Embed Size (px)
Citation preview

International Journal of Play Therapy, 14(1), pp. 51-79 Copyright 2005, APT, Inc.
SCHOOL-BASED CHILD-CENTERED PLAYTHERAPY WITH HISPANIC CHILDREN:
OUTCOMES AND CULTURALCONSIDERATIONS
Yvonne GarzaSam Houston State University
Sue C. BrattonUniversity of North Texas
Abstract: Hispanic children are the fastest growing segment of thepopulation. Numerous factors place them at-risk for school success. This studyexamined the effects of Child-Centered Play Therapy (CCPT) compared to acurriculum-based small group intervention with 29 Hispanic children referredfor school counseling due to behavior problems. Children were assigned totreatment groups by random drawing within grade levels. Treatment wasprovided by Hispanic bilingual counselors. Statistical analysis revealed that,according to parent report, children receiving CCPT showed statisticallysignificant decreases in externalizing behavior problems, compared to thecurriculum-based treatment group. Effect size calculations revealed that CCPTdemonstrated a large treatment effect on externalizing behavior problems and amoderate treatment effect on internalizing behavior problems. Culturalconsiderations and recommendations for practice and future research arediscussed.
Grant funding for this research project was in part from the Texas Higher EducationCoordinating Board, University of North Texas Faculty Research Grant and the Associationfor Play Therapy. Yvonne Garza, Ph.D., is an Assistant Professor at Sam Houston StateUniversity and can be reached at the Educational Leadership & Counseling Department,P.O. Box 2119, Huntsville, TX 77341-2119, or by email at: [email protected]. SueC. Bratton, Ph.D., is an Associate Professor in the Counseling Program at the University ofNorth Texas and is the Director for the Center of Play Therapy.

52 Garza & Bratton
Advocates for cultural competency have fervently urged mentalhealth professionals to identify issues in cultural diversity and researchthe effectiveness of treatment modalities across cultures (Baruth &Manning, 1992; Cochran, 1996; Santiago-Rivera, 1995). Regardless of thiscogent push, there remains a dearth of information in the area oftreatment of culturally diverse populations, particularly related tochildren. Hispanics are the largest and fastest-growing minority group inthe United States (U.S. Bureau of Census, 2000). Currently, Hispanicchildren represent 35% of the population in U.S. public schools, and thisnumber is expected to grow (U.S. Bureau of Census, 2000). Numerousfactors place these children at-risk for school success. The NationalCenter for Education Statistics (NCES, 2003) cited poverty and Englishspoken as a second language as risk factors for school dropout. ManyHispanic children fall in both categories. In fact, the National Center forEducational Statistics (2003) reported that Hispanic students had thehighest dropout rates in the United States, four times the rate of theirnon-Hispanic white peers (Collins & Ribeiro, 2004). Furthermore,statistics show that in addition to academic difficulties, Hispanicdropouts struggle with a myriad of personal and social problems,including delinquency, teen pregnancy, substance abuse, and criminalbehavior (DCCY, 2000).These statistics bring a sense of urgency toidentifying culturally responsive interventions to address psycho-socialand behavioral problems that place Hispanic children at-risk (Cochran,1996; Santiago-Rivera, 1995). This dilemma is further complicated by acritical shortage of appropriate mental health services for all children.Indeed, the most recent U.S. Surgeon General's report, "A NationalAction Agenda for Children's Mental Health," described this shortage asa "national health crisis" (U.S. Public Health Service, 2000, p.3). Thereport further targeted the needs of children from minority populations,calling for proven early interventions and more accessible services.

School-Based Child-Centered Play Therapy 53
Rationale for culturally responsive, school-based mental healthservices
The literature suggests that Hispanic families are not likely toutilize community mental health clinics, resulting in significant unmetpsycho-social needs for these children (Foulks, 2004). Authorities haveemphasized the need to provide mental health services in schools whereminority children are afforded equal access at the earliest sign of need(U.S. Public Health Service, 2000). However, answering the call forculturally responsive school-based mental health services for Hispanicchildren is challenging and complicated. D'Andrea and Bradley (1995)emphasized that with the rapid growth in the Hispanic population,schools are limited by the few resources available to help these childrenrealize their academic and personal potential. School counselors, alreadyoverburdened with referrals, are increasingly faced with treating apopulation with unique cultural and language needs. Hispanic childrenare often misdiagnosed and underserved due to a variety of factors,including a lack of culturally competent professionals and a lack ofculturally responsive resources. Most notable is a significant shortage ofSpanish-speaking counselors trained specifically to provide culturallyresponsive interventions to young Hispanic children. Advocates forcultural competency emphasize that therapists need to adopt a"culturally responsive" rather than a "culturally sensitive" stance withclients; meaning the therapist responds actively to the client's uniquecultural needs (Durodoye, 2002; Koss-Chioino & Vargas, 1992). Whileschool counselors and other mental health professionals are oftenrequired to attend workshops on cultural diversity in an attempt tounderstand the barriers that affect treatment, what is most needed isfurther study that adapts knowledge and explores effectiveness(Cochran, 1996).
Rationale for child-centered play therapy with Hispanic childrenPlay therapy is a research-supported intervention that is
responsive to the unique and varied developmental needs of children.Landreth (2002) indicated that play is the "native language" of children,

54 Garza & Bratton
an innate and universal method of communication through which theycan express and work through their difficulties. This modality hasgained widespread acceptance and use among practitioners incommunity settings, and to a lesser degree in school settings, as a viabletreatment intervention for a variety of social, emotional, behavioral, anddevelopmental issues (Bratton & Ray 2000). A recent meta-analysis ofover five decades of play therapy outcome studies (N = 93) revealed alarge treatment effect (ES = .80) and concluded that play therapy was aneffective treatment when compared primarily to no treatment controlgroups (Bratton, Ray, Rhine & Jones, in press). The authors specificallynoted a lack of ethnic diversity in populations studied and called forincreased research on play therapy with culturally diverse children. Areview of the literature revealed only two controlled studiesinvestigating play therapy's effects with Hispanic children (Constantino,Malgady, & Rogler, 1986; Trostle, 1988).
Current research on cultural or theoretical considerations incounseling Hispanic children is scarce and provides little guidance to thepractitioner. Advocating for culturally responsive counseling, Koss-Chioino and Vargas (1992) emphasized the importance of therapistempathy and congruence. Cochran (1996) suggested that person-centered therapies are the treatment of choice for treating culturallydiverse populations of students. Del Castillo and Torres (1988)emphasized that Hispanics value the concept of "being," which is morepresent-focused and spontaneous, rather than on the "doing" value ofEuropean Americans, which is more goal-oriented and focused onachievement. Other advocates for the use of person-centered principleswith Hispanics have suggested that Hispanics tend to preferinterpersonal relationships that are nurturing, loving, intimate, andrespectful (Altarriba & Bauer, 1998; Constantine, 2001). Ramirez (1999)described these characteristics as the Hispanic value of "personalismo,"and argued that Child-Centered Play Therapy (CCPT) was, therefore, agood fit for this population. In CCPT, built on the approaches of Rogers(1951) and Axline (1969), the child is free to direct the course of therapy;the therapist does not impose values, past experiences, or pre-conceived
School-Based Child-Centered Play Therapy 55
ideas on the child (Landreth, 2002). In this approach, each child isviewed as unique and worthy of respect. The basic tenets of CCPT seemto be congruent with suggestions regarding cultural needs of Hispanicsand what constitutes culturally responsive counseling; however, thereader is cautioned to avoid over-generalizing culturally specificinformation, but rather apply knowledge with caution.
Rationale for cultural responsiveness in play therapyIrwin (1983) suggested that cultural influences are often fused into
the expression of pretend play by children. In fact, studies in evolutionhave demonstrated that children integrate cultural information throughimitation done in ritualistic play. Developmental theories suggest thatcultural values, traditions, roles, and ethnic identity are expressed andpracticed through play (Vygotsky, 2002; Vandenberg & Kielhofner,1982). Leading advocates of play therapy espouse the notion that toysare the words through which young children can express themselvesmost meaningfully (Axline, 1969; Landreth, 2002; Kottman, 2001;Moustakas, 1973). Therefore, it is plausible that, for Hispanic children,the use of culturally responsive toys and materials would encouragethem to express themselves more comfortably and freely, while toys thatreflect primarily Western values might convey a value of conforming tothe dominant culture, thus inhibiting certain expressions (Hinman,2003). Martinez and Valdez (1992) and Santiago-Rivera (1995)emphasized the importance of cultural responsiveness in theclient/therapist relationship, suggesting that a therapeutic environmentthat has been modified in an attempt to express an understanding of aclient's culture, demonstrates to the client the counselor's openness tothe client's world. Santiago-Rivera (1995) further stated that clientsshould be allowed to express their customs, values, and beliefs in theirpreferred language, when possible.
A review of the literature found little reference to what constitutesculturally responsive play therapy or suggestions for culturally specifictoys and materials. The prevailing attitude in the literature seems toreflect that children use toys to "communicate their world to the
56 Garza & Bratton
counselor" (Landreth, 2002); yet, there is little to no mention of specificcultural considerations in selection of toys for children from diversepopulations. Glover (1998) addressed the need for culturalresponsiveness in play therapy, urging therapists to gain anunderstanding of a particular ethnic group or culture in order to moreappropriately choose culturally specific toys for their familiarity andprevalence to the child. A synthesis of the literature suggests thatadapting the play therapy environment to include culturally specific toysand materials would constitute a more culturally responsive approach tothe delivery of play therapy services to Hispanic children.
METHOD
A pre-test post-test comparison group design was used todetermine the effects of Child-Centered Play Therapy (CCPT) on school-age Hispanic children experiencing behavioral problems that place themat risk for academic failure, compared to curriculum-based small groupcounseling.
ParticipantsThe study was conducted in a school district in the Southwest
United States with a population consisting of approximately 35%Hispanic students. Participants (n = 30) were selected from Hispanic,Spanish speaking kindergarten through fifth grade students ranging inage from 5 to 11 years who were referred to school counseling servicesby their parents and teachers due to internalizing or externalizingbehavior problems. Children who scored in the At-Risk or ClinicallySignificant range on the Behavior Assessment Scale for Children (BASC)were included in the study (Reynolds and Kamphaus, 1992). Participantswere assigned to the CCPT treatment (n = 15) or curriculum-based smallgroup counseling (n = 15) by a random drawing within grade levels.Neither parents nor teachers were advised of a child's treatment groupassignment until after the completion of the study. One student in thecomparison treatment group moved during the course of treatment, thus

School-Based Child-Centered Play Therapy 57
29 participants completed the study. Random drawing produced groupsthat were almost identical with respect to gender. The CCPT groupconsisted of 9 males and 6 females, while the comparison groupconsisted of 8 males and 6 females. The study's ratio of males to femalesis slightly more balanced than the 2/3 male to 1/3 female that has beentypical in most child psychotherapy research (Bratton et alv in press).
Of interesting note, although school officials identified allsubjects as "Hispanic," on child demographic sheets, parents were moreexplicit during parent interviews and clearly identified their child asHispanic if born in the United States and Mexican if born in Mexico. All30 parents who completed the paperwork indicated that they were bornin Mexico, thus identified themselves as Mexican. Of the children, 16were identified by their parents as Hispanic and 13 children wereidentified as Mexican. This may indicate that parents of children in thestudy are fairly traditional to the Mexican culture and that informationgathered from this population may be unique to a more indigenouspopulation of Hispanics. Since the majority of children were identified asHispanic, for the purpose of this study, "Hispanic" is used throughout torefer to all subjects.
TreatmentTo accommodate to the school schedule, children in both
treatment groups received a 30-minute intervention, once per week for15 weeks (both treatments typically call for 45-minute interventions).Both treatment providers were bilingual Hispanic counselors with post-masters training and experience in person-centered counseling. Thecounselor for the play therapy treatment group had completed advancedtraining and supervision in the theory and application of CCPT. Thecounselor for the curriculum-based small group counseling was certifiedto teach the chosen curriculum and had received advanced training andsupervision in person-centered group counseling. Both counselorsintroduced their respective intervention in both Spanish and English,informing children that they could choose to speak either Spanish orEnglish or both during sessions. Additionally, throughout treatment,

58 Garza & Bratton
counselors responded in-kind to the children's spontaneous use oflanguage; that is, when the child spoke English the therapist respondedin English; and when the child spoke Spanish the therapist responded inSpanish. To ensure treatment integrity, all sessions were videotaped andrandomly viewed for adherence to treatment protocol. Particularattention was given to the selection of therapists and treatments to bestadhere to a culturally responsive approach as encouraged by theliterature.
Experimental treatment. The 15 experimental treatment groupchildren received 30 minutes of Child-Centered Play Therapy (CCPT)once per week for 15 weeks, following the basic principles andmethodology of CCPT proposed by Landreth (2002). Play therapysessions were held in specially-equipped playrooms in a confidentialschool setting. Playrooms were equipped with a variety of specific toysto facilitate a broad range of expression, following Landreth's (2002)general guidelines. However, based on the urging of advocates for moreculturally responsive treatments, the researchers adapted Landreth's listto accommodate to the needs and experiences of the Hispanic culture.Selection of multicultural toys was decided by a panel of five Hispanic,Spanish-speaking, registered play therapists who conduct CCPT withHispanic children in the Southwest United States. All five panelistsagreed that the use of multicultural toys would provide a moreculturally responsive playroom. They based their selection of toys onwhat they believed would appropriately capture elements of Hispanicculture specific to the families involved in this study (Table 1).Interestingly, none of the panel members had made any significantadaptations to their own playrooms; instead they all adhered to a more"one-size-fits-all" approach, equipping their playrooms asrecommended by Landreth (2002).
Initially, the children were introduced to the playroom by thetherapist (in both Spanish and English): "This is our special playroomand in here you can say and do many things that you would like, andyou also can decide to speak English, Spanish, or both." "Este es el cuartoespecial de jugar y aqui puedes acer y decir muchas cosas que te gustan, aqui

School-Based Child-Centered Play Therapy 59
puedes escojer hablar Ingles, Espanol, o los dos." As stated earlier, the playtherapist's responses matched the language used by the child. A CCPTtreatment protocol was strictly adhered to and included the principlesand methods of (a) creating a safe, accepting, and permissiveenvironment, (b) facilitating the child's internal locus of control andevaluation through encouraging self-directed play, (c) following thechild's lead, (d) accurately reflecting thoughts, feelings and behaviors soas to convey empathy and genuineness, as well as to facilitateunderstanding, (e) enhancing the child's self-esteem, creativity, andsense of competence, (f) facilitating self-directed decision making andproblem-solving, and (g) setting therapeutic limits as needed to ensurethe emotional and physical safety of the child and therapist. In thisapproach, the relationship between the therapist and child is viewed asthe catalyst for change, with all authentic change originating within thechild. Therefore, the therapist consistently responded in ways thatconveyed a deep respect for and trust in the child's capacity for growthand change. (For more specific information on the CCPT protocolfollowed in this study, contact the authors).
Comparison Treatment. The comparison treatment group (n = 14)received 30 minutes of curriculum-based small group counseling onceper week for 15 weeks. Kids Connection, a designated Center forSubstance Abuse Prevention "Exemplary" program, was selected basedon the following criteria: (a) defined as a culturally competentcurriculum, with both English and Spanish versions; (b)developmentally responsive, with materials and activities specificallytargeting different grade levels; (c) targets children exhibiting at-riskbehaviors; (d) designed as a school-based counseling curriculum,currently utilized in school districts in 33 states, and finally; (e) providedempirical support for its effectiveness in reducing behavior problemsand improving pro-social skills (Rainbow Days, 2002).
Curriculum-based treatment groups were facilitated by a bilingualHispanic counselor who was a trained group facilitator for the KidsConnection curriculum. Groups met in a confidential setting within eachschool. While Kid's Connection recommends a group size of
60 Garza & Bratton
approximately six to eight children, the group size in this study was twoto three children due to (a) the limited number of subjects, (b)assignment of children by grade level, and (c) availability of children forscheduling. As mentioned previously, the counselor introduced childrento the group experience in both Spanish and English, informing childrenthat they could choose to speak either Spanish or English or both duringsessions. The format for the 30-minute group included a topic of focus,time for discussion of children's experiences related to the assignedtopic, followed by a play-based activity. Topics included developingautonomy, self-esteem, problem-solving and improving peerrelationships. Play-based activities included the use of puppets for role-play and a variety of art activities. The curriculum was grade-levelspecific and provided materials and content that was developmentallyappropriate to a specific age group's academic, personal and socialneeds. The therapist provided both English and Spanish activity sheets;children were allowed to select their preference depending on need orinterest.
InstrumentationThe Behavior Assessment System for Children-Parent Rating
Scale (BASC-PRS) and Teacher Rating Scale (BASC-TRS) by Reynoldsand Kamphaus (1992) is designed to rate child behavior at home and atschool. This measure was chosen for its reliability and validity, andbecause it is published in both English and Spanish. The Spanish versionof the BASC-PRS was utilized with most parents who were not fluent inEnglish. The BASC has two scales: Adaptive and Clinical. For thepurpose of this study the two composite scores within the Clinical scale,Externalizing Behaviors (aggression, conduct, and hyperactivity) andInternalizing Behaviors (anxiety, depression, and somatization) wereutilized to assess problem behaviors. Reynolds and Kamphaus (1992), ina summarization of reliability and validity studies for the BASC-PRS andBASC-TRS, indicated that all PRS and TRS composites have high internalconsistency and test-retest reliability, with scores in the .80s to low .90s.The test was shown to be reliable with both genders. Test-retest

School-Based Child-Centered Play Therapy 61
reliability, with a median value of .88 for BASC-PRS and .89 for BASC-TRS, indicated a high degree of reliability. Overall scale reliabilities showan average of .70. Currently, tests on reliability and validity have notbeen conducted for the Spanish version of the BASC-PRS.
Data collectionPrior to treatment, parents and teachers of all Hispanic students
referred for counseling were asked by the school counselor to completethe Behavior Assessment Scale for Children (BASC). Data served toscreen participants for inclusion criteria, as well as to measure pre-treatment behavior. In designing the research methodology, theresearchers were concerned about insuring the integrity of datacollection from parents. School officials had reported difficulty incollecting paperwork from this population of parents and difficulty inmotivating them to come to school to participate in activities. Thus, fromthe beginning, the researchers planned carefully to avoid similarproblems that would threaten the integrity of data. Home visits wereconducted by Spanish-speaking therapists both at pretesting andposttesting for the majority of parents due to lack of transportation orinability to come to the school setting during school hours to completethe BASC-PRS and parent interview. In cases where families had manychildren, and for those who lived in a multi-family home, a researchassistant was enlisted to supervise the children in the home, so theresearcher could be available to answer questions or clarify informationon the forms. This approach allowed parents to focus their attention andcomplete the behavior questionnaire on their child with limiteddistractions, thus insuring consistency in data collection proceduresacross subjects.
The BASC-TRS was distributed pre- and post-treatment toteachers, along with a deadline for returning to researchers. Theresearchers assumed that teachers would be responsible for finding aquiet time outside of class to complete the questionnaires; therefore, acontrolled environment for collecting teacher data was not provided.Teachers returned pre-test data in a timely manner; however, problems
62 Garza & Bratton
became apparent during posttesting when multiple requests were issuedto obtain post BASCs from teachers, and several teachers were observedhurriedly completing instruments during class time. Several end-of-the-year factors likely contributed to the difference in pre-test and post-testdata collection. The researchers' failure to provide a controlledenvironment for teachers to complete the BASC-TRS resulted ininconsistency in data collection procedures across subjects.
Anecdotal data was recorded by the researchers throughout thestudy in order to identify notable happenings and to better understandthe clinical significance of findings (Kazdin, 1999). Data includedobservations and field notes regarding the Hispanic treatment providers'experiences specific to culturally relevant issues noted during treatment,as well as comments from parents, family members, teachers, and schooladministrators regarding the effects of treatment. Therapists for bothtreatment groups completed session summary forms on each child,specifically noting significant verbalizations and interactions, use ofSpanish and English, significant play behaviors, and use of traditionalplayroom toys and culturally-specific toys.
RESULTS AND DISCUSSION
To statistically analyze the effects of Child-Centered PlayTherapy (CCPT) compared to curriculum-based small group counselingwith Hispanic children, a two factor repeated measures Analysis ofVariance (ANOVA) was performed on all appropriate data. Significantdifferences between the means across time were tested at the 0.05 alphalevel in order to assess the significance of the change between the twogroup's pretest and posttest scores. Cohen's d effect size was calculatedin order to assess the practical significance of findings, or the magnitudeof the difference between the two groups. Effect size calculations alsoallow for treatment effect comparisons across studies. Thompson (2000)suggested that researchers report results in ways that are relevant totheir discipline and to similar research in the field. In determining thepractical significance of the findings in this study, the authors followed

School-Based Child-Centered Play Therapy 63
Cohen's (1988) guidelines for interpretation, in which he proposed that0.20 is considered a "small" treatment effect, 0.50 a "medium" effect, and0.80, a "large" effect.
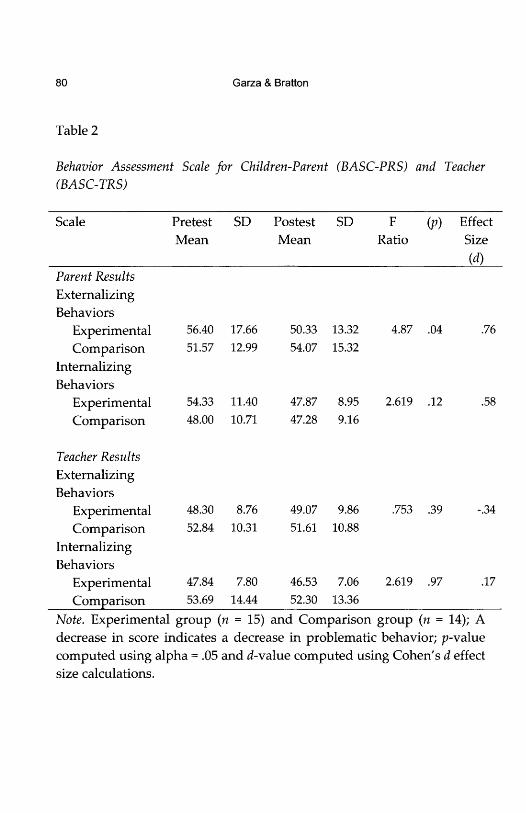
Externalizing problemsAs shown in Table 2, the Externalizing Problems composite scale
of the BASC-PRS yielded statistically significant results (p = .04) insupport of the CCPT treatment. Cohen's d was calculated to assess themagnitude of the treatment effect. Results indicate that according toparents' reports, the CCPT intervention had a large treatment effect (d =.76) on children's externalizing problem behaviors, when compared tochildren receiving curriculum-based small-group counseling. Resultsfrom teacher report on the Externalizing Problems scale of the BASC-TRSdid not reveal statistical or practical significance. As previously stated,irregularities in post-test collection of teacher data were observed. Theresearchers' failure to control for the integrity of teacher data collectionmakes it difficult to confidently interpret these results.
Parent-reported findings are consistent with a study done witha similar population that showed group play therapy was effective inimproving Puerto Rican children's self-control, when compared to no-treatment (Trostle, 1988). These findings are also similar to meta-analyticfindings on effects of play therapy outcomes (Bratton et al., in press) thatshowed that play therapy had a large treatment effect on children'sexternalizing behavior problems (ES = 0.78), when compared to notreatment. Other controlled play therapy studies conducted primarilywith Caucasian children have shown moderate to large treatment effectson externalizing problems when play therapy was compared to notreatment (Jones, Rhine, & Bratton, 2002; Kot, 1995; Packman & Bratton,2003; Tyndall-Lind, 1999), while other controlled play therapy studieshave reported less favorable results on externalizing behaviors(McGuire, 2001; Rennie, 2000). In light of previous findings regarding theeffects of play therapy on externalizing problems compared to notreatment, the findings in the present study are particularly noteworthy.

64 Garza & Bratton
Conduct problems were the most common referral complaint fromparents; as a result a post hoc analysis was executed on the Conductsubscale, one of three subscales in the Externalizing composite scale onthe BASC-PRS. Of note, during pretest interviews with parents, theresearcher asked the following two questions to solicit spontaneousfeedback: "What concerns you most about your child?" and "What doyou like most about your child?" Parents' responses were similar in thata majority verbalized "No me hace caso" or, "He doesn't mind me"when responding to the question about concerns. This focus on conductwas repeated in their response to the second question, "What do you likemost about your child," in which parents verbalized, "Me gusta cuandome hace caso" or "I enjoy him when he minds me." The frequency inwhich these parents focused on conduct may be unique to this culture,particularly since all thirty of the parents in the parent interviews wereborn in Mexico. This information may be beneficial to school counselorsand other mental health professionals in understanding the values oftraditional Hispanic parents.
According to parent results, children who received the CCPTtreatment experienced a statistically significant (p = .02) reduction inconduct problem behaviors, when compared to the children whoreceived curriculum-based counseling. More important to thepractitioner, effect size results indicate that CCPT demonstrated a largetreatment effect (d = .86) on children's conduct problems. This findingseems particularly important in the context of the high value theHispanic parents in this study placed on good conduct. Additionally, thelist of behaviors identified under conduct problems are consistent withbehaviors that have been identified as placing Hispanic children at ahigher risk for academic struggles and delinquency (Cortez, 1999; NCES,2003). Thus, this treatment has the potential to prevent future problemsoften associated with this population.
Internalizing problemsAs shown in Table 2, the children receiving CCPT showed a
reduction in internalizing behavior problems on the BASC-PRS over the

School-Based Child-Centered Play Therapy 65
comparison group, but not at a statistically significant level (p = .12). Toassess the practical significance of these findings, an effect size wascalculated, revealing that CCPT produced a moderate treatment effect (d= .58) over the comparison group. These results indicate that per parents'report, children in the CCPT group demonstrated moderateimprovements in internalizing behaviors over the children receivingcurriculum-based small group counseling. Results from teachers' reporton the Internalizing Problems scale of the BASC-TRS did not revealstatistical or practical significance. As noted previously, irregularities inpost-test collection of teacher data made it difficult to confidentlyinterpret teacher results.
The moderate treatment effect on internalizing problems reportedby parents is of particular clinical importance since these types ofbehaviors are generally less disruptive and often go unnoticed byparents and teachers. If left untreated, these problems can lead to moreserious and costly problems in adolescence (U.S. Public Health Service,2000). Other controlled play therapy outcome studies, conducted withprimarily Caucasian children, have shown moderate to large treatmenteffects on internalizing problems when play therapy was compared to notreatment (Brandt, 1999; Constantino et al, 1986; Jones et al., 2002;Packman & Bratton, 2003); while other play therapy studies havereported less favorable results on internalizing behaviors (Rennie, 2000;McGuire, 2001; Danger, 2003).
Anxiety and anxiety related issues was the second major concern atthe time of parent intake; as a result, a post hoc analysis was conductedon the Anxiety subscale, one of three subscales on the Internalizingcomposite scores on the BASC-PRS. When measured against thecomparison group, children receiving CCPT showed a reduction inanxiety, but not at a statistically significant level (p = 0.10). Effect sizecalculation showed that, according to parents, CCPT demonstrated amoderate treatment effect (d = 0.60) on children's anxiety, whencompared to curriculum-based counseling. Considering parents'frequently reported concerns about their children's anxiety related toschoolwork, tests and homework, CCPT's moderate treatment effect on

66 Garza & Bratton
anxious behaviors seems noteworthy. Anxiety has also been identified asa warning sign among school drop outs (Cortez, 1999; NCES, 2003); thus,this intervention has the potential to lessen the symptoms of schoolrelated anxiety and could improve the likelihood of these childrenstaying in school.
SUBJECTIVE OBSERVATIONS
Anecdotal data from this study, including direct observation andfeedback from parents and teachers, provides important information topractitioners who are primarily concerned with the clinical significanceof research findings, or how treatment impacted children's day-to-dayfunctioning. Kazdin (1999) explained the importance of clinicalsignificance as, "whether the intervention makes a real (e.g., genuine,palpable, practical, noticeable) difference in everyday life to clients or toothers with whom the client interacts" (p. 332). Throughout the study,the researchers recorded data obtained from the therapists' observationsfor both treatment interventions, as well as recorded feedback fromparents, teachers and school administrators regarding participantbehaviors.
School personnel observations and commentsTeachers and school administrators noted that office referrals had
ceased for several participants who had been "regulars" in theprincipal's office prior to treatment. In fact, in two cases, office referralshad ceased after the first two treatments. Teachers reported that severalchildren who had been referred due to being excessively reserved orwithdrawn in class had "come out of their shell," and as a result wereparticipating more in class discussions, seemed to benefit more fromlearning opportunities, and interacted more appropriately with otherchildren.
School-Based Child-Centered Play Therapy 67
Parent observations and commentsParents' comments also focused on improvements in problem
behaviors and anxiety. However, parents tended to talk more about theirown feelings of relief that their children were exhibiting fewer behaviorproblems at school, evidenced by a noted reduction in behavioral reportsfrom teachers. Increased parental acceptance was also noted in parents'post treatment comments. As discussed previously, parents in this studyplaced a high value on their children behaving in ways consistent with"good conduct," therefore it is plausible that parents' perceivedimprovements in this area impacted their acceptance of their children.Additional observations commonly expressed by parents included thattheir children seemed less "worried" about school, "played" better withsiblings and neighbors, and seemed "happier."
Culturally-relevant observationsIn general, culturally specific information related to mental health
treatment has been under-researched or under-reported; therefore, thefollowing preliminary observations are offered because of their potentialclinical significance and to stimulate further investigation. However, thereader is again cautioned to avoid over-generalizing culturally specificinformation. Therapists' observations supported the notion thatincluding culturally relevant craft materials and toys facilitatescommunication and a sense of familiarity, especially in initial sessions.Children seemed to find comfort in entering the playroom and findingtoys specific to their culture. Many of the children would eagerly go toeach of the "Mexico" toys, exclaiming, "I have one like this!" or "you gotthis in Mexico!" Additional cultural observations include (a) olderchildren's preference for using Spanish when disclosing personal orintimate information on such topics as smoking cigarettes, stealing,drugs, and skipping school; one girl disclosed issues around hermother's promiscuous behavior in Spanish, but spoke English for themajority of sessions, (b) frequency in selection of toys from the culturallyresponsive toy list, (c) use of the Spanish language and/or cultural toysseemed to help create an atmosphere of familiarity and security,

68 Garza & Bratton
particularly in relationship building with the Hispanic play therapist,and (d) males in the small group intervention seemed to formparticularly close bonds and used informal Spanish more frequently,often referring to each other as "compadres," which translates to kinship.Esquivel and Keitel (1990) noted that a sense of closeness in regards tofamily and community is of high value among Hispanics. This valuemay have been a factor in the quality of interactions noted in the childrenreceiving the small group interaction. Both Hispanic treatment providersreported a shared experience that efforts to provide a more culturally-relevant environment for the children in the study resulted in a moreresponsive approach to understanding the children's needs andexperiences, and ultimately helped build a more positive therapeuticrelationship with the child, family, and Hispanic community.
CONCLUSIONS
This preliminary investigation indicates that according to parentreport, Child-Centered Play Therapy (CCPT) demonstrated a moderateto large treatment effect on the reduction of behavior problems ofHispanic, school-age children. Specifically, CCPT showed a largetreatment effect on externalizing problem behaviors and a moderatetreatment effect on internalizing problem behaviors, when measuredagainst a curriculum-based small group counseling intervention. Thesepositive findings were supported by parent, teacher, and therapistobservations. Taking into consideration parents' strong concerns aboutconduct problems prior to treatment, CCPT's large treatment effect inthis area seems especially meaningful. More investigation is needed toknow if the value placed on "good conduct" was limited to the Mexican-born parents in this study or is consistent with traditional Mexicanfamilies residing in the United States.
The results of this study are further noteworthy because, unlikethe majority of outcome research in play therapy and childpsychotherapy, in which the experimental treatment is compared to notreatment, this study compares CCPT to a research-supported
School-Based Child-Centered Play Therapy 69
intervention (Rainbow Days, 2003). In light of previous research findingsthat showed moderate to large treatment effects for play therapycompared to no treatment, the findings in this study are promising. It isreasonable to assume that comparing play therapy to no treatmentwould produce larger treatment effects than comparing play therapy to aproven intervention.
Finally, results indicate that CCPT can be implementedsuccessfully in the school setting as an early intervention for Hispanicchildren. Advocates for the mental health needs of this population haveemphasized the need to provide research-based, culturally responsiveservices in settings that provide Hispanic children with equal access toservices. These findings suggest that school-based CCPT is a viablesolution.
LIMITATIONS
The following limitations are offered for the reader'sconsideration when interpreting the data. As is true of most research inthe mental health field, the sample size was small, impactinggeneralizability and power of findings. Participants were restricted toHispanic children in one school district in the Southwest United States;thus, limiting the ability to generalize the results to other Hispanicpopulations. Another limitation is that treatment format (e.g."individual" CCPT vs. "small group" curriculum-based counseling) wasnot controlled for and could have impacted results. This issue may beparticularly relevant in designing mental health interventions forHispanic children. Traditionally, Hispanics have valuedinterdependence and family/peer relationships, dynamics found ingroup interventions, but not individual therapy. And finally, asdiscussed the researchers noted problems in the integrity of datagathered from teachers, resulting in an inability to confidently interpretteacher results.

70 Garza & Bratton
RECOMMENDATIONS FOR RESEARCH AND PRACTICE
In this study, Child-Centered Play Therapy (CCPT) wassuccessfully implemented in a school setting where Hispanic childrenare more likely to have access to services and are less likely to drop outof treatment. This is particularly important since Hispanics generallyunder-utilize community mental health services (Falicov, 1998).Therefore, the primary recommendation for future practice is toimplement CCPT in the schools, where all Hispanic children can beafforded services when at-risk behaviors are first detected. To achievethis aim, elementary schools must recruit more culturally competent,Spanish-speaking counselors, with specific training and experience inCCPT procedures. This recommendation had obvious implications foruniversities and the recruitment and training of Hispanic and bilingualmental health professionals. Additionally, counselors should strive forcultural-responsiveness in all ways possible, such as (a) consulting withcolleagues on toys and materials that capture elements of culture andenvironment for clientele, (b) utilizing community resources to betterunderstand the unique cultural needs of Hispanic families in a specificarea; and most importantly, (c) applying cultural knowledge learnedfrom clients and their families.
Based upon results of this study, the following recommendationsare offered to future researchers: (a) replicate study using a largersample size in order to increase generalizability and power of findings,adding a no-treatment control group to help control for maturation ofthe children over time; (b) replicate study in several different locations toallow generalization of results to a broader group of Hispanics; (c)conduct a study comparing individual and group Child-Centered PlayTherapy (CCPT) with Hispanic children in order to control for the"compadre" factor observed in the small group intervention; (d) conductqualitative research to explore culturally specific factors noted in thisstudy, including children's use of multicultural toys versus traditionalplay room toys, the impact of ethnicity in client-therapist pairings, andchildren's use of language (English and Spanish) in relation to specific
School-Based Child-Centered Play Therapy 71
play behaviors, toys and topics; (e) consider utilizing assessment toolsthat reduce the reliance upon outside observation from teachers orparents, such as instruments that assess child variables from the child'spoint of view and/or direct observation by trained professionals; andfinally, (f) control for outside influences that undermine the integrity ofdata collection. The researchers learned that home visits to collect parentdata are essential with this population. Teacher data should be collectedin a controlled environment, not left to chance and to avoid collectingdata, particularly from teachers, during the last few weeks of the schoolyear.

72 Garza & Bratton
REFERENCES
Altarriba, J., & Bauer, L. M. (1998). Counseling the Hispanic client:Cuban Americans, Mexican Americans, and Puerto Ricans.Journal of Counseling & Development, 76(4), 389-398.
Axline, V. (1969). Play therapy (rev. ed.). New York: Ballantine.Baruth, L. G., & Manning, M. L. (1992). Understanding and counseling
Hispanic American children. Elementary School Guidance &Counseling, 27(2), 113-123.
Brandt, M. A. (1999). An investigation of the efficacy of play therapywith young children. Dissertation Abstracts International, 61(07).2603.
Bratton, S., & Ray, D. (2000). What the research shows about playtherapy. International Journal of Play Therapy, 9(1), 47-88.
Bratton, S., Ray, D., Rhine, T., & Jones, L. (in press). The efficacy of playtherapy with children: A meta-analysis review of treatmentoutcomes. Professional Psychology: Research and Practice.
Cochran, J. L. (1996). Using play and art therapy to help culturallydiverse students overcome barriers to school success. SchoolCounselor, 43(4), 287-299.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nded.). New York: Academic Press.
Collins, R., & Ribeiro, R. (2004). Toward an early care and educationagenda for Hispanic children. Early Childhood Research & Practice.Retrieved March 30, 2005 from www.ecrp.uiuc.edu/v6n2/collins.html.
Constantine, M. G. (2001). Multicultural training, theoretical orientation,empathy, and multicultural case conceptualization ability incounselors. Journal of Mental Health Counseling, 23(4), 357-374.
Constantino, G., Malgady, R., & Rogler, L. (1986). Cuento therapy: Aculturally sensitive modality for Puerto Rican children. Journal ofConsulting and Clinical Psychology, 54(5), 639-645.
Cortez, A. (1999, January). Missing Texas youth-Dropout and attrition ratesin Texas public high schools (An Excerpt). Interdisciplinary

School-Based Child-Centered Play Therapy 73
Research Association. Retrieved October 6, 2004 fromhttp://www.idra.gov.
D'Andrea, M., & Bradley, L. (1995). A comparative study of the worriesof Mexican American and White students: Implications forschool counselors. Journal of Humanistic Education & Development,33(4), 183-193.
Dallas Commission on Children and Youth. (2000, April). Student dropoutsummary report and recommendations. Dallas, TX: CommunityCouncil of Greater Dallas.
Danger, S. (2003). Adaptive doll play: Helping children cope withchange. International Journal of Play Therapy, 22(1), 105-116.
Del Castillo, A. R. & Torres, M. (1988). The interdependency ofeducational institutions and cultural norms: The Hispanicexperience. In T. McKenna & F.I. Ortiz (Eds.), The broken web: Theeducational experience of Hispanic American Women (pp. 39-60).Encino, CA: Floricanto Press.
Durodoye, B. A. (2002). Preparing counselors to dialogue about race.Texas Counseling Association Journal, 30(2), 18-23.
Esquivel, G. B., & Keitel, M. A. (1990). Counseling immigrant children inthe schools. Elementary School Guidance & Counseling, 24, 213-221.
Falicov, C. J. (1998). Latino families in therapy: A guide to multiculturalpractice. New York: Guilford Press.
Foulks, E. (2004). Cultural variables in psychiatry. Psychiatric Times,24(4), 28-30.
Glover, G. J. (2001). Cultural considerations in play therapy. In G.Landreth (Ed.), Innovations in play therapy: Issues, process, andspecial populations (pp. 31—41). Philadelphia: Brunner-Routledge.
Hinman, C. (2003). Multicultural considerations in the delivery of playtherapy services. International Journal of Play Therapy, 12(2), 107-119.
Irwin, E. C. (1983). The diagnostic and therapeutic use of pretend play.In C. E. Shaefer and K. J. O'Connor (Eds.), Handbook of playtherapy (pp.148-173). New York: John Wiley and Sons.

74 Garza & Bratton
Jones, L., Rhine, T., & Bratton, S. (2002). High school students astherapeutic agents with young children experiencing adjustmentdifficulties: The effectiveness of a filial therapy training model.International Journal of Play Therapy, 11(2), 43-62.
Kazdin, A. (1999). The meanings and measurement of clinicalsignificance. Journal of Consulting and Clinical Psychology, 67, 332-339.
Koss-Chioino, J. D., & Vargas, L. A. (1992). Working with culture. SanFrancisco: Jossey-Bass.
Kot, S. (1995). Intensive play therapy with child witnesses of domesticviolence (Doctoral dissertation, University of North Texas).Dissertation Abstracts International, 56, 3002.
Kottman, T. (2001). Play therapy: Basics and beyond. Alexandria, VA:American Counseling Association.
Landreth, G. L. (2002). Play therapy: The art of the relationship. Bristol, PA:Accelerated Development Inc.
Landreth, G. L., Homeyer, L. E., Glover, G., & Sweeney, D. S. (1998). Playtherapy Interventions with children's problems. Horthvale, NJ: JasonAronson.
Martinez, K., & Valdez, D. (1992). Cultural considerations in playtherapy with Hispanic children. In L. A. Vargas & J. D. Koss-Chioino (Eds.), Working with culture: Therapeutic interventions withethnic minority children and adolescent (pp. 85-101). San Francisco:Jossey-Bass.
McGuire, D. (2001). Child-centered group play therapy with childrenexperiencing adjustment difficulties (Doctoral dissertation,University of North Texas). Dissertation Abstracts International,61,10.
Moustakas, C. (1973). The child's discovery of himself. New York: Aronson.National Center for Educational Statistics. (2003, April). Status and trends
in the education of Hispanics. Retrieved [date] fromhttp://www.nces.ed.gov/pubs2003/2003008.pdf.

School-Based Child-Centered Play Therapy 75
Packman, }., & Bratton, S. C. (2003). A school-based group play/activitytherapy intervention with learning disabled preadolescentsexhibiting behavior problems. International Journal of PlayTherapy, 22(2), 7-29.
Rainbow Days Inc. (2003). Kids' Connection: A support group curriculum forchildren, ages 4-12. Dallas, TX: Rainbow Days, Inc.
Ramirez, L. (1999). A reader's response to working with Latino clients:Five common mistakes. Association for Play Therapy Newsletter,18(1), 3-4.
Rennie, R. (2000). A comparison study of the effectiveness of individualand group play therapy in treating kindergarten children withadjustment problems (Doctoral dissertation, University of NorthTexas). Dissertation Abstracts International, A63 (09), 3117.
Reynolds, C. R., & Kamphaus, R. W. (1992). Behavior assessment scale forchildren. Circle Pines, MN: American Guidance Service.
Rogers, C. R. (1951). Client-centered therapy: Its current practice,implications, and theory. Boston: Houghton Mifflin.
Santiago-Rivera, A. (1995). Developing a culturally sensitive treatmentmodality for bilingual Spanish-speaking clients: Incorporatinglanguage and culture in counseling. Journal of Counseling &Development, 74(1), 12-18.
Thompson, B. (2000). A suggested revision to the forthcoming 5th edition ofthe APA publication manual. Retrieved October 15, 2004 fromhttp://coe.tamu.edu/~bthompson/apaeffec.htm.
Trostle, S. L. (1988). The effects of child-centered group play sessions onsocial-emotional growth of three to six year old bilingual PuertoRican children. Journal of Research in Childhood Education, 2(3), 93-106.
Tyndall-Lind, M. (1999). A comparative analysis of intensive individualplay therapy and intensive sibling group play therapy withwitnesses of domestic violence (Doctoral dissertation, Universityof North Texas). Dissertation Abstracts International, 60 (05), 1465.
United States Bureau of the Census. (2000). Hispanic population. RetrievedOctober 6, 2004 from http://www.census.gov/prod/2001pubs/.
76 Garza & Bratton
United States Bureau. (2003). PPL Table 2A: Primary child carearrangement of preschoolers of employed mothers, Spring 1999.In Survey of income and program participation (SIPP), 1996 panel,wave 10. Retrieved August 4, 2004 fromhttp://www.census.gov/population/socdemo/child/ppl-168AabO2A.pdf.
United States Public Health Service. (2000). Report of the Surgeon General'sconference on children's mental health: A national action agenda.Washington, DC: Department of Health and Human Services
Vandenberg, B., & Kielhofner, G. (1982). Play in evolution, culture, andindividual adaptation: Implications for therapy. American Journalof Occupational Therapy, 36(1), 20-28.
Vygotsky, L. S. (2002). Play and its role in the mental development ofthe child. Retrieved October 15, 2004 fromhttp://marxists.org/archive/vygotsky/works/1933/play.htm.

School-Based Child-Centered Play Therapy 77
Table 1
Toys and materials in addition to the toy list recommended by Landreth (2002)
Toys & Materials DescriptionAlcoholic beverages Small empty plastic bottle (can be found bycontainers suppliers)
Animals Rooster, parrot, rattle snake
Assortment of musical Accordian, bongos, maracasinstruments
Bus Representative of public transportation
Bingo cards Loteria, cultural pictures and words
Cars and trucks "Beefed up" tires and rims, lowriders andvehicles of customized color tones
Coffin and skeleton Representative of the Mexican holiday "day ofthe dead"(sandtray figure size)
Cooking Utensils with Mexican designs, molcajete,tortilla rolling pin
Dolls Darker skin tones (Baby doll and doll housesize)
Dress-up Attention to customs and male/female roles, aswell as to the cultural celebration of thequinceanera
Food Common to culture, avocado, chili pepper, andtaco

78 Garza & Bratton
Toys & Materials Description
Markers Multicultural skin tones
Religious symbols Sandtray miniatures
Tools Realistic hammer, screwdriver, wood pieces,nails (as developmentally appropriate)
Note. The toys listed were used in the study and are perceived to bespecific to the environment, culture and lifestyle of the Hispanic childrenin the study. Many of these items were actually purchased in Mexico forauthenticity and may be difficult to find in the United States. For moredetails about toys, contact authors.

School-Based Child-Centered Play Therapy 79
Table 2
Behavior Assessment Scale for Children-Parent (BASC-PRS) and Teacher(BASC-TRS)
Scale Pretest SD Postest SD F (p) EffectMean Mean Ratio Size
( & _Parent ResultsExternalizingBehaviors
Experimental 56.40 17.66 50.33 13.32 4.87 .04 .76Comparison 51.57 12.99 54.07 15.32
InternalizingBehaviors
Experimental 54.33 11.40 47.87 8.95 2.619 .12 .58Comparison 48.00 10.71 47.28 9.16
Teacher ResultsExternalizingBehaviors
Experimental 48.30 8.76 49.07 9.86 .753 .39 -.34Comparison 52.84 10.31 51.61 10.88
InternalizingBehaviors
Experimental 47.84 7.80 46.53 7.06 2.619 .97 .17Comparison 53.69 14.44 52.30 13.36
Note. Experimental group (n = 15) and Comparison group (n = 14); Adecrease in score indicates a decrease in problematic behavior; p-valuecomputed using alpha = .05 and d-value computed using Cohen's d effectsize calculations.
80 Garza & Bratton
Table 2
Behavior Assessment Scale for Children-Parent (BASC-PRS) and Teacher(BASC-TRS)
Scale Pretest SD Postest SD F (p) EffectMean Mean Ratio Size
(d)_Parent ResultsExternalizingBehaviors
Experimental 56.40 17.66 50.33 13.32 4.87 .04 .76Comparison 51.57 12.99 54.07 15.32
InternalizingBehaviors
Experimental 54.33 11.40 47.87 8.95 2.619 .12 .58Comparison 48.00 10.71 47.28 9.16
Teacher ResultsExternalizingBehaviors
Experimental 48.30 8.76 49.07 9.86 .753 .39 -.34Comparison 52.84 10.31 51.61 10.88
InternalizingBehaviors
Experimental 47.84 7.80 46.53 7.06 2.619 .97 .17Comparison 53.69 14.44 52.30 13.36
Note. Experimental group (ft = 15) and Comparison group (ft = 14); Adecrease in score indicates a decrease in problematic behavior; p-valuecomputed using alpha = .05 and d-value computed using Cohen's d effectsize calculations.








![No. OCS11 TECHNICAL DATA BOOKR410A INVERTER PLA-RP·BA(2 ...mitsubishitech.co.uk/.../PLA-RP-BA/PLA-RP-BA_PUHZ-HRP-V[Y]HA2_… · 2 SPECIFICATIONS 2-1. CEILING CASSETTE TYPE Model](https://img.pdfslide.us/doc/110x75/603ed7f6c267564f1b52b3b3/no-ocs11-technical-data-bookr410a-inverter-pla-rpba2-yha2-2-specifications.jpg)




















