Embed Size (px)
Citation preview
Procedures for the management of Central Venous Access Devices (CVAD) forPatients on Home Parenteral Nutrition
Disclaimer: This document was prepared by the Scottish Nutrition Nurses Group and was up to date at the time of printing. It is the responsibility of the end user to ensure care when implementing.
Guidelines and Policies for central catheter managementStaff caring for the patient on HPN should have access to guidelines and policies to prevent
complications occurring with the central catheter. Evidence-based guidelines for preventing hospital-
acquired infections associated with the use of central venous access devices have been published by
(Pratt RJ et al 2007, O’Grady et al 2002).
The following procedures and protocols are available within this document:
Procedures/ Policies Page Number
Care of Exit site 10
Changing a connection device 11
Commencing Parenteral Nutrition via a external central catheter 12
Flushing the catheter 13
Commencing Parenteral Nutrition via a subcutaneous port 14
Flushing a catheter via subcutaneous port 15
Taking blood cultures 16
Complications 17
Fractured/ruptured catheter 23
Unblocking central venous access device 25
References 27
Managed Clinical Network members 29
Hand wash technique 36
Hand hygiene chart 37
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
1

Venous Access for Home Parenteral Nutrition
Definition
An intravascular catheter is defined as a ‘tubular device, single or multi lumen, designed to be partially or
totally inserted or implanted into the cardiovascular system for diagnostic and /or therapeutic purposes’.
Central venous access
Central catheters are used when permanent access is required for parenteral nutrition (PN). The routes
most commonly used for venous access are the subclavian vein or internal jugular vein. There is a vast
array of catheters available for the administration of PN.
The most frequently used catheters are:
External cuffed tunneled catheters: i.e. Broviac, Hickman
External tunneled catheter: i.e. Vygon Nutricath
Subcutaneous ports
Peripheral inserted central catheters
Single versus multi lumen catheters
Multi lumen central catheters can be used for a combination of HPN and other treatments such as,
chemotherapy or antibiotic therapy. It has previously been suggested that multi lumen catheters increase
the risk of catheter-related sepsis and should not be used for the administration of PN. Many authors
have refuted this. They report that there is no statistical difference in catheter-related sepsis, between
the uses of single or triple lumen catheters.
Unless there is a particular need for a multi lumen catheter, a single lumen catheter is generally
preferred for the patient on home parenteral nutrition. The workload associated with its use is less and is
generally preferred by the patient.
The choice of catheter is dependent on venous access available, duration of therapy and most
importantly patient preference. Table 1 lists the factors that should be taken into consideration when
determining the most suitable catheter for the patient.
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
2
Table 1 – Factors in choosing a catheter for HPN
Short or long term use
Catheter material: i.e. silicone or Polyurethane
Multi or single lumen catheter, Cuffed or non-cuffed catheter
Implantable or external device
Patient preference/ body image, patients ability to care for central catheter
Ease of sterile dressing applications
Cost
Gauge of catheter and vein diameter. The narrowest catheter in the largest vein will provide better flow and reduce vein damage
Method of catheter removal
As the availability of these intravascular devices increases, so must the health professional's knowledge
base. It is essential that the nutrition team have knowledge of which device may be best suited for each
patient and be aware of which catheter has the fewest known complications.
There is a place for each catheter in the care of the patient with HPN; the choice will often be determined
by the patient and their needs. Table 2 lists the common advantages and disadvantages of each
catheter.
Catheter insertion
The central catheter should be inserted in an aseptic environment under the supervision of an
experienced clinician. There is strong evidence that using ultrasound guidance is a more effective
method of insertion (British Committee for Standards in Haematology, 2006). Potential complications
associated with the insertion of the catheter include:
Pneumothorax Venous air embolism
Arterial puncture Catheter misplacement
Cardiac tamponade Cardiac arrhythmias
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
3

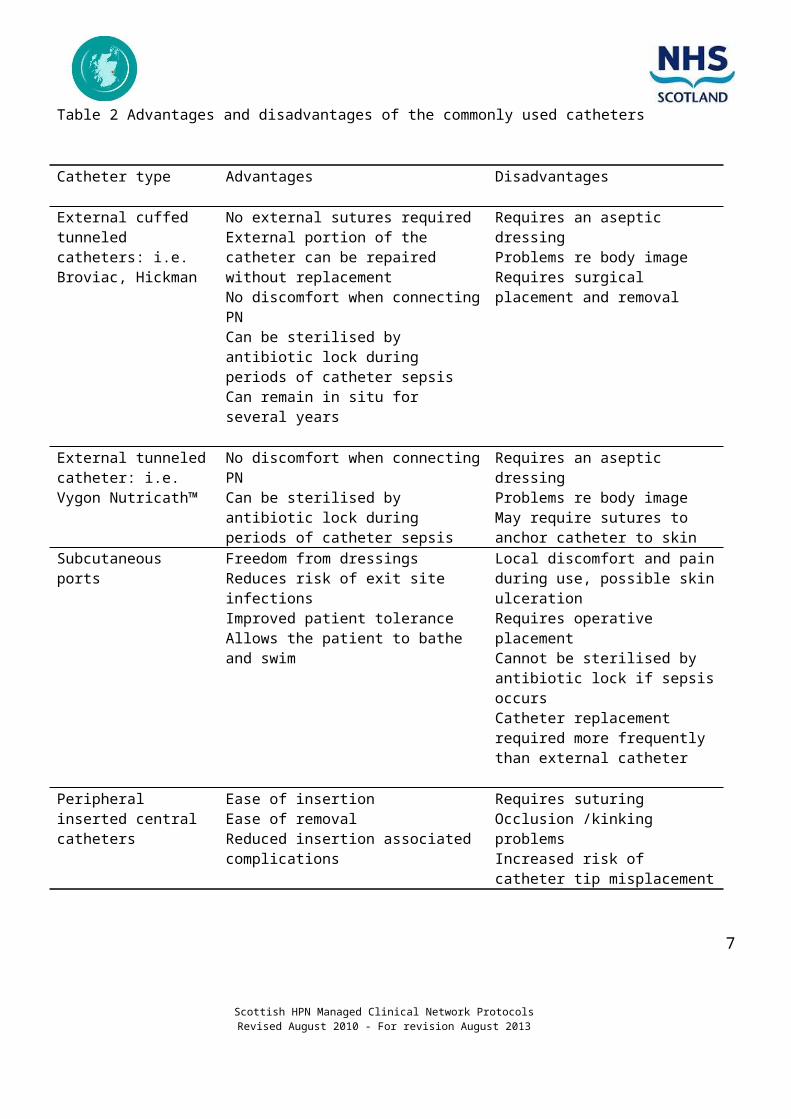
Table 2 Advantages and disadvantages of the commonly used catheters
Catheter type Advantages Disadvantages
External cuffed tunneled catheters: i.e. Broviac, Hickman
No external sutures requiredExternal portion of the catheter can be repaired without replacementNo discomfort when connecting PNCan be sterilised by antibiotic lock during periods of catheter sepsisCan remain in situ for several years
Requires an aseptic dressingProblems re body imageRequires surgical placement and removal
External tunneled catheter: i.e. Vygon Nutricath™
No discomfort when connecting PNCan be sterilised by antibiotic lock during periods of catheter sepsis
Requires an aseptic dressingProblems re body imageMay require sutures to anchor catheter to skin
Subcutaneous ports Freedom from dressingsReduces risk of exit site infectionsImproved patient toleranceAllows the patient to bathe and swim
Local discomfort and pain during use, possible skin ulcerationRequires operative placementCannot be sterilised by antibiotic lock if sepsis occursCatheter replacement required more frequently than external catheter
Peripheral inserted central catheters
Ease of insertionEase of removalReduced insertion associated complications
Requires suturingOcclusion /kinking problemsIncreased risk of catheter tip misplacement
A catheter placed in an optimal position, taking into consideration if patient is left or right handed, will
reduce potential complications. When inserting the catheter the clinician will consider the following
points:
The catheter tip should lie above the junction of the superior vena cava and right atrium
If a Dacron cuffed catheter is used, the cuff should be placed in the mid point of the tunnel away from
the exit site
A Chest X-Ray should be carried out to check the position of the catheter before PN is commenced
(unless inserted in radiology).
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
4

Central venous access device care
Central venous access device-related infections account for 90% of nosocomial (hospital acquired)
bloodstream infections. Despite the profuse availability of evidence, there continues to be a significant
diversity in practice of health care professionals. It has been well documented that experienced staff and
educational programs can have a significant impact on the rate of catheter related problems. For this
reason it is essential that all staff caring for a patient with a central venous access device have access to
educational material and researched based protocols and procedures.
Hand washing
It is well documented that the most common cause of the spread of nosocomial infection is via the hands
of health care workers because of their inability to correctly wash their hands. Therefore, the first crucial
step in the reduction of catheter related sepsis is knowledge of the principles of hand washing and the
use of gloves. Any procedure connected with an intravenous catheter requires the health care worker to
wash with an antibacterial handwash. The purpose of a handwash is to remove dirt and to reduce the
load of bacteria on the skin of the hands. Washing with soap and water will remove the transient
bacterial flora, and washing with a cleansing agent will reduce the resident bacteria on hands. It should
be noted however, that resident bacteria will not be totally eliminated by hand washing.
There are several types of handwash available for use, each have different properties and advantages.
Choosing the appropriate agent will depend on several factors. APIC guidelines for hand washing and
hand cleansing in heath care settings (1995) describe three stages:
Characteristics that are desired (e.g. rapid destruction in flora, spectrum of activity)
Evidence of safety and efficacy
Staff acceptance
The practice of hand washing
The use of any handwash solution will prove to be ineffective if staff do not employ the correct hand
washing technique. Various studies have concluded that health care workers do not wash their hands
effectively, leaving many parts of the hands not exposed to soap, water or handwash. In practice the
most commonly missed areas are the fingertips, the thumb and the inside of the fingers.
The use of an alcohol hand rub/gel is known to be effective. It is a powerful cleansing agent that can be
applied quickly to hands that are not soiled. It will rapidly kill transient bacteria and a proportion of the
resident bacteria.
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
5

The use of gloves
It is important that gloves are used in conjunction with hand washing and not in place of hand washing.
Many health care workers believe that gloves protect staff and patients from cross contamination, but in
reality this is not the case as hands can become easily contaminated under gloves when they are
unwittingly punctured or when they are removed. The lack of evidence regarding the benefits of using
sterile gloves has resulted in many teams developing procedures based on using a non-touch technique.
The care of the hub/the use of connection devicesSeveral studies have implicated contamination of the hub as the major source of catheter related sepsis
in catheters that remain in situ for more than two weeks. It is recommended that limited manipulations to
the catheter should occur, as each junction break brings additional risk of infection.
To reduce the risk of hub contamination:
Meticulous care must be taken when a break in the closed system occurs. Strict adherence to
policies and effective hand washing techniques are essential
If a multi lumen catheter is used, one lumen should be designated for the PN
A single lumen catheter should not be used for the administration of drug therapy or additional
intravenous fluids
The catheter should not be used for routine blood samples
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
6
The use of closed luer lock connection devices with a membrane allows access to the catheter whilst
maintaining a closed system. (E.g. Bionector, Interlink, Smartsite).
The perceived benefit of this system is:
Reduction in nursing workload
Reduction in use of sterile equipment / reduce costs
Reduction in needle stick injuries
Reduction in catheter related sepsis
Reduction in air embolus
Connection devices are now widely used in clinical practice. Some health professionals are concerned
about the potential risk of contamination. Several studies have addressed this issue and conclude that
there is no evidence that their use is associated with increased risk of catheter related infection. When
using connection devices the greatest risk leading to contamination is an inability to disinfect the device
before puncture. The most effective method of disinfection is the use of a combination of antiseptic spray
and alcohol.
Anecdotal evidence suggests that using the closed system is much less cumbersome for nursing staff
and patients to use and thus compliance with procedures may be better. However, the use of the closed
systems does not diminish the need for careful catheter techniques, and the adherence of staff to
guidelines and educational programmes, remains the most vital aspect in the rate of catheter related
sepsis.
Changing connection devices
Routine connection device changes should occur as per manufacturer’s instructions. It will be necessary
to change earlier if blood products or lipid deposits are present, if damaged, contaminated or after
routine flushing.
Care of central venous access device exit site – Principles of careThe exit site forms an artificial break in the skin and is, with the tunnel, a potential source of infection. An
aseptic technique is therefore required when cleaning the exit site and changing the dressing. It has
been suggested that the use of an aseptic technique by a specially trained person has more effect on
reducing the rate of catheter related infection than the type of cleansing agent or dressing used.
There are several issues that require to be addressed when developing guidelines for care of the
catheter exit site. These are firstly the most appropriate cleansing solution secondly the most appropriate
dressing and thirdly how often the dressing should be changed.
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
7

Cleansing Solutions
An alcoholic chlorhexidine gluconate solution (preferably gluconate in 70% isopropyl alcohol) should be
used to clean the catheter insertion site during dressing changes, and allowed to air dry (Pratt et al,
2007). An aqueous solution of chlorhexidine gluconate should be used if the manufacturer’s
recommendations prohibit the use of alcohol with their product (Pratt et al, 2007).
1. Dressings
The optimal dressing for the exit site remains controversial. The type of dressings frequently used
includes sterile gauze dressing and transparent occlusive dressing. Several studies have reported an
increased rate of infection associated with the use of transparent dressings. This is believed to be due to
an increase of moisture at the exit site. However, other studies have found no statistical difference in
rates of infection between transparent or gauze dressing. (It has been suggested than transparent
occlusive dressings are preferred by the patient, are cost effective, and can result in a reduction of
nursing time. The need for any type of dressing has also been studied. The frequency of exit site
infection is no greater when there was no dressing applied.
Dry dressing - Mepore™, Primapore™
Limitations associated with the use of this dressing, is the inability to visualise the exit site, and the need
for frequent manipulation of the dressing if the site needs to be checked. Their inability to provide a
bacterial and water barrier allows for the potential contamination from secretions or external moisture.
Transparent/ occlusive dressing – IV 3000™, Tegaderm™
The advantage of a transparent dressing is the ability to secure the catheter, to permit continuous
inspection of the site, to adhere well to dry skin, and to provide protection against external moisture
sources.
2. Dressing Changes
A Cochrane Review of gauze and tape versus transparent polyurethane dressings for CVAD concluded
that there was no evidence demonstrating any difference in the incidence of CR-related infections
between any of the dressing types compared in this review. Preferably, a sterile, transparent, semi-
permeable polyurethane dressing should be used to cover the catheter site. Transparent dressings
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
8

should be changed every 7 days or sooner if they are no longer intact or moisture collects under the
dressing. (Pratt et al, 2007)
Recommendations for care of the exit site
1. The procedure should be carried out by an experienced member of staff
2. Cleansing solution is recommended to cleanse the exit site
3. The exit site should be cleansed with swabs working away from the catheter site, outward and
downward. The movement of the catheter should be limited to prevent unnecessary trauma.
4. Assessment of the exit site at dressing changes is important to detect any sign of redness,
inflammation or exudates. Any changes should be documented.
5. If the area is encrusted or appears infected take a culture swab from the exit site
6. Do not use occlusive dressing if exit site is moist or leaking
7. Occlusive dressing should be changed weekly or before if there is drainage from the exit site or the
dressing has becomes non-occlusive
8. The need for a gauze dressing should be assessed daily and changed when inspection of the
insertion site is necessary or when the dressing becomes damp, loosened or soiled. A gauze
dressing should be replaced by a transparent dressing as soon as possible. (Pratt et al, 2007)
9. Dressings used on tunneled or implanted catheter insertion sites should be replaced every 7 days
until the insertion site has healed, unless there is an indication to change them sooner. (Pratt et al,
2007).
Procedure for dressing catheter exit site
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
9
Equipment
Antiseptic Hand Wash (as per hospital policy)
Dressing pack
Alcohol hand rub Individual single use chlorhexidine 2% alcoholSterile Gloves Sterile dressingDisposal Bag Alcohol wipes
Procedure
1. Explain procedure to the patient
2. Level 1 / Social hand wash.
3. Clean surface of trolley or tray as per local policy.
4. Level 2 / antiseptic hand wash.
5. Open outer pack of sterile dressing pack, place on trolley. Apply alcohol rub and
open inside of dressing pack, touching corners only.
6. Place gloves and dressing on sterile field and pour cleansing solution into receiver.
7. Remove existing dressing from the exit site, taking care not to disturb the catheter.
8. Apply alcohol hand rub to hands and allow to dry. Apply sterile gloves.
9. Using a cleansing solution, clean the catheter exit site from inside outwards and
downwards, limit movement of the catheter.
10. Allow cleansing solution to dry for a minimum of 30 seconds, apply dressing.
11. Tape catheter to chest wall.
12. Dispose of waste according to hospital policy.
13. Document in nursing notes
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
10

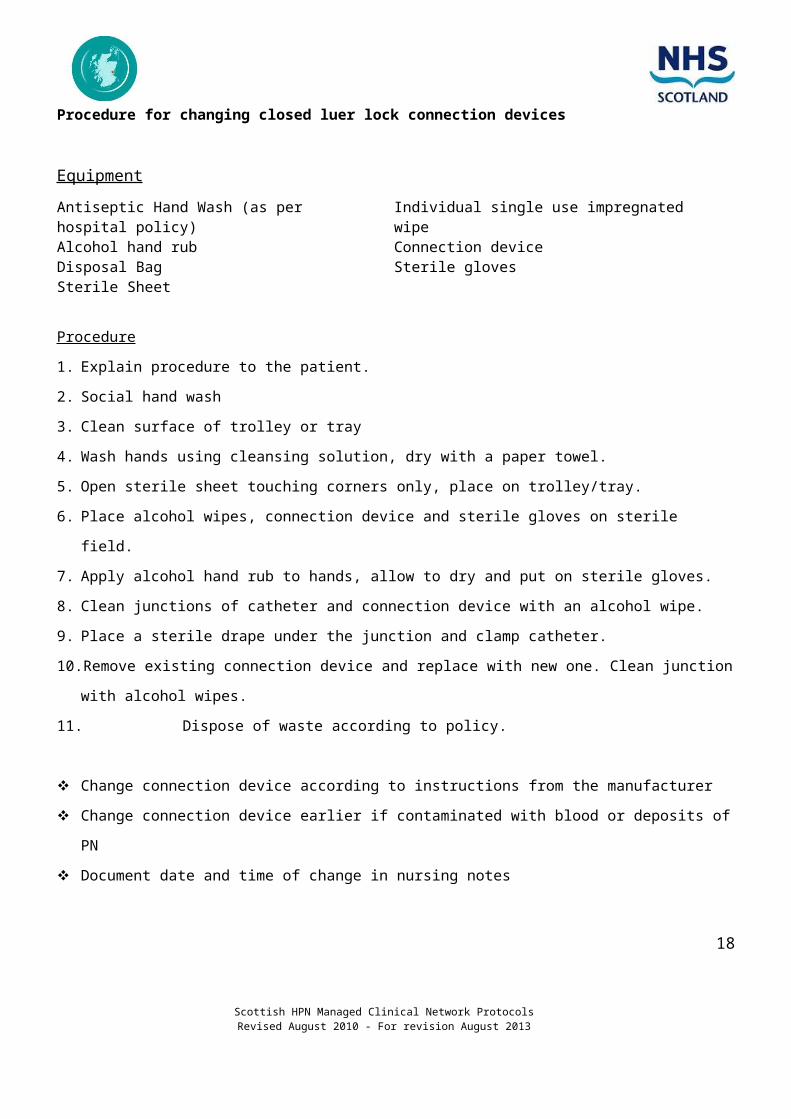
Procedure for changing closed luer lock connection devices
Equipment
Antiseptic Hand Wash (as per hospital policy) Individual single use impregnated wipeAlcohol hand rub Connection device Disposal Bag Sterile glovesSterile Sheet
Procedure
1. Explain procedure to the patient.
2. Social hand wash
3. Clean surface of trolley or tray
4. Wash hands using cleansing solution, dry with a paper towel.
5. Open sterile sheet touching corners only, place on trolley/tray.
6. Place alcohol wipes, connection device and sterile gloves on sterile field.
7. Apply alcohol hand rub to hands, allow to dry and put on sterile gloves.
8. Clean junctions of catheter and connection device with an alcohol wipe.
9. Place a sterile drape under the junction and clamp catheter.
10. Remove existing connection device and replace with new one. Clean junction with alcohol wipes.
11. Dispose of waste according to policy.
Change connection device according to instructions from the manufacturer
Change connection device earlier if contaminated with blood or deposits of PN
Document date and time of change in nursing notes
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
11

Procedure for commencing PN
Equipment
Parenteral Nutrition Bag Administration set Antiseptic hand washAlcohol hand rubPre-filled saline syringe (10ml)
Disposal BagSterile sheetAlcohol wipes Sterile Gloves (if used)
Procedure
1. Explain procedure to the patient.
2. Social hand wash.
3. Hang the solution bag from the IV drip stand
4. Clean surface of trolley or tray
5. Wash hands using cleansing solution, dry with a paper towel.
6. Open sterile sheet, alcohol hands and allow to dry, touch the corners only, and place on trolley/tray.
7. Place administration set, alcohol wipes and sterile gloves onto the sterile field.
8. Apply alcohol hand rub.
9. Open out the infusion set; do not touch either end of the set. Close the roller clamp.
10. Remove cap at end of the infusion set.
11. Clean the infusion port of the PN bag with an alcohol wipe, allow to dry.
12. Break the seal; do not touch the port after the seal is broken.
13. Insert the spike of the admin set into the port of the PN bag, using a gentle pushing/ twisting motion.
14. Prime the administration set as instructed.
15. Apply alcohol hand rub, allow to dry. (Put on sterile gloves if used).
16. Cleanse closed IV device with alcohol wipes, allow to dry.
17. Flush with saline.
18. Attach administration set to closed IV device.
19. Unclamp catheter, commence infusion via volumetric pump, and observe for
leakage.
20. Secure catheter with tape.
21. Dispose of waste according to Hospital policy.
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
12

Procedure for completing PN / Flushing Catheter
Equipment
Antiseptic hand wash 2 pre-filled syringes**Alcohol hand rub Needles x 2 + 2 syringes if not using pre-filled syringesDisposal Bag Prescribed flushing solutionSterile Sheet Sodium chloride 0.9 % 10mlAlcohol wipes Sterile Gloves (if used)
Procedure
1. Explain procedure to the patient.
2. Social hand wash
3. Discontinue PN by switching off pump and disconnect.
4. Clean surface of trolley or tray as per policy.
5. Wash hands using cleansing solution, dry with a paper towel.
6. Open sterile sheet, alcohol hands and allow to dry. Touch corners only, place on trolley/tray.
7. Place open alcohol wipes, /pre filled syringes onto sterile field. Apply alcohol hand rub to hands, allow
drying and put on sterile gloves.
8. Cleanse closed IV device / bung with alcohol wipes allow to dry for a minimum of 30 seconds
9. Inject flushing solution using a push pause technique, maintain positive pressure when removing
syringe.
10. If required, instill prescribed solution to lock the CVAD
11. Dispose of waste according to hospital policy.
12. Document.
* Do not use less than a 10ml syringe for flushing the catheter
** Pre-filled syringes with saline or heparin
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
13

Procedure for commencing PN via a Subcutaneous Port
Equipment
Parenteral Nutrition Bag Disposal BagAdministration set Dressing packAntiseptic hand wash Alcohol wipes Alcohol hand rub Sterile GlovesAntiseptic solution Gauze DressingHuber needle Pre-filled syringes
Procedure
1. Social hand wash
2. Hang the solution bag from the IV drip stand.
3. Clean surface of trolley or tray as per Hospital policy.
4. Wash hands using cleansing solution, dry with a paper towel.
5. Open sterile dressing pack, alcohol hands and allow to dry. Touch corners only arrange sterile pack
on trolley/tray.
6. Place open administration set, alcohol wipes, gauze dressing, needle, syringe and sterile gloves onto
the sterile field.
7. Pour antiseptic solution into receiver.
8. Apply alcohol hand rub, allow to dry.
9. Clean the infusion port of the PN bag with an alcohol wipe, allow to dry.
10. Break the seal; do not touch the port after the seal is broken.
11. Remove the cover from the administration set, do not touch the spike
12. Insert the spike of the IV tubing into the port of the PN bag, using a gentle pushing/ twisting motion.
13. Prime the administration set, place end of infusion set in an alcohol wipe.
14. Apply sterile gloves.
15. Attach pre-filled syringe sodium chloride 0.9%, prime Huber needle with solution.
16. Clean port site with cleanse solution, allow to dry.
17. Palpate port and hold between the index and middle finger of one hand. Pull the
skin tightly over the port to prevent slipping.
18. Push the needle firmly through the skin and port until it hits the bottom of the portal
chamber. Use a different part of the port for each insertion.
19. Flush the port with sodium chloride0.9%; confirm that fluid flows through the system.
20. Attach administration set to Huber needle.
21. Apply gauze dressing to secure Huber needle.
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
14

22. Set pump, volume and rate and commence infusion.
23. Dispose of waste according to hospital policy.
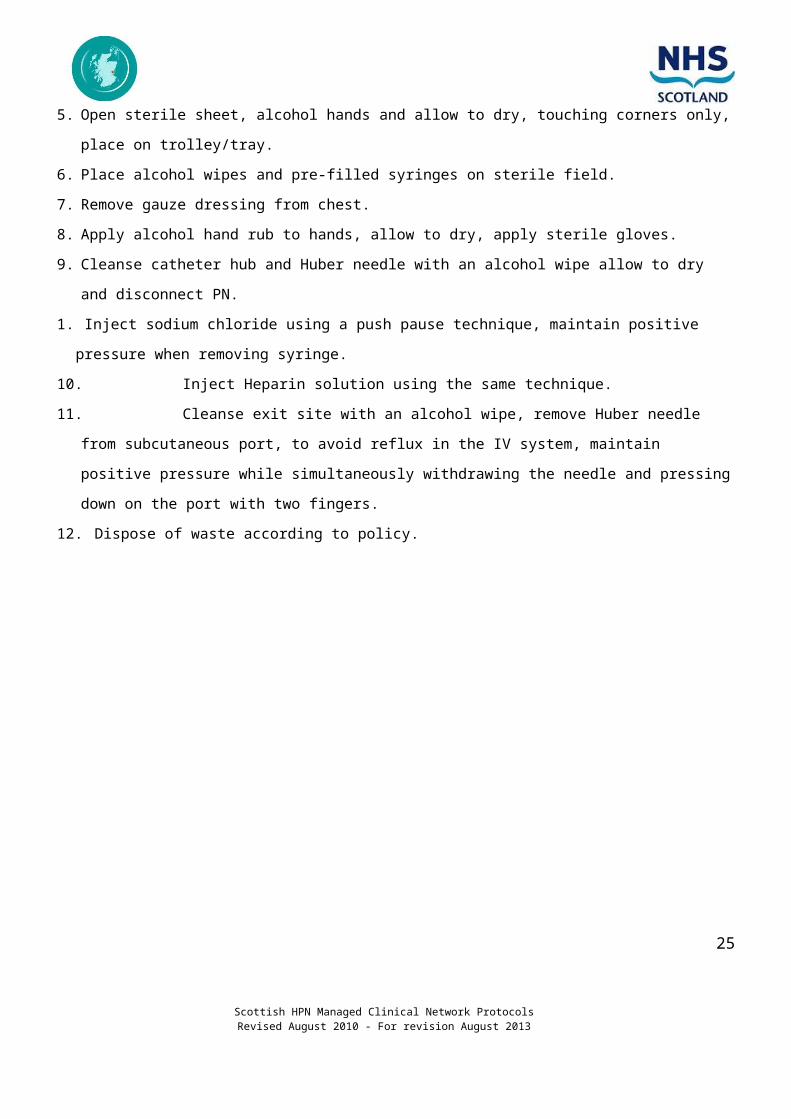
Procedure for flushing Subcutaneous Port (if removing the needle)
Equipment
Antiseptic Hand Wash pre-filled syringe Sodium chloride 0.9 % 10mlAlcohol hand rub Alcohol wipesDisposal Bag Heparin solutionSterile Sheet Sterile gloves
Procedure
1. Social hand wash
2. Discontinue PN by switching off pump.
3. Clean surface of trolley or tray as per Hospital policy
4. Wash hands using cleansing solution, dry with a paper towel.
5. Open sterile sheet, alcohol hands and allow to dry, touching corners only, place on trolley/tray.
6. Place alcohol wipes and pre-filled syringes on sterile field.
7. Remove gauze dressing from chest.
8. Apply alcohol hand rub to hands, allow to dry, apply sterile gloves.
9. Cleanse catheter hub and Huber needle with an alcohol wipe allow to dry and disconnect PN.
1. Inject sodium chloride using a push pause technique, maintain positive pressure when removing
syringe.
10. Inject Heparin solution using the same technique.
11. Cleanse exit site with an alcohol wipe, remove Huber needle from subcutaneous port, to avoid reflux
in the IV system, maintain positive pressure while simultaneously withdrawing the needle and
pressing down on the port with two fingers.
12. Dispose of waste according to policy.
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
15

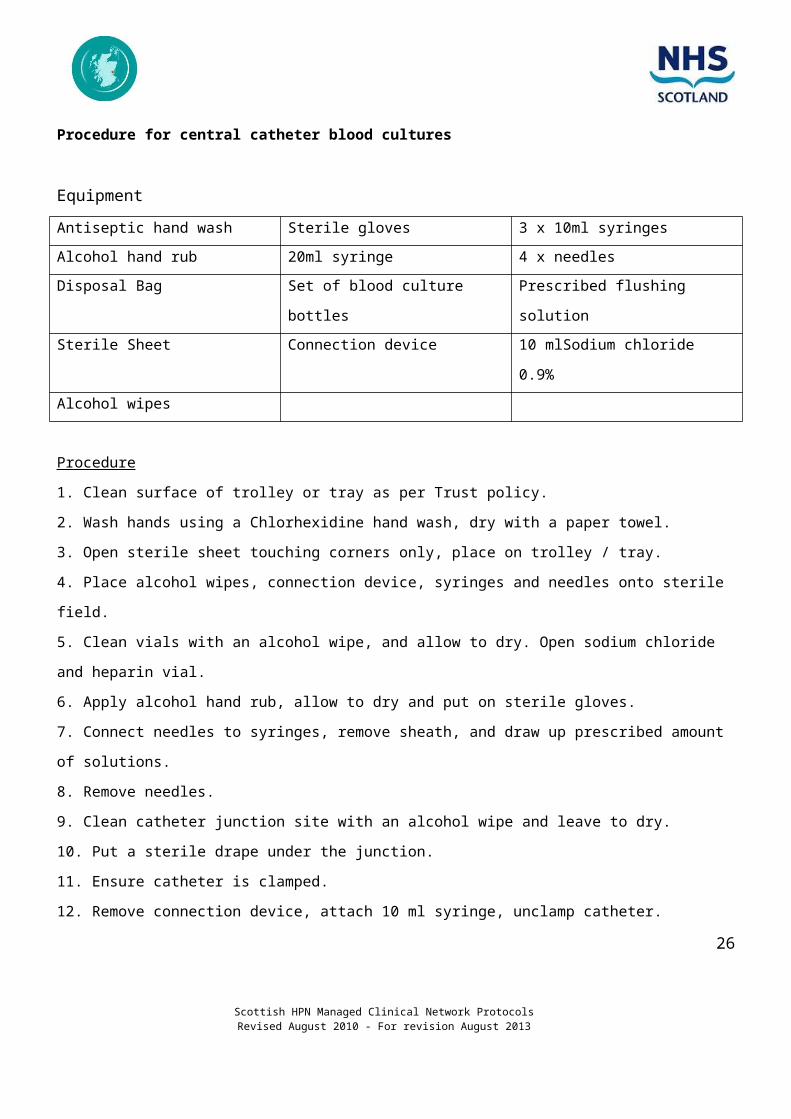
Procedure for central catheter blood cultures
Equipment
Antiseptic hand wash Sterile gloves 3 x 10ml syringesAlcohol hand rub 20ml syringe 4 x needlesDisposal Bag Set of blood culture bottles Prescribed flushing solutionSterile Sheet Connection device 10 mlSodium chloride 0.9%Alcohol wipes
Procedure1. Clean surface of trolley or tray as per Trust policy.2. Wash hands using a Chlorhexidine hand wash, dry with a paper towel.3. Open sterile sheet touching corners only, place on trolley / tray.4. Place alcohol wipes, connection device, syringes and needles onto sterile field.5. Clean vials with an alcohol wipe, and allow to dry. Open sodium chloride and heparin vial.6. Apply alcohol hand rub, allow to dry and put on sterile gloves.7. Connect needles to syringes, remove sheath, and draw up prescribed amount of solutions.8. Remove needles.9. Clean catheter junction site with an alcohol wipe and leave to dry.10. Put a sterile drape under the junction.11. Ensure catheter is clamped.12. Remove connection device, attach 10 ml syringe, unclamp catheter.13. Draw back 10ml of blood, clamp catheter then remove syringe.14. Attach 20-ml syringe; unclamp catheter, draw back 15 ml of blood using a 20-ml syringe.15. Clamp catheter and remove syringe.16. Flush catheter with 10 ml of sodium chloride 0.9%.17. Attach new connection.18. Inject Heparin solution into catheter.19. Clean top of culture bottles with an Alcohol wipe and allow to dry.20. Inject 7 ml of blood into each bottle using a separate needle for each culture bottle.
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
16

21. Dispose of waste according to Trust policy.
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
17
Complications
The network has prepared documents for the management of complications:
These include:
Protocol for the detection, prevention and treatment of central vein thrombosis.
Protocol for the management of catheter related sepsis.
Please contact your nutrition nurse specialist for a copy of the above.
InfectionDefinition of catheter related blood stream infection (CR, BSI) - “Clinical picture of spiking fever and
chills resulting from blood passage of micro organisms from an intra-vascular infusion system. Isolation
of the same organism from blood and catheter segments is considered definite proof”.
Definitions for CR, BSI Exit site infection – erythema, tenderness, induration or purulence within 2cm of the skin at the exit
site of the catheter
Tunnel infection- erythema, tenderness and induration in the tissues overlying the catheter and > 2cm
from the exit site
Catheter related bloodstream infection (CR, BSI) - isolation of the same organism from a semi-
quantitative or quantitative culture of the catheter segment and from the blood of a patient with
accompanying clinical symptoms of BSI and no other apparent source of infection
(Guidelines for prevention of intravascular device related infections: an overview 1996)
In practice, CR, BSI would be diagnosed by positive central blood cultures, clinical signs of septicaemia,
even in the absence of negative peripheral blood cultures.
The detection and treatment of CR, BSI This protocol should be available for all staff looking after patients on Home Parenteral Nutrition (HPN).
The decisions on whether to use antibiotics, to treat the sepsis or to immediately remove the catheter are
based on the:
type of micro-organism present
continuing need for the catheter
venous access of the patient
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
18

future need for PN
the general condition of the patient
previous or recent CR,BSI (recent sepsis sensitivities)
If patient with a central venous access device presents with an acute febrile episode:
Assess: history and examination to exclude other infections
Blood cultures (from each lumen): 1 x peripheral
1 x central
see Protocol – minimum volume required 0.5ml/bottle
- Check with local microbiologist
Blood sample for FBC & CRP, U+E’s, LFT’s, ESR glucose + creatinine
Exit site swab if inflamed
Chest X-ray(if clinically indicated)
Urinalysis / urine culture
Other samples as directed by assessment
Then follow protocol for suspected CR, BSI (see over).
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
19

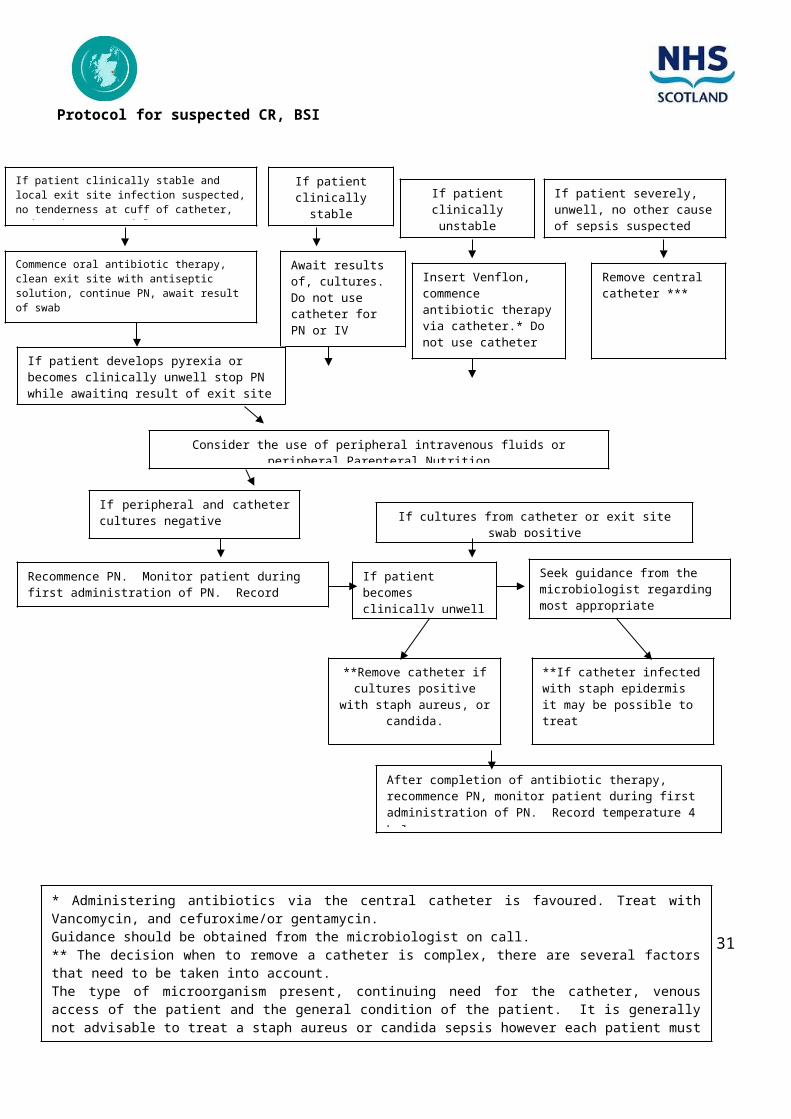
Protocol for suspected CR, BSI
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
20
If patient clinically stable and local exit site infection suspected, no tenderness at cuff of catheter, and patient apyrexial
If patient clinically stable If patient clinically
unstableIf patient severely, unwell, no other cause of sepsis suspected
Commence oral antibiotic therapy, clean exit site with antiseptic solution, continue PN, await result of swab
Await results of, cultures. Do not use catheter for PN or IV fluids
Insert Venflon, commence antibiotic therapy via catheter.* Do not use catheter for PN or IV fluids
Remove central catheter ***
If patient develops pyrexia or becomes clinically unwell stop PN while awaiting result of exit site swab
Consider the use of peripheral intravenous fluids or peripheral Parenteral Nutrition
If peripheral and catheter cultures negative If cultures from catheter or exit site swab
positive
Recommence PN. Monitor patient during first administration of PN. Record temperature 4 hrly
If patient becomes clinically unwell or pyrexial
Seek guidance from the microbiologist regarding most appropriate treatment
**Remove catheter if cultures positive with
staph aureus, or candida.
**If catheter infected with staph epidermis it may be possible to treat
After completion of antibiotic therapy, recommence PN, monitor patient during first administration of PN. Record temperature 4 hrly.
* Administering antibiotics via the central catheter is favoured. Treat with Vancomycin, and cefuroxime/or gentamycin.Guidance should be obtained from the microbiologist on call.** The decision when to remove a catheter is complex, there are several factors that need to be taken into account.The type of microorganism present, continuing need for the catheter, venous access of the patient and the general condition of the patient. It is generally not advisable to treat a staph aureus or candida sepsis however each patient must be considered individually.*** In paediatrics this may be the only IV access available.

CONFIRMED LINE INFECTION
If line infection is confirmed, consideration must be given to catheter removal and antibiotic treatment.
Catheter removal was once thought essential in the treatment of line infection but in recent years
catheter salvage rates of around 50% have been reported using antibiotics. Attempts at catheter salvage
are certainly justified in stable patients with blood stream infections with Staph epidermidis. Tunnel
infections with obvious pus are unlikely to respond to antibiotics. Exit site infections may be successfully
treated. Blood stream infections with coagulase positive staphylococci, MRSA, gram negative bacteria,
and yeasts are more dangerous and serious consideration should be given to catheter removal.
However, as far as possible catheter salvage should be attempted. Discuss with the nutrition team
consultant or SR and microbiologist prior to line removal. In particular yeast infections carry a significant
risk of spread to the eye with potential for loss of sight (Nightingale 1995). Therefore catheters infected
with yeasts should virtually always be removed. For other infections the benefits of more certain
eradication of sepsis by catheter removal must be balance against the difficulty of venous access in that
patient.
Antibiotic treatment depends on the bacterial sensitivities. Vancomycin administered into the catheter is
the mainstay but the antibiotic used will depend on local bacteriological advice. It seems sensible to
infuse the antibiotics down the catheter but this must be done with sterile precautions, preferably with the
antibiotic made up in the pharmacy sterile unit. If a single daily dosage can be given the number of
catheter interventions is reduced. Thereafter the antibiotic can be left in the catheter before flushing at
the commencement of the next infusion.
Confirmed line infection: Complications Port abscess
Septic thrombosis
Endocarditis
Osteomyelitis
Consider line removal and treat, guided by sensitivities and advice from pharmacist and
microbiologist.
General comments1. Consider line cultures at end of treatment completion where line salvage attempted.
2. Nearly every patient will require peripheral access for continued fluid and nutritional needs.
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
21

3. Consider advice from a microbiologist when planning a new line insertion. The interval before line
insertion is determined by the clinical case. Preferably, antibiotic treatment should be completed
before CVC insertion.
4. Consider screening fro MRSA and topical treatment in keeping with agreed local protocols.
5. When patients are slow to recover, consider complications and further investigation. Access to trans-
oesophageal echo-cardiograph may be helpful
6. Consider re-assessing patient line care technique.
Catheter occlusion There are many factors that may lead to occlusion of the central venous access device
Malposition of the catheter
A kink in the catheter
The formation of a fibrin sheath at the tip of the catheter can act as a one-way valve, allowing
saline to be flushed but preventing the withdrawal of blood into the catheter.
Fibrin deposits caused by the formation of a clot due to stagnate blood which has been left within
the lumen of the catheter
Lipid sludge caused by the formation of lipid deposits
Drug precipitation
Factors affecting the incidence intra luminal occlusion: Catheter material
The catheter flushing technique
Inappropriate use of heparin solution
The early detection and treatment of a partial blockage
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
22

Flushing the catheter The patency of the CVAD should be checked prior to administration of feed. Central venous catheters
should be flushed with an anticoagulant when the device is not in regular use, unless advised otherwise
by the manufacturer (Pratt et al., 2007). It is usually recommended that pressure-activated valved
catheters and some positive pressure flush devices are flushed with 0.9% sodium chloride (Camp
Sorrell, 2004; INS, 2006; Pratt et al., 2007). The volume of the flush solution should be equal to at least
twice the volume of the catheter and add-on devices – usually 5–10 ml. The concentration of heparin
should be the lowest possible that will maintain patency – usually 10iu heparin in 1 ml 0.9% sodium
chloride (except with implanted ports which may require 100iu/ml heparin). Frequency of flushing should
be weekly for long term central venous access devices, unless occlusive problems indicate otherwise
(Kelly et al., 1992; Dougherty and Watson, 2008) or every 4 weeks for an implanted port (Camp Sorrell,
2004). Flushing with 0.9% sodium chloride solution to ensure and maintain patency should be performed
using a pulsated push-pause and positive pressure method. (NICE, 2003; INS, 2006).
Detection of an intra luminal occlusion:
1. Determine whether there is a mechanical cause for the blockage
2. Rule out a kink in the tubing or an external force causing obstruction
3. Arrange for a chest X-ray to be carried out to determine the position of the tip of the catheter.
4. Exclude the presence of a central venous thrombosis
5. If the catheter remains blocked, aspirate the catheter then flush with saline. Do not use extreme force
as forceful flushing can rupture the catheter and cause serious problems to the patient e.g. transitory
embolus. A syringe smaller than 10 ml should not be used due to the increased pressure that can be
exerted on the catheter
6. If the catheter remains occluded determine the most likely cause of occlusion, and consider
treatment options
Treatment options – see Protocol for the detection, prevention and treatment of central vein thrombosisFibrin deposits
Fibrin deposits may respond to the administration of urokinase (Wachs 1990). Obstructed catheters are
injected with 5,000 units of urokinase, left in situ for an hour, then aspiration of the solution and residual
clot attempted. If aspiration is unsuccessful, repeat attempts can be made. If this remains unsuccessful,
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
23

a urokinase infusion of 40,000 units can be infused over 6 hours. If occlusion is still present a further 6
hour infusion of 40,000 units can be prescribed.
Lipid Occlusions
The use of lipid 3 in 1 mixes can result in the presence of lipid deposits within the lumen of the catheter.
In an attempt to prevent this problem, some centres infuse the lipid infusion separately however the
practicality of this for the patient on home parenteral nutrition is much more difficult. The use of 70 %
ethanol solution can often clear the catheter (Pennington 1992). Replacing a saline flush with a 20 %
ethanol flush after lipid infusions may also prevent the problem of lipid occlusion.
Obstructed catheters are injected with 4 ml of a 70% solution of ethanol in sterile water. Ethanol is left in
the catheter for an hour then aspirated and flushed.
Drug Precipitation / Mineral deposits
Catheters can become blocked with drug precipitation or a build up of mineral deposits. These can
occasionally be reversed by the use of hydrochloric acid 0.1% in 3ml (Werlin et al 1995).
Ter Borg et al (1993) suggest that central venous access devices, which are unresponsive to treatment
with urokinase, ethanol, or hydrochloric acid, can be unblocked with a perfusion of 10 to 20 ml of 0.1
sodium hydroxide solution. They do point out however, that it is important to establish the safety of
catheter materials before attempting to administer a sodium hydroxide solution.
Fractured / Ruptured central catheters
Reasons for rupture
Rupture from an attempt to irrigate occluded catheter with a small syringe. Infusion pressures should
never exceed 25 psi. As smaller syringes generate more pressure than larger syringes, the catheter
should be never be flushed with a syringe smaller than 10 ml
Repeated clamping (wear and tear)
Contact with a sharp object (accidentally cut or pierced)
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
24
Rupture of the external part of the catheter is often easily detected as leakage of PN solution can be
seen. However internal fractures, which can cause infiltration of fluids into the surrounding tissues, may
not be easily recognized. Symptoms of pain and swelling around the catheter may alert staff to the
problem. A diagnosis can be made by the use of contrast studies (Verhage and Van Bommel 1999). If an
internal fracture is diagnosed the catheter should be removed immediately.
What to do if the event of an external catheter rupture
1. When damage occurs, the catheter should be immediately clamped or kinked to prevent the
possibility of air embolism, loss of blood or entry of microorganisms.
2. The catheter should be clamped between the catheter exit site and damaged area. The clamp must
remain in place during the repair procedure.
3. To repair the damaged external segment of the catheter it is recommended that there is at least 3cm
of undamaged catheter remaining beyond the skin exit site.
4. The catheter can be repaired on several different occasions, as long as there is sufficient length of
catheter externally.
It is important that the patient has access to the following:
A clamp to seal off the catheter in case of fracture or puncture
A repair kit and silicone gel which is within 'use by' date should be held in the designated area of the
hospital……………………………………………………………………………………
A supply of Urokinase and alcohol should be held in the parent ward of the hospital
Urokinase is available from pharmacy in 10000 unit ampoules of freeze dried powder
One ampoule mixed with 2ml water provides 5000 units / ml
This 1ml should then be diluted to 3ml with sodium chloride
The dosage is 5000units in 3ml
The paediatric dose is 5000 unit in 2 ml
The patient on HPN should be given written instructions on the first- aid management of an external
catheter rupture. Each patient should be supplied with a small clamp at home.
Repair of ruptured catheters
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
25
1. Contact nursing/medical member of multidisciplinary nutrition team
2. The appropriate repair kit should be available
3. The catheter repair is carried out under strict aseptic technique as per manufactures instructions
4. If necessary the catheter may be used after 4 hours, although the joint will not achieve full
mechanical strength for 48 hours. If possible the catheter should not be used for 48 hours,
decreasing further risk of rupture/fracture.
5. A prophylactic antibiotic may be of use if appropriate.
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
26

Procedure for unblocking central venous access device
Equipment
Cleansing Hand Wash 10ml syringes x 3Alcohol hand rub Needles x 3Disposal Bag Ampoule of Heparin saline solutionSterile Sheet Ampoule of Sodium chloride 0.9 % 10mlAlcohol wipes Alcohol or 70% Urokinase solution
Procedure
1. Explain to patient
2. Social hand wash
3. Clean surface of trolley or tray as per Hospital policy.
4. Wash hands using antiseptic hand wash, dry with a paper towel.
5. Open sterile sheet, alcohol hands and allow to dry. Arrange sterile sheet, touching corners only,
place on trolley/tray.
6. Place alcohol wipes, syringes, ampoules and needles onto sterile field.
7. Apply alcohol hand rub to hands, allow to dry, apply sterile gloves.
8. Attempt aspiration of the catheter.
9. Instill Urokinase / alcohol. Do not use extreme force
10. Leave the Urokinase / alcohol in situ for 2-4 hours. Aspirate back
11. Flush catheter with sodium chloride 10 ml using push pause technique then instill heparin solution
using push pause technique.
12. Dispose of waste according to Hospital policy.
* Do not use less than a 10ml syringe for flushing the catheter
Alcohol 70% in 4ml for lipid occlusion
Urokinase 5000iu for fibrin occlusions
AS PER MANUFACTURER’S INSTRUCTIONS
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
27
The following contacts can be used in an emergency for advice:
Name & position Telephone number
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
28

References
APIC Guidelines for hand washing and hand antisepsis in health care settings (1995) American Journal of Infection Control 23 (4) 251-69.
Appelgren P Ransjo U Bindslev L et al (1996) Surface heparinization of central venous access devices reduces microbial colonization in vitro and in vivo: results from a prospective randomized trial. Critical Care Medicine 24 (9) 1482-9.
Barzaghi A, Dell'Orto M, Rovelli A, et al (1995) Central venous access device clots: incidence, clinical significance and catheter care in patients with hematologic malignancies. Pediatric Hematology and Oncology 12(3) 243-50. Department of Health (2001). Guidelines for preventing infections associated with the insertion and maintenance of central venous access devices. Journal of Hospital Infection. 47 (suppl): S47-67. Kyle LA Turner BS (1999) Efficacy of saline vs. heparin in maintaining 24 gauge intermittent intravenous catheters in a rabbit model. Neonatal Netw 18 (6) 49-54. Le Duc K (1997) Efficacy of normal saline solution versus heparin solution for maintaining patency of peripheral intravenous catheters in children Journal of Emergency Nurse (4) 306-9.
Mudge B, Forcier D, Slattery MJ (1998) Patency of 24-gauge peripheral intermittent infusion devices: a comparison of heparin and saline flush solutions. Pediatric Nursing 24(2) 142-5. Pennington CR, Pithie AD (1987) Ethanol lock in the management of catheter occlusion Journal of Parenteral and Enteral Nutrition 11 (5) 507-8. Randolf AG Cook DJ Gonzales CA Andrew M (1998) Benefit of heparin in peripheral venous and arterial catheters: systematic review and meta-analysis of randomized trials British Medical Journal 316 (7136) 969-75. Sitges-Serra A, Pi-Serra T, Garces JM et al (1995). Pathogenesis and prevention of catheter related septicaemia. American Journal of Infection Control 23 (5) 310-16.
Taylor D Myers ST Monarch K 1996 Use of occlusive dressings on central venous access device sites in hospitalised children. Journal of Pediatric Nursing 11 (3) 169-74. ter Borg F, Timmer J, de Kam SS, Sauerwein HP (1993) Use of sodium hydroxide solution to clear partially occluded vascular access ports. Journal of Parenteral Enteral Nutrition 17(3):289-91.
Verhage AH van Bommel EFC (1999) Catheter fracture: an under recognised and serious condition Journal of Vascular Access Devices 4 (2) 33-4. Wachs T (1990) Urokinase administration in pediatric patients with occluded central venous access devices Journal of intravenous nursing 13 (2) 100-2. Weber DR (1991) is heparin really necessary in the lock, and if so how much? DICP (4) 399-407.
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
29

Werlin SL, Lausten T, Jessen S, Toy L, Norton A, Dallman L, Bender J, Sabilan L, Rutkowski D (1995) Treatment of central venous access device occlusions with ethanol and hydrochloric acid. Journal of Parenteral Enteral Nutrition 19 (5)416-8. Zevola DR Dioso J Moggio R (1997) Comparison of heparinized and non heparinized solutions for maintaining patency of arterial and pulmonary artery catheters American Journal of Critical Care 6 (1) 52-5.
Pratt RJ, Pellowe CM, Wilson JA, et al (2007) National Evidence-Based Guidelines for Preventing Healthcare-Associated Infections in NHS Hospitals in England. Journal of Hospital Infection 65S, S1-S64.
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
30
Members of the Managed Clinical Network
Name Telephone E-mail AddressNutrition Support NursesDorothy Barber 01224 552946 [email protected] Aberdeen Royal Infirmary, ABERDEEN, AB25 2ZNLinda Davidson 0141 201 5243 [email protected] Victoria Infirmary, Langside Rd , GLASGOWMerrie Dwan 01224 553641 [email protected] Royal Aberdeen Children’s Hospital, ABERDEENLesley Faulds 01562 521133 [email protected] Crosshouse Hospital, KILMARNOCK, KA2 0BEJulie Fyall 01382 660111 [email protected] Ninewells Hospital, DUNDEE, DD1 9SYCraig Hurnauth 0141 201 6060 [email protected] Southern General Hospital, GLASGOWDawn Jordan 0141 211 4077 [email protected] Glasgow Royal Infirmary, Alexandra Parade, GLASGOWFiona MacKay 0141 211 4077 [email protected] Glasgow Royal Infirmary, Alexandra Parade, GLASGOWIsobel MacLeod 01412 321877 [email protected] Yorkhill Hospital, GlasgowChristina McGuckin 0141 201 9343 [email protected] Yorkhill Hospital, GLASGOWGill McHattie 0141 201 6060 [email protected] Southern General Hospital, GLASGOWKaren McIntyre 01382 740092 [email protected] Ward 28 Ninewells Hospital, DUNDEELorraine McVie 01315 373695 [email protected] Western General Hospital, EdinburghCarol Muir 0131 242 3635 [email protected] Royal Infirmary of Edinburgh, Little France, EDINBURGHCatherine Paxton 0131 537 1669 [email protected] Royal Hospital for Sick Children, EdinburghMay Shaw 01383 623623 m.shaw1@ nhs.net Queen Margaret Hospital, DUNFERMLINENancy Smith 0141 314 7117 [email protected] Royal Alexandra Hospital, Corsebar Rd, Paisley, PA2 9PNJan Tait 01382 740078 [email protected] Ninewells Hospital, DundeeKirsty Turnbull 01382 660111 [email protected] Ninewells Hospital, DUNDEE, DD1 9SYLynsey Watt 01412 111014 [email protected] Gartnavel General Hospital, Glasgow
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
31
ConsultantsRachel Edwards (clinical scientist)
01412 010350 [email protected] Yorkhill Hospital, Glasgow
Dan Lassman 07875836662 [email protected] Consultant GastroenterologistSabarinathan Loganathan
01224 558565 [email protected] Consultant Gastroenterologist, Aberdeen
Jonathan Manning 01896 826211 [email protected] Consultant Gastroenterologist, Melrose, BordersDavid Mitchell [email protected] Oliver 01786 434067 [email protected] SRIArindam Sengupta [email protected] DunfermlineSaha Subrata 01387 246246 [email protected] Dumfires&Galloway Royal Infirmary
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
PhysiciansAlistair McKinlay 01224 552312 [email protected] Consultant Gastroenterologist, Aberdeen Royal Infirmary
ABERDEEN, AB25 2ZNNigel Reynolds 01382 660111 [email protected] Consultant Gastroenterologist, Ninewells Hospital
DUNDEE, DD1 9SYAlan Shand 01315 371755 [email protected] Consultant Gastroenterologist, Western General Hospital,
EDINBURGHJohn Todd 01383 660111 [email protected] Consultant Gastroenterologist, , Ninewells Hospital
DUNDEE, DD1 9SYBrian Tregaskis 01397 702481 [email protected] Belford Hospital, NHS HighlandHazel Younger 01463 705442 [email protected] Raigmore Hospital, Inverness
32
Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
SurgeonsRon Coggins 01463 706360 [email protected] Consultant Surgeon, Assynt House, NHS HighlandKen Fearon 0131 536 9009 [email protected] Consultant Surgeon, New Royal Infirmary, Little France,
EDINBURGHRuth McKee 0141 211 4286 [email protected] Consultant Colorectal Surgeon, Royal Infirmary
16 Alexandra Parade, GLASGOW G31 2ERFraser Munro 01315 360649 [email protected] Consultant Paediatric Surgeon, EdinburghSatheesh Yalamarthi [email protected] Consultant Surgeon, Dunfermline
BiochemistsAlison Avenell 01224 554336 [email protected] Clinical Biochemist, Aberdeen Royal Infirmary,
ABERDEEN, AB25 2ZNBernie Croall 01224 554620 [email protected] Clinical Biochemist, Aberdeen Royal Infirmary
ABERDEEN, AB25 2ZNAnne Cruikshank [email protected] Department of Biochemistry, Southern General Hospital
GLASGOW G51 4TFAndy Duncan 0141 211 4494 [email protected] Biochemist, Macewan Building, Royal Infirmary, 84 Castle
Street, GLASGOW G4 OSFPeter Galloway [email protected] Yorkhill Hospital, GlasgowMatty Lough 01292 610555 [email protected] Consultant Biochemist, Crosshouse Hospital,
KILMARNOCK, KA2 0BEArchie McConnell 0141 2014444 [email protected] Dept. Clinical Biochemistry, Inverclyde Royal Hospital,
Greenock, PA16 0XN.Denis O'Reilly 0141 211 4631 [email protected] Consultant Clinical Biochemist, McEwen Building, Royal
Infirmary, 84 Castle Street, GLASGOW G4 OSFBill Simpson 01224 554620 [email protected] Consultant Clinical Biochemist, Aberdeen Royal Infirmary
ABERDEEN, AB25 2ZNRajeev Srivastava 0141 201 4444 [email protected] Yorkhill Hospital, Glasgow
33

Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
PharmacistsLynn Aitchison 01463 236189 [email protected] Senior Pharmacist, Assynt House, NHS HighlandNicola Cairns 01412 114265 [email protected] Senior Pharmacist, GRI, GlasgowGraham Conkie 0141 2010625 graham.conkie@ggc scot.nhs.uk Principal Pharmacist (Production), Pharmacy Production
Unit, Western Infirmary, Dumbarton Road, GLASGOW G11 6NT
Utie Dediare 01224 553221 [email protected] Pharmacist, AberdeenJoanne Dunne 01419 515000 [email protected] Specialist clinical pharmacist, ClydebankSimon Fraser [email protected] Yorkhill Hospital, GlasgowDavid Hoole 01315 369009 [email protected] Clinical Pharmacist, EdinburghSteven Leadbetter 0141 2010625 [email protected] Senior Pharmacist, Aseptic Unit, Glasgow Royal
Infirmary,GLASGOW
Tommy McEwan 01382 660111 [email protected] Pharmacy Dept. Ninewells Hospital, DundeeVicki Welch [email protected] Nutritional Prescribing Advisor, GlasgowLorna Wilson 01412 019321 [email protected] Senior Pharmacist, Glasgow
DietitiansKimberley Brown 01412 012154 [email protected] Southern General Hospital, GlasgowElaine Buchanan 01412 019368 [email protected] Yorkhill Hospital, GlasgowEmma Hughes 01463 235189 [email protected] Renal dietitian, Assynt House, NHS HighlandJennifer Livingstone 01315 360311 [email protected] Senior Paediatric Dietitian, EdinburghJanice McKinlay 01224 552935 [email protected] Senior Dietician, Department & Nutrition & Dietetics,
Aberdeen Royal Infirmary, ABERDEEN AB25 2ZNLinda Murray 0141 211 4763 [email protected] Department of Nutrition & Dietetics, The Royal Infirmary
Alexandria Parade, GLASGOWRegina O’Connor [email protected] Paeds dietitian, Ninewells Hospital, DundeeEvelyn Ogilvie 07999980083 [email protected] Lead dietitian, InvernessKathryn Ralston 01382 660111 [email protected] Dietician, Ninewells Hospital, DUNDEE, DD1 9SY
Kathleen Ross [email protected] Dietitian, AberdeenElizabeth Stevenson 01343 567396 [email protected] Senior dietitian, ElginKerry Yuill 01315 369009 [email protected] Deaconess House, Edinburgh
34

Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
PaediatricsMike Bisset 01224 553035 [email protected] Royal Aberdeen Children’s HospitalDiana Flynn 0141 201 0313 [email protected] Yorkhill Hospital, Glasgow
Dagmar Kastner 01382 660111 [email protected] Ninewells Hospital, DundeeParaic McGrogan [email protected] Yorkhill, GlasgowDavid Wilson 0131 536 0661 [email protected] Consultant Paediatric Gastroenterologist, Royal Hospital
for Sick Children, EDINBURGH
35

Scottish HPN Managed Clinical Network ProtocolsRevised August 2010 - For revision August 2013
Patient representativesSharon Bell [email protected] GlasgowRuth Grant [email protected] AberdeenMargaret McDonald
01382 819072 Dundee
Thelma Milne Aberdeen
Other staffWendy Cunningham
[email protected] Nurse, Queen Margaret Hospital, Dunfermline
Kevin Deans 01224 558565 [email protected] Specialist Registrar, Aberdeen
36

Name ___________________________
Date_____________________________
Practical assessment of procedures
ProceduresDate and Sign
Discuss Observe Practice under supervision
Competent
Preparation of feed and pump
Use of sterile field and non- touch technique
Social and antiseptic handwash
Commencing and disconnecting PN via central catheter
Commencing and disconnecting PN via peripheral catheter or venflon
Changing exit site dressing
Changing closed IV
Commence PN using subcutaneous port
Disconnecting PN using subcutaneous port
Completion of objectives
Signature of Assessor___________________________
Signature of Nurse_________________________
Date_________________
Scottish HPN Managed Clinical Network ProtocolsRevised July 2010 - For revision July 2013
37

Hand wash technique
Scottish HPN Managed Clinical Network ProtocolsRevised July 2010 - For revision July 2013
38
Hand Hygiene Chart
Level of hand hygiene
Choice of agent Frequency (this list is not exhaustive)
Procedure Duration Comments
Routine / Social Liquid soap & water Between patients, before and after tasks that may contaminate hands:- Before preparing,
handling, eating food- After visiting the toilet- When hands are visibly
soiled
Follow Hand Hygiene Technique as per Appendix 4
10-15 seconds after contact with cleansing agent
Ensure hands are wet before applying soap
Alcohol based hand disinfectant
If hands have contact before of after a task, but are not visibly soiled
Follow Alcohol Hand Based Disinfectant Technique as per Appendix 3
20-30 seconds
Ensure hands are dry before commencing next task
Hygienic Liquid soap & water followed by alcohol based hand disinfectant
Follow Hand Hygiene Technique as per Appendix 4 and then Alcohol Hand Based Disinfectant Technique as per Appendix 3
10-15 seconds after contact with cleansing agent
Do not apply alcohol based hand disinfectant with antiseptic hand hygiene agent. Do not use when caring for a patient with an infection caused by a spore-producing organism, e.g. Clostridium Difficile
General Clinical Use: Chlorhexidine gluconate 4% skin cleanser e.g. Hydrex, Hibiscrub
Before aseptic procedures and after performing tasks that may contaminate hands:
- Before undertaking aseptic procedures
- Before leaving standard isolation rooms
- Before and after handling wounds, and
- Wet hands under running water
- Dispense 5mls of handwash solution into cupped hands
- Follow recommended handwash technique
10-15 seconds after contact with cleansing agent
Ensure hands are wet before applying handwash solution.
Residual activity following hand hygiene.
Scottish HPN Managed Clinical Network ProtocolsRevised July 2010 - For revision July 2013
39

IV lines- During outbreaks of
infection- Before undertaking
operative and invasive procedures
- Rinse under running water
- Dry thoroughly with a disposable paper towel
Surgical In Theatre/Neonatal:
Chlor-hexidine gluconate 4% skin cleanser e.g. Hydrex
- Before undertaking operative and invasive procedures
- Wet hands under running water
- Dispense 5 mls of handwash solution into cupped hand
- Rub thoroughly over all surfaces of hands and forearms
- Dispense 5mls antiseptic handwash onto sterile nail brush, and scrub nails
- Rinse hands and forearms
- Dispense 5mls of antiseptic handwash and rub over all surfaces of hands and forearms again
- Rinse hands and forearms
- Dry thoroughly using sterile hand towel
Rub for 1 minute after contact with cleansing agent
Scrub for 1 minute (maximum)
Rub for 2-3 minutes
Repeat full procedure if any contact occurs with non-sterile surface
Do not scrub skin with nail brush
Rinse from tips of finders to elbows
Rinse from tips of fingers to elbows
OR
Povidone-iodine 7.5% (an alternative to chlorhexidine if skin reactions occur)
Scottish HPN Managed Clinical Network ProtocolsRevised July 2010 - For revision July 2013
40

Scottish HPN Managed Clinical Network ProtocolsRevised July 2010 - For revision July 2013
41