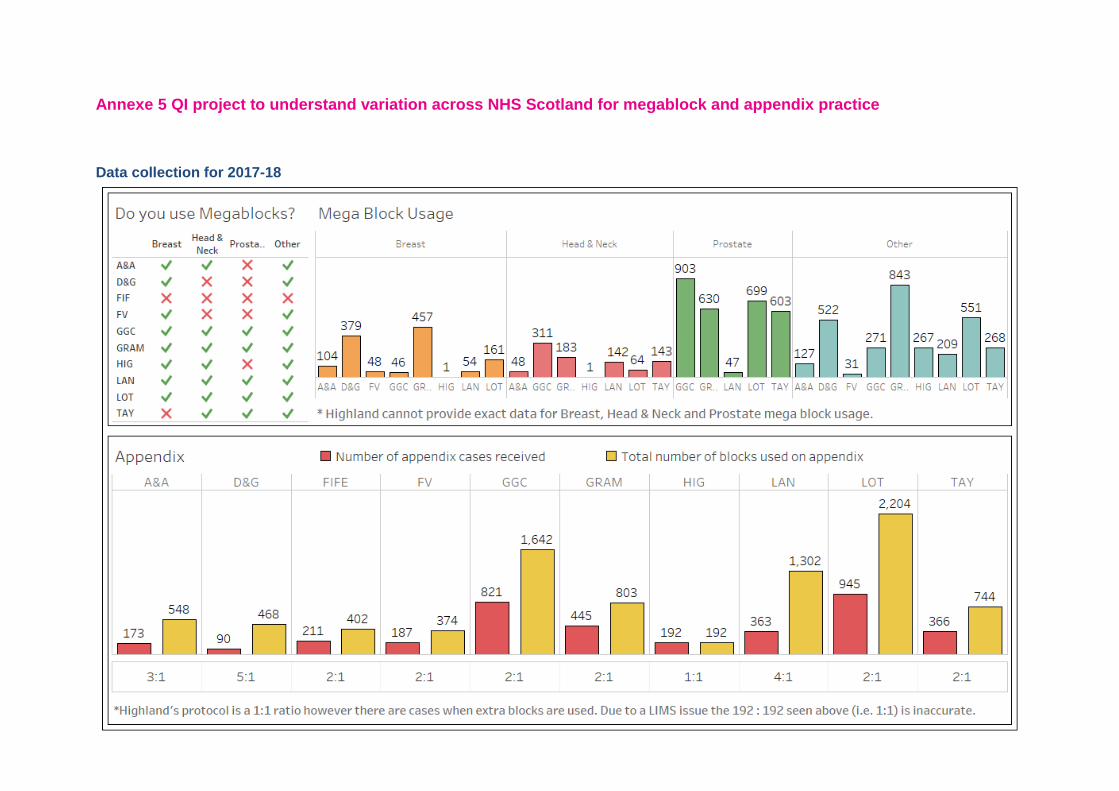
Annexe 5 QI project to understand variation across NHS Scotland for megablock and appendix practice Data collection for 2017-18
18
Annexe 6 NHS Lanarkshire audit on appendix practice
Audit of sampling appendectomy specimens for histopathological
assessment
(Dr M Benkovicova)
Introduction: Appendices are usually removed due to appendicitis or accompanying other operations.
Although the majority of cases have the usual features, there are cases which also may
contain incidental tumours or other abnormal lesions which were not suspected
preoperatively or intra-operatively by the surgeon. Within appendicitis over the age of 50
there is significant chance that an occult malignancy is also present. Non - expected
histopathological findings could potentially impact on the further management of the patients.
Appropriate sections depend on the indication for appendectomy. Standard sections
recommended by Royal College of Pathologists include the tip and the resection margin
together with at least one transverse section. There is no specific advice on the minimum
number of the blocks that should be taken. The tip should be bisected longitudinally with
mesoappendix and the base/resection margin should be microscopically identifiable (inked or
use of separate cassette) and cut longitudinally or transversely. The remaining intervening
tissue between the margin and the tip can be sliced transversely or longitudinally.
It is advised by RCP to sample the entire appendix if neoplasia is suspected clinically, or at
trimming, or the appendix looks normal and not inflamed or the initial examination shows
peritonitis without transmural inflammation. If hyperplastic, serrated lesion, dysplasia,
mucinous lesions or any features suggestive of carcinoma are seen, sampling of the entire
appendix is advised.
Other sources also advise complete submission of the appendectomy specimen when
accompanying ovarian carcinoma.
The objective of this study was to analyse the histopathological finding in appendectomy
specimens in relation to the provisional clinical diagnosis and to analyse if appropriate
numbers of tissue blocks were taken in relation to the RCP recommendations.
Based on histopathological findings the appendectomy specimens were classified as either
positive for appendicitis, negative for appendicitis, abnormal lesions including appendiceal
tumours as incidental finding or clinically suspected and appendectomies accompanying
other specimens.
• Positive specimens included findings which likely do not require further
postoperative management and those include acute inflammation with or without
perforation, reactive hyperplasia, granuloma to faecal material( may indicate resolved
inflammation) and diverticulum.
• Negative appendectomies for suspected appendicitis were normal, without evidence
of inflammation, tumour or parasitic infestation. It is suggested that the presence of
faecolith, fibrous obliteration of the lumen and lymphoid hyperplasia without acute
inflammation most likely is not the cause of the patient symptoms of appendicitis or
19
abdominal pain, therefore these changes are classified as negative findings.
• Abnormal findings were identified as granulomatous inflammation, worms,
endometriosis, peritonitis without transmural inflammation and IBD (Crohn's or
ulcerative colitis). Appendiceal tumours included sessile serrated polyp, adenomas,
mucinous neoplasia, carcinoma and carcinoid.
• Some appendectomy specimens were accompanying other specimens removed for
various indications. These are complicated inflammatory/benign lesions or malignant
tumours.
Negative appendectomies, abnormal findings and tumours most usually require further
postoperative management/ follow up the patient.
Materials and Methods:
The demographic and pathological data of all patients who underwent appendectomy at
Lanarkshire NHS (Monklands, Hairmyres and Wishaw Hospitals) between 1st January and
30th June 2017 were retrieved from the NHS Lanarkshire electronic record system and
retrospectively analysed.
All patients were included and evaluated by gender and age (<16y, 16-50y, >50y). In all cases
available number of tissue blocks was recorded.
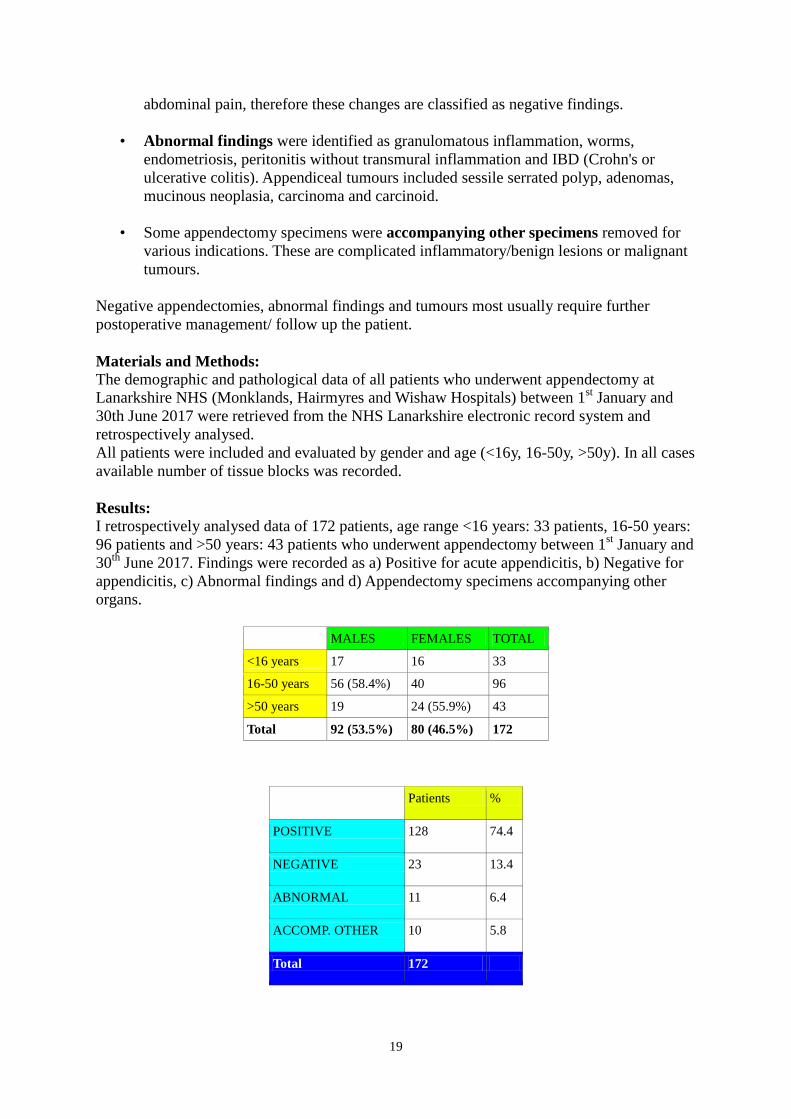
Results: I retrospectively analysed data of 172 patients, age range <16 years: 33 patients, 16-50 years:
96 patients and >50 years: 43 patients who underwent appendectomy between 1st January and
30th
June 2017. Findings were recorded as a) Positive for acute appendicitis, b) Negative for
appendicitis, c) Abnormal findings and d) Appendectomy specimens accompanying other
organs.
MALES FEMALES TOTAL
<16 years 17 16 33
16-50 years 56 (58.4%) 40 96
>50 years 19 24 (55.9%) 43
Total 92 (53.5%) 80 (46.5%) 172
Patients %
POSITIVE 128 74.4
NEGATIVE 23 13.4
ABNORMAL 11 6.4
ACCOMP. OTHER 10 5.8
Total 172
20
BLOCKS Positive
for acute
inflamm
ation
Negative
for
acute
inflamm
ation
Abnorm
al
finding
Accompa
nying
other
specimen
s
TOTAL %
1 1 1 2 1.2
2 5 3 2 10 5.8
3 78 18 5 4 105 61
4 22 1 3 2 28 16.2
5 13 1 1 15 8.7
6 2 1 3 1.7
7 2 2 1.2
8 1 1 0.6
10 1 1 0.6
11 2 2 1.2
12 1 1 0.6
15 1 1 2 1.2
Cases 128 23 11 10 172
% 74.4 19.8 5.8
21
POSITIVE FOR ACUTE APPENDICITIS
Clinical dg
Acute Mass ?Neopl ?Carcinoid ? Mucocele Dg
Illegibl
e
Dg
not
given
Review All
process
ed
Pathology dg:
ACUTE
INFLAMMATION
104
(81.3%)
3 2 1 1 1 16
Total
B
L
O
C
K
S
1 1 1 0
2 5 3 2 0
3 78
(61%)
64 1 1 1 11 4
4 22
(17.2%)
19 3
5 13
(10.2%)
12 1 3
6 2 1 1 2
7 2 1 1 1
8 1 1 ?
9
10
11 2 2 2
Basings
toke
2
12 1 1 1
13
14
15 1 1
Frozen
1
Total 128 14
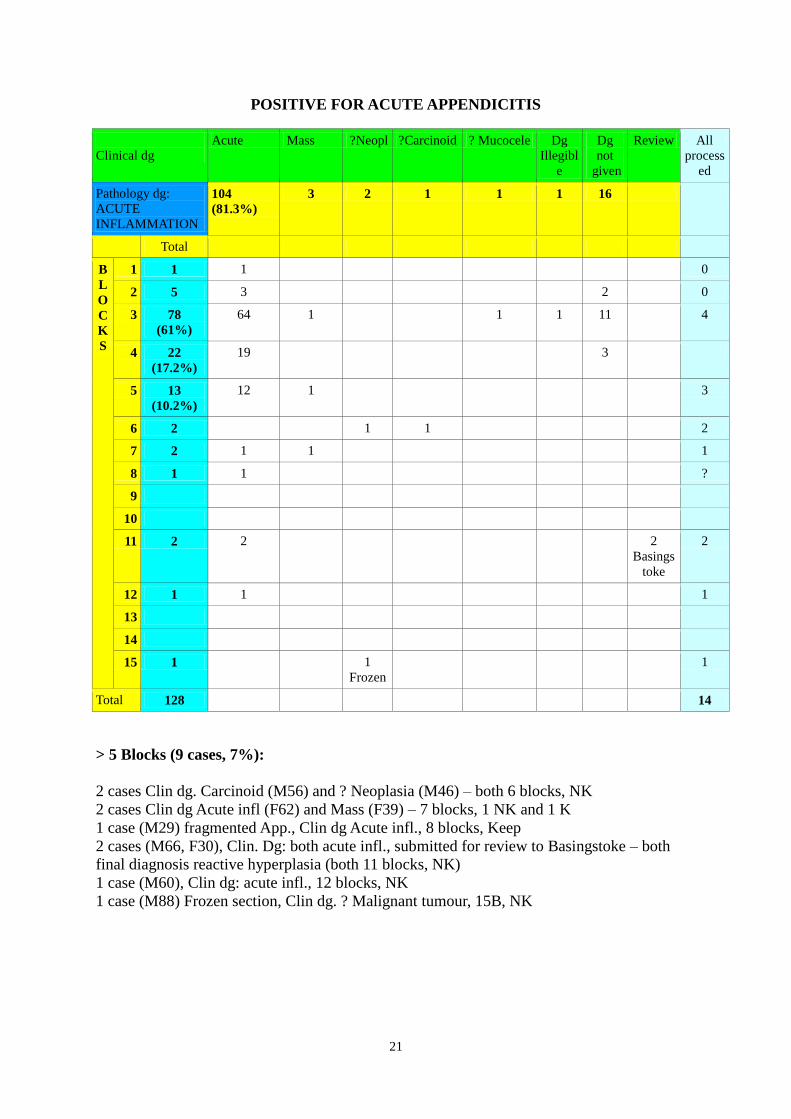
> 5 Blocks (9 cases, 7%):
2 cases Clin dg. Carcinoid (M56) and ? Neoplasia (M46) – both 6 blocks, NK
2 cases Clin dg Acute infl (F62) and Mass (F39) – 7 blocks, 1 NK and 1 K
1 case (M29) fragmented App., Clin dg Acute infl., 8 blocks, Keep
2 cases (M66, F30), Clin. Dg: both acute infl., submitted for review to Basingstoke – both
final diagnosis reactive hyperplasia (both 11 blocks, NK)
1 case (M60), Clin dg: acute infl., 12 blocks, NK
1 case (M88) Frozen section, Clin dg. ? Malignant tumour, 15B, NK
22
NEGATIVE FOR ACUTE APPENDICITIS
NEGATIV
E
<16 YEARS 16 – 50 YEARS >50 YEARS Total %
FEMALE 4 11 0 15 65.2
MALE 3 5 0 8 34.8
Total 7 (30.5%) 16 (69.5%) 0 23
Negative Clinical diagnoses
Pathology Cases Acute,
injected
Normal RIF
pain /fluid
Fecolith Not
given
Endo
metriosis
Prophy
lactic
Normal 14 (60.9%) 8 1 2 3
Faecolith 6 1 1 1 2 1
Fibr. obliter. 2 1 1
Lymph hyperpl 1 1
Total 23 10
(43.5%)
2 2 1 6 1 1
Total NO KEEP*
B
L
O
C
K
S
2 3 1 2 1*
3 18
(78.3
%)
1 8 1 2 1 5 1
4 1 1*
5 1 1 1*
Total cases
23 3 (13%) 10 2 2 1 6 1 1
ABNORMAL PATHOLOGY
<16 YEARS 16 – 50 YEARS >50 YEARS Total %
FEMALE 1 3 2 6 54.5
MALE 1 3 1 5 45.5
Total 2 6 (54.5%) 3 11
23
Abnormal pathology
11 cases
Clinical diagnoses
Path Diagnosis Cases Gen /
Age
Clin. dg
Blocks Base Tip K/NK S. Review Need further
manag/FU
SSL LD perf 1 F 67 acute 4 y y NG
y
LAMN perf 1 F47 ? Muc tu 15 y y K Basingstoke
y
Granulomas 1 M18 NG 6 y y NK
y
Granulomas 1 F58 ?Infl, ?neopl 4 y y NK
y
Perit. reaction 1 F15 NG 3 NG y NG y
Inactive chronic
appendicitis
1 M35 Acute 2 month
ago
4 y y K y
Periappendicitis 1 F45 ? acute 3 y y NK y
Peritonitis 1 M41 ? acute 3 y NG NG y
Enterobius 1 M13 RIFpain, mLN 3 y y K y
Adenocarcinoma 1 M66 ?comp infl, ?tu 10 y y NK y
Neuroendocrine
ca, gr
1(carcinoid)
1 F18 acute 3 y NG NG y
Clin dg ? Tumour Inflammation RIF pain Not given
Pathology Cases
SSL 1 1
LAMN 1 1
Adenocarcino
ma
1 1
Carcinoid 1 1
Granulom.
inflam.
2 1 1
Peritonitis 3 2 1
Worm 1 1
Chronic
inflam.
1 1
Total 11 3 5 1 2
24
SS
L
LAM
N
Adenoc
a
Carcinoi
d
Worm Peritonit
is
Granulom.
inf.
Chronic
inf. Total-
cases
B
L
O
C
K
S
3 1 1 3 5
4 1 1 1 3
6 1 1
10 1 1
15 1 1
ACCOMPANYING OTHER SPECIMENS
Accompanying other
specimens
Clinical diagnoses
Path Diagnosis 10
Cases
Gen /
Age
Clin. dg
Blocks Base Tip K/NK Further
manag
Fibr.obliter 1 F48 Perf sigm divert 3 y y K
Small ulcer 1 F64 Ov. mucinous
cystadenoma
4 y y NK
Fibr.obliter 1 F59 Ov.cystadenofib.
(likely serous)
3 y y K
Normal 1 M27 Meckel's diverticulum 2 y y K
Acute 1 M62 Compl. divert.d. 4 y NG K
Fibr. obliter 1 F60 Ov. endom.carcinoma 1 y y NG
Normal 1 M56 PostDXT, rectal ca 3 y Typo
deep
NG
SSP, clear RM 1 F55 Ov.borderline muc.tu 5 y y NK Y
Normal 1 M27 Meckel's diverticulum 3 y y K
Normal 1 F46 Ov HG serous ca 2 y y K
Appendectomy
BLOCKS
Small/Large
intestine
Ovary Total
Benign Malign Benign Malign.
1 1 1
2 1 1 2
3 2 1 1 4
4 1 1 2
5 1 1
Total 4 1 2 3 10 cases
25
Discussion:
The histopathological examination allows the diagnosis of acute appendicitis to be confirmed
especially where this was not evident intra-operatively. Specimens reported as negative for acute
appendicitis are useful in eliminating acute appendicitis as a cause of symptoms allowing further
investigation. Histopathological examination may also disclose additional pathologies which may
affect subsequent clinical management of the patient.
Standard sectioning (recommended by RCP) of the appendectomy specimens with obvious
inflammation at trimming are sampled into 3 cassettes including, transverse or longitudinal section of
the resection margin / base, at least one longitudinal half of the tip and a transverse or longitudinal
section of the mid of the appendix.
Within this study among 172 patients, 92 (53.3%) were male and 80 (46.5%) were female. Most of
the patients (96) were between 16 – 50 years of age with slightly predominant male group (58.4%).
55.6 % female predominance is noted in group over 50 years.
128 cases (74.4%) were positive for acute appendicitis, 23 cases (13.4%) negative for acute
appendicitis and 11 cases (6.4%) showed other benign or malignant lesions. 10 additional
appendectomy specimens were accompanying other resections.
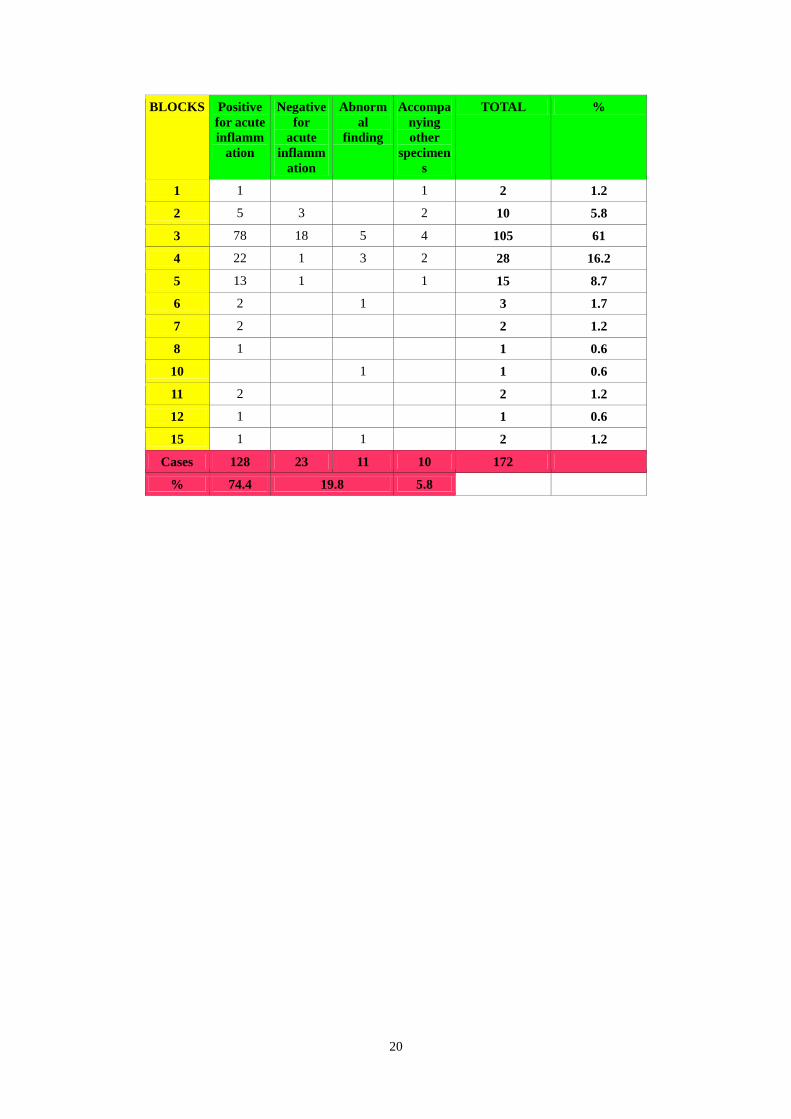
Most of the appendectomy specimens, 105 cases (61%) from 172 were sampled into 3 cassettes. 28
cases (16.2%) were submitted into 4 cassettes, and 15 cases (8.7%) into 5 cassettes. Only 10 cases
(5.8%) were provided with 2 cassettes and 2 cases with a single cassette.
12 appendectomy specimens (7%) from 172 were sampled into more than 5 cassettes. 9 of them
(5.2%) were positive for acute inflammation. These also include 2 specimens submitted for review to
Basingstoke (both entirely processed in 11 cassettes) and 1 case was clinically suspicious of cancer
and intra-operative frozen section biopsy was performed. None of these cases were confirmed
malignant or required further management of the patient.
A further 3 cases were sampled in more than 5 cassettes (LAMN - x15, adenocarcinoma- x10 and
granulomatous inflammation- x6).
78 (61%) cases from 128 cases positive for acute appendicitis were sampled into 3 cassettes, 22 cases
(17.2%) into 4 and 13 cases (10.2%) into 5 cassettes.
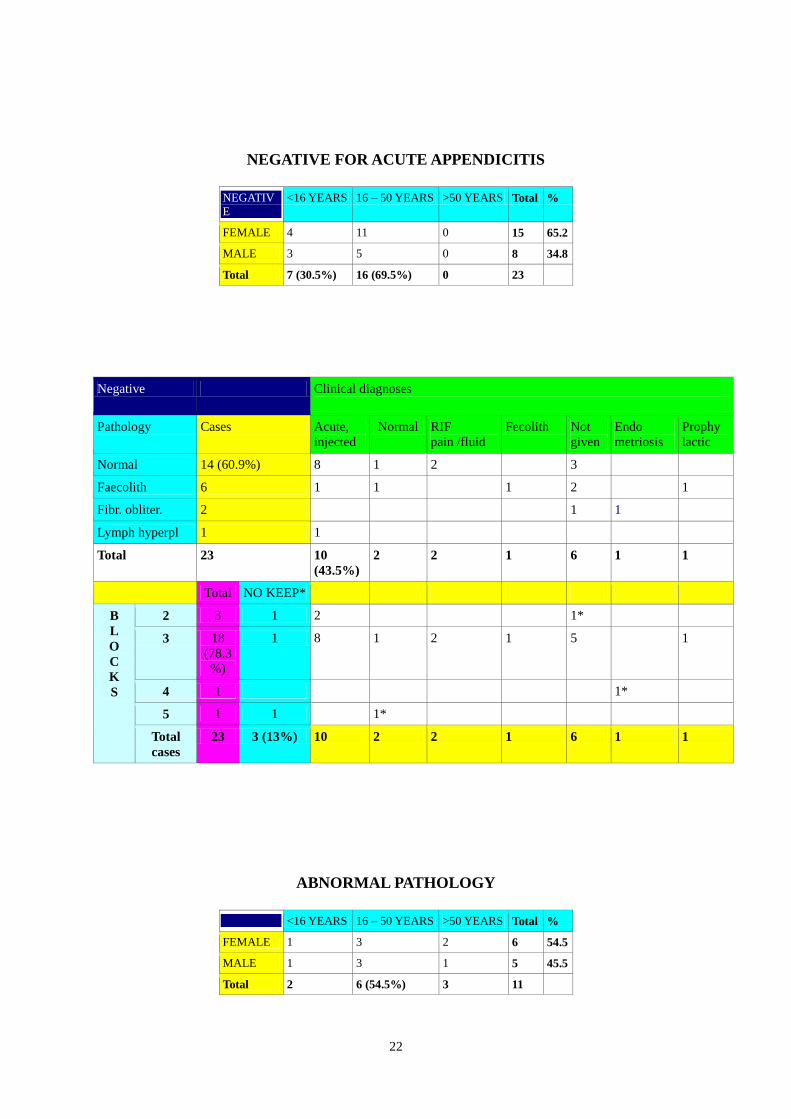
23 cases were negative for acute appendicitis with predominant 15 (65.2%) females. Most of the
patients, 16 (69.5%) were between 16-50 years old, 11 of them (68.7%) were female and 5 (31.3%)
male. 10 out of 23 cases were diagnosed clinically as acute appendicitis. In 2 cases there was RIF pain
/ fluid and in 6 cases no clinical diagnosis was provided. Additional 2 cases were clinically normal, 1
case was suspicious of faecolith and1 case of endometriosis. A further single case was a prophylactic
appendectomy for mesenteric adenitis not settling for 2/52.
Histological examination showed 14 normal appendices, faecolith within 6, fibrous obliteration in 2
and lymphoid hyperplasia in 1 case.
18 (78.3%) appendectomy specimens were sampled into 3 cassettes, 3 cases in 2 cassettes, 1 case in 4
cassettes and 1 case in 5 cassettes.
By RCP recommendation the entire appendix should be processed before reporting that it is not
inflamed. Only in 3 (13%) cases was the entire appendix submitted ( 1 clinically normal appendix – 5
blocks, 1 case suspicious of endometriosis – 4 blocks and in 1 case without clinically diagnosis – 2
blocks). Remaining appendectomy specimens, 20 (87%) underwent standard sectioning (all in 3
cassettes).
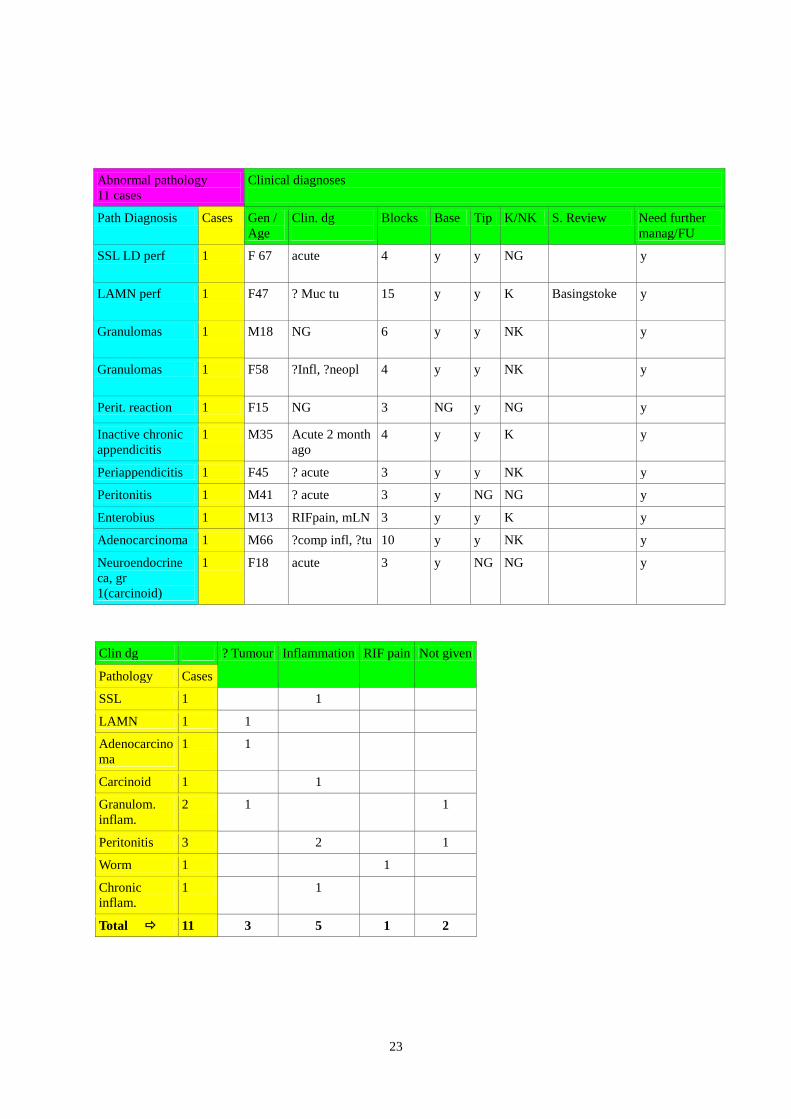
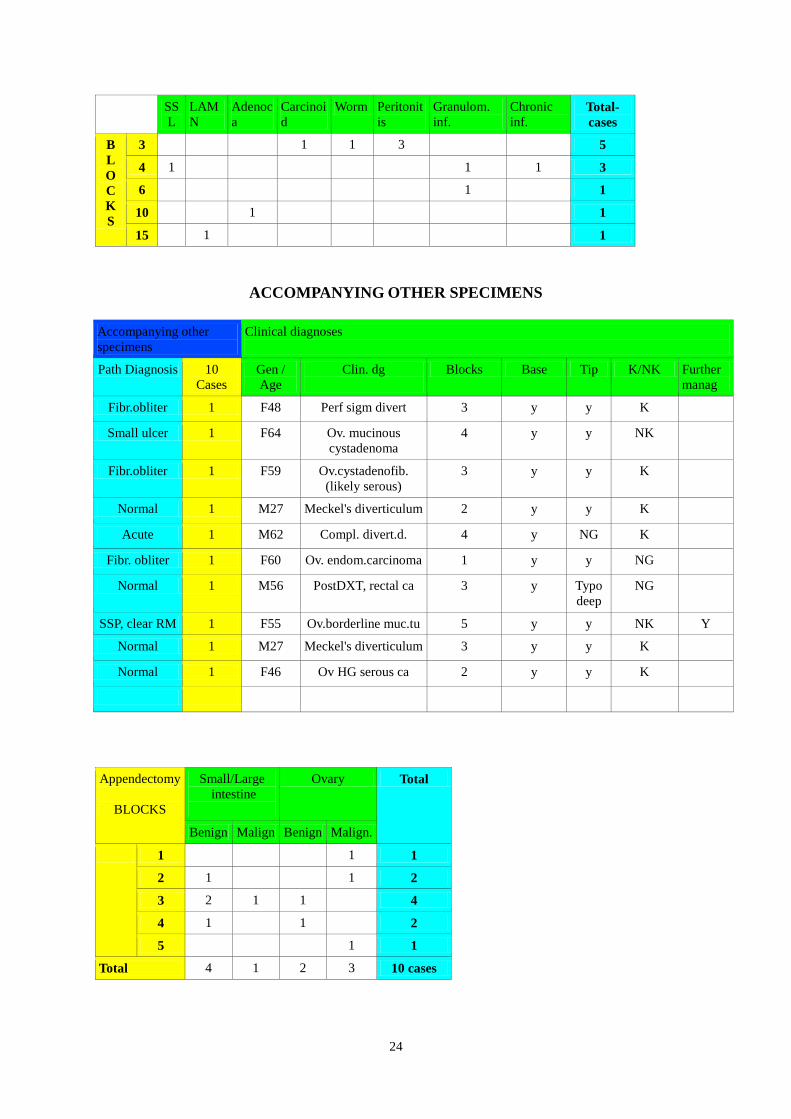
There were 11 (6.4%) cases diagnosed with other abnormal pathological findings 6 (54.5%) patients
26
were female. Most of the patients were of age between 16-50 yr. There were 3 specimens clinically
suspicious of tumour. 1 of them was LAMN and 1 adenocarcinoma. The 3rd
case was diagnosed with
granulomatous inflammation. 5 cases were clinically diagnosed as inflamed appendix, 1 of them
contained SSL, 1 carcinoid, 1 chronic inflammatory change and 2 cases showed peritonitis without
intramural inflammation. In 1 case with oxyuriasis the clinical diagnosis was RIF pain and in 2 cases
(peritonitis and granulomatous inflammation) no clinical diagnosis was given.
5 of the cases were trimmed into 3 cassettes (carcinoid, oxyuriasis and x3 cases of peritonitis), 3 cases
into 4 cassettes (x1 granulomatous inflammation, x1 chronic inflammatory changes, 1 SSL), 1 case
with granulomatous inflammation into 6 cassettes, 1 adenocarcinoma 10 cassettes and LAMN 15
cassettes. Within the pathology reports in 10 cases there was specified the resection margin /base and
11 cases the tip of the appendix. In 1 case (peritonitis) the possible sampling of the base and in 2
cases of the tip was not recorded within the pathology report.
1 case with perforated LAMN was submitted for specialist review to Basingstoke.
Appendectomy specimens were also accompanying other specimens in 10 (5.8%) cases. Only of them
with SSL was sent with an ovarian borderline mucinous tumour. The appendix was completely
submitted in 5 cassettes. This case was also reviewed by Gynaecopathology team in Glasgow.
It appears that from the information gathered on blocks taken that NHS Lanarkshire is taking a block
number commensurate with the adequate diagnosis of the cases submitted. As there are no definitive
guidelines on the number of blocks to be taken for a given clinical diagnosis it is difficult to determine
if NHS Lanarkshire is oversampling appendectomies.
By recommendation of the RCP, in all appendectomy specimens the resection margin and the tip
should be sampled together with at least one transverse section. In standard sampling 2 cassettes
would be probably appropriate if the appendix is only inflamed without perforation. 1 cassette would
be suitable if the appendix is small and narrow. Although, cassettes should not be overfilled.
In this study 35 (20.4%) cases were diagnosed as other than acute inflammation or were negative for
acute inflammation and 1 of the appendices was accompanying other specimen. Only 2 of them were
clinically suspicious of malignancy. In all other cases histopathological examination revealed
unexpected lesions which also required subsequent management or follow up of the patient.
It is not possible to determine that if a smaller number of blocks were taken if this would disclose all
lesions not visible intra-operatively or during trimming.
Comment:
NHS Lanarkshire will move to a new LIMS in 2019 and there is a plan to provide 2 cassettes for
standard sampling of the appendix. Further cassettes could be added if required by the dissectors.
27
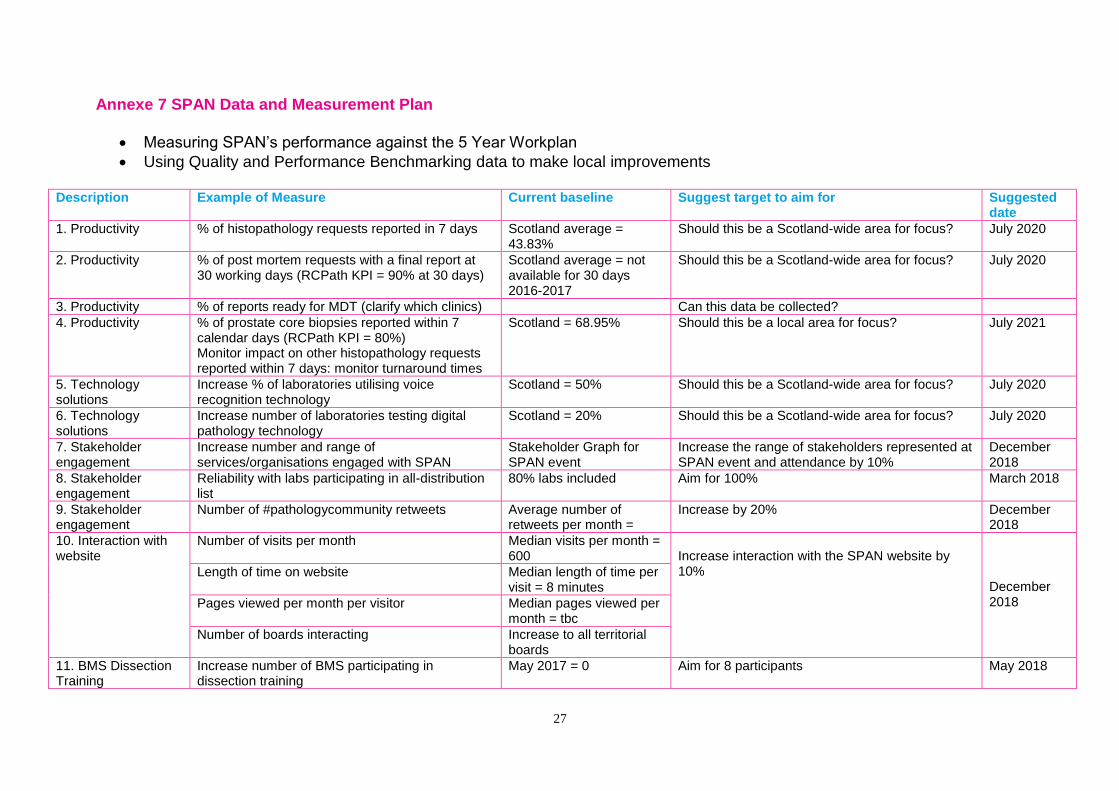
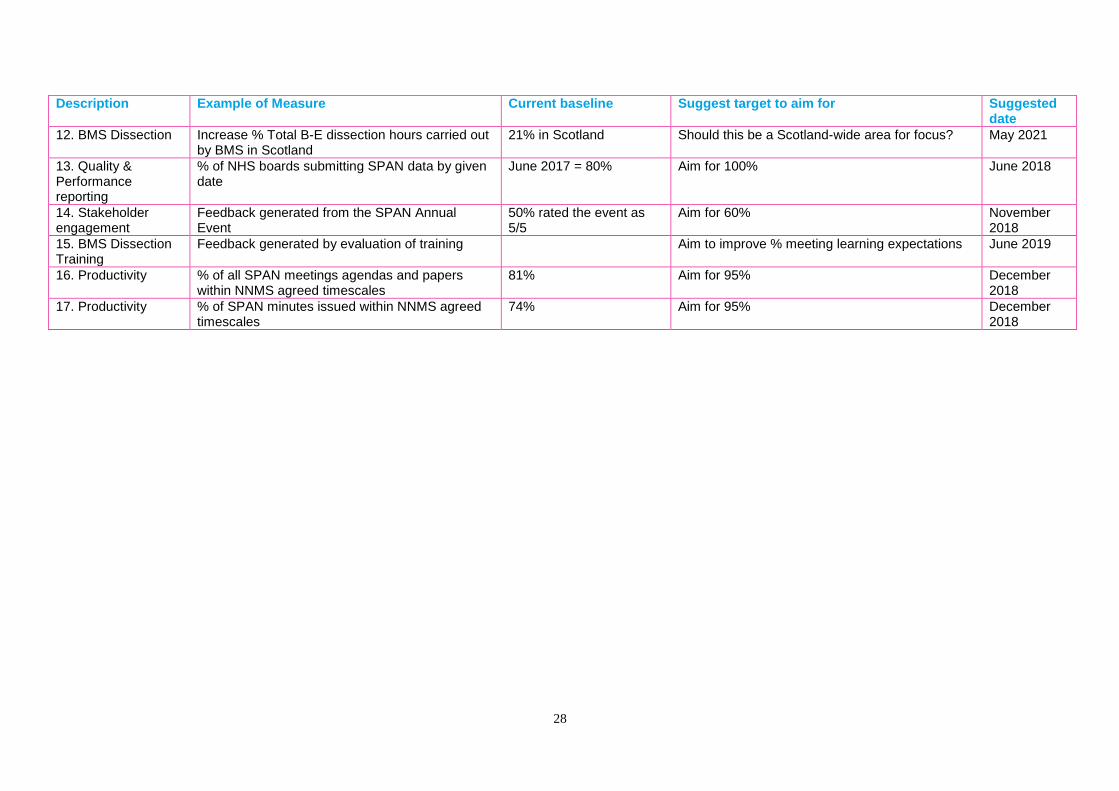
Annexe 7 SPAN Data and Measurement Plan
Measuring SPAN’s performance against the 5 Year Workplan
Using Quality and Performance Benchmarking data to make local improvements
Description Example of Measure Current baseline Suggest target to aim for Suggested date
1. Productivity % of histopathology requests reported in 7 days Scotland average = 43.83%
Should this be a Scotland-wide area for focus? July 2020
2. Productivity % of post mortem requests with a final report at 30 working days (RCPath KPI = 90% at 30 days)
Scotland average = not available for 30 days 2016-2017
Should this be a Scotland-wide area for focus? July 2020
3. Productivity % of reports ready for MDT (clarify which clinics) Can this data be collected?
4. Productivity % of prostate core biopsies reported within 7 calendar days (RCPath KPI = 80%) Monitor impact on other histopathology requests reported within 7 days: monitor turnaround times
Scotland = 68.95% Should this be a local area for focus? July 2021
5. Technology solutions
Increase % of laboratories utilising voice recognition technology
Scotland = 50% Should this be a Scotland-wide area for focus? July 2020
6. Technology solutions
Increase number of laboratories testing digital pathology technology
Scotland = 20% Should this be a Scotland-wide area for focus? July 2020
7. Stakeholder engagement
Increase number and range of services/organisations engaged with SPAN
Stakeholder Graph for SPAN event
Increase the range of stakeholders represented at SPAN event and attendance by 10%
December 2018
8. Stakeholder engagement
Reliability with labs participating in all-distribution list
80% labs included Aim for 100% March 2018
9. Stakeholder engagement
Number of #pathologycommunity retweets Average number of retweets per month =
Increase by 20% December 2018
10. Interaction with website
Number of visits per month Median visits per month = 600
Increase interaction with the SPAN website by 10%
December 2018
Length of time on website Median length of time per visit = 8 minutes
Pages viewed per month per visitor Median pages viewed per month = tbc
Number of boards interacting Increase to all territorial boards
11. BMS Dissection Training
Increase number of BMS participating in dissection training
May 2017 = 0 Aim for 8 participants May 2018
28
Description Example of Measure Current baseline Suggest target to aim for Suggested date
12. BMS Dissection Increase % Total B-E dissection hours carried out by BMS in Scotland
21% in Scotland Should this be a Scotland-wide area for focus? May 2021
13. Quality & Performance reporting
% of NHS boards submitting SPAN data by given date
June 2017 = 80% Aim for 100% June 2018
14. Stakeholder engagement
Feedback generated from the SPAN Annual Event
50% rated the event as 5/5
Aim for 60% November 2018
15. BMS Dissection Training
Feedback generated by evaluation of training Aim to improve % meeting learning expectations June 2019
16. Productivity % of all SPAN meetings agendas and papers within NNMS agreed timescales
81% Aim for 95% December 2018
17. Productivity % of SPAN minutes issued within NNMS agreed timescales
74% Aim for 95% December 2018
29
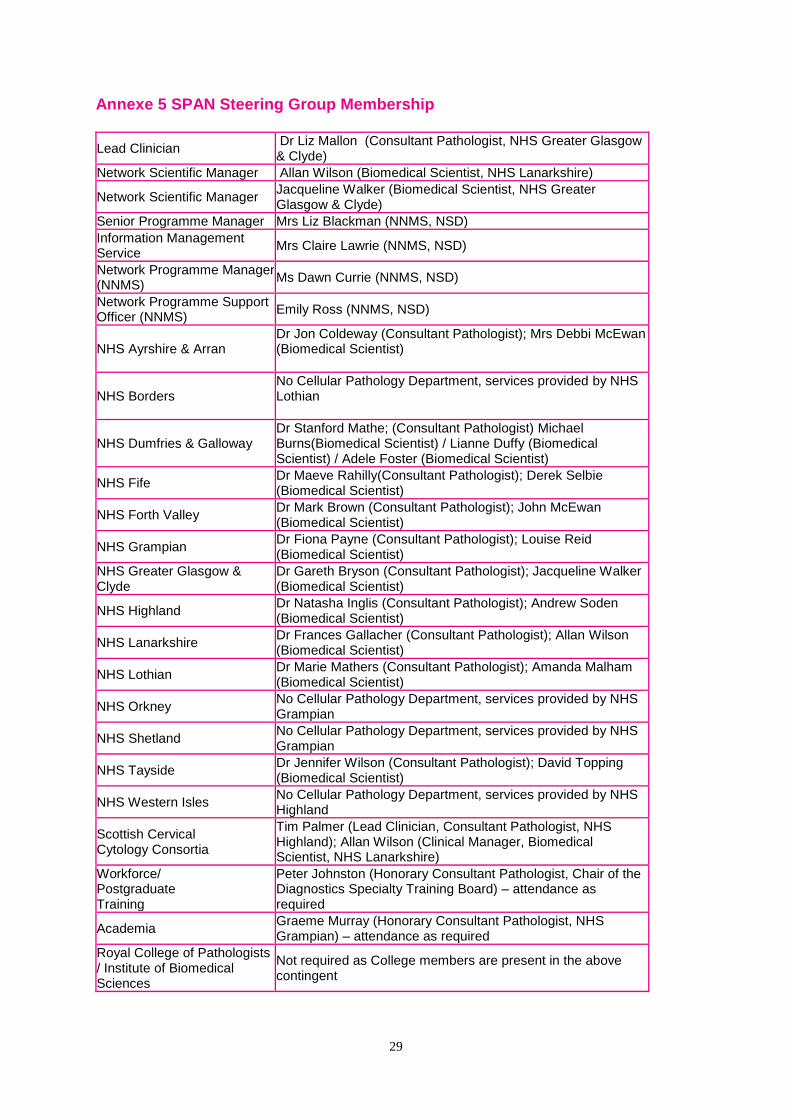
Annexe 5 SPAN Steering Group Membership
Lead Clinician Dr Liz Mallon (Consultant Pathologist, NHS Greater Glasgow & Clyde)
Network Scientific Manager Allan Wilson (Biomedical Scientist, NHS Lanarkshire)
Network Scientific Manager Jacqueline Walker (Biomedical Scientist, NHS Greater Glasgow & Clyde)
Senior Programme Manager Mrs Liz Blackman (NNMS, NSD)
Information Management Service
Mrs Claire Lawrie (NNMS, NSD)
Network Programme Manager (NNMS)
Ms Dawn Currie (NNMS, NSD)
Network Programme Support Officer (NNMS)
Emily Ross (NNMS, NSD)
NHS Ayrshire & Arran Dr Jon Coldeway (Consultant Pathologist); Mrs Debbi McEwan (Biomedical Scientist)
NHS Borders No Cellular Pathology Department, services provided by NHS Lothian
NHS Dumfries & Galloway Dr Stanford Mathe; (Consultant Pathologist) Michael Burns(Biomedical Scientist) / Lianne Duffy (Biomedical Scientist) / Adele Foster (Biomedical Scientist)
NHS Fife Dr Maeve Rahilly(Consultant Pathologist); Derek Selbie (Biomedical Scientist)
NHS Forth Valley Dr Mark Brown (Consultant Pathologist); John McEwan (Biomedical Scientist)
NHS Grampian Dr Fiona Payne (Consultant Pathologist); Louise Reid (Biomedical Scientist)
NHS Greater Glasgow & Clyde
Dr Gareth Bryson (Consultant Pathologist); Jacqueline Walker (Biomedical Scientist)
NHS Highland Dr Natasha Inglis (Consultant Pathologist); Andrew Soden (Biomedical Scientist)
NHS Lanarkshire Dr Frances Gallacher (Consultant Pathologist); Allan Wilson (Biomedical Scientist)
NHS Lothian Dr Marie Mathers (Consultant Pathologist); Amanda Malham (Biomedical Scientist)
NHS Orkney No Cellular Pathology Department, services provided by NHS Grampian
NHS Shetland No Cellular Pathology Department, services provided by NHS Grampian
NHS Tayside Dr Jennifer Wilson (Consultant Pathologist); David Topping (Biomedical Scientist)
NHS Western Isles No Cellular Pathology Department, services provided by NHS Highland
Scottish Cervical Cytology Consortia
Tim Palmer (Lead Clinician, Consultant Pathologist, NHS Highland); Allan Wilson (Clinical Manager, Biomedical Scientist, NHS Lanarkshire)
Workforce/ Postgraduate Training
Peter Johnston (Honorary Consultant Pathologist, Chair of the Diagnostics Specialty Training Board) – attendance as required
Academia Graeme Murray (Honorary Consultant Pathologist, NHS Grampian) – attendance as required
Royal College of Pathologists / Institute of Biomedical Sciences
Not required as College members are present in the above contingent