Embed Size (px)
Citation preview

Scleroderma and
the Kidney
David ShureJuly 14, 2009

DD: Renal Failure
• ATN• Renal Scleroderma Crisis

Epidemiology
• Prevalence: 19-75 cases per 100,000• Susceptibility– Age: peak occurrence 35-65– F:M 7-12:1– Environmental Factors: infection– Occupational exposure: silica dust– Usually occurs w/in 4-5 yrs of SSc onset

Local vs Systemic Disease

Classification
– dcSSC: diffuse cutaneous SSc– lcSSc: limited cutaneous SSC– SSc sine scleroderma – internal organ involvement– Environmentally induced scleroderma– Overlap syndrome: ie MCTD

• Calcinosis cutis• Raynaud Phenomenon• Esophageal dysmotility• Sclerodactyly• Telangiectasia

Pathogenesis• Complex and poorly
understood• Immune activation• Inflammatory response• Vascular damage• Excessive synthesis EC matrix
and collagen deposition• Hypothesis: interplay between
early immunological events and vascular changes leading to generation of a pop of activated fibrogenic fibroblasts believed to be effector cells in disease

Vascular and Endothelial Changes• Appear to precede other features of SSc• Vasoconstriction
– ET-1: significantly elevated in SSc and assoc with pulm htn, may initiate fibrosis
– Superoxide anions: released from endothelium neutralize NO– Defective vasculogenesis: fewer circulating endothelial ell
precursors ie CD34+, CD133+ and VEGF type 2– Pts with SSc have incr in endothelial cell surface expression
of adhesion molecules and elevation in circulating levels of their soluble forms. Cytokine induced upregulation of adhesion molecules ie ICAM-1, VCAM-1, ELAM-1

Autoantibodies
• 75% pts with SSc have circulating autoantibodies– Topoisomerase I (anti-scl 70)• anti-topoisomerase antibodies highly specific for SSc,
and correlate with greater risk for ILD and more extensive skin involvement
– Centromere antigens (12-44%)• Anticentromere antibodies assoc with limited
cutaneous involvement

Fibrosis• Fibrosis gradually replaces vascular
inflammatory phase and ultimately disrupts architecture of affected tissue
1.TGF-b2.CTGF3.PDGF

TGF b• Main Cell Source: macrophages, fibroblasts, T/B
cells, platelets, endothelial cells• Pathogenic relevance:– Induces proliferation fibroblasts and production CTGF
and endothirlin-1– Stimulates synthesis collagen, fibronectin– Inhibits EC matrix degradation by reduced synthesis of
MMP and induction of TIMP-1• Effect in SCL– Increased levels in skin– Elevated expression/ phosphorylation of smad2,3
effectors of TGF b signaling pathway

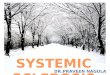
Blobe G et al. N Engl J Med 2000;342:1350-1358
Mechanism of Signal Transduction Mediated by Transforming Growth Factor {beta} (TGF-{beta})

CTGF
• Cell source: fibroblasts, endothelial cells, smooth muscle cells
• Pathogenic relevance: – induced by TGFb, IL-4, and VEGF– Induces proliferation and chemotaxis of
fibroblasts and stimulates production of EC matrix• Effect in SCL– Elevated levels in serum– Incr gene expression in skin and in fibroblasts

PDGF
• Cell source: platelets, macrophages, endothelial cells, fibroblasts
• Pathogenic Relevance: – Mitogen and chemoattractant for fibroblasts– Induces syntehsis of collagen, fibronectin,
proteoglycans, – Stimulates secretion of TGF b type I, MCP-1, IL-6
• Effect in SCL– Elevated expression PDGN in skin– Incr levels in BAL


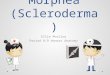
Tan F. N Engl J Med 2006;354:2709-2711
Selective Up-Regulation of PDGFR by Fibroblasts in Scleroderma

SRC: Diagnosis
• New/abrupt onset BP >150/85• Progressive/sudden rise in creat• Additional findings– MAHA and thrombocytopenia– Acute retinal changes of malignant HTN– New onset proteinuria/ hematuria– Urine sediment is bland with limited but incr protein– MAHA/TMA– Characteristic changes on renal bx

Renal BiopsySubintimal Fibrin Deposition – Interlobular artery Muscular Renal Artery –
Onion Skin thickening with complete obliteration of vascular lumen

Fibrin Deposition

Prevention/Treatment• Prevention: avoidance glucocorticoids• If left untreated, SRC can progress to ESRD over 1-2
months and death usually within 1 yr• Treatment: – Mainstay prompt control HTN, return to baseline bp in 72
hrs– Optimal anti-HTN is ACE-I ie captopril – Captopril? Advantage = rapid onset and short DOA
allowing for more frequent titration– Also follow: plt count, LDH, Hb, haptoglobin, LDH for
resolution of intravascular hemolysis– Indefinite continuation of ACE for bp control

ACE Inhibitors
–Retrospective & case-control studies show no efficacy in prevention of SRC –Prospective cohort study- treated vs.
untreated: treated w/↑ recovery of renal fxn & ↑ survival at 1 yr (76% vs 15%)

Long-term Outcomes of Scleroderma Reanl Crisis
• Steen V, et al, Annals of Int Med, 2000– Prospective observational cohort w5-10 yr f/u– 145 pts with SRC who received continuous ACE-I, and
662 pts with SCL who did not have renal crisis– Results:
• At time of renal crisis, 75% pts had SCL sxs for <4 yrs• 61 % pts with SRC had good outcomes (55 received no HD,
34 received temp HD). Only 4% of later group progressed to ESRD
• >1/2 of pts who began HD could dc it 3 to 18 mths later• Survival of pts in good outcome group was similar to pts
with diffuse SCL without renal crisis


Autologous non-myeloablative hematopoietic stem cell transplantation in pts with systemic sclerosis
• Burt RK, et al 2007 Bone Marrow Transplantation– Phase I non-myeloablative autologous HSCT– 10 pts with SSc and poor prognostic features– PBCS mobilized with CY and G-CSF– PBSC graft re-infused after tx with non-myeloablative
conditioning regimen– statistically significant improvement of modified Rodnan skin
score, however cardiac, pulmonary function, and creat remained unchanged
– F/U: 25 mths, overall and progression free survival rates are 90 and 70%
– Concl: Autologous HSCT with non-myeloablative conditioning regimen may lead to improved skin flexibility similar to a myeloablative TBI , but without the toxicity and risks