Embed Size (px)
Citation preview

Esophageal CancerScott T. Kelley, MD
Board-certified SurgeonSurgical Oncologist
Introduction: One of the goals of Dr. Kelley’s practice is to provide you with the highest quality of care through education, research and service. The following information has been developed to give you a better understanding of esophageal cancer and its treatment. Your doctor or nurse will review this information with you and answer any questions you may have.
Esophageal Cancer: An OverviewAccording to the American Cancer Society, almost 17,000 Americans were diagnosed with esophageal cancer in 2009. The incidence of esophageal cancer has been increasing at an alarming rate, faster than that of any other cancer in the United States- about a 700% rise in the last decades.

3
Esophageal cancer has become the 8th most common cancer worldwide. The reason for this sudden increase is not clear, but it is known that many of these cases start with damage and ulceration in the lower esophagus due to chronic acid reflux, or heartburn.
What is Esophageal Cancer? Esophageal cancer is the abnormal growth of cells in the esophagus, the tube that carries food and liquid from your throat to your stomach.
Esophagus
Stomach

4
There are two types of esophageal cancer:
Adenocarcinona is the more common type of esophageal cancer and starts in the lower portion of the esophagus near the opening to the stomach. It begins when cells in the lining of the esophagus change into abnormal (or glandular) cells. This condition is known as Barrett’s esophagus.
Squamous cell carcinoma is another type of esophageal cancer. This type can occur anywhere in the esophagus.
Risk Factors:No one is certain what causes esophageal cancer, but risk factors include the following:
• Gastroesophageal Reflux Disease (GERD) - This condition occurs when stomach contents leak into the esophagus due to the pressure in the stomach being greater than the esophagus.
Esophagus
Stomach
Gastro Esophageal
Junction (GE)

5
The most common symptom of this condition is heartburn, which usually feels like burning chest pain starting behind the breastbone and moving upward. Cells in the lower esophagus change into the Barrett’s esophagus (especially if one has reflux for ten years or longer).
It is not recommended to treat symptoms of GERD with over the counter medication without first being evaluated by a doctor.
• Barrett’s esophagus - This is a condition in which columnar cells like those in the stomach replace the normal cells lining the esophagus. This process is caused by irritation and damage to the lining of the esophagus by the acid of reflux disease (GERD).
• Tobacco use - Tobacco use, in any form, increase the risk of esophageal cancer. The longer you smoke and the more you smoke each day, the greater the risk. This is primarily true for squamous cell esophageal cancer.
• Alcohol use - Chronic or excessive use of alcohol, especially when combined with tobacco use, increases the risk. Again, this is primarily true for squamous cell esophageal cancer.
• Diet - A diet that is low in fruits, vegetables, and certain vitamins and minerals can increase the risk of this form of cancer. Esophageal cancer risk appears to be reduced by consuming a diet high in fruits and vegetables.
• Age - most people who develop esophageal cancer are over 50.
• Sex - esophageal cancer occurs about three times more often in men than women.
• Race - Caucasians have a higher incidence of adenocarcinomas of the lower esophagus than African-Americans. Squamous cell esophageal cancer is three times more common among African-Americans.
Although there is no sure means of preventing esophageal cancer, avoiding smoking and alcohol is the best way to reduce your risk.

6
Screening:If you have risk factors for esophageal cancer - particularly Barrett’s esophagus - you may benefit from screening tests such as endoscopy with tissue biopsy. When diagnosed early, esophageal cancer can often be successfully treated. Watson Clinic offers screening tests for esophageal cancer.
If you are interested in finding out more about screening for esophageal cancer, you may call Watson Clinic Main at 863-680-7875.
Symptoms:Early esophageal cancer may not cause any symptoms. However, as the cancer progresses, it usually causes one or more of the following symptoms:
• Difficulty swallowing (a condition called dysphagia) is the most common symptom of esophageal cancer. This usually occurs when the cancer has grown large enough to fill about half of the opening of the esophagus. Pain may be present along with the dysphagia.
• Hoarseness or chronic coughing
• Vomiting or regurgitation of food
• Severe weight loss
• Pain in the throat, chest or back
If you experience any of these, you should see your doctor.

7
Diagnosis and StagingIf esophageal cancer is suspected, several tests may be ordered. If cancer is detected, staging is the process that doctors use to determine how advanced the cancer is and whether the cancer has spread.
• Upper Endoscopy (EGD) is usually the first step in evaluation. This is an outpatient test performed under sedation in which a flexible telescope is passed through your mouth and down your esophagus into your stomach. The telescope allows the doctor performing the test to look at the lining of the esophagus and take a small sample of tissue, or biopsy, of any areas that do not look normal. The tissue is examined under a microscope to determine whether there is cancer present.
• Endoscopic Ultrasound (EUS) uses a tiny ultrasound device at the end of a tube that is inserted into the esophagus to create pictures with sound waves. This test is better than the CT scan at determining how far cancer has grown into the wall of the esophagus and surrounding tissue and lymph nodes. This information is especially important in making decisions about the timing and extent of surgery.
• CT scans and PET scan (CT/PET scan) (combination of both images) is performed in the Radiology Department. These tests look for any masses and are especially useful for determining the extent of cancer and its spread to other organs. The results help guide decisions about treatment.
Treatment of Esophageal Cancer:Treatment for esophageal cancer depends on the size and location of the tumor, the individual’s symptoms and general health and whether the cancer has spread to other organs. Many different treatments may be used. Here at the Watson Clinic and the Center for Cancer Care & Research, the multidisciplinary team includes Dr. Kelley a gastroenterologist, a medical oncologist, a radiation oncologist and specialist in swallowing evaluation, physical therapy and clinical nutrition.

8
Surgery - Removing the tumor and affected tissue offers the best chance to cure esophageal cancer. Dr. Kelley removes a large portion of the esophagus and the upper part of the stomach. Additionally, neighboring lymph nodes are removed to prevent the cancer from spreading. The surgeon then uses the remaining portion of the stomach to reconnect the digestive tract, to allow for swallowing. Surgery is recommended as the first line of treatment for early stage cancers.
Neoadjuvant (preoperative) chemotherapy and radiotherapy followed by surgery - For most cancers that have not spread to other areas, chemotherapy (medication given intravenously to kill cancer cells) combined with radiation therapy is given first. This is then followed by surgery approximately six to eight weeks after completion of these treatments.
Chemotherapy and/or radiation therapy alone - this option is for patients whose cancer has spread to organs beyond the esophagus, or in situations where the patient has other medical conditions that rule out surgery.
The following are options to improve symptoms:• A stent (a small mesh tube) is placed into the esophagus to ease
the passage of food or liquid.• A laser and/or a therapy known as photodynamic therapy,
(PDT) is used to reduce the size for a tumor. This can relieve blockage and improve swallowing.
• A feeding tube is inserted into the stomach or intestine for nutritional purposes. This is done by a simple operation or endoscopic procedure.
There are many clinical trials available through the Watson Clinic Center for Research that offer promise for patients. They are used when laboratory research shows that a new method might have some benefit.

9
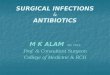
Esophageal Cancer Surgery:Esophagectomy
Surgery is the most common form of treatment for esophageal cancer - when the patient is healthy enough to withstand surgery - and is used alone or in combination with chemotherapy and radiation therapy to cure the cancer. Surgery alone can be curative if the cancer is found early and has not spread beyond the esophagus.
Diseased portion to be removed
Figure 1An esophagectomy is the surgical removal of a large portion of the esophagus

10
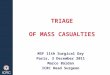
In most cases, the stomach is connected to the remaining part of the esophagus to allow you to eat (figure2).
The surgery takes approximately 4 hours. Additional time may be needed before surgery to put you to sleep and properly position you for the procedure.
Stomach pulled up and reconnectedto esophagus
Figure 2

11
There are several ways to perform an esophagectomy. The decision as to which method to use is complex and bases upon a variety of factors including the location of the tumor, and the overall health of the patient. This will be discussed with you during the consultation.
• Ivor Lewis is a surgical procedure where the esophagus is reached through incisions in the chest and abdomen.
• Transhiatal is a surgical procedure where the esophagus is reached through incisions in the neck and abdomen.
Incision Sites
Ivor-Lewis
Abdominal incision
Transhiatal
Sideincision
Neckincision

12
Incision Sites
Smallabdominal
incisionNeck
incision
Entrysites
The “Dr. Kelley” Minimally invasive esophagectomy
• The “Dr. Kelley” Minimally invasive esophagectomy is a surgical procedure Dr. Kelley pioneered with the assistance of a video camera and several thin instruments. This avoids the traditional large incisions used for these procedures. Benefits of this minimally invasive procedure include less discomfort after surgery, less recovery time, a shorter hospital stay, earlier return to full activities, and smaller scars.
Dr. Kelley is one of only a handful of surgeons in the world who regularly performs this procedure.

13
At the time of esophageal cancer surgery, a temporary feeding tube will be placed into your small intestine during the operation. It serves to feed you in case you are unable to eat by mouth or to add to your diet when you resume eating. This helps keep your body in good condition during the postoperative period. It is usually removed during the first postoperative visit, two weeks after your discharge from the hospital.
Risks and Potential ComplicationsThe removal of the esophagus is an extensive procedure, requiring a significant amount of time under general anesthesia. Every possible precaution will be taken for your safety and
Feeding tube insmall intstine

14
well-being. The major risks of an esophagectomy are leaks from the connection between the esophagus and stomach, pneumonia, infection, bleeding, abnormal heart rhythms, and rarely heart attack and death.
Only those surgeons who are experts in the field and those who have done many of these surgical procedures should perform your esophageal surgery.
HospitalizationYou will be in the hospital between 7 to 10 days. The first night is typically spent in the special care unit (SCU). Most likely, you will be transferred to one of our surgical floors on the first or second day after surgery. Members of the team, including nurses, physical therapists, physician assistants, speech and swallowing experts, nutritionists, social workers and case managers will visit you. A swallowing study will be performed during your hospital stay to check healing at the surgery site. After the study is completed, a nutritionist will meet you to discuss any changes to your usual diet. This will involve more frequent, smaller meals.
Going homeBefore you leave the hospital, your care team will speak with you and your family to decide what you will need when you go home. For example, you may need a nurse to come to your home once or twice a week to assist with tube feedings, to examine your incision sites and/or to check on how you are recovering.
Even though you leave the hospital, our team is always available to guide you through the 6-8 week recovery period after surgery. You will be given a prescription for pain medication for any discomfort you may have at your incision sites and any other medications you may need. You will also be given phone numbers to call if you have questions.

15
If you experience any of the following, please call your doctor or nurse:
• Fever over 100.5• Chills • Pain not eased by pain medicine• Drainage, redness or increasing pain at any of the incision sites• Difficulty breathing or swallowing• Problems with the feeding tube (such as not being able to
flush it)• Difficulty increasing activity level• Difficulty eating or drinking by mouth• Any symptom not usual for you• Any change in how you feel
The hospital will call Dr. Kelley’s office to schedule an appointment to see him two weeks after discharge from the hospital. Any further appointments will depend upon how you are feeling and the results of your final pathology report. Dr. Kelley will discuss this with you at your first postoperative visit.
Do not hesitate to call Dr. Kelley’s office for guidance at any time.
Phone: 863-680-7875

16
For more information:National Cancer Institute (NCI)Toll-Free 800-422-6237TTY 800-332-8615E-Mail [email protected] www.nci.nih.gov
American Cancer Society (ACS)Local Office: 809 South Florida Ave., Lakeland, FL 33801Phone: 863-688-2326Toll-Free 800-227-2345www.cancer.orgCancer Research InstituteToll-Free 800-992-2623E-Mail [email protected] www.cancerrecarch.org
NOTES____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Written by Scott T. Kelley, MD edited & produced by Watson Clinic Marketing Communications Department

1600 Lakeland Hills Boulevard Lakeland, FL 33805
863-680-7875www.WatsonClinic.com
Scott T. Kelley, MD is part of the surgical oncology and general surgery team at Watson Clinic. He is an expert in the treatment of esophageal cancer and is one of only a handful of surgeons in the world who performs minimally invasive esophageal resection – having pioneered the “Kelley
Minimally Invasive Esophagectomy.” In addition, he performs complex gastrointestinal surgery of all kinds, including pancreatic, stomach, colon/rectal and sarcoma surgery.
Dr. Kelley received his medical degree from Columbia University, College of Physicians & Surgeons, in New York. He performed his internship and residency in General Surgery at the Hospital of the University of Pennsylvania in Philadelphia, where he also completed research fellowships in Cardiothoracic Surgery and Surgical Oncology. Dr. Kelley then completed an additional surgical oncology fellowship at H. Lee Moffitt Cancer Center & Research Institute.
Prior to joining Watson Clinic in 2008, Dr. Kelley practiced at Moffitt Cancer Center, where he served as the Section Head for Esophageal & Gastric Oncology and Associate Professor of Oncology & Surgery. He is board-certified in general surgery.