Embed Size (px)
Citation preview

SCHARIOTH MACULA LENSThe Magnifier in The Eye – The New Hope for Patients with Dry AMD
Introduction - Age-Related Macular Degeneration
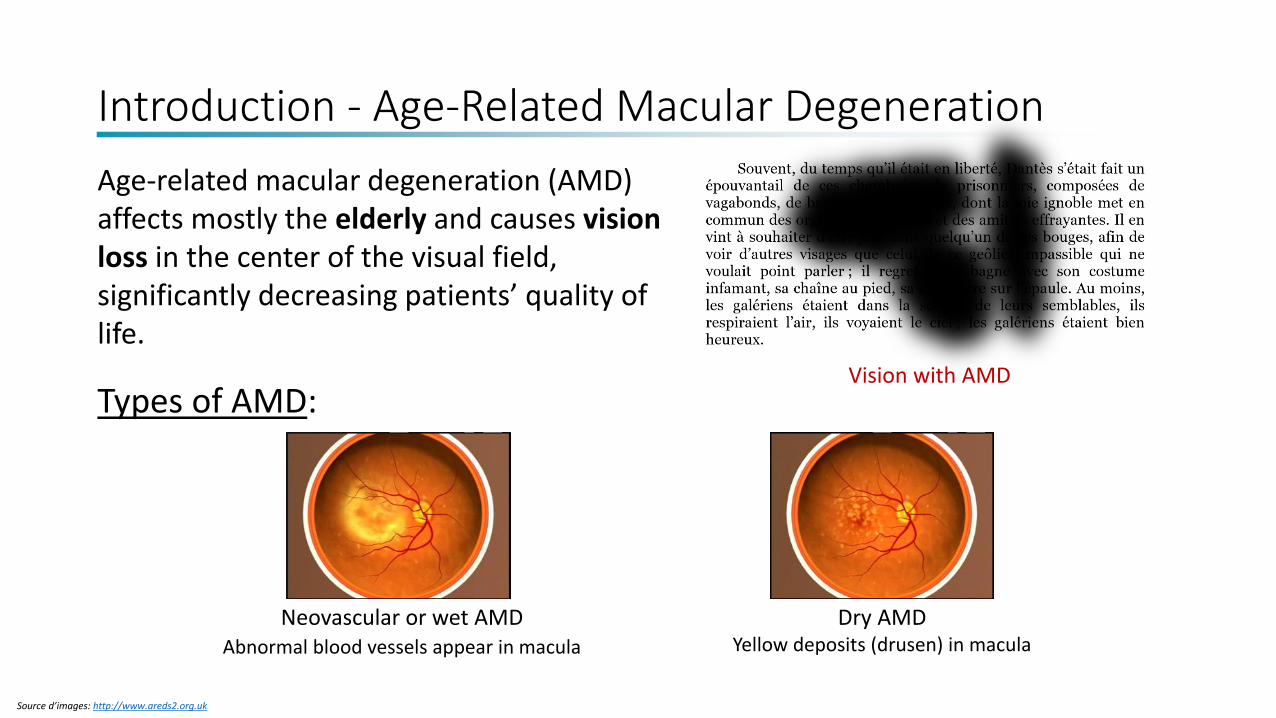
Age-related macular degeneration (AMD) affects mostly the elderly and causes vision loss in the center of the visual field, significantly decreasing patients’ quality of life.
Types of AMD:Healthy visionVision with AMD
Neovascular or wet AMDAbnormal blood vessels appear in macula
Dry AMDYellow deposits (drusen) in macula
Source d’images: http://www.areds2.org.uk
Introduction - Age-Related Macular Degeneration
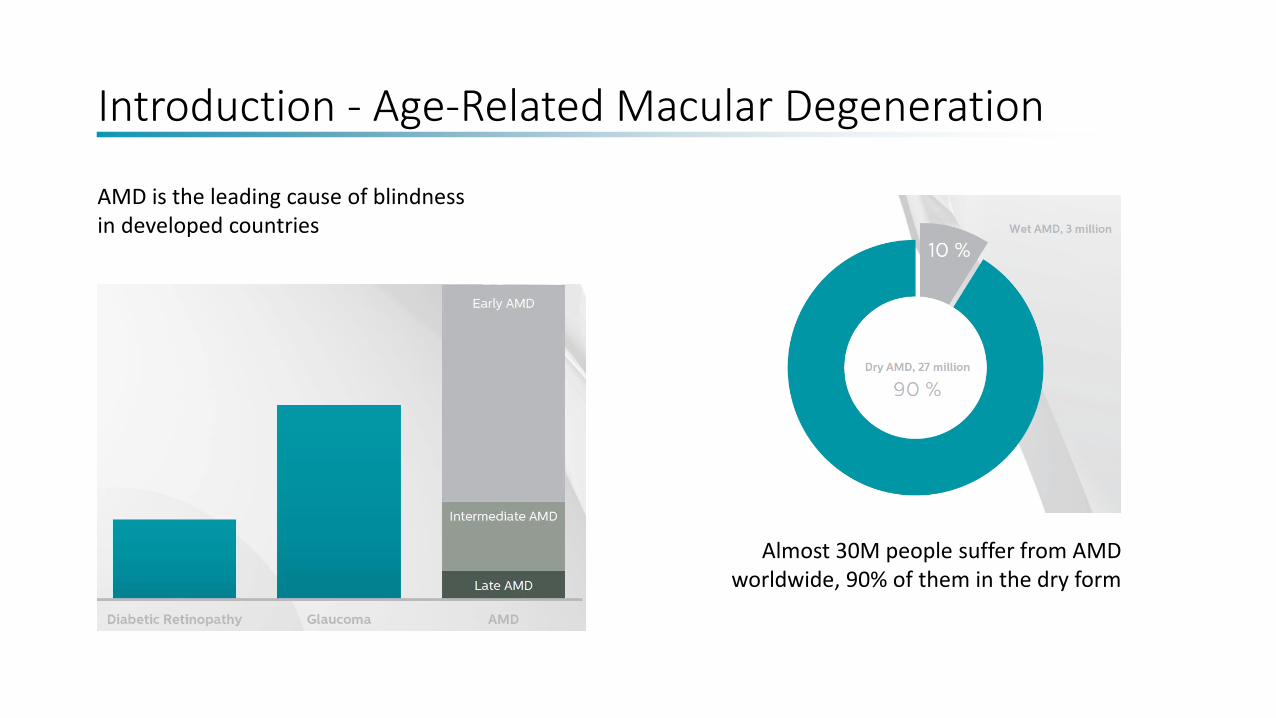
AMD is the leading cause of blindness in developed countries
Almost 30M people suffer from AMD worldwide, 90% of them in the dry form
Introduction - Age-Related Macular Degeneration
HUGE MARKET
Treatment Options
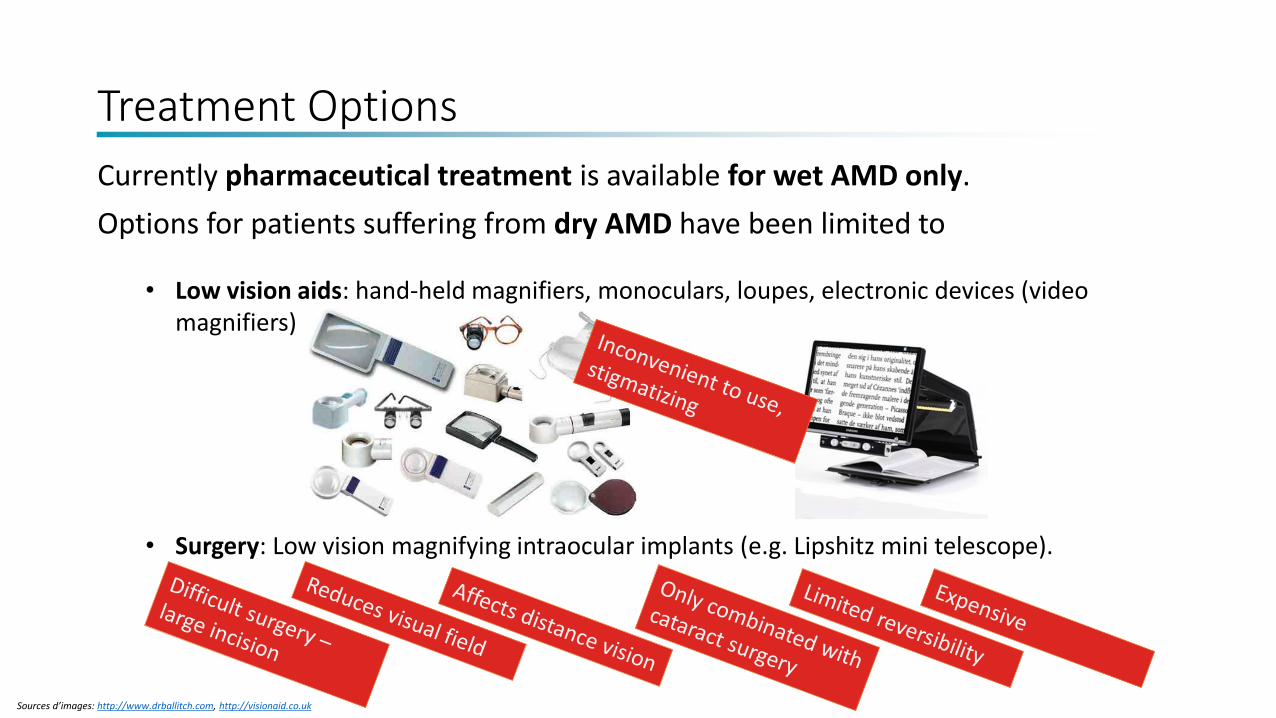
Currently pharmaceutical treatment is available for wet AMD only.
Options for patients suffering from dry AMD have been limited to
• Low vision aids: hand-held magnifiers, monoculars, loupes, electronic devices (video magnifiers)
• Surgery: Low vision magnifying intraocular implants (e.g. Lipshitz mini telescope).
Sources d’images: http://www.drballitch.com, http://visionaid.co.uk
The New Hope – The Scharioth Macula Lens
• Easy and safe surgery
• Small incision
• No visual field reduction
• Unaffected distance vision
• Independent from lens status
• Reversible
• Affordable
Goals for developing a novel solution:The Scharioth Macula Lens
A45SML/A45SMYfrom Medicontur
Developed by Prof. Gabor B. Scharioth
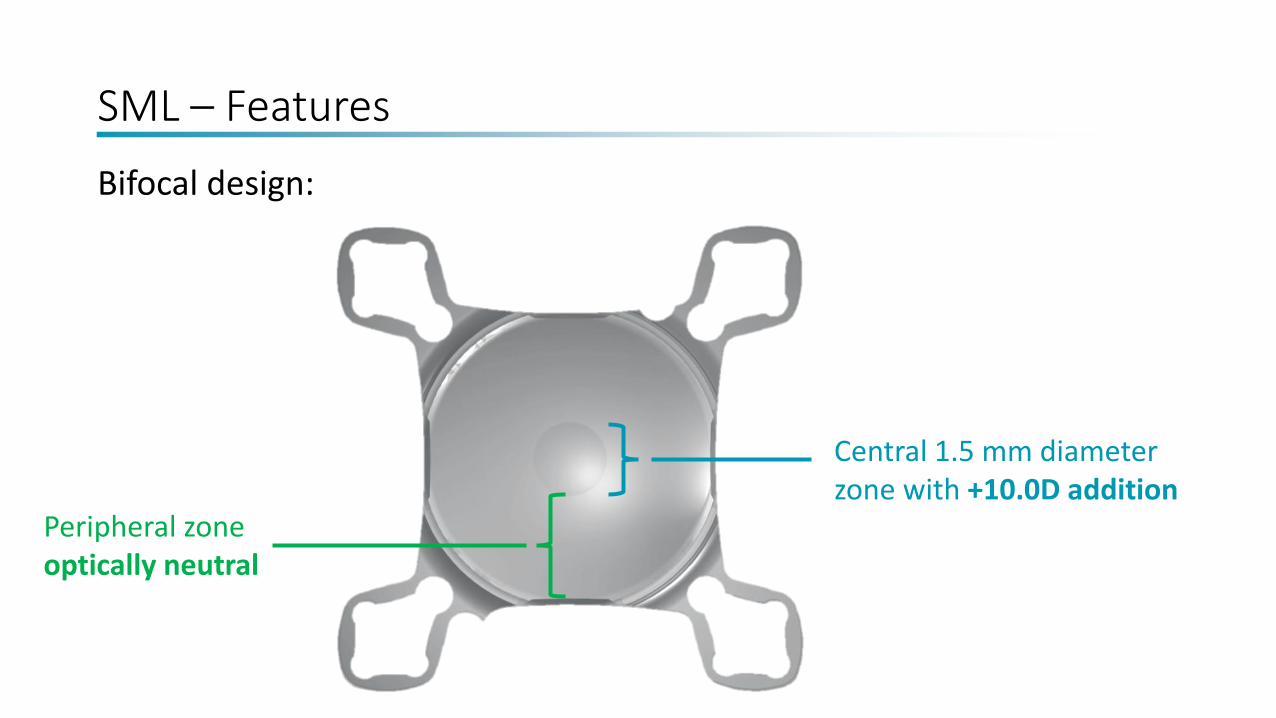
SML – Features
Central 1.5 mm diameter zone with +10.0D addition
Peripheral zone optically neutral
Bifocal design:
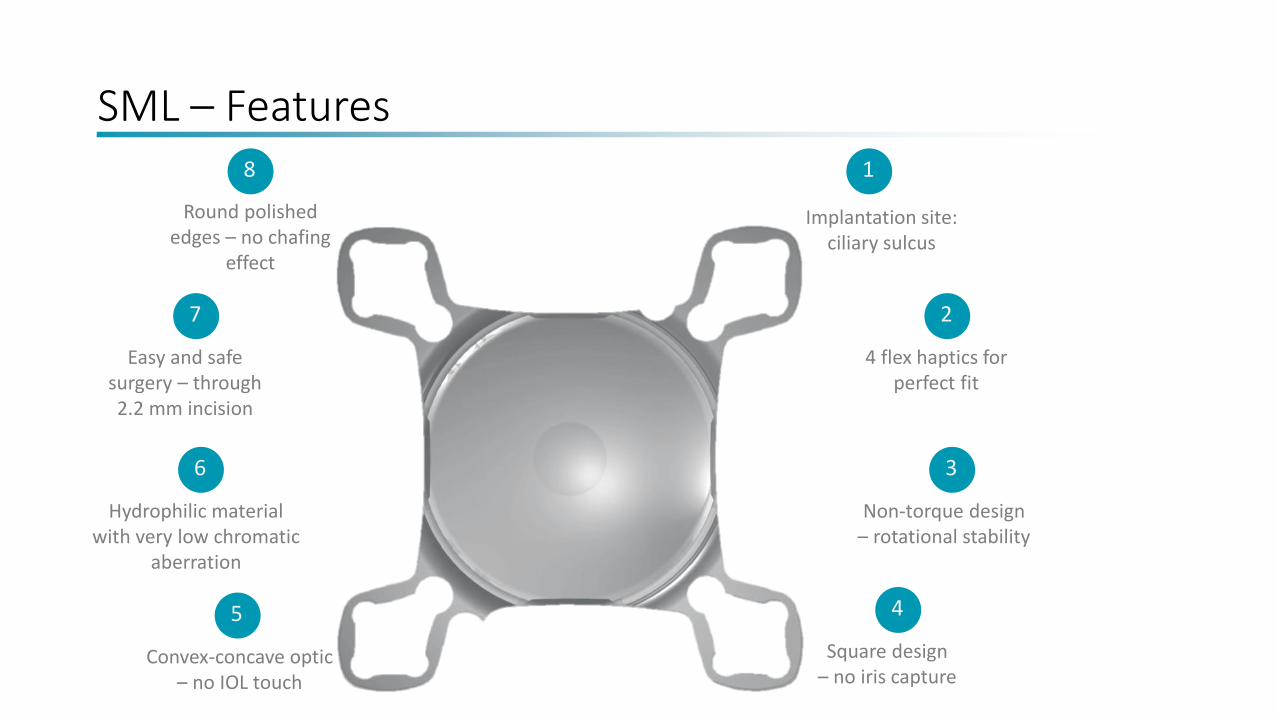
SML – Features
Round polished edges – no chafing
effect
8 1
Implantation site: ciliary sulcus
2
4 flex haptics for perfect fit
3
Non-torque design – rotational stability
4
Square design – no iris capture
7
Easy and safe surgery – through 2.2 mm incision
6
Hydrophilic material with very low chromatic
aberration
5
Convex-concave optic – no IOL touch
SML is safe
Proofs:
• implanted more than 3.000 patented Add-On platform
• In vitro evaluation of the lens
SML – Mode of Action
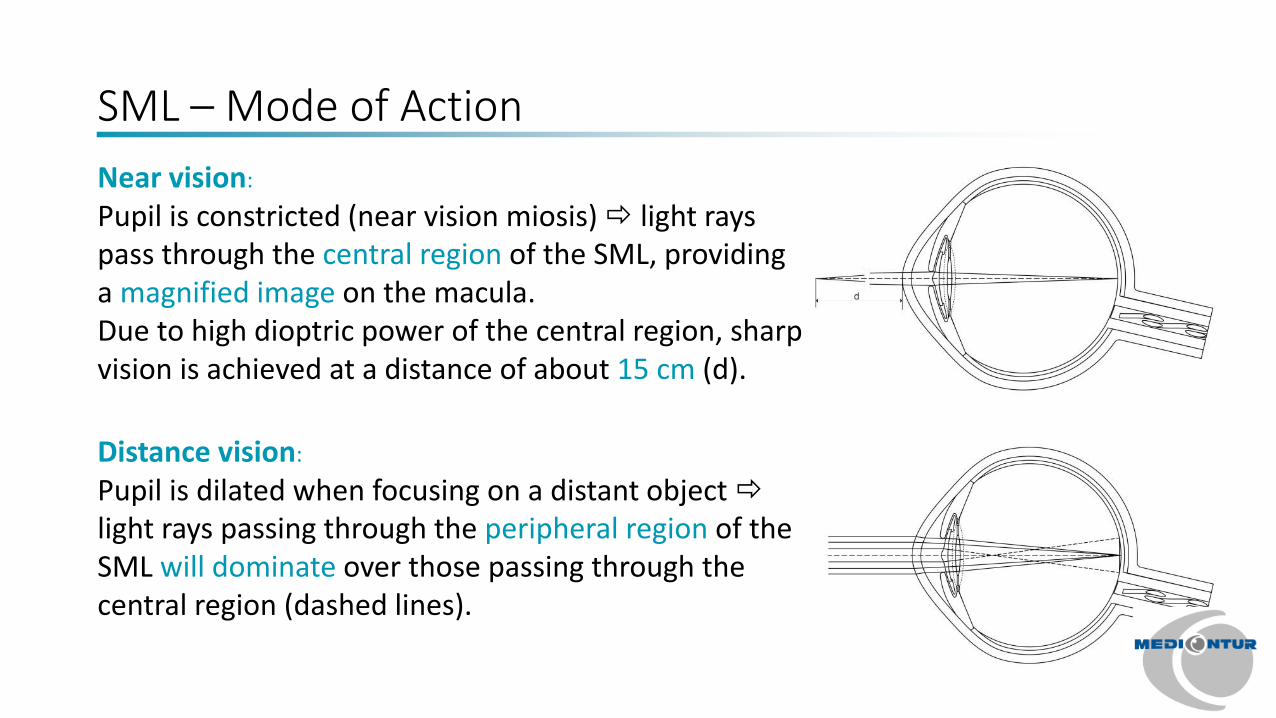
Near vision:
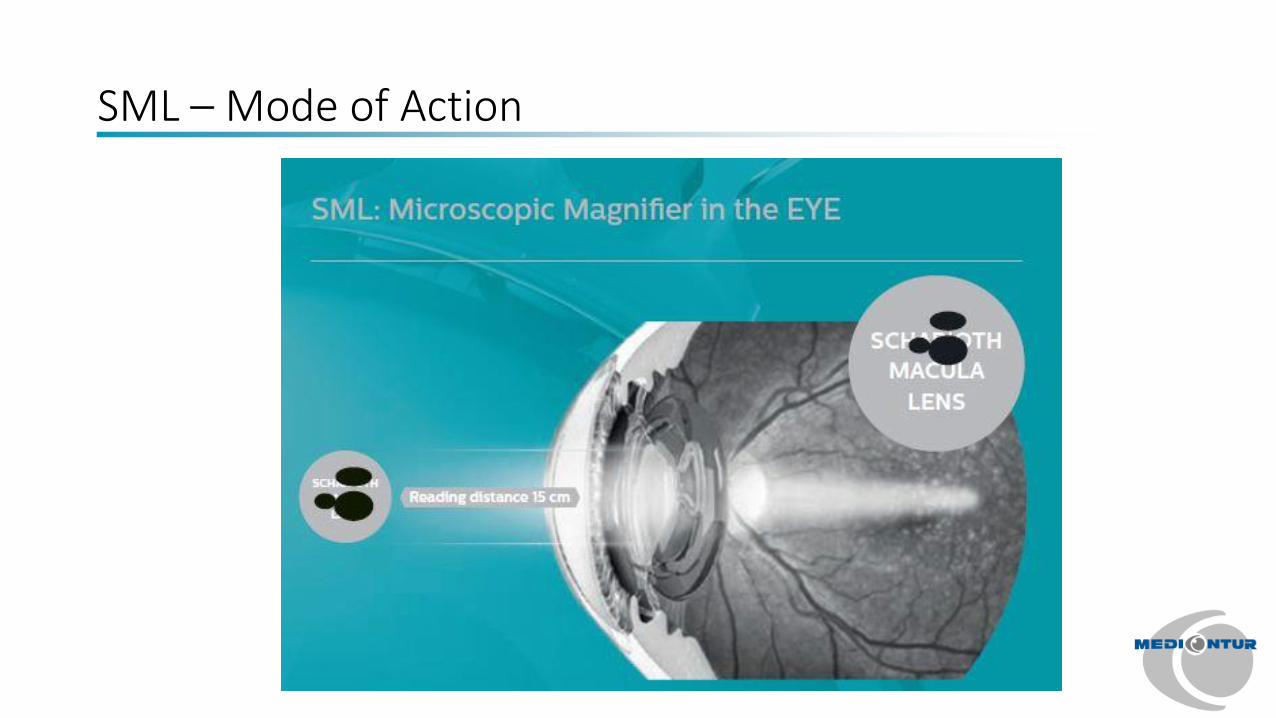
Pupil is constricted (near vision miosis) light rays pass through the central region of the SML, providing a magnified image on the macula. Due to high dioptric power of the central region, sharp vision is achieved at a distance of about 15 cm (d).
Distance vision:
Pupil is dilated when focusing on a distant object light rays passing through the peripheral region of the SML will dominate over those passing through the central region (dashed lines).
SML – Mode of Action
SML – Mode of Action
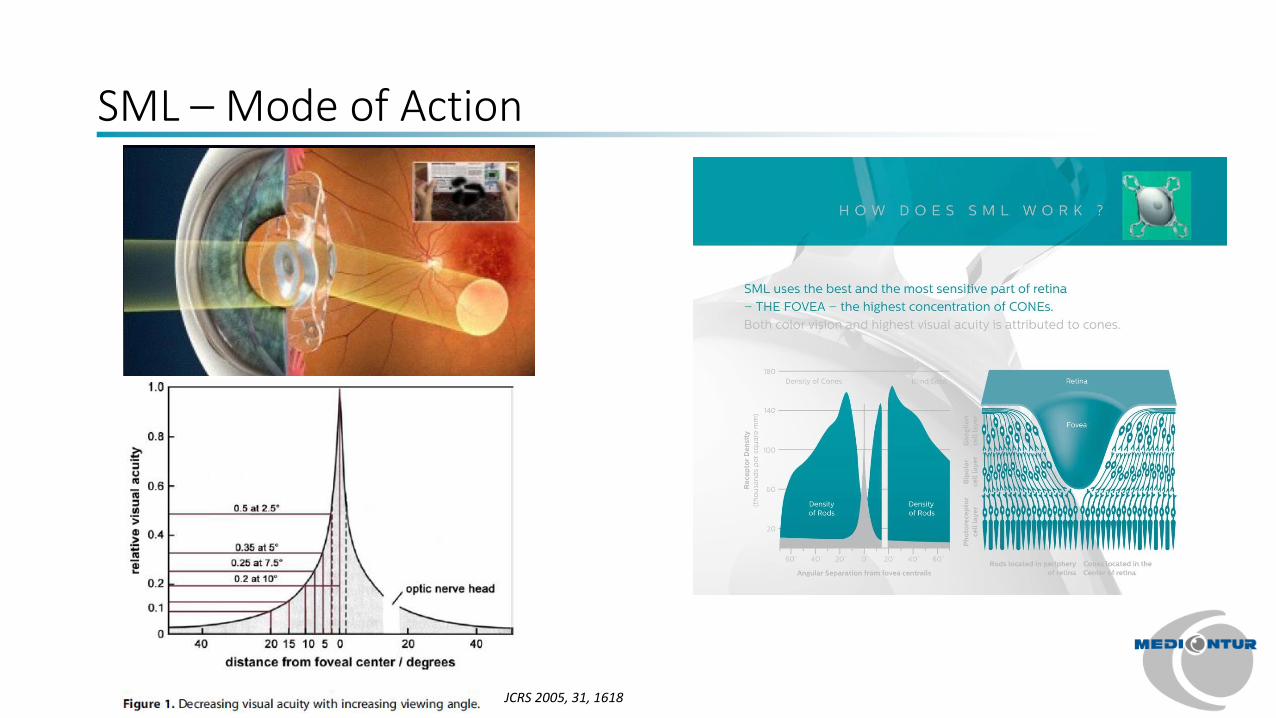
JCRS 2005, 31, 1618
SML – Mode of Action
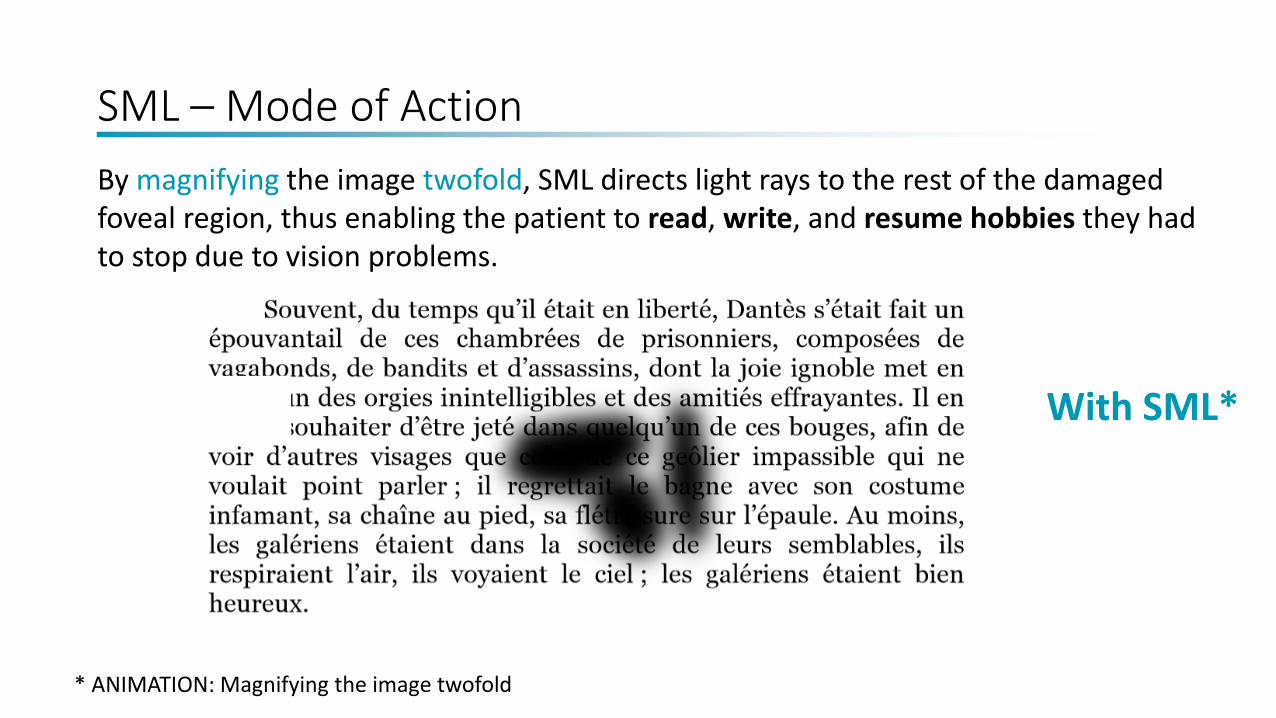
By magnifying the image twofold, SML directs light rays to the rest of the damaged foveal region, thus enabling the patient to read, write, and resume hobbies they had to stop due to vision problems.
Without SML With SML*
* ANIMATION: Magnifying the image twofold
SML – Implantation
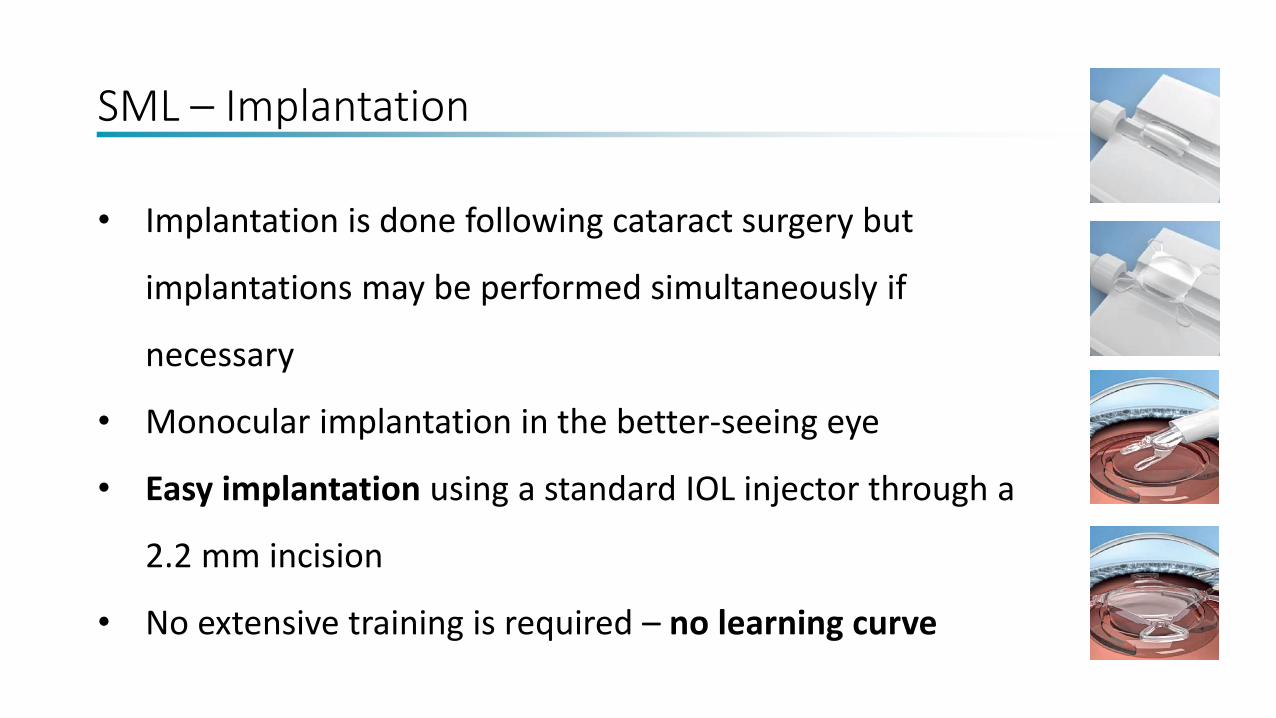
• Implantation is done following cataract surgery but
implantations may be performed simultaneously if
necessary
• Monocular implantation in the better-seeing eye
• Easy implantation using a standard IOL injector through a
2.2 mm incision
• No extensive training is required – no learning curve
SML – Clinical Evidence
• Prospective study; follow up 6 months
• 8 patients/8 eyes
• Distance VA was NOT AFFECTED
• NVA improved in 7 eyes
• One patient out of 7 did not have any
improvement of NVA due to very low BCDVA before
surgery (0.05 ETDRS)
• Most patients were able to read newspaper
• There were not any complications related to
surgery or to the implant occurring during
follow up period
• Overall satisfied patients
Scharioth GB: New add-on intraocular lens for patients with age related macular degeneration. JCRS;41:1559-1563
SML – Clinical Evidence
SML – Indications
• Who have dry AMD and have near vision difficulties
• Who suffer from other retinal conditions (diabetic retinopathy, myopic
retinopathy, hereditary retinal diseases)
• Whose distance vision is better than 0.05 (ETDRS, decimal)
• Who are motivated
• Who are pseudophakic or are candidates for cataract surgery
The Scharioth Macula Lens is recommended for patients
SML – Contraindications
• Wet AMD (active/exudative stage)
• Zonulopathy
• Subluxation
• Progressive glaucoma
• Active iris neovascularization
• Shallow ACD (<2.8; pseudophakic)
• Aphakia
The Scharioth Macula Lens is contraindicated in the following cases:
SML in Use
Better quality of life Happy patient
Patient with vision aid Patient with SML
HOW TO CHOSE A PROPER PATIENT?
• KEY: MOTIVATION & COMMUNICATION WITH THE PATIENT
• implanted should be better seeing eye of the patient
• Pseudophakic patients and with dry form AMD or maculopathy or inactive neovascular AMD/othre maculopythy• interval between cataract surgery and the SML implantation has to be equal or bigger than 1 months• In case of clear lens crystalline in some cases might be both surgeries performed in one session
• BCDVA • equal or less than 0.32 • and equal or more than 0.1 (decimal ETDRS charts)
• Preoperative NVA acuity will be examined as follows: Patients will read from distance about 40 cm with the addition of +2.5 dpt(examination A) and from distance about 15 cm with the addition of +6 dpt (examination B). Only if there will be an improvement; the best 3 or more lines with the examination B compare to examination A; BUT if 1 or 2 lines improved and patients is happy with it –the SML is indicated
• IMPORTANT: based on below explained test, we can PREDICT patient NVA after the SML implantation – important for communication and for patients understanding about the probable vision after surgery
EXCLUSION CRITERIA:
• Active neovascular AMD/maculopathy
• BCDVA worse than 0.1 or better than 0.32 (ETDRS charts; decimal)
• iris neovascularisation
• severe zonulopathy
• ACD < 2.8 mm (from endotel)
• Narrow angle, i.e., < Schaefer grade 2
• Status post complicated eye surgery
• congenital eye abnormality
• advanced glaucoma with significant visual field defects
• pigment dispersion syndrome
• uveitis
• long-term anti-inflammatory treatment
• retinal detachment
• corneal diseases involving the central cornea
• inadequate visualization of the fundus on preoperative examination
• patients deemed by the clinical investigator because of any systemic disease.
• Pupilary abnormalities; photopic pupil less than 2.5 mm
• no-go criteria :
• unexpected surgical complication

SML CompetitorsMarket overview
Telescopic solution
• IOL-VIP
• IOL-Revolution
• IOL-Foldable
• IOL-K
• 9G-X2
• Lipshitz telescope
The SchariothMacula Lens
Real Competitors
• iolAMD
• iolAMD EyeMax
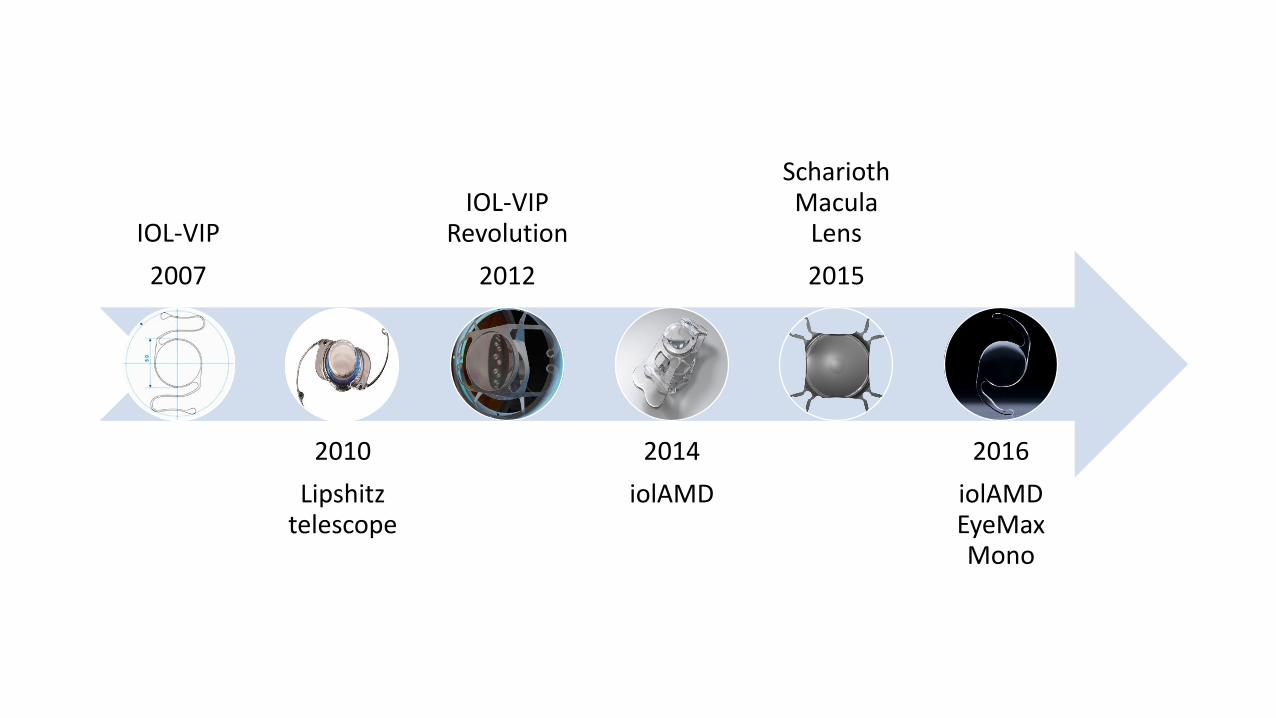
IOL-VIP
2007
2010
Lipshitztelescope
IOL-VIP Revolution
2012
2014
iolAMD
SchariothMacula
Lens
2015
2016
iolAMDEyeMaxMono
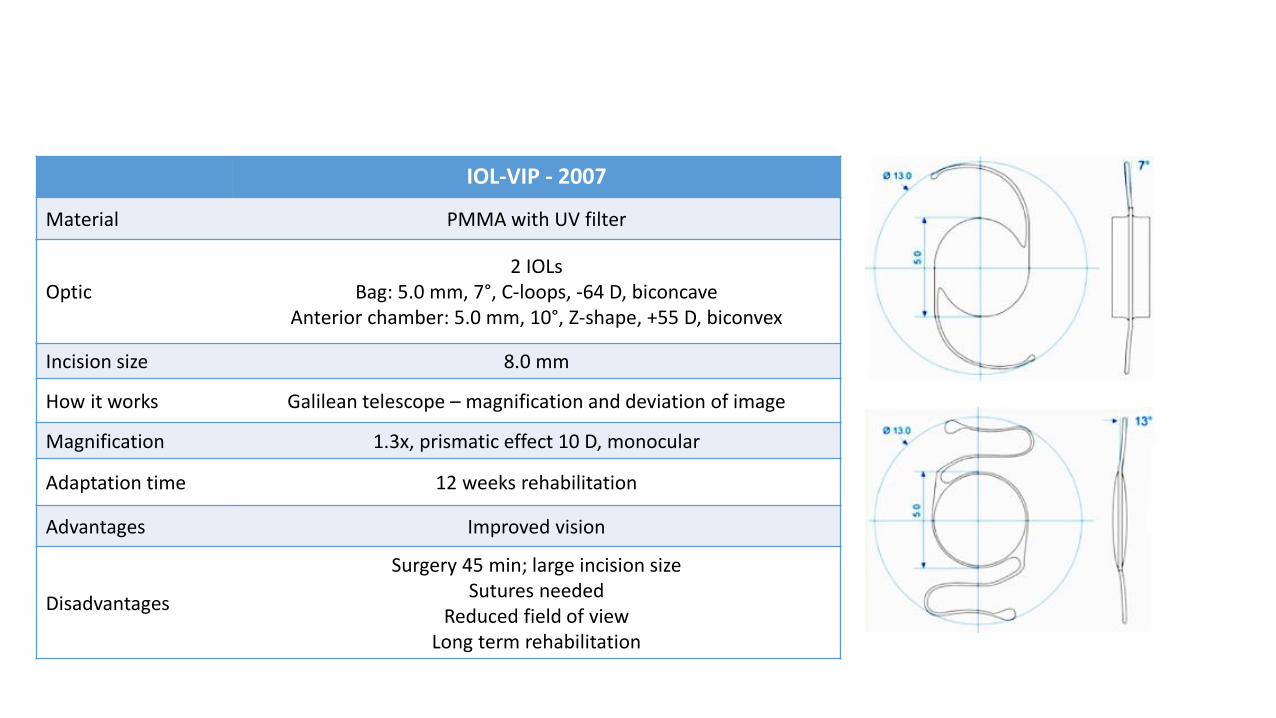
IOL-VIP - 2007
Material PMMA with UV filter
Optic2 IOLs
Bag: 5.0 mm, 7°, C-loops, -64 D, biconcaveAnterior chamber: 5.0 mm, 10°, Z-shape, +55 D, biconvex
Incision size 8.0 mm
How it works Galilean telescope – magnification and deviation of image
Magnification 1.3x, prismatic effect 10 D, monocular
Adaptation time 12 weeks rehabilitation
Advantages Improved vision
Disadvantages
Surgery 45 min; large incision sizeSutures needed
Reduced field of viewLong term rehabilitation
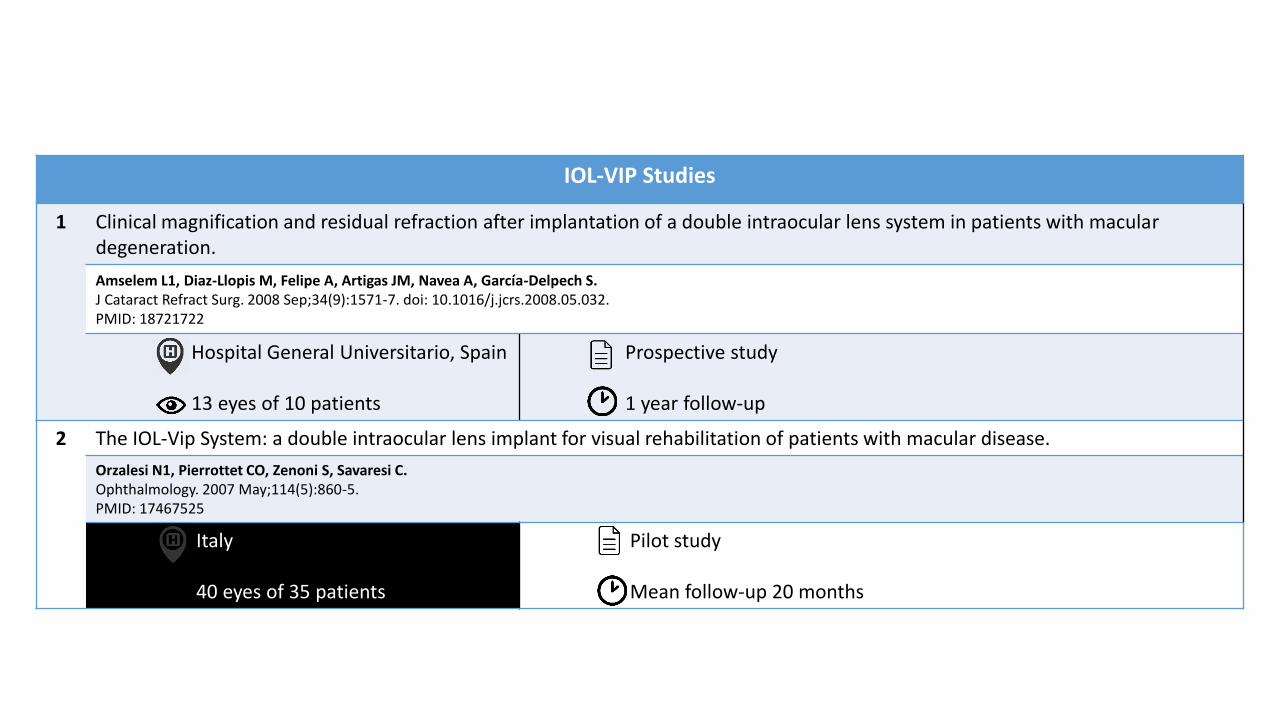
IOL-VIP Studies
1 Clinical magnification and residual refraction after implantation of a double intraocular lens system in patients with macular degeneration.
Amselem L1, Diaz-Llopis M, Felipe A, Artigas JM, Navea A, García-Delpech S.J Cataract Refract Surg. 2008 Sep;34(9):1571-7. doi: 10.1016/j.jcrs.2008.05.032.PMID: 18721722
Hospital General Universitario, Spain
13 eyes of 10 patients
Prospective study
1 year follow-up
2 The IOL-Vip System: a double intraocular lens implant for visual rehabilitation of patients with macular disease.
Orzalesi N1, Pierrottet CO, Zenoni S, Savaresi C.Ophthalmology. 2007 May;114(5):860-5.PMID: 17467525
Italy
40 eyes of 35 patients
Pilot study
Mean follow-up 20 months
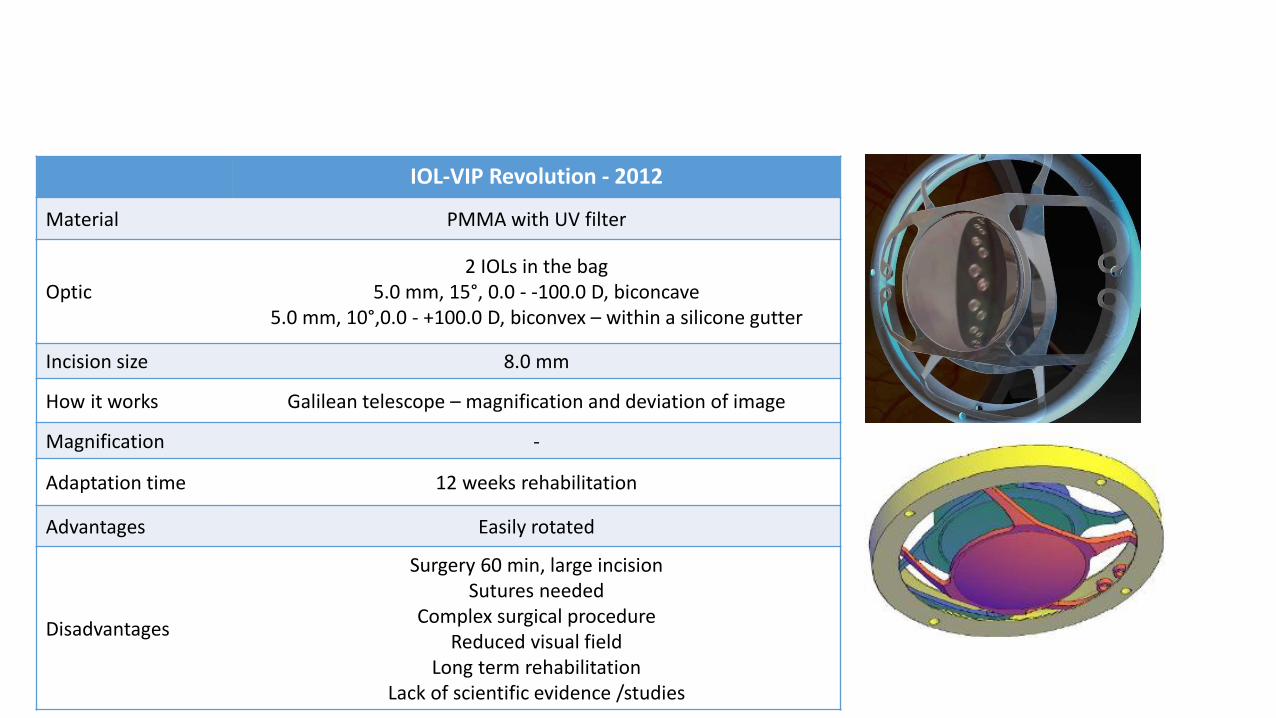
IOL-VIP Revolution - 2012
Material PMMA with UV filter
Optic2 IOLs in the bag
5.0 mm, 15°, 0.0 - -100.0 D, biconcave5.0 mm, 10°,0.0 - +100.0 D, biconvex – within a silicone gutter
Incision size 8.0 mm
How it works Galilean telescope – magnification and deviation of image
Magnification -
Adaptation time 12 weeks rehabilitation
Advantages Easily rotated
Disadvantages
Surgery 60 min, large incisionSutures needed
Complex surgical procedure Reduced visual field
Long term rehabilitationLack of scientific evidence /studies
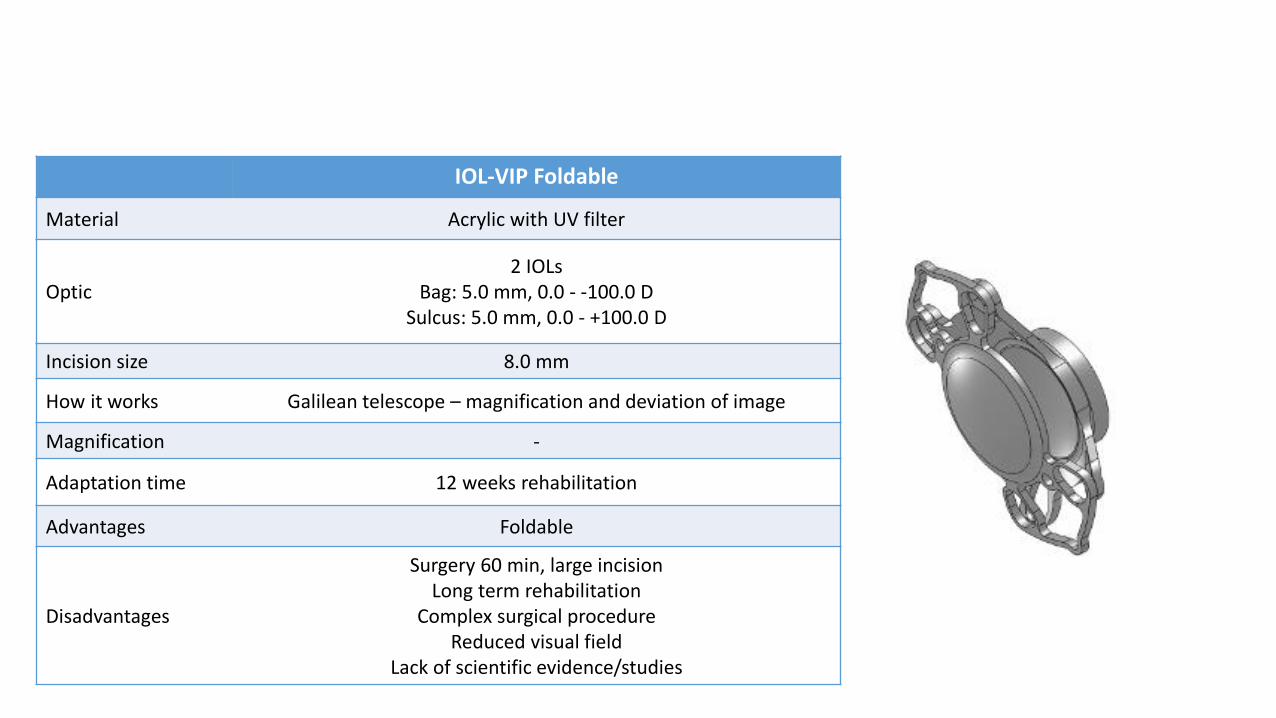
IOL-VIP Foldable
Material Acrylic with UV filter
Optic2 IOLs
Bag: 5.0 mm, 0.0 - -100.0 D Sulcus: 5.0 mm, 0.0 - +100.0 D
Incision size 8.0 mm
How it works Galilean telescope – magnification and deviation of image
Magnification -
Adaptation time 12 weeks rehabilitation
Advantages Foldable
Disadvantages
Surgery 60 min, large incisionLong term rehabilitation
Complex surgical procedure Reduced visual field
Lack of scientific evidence/studies
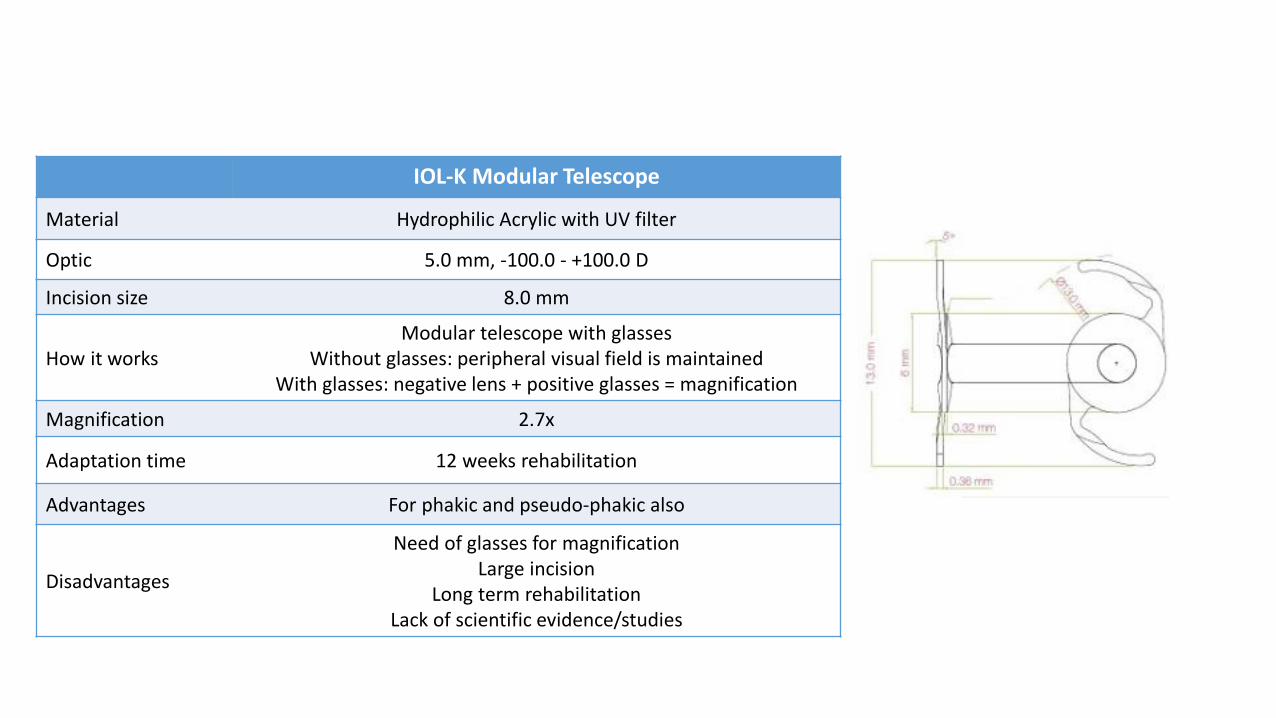
IOL-K Modular Telescope
Material Hydrophilic Acrylic with UV filter
Optic 5.0 mm, -100.0 - +100.0 D
Incision size 8.0 mm
How it worksModular telescope with glasses
Without glasses: peripheral visual field is maintainedWith glasses: negative lens + positive glasses = magnification
Magnification 2.7x
Adaptation time 12 weeks rehabilitation
Advantages For phakic and pseudo-phakic also
Disadvantages
Need of glasses for magnificationLarge incision
Long term rehabilitationLack of scientific evidence/studies
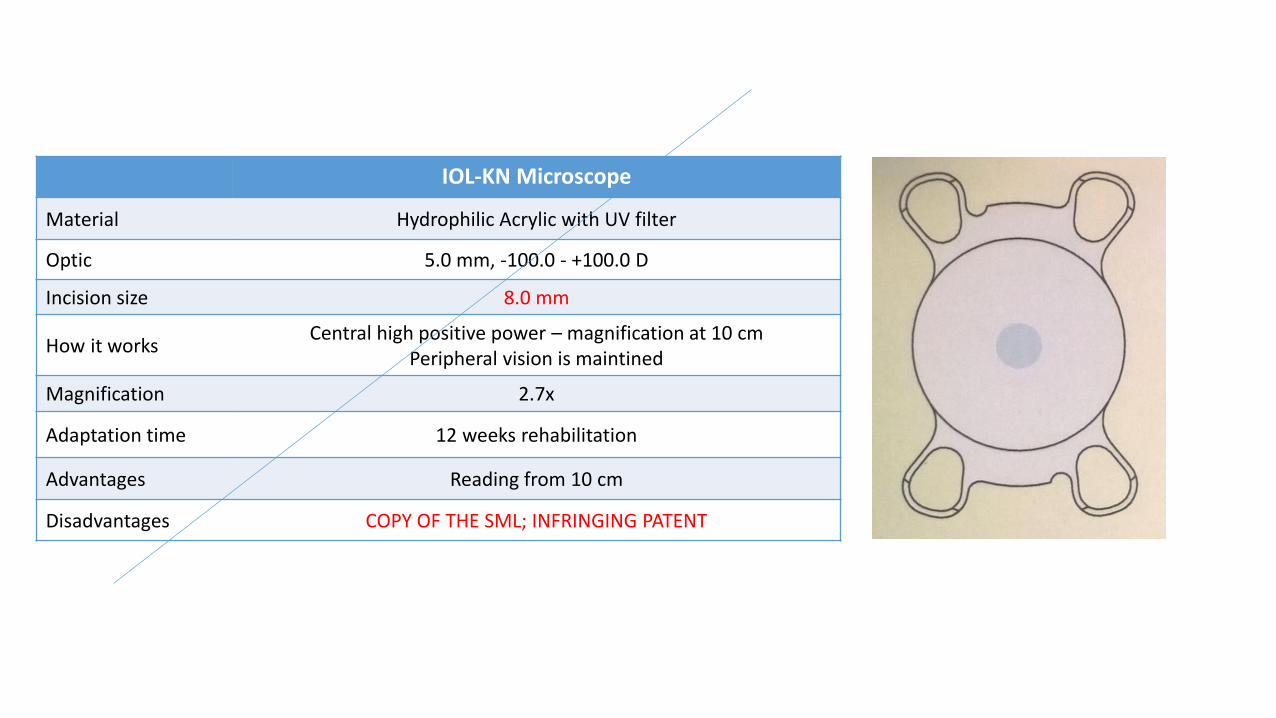
IOL-KN Microscope
Material Hydrophilic Acrylic with UV filter
Optic 5.0 mm, -100.0 - +100.0 D
Incision size 8.0 mm
How it worksCentral high positive power – magnification at 10 cm
Peripheral vision is maintined
Magnification 2.7x
Adaptation time 12 weeks rehabilitation
Advantages Reading from 10 cm
Disadvantages COPY OF THE SML; INFRINGING PATENT
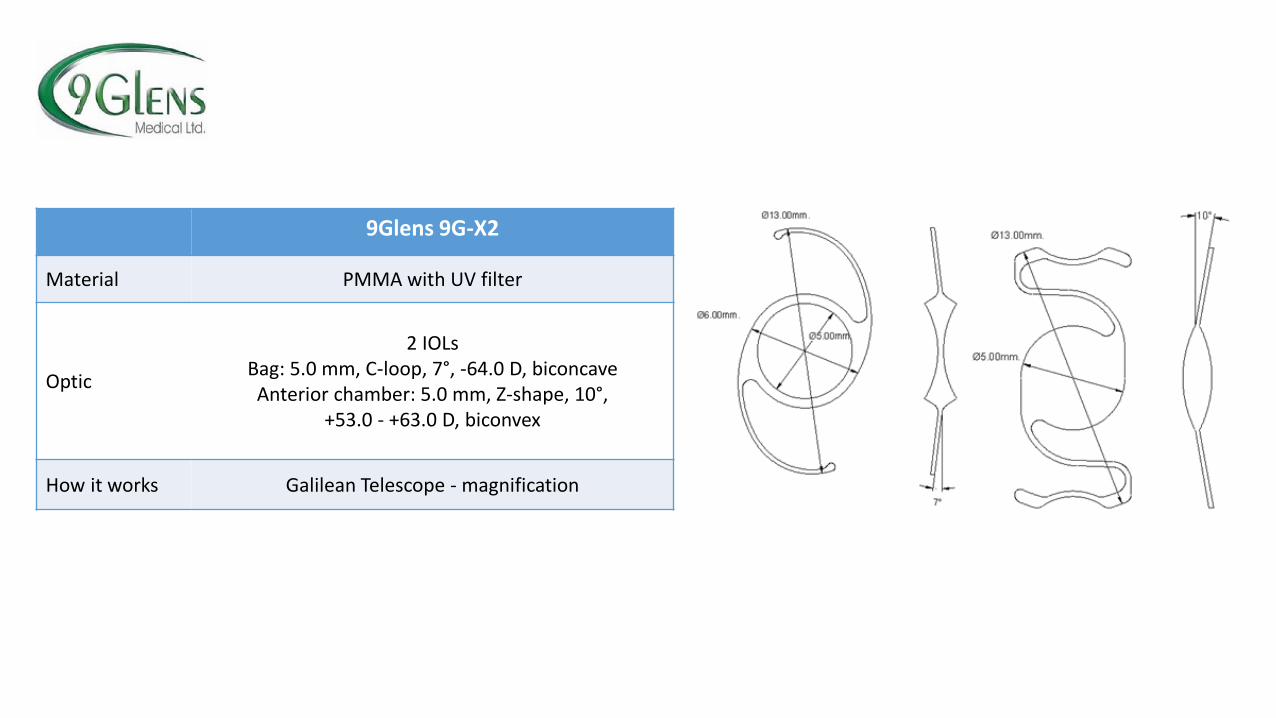
9Glens 9G-X2
Material PMMA with UV filter
Optic
2 IOLsBag: 5.0 mm, C-loop, 7°, -64.0 D, biconcaveAnterior chamber: 5.0 mm, Z-shape, 10°,
+53.0 - +63.0 D, biconvex
How it works Galilean Telescope - magnification
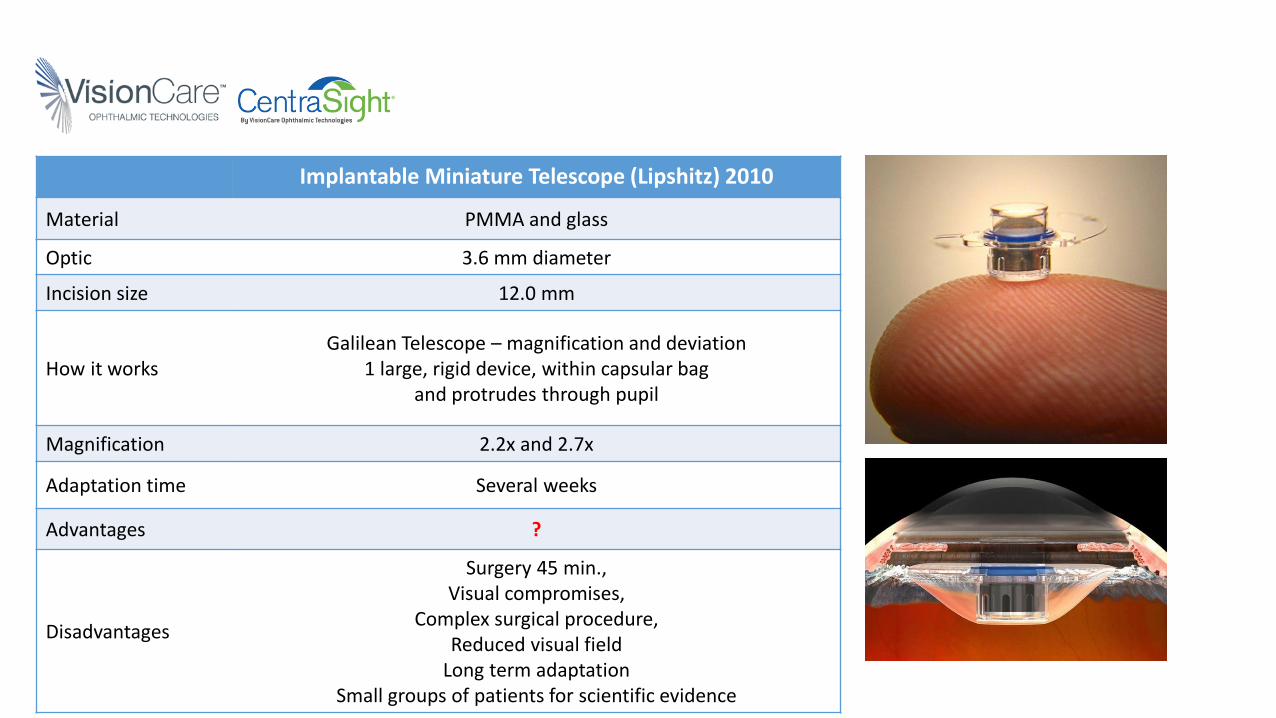
Implantable Miniature Telescope (Lipshitz) 2010
Material PMMA and glass
Optic 3.6 mm diameter
Incision size 12.0 mm
How it worksGalilean Telescope – magnification and deviation
1 large, rigid device, within capsular bagand protrudes through pupil
Magnification 2.2x and 2.7x
Adaptation time Several weeks
Advantages ?
Disadvantages
Surgery 45 min., Visual compromises,
Complex surgical procedure, Reduced visual field
Long term adaptationSmall groups of patients for scientific evidence
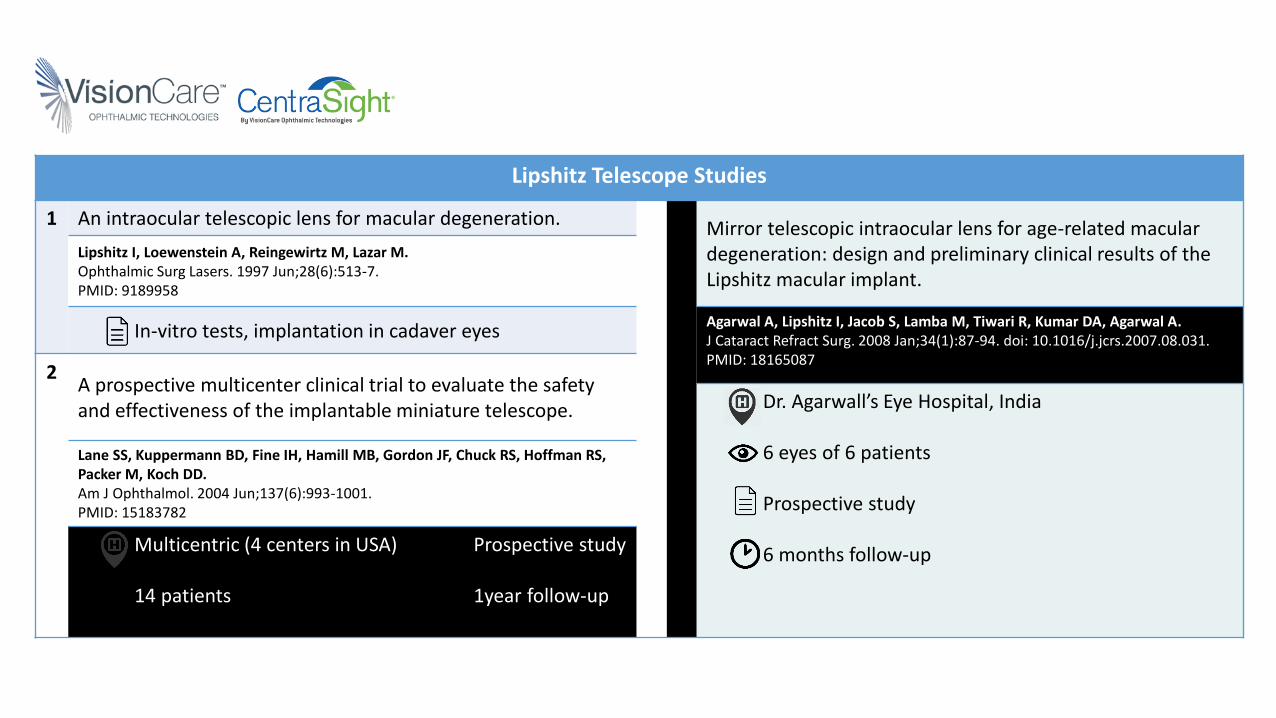
Lipshitz Telescope Studies
1 An intraocular telescopic lens for macular degeneration. 3 Mirror telescopic intraocular lens for age-related macular degeneration: design and preliminary clinical results of the Lipshitz macular implant.
Lipshitz I, Loewenstein A, Reingewirtz M, Lazar M.Ophthalmic Surg Lasers. 1997 Jun;28(6):513-7.PMID: 9189958
In-vitro tests, implantation in cadaver eyesAgarwal A, Lipshitz I, Jacob S, Lamba M, Tiwari R, Kumar DA, Agarwal A.J Cataract Refract Surg. 2008 Jan;34(1):87-94. doi: 10.1016/j.jcrs.2007.08.031.PMID: 18165087
2A prospective multicenter clinical trial to evaluate the safety and effectiveness of the implantable miniature telescope. Dr. Agarwall’s Eye Hospital, India
6 eyes of 6 patients
Prospective study
6 months follow-up
Lane SS, Kuppermann BD, Fine IH, Hamill MB, Gordon JF, Chuck RS, Hoffman RS, Packer M, Koch DD.Am J Ophthalmol. 2004 Jun;137(6):993-1001.PMID: 15183782
Multicentric (4 centers in USA) Prospective study
14 patients 1year follow-up
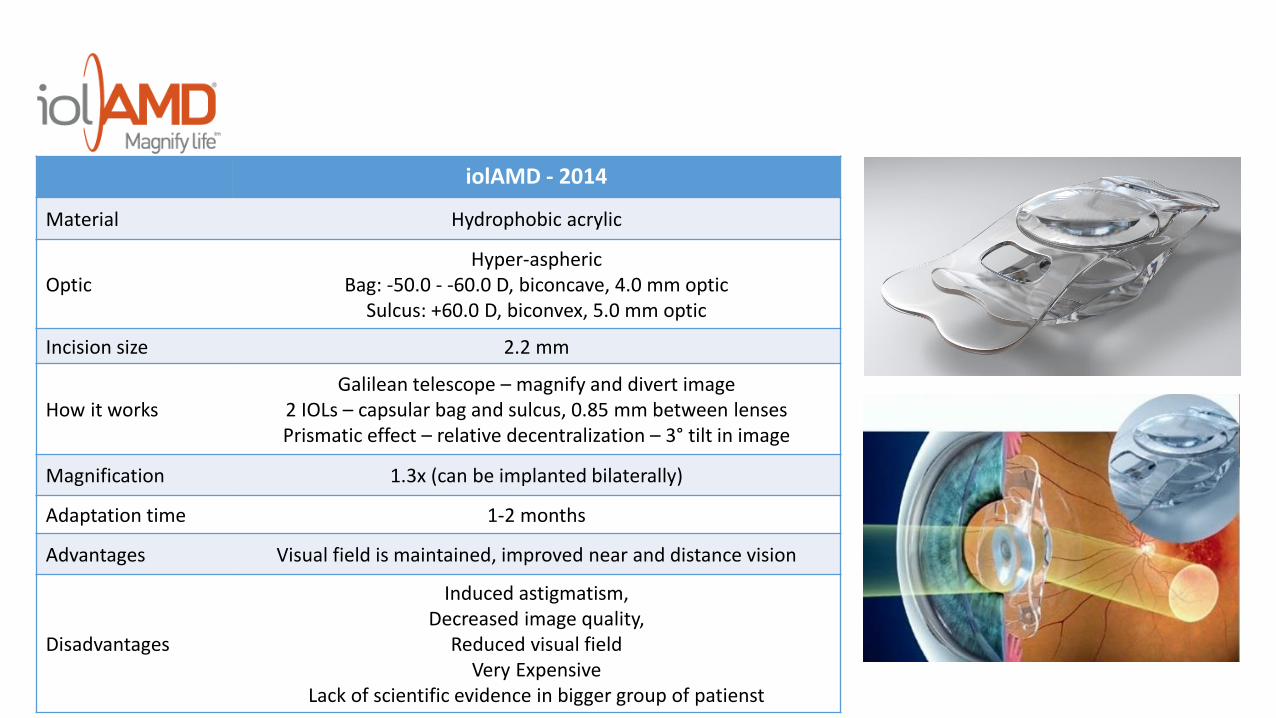
iolAMD - 2014
Material Hydrophobic acrylic
OpticHyper-aspheric
Bag: -50.0 - -60.0 D, biconcave, 4.0 mm opticSulcus: +60.0 D, biconvex, 5.0 mm optic
Incision size 2.2 mm
How it worksGalilean telescope – magnify and divert image
2 IOLs – capsular bag and sulcus, 0.85 mm between lensesPrismatic effect – relative decentralization – 3° tilt in image
Magnification 1.3x (can be implanted bilaterally)
Adaptation time 1-2 months
Advantages Visual field is maintained, improved near and distance vision
Disadvantages
Induced astigmatism, Decreased image quality,
Reduced visual fieldVery Expensive
Lack of scientific evidence in bigger group of patienst
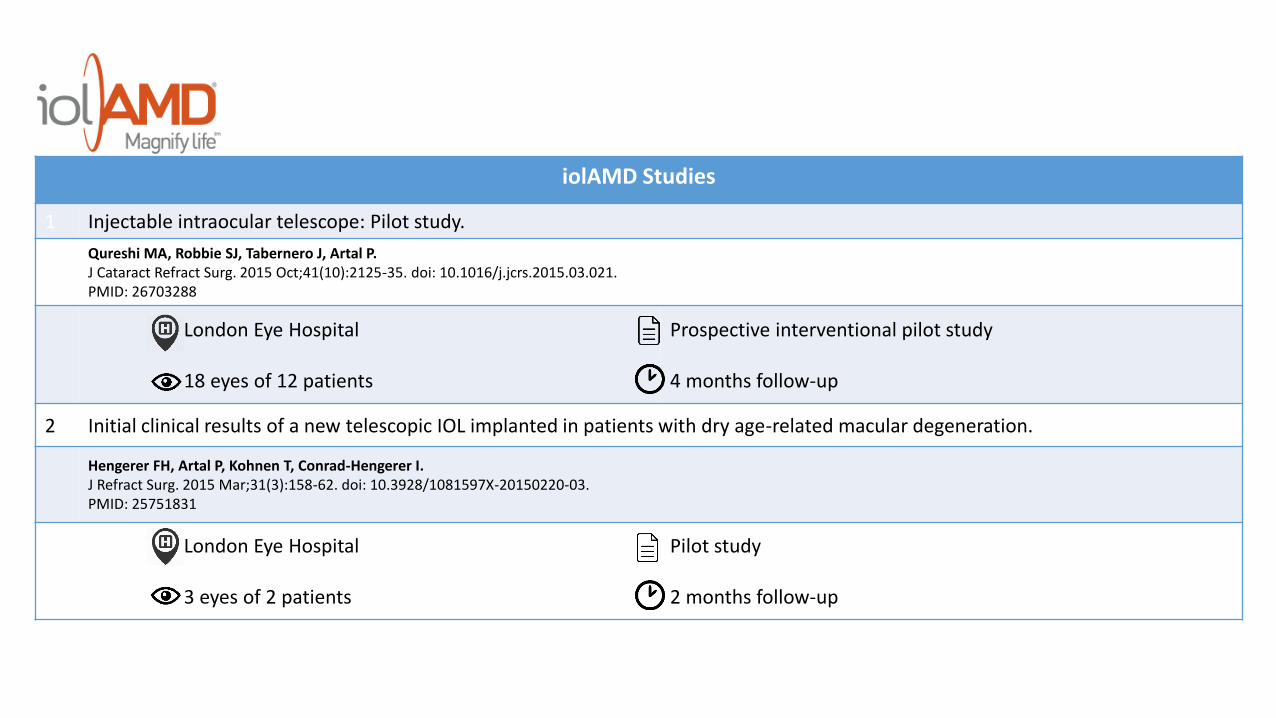
iolAMD Studies
1 Injectable intraocular telescope: Pilot study.
Qureshi MA, Robbie SJ, Tabernero J, Artal P.J Cataract Refract Surg. 2015 Oct;41(10):2125-35. doi: 10.1016/j.jcrs.2015.03.021.PMID: 26703288
London Eye Hospital
18 eyes of 12 patients
Prospective interventional pilot study
4 months follow-up
2 Initial clinical results of a new telescopic IOL implanted in patients with dry age-related macular degeneration.
Hengerer FH, Artal P, Kohnen T, Conrad-Hengerer I.J Refract Surg. 2015 Mar;31(3):158-62. doi: 10.3928/1081597X-20150220-03.PMID: 25751831
London Eye Hospital
3 eyes of 2 patients
Pilot study
2 months follow-up
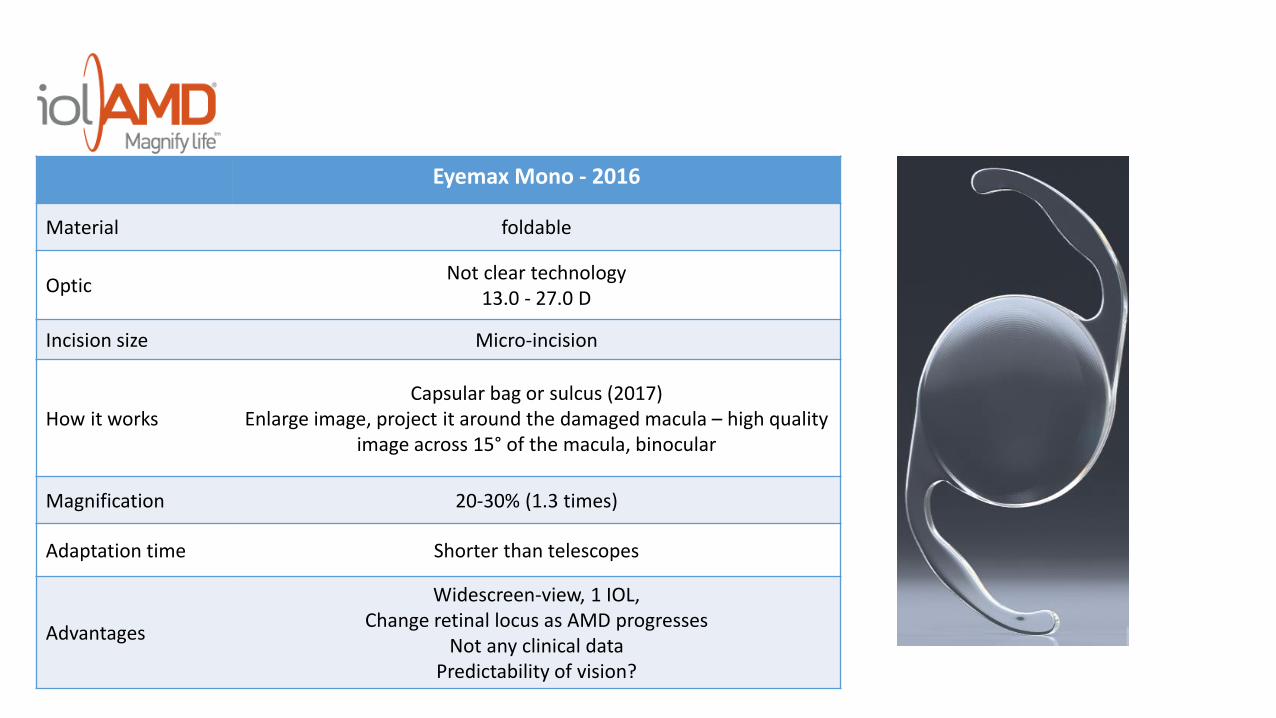
Eyemax Mono - 2016
Material foldable
OpticNot clear technology
13.0 - 27.0 D
Incision size Micro-incision
How it worksCapsular bag or sulcus (2017)
Enlarge image, project it around the damaged macula – high qualityimage across 15° of the macula, binocular
Magnification 20-30% (1.3 times)
Adaptation time Shorter than telescopes
Advantages
Widescreen-view, 1 IOL, Change retinal locus as AMD progresses
Not any clinical dataPredictability of vision?
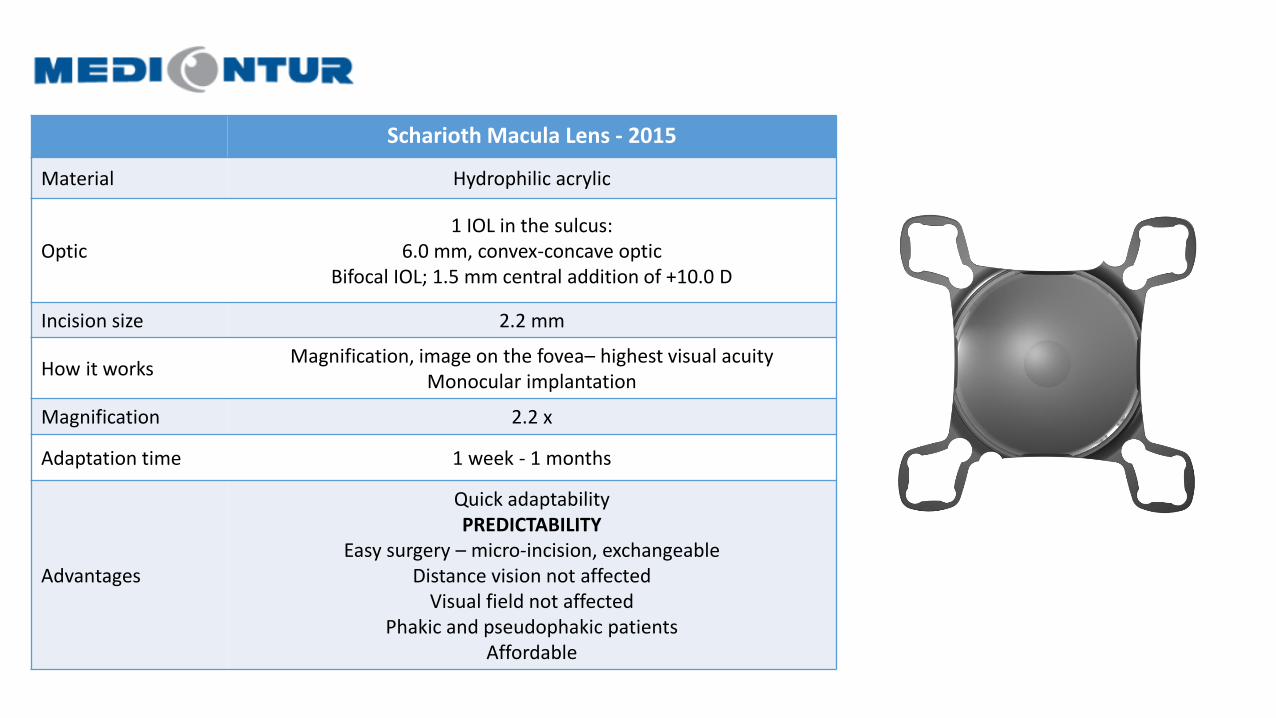
Scharioth Macula Lens - 2015
Material Hydrophilic acrylic
Optic1 IOL in the sulcus:
6.0 mm, convex-concave opticBifocal IOL; 1.5 mm central addition of +10.0 D
Incision size 2.2 mm
How it worksMagnification, image on the fovea– highest visual acuity
Monocular implantation
Magnification 2.2 x
Adaptation time 1 week - 1 months
Advantages
Quick adaptabilityPREDICTABILITY
Easy surgery – micro-incision, exchangeableDistance vision not affected
Visual field not affectedPhakic and pseudophakic patients
Affordable
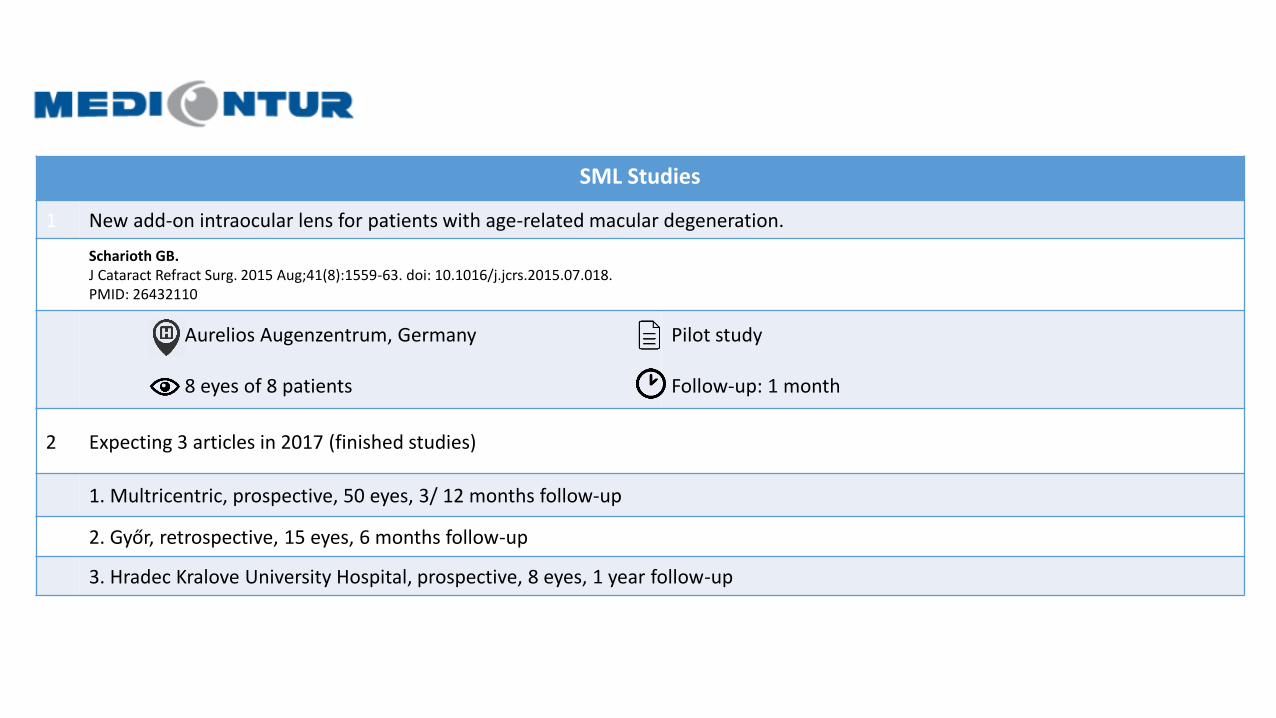
SML Studies
1 New add-on intraocular lens for patients with age-related macular degeneration.
Scharioth GB.J Cataract Refract Surg. 2015 Aug;41(8):1559-63. doi: 10.1016/j.jcrs.2015.07.018.PMID: 26432110
Aurelios Augenzentrum, Germany
8 eyes of 8 patients
Pilot study
Follow-up: 1 month
2 Expecting 3 articles in 2017 (finished studies)
1. Multricentric, prospective, 50 eyes, 3/ 12 months follow-up
2. Győr, retrospective, 15 eyes, 6 months follow-up
3. Hradec Kralove University Hospital, prospective, 8 eyes, 1 year follow-up
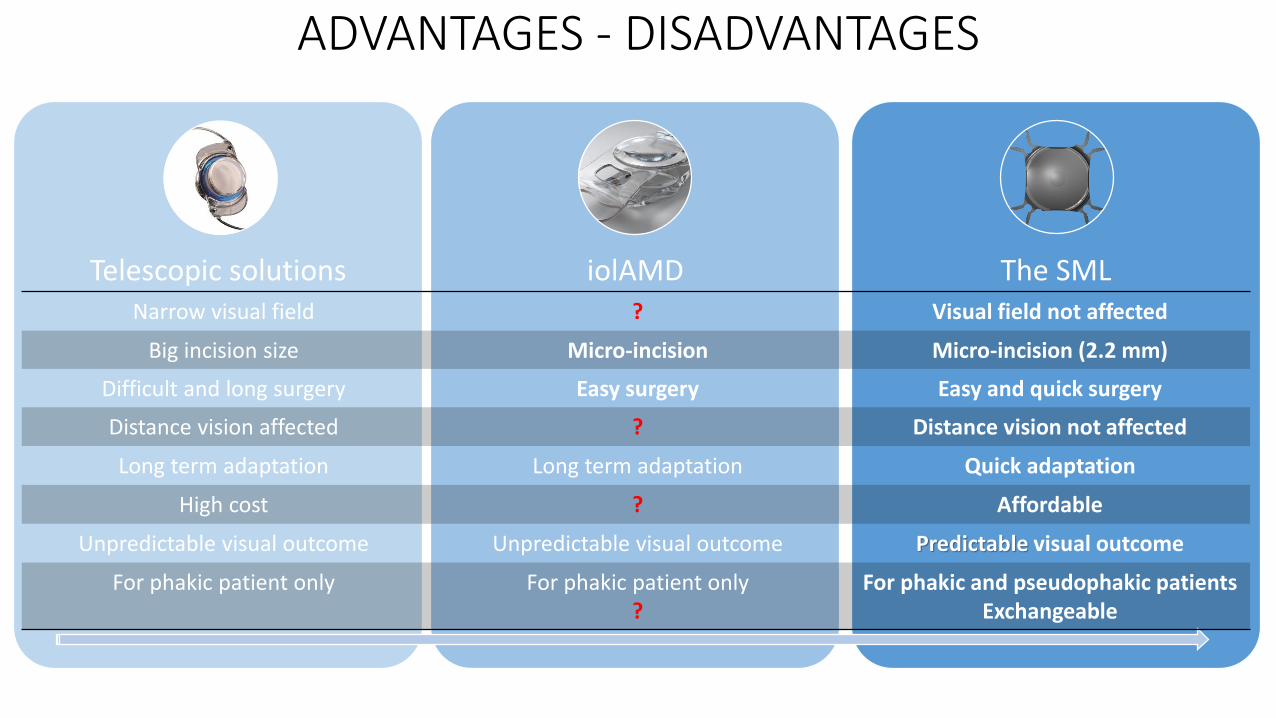
ADVANTAGES - DISADVANTAGES
Telescopic solutions iolAMD The SMLNarrow visual field ? Visual field not affected
Big incision size Micro-incision Micro-incision (2.2 mm)
Difficult and long surgery Easy surgery Easy and quick surgery
Distance vision affected ? Distance vision not affected
Long term adaptation Long term adaptation Quick adaptation
High cost ? Affordable
Unpredictable visual outcome Unpredictable visual outcome Predictable visual outcome
For phakic patient only For phakic patient only?
For phakic and pseudophakic patientsExchangeable
Clinical outcomes of eyes implanted with the Scharioth Macula Lens (A45 SML/SMY) in patients with Age
Related Macular Degeneration
Gabor B Scharioth (Recklinghausen, Germany), Anneliese Riehl (Kiehl, Germany), Ivan Tanev (Sofia, Bulgaria), Pavel Rozsival (Hradec Kralove, Czech republic), Jana Nekolova (Hradec Kralove, Czech republic), Florian Balta (Bucharest,
Romania), Emmanuel van Acker (Brussels, Belgium), Zoltan Z. Nagy (Budapest, Hungary),
SML - Scharioth Macula Lens
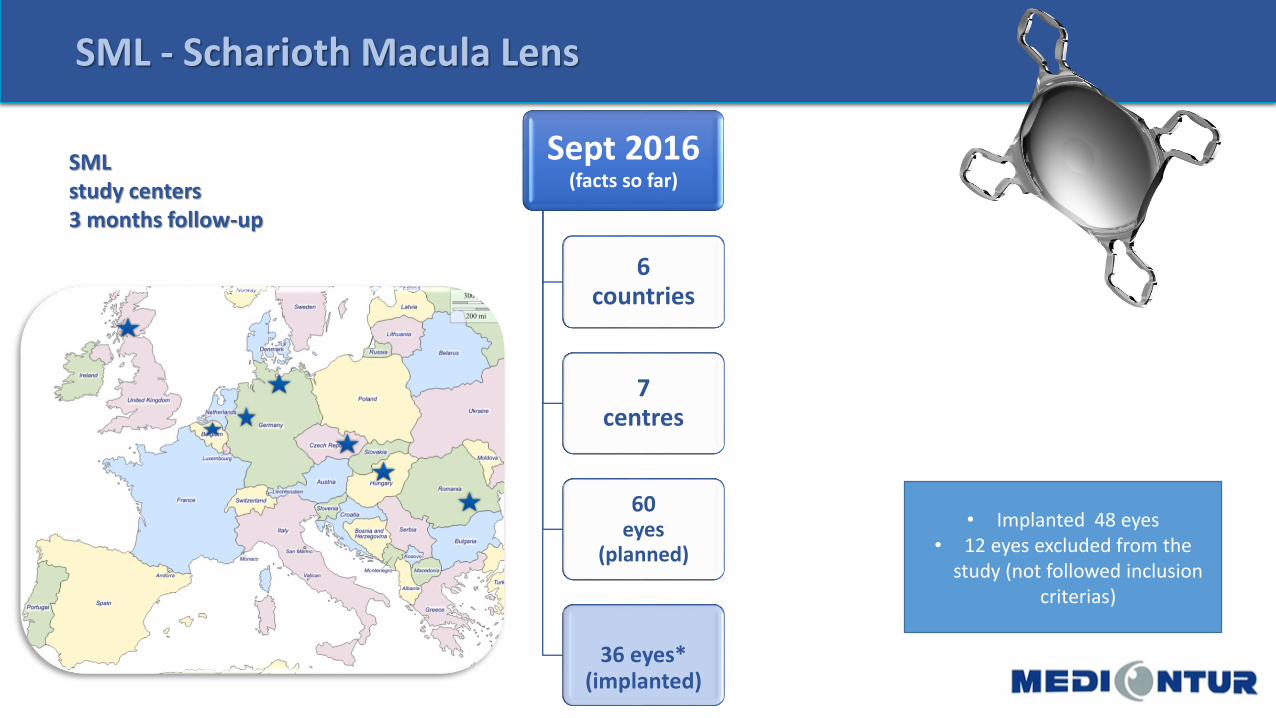
Sept 2016(facts so far)
6countries
7centres
60eyes
(planned)
36 eyes*(implanted)
SMLstudy centers3 months follow-up
SML - Scharioth Macula Lens
• Implanted 48 eyes• 12 eyes excluded from the
study (not followed inclusioncriterias)
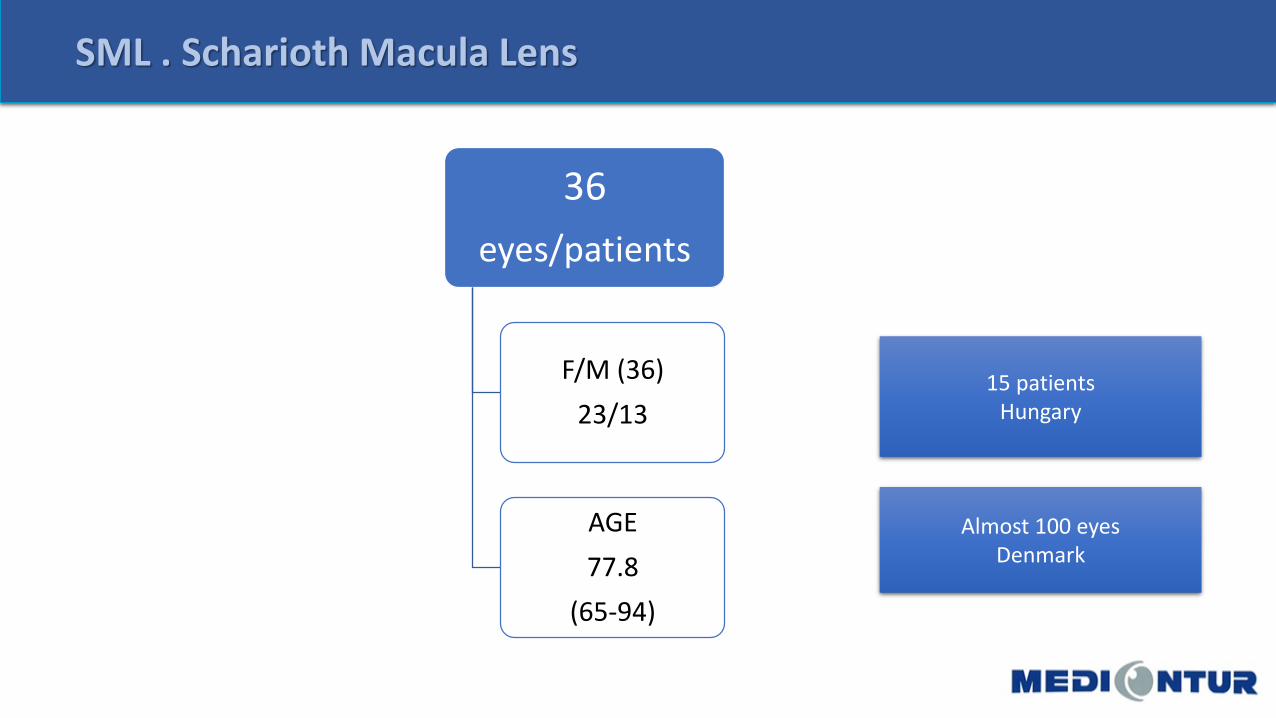
36
eyes/patients
F/M (36)
23/13
AGE
77.8
(65-94)
SML . Scharioth Macula Lens
15 patientsHungary
Almost 100 eyes Denmark
• ETDRS CHARTs
for testing
SML . Scharioth Macula Lens
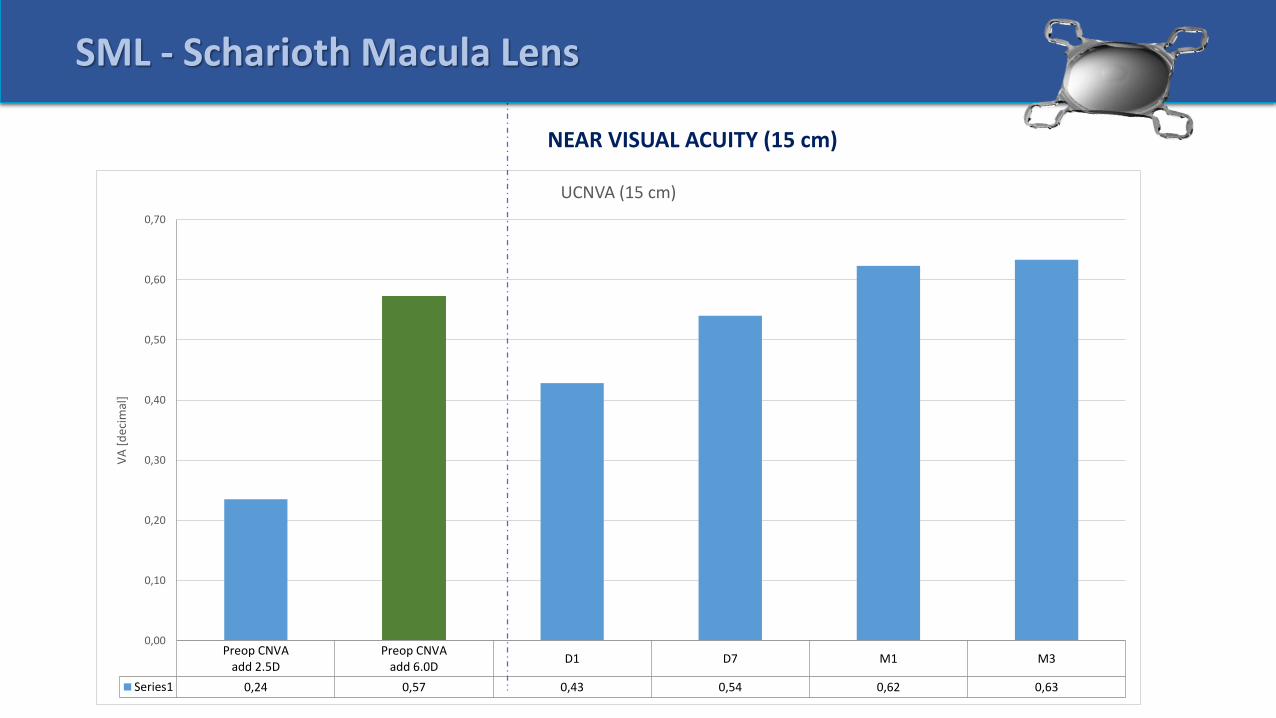
Preop CNVAadd 2.5D
Preop CNVAadd 6.0D
D1 D7 M1 M3
Series1 0,24 0,57 0,43 0,54 0,62 0,63
0,00
0,10
0,20
0,30
0,40
0,50
0,60
0,70
VA
[d
ecim
al]
UCNVA (15 cm)
SML - Scharioth Macula Lens
NEAR VISUAL ACUITY (15 cm)
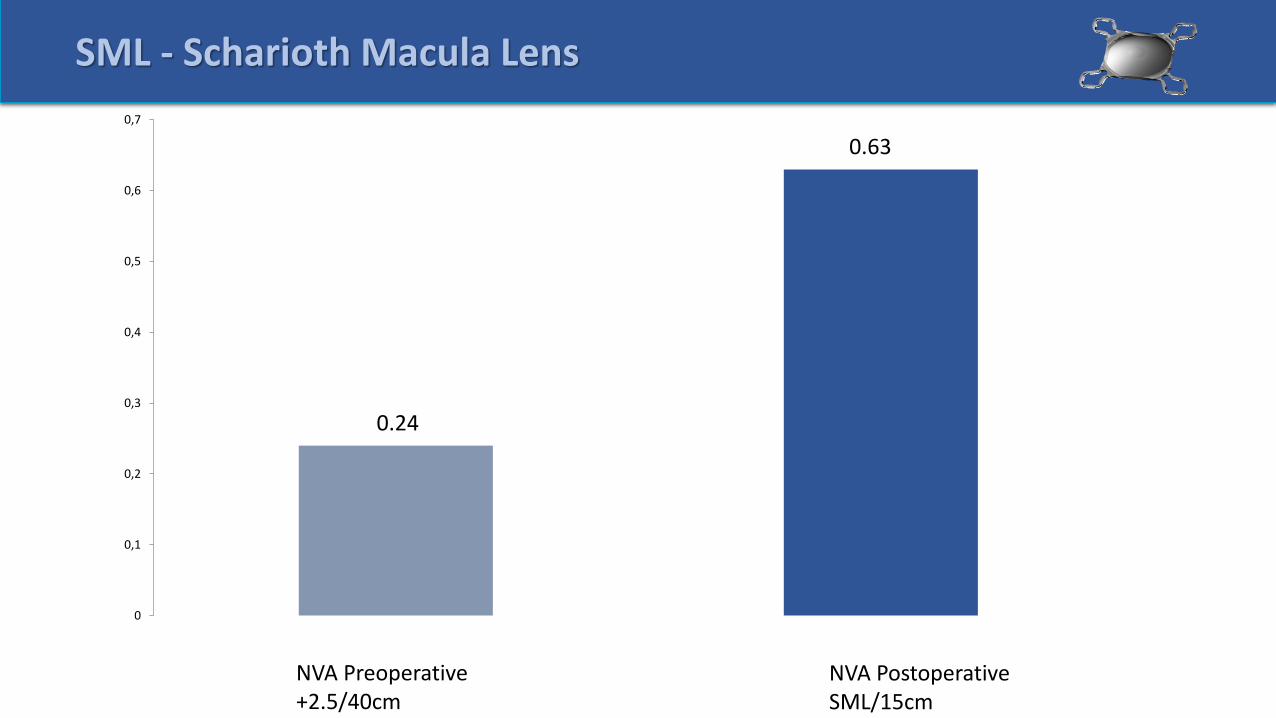
NVA Postoperative SML/15cm
NVA Preoperative+2.5/40cm
SML - Scharioth Macula Lens
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0.24
0.63
SML - Scharioth Macula Lens
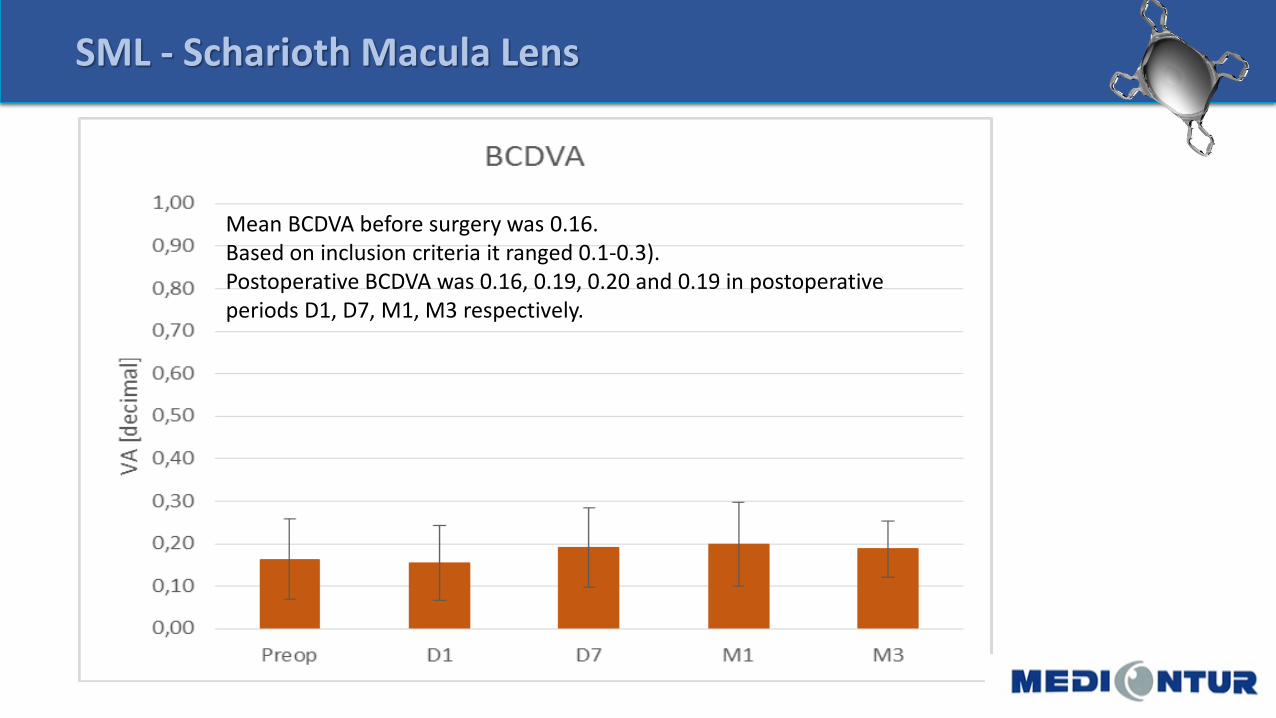
Mean BCDVA before surgery was 0.16. Based on inclusion criteria it ranged 0.1-0.3). Postoperative BCDVA was 0.16, 0.19, 0.20 and 0.19 in postoperative periods D1, D7, M1, M3 respectively.
SML - Scharioth Macula Lens
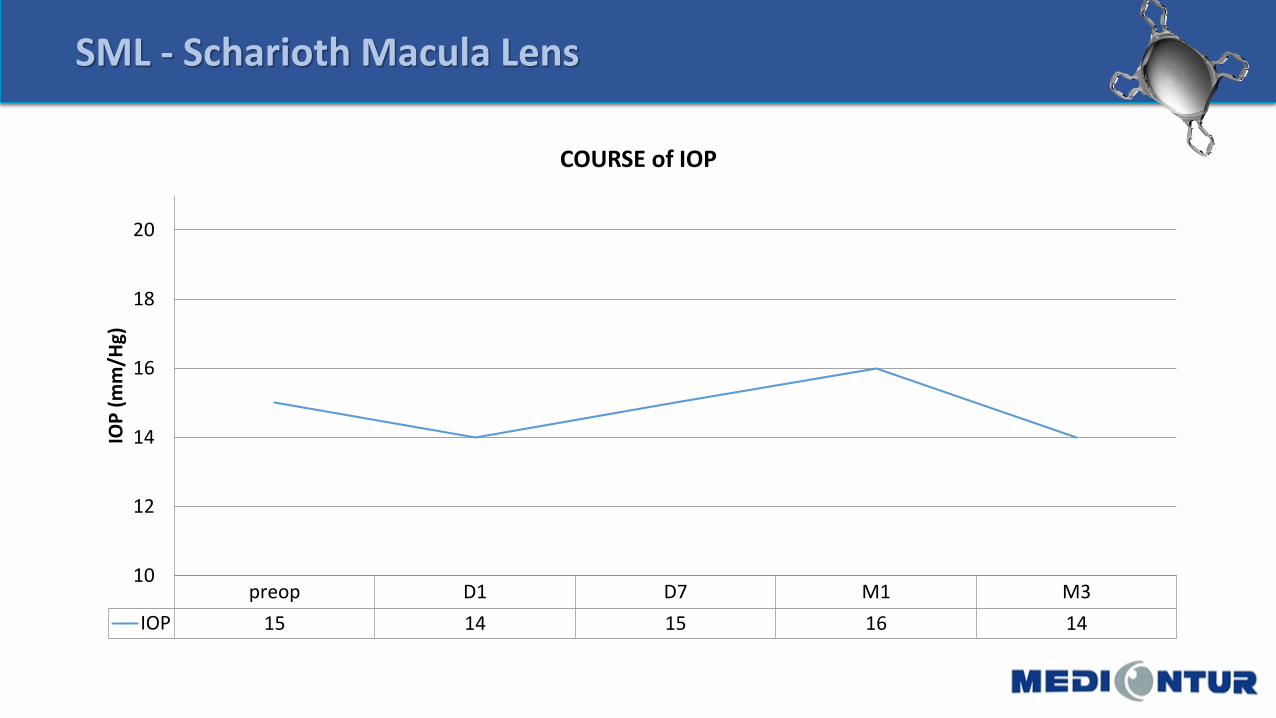
preop D1 D7 M1 M3
IOP 15 14 15 16 14
10
12
14
16
18
20
IOP
(m
m/H
g)
COURSE of IOP
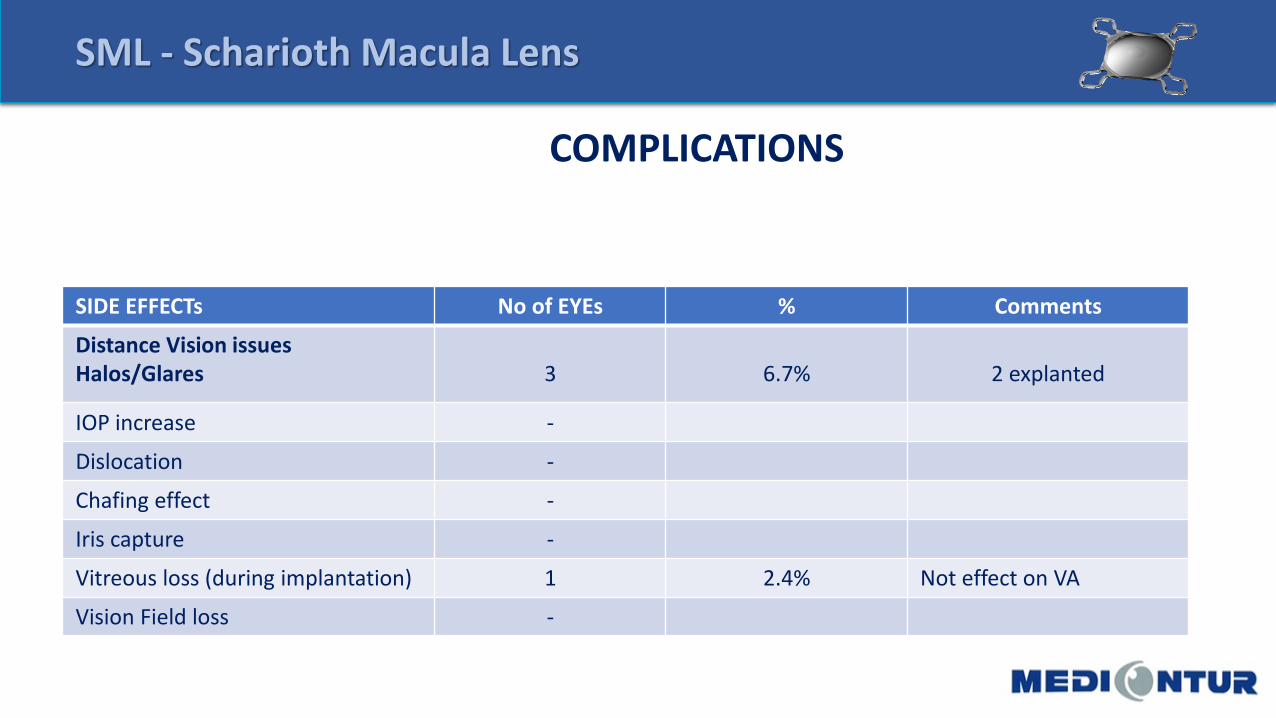
SIDE EFFECTs No of EYEs % Comments
Distance Vision issuesHalos/Glares 3 6.7% 2 explanted
IOP increase -
Dislocation -
Chafing effect -
Iris capture -
Vitreous loss (during implantation) 1 2.4% Not effect on VA
Vision Field loss -
COMPLICATIONS
SML - Scharioth Macula Lens
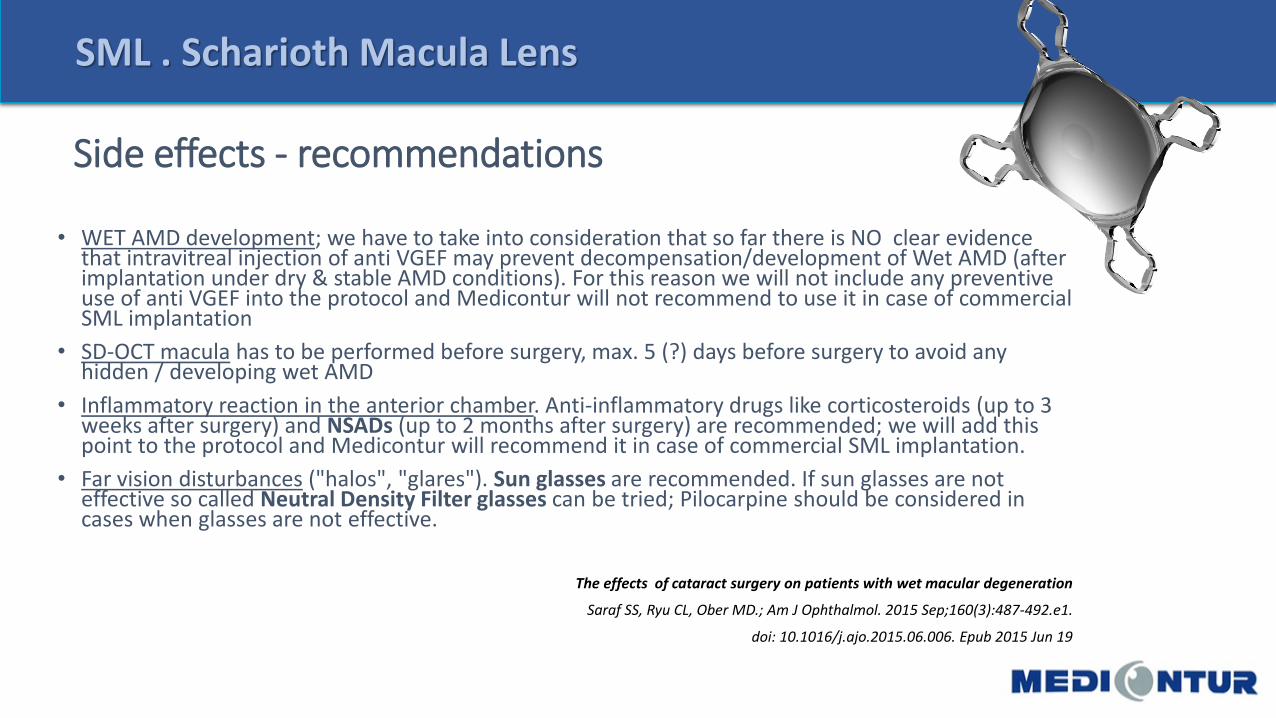
Side effects - recommendations
• WET AMD development; we have to take into consideration that so far there is NO clear evidence that intravitreal injection of anti VGEF may prevent decompensation/development of Wet AMD (after implantation under dry & stable AMD conditions). For this reason we will not include any preventive use of anti VGEF into the protocol and Medicontur will not recommend to use it in case of commercial SML implantation
• SD-OCT macula has to be performed before surgery, max. 5 (?) days before surgery to avoid any hidden / developing wet AMD
• Inflammatory reaction in the anterior chamber. Anti-inflammatory drugs like corticosteroids (up to 3 weeks after surgery) and NSADs (up to 2 months after surgery) are recommended; we will add this point to the protocol and Medicontur will recommend it in case of commercial SML implantation.
• Far vision disturbances ("halos", "glares"). Sun glasses are recommended. If sun glasses are not effective so called Neutral Density Filter glasses can be tried; Pilocarpine should be considered in cases when glasses are not effective.
The effects of cataract surgery on patients with wet macular degeneration
Saraf SS, Ryu CL, Ober MD.; Am J Ophthalmol. 2015 Sep;160(3):487-492.e1.
doi: 10.1016/j.ajo.2015.06.006. Epub 2015 Jun 19
SML . Scharioth Macula Lens
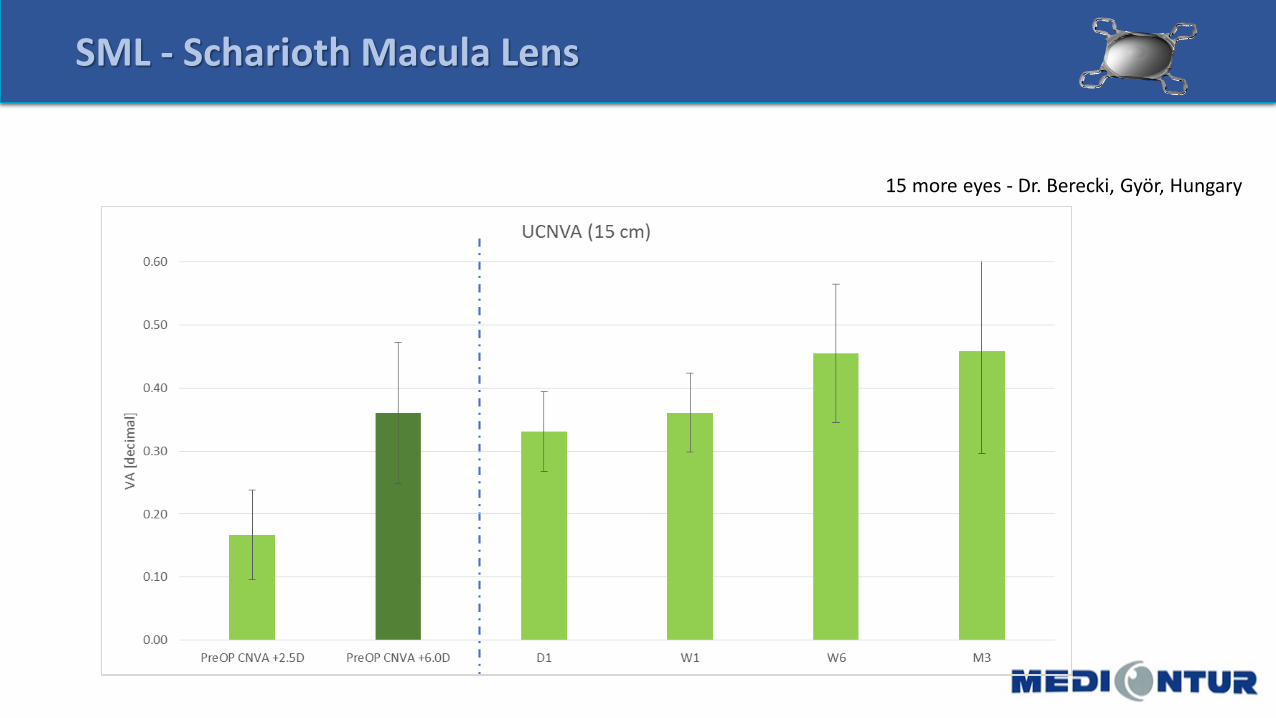
SML - Scharioth Macula Lens
15 more eyes - Dr. Berecki, Györ, Hungary
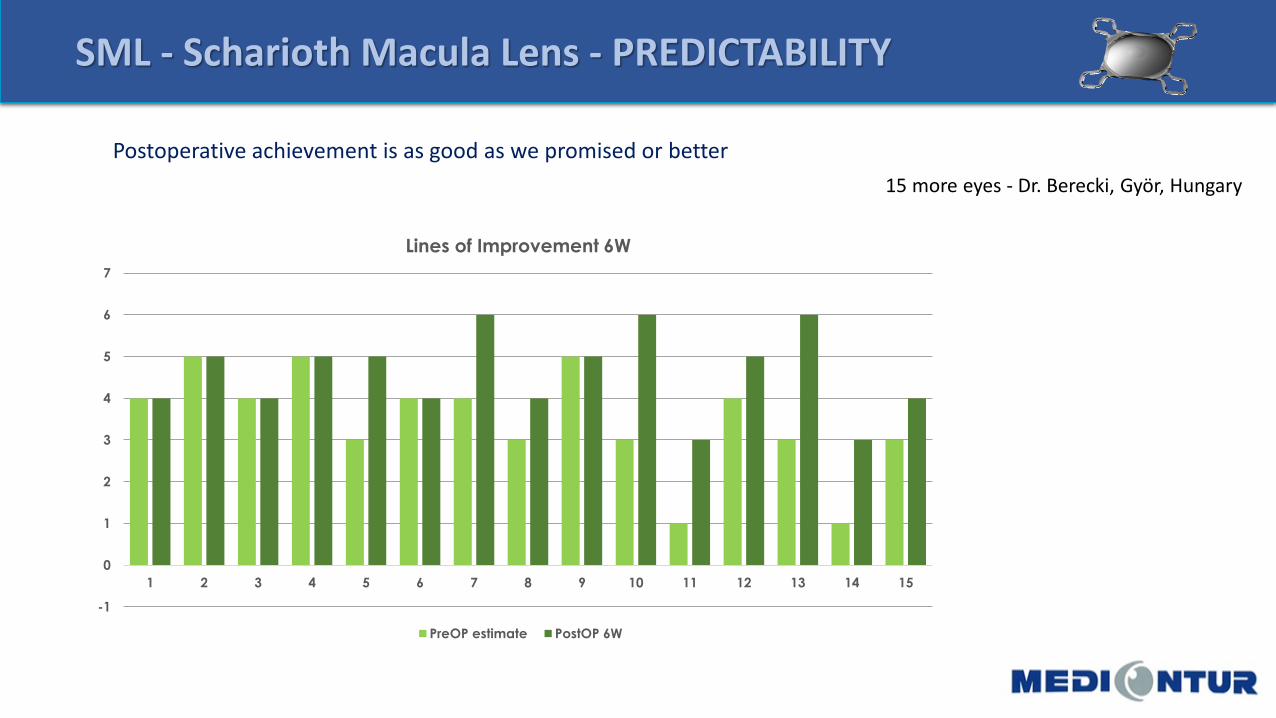
SML - Scharioth Macula Lens - PREDICTABILITY
15 more eyes - Dr. Berecki, Györ, Hungary
-1
0
1
2
3
4
5
6
7
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Lines of Improvement 6W
PreOP estimate PostOP 6W
Postoperative achievement is as good as we promised or better
SML . Scharioth Macula Lens
CONCLUSION:
MAIN MESSAGES:
• If indications are set preoperly results are good or excellent
• PREDICTABILITY = Strong correlation betweenCNVA +6.D 15 cm preop / NVA 15 cm postop• Allow to predict postoperative results and help in communication with patients, lead their expectations
• Patients were satisfied or highly satisfied
• Improvement with time/training(NVA: D1 < D7 < M1)
• TRAINING• Postsurgical training of patients• Clear instructions for doctors/patients

SML – WAY TO SUCCESS
CHOSE THE RIGHT DOCTOR
(CLINIC)
• Clinic with anterior & posterior segments departments
• = pool of patients
• = precondition of correct indication
• = proper examinations & communication
• Postsurgical treatment, training & observation of patients (centres for low vison patients training)
PATIENTs INDICATION
•MOTIVATION is the KEY
• INDICATION CRITERIAs
TRAINING & MOTIVATION
•Patients for „life“
•Never ending motivation & take care of patients

SML & Marketing Support….and much more

PATIENT SELECTION/INDICATION
MOTIVATION & PROPER TRAINING POSTOPERATIVE CARE
= crucial for success & happy patients
SML ADVISER /CONSULTANT
• Easy to use
• Time saving - quick (5 min)
• To select optimal patients who will BENEFIT from the SML
• To discuss & learn for all: doctors- distributor partners- Medicontur
• To support/increase services for doctors (especially at the starting point)














![Your guide to age-related macular degeneration · Your guide to age-related macular degeneration Cross-section of the eye Lens Cornea] Macula ... checked using an Amsler grid (see](https://img.pdfslide.us/doc/110x75/5b5cd3fd7f8b9ad21d8cf854/your-guide-to-age-related-macular-degeneration-your-guide-to-age-related-macular.jpg)















