Embed Size (px)
Citation preview

9/06/2016
1
SCHNWestmead
EATINGDISORDER
SERVICE
Where do we start? Doing something locally to treat children and adolescents
with eating disorders
Andrew WallisSloane Madden
EDSWestmeadInpa/entClinicalPathway
WardbasedProgram
Medicalstabilisa2on/re-feeding
SupervisedmealsPsychiatry
FamilyassessmentIndividualsuppor2ve
therapyTrafficlights
Discharge
CHWOutpa/ent
Clinic
Localservice
RuralSupport/consulta/on
CAPTOSIFAEDRuralsupport
Re-assess
FamilyAdmissionProgram
IFAEDDayProgram
Mul/familyTherapy
Tailoredinterven2on
SchoolPhysioDiete2cs
Adolescentgroup
Rural/remotePoorinpa2entresponseProblemunclearHighriskANbehaviours++Parentcapacityboost
Poorin/outpa2entresponseComorbiddifficulty++RiskofchronicityParentcapacityboostHighEE
Re-admission
8BEDS
8-12PLACES10-18y.o
8FAMILIES/6peryear
~3FAMILIESPerTerm
Guiding Principles
1. Multidisciplinary specialist care essential to positive outcome
2. Evidence based practice and treatments central
3. Developmentally sensitive to medical and psychological needs
4. Family focused, inclusive and enabling
5. Intensity and support to target illness complexity
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 3
What we know?
Key issues• Specialist vs generalist care
• Systems support• Treatment efficacy
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 4
2012 N=378 (34 services)
Specialist services -• Identify 2-3 more cases
• Lower rates of inpatient admission• Higher consistency of care 5
Comparison of Specialist and Nonspecialist CarePathways for Adolescents with Anorexia Nervosa and
Related Eating Disorders
Jennifer House, PhD1
Ulrike Schmidt, PhD, MD2
Meghan Craig, CPsychol1
Sabine Landau, PhD3
Mima Simic, MD4
Dasha Nicholls, MD5
Pippa Hugo, MRCPsych6
Mark Berelowitz, FRCPsych7
Ivan Eisler, PhD1*
ABSTRACTObjective: To explore the role of spe-cialist outpatient eating disorders serv-ices and investigate how direct access tothese affects rates of referral, admissionsfor inpatient treatment, and continuityof care.
Method: Services beyond primary carein Greater London retrospectively identi-fied adolescents who presented with aneating disorder over a 2-year period.Data concerning service use were col-lected from clinical casenotes.
Results: In areas where specialist out-patient services were available, 2–3 timesmore cases were identified than in areas
without such services. Where initial out-patient treatment was in specialist ratherthan nonspecialist services, there was asignificantly lower rate of admission forinpatient treatment and considerablyhigher consistency of care.
Discussion: Developing specialist out-patient services with direct access fromprimary care is likely to lead to improve-ments in treatment and reduce overallcosts. VVC 2012 by Wiley Periodicals, Inc.
Keywords: adolescents; anorexia nervosa;care pathways; inpatient treatment; outpatienttreatment; service organization
(Int J Eat Disord 2012; 45:949–956)
Introduction
The growing body of literature on the efficacy ofoutpatient treatments for adolescents with ano-rexia nervosa shows that family therapy is effective1
and has excellent long-term outcomes,2–4 and it isconsequently recommended in clinical guidelines.5
Studies show that the great majority of young peo-ple with anorexia nervosa can be treated on a purelyoutpatient basis, with 70%–90% at least partiallyrecovered by the end of 6–12 months of treatmentand relapse rates of less than 10%.1–4 Although theuse of such evidence-based treatments is growing inthis area, clinical practice still varies considerably.UK national figures show that prolonged inpatienttreatment is relatively common, with admissionrates of over 35% for adolescents6 and over 50% foryounger patients,7 and psychiatric bed use foryoung people with eating disorders being higherthan for any other diagnostic group.8 There is noclear evidence in favor of inpatient care over outpa-tient care,9 and some evidence that long-termadmission may have a negative impact on out-come,10 as well as being more costly.11
In the United Kingdom, outpatient treatment set-tings for adolescents with anorexia nervosa rangefrom general mental health services to highly speci-alized eating disorders services, but little is knownabout the impact of these different settings ontreatment outcomes. One randomized-controlledtrial, the Treatment Outcome for Child and Adoles-cent Anorexia Nervosa (TOuCAN) trial, which com-pared general and specialist outpatient treatment,found no association between physical and psy-
Presented at the Academy for Eating Disorders’ International
Conference on Eating Disorders 2011: Miami, Florida.
This work is supported by the National Institute for Health
Research (NIHR) under its Programme Grants for Applied Research
Scheme (RP-PG-0606-1043). The views expressed herein are not
necessarily those of the NHS, the NIHR or Department of Health.
*Correspondence to: Ivan Eisler, Section of Family Therapy, P.O.
Box 73, Institute of Psychiatry, King’s College London, DeCrespigny Park, London SE5 8AF, UK. E-mail: [email protected]
Accepted 26 August 2012
1 Department of Psychology, Section of Family Therapy, Institute
of Psychiatry, King’s College London, London, United Kingdom2 Department of Psychological Medicine, Section of Eating Disor-
ders, Institute of Psychiatry, King’s College London, London,
United Kingdom3 Department of Biostatistics, Institute of Psychiatry, King’s
College London, London, United Kingdom4 South London and Maudsley NHS Foundation Trust, Child and
Adolescent Eating Disorders Service, London, United Kingdom5 Great Ormond Street Hospital for Children NHS Foundation Trust,
Feeding and Eating Disorders Service, London, United Kingdom6 South West London and St George’s Mental Health NHS Trust,
Child and Adolescent Eating Disorders Service, London, United
Kingdom7 Royal Free Hampstead NHS Trust, Child and Adolescent Eating
Disorders Service, London, United Kingdom
Published online 4 October 2012 in Wiley Online Library(wileyonlinelibrary.com). DOI: 10.1002/eat.22065
VVC 2012 Wiley Periodicals, Inc.
International Journal of Eating Disorders 45:8 949–956 2012 949
REGULAR ARTICLE (CE ACTIVITY)
Specialistservice=>25newEDreferrals,MDT,
onepersonwithexperiencetrea2ngED’s,exper2setodeliverEBT
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 6
Figure1- Directhealthcarecostsbycarepathway
£17,149
£34,780£41,641£43,306
£111,118
£125,048
£0
£20,000
£40,000
£60,000
£80,000
£100,000
£120,000
£140,000
AssessedandtreatedinSpecialist
AssessedinNon-specialisttreatedinSpecialist
AssessedandstartedtreatmentinNon-specialist
Averagecostpercase Averagecostpergoodoutcome
Schmidtetal(submiXed)paperDatafromEisler&Simic2014SubmissiontotheHouseofCommonsHealthSelectCommi3ee
Cost by care pathway

9/06/2016
2
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 7
Figure2- Averageoutpatientandinpatientcostsbycarepathway
£9,572 £10,342£8,789£7,981
£24,774
£33,282
£0
£5,000
£10,000
£15,000
£20,000
£25,000
£30,000
£35,000
AssessedandtreatedinSpecialist
AssessedinNon-specialisttreatedinSpecialist
AssessedandstartedtreatmentinNon-specialist
Outpatientcosts Inpatientcosts
Schmidtetal(submiXed)paperDatafromEisler&Simic2014SubmissiontotheHouseofCommonsHealthSelectCommi3ee
Inpatient and outpatient costs
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 8
2016N=34• Admission % EBW 82.72 (7.28)• EOT 45.9% EBW > 95%; 89% EBW > 85%• Comorbid rate 54.1%
Meansessions14.14(9.19)Dropoutrate28%
2013N=40• Poor fidelity is the rule rather than the exception!• Not one therapist included
• Weighing patient, Family meal, Providing nutritional guidance without involving a dietician
Understanding the Uptake of Family-Based Treatmentfor Adolescents with Anorexia Nervosa: Therapist
Perspectives
Jennifer Couturier, MD, MSc,FRCPC1,2,3*
Melissa Kimber, MSW1,3
Susan Jack, PhD3,4
Alison Niccols, PhD1
Sherry Van Blyderveen, PhD1,2
Gail McVey, PhD5,6
ABSTRACTObjective: To explore and describetherapists’ perceptions of the factorsaffecting their uptake of family-basedtreatment (FBT) for adolescents with ano-rexia nervosa (AN).
Method: Fundamental qualitativedescription guided the sampling and datacollection in this study. A purposeful sam-ple of 40 therapists providing treatmentto youth with AN, completed an in-depthinterview. Conventional content analysisguided the development of initial codesand categories, whereas constant compar-ison analytic techniques were used tocompare and contrast therapist percep-tions across contexts. Summative contentanalysis was used to provide counts ofkeywords, phrases, and themes.
Results: Therapists face several barriersto the implementation of FBT, dividedbroadly into interventional, organizational,
interpersonal, patient/family, systemic, andillness factors. Therapists support theimplementation of evidence-based prac-tices, including FBT for AN, but fidelity tothis model is not practiced. Specific con-cerns about the intervention includedweighing the patient, providing nutritionaladvice, and the family meal. Ninety-fivepercent of therapists requested furthertraining in the FBT model.
Discussion: Further investigation intothe barriers and facilitating factors to theuse of FBT is warranted. Understandingeffective dissemination and trainingstrategies is critical to ensuring patientsreceive the best possible care. VVC 2012 byWiley Periodicals, Inc.
Keywords: family-based treatment;evidence-based practices; qualitative
(Int J Eat Disord 2012; 00:000–000)
Introduction
Characterized by an excessive preoccupationwith body weight or shape, eating disorders can
have serious adverse physical and psychologicalcomplications. The mortality rate, particularly foranorexia nervosa (AN) is high, and has been shownto increase by 5.6% for each decade that an individ-ual remains ill.1,2 The patients who experience ANmay experience recurrent inpatient admissions dueto the serious medical complications causedby starvation, including cardiac arrhythmias, andelectrolyte abnormalities.3 Chronic medical com-plications include cerebral atrophy, reduced bonemineral density, and cardiac muscle wasting.3
According to the DSM-IV-TR,4 the criteria for adiagnosis of AN include a refusal to maintain acurrent body weight at 85% or higher of the normalexpected weight, an intense fear of gaining weightor becoming overweight, a disturbed experience ofone’s own body weight and shape, and amenorrheafor at least three consecutive months.
Although there remains relatively little researchon interventions that address the complex mentaland physical health needs of children and adoles-cents with AN, family-based treatment (FBT) isone form of treatment that has been gaining anevidence base, and is a recommended practice bythe American Psychiatric Association.5 Developed
Supported by Hamilton Academic Health Sciences Organization
Alternate Funding Plan Innovation Fund.
*Correspondence to: Jennifer Couturier, Pediatric Eating Disor-
ders Program, McMaster Children’s Hospital, Department of Psy-
chiatry and Behavioural Neurosciences, McMaster University, 1200
Main St. West, Hamilton, Ontario, Canada L8N3Z5.
E-mail: [email protected]
Accepted 14 July 2012
1 Department of Psychiatry and Behavioural Neurosciences,
McMaster University, Hamilton, Canada2 Department of Pediatrics, McMaster University, Hamilton, Canada3 Department of Clinical Epidemiology and Biostatistics,
McMaster University, Hamilton, Canada4 School of Nursing, McMaster University, Hamilton, Canada5 Department of Community Health Systems Resource Group,
The Hospital for Sick Children, Toronto, Canada6 Dalla Lana School of Public Health, University of Toronto,
Toronto, Canada
Published online in Wiley Online Library(wileyonlinelibrary.com). DOI: 10.1002/eat.22049
VVC 2012 Wiley Periodicals, Inc.
International Journal of Eating Disorders 00:0 000–000 2012 1
REGULAR ARTICLEEMPIRICAL ARTICLE
Clinician Adherence to Guidelines in the Delivery ofFamily-Based Therapy for Eating Disorders
Stacey Kosmerly, BA1
Glenn Waller, DPhil2
Adele Lafrance Robinson, PhD1*
ABSTRACTObjective: Clinicians have been shownto drift away from protocol in their deliv-ery of evidence-based treatments. Thisstudy explores this phenomenon in thedelivery of family-based therapy (FBT) foreating disorders, and the clinician charac-teristics that might explain such therapistdrift.
Method: The participants were 117 clini-cians who reported using FBT for eatingdisorders. They completed an online sur-vey, which included questions relating toclinician characteristics, caseload, andreported use of FBT manuals and coretherapeutic tasks, as well as a measure ofanxiety.
Results: The use of core FBT tasks washigher than for other therapies, but therewere still noteworthy gaps between rec-ommended and reported practice.Approximately a third of cliniciansreported delivering “FBT” that deviatedvery substantially from evidence-basedprotocols, often appearing to be on an
individual therapy basis. Using an FBTmanual to guide treatment delivery wasassociated with greater adherence to rec-ommended techniques. Clinician case-load and anxiety were associated withdifferences in the use of specific FBTtasks.
Discussion: Consistent with previousresearch regarding clinicians’ use of othertherapies, the delivery of FBT for the eat-ing disorders is not homogeneous.
Conclusion: Further investigation of thisphenomenon is needed to determinethe impact of deviating from treatmentprotocols on the effectiveness of FBT forthe eating disorders. VC 2014 Wiley Peri-odicals, Inc.
Keywords: family-based treatment;evidence-based practice; eatingdisorders
(Int J Eat Disord 2014; 00:000–000)
Introduction
Psychological therapies are central to the effectivetreatment of eating disorders, but only a limitednumber have empirical support. Those outpatienttherapies with the strongest evidence base arecognitive-behavioral therapies (CBT) for adults andfamily-based therapy (FBT) for younger cases.1,2
Each approach is based on the use of manualizedprotocols.3–6 Such protocol-based approaches havebeen shown to be more effective than less struc-tured versions of therapies.7 In the case of FBT, thismanual-based approach has been shown to beeffective in treating anorexia nervosa in children,adolescents and young adults,8–11 and bulimia
nervosa in adolescents.12 However, it does notwork for all cases11,13 and cannot be relied on asthe only treatment approach.14
Evidence-based FBT for eating disorders haswell-established principles and protocols.4,15 Forexample, during the first phase of treatment foranorexia nervosa, the clinician focuses on support-ing the parents to promote weight gain in theirchild, interrupting eating disorder symptoms, andnormalizing eating behaviors.15 Within this phaseare specific therapeutic tasks, for example, the cli-nician is to weigh the client at the beginning ofevery session. Next, the clinician supports the fam-ily in returning control over eating to their child,and helps the family to explore previously set-asideissues outside of the illness. Finally, the focus shiftsto the development of the child’s identity and thefamily’s adjustment to their child’s emerging inde-pendence. The treatment of bulimia nervosa issimilar.4 For example, the clinician first focuses onsupporting the parents to interrupt their child’s eat-ing disorder behaviors (e.g., inappropriate com-pensatory behaviors), and then the family issupported to explore issues outside of the illness,
Accepted 2 March 2014
*Correspondence to: Adele Lafrance Robinson, 935 Ramsey LkRd., Sudbury, ON, Canada P3E 2C6.E-mail: [email protected]
1 Department of Psychology, Laurentian University, Canada2 Department of Psychology, University of Sheffield, United
KingdomPublished online 00 Month 2014 in Wiley Online Library
(wileyonlinelibrary.com). DOI: 10.1002/eat.22276VC 2014 Wiley Periodicals, Inc.
International Journal of Eating Disorders 00:00 00–00 2014 1
2014N=117• Use of manual related to use of specific techniques• 57% or less focused on each core elements 90-100% of the time• 30% deviated substantially from model
Wallis et al 2014 Do not use without permission
Specialist LHD teams
• Identified people (medical and non-medical)
• Specialist knowledge development • Identified ‘expert’
• Standardized approaches• Assessment• Admission
• Identified sequence of care (clinical pathway)
• Organisational support and recognition
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 11 9/06/2016 SCHN Westmead EATING DISORDER SERVICE 12
A randomized controlled trial of in-patienttreatment for anorexia nervosa in medicallyunstable adolescents
S. Madden1,2*, J. Miskovic-Wheatley1,3, A. Wallis1, M. Kohn1,2,4, J. Lock5, D. Le Grange6, B. Jo5,S. Clarke4, P. Rhodes7, P. Hay8 and S. Touyz7
1Eating Disorder Service at The Sydney Children’s Hospitals Network, Westmead, Australia2Discipline of Pediatrics, Faculty of Medicine, The University of Sydney, Australia3Westmead Clinical School, The University of Sydney, Australia4Centre for Research into Adolescents’ Health (CRASH), Adolescent Medicine Unit, Westmead Hospital, Australia5Psychiatry and Behavioral Science, School of Medicine, Stanford University, USA6Department of Psychiatry and Behavioral Neuroscience, The University of Chicago, USA7School of Psychology, The University of Sydney, Australia8Centre for Health Research, School of Medicine, The University of Western Sydney and School of Medicine, James Cook University, Australia
Background. Anorexia nervosa (AN) is a serious disorder incurring high costs due to hospitalization. Internationaltreatments vary, with prolonged hospitalizations in Europe and shorter hospitalizations in the USA. Uncontrolledstudies suggest that longer initial hospitalizations that normalize weight produce better outcomes and fewer admissionsthan shorter hospitalizations with lower discharge weights. This study aimed to compare the effectiveness ofhospitalization for weight restoration (WR) to medical stabilization (MS) in adolescent AN.
Method. We performed a randomized controlled trial (RCT) with 82 adolescents, aged 12–18 years, with a DSM-IVdiagnosis of AN and medical instability, admitted to two pediatric units in Australia. Participants were randomizedto shorter hospitalization for MS or longer hospitalization for WR to 90% expected body weight (EBW) for gender,age and height, both followed by 20 sessions of out-patient, manualized family-based treatment (FBT).
Results. The primary outcome was the number of hospital days, following initial admission, at the 12-month follow-up.Secondary outcomes were the total number of hospital days used up to 12 months and full remission, defined as healthyweight (>95% EBW) and a global Eating Disorder Examination (EDE) score within 1 standard deviation (S.D.) ofpublished means. There was no significant difference between groups in hospital days following initial admission.There were significantly more total hospital days used and post-protocol FBT sessions in the WR group. There wereno moderators of primary outcome but participants with higher eating psychopathology and compulsive featuresreported better clinical outcomes in the MS group.
Conclusions. Outcomes are similar with hospitalizations for MS or WR when combined with FBT. Cost savings wouldresult from combining shorter hospitalization with FBT.
Received 9 November 2013; Revised 30 May 2014; Accepted 6 June 2014
Key words: Anorexia nervosa, family-based treatment, in-patient treatment, medical instability, treatment optimization.
Introduction
Anorexia nervosa (AN) has a lifetime prevalence of0.9–2.3% with its onset primarily in adolescence(Lewinsohn et al. 2000; Wade et al. 2006; Keski-Rahkonen et al. 2007; Preti et al. 2009). AN is the thirdmost common chronic disorder affecting adolescentfemales, with an average mortality rate of 5%
(Steinhausen, 2002). Treatment costs are among thehighest of all psychiatric disorders due to the extensiveuse of hospitalization (Striegel-Moore et al. 2000;Agras, 2001; Crow&Nyman, 2004). Although hospital-ization for the management of acute medical instability(e.g. hypothermia, hypotension, bradycardia, electro-lyte abnormalities and cardiac arrhythmias) may be es-sential in preventing morbidity and mortality (Goldenet al. 2003; Katzman, 2005), the benefits of further hospi-talization for weight normalization are unclear.
There are few studies on the role of hospitalizationin AN and no randomized controlled trials (RCTs)comparing different in-patient interventions. Resultsfrom uncontrolled studies in adolescents are
* Address for correspondence: Dr S. Madden, Department ofPsychological Medicine, The Sydney Children’s Hospitals Network,Westmead Campus, Locked Bag 4001, Westmead, NSW 2145,Australia.
(Email: [email protected])
Psychological Medicine, Page 1 of 13. © Cambridge University Press 2014doi:10.1017/S0033291714001573
ORIGINAL ARTICLE
The online version of this article is published within an Open Access environment subject to the conditions of the CreativeCommons Attribution licence <http://creativecommons.org/licenses/by/3.0/>.
9/06/2016
3
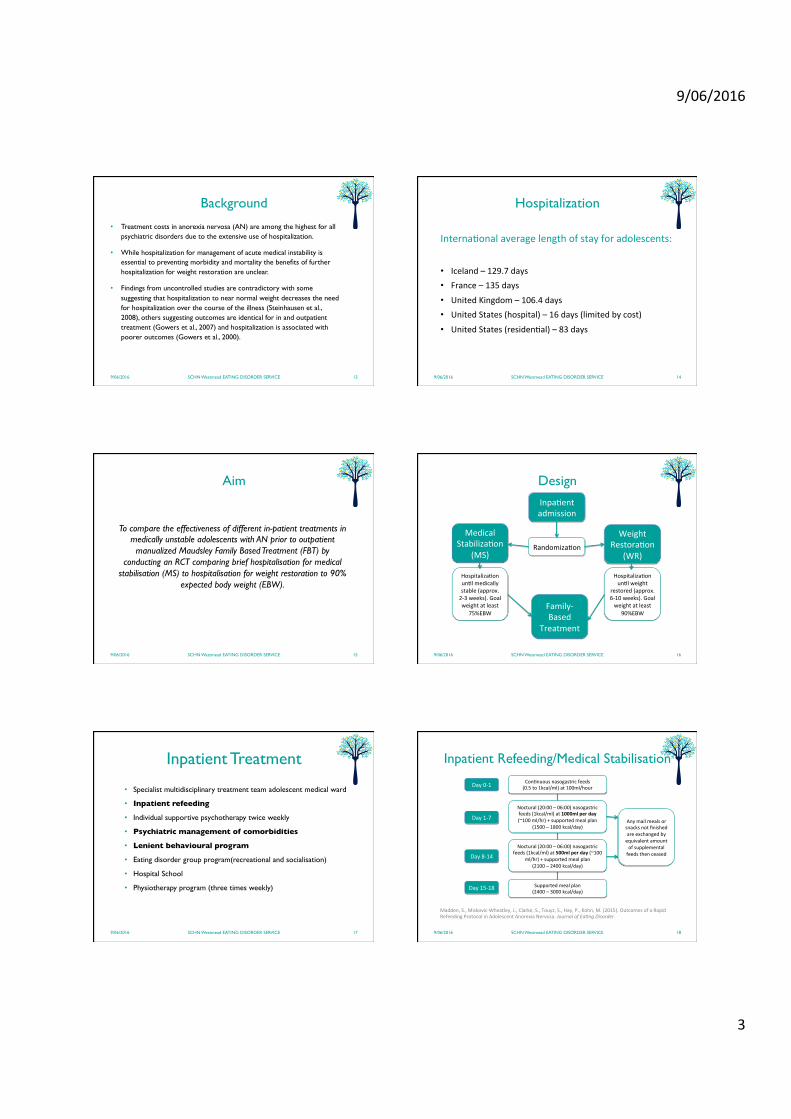
Background
• Treatment costs in anorexia nervosa (AN) are among the highest for all psychiatric disorders due to the extensive use of hospitalization.
• While hospitalization for management of acute medical instability is essential to preventing morbidity and mortality the benefits of further hospitalization for weight restoration are unclear.
• Findings from uncontrolled studies are contradictory with some suggesting that hospitalization to near normal weight decreases the need for hospitalization over the course of the illness (Steinhausen et al., 2008), others suggesting outcomes are identical for in and outpatient treatment (Gowers et al., 2007) and hospitalization is associated with poorer outcomes (Gowers et al., 2000).
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 13
Hospitalization
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 14
Interna2onalaveragelengthofstayforadolescents:• Iceland–129.7days• France–135days• UnitedKingdom–106.4days• UnitedStates(hospital)–16days(limitedbycost)
• UnitedStates(residen2al)–83days
Aim
To compare the effectiveness of different in-patient treatments in medically unstable adolescents with AN prior to outpatient
manualized Maudsley Family Based Treatment (FBT) by conducting an RCT comparing brief hospitalisation for medical
stabilisation (MS) to hospitalisation for weight restoration to 90% expected body weight (EBW).
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 15
Design
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 16
Inpa2entadmission
Randomiza2on
MedicalStabiliza2on
(MS)
WeightRestora2on
(WR)
Hospitaliza2onun2lmedicallystable(approx.2-3weeks).Goalweightatleast
75%EBW
Hospitaliza2onun2lweight
restored(approx.6-10weeks).Goalweightatleast
90%EBWFamily-Based
Treatment
Inpatient Treatment
• Specialist multidisciplinary treatment team adolescent medical ward
• Inpatient refeeding
• Individual supportive psychotherapy twice weekly
• Psychiatric management of comorbidities
• Lenient behavioural program
• Eating disorder group program(recreational and socialisation)
• Hospital School
• Physiotherapy program (three times weekly)
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 17
Inpatient Refeeding/Medical Stabilisation
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 18
Madden,S.,Miskovic-Wheatley,J.,Clarke,S.,Touyz,S.,Hay,P.,Kohn,M.(2015).OutcomesofaRapidRefeedingProtocolinAdolescentAnorexiaNervosa.JournalofEa7ngDisorder.
Con2nuousnasogastricfeeds(0.5to1kcal/ml)at100ml/hour
Supportedmealplan(2400–3000kcal/day)
Anymailmealsorsnacksnotfinishedareexchangedbyequivalentamountofsupplementalfeedsthenceased
Day0-1
Day1-7
Day8-14
Day15-18
Noctural(20:00–06:00)nasogastricfeeds(1kcal/ml)at1000mlperday(~100ml/hr)+supportedmealplan
(1500–1800kcal/day)
Noctural(20:00–06:00)nasogastricfeeds(1kcal/ml)at500mlperday(~100
ml/hr)+supportedmealplan(2100–2400kcal/day)
9/06/2016
4
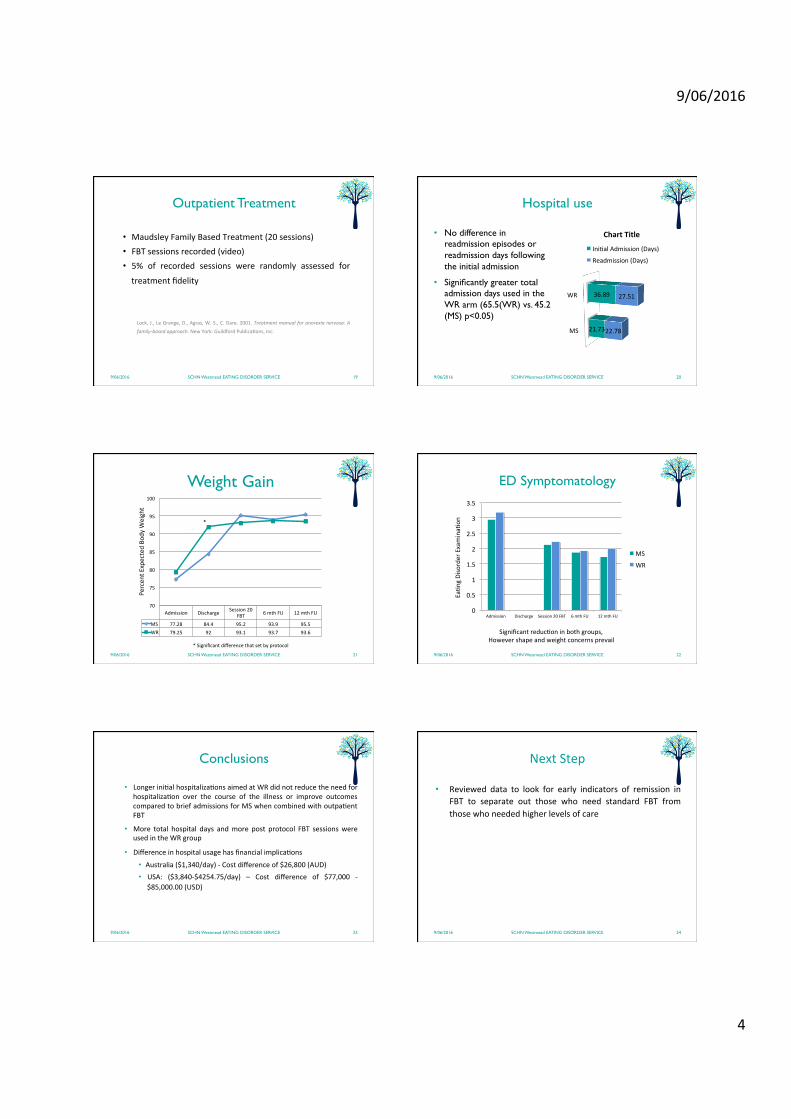
Outpatient Treatment
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 19
• MaudsleyFamilyBasedTreatment(20sessions)• FBTsessionsrecorded(video)• 5% of recorded sessions were randomly assessed for
treatmentfidelity
Lock,J.,LeGrange,D.,Agras,W.S.,C.Dare.2001.Treatmentmanualforanorexianervosa:Afamily-basedapproach.NewYork:GuildfordPublica2ons,Inc.
Hospital use
• No difference in readmission episodes or readmission days following the initial admission
• Significantly greater total admission days used in the WR arm (65.5(WR) vs. 45.2 (MS) p<0.05)
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 20
MS
WR
21.73
36.89
22.78
27.51
ChartTitle
Ini2alAdmission(Days)
Readmission(Days)
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 21
Weight Gain
Admission Discharge Session20FBT 6mthFU 12mthFU
MS 77.28 84.4 95.2 93.9 95.5WR 79.25 92 93.1 93.7 93.6
70
75
80
85
90
95
100
Percen
tExpectedBo
dyW
eight
1
*
*Significantdifferencethatsetbyprotocol
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 22
ED Symptomatology
Ea2n
gDisorderExamina2
on
0
0.5
1
1.5
2
2.5
3
3.5
Admission Discharge Session20FBT 6mthFU 12mthFU
MS
WR
Significantreduc2oninbothgroups,Howevershapeandweightconcernsprevail
Conclusions
• Longerini2alhospitaliza2onsaimedatWRdidnotreducetheneedforhospitaliza2on over the course of the illness or improve outcomescomparedtobriefadmissionsforMSwhencombinedwithoutpa2entFBT
• More total hospital days andmore post protocol FBT sessionswereusedintheWRgroup
• Differenceinhospitalusagehasfinancialimplica2ons
• Australia($1,340/day)-Costdifferenceof$26,800(AUD)• USA: ($3,840-$4254.75/day) – Cost difference of $77,000 -
$85,000.00(USD)
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 23
NextStep
• Reviewed data to look for early indicators of remission inFBT to separate out those who need standard FBT fromthosewhoneededhigherlevelsofcare
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 24
9/06/2016
5
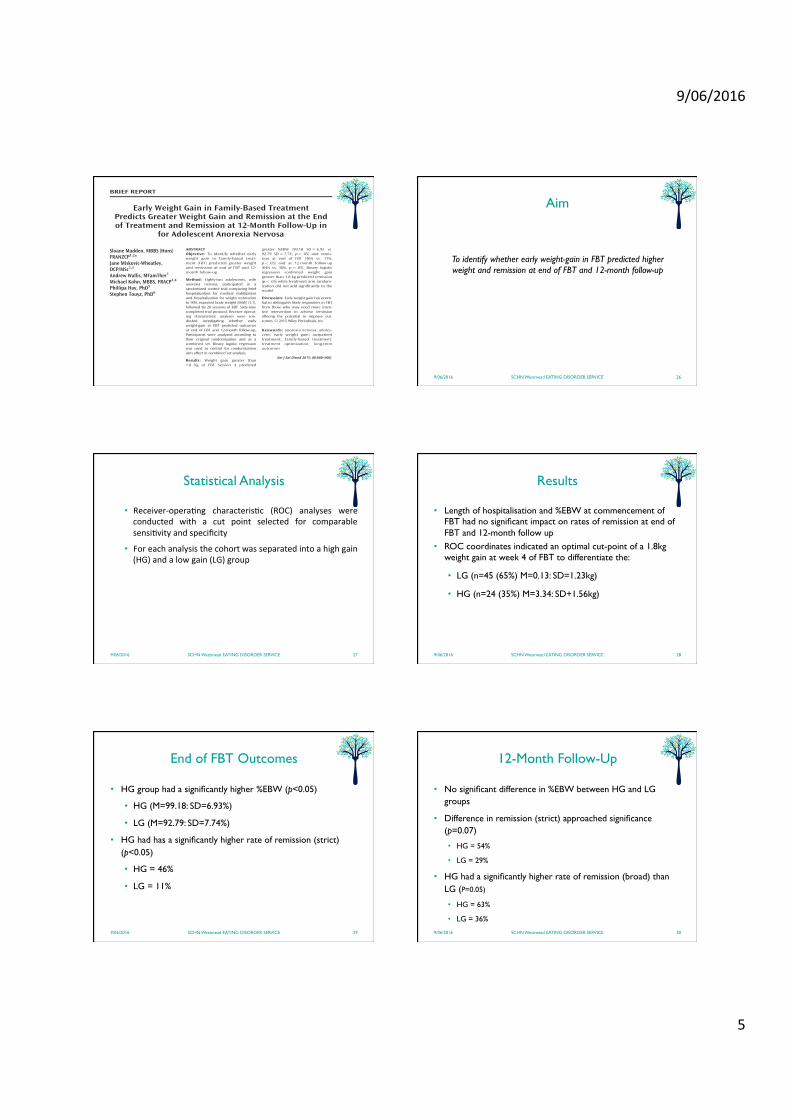
BRIEF REPORT
Early Weight Gain in Family-Based TreatmentPredicts Greater Weight Gain and Remission at the Endof Treatment and Remission at 12-Month Follow-Up in
for Adolescent Anorexia Nervosa
Sloane Madden, MBBS (Hons)FRANZCP1,2*Jane Miskovic-Wheatley,DCP/MSc1,3
Andrew Wallis, MFamTher1
Michael Kohn, MBBS, FRACP1,4
Phillipa Hay, PhD5
Stephen Touyz, PhD6
ABSTRACTObjective: To Identify whether earlyweight gain in family-based treat-ment (FBT) predicted greater weightand remission at end of FBT and 12-month follow-up.
Method: Eighty-two adolescents, withanorexia nervosa, participated in arandomized control trial comparing briefhospitalization for medical stabilizationand hospitalization for weight restorationto 90% expected body weight (EBW) (1:1),followed by 20 sessions of FBT. Sixty-ninecompleted trial protocol. Receiver operat-ing characteristic analyses were con-ducted investigating whether earlyweight-gain in FBT predicted outcomesat end of FBT and 12-month follow-up.Participants were analyzed according totheir original randomization and as acombined set. Binary logistic regressionwas used to control for randomizationarm effect in combined set analysis.
Results: Weight gain greater than1.8 kg at FBT Session 4 predicted
greater %EBW (99.18 SD 5 6.93 vs.92.79 SD 5 7.74, p< .05) and remis-sion at end of FBT (46% vs. 11%,p< .05) and at 12-month follow-up(64% vs. 36%, p 5 .05). Binary logisticregression confirmed weight gaingreater than 1.8 kg predicted remission(p< .05) while treatment arm random-ization did not add significantly to themodel.
Discussion: Early weight gain has poten-tial to distinguish likely responders in FBTfrom those who may need more inten-sive intervention to achieve remissionoffering the potential to improve out-comes. VC 2015 Wiley Periodicals, Inc
Keywords: anorexia nervosa; adoles-cent; early weight gain; outpatienttreatment; family-based treatment;treatment optimization; long-termoutcomes
(Int J Eat Disord 2015; 00:000–000).
Introduction
Eleven randomized controlled trials (RCTs) inadolescent anorexia nervosa (AN) have includedfamily interventions though only the MaudsleyModel of Family-Based Treatment (FBT) hasbeen investigated in multiple RCTs.1 In sevenRCTs, FBT has demonstrated efficacy in adoles-cents, 12–18 years, with AN of less than a 3-yearsduration2 and is regarded as first-line treatmentfor this group.3 Regardless, rates of remissionremain low: 31–49% with a strict definition (per-centage expected body weight (%EBW)>95 andEating Disorder Examination (EDE) Global scorewithin 1S.D. of community norms)2,4 and 67–73%with a broader definition (%EBW>95 and EDEwithin 2S.D. of norm).2,5
A possibility to improve FBT outcomes is earlytreatment response. Differentiating responders fromnon-responders early in FBT allows potential aug-mentations to improve outcomes in those less likely
Accepted 24 March 2015
Conflict of interest: Sloane Madden, Michael Kohn and StephenTouyz have received consultancy fees from Shire Pharmaceuticals.Andrew Wallis receives royalties from IP Communications. Phil-lipa Hay and Stephen Touyz receive royalties from Hogrefe andHuber and McGraw Hill.
Ethical Standards: Sloane Madden (Primary and correspondingauthor) had full access to all of the data in the study and takesresponsibility for the integrity of the data and the accuracy of thedata analysis.
Supported by 457235 from National Health and MedicalResearch Council of Australia (NHMRC).
*Correspondence to: Dr. Sloane Madden, Department of Psycho-logical Medicine, The Sydney Children’s Hospitals Network, West-mead Campus, Locked Bag 4001 Westmead NSW 2145 Australia.E-mail: [email protected]
1 Eating Disorder Service, The Sydney Children’s Hospitals Net-work, Westmead, Australia
2 Discipline of Psychiatry, Faculty of Medicine, The University ofSydney, Australia
3 Westmead Clinical School, The University of Sydney, Australia4 Discipline of Paediatrics, Faculty of Medicine, The University
of Sydney, Australia5 School of Medicine, University of Western Sydney, Australia6 School of Psychology, The University of Sydney, AustraliaPublished online 00 Month 2015 in Wiley Online Library
(wileyonlinelibrary.com). DOI: 10.1002/eat.22414VC 2015 Wiley Periodicals, Inc.
International Journal of Eating Disorders 00:00 00–00 2015 1
Aim
To identify whether early weight-gain in FBT predicted higher weight and remission at end of FBT and 12-month follow-up
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 26
Statistical Analysis
• Receiver-opera2ng characteris2c (ROC) analyses wereconducted with a cut point selected for comparablesensi2vityandspecificity
• Foreachanalysisthecohortwasseparatedintoahighgain(HG)andalowgain(LG)group
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 27
Results
• Length of hospitalisation and %EBW at commencement of FBT had no significant impact on rates of remission at end of FBT and 12-month follow up
• ROC coordinates indicated an optimal cut-point of a 1.8kg weight gain at week 4 of FBT to differentiate the:
• LG (n=45 (65%) M=0.13: SD=1.23kg)
• HG (n=24 (35%) M=3.34: SD+1.56kg)
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 28
End of FBT Outcomes
• HG group had a significantly higher %EBW (p<0.05)
• HG (M=99.18: SD=6.93%)
• LG (M=92.79: SD=7.74%)
• HG had has a significantly higher rate of remission (strict) (p<0.05)
• HG = 46%
• LG = 11%
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 29
12-Month Follow-Up
• No significant difference in %EBW between HG and LG groups
• Difference in remission (strict) approached significance (p=0.07)
• HG = 54%
• LG = 29%
• HG had a significantly higher rate of remission (broad) than LG (P=0.05)
• HG = 63%
• LG = 36%
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 30

9/06/2016
6
Conclusions
• Aweightgainof1.8kgbySession4ofFBTpredictedhigher%EBW and remission (strict) at end of FBT and remission(broad)at12-monthfollow-up.
• Early weight gain as a predictor of remission (strict)approachedsignificance
• Earlyweightgainhasthecapacitytodis2nguishthosewhoare likelytorespondtostandardFBTfromthosewhomaybenefit for increased treatment intensity offering thepoten2altoimprovetreatmentoutcomes
9/06/2016 SCHN Westmead EATING DISORDER SERVICE 31





























