Embed Size (px)
Citation preview

50
SCIATICABy LESLIE C. OLIVER, F.R.C.S.
Neurosurgeon, West End Hospital for Nervous Diseases, and Royal Northern Hospital, London; Southend GeneralHospital; and Surgeon in Charge of Neurosurgical Centre, Oldchurch Hospital, Romford
A notable advance in surgery was made whenMixter and Barr (I934) showed that sciatica isfrequently caused by backward protrusion of thenucleus pulposus of the fourth or fifth lumbarintervertebral discs. Since then many patientswith sciatica have becn referred to orthopaedic andneurological surgeons; this account is based on thecase records of a neurosurgical centre.
Protrudetd lumbar disc is encountered in all theadult decades, and is the commonest cause of painin the distribution of the sciatic nerve. The onsetmay be precipitated by trauma, often of a trivialnature, or it may occur spontaneously. Pain in thelumbar region usually, but not invariably, pre-cedes or accompanies the pain in the lower limb.The pain radiates down the back of the thigh to theback or outer side of the calf and frequently intothe ankle and outer side of the foot. It is madeworse by flexion of the back and the patient oftensuffers less when sitting upright on a hard chairthan when sitting in an easy chair. The pain isaggravated by coughing and sneezing. Re-missions may occur lasting months or even years;in some cases the pain subsides completely andnever returns. Patients seldom complain ofmuscular weakness or sphincter disturbances,although very occasionally a complete caudaequina lesion is caused by a disc protrusion.
Examination often shows flattening of thenormal lumbar lordosis. Scoliosis is common butthe concavity may be directed towards or awayfrom the side of the protrusion. Forward flexionof the spine is limited but lateral flexion is normal.Firm pressure in the back over the site of the pro-trusion will in many cases cause severe pain toshoot down the leg. This is a most valuable signfor it both establishes the diagnosis and localiza-tion of the protrusion. The lumbo-sacral disc ismore often involved than the disc between thefourth and fifth lumbar vertebrae; higher lumbardiscs are rarely affected. Passive flexion of the hipwith the knee extended is painful and limited,especially on the affected side. There is usuallysome weakness offlexion of the knee, and frequentlyalso of plantar flexion of the ankle. The ankle jerkmay be absent, diminished or unaffected. There isloss of tone of the hamstring and calf muscles.
The gluteal fold may lack definition owing todiminished tone of the underlying muscles.Objective sensory changes are slight and neverabsolute; the most to be expected is hypalgesia ofthe outer aspect of the calf and the lateral borderor dorsal &,urface of the foot.
Radiographs of the lumbar spine and sacro-iliac joints are always taken to exclude other moreserious causes of sciatic pain; in the majority ofcases of disc protrusion there is no radiologicalabnormality. The normal disc space between thefifth lumbar vertebra and the sacrum is different inshape and depth from those above, and is fre-quently reported as diminished when it is normal.However, sometimes with disc protrusions there is' lipping 'of contiguous vertebrae, associated withmarked diminution of the disc space. Lumbarpuncture may show a slight increase in the proteincontent of the cerebrospinal fluid. When thediagnosis is uncertain myelography may be em-ployed, although a negative result does not excludea disc protrusion. Myodil (3 ml.) is injected bylumbar puncture and the patient is examined underthe fluorescent screen on a tilting table. Myodil issaid to be less irritating than lipiodol, but neverthe-less it should only be used if operation is beingseriously considered; at operation the contrastmedium should be removed.A lumbar disc protrusion may be diagnosed
with the utmost confidence if the following syn-drome is found:-(a) Severe pain in the lumbarregion radiating to the calf or beyond. (b) Grosslyrestricted and painful straight leg raising. (c)Paresis of flexion of the knee and sometimesplantar flexion of the ankle. (d) An absent ordiminished ankle jerk; this is an excellent positivesign but frequently the ankle jerk is unaffected bya protruded disc.
If patients with fewer objective signs are sub-mitted to operation a disc protrusion may not befound. On the other hand, if marked paresis,extensive sensory loss and a disturbance of thesphincters are present, one of the more seriouscauses of sciatic pain should be suspected.
Treatment. Whenever possible the effect ofconservative treatment should be tried; the
copyright. on M
arch 11, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.304.50 on 1 F
ebruary 1951. Dow
nloaded from
February I 951 OLIVER: Sciatica
s-
i~~~...s'-! s
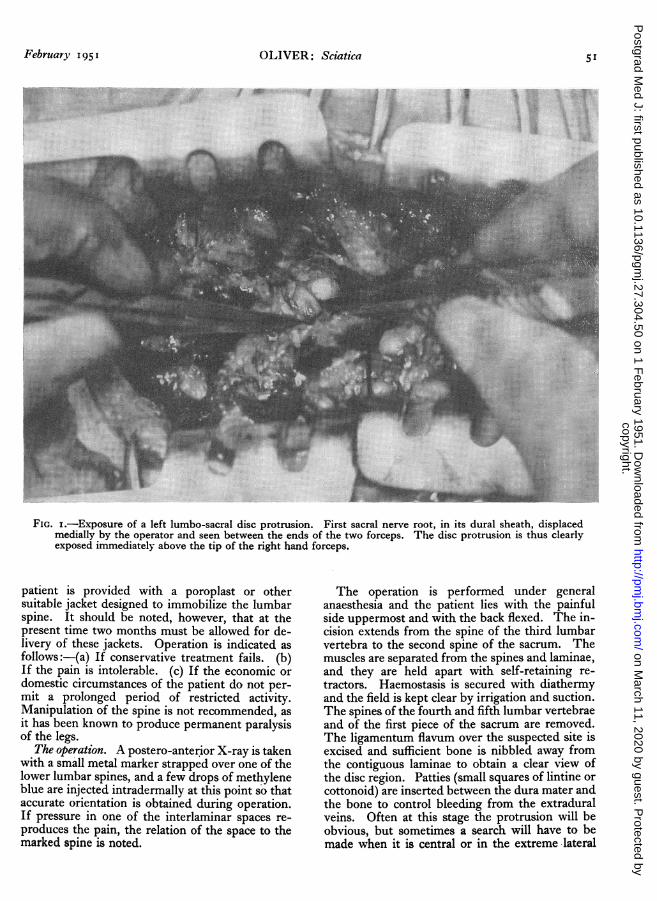
FIG. i.-Exposure of a left lumbo-sacral disc protrusion. First sacral nerve root, in its dural sheath, displacedmedially by the operator and seen between the ends of the two forceps. The disc protrusion is thus clearlyexposed immediately above the tip of the right hand forceps.
patient is provided with a poroplast or othersuitable jacket designed to immobilize the lumbarspine. It should be noted, however, that at thepresent time two months must be allowed for de-livery of these jackets. Operation is indicated asfollows:-(a) If conservative treatment fails. (b)If the pain is intolerable. (c) If the economic ordomestic circumstances of the patient do not per-mit a prolonged period of restricted activity.Manipulation of the spine is not recommended, asit has been known to produce permanent paralysisof the legs.
The operation. A postero-anterior X-ray is takenwith a small metal marker strapped over one of thelower lumbar spines, and a few drops of methyleneblue are injected intradermally at this point so thataccurate orientation is obtained during operation.If pressure in one of the interlaminar spaces re-produces the pain, the relation of the space to themarked spine is noted.
The operation is performed under generalanaesthesia and the patient lies with the painfulside uppermost and with the back flexed. The in-cision extends from the spine of the third lumbarvertebra to the second spine of the sacrum. Themuscles are separated from the spines and laminae,and they are held apart with self-retaining re-tractors. Haemostasis is secured with diathermyand the field is kept clear by irrigation and suction.The spines of the fourth and fifth lumbar vertebraeand of the first piece of the sacrum are removed.The ligamentum flavum over the suspected site isexcised and sufficient bone is nibbled away fromthe contiguous laminae to obtain a clear view ofthe disc region. Patties (small squares of lintine orcottonoid) are inserted between the dura mater andthe bone to control bleeding from the extraduralveins. Often at this stage the protrusion will beobvious, but sometimes a search will have to bemade when it is central or in the extreme lateral
copyright. on M
arch 11, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.304.50 on 1 F
ebruary 1951. Dow
nloaded from

52 POSTGRADUATE MEDICAL JOURNAI, February 1951
FIG. 2.-Spondylolisthesis-marked displacement for-ward of the fifth lumbar vertebra in relation to thefirst piece of the sacrum.
position. The nerve root, in its dural sheath, liesstretched over the protrusion, and great care mustbe taken to see that the nerve is completely re-tracted before the dome of the disc is incised (Fig.i). When exposed in this way the protrusion hasa glistening yellowish-white appearance. It is in-cised with the cutting edge of the knife directedaway from the nerve root, and at once the discmaterial will begin to extrude itself. The bestinstrument for extracting the disc is a smallpituitary rongeur which can be inserted betweenthe vertebrae. Sometimes the disc tissue will bepulled out as a large mass, while at other times it isremoved piecemeal. It is important that a verythorough removal should be carried out if re-currence is to be avoided. If, after careful search,a protrusion is not found in the lumbo-sacralspace, the space above is investigated. The duramater will sometimes have to be opened for theremoval of a midline protrusion or for explorationwhen no protrusion has been found and an intra-dural tumour is therefore suspected.
In a small proportion of cases a protrusion willnot be found but instead the dural sheath of thenerve is firmly bound to the posterior longitudinalligament by strong adhesions. This lesion may befound in patients giving a long history of sciatica
without remissions. There is a good prospect ofrelief from pain if the nerve sheath is liberated.The adhesions may be so tough that they have tobe divided with a knife. This condition isprobably the aftermath of a protrusion.
Other Causes of SciaticaIn comparison with lumbar disc protrusion the
conditions listed below are rare causes of sciatica,but they make a thorough investigation of eachcase a necessity.
i. Lesions of the Sacro-Iliac JointSubluxation and dislocation are rare injuries
which may give rise to a typical sciatica syndrome.Arthritis. Pain in the sacral region together with
pain radiating down one or both legs may occurin Marie's spondylitis ankylopoietica and in Paget'sosteitis deformans. In the former disease thesacra-iliac joint is frequently the first to be in-volved and X-rays show increased density of bonein the region of the joint, which has almost lost itsdefinition. In the latter disease the X-ray ap-pearances of the joint are similar, but the bonesof the pelvis show the signs of Paget's disease.
Tuberculosis of the sacro-iliac joint is a rare causeof sciatic pain. The objective signs are likely tobe more advanced than those found with a discprotrusion. Radiography shows irregular rarefac-tion of the bone and eventually destruction of thejoint.
Metastatic carcinoma may be found in the bonein the neighbourhood of the sacro-iliac joint,giving rise to sciatica. The primary growth isusually in one of the pelvic viscera, especially theprostate. The pain is likely to be severe and torequire spinothalamic tractotomy for its relief.
Chordoma is a very rare tumour but when itoccurs in the sacrum it produces pain and paralysisin the distribution of the sacral plexus. Thetumour can be palpated through the rectum; it isof rubbery consistency and is fixed to the sacrum.X-ray shows destruction of the sacrum withoutbone reaction. The tumour is inoperable both onanatomical and pathological grounds. Pain may berelieved by spinothalamic tractotomy.
2. Lesions of the Lumbar VertebraeSpondylolisthesis. In this condition the fifth
lumbar vertebra, together with the spinal columnabove it, is displaced forward in relation to thesacrum (Fig. 2). It is caused by a bilateral con-genital or traumatic cleavage between the upperand lower articular facets of the fifth lumbarvertebra; the upper facets together with thevertebral body remain articulated with the vertebraabove, and the lower facets, laminae and spinewith the first piece of the sacrum below. There
copyright. on M
arch 11, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.304.50 on 1 F
ebruary 1951. Dow
nloaded from

February 1951 OLIVER: Sciatica 53
is evidence that the sciatic pain which is some-times associated with spondylolisthesis is causedby a disc protrusion (Meyerding, 1941), thoughnot necessarily of the lumbo-sacral disc. Theeffect of conservative treatment should be triedfirst. If this does not succeed exploration for adisc protrusion should be undertaken. Fusion ofthe lower lumbar vertebrae and the sacrum mayalso be necessary.
Metastatic carcinoma is especially likely to arisefrom a primary tumour of the prostate. Radio-graphy then shows increased density of the affectedbones.
3. Intrapelvic DiseaseLocal infiltration of the sacral plexus may arise
from carcinoma of the rectum or cervix and causesciatic pain. Spinothalamic tractotomy should beperformed.
4. Cauda Equina TumoursThe following tumours may be found in the
cauda equina:-Ependymoma of the filum ter-minale or conus; neurofibroma; meningioma;cholesteatoma (epidermoid); dermoid; angioma;and extradural cyst. A cauda equina tumour mayin the first place produce a syndrome indistinguish-able from that of a lumbar disc, but later 'saddle 'analgesia and retention of urine will be found.Large tumours of the cauda equina become in-separably attached to the many nerve roots in thissituation and tend to produce irreversible paralysis,sensory loss and sphincter disturbance; an intra-capsular removal is all that is possible if furtherdamage to the cauda equina is to be avoided. It istherefore important to keep in mind the possibilityof an early cauda equina tumour when sciatic painis being investigated, or when exploration for adisc protrusion has proved negative (Fig. 3). Indisc protrusions an increase in protein in thecerebrospinal fluid up to approximately ioo mg.per ioo ml. may be found; increases above thislevel and an obviously positive Queckenstedt testshould lead to the suspicion of a tumour of thecauda equina.
5. Sciatica of Unknown OriginIt is easy to understand that an inexperienced
surgeon may fail to find a disc at operation, es-pecially when diathermy haemostasis is not em-ployed. However, most neurosurgeons will admitto some completely negative explorations when noconvincing lesion of any kind is found, even after
FIG. 3.-Cisternal injection of 3 ml. myodil held up bya meningioma of the cauda equina. Operationpreviously performed for an unconvincing discprotrusion in a patient with a typical syndrome.Recurrence, with onset of constipation, led to re-investigation.
an extensive intradural search. There may be aneven higher percentage of these cases in the groupthat is not considered suitable for operation. Thecause of the sciatica in these patients is at presentunknown.
6. Sciatica and PregnancySciatica occurring in pregnancy was formerly
thought to be due to pressure on the lumbo-sacralplexus by the foetal head, but it is now believed tobe caused in most cases by a disc protrusion pre-cipitated by the softening of the ligaments duringpregnancy.
BIBLIOGRAPHYMIXTER, W. J., and BARR, J. S. (1934), New England Y. Med.,
211, 210.MEYERDING, H. W. (I94I), Journal Bone and Joint Surg., 23, 461.
copyright. on M
arch 11, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.304.50 on 1 F
ebruary 1951. Dow
nloaded from





























