Embed Size (px)
Citation preview
INTERVENTION IN CHD INTERVENTION IN CHD
WHEN WHEN AND AND HOWHOW
SCENARIO OF CARDIOVSCILAR SCENARIO OF CARDIOVSCILAR DISEASE IN NEPALDISEASE IN NEPAL
DR. YADAV BHATTDR. YADAV BHATT
MBBS, MDMBBS, MD (Med)(Med)
DM DM ((Cardiology)Cardiology)
DNB Fellow in Interventional CardiologyDNB Fellow in Interventional Cardiology
(Escorts heart institute)(Escorts heart institute)
CARDIOLOGISTCARDIOLOGIST
GANGALAL NATIONAL HEART CENTERGANGALAL NATIONAL HEART CENTER
DR. YADAV BHATTMBBS, MD (Med)
DM (Cardiology)
DNB Interventional Cardiology
(Escorts Heart Institute)
PROFESSOR CARDIOLOGY
NATIONAL ACADEMY OF MEDICAL SCIENCES
GANGALA NATIONAL HEART CENTER
CHIEF OF CATH LAB,
NORVIC ESCORTS INTERNATIONAL HOSPITAL
SCENARIO OF CARDIOVASCULAR DISEASE IN NEPAL
CHINA
INDIA
• Area: 147171 sq. kilometers
• Population: 27,000,000
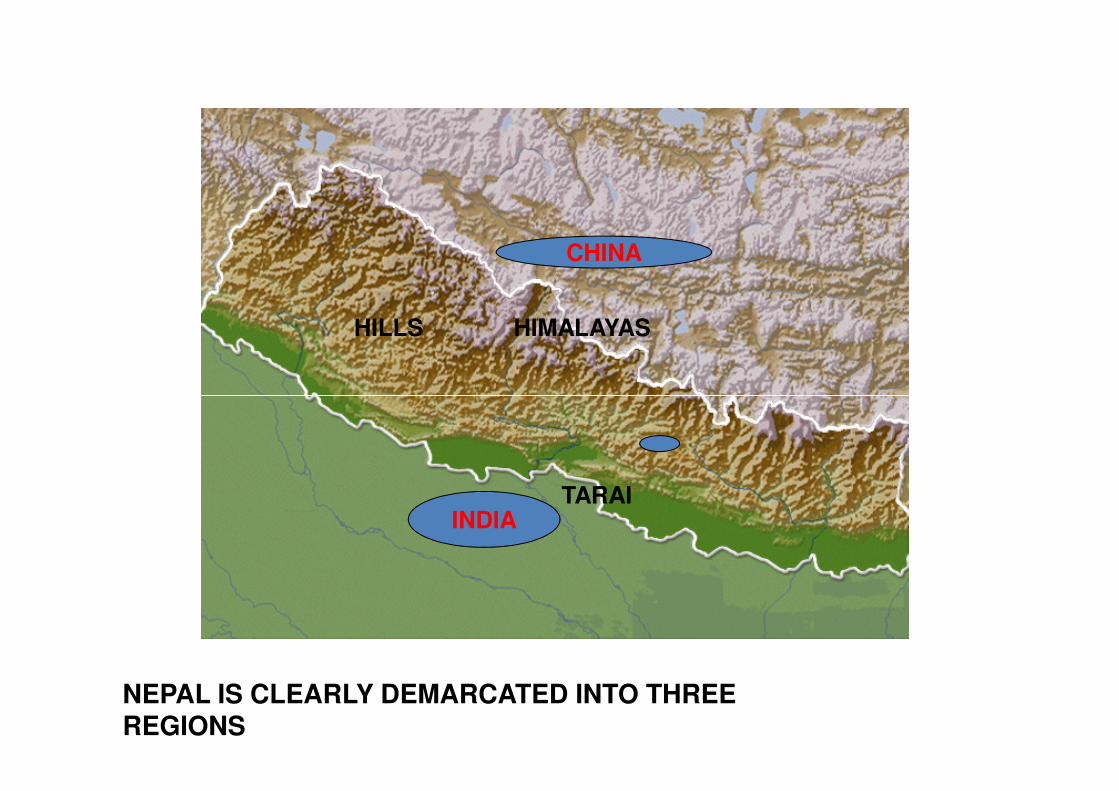
HIMALAYASHILLS
CHINA
NEPAL IS CLEARLY DEMARCATED INTO THREE REGIONS
TARAIINDIA
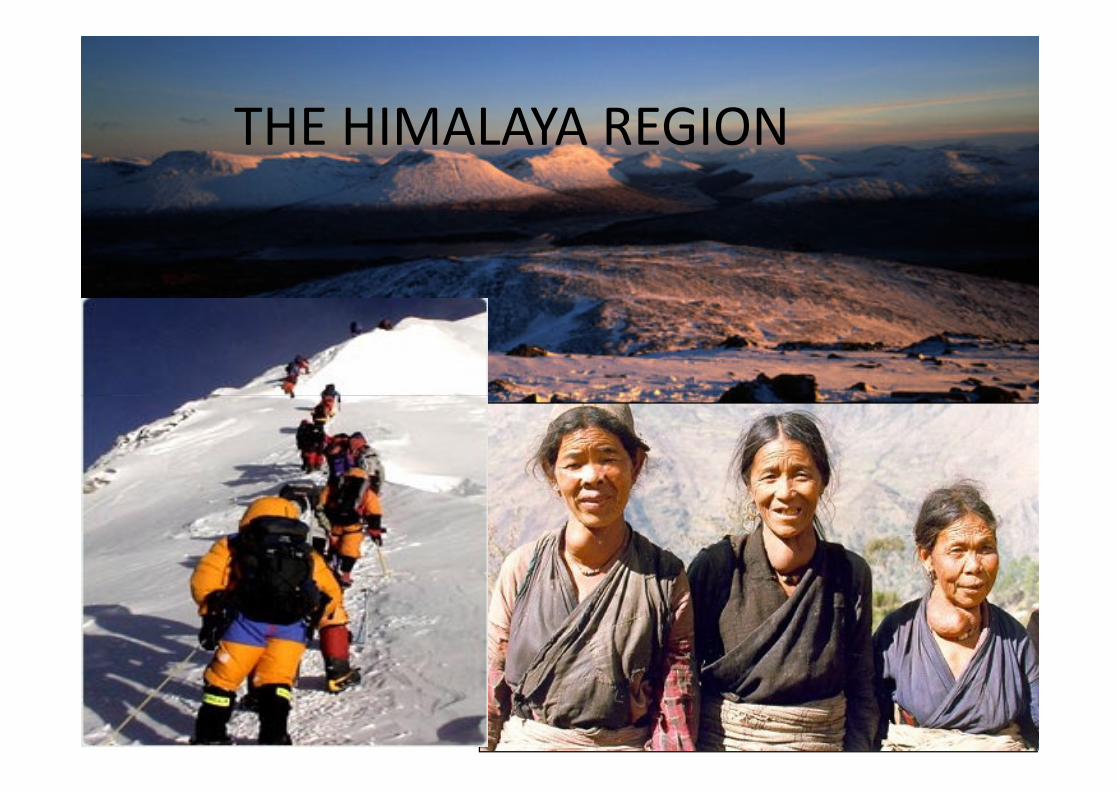
THE HIMALAYA REGION
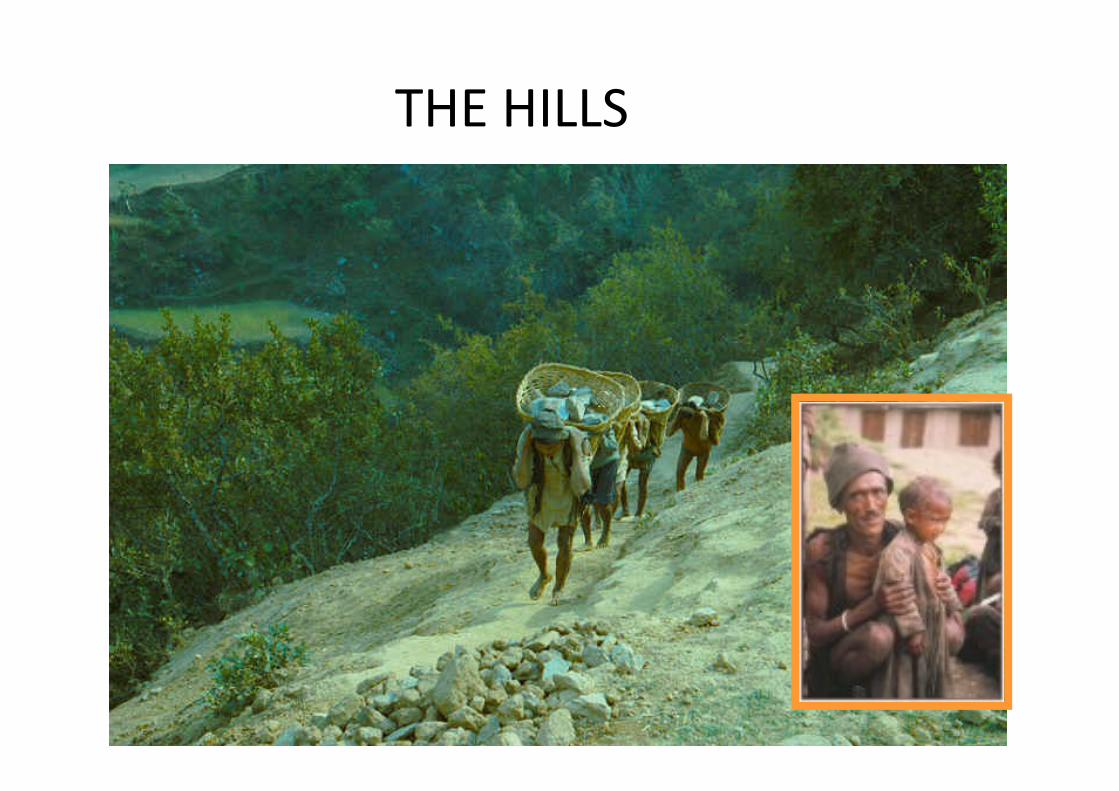
THE HILLS

ACCESSIBILITIES
• International & domestic airports
• International flight connections
– 13 online carriers: Thai Airways, Austrian Air, Indian Airlines, Jet Airways, Sahara Air, China Southwest Airlines, Druk Airlines, Gulf Air, Qatar Airways, PIA, RNAC, Cosmic Air, Air Nepal
– Catering Services to: 20 major international cities including Mumbai, – Catering Services to: 20 major international cities including Mumbai, Bangkok, New Delhi, Singapore, Hong Kong, Kolkata, Dubai, Shanghai, Osaka, Dhaka, Karachi, Thimpu, Abu dhabi, Varanasi, Kuala Lampur
– 22 Direct flights per week from Europe
– 15 Direct flights per week from middle east
– 24 Direct flights per week from far east
– 53 Direct flights per week from south asia
– 8-10 flights from china/week
• Adequate local ground transportation
Cardiovascular disease
has become
ubiquitous cause of
morbidity and morbidity and
mortality
TRAGEDY WITH CVD
• ACCORDING TO WHO 30% OF GLOBAL DEATH
IN 1998 DUE TO CVD = 15.3 MILLION LIVES
LOST THAT YEARLOST THAT YEAR
• LOW AND MIDDLE INCOME COUNTRIES
CONTRIBUTED 78% OF DEATHS
SAHID GANGALAL NATIONAL HEART CENTER
80000/ year
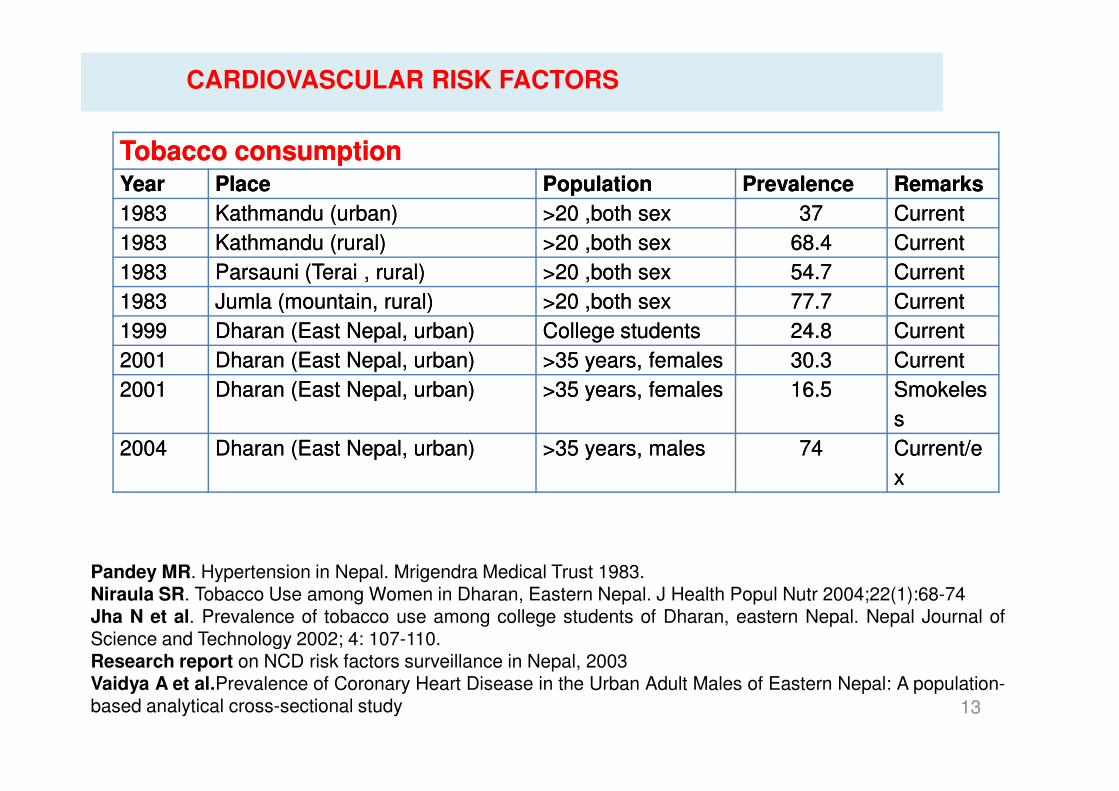
TobaccoTobacco consumptionconsumptionYearYear PlacePlace PopulationPopulation PrevalencePrevalence RemarksRemarks
19831983 Kathmandu (urban)Kathmandu (urban) >>2020 ,both,both sexsex 3737 CurrentCurrent
19831983 Kathmandu (rural)Kathmandu (rural) >>2020 ,both,both sexsex 68.468.4 CurrentCurrent
19831983 Parsauni (Terai , rural)Parsauni (Terai , rural) >>2020 ,both,both sexsex 54.754.7 CurrentCurrent
19831983 Jumla (mountain, rural)Jumla (mountain, rural) >>2020 ,both,both sexsex 77.777.7 CurrentCurrent
19991999 Dharan (East Nepal, urban)Dharan (East Nepal, urban) CollegeCollege studentsstudents 24.824.8 CurrentCurrent
20012001 Dharan (East Nepal, urban)Dharan (East Nepal, urban) >35 years, females>35 years, females 30.330.3 CurrentCurrent
20012001 Dharan (East Nepal, urban)Dharan (East Nepal, urban) >35 years, females>35 years, females 16.516.5 SmokelesSmokeles
CARDIOVASCULAR RISK FACTORS
13
Pandey MR. Hypertension in Nepal. Mrigendra Medical Trust 1983.Niraula SR. Tobacco Use among Women in Dharan, Eastern Nepal. J Health Popul Nutr 2004;22(1):68-74Jha N et al. Prevalence of tobacco use among college students of Dharan, eastern Nepal. Nepal Journal ofScience and Technology 2002; 4: 107-110.Research report on NCD risk factors surveillance in Nepal, 2003Vaidya A et al.Prevalence of Coronary Heart Disease in the Urban Adult Males of Eastern Nepal: A population-based analytical cross-sectional study
20012001 Dharan (East Nepal, urban)Dharan (East Nepal, urban) >35 years, females>35 years, females 16.516.5 SmokelesSmokeles
ss
20042004 Dharan (East Nepal, urban)Dharan (East Nepal, urban) >>3535 years,years, malesmales 7474 Current/eCurrent/e
xx
CARDIOVASCULAR RISK FACTORS
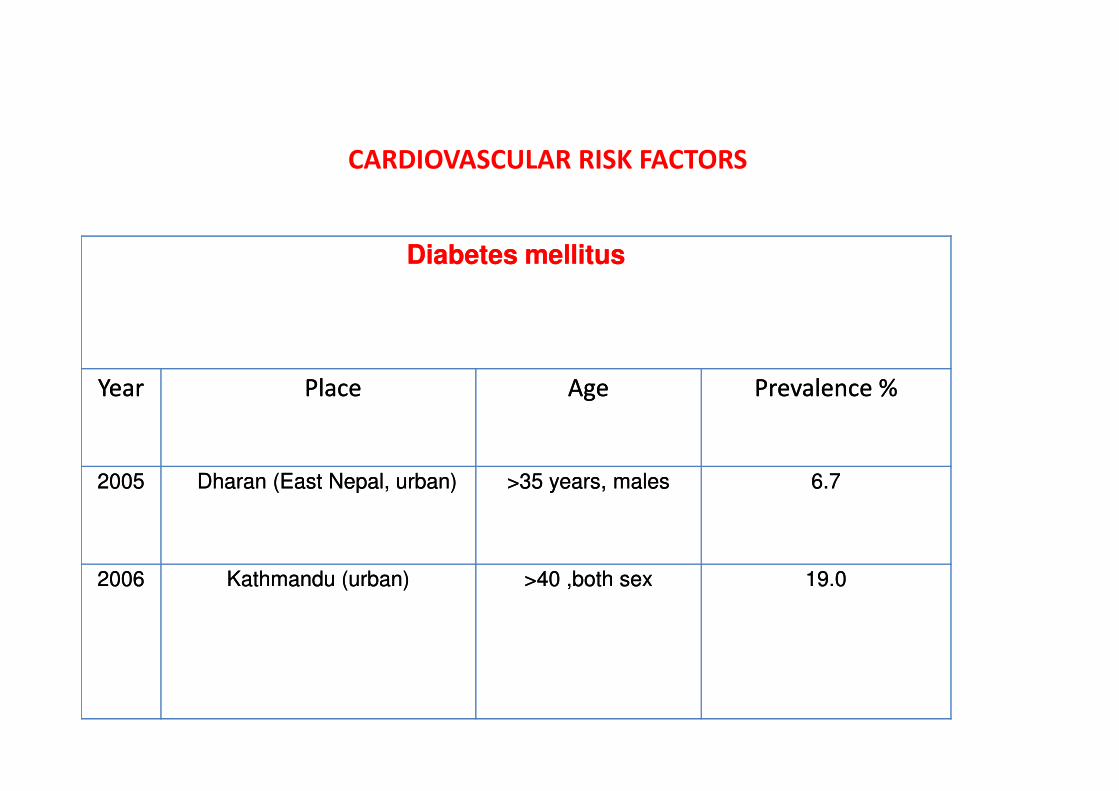
Diabetes mellitusDiabetes mellitus
YearYear PlacePlace AgeAge Prevalence %Prevalence %YearYear PlacePlace AgeAge Prevalence %Prevalence %
20052005 Dharan (East Nepal, urban)Dharan (East Nepal, urban) >35 years, males>35 years, males 6.7 6.7
20062006 Kathmandu (urban)Kathmandu (urban) >40 ,both sex>40 ,both sex 19.019.0
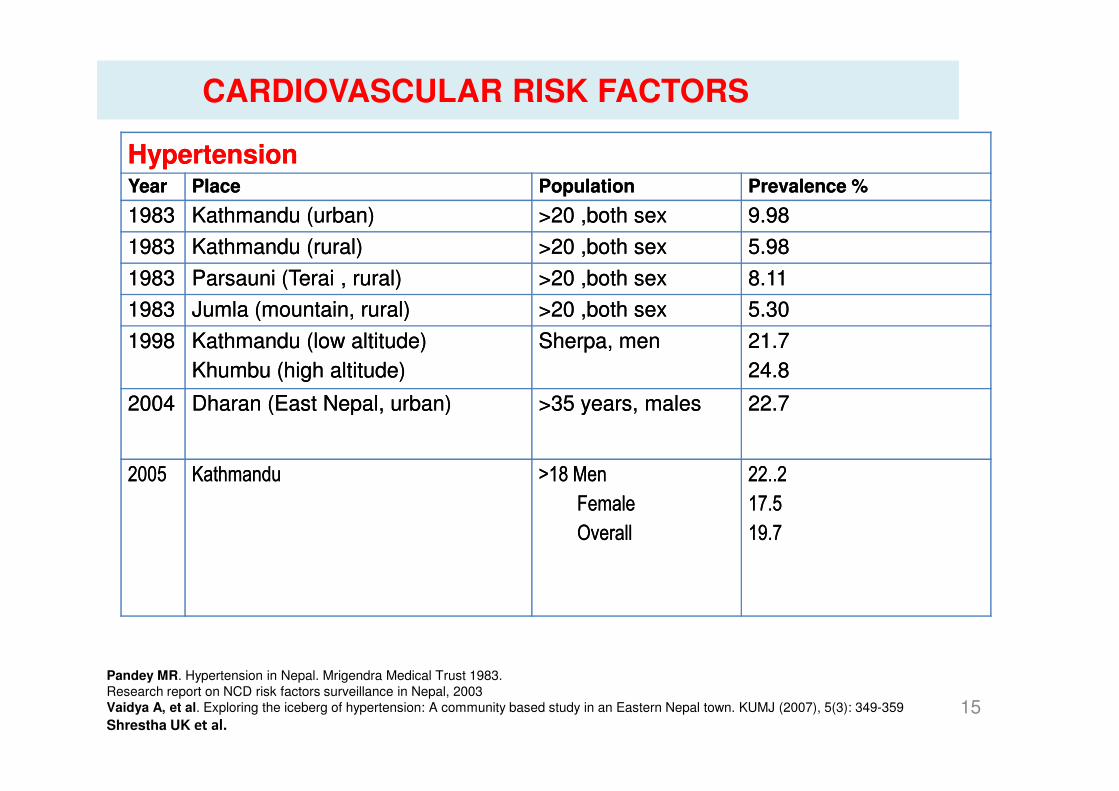
HypertensionHypertensionYear Year PlacePlace Population Population Prevalence %Prevalence %
1983 1983 Kathmandu (urban)Kathmandu (urban) >20 ,both sex>20 ,both sex 9.989.98
1983 1983 Kathmandu (rural)Kathmandu (rural) >20 ,both sex>20 ,both sex 5.985.98
1983 1983 Parsauni (Terai , rural)Parsauni (Terai , rural) >20 ,both sex>20 ,both sex 8.118.11
1983 1983 Jumla (mountain, rural)Jumla (mountain, rural) >20 ,both sex>20 ,both sex 5.305.30
19981998 Kathmandu (low altitude) Kathmandu (low altitude)
Khumbu (high altitude) Khumbu (high altitude)
Sherpa, men Sherpa, men 21.721.7
24.824.8
20042004 Dharan (East Nepal, urban)Dharan (East Nepal, urban) >35 years, males>35 years, males 22.722.7
CARDIOVASCULAR RISK FACTORS
15
Pandey MR. Hypertension in Nepal. Mrigendra Medical Trust 1983.
Research report on NCD risk factors surveillance in Nepal, 2003
Vaidya A, et al. Exploring the iceberg of hypertension: A community based study in an Eastern Nepal town. KUMJ (2007), 5(3): 349-359
Shrestha UK et al.
20042004 Dharan (East Nepal, urban)Dharan (East Nepal, urban) >35 years, males>35 years, males 22.722.7
20052005 KathmanduKathmandu >18 Men>18 Men
FemaleFemale
OverallOverall
22..222..2
17.517.5
19.719.7
HYPERTENSION
• STUDY NUMBER 1114 ( 2005)
• MEN 541• MEN 541
• FEMALE 573
• AGE 18 – 97 YEARS MEAN 37.8 ±16.3
HYPERTENSION
PREVALENCE OF HTN
• 22.2% IN MEN
• 17.3% IN WOMEN
• OVERALL PREVALENCE 19.7%• OVERALL PREVALENCE 19.7%
AGE DISTRIBUTION
• 4.1% < 30 YEARS
• >40% IN > 50YEARS
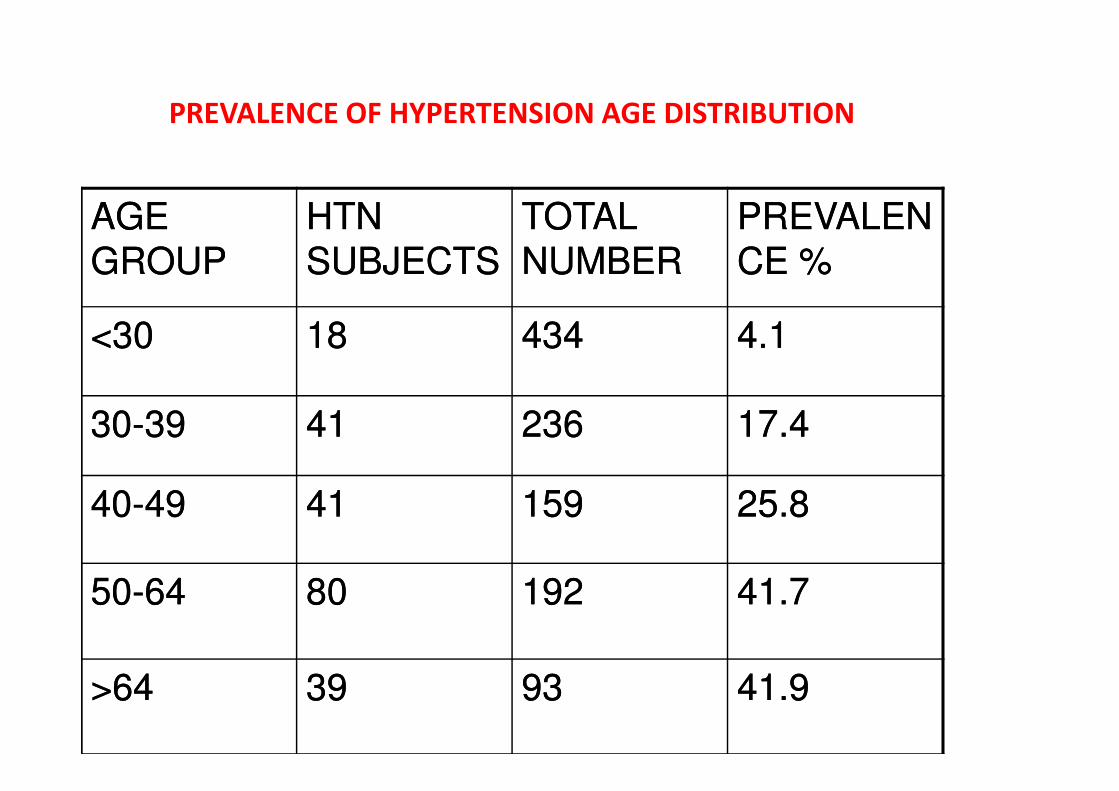
PREVALENCE OF HYPERTENSION AGE DISTRIBUTION
AGE AGE
GROUPGROUP
HTN HTN
SUBJECTSSUBJECTS
TOTAL TOTAL
NUMBERNUMBER
PREVALENPREVALEN
CE %CE %
<30<30 1818 434434 4.14.1
3030--3939 4141 236236 17.417.4
4040--4949 4141 159159 25.825.8
5050--6464 8080 192192 41.741.7
>64>64 3939 9393 41.941.9
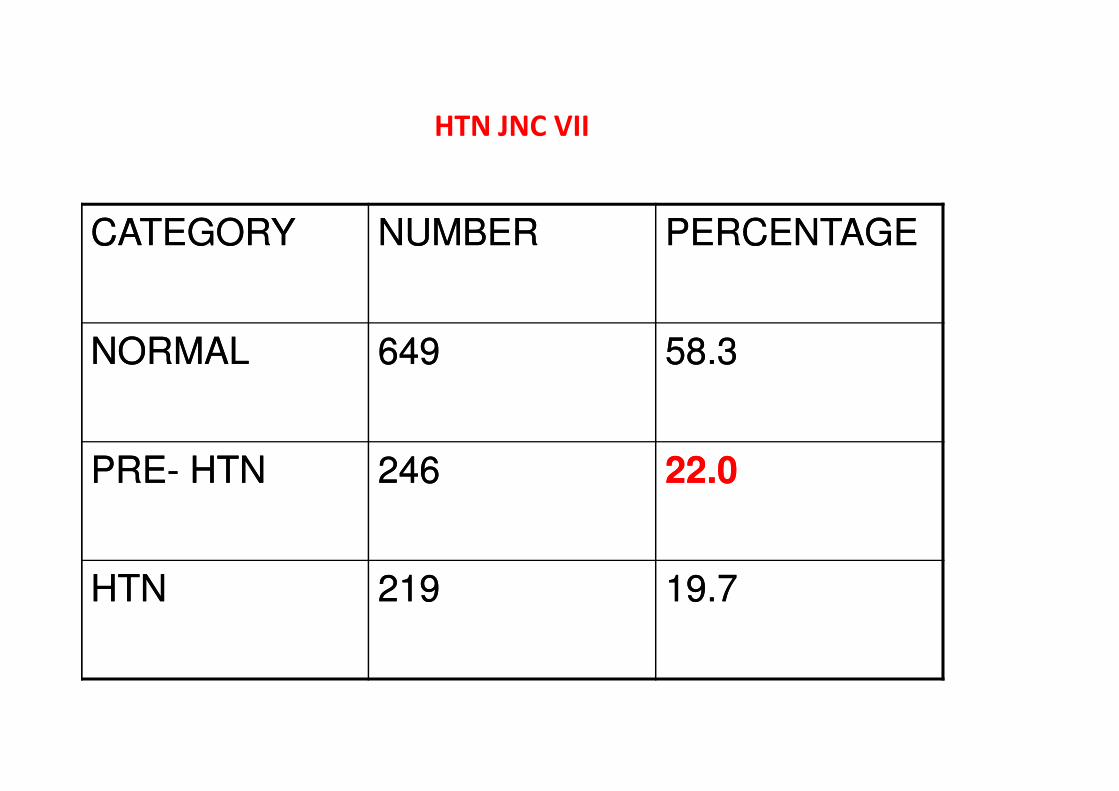
HTN JNC VII
CATEGORYCATEGORY NUMBERNUMBER PERCENTAGEPERCENTAGE
NORMALNORMAL 649649 58.358.3
PREPRE-- HTNHTN 246246 22.022.0
HTNHTN 219219 19.719.7
HTN AWARENESS
• 44.7% ASYMPTOMATIC
• 55% SYMPTOMATIC
• 76% HEADACHE
• 48.8% DIZZINESS
• 58.9% UNAWARE OF THEIR HTN
• 41.1% AWARE OF THEIR HTN
CHANGING TREND IN HTN
• STUDY IN 1981: PREVALENCE 5.98% (WHO 1978
CRITERIA ± 165/95)
• LATEST 2005 STUDY (SAME CRITERIA) PREVALENCE
WOULD BE 11%
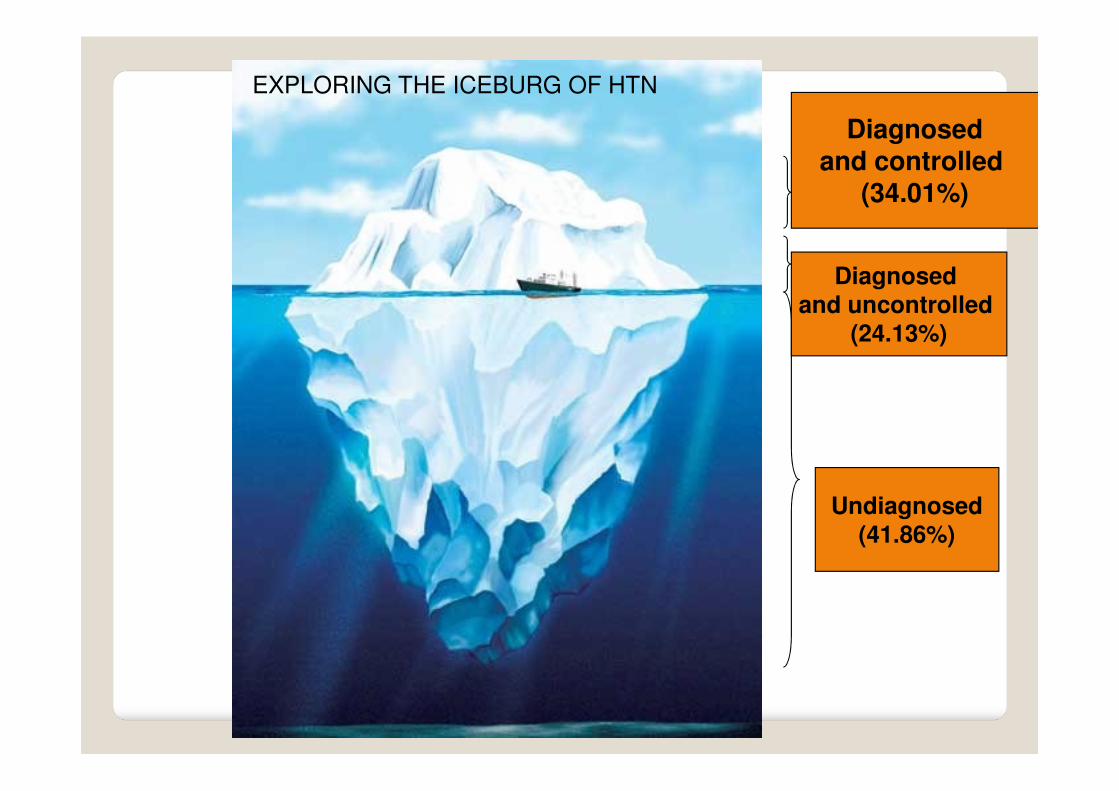
Diagnosedand controlled
(34.01%)
Diagnosed
and uncontrolled (24.13%)
EXPLORING THE ICEBURG OF HTN
Undiagnosed(41.86%)
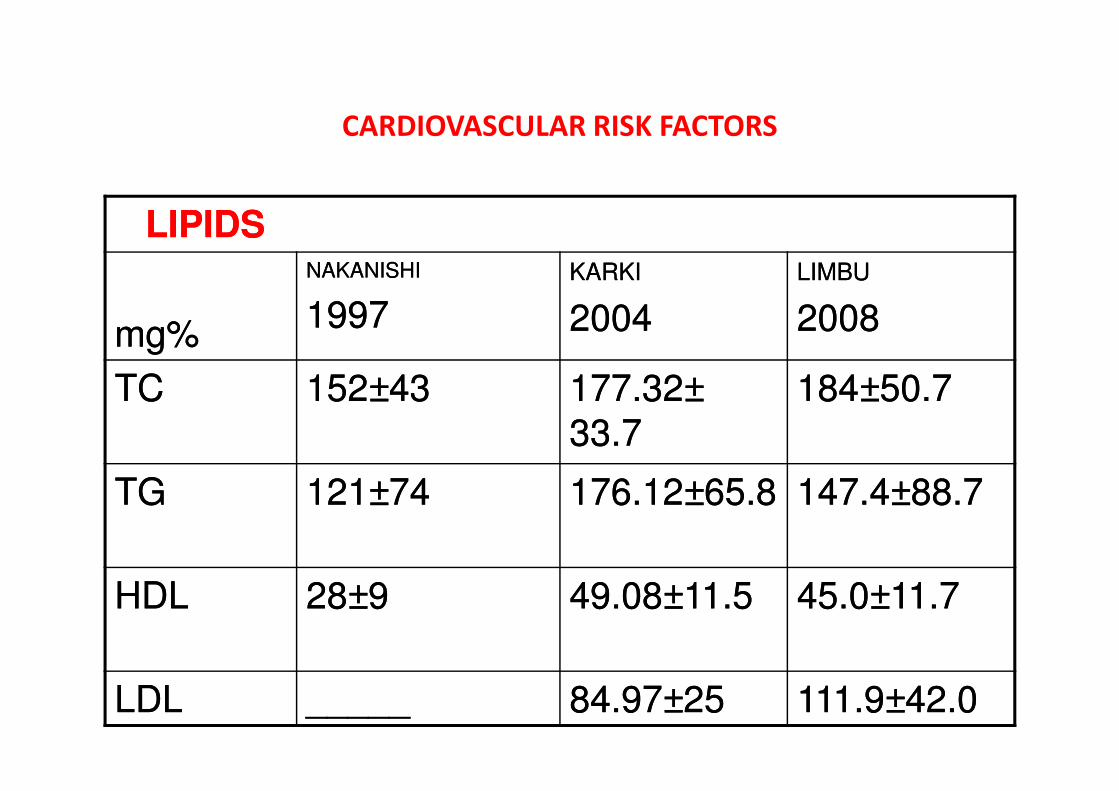
LIPIDSLIPIDS
mg%mg%
NAKANISHINAKANISHI
19971997
KARKIKARKI
20042004
LIMBULIMBU
20082008
TCTC 152152±±4343 177.32177.32±± 184184±±50.750.7
CARDIOVASCULAR RISK FACTORS
TCTC 152152±±4343 177.32177.32±±
33.733.7
184184±±50.750.7
TGTG 121121±±7474 176.12176.12±±65.865.8 147.4147.4±±88.788.7
HDLHDL 2828±±99 49.0849.08±±11.511.5 45.045.0±±11.711.7
LDLLDL __________ 84.9784.97±±2525 111.9111.9±±42.042.0
CARDIOVASCULAR RISK FACTORS
SEDENTARY LIFESTYLE
• < 10 mins of walk / day
• No physical activity Job, leasure time, house hold 4 days a week
• Broca’s index- ht in cm – 100
• Smokeless--- khaini etc
CARDIOVASCULAR RISK FACTORS
METAB0LIC SYNDROME
• IN INDIA 1/3rd URBAN POPULATION HAVE METABOLIC SYNDROME
• ONSET AT AGE 15-20
• MENIFESTATION 15- 20 YEARS LATER
• Ie. AT AGE 30- 40 YEARS
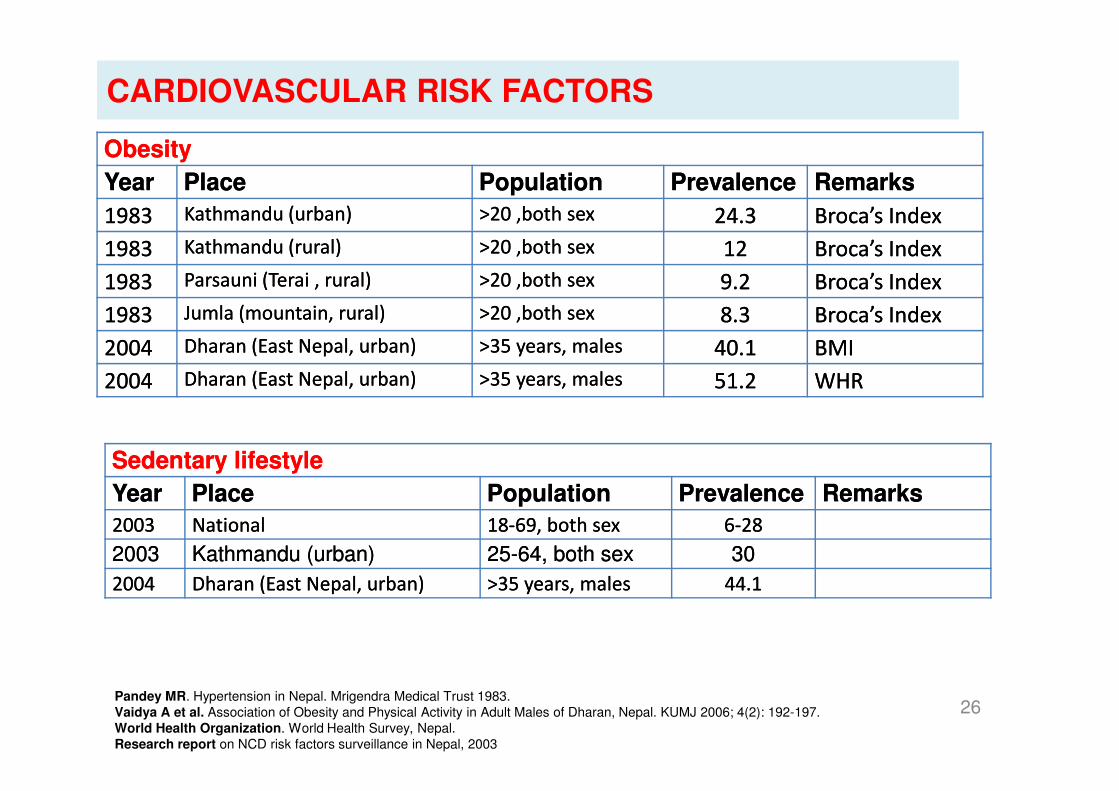
ObesityObesity
YearYear PlacePlace PopulationPopulation PrevalencePrevalence RemarksRemarks
19831983 Kathmandu (urban)Kathmandu (urban) >20 ,both sex>20 ,both sex 24.324.3 Broca’sBroca’s IndexIndex
19831983 Kathmandu (rural)Kathmandu (rural) >20 ,both sex>20 ,both sex 1212 Broca’sBroca’s IndexIndex
19831983 Parsauni (Terai , rural)Parsauni (Terai , rural) >20 ,both sex>20 ,both sex 9.29.2 Broca’sBroca’s IndexIndex
19831983 Jumla (mountain, rural)Jumla (mountain, rural) >20 ,both sex>20 ,both sex 8.38.3 Broca’sBroca’s IndexIndex
20042004 Dharan (East Nepal, urban)Dharan (East Nepal, urban) >35 years, males>35 years, males 40.140.1 BMIBMI
20042004 Dharan (East Nepal, urban)Dharan (East Nepal, urban) >35 years, males>35 years, males 51.251.2 WHRWHR
CARDIOVASCULAR RISK FACTORS
26Pandey MR. Hypertension in Nepal. Mrigendra Medical Trust 1983.
Vaidya A et al. Association of Obesity and Physical Activity in Adult Males of Dharan, Nepal. KUMJ 2006; 4(2): 192-197.
World Health Organization. World Health Survey, Nepal.
Research report on NCD risk factors surveillance in Nepal, 2003
SedentarySedentary lifestylelifestyle
YearYear PlacePlace PopulationPopulation PrevalencePrevalence RemarksRemarks
20032003 NationalNational 1818--6969,, bothboth sexsex 66--2828
20032003 KathmanduKathmandu (urban)(urban) 2525--6464,, bothboth sexsex 3030
20042004 DharanDharan (East(East Nepal,Nepal, urban)urban) >>3535 years,years, malesmales 44.144.1
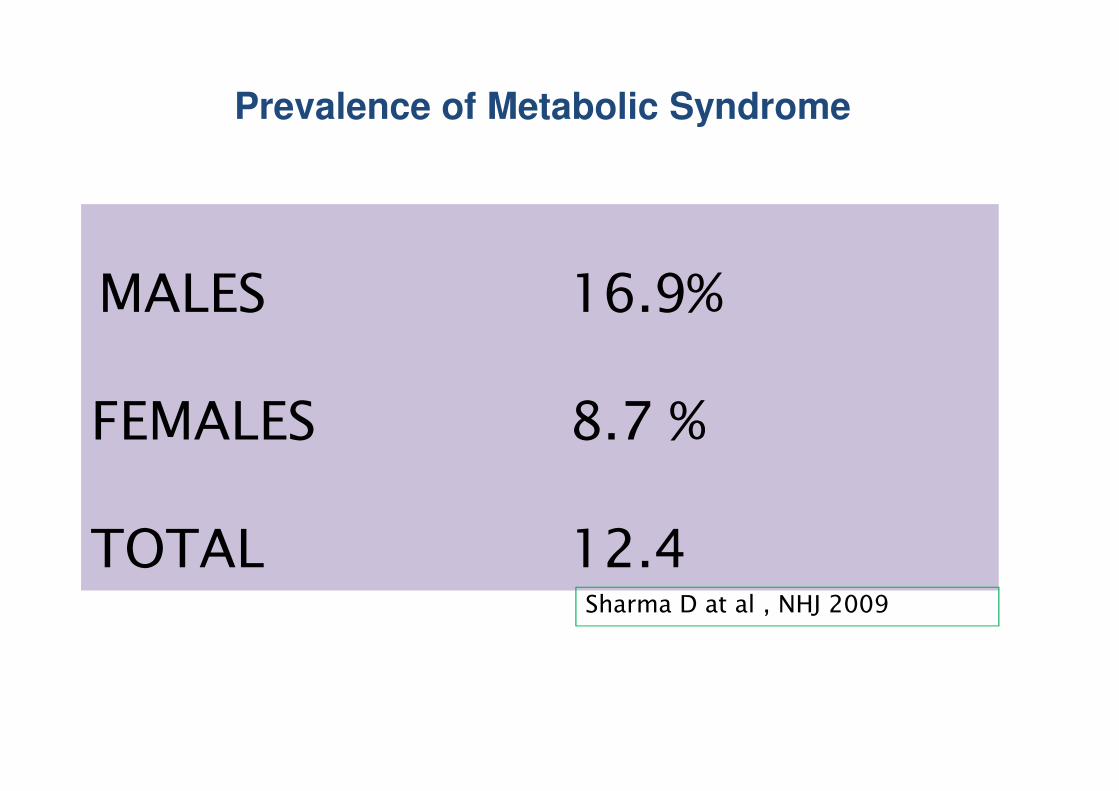
MALES 16.9%
FEMALES 8.7 %
Prevalence of Metabolic Syndrome
FEMALES 8.7 %
TOTAL 12.4Sharma D at al , NHJ 2009
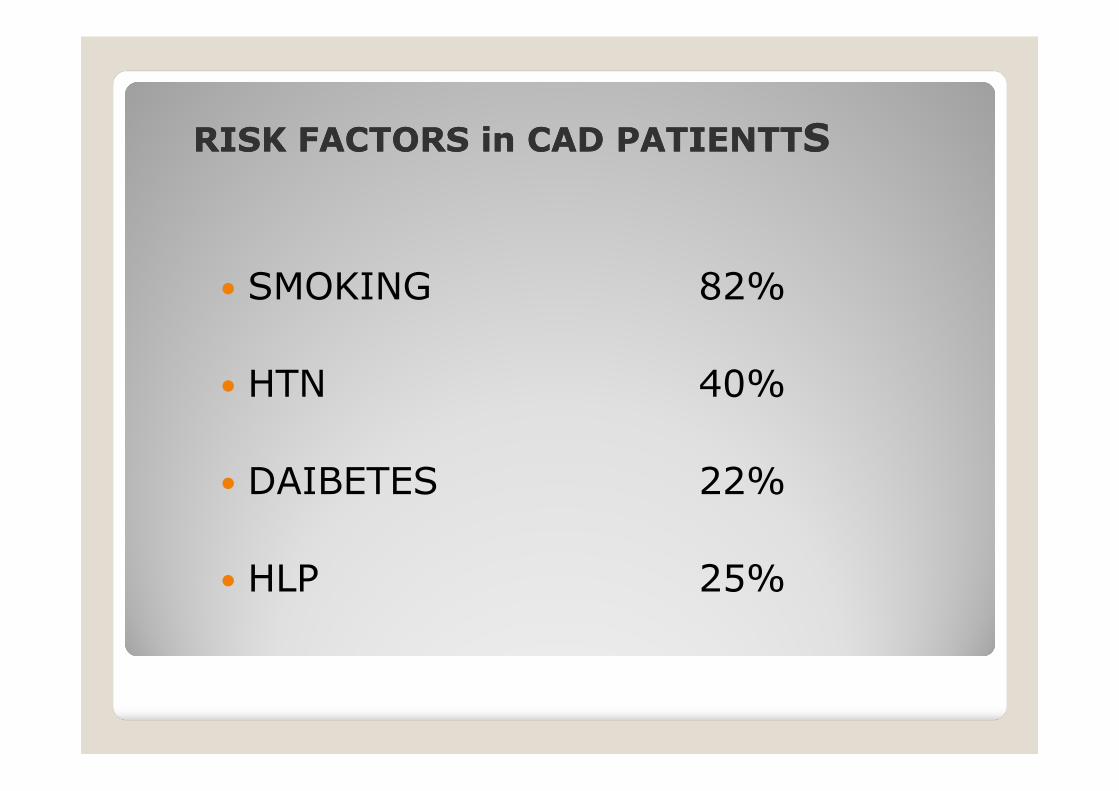
RISK FACTORS in CAD PATIENTTRISK FACTORS in CAD PATIENTTSS
� SMOKING 82%
� HTN 40%� HTN 40%
� DAIBETES 22%
� HLP 25%
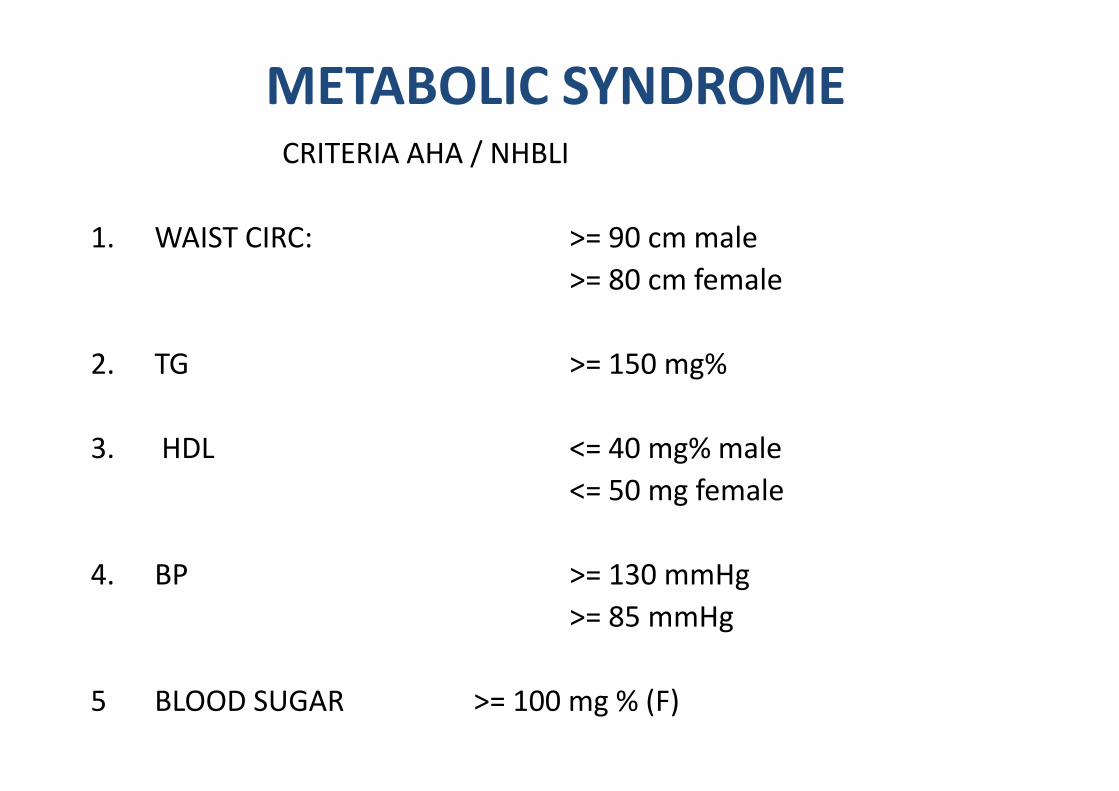
METABOLIC SYNDROMECRITERIA AHA / NHBLI
1. WAIST CIRC: >= 90 cm male
>= 80 cm female
2. TG >= 150 mg%
3. HDL <= 40 mg% male
<= 50 mg female
4. BP >= 130 mmHg
>= 85 mmHg
5 BLOOD SUGAR >= 100 mg % (F)
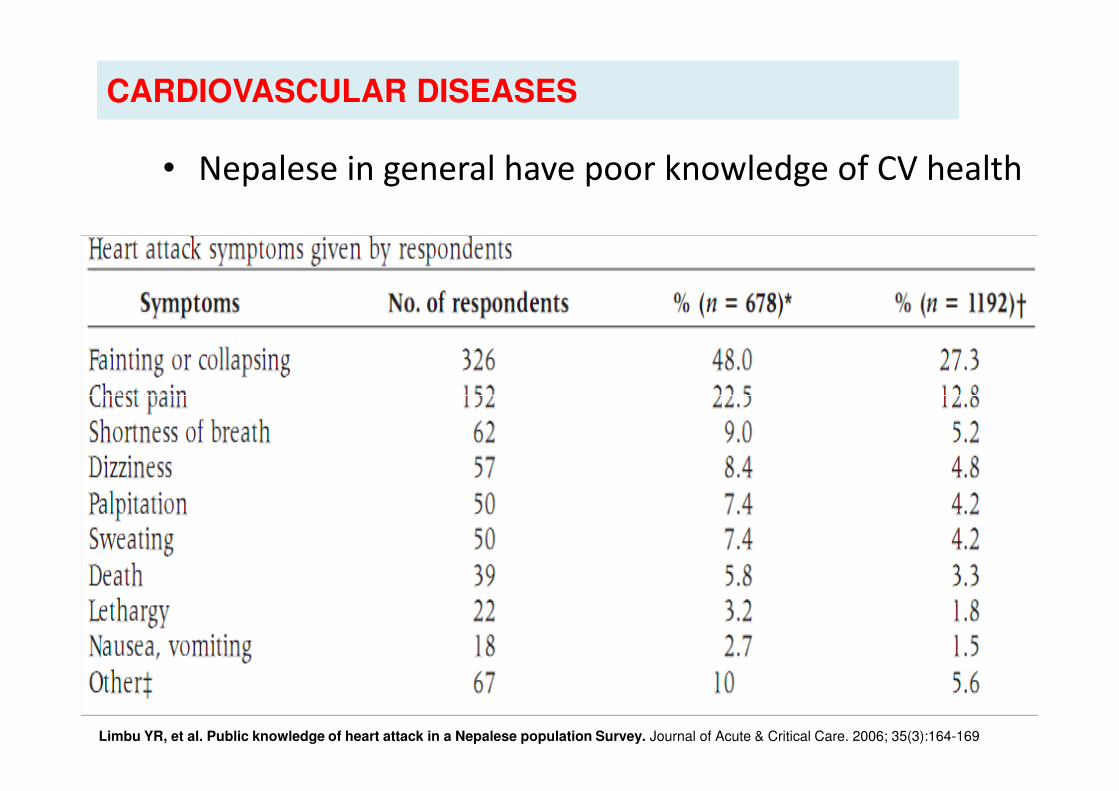
• Nepalese in general have poor knowledge of CV health
CARDIOVASCULAR DISEASES
30
Limbu YR, et al. Public knowledge of heart attack in a Nepalese population Survey. Journal of Acute & Critical Care. 2006; 35(3):164-169
RHEUMATIC HEART DISEASE
PREVALENCE
• RHD: 1.2/1000

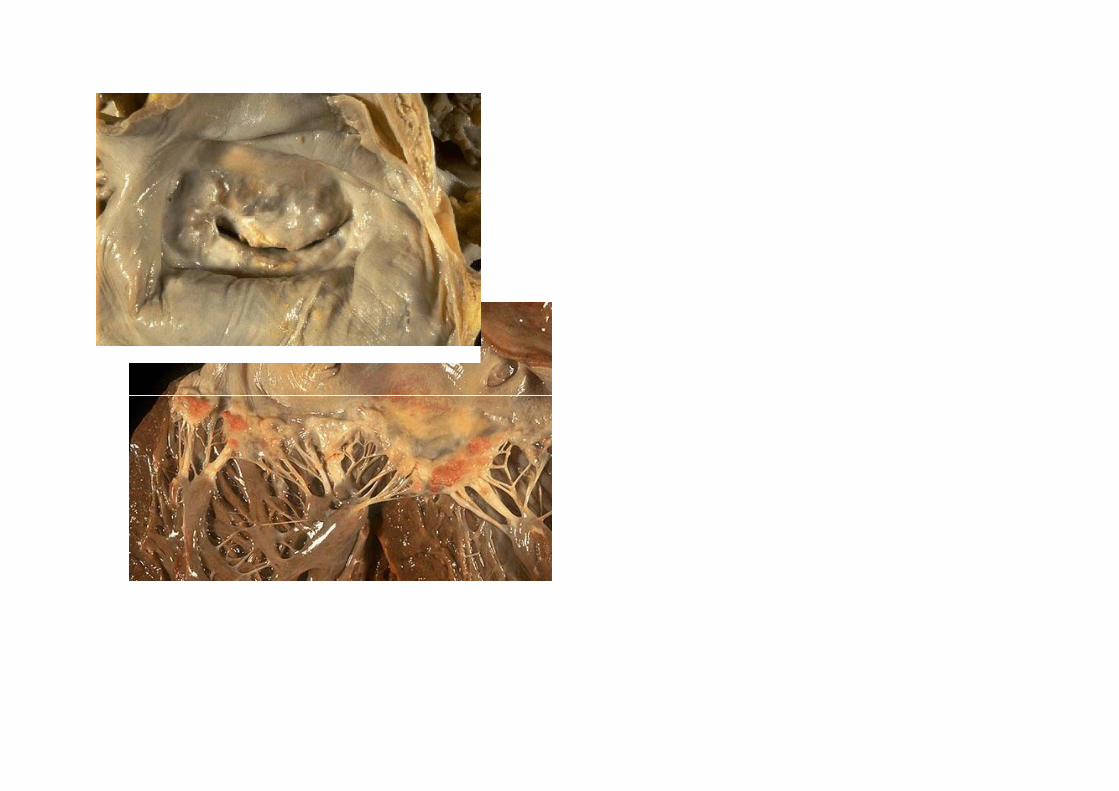
PATTERN OF VALVULAR INVOLVEMENT IN RHD
• N= 9521 RHD CASES
• 2002-2008
• 3867 MALES ( 40.6%)
• 5654 FEMALES (50.4%)
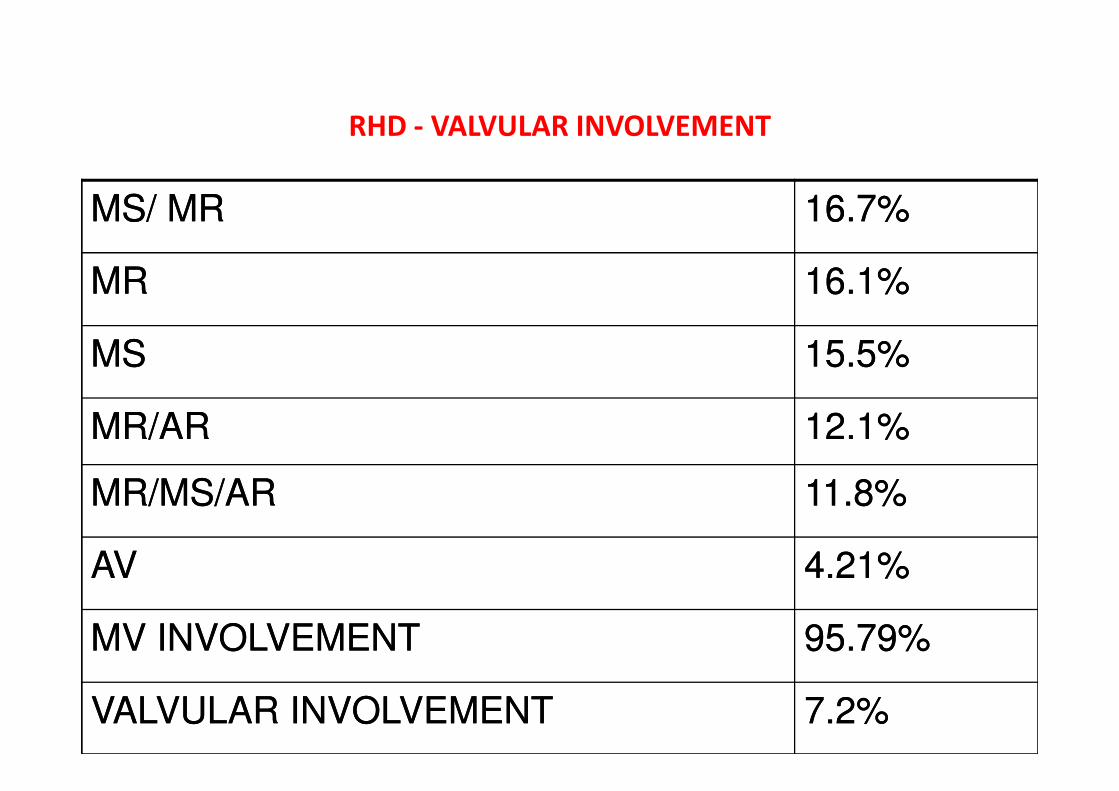
RHD - VALVULAR INVOLVEMENT
MS/ MRMS/ MR 16.7%16.7%
MRMR 16.1%16.1%
MSMS 15.5%15.5%
MR/ARMR/AR 12.1%12.1%
MR/MS/ARMR/MS/AR 11.8%11.8%
AVAV 4.21%4.21%
MV INVOLVEMENTMV INVOLVEMENT 95.79%95.79%
VALVULAR INVOLVEMENTVALVULAR INVOLVEMENT 7.2%7.2%
RHD INTERVENTIONS
• 400 PERCUTANEOUS MITRAL VALVOTOMIES LAST
YEAR
• 1300 SURGERIES DONE LAST YEAR
• 30% WERE RHD CASES
CONGESTIVE HEART FAILURE
• BECOMING COMMONEST DISEASE IN THE
WORLD
• SAME TREND IN OUR COUNTRY
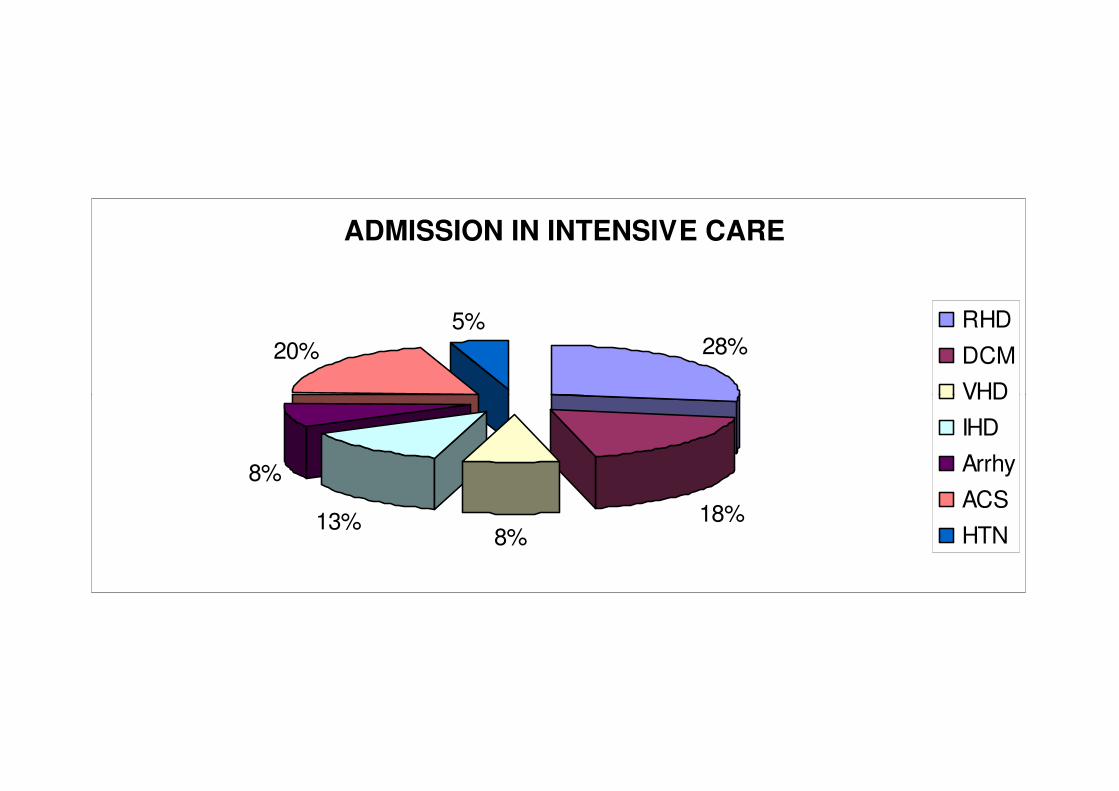
ADMISSION IN INTENSIVE CARE
28%20%
5% RHD
DCM
VHD
18%8%
13%
8%
VHD
IHD
Arrhy
ACS
HTN
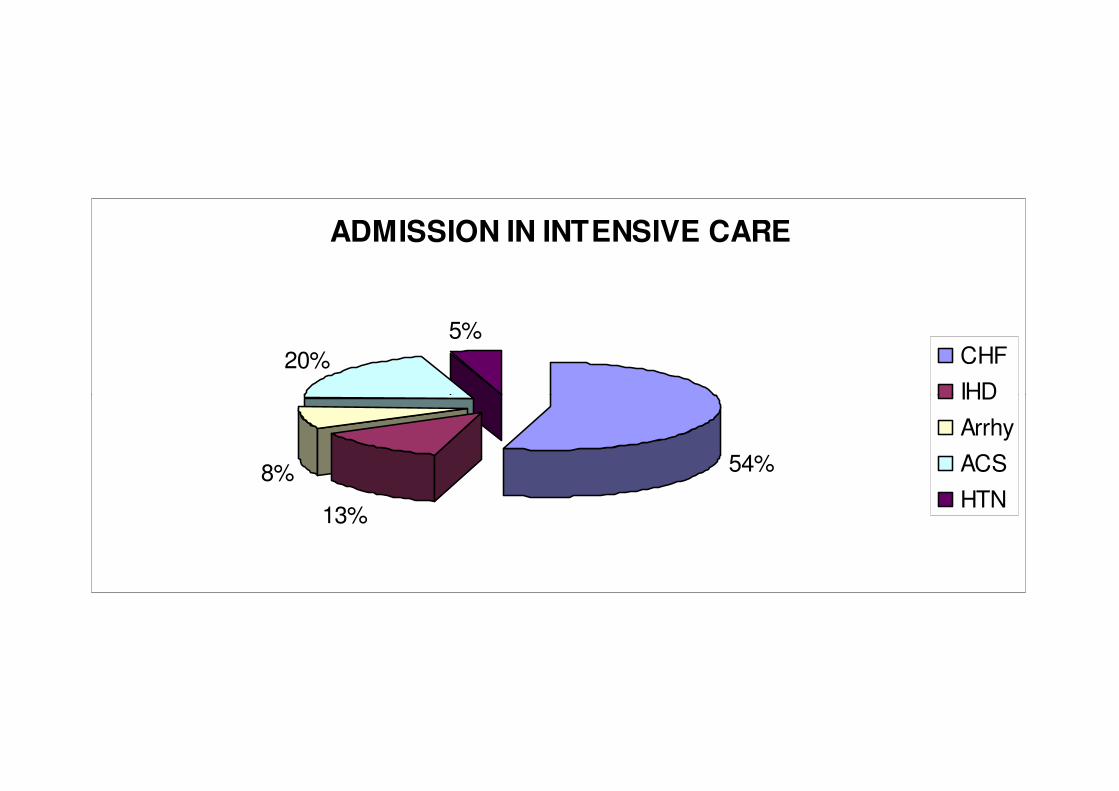
ADMISSION IN INTENSIVE CARE
20%
5%CHF
IHD
54%
13%
8%
IHD
Arrhy
ACS
HTN
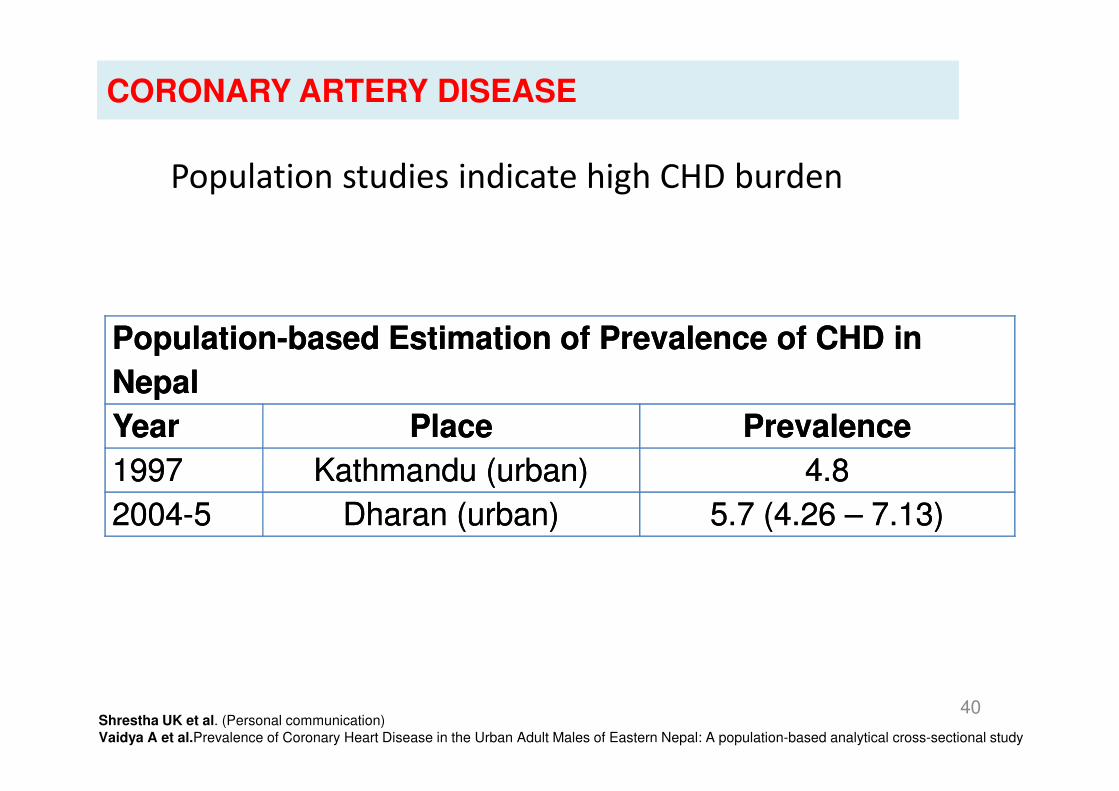
Population studies indicate high CHD burden
PopulationPopulation--based Estimation of Prevalence of CHD in based Estimation of Prevalence of CHD in
NepalNepal
CORONARY ARTERY DISEASE
40
NepalNepal
Year Year PlacePlace Prevalence Prevalence
19971997 Kathmandu (urban)Kathmandu (urban) 4.84.8
20042004--55 Dharan (urban)Dharan (urban) 5.7 (5.7 (4.26 4.26 –– 7.13)7.13)
Shrestha UK et al. (Personal communication)
Vaidya A et al.Prevalence of Coronary Heart Disease in the Urban Adult Males of Eastern Nepal: A population-based analytical cross-sectional study
CORONARY ARTERY DISEASE
Among hospital admissions
• CAD 21.7%
• MALES 74%
• FEMALES 26%
RISK FACTORS in CAD PATIENTTS
• SMOKING 82%
• HTN 40%• HTN 40%
• DAIBETES 22%
• HLP 25%
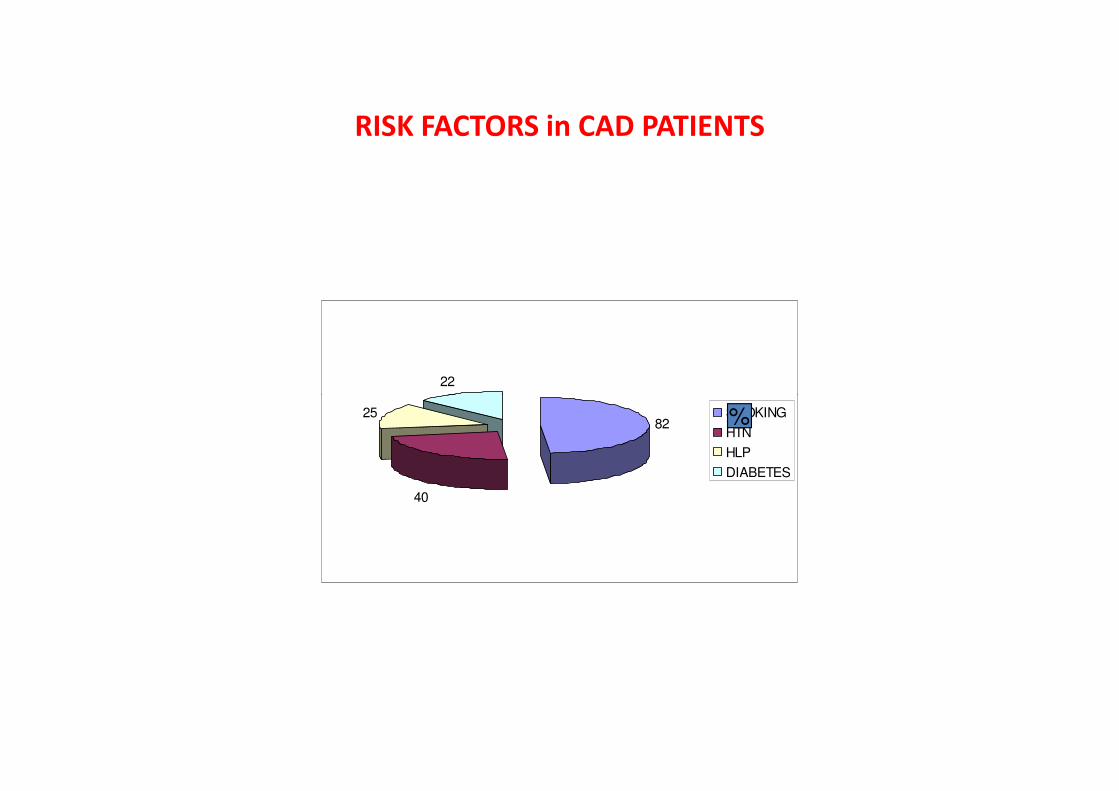
RISK FACTORS in CAD PATIENTS
22
82
40
25 SMOKING
HTN
HLP
DIABETES
%
TRENDS IN CAD
• YOUNGER POPULATION
• NO PREVIOUS ANGINA• NO PREVIOUS ANGINA
• INFERIOR MI FREQUENT CAUSE OF DEATH
CONGENITAL HEART DISEASE
• CONGENITAL HEART DISEASE PREVALENCE
1.3/1000
• COMMONEST LESION ATRIAL SEPTAL DEFECT• COMMONEST LESION ATRIAL SEPTAL DEFECT
• VENTRICULAR SEPTAL DEFECT
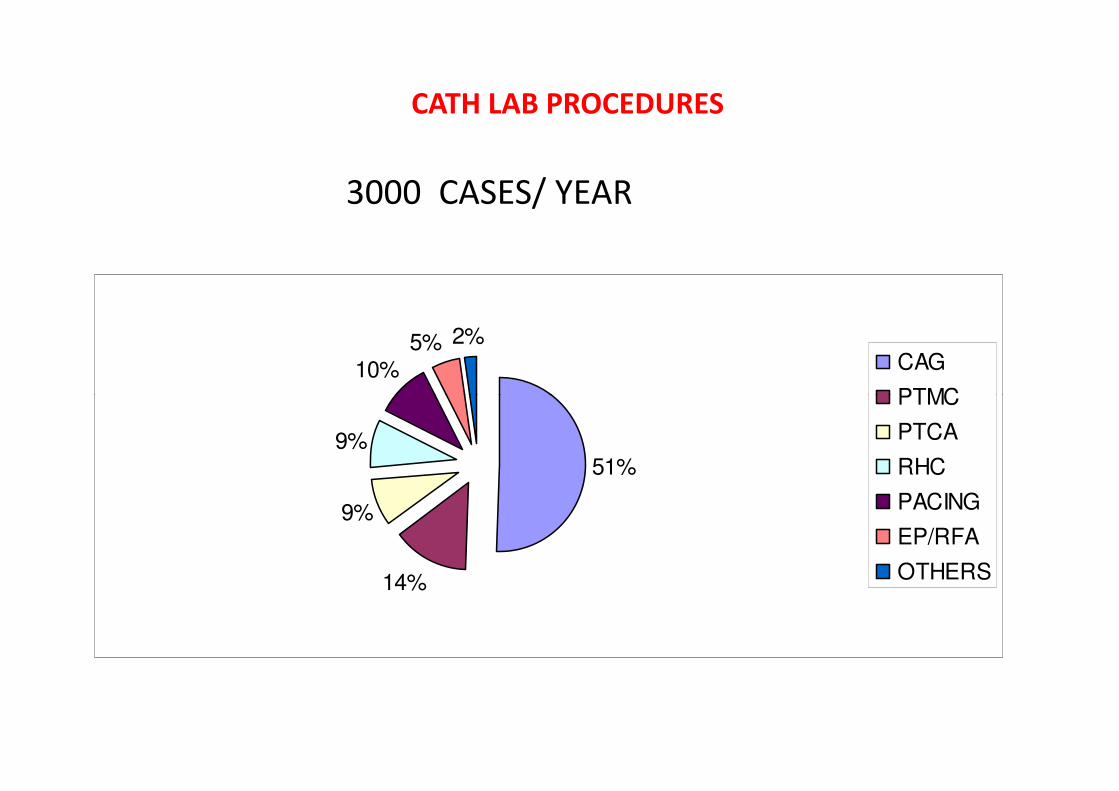
CATH LAB PROCEDURES
3000 CASES/ YEAR
10%5% 2%
CAG
PTMC
51%
14%
9%
9%
PTMC
PTCA
RHC
PACING
EP/RFA
OTHERS
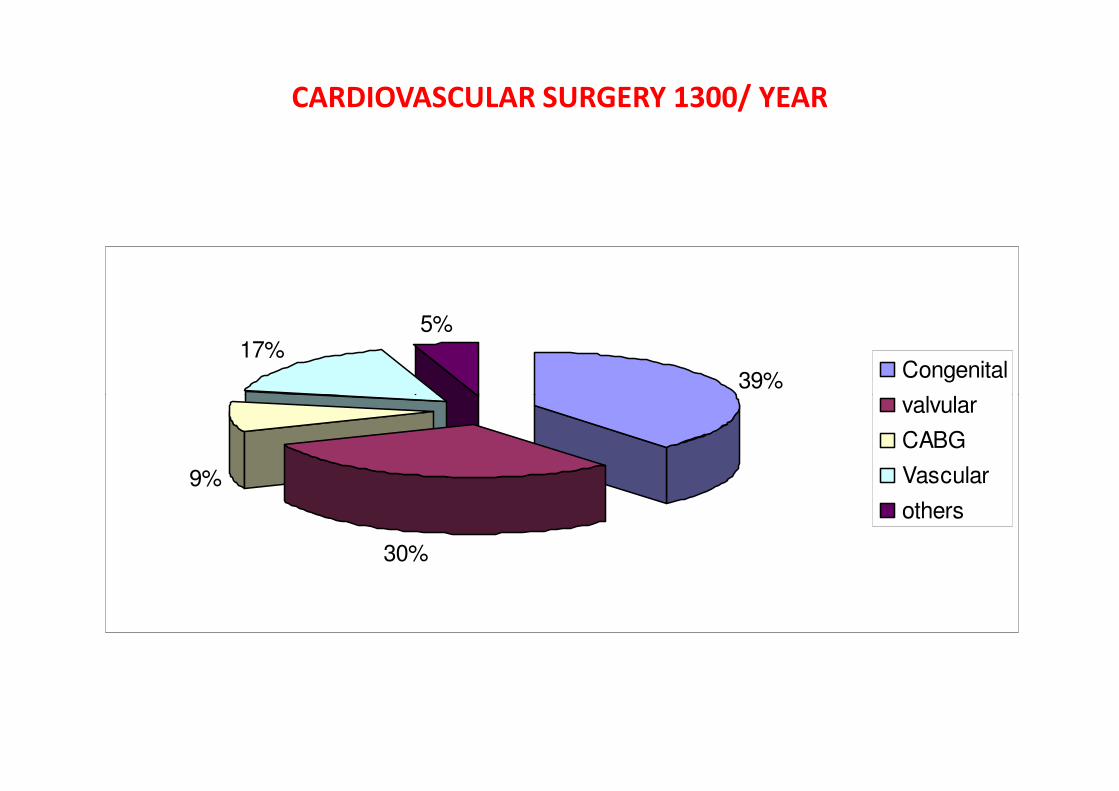
CARDIOVASCULAR SURGERY 1300/ YEAR
39%
17%5%
Congenital
valvular
30%
9%
valvular
CABG
Vascular
others
WHAT ARE WE DOING
• Where advanced health care service is in
accessible.accessible.
RHD
• FREE PENICILLINE PROPHYLAXIS



Problems
• Lack of adequate research on risk factors and other
aspects on CVD
• Lack of intermediate-level manpower
• No national policy/programme on CV diseases• No national policy/programme on CV diseases
• Centralization of specialist heart care
• CVD not included in primary health care system
• Cost of intervention/surgery unaffordable
• Insufficient emphasis on preventive measures
THANK YOU