-
7/29/2019 Sce Acute Med Sample Qs
1/39
Updated 17-Aug-2012
Specialty Certificate in Acute Medicine Sample Questions
Question 141
A 50-year-old woman was admitted with sepsis secondary to
pneumonia. She was treated
with oxygen, intravenous antibiotics and repeated fluid
challenges to a total volume of4.5 L (equivalent to 60 mL/kg) of
sodium chloride 0.9%.
On re-assessment, her pulse was 122 beats per minute, her blood
pressure was82/40 mmHg (mean arterial pressure 54) and her
respiratory rate was 24 breaths perminute. Oxygen saturation was
92% (9499), breathing 40% oxygen. Her central venouspressure was 12
mmHg.
In attempting to restore the blood pressure, what is the most
appropriate intravenoustherapy?
A colloidB dopamineC furosemideD further crystalloidE
noradrenaline (norepinephrine)
-
7/29/2019 Sce Acute Med Sample Qs
2/39
Updated 17-Aug-2012
Question 2
A 73-year-old woman was referred to the acute medical unit for
assessment of herpalpitations. One hour after arriving, she
complained of a return of her palpitations with acentral crushing
chest pain. She became distressed and agitated. She was given
aspirin
and sublingual glyceryl trinitrate. Oxygen was given at 15 L per
minute via a reservoirmask.
On examination, her pulse was thready and hard to count. Her
blood pressure was88/55 mmHg, her respiratory rate was 20 breaths
per minute and her oxygen saturationwas 98% (9499). A cardiac
monitor was attached and showed a narrow-complex
irregulartachycardia with a ventricular rate between 150 and 160
beats per minute. A large-boreintravenous cannula was inserted.
What is the most appropriate next step in management?
A intravenous adenosineB intravenous digoxinC intravenous
flecainideD intravenous verapamilE synchronised cardioversion
-
7/29/2019 Sce Acute Med Sample Qs
3/39
Updated 17-Aug-2012
Question 3
A 77-year-old man presented after a single episode of unilateral
weakness of the left armthat lasted for 2 hours. On examination,
his pulse was 80 beats per minute and regular,and his blood
pressure was 170/100 mmHg. There was no neurological deficit. His
ABCD2
score was 6.
He was given 300 mg of aspirin while awaiting
investigations.
What is his chance of having a stroke in the first week?
A 5%B 10%C 20%D 30%E 40%
-
7/29/2019 Sce Acute Med Sample Qs
4/39
Updated 17-Aug-2012
Question 4
A 43-year-old woman was referred to hospital with a persistent
headache of 4 daysduration. It had come on gradually and had not
been associated with vomiting. Her generalpractitioner had found
her blood pressure to be elevated at 214/118 mmHg and had
arranged emergency admission. She had no other significant
medical history and wastaking no regular medication.
On examination, she appeared well. She had a round face and her
body mass index was32 kg/m2 (1825). Her pulse was 90 beats per
minute and her blood pressure was218/116 mmHg. Peripheral pulses
were normal with no radiofemoral delay. Heart soundswere normal.
Fundoscopy showed grade 2 hypertensive changes but no
papilloedema.Urinalysis showed protein 2+, blood negative, nitrite
negative, leucocytes negative.
Investigations:
12-lead ECG sinus rhythm with changesconsistent with left
ventricularhypertrophy
What is the most likely diagnosis?
A acute glomerulonephritisB cerebral tumourC Cushings syndromeD
essential hypertensionE phaeochromocytoma
-
7/29/2019 Sce Acute Med Sample Qs
5/39
Updated 17-Aug-2012
Topic: SGQuestion 5
A 42-year-old woman presented with a 1-week history of vomiting
and diarrhoea. This hadbegun after she was involved in a road
traffic collision. She also complained of feeling
dizzy on standing. Her family said that she had been slightly
confused and slurred herwords.
On examination, her pulse was 114 beats per minute and her blood
pressure was85/40mmHg.
Investigations:
haemoglobin 116 g/L (115165)
platelet count 364 109/L (150400)
serum sodium 123 mmol/L (137144)serum potassium 6.4 mmol/L
(3.54.9)serum creatinine 123 mol/L (60110)random plasma glucose 2.8
mmol/L
What is the most likely diagnosis?
A autoimmune adrenal failure (Addison's disease)B
gastroenteritisC hypothyroidismD insulinomaE syndrome of
inappropriate antidiuretic hormone
-
7/29/2019 Sce Acute Med Sample Qs
6/39
Updated 17-Aug-2012
Question 6
A 23-year-old man presented after having collapsed in a Chinese
restaurant. He gave ahistory of a previous similar episode after
having eaten nuts. On examination, his pulsewas 120 beats per
minute and his blood pressure was 95/60 mmHg. His chest was
wheezy with an oxygen saturation of 89% (9499).
High-flow oxygen was administered and a dose of adrenaline
(epinephrine) wasrequested.
In what dose and by what route should adrenaline (epinephrine)
be given?
A 500 g intramuscularlyB 500 g intravenouslyC 1 mg
intramuscularlyD 1 mg intravenously
E 10 mg intravenously
-
7/29/2019 Sce Acute Med Sample Qs
7/39
Updated 17-Aug-2012
Question 7
A 32-year-old man presented with a 3-week history of headaches,
fever, sore throat,myalgia, anorexia and generalised non-pruritic
rash. He had no other significant medicalhistory and had not been
given a blood transfusion in the past.
On examination, vital signs were normal except for a temperature
of 37.4C. Enlargednon-tender lymph nodes were noted in the axillae,
submandibular areas and both groins.Throat examination was normal.
He had no meningeal signs and detailedcardiorespiratory, abdominal
and neurological examinations were normal. Generalisedmaculopapular
rash was noted.
Investigations:
heterophil antibody test negative
blood film atypical lymphocytosis
What is the most likely diagnosis?
A cytomegalovirus infectionB group A streptococcus infectionC
HIV seroconversionD secondary syphilisE toxoplasmosis
-
7/29/2019 Sce Acute Med Sample Qs
8/39
Updated 17-Aug-2012
Question 8
A 70-year-old man was admitted to hospital with severe shortness
of breath. He had ahistory of emphysema. On examination, he had
diminished breath sounds over the leftside of the chest.
Investigations:
chest X-ray large left pneumothorax
What is the most appropriate next step in management?
A insert 14F drain immediately above a rib marginB insert 14F
drain immediately below a lower rib marginC insert 14F drain in the
scalene triangleD insert 28F drain immediately below a lower rib
margin
E insert 28F drain in the scalene triangle
-
7/29/2019 Sce Acute Med Sample Qs
9/39
Updated 17-Aug-2012
Question 9
A 72-year-old man was admitted with community-acquired
pneumonia. He had permanentatrial fibrillation and was taking
digoxin. He had been treated with high-flow oxygen andintravenous
benzylpenicillin and clarithromycin.
On examination, his pulse was 120 beats per minute and
irregular, and his blood pressurewas 90/60 mmHg. His capillary
refill time was 3 seconds. His respiratory rate was 24breaths per
minute and oxygen saturation was 98% (9499), breathing 4 L/min
oxygen viaa simple face mask.
What is the most appropriate management of his haemodynamic
state?
A intravenous amiodaroneB intravenous digoxinC intravenous
magnesium
D intravenous sodium chloride 0.9%E synchronised
cardioversion
-
7/29/2019 Sce Acute Med Sample Qs
10/39
Updated 17-Aug-2012
Question 10
A 48-year-old man with a history of alcohol dependency was
admitted with confusion. Onexamination, he was unkempt and showed
signs of poor nutrition. He had cool peripheries.His temperature
was 35.6C and his blood pressure was 86/58 mmHg. He had mild
dysdiadochokinesis but no evidence of ophthalmoplegia or
nystagmus. His capillary bloodglucose concentration was 2.6
mmol/L.
Intravenous access was established and he was immediately
treated with glucose 10%250 mL and vitamins B and C (Pabrinex) by
intravenous infusion. His blood pressureimproved to 106/80 mmHg and
his capillary glucose to 4.9 mmol/L. He became moredrowsy. His
neurological condition was noted to have deteriorated by the
nursing staff.They re-checked his capillary glucose, which was 3.5
mmol/L. His blood pressure was98/68 mmHg.
What is the most appropriate next management step?
A CT scan of headB intravenous co-amoxiclavC intravenous sodium
chloride 0.9%D repeat intravenous glucose 10% 250 mLE repeat
vitamins B and C (Pabrinex) by intravenous infusion
-
7/29/2019 Sce Acute Med Sample Qs
11/39
Updated 17-Aug-2012
Question 11
A 29-year-old woman was brought to hospital by ambulance. She
had been foundunconscious by her husband with imipramine tablets by
her bed. On arrival in thedepartment she had a tonicclonic seizure,
which lasted for 2 minutes. She was otherwise
fit and well.
Investigations:
ECG broad-complex tachycardia
What is the most appropriate immediate treatment?
A amiodaroneB DC cardioversionC lorazepam
D phenytoinE sodium bicarbonate
-
7/29/2019 Sce Acute Med Sample Qs
12/39
Updated 17-Aug-2012
Question 12
A 72-year-old woman presented with a 4-day history of
palpitations. She had notexperienced any dyspnoea or chest
discomfort and was not distressed by the palpitations.Her general
practitioner had noted rapid atrial fibrillation and referred her
for assessment.
She had type 2 diabetes mellitus and hypertension but no other
significant medical history.Her medication comprised irbesartan,
gliclazide, amlodipine and simvastatin.
On examination, she was comfortable. Her pulse was 130 beats per
minute, her bloodpressure was 138/82 mmHg and her respiratory rate
and oxygen saturation were normal.Her heart sounds were normal and
her chest was clear. She had no oedema.
Investigations:
haemoglobin 146 g/L (115165)
platelet count 164 109/L (150400)
serum sodium 143 mmol/L (137144)serum potassium 4.4 mmol/L
(3.54.9)serum creatinine 123 mol/L (60110)
plasma thyroid-stimulating hormone 3.2 mU/L (0.45.0)
12-lead ECG atrial fibrillation with rapid
ventricularresponse
What is the most appropriate next step in management?
A DC cardioversionB intravenous digoxinC intravenous flecainideD
oral bisoprololE oral digoxin
-
7/29/2019 Sce Acute Med Sample Qs
13/39
Updated 17-Aug-2012
Question 13
A 54-year-old man was referred to the rapid access chest pain
clinic for assessment.Based on a thorough history, his likelihood
of coronary artery disease was calculated to be
25%.
What is the most appropriate investigation?
A cardiac stress echocardiographyB CT coronary angiographyC CT
coronary artery calcium scoringD invasive coronary angiographyE
myocardial perfusion imaging
-
7/29/2019 Sce Acute Med Sample Qs
14/39
Updated 17-Aug-2012
Question 14
A 53-year-old woman was admitted to the emergency department
following a tonicclinicseizure at home. Her husband, who was with
her, said that she had developed a suddensevere headache while
doing the washing up about 2 hours previously. She had gone to
bed because of the severity of the pain and he had found her
convulsing.
On arrival, she was not convulsing but her Glasgow coma score
was 10. Her temperaturewas 36.9C, her pulse was 85 beats per minute
and her blood pressure was 168/93mmHg. Fundal examination was
normal. Tone and reflexes in her limbs were normal.Neck stiffness
was present.
Investigations:
CT scan of head see image
What is the most appropriate next investigation?
A blood culture
B CT cerebral angiography
C lumbar puncture 12 h after headache onset
D lumbar puncture immediatelyE MR cerebral angiography
-
7/29/2019 Sce Acute Med Sample Qs
15/39
Updated 17-Aug-2012
Question 15
A 67-year-old man was admitted with chest pain. He had recently
returned from atransatlantic holiday. He smoked heavily and his
alcohol consumption was 40 unitsweekly. He had no past medical
history of note and was taking no medication.
On examination, his temperature was 37.5C, his pulse was 90
beats per minute and hisblood pressure was 160/96 mmHg. His
respiratory rate was 30 breaths per minute and hisoxygen saturation
was 90% (9499) breathing air. There were crackles over the right
lungbase.
Investigations:
chest X-ray see image
ECG flat T waves in V1, V2, V3
He was treated with oral amoxicillin.
What is the most appropriate next step?
A assess clinical probability score for pulmonary
thromboembolismB CT pulmonary angiographyC D-dimer concentrationD
serum troponin I test
E ventilation/perfusion isotope scan of lung
-
7/29/2019 Sce Acute Med Sample Qs
16/39
Updated 17-Aug-2012
Question 16
A 32-year-old woman was admitted with a 7-day history of nausea,
sparse bloodstaineddiarrhoea and cramping lower abdominal pains.
She was feeling increasingly exhaustedand short of breath.
On examination, she appeared pale and mildly icteric, with ankle
oedema. There was apetechial rash over her face. Her temperature
was 37.2C, her pulse was 104 beats perminute and regular, and her
blood pressure was 160/92 mmHg. No neurologicalabnormality was
identified. Urinalysis was positive for blood and protein.
Investigations:
haemoglobin 70 g/L (115165)
platelet count 56 109/L (150400)prothrombin time 18.0 s
(11.515.5)
activated partial thromboplastin time 46 s (3040)
serum sodium 139 mmol/L (137144)serum urea 37.0 mmol/L
(2.57.0)serum creatinine 440 mol/L (60110)serum total bilirubin 63
mol/L (122)serum lactate dehydrogenase 2600 U/L (10250)
What is the most likely underlying diagnosis?
A acute lymphatic leukaemiaB disseminated intravascular
coagulationC haemolytic uraemic syndromeD idiopathic
thrombocytopenic purpuraE thrombotic thrombocytopenic purpura
-
7/29/2019 Sce Acute Med Sample Qs
17/39
Updated 17-Aug-2012
Question 17
A 70-year-old woman was admitted with chest and upper abdominal
pain associated withsweating. She described the pain as having
intensity 8/10. She had been previously fit andwell.
On examination, her pulse was 82 beats per minute and her blood
pressure was 168/94mmHg in the right arm and 156/88 in the left.
Her respiratory rate was 15 breaths perminute and oxygen saturation
was 95% (9498), breathing air. There were no heartmurmurs and the
chest was clinically normal. There was epigastric tenderness.
Initial investigations showed a normal full blood count, normal
electrolytes and creatinine,and normal serum C-reactive protein.
Her ECG was normal. A chest X-ray was performed(see image).
A working diagnosis of dyspepsia was made. Early the following
morning, she had a
cardiac arrest and died.
What is most likely to have caused her death?
A aortic dissection
B massive gastrointestinal bleedingC perforated duodenal ulcerD
pulmonary embolismE tension pneumothorax
-
7/29/2019 Sce Acute Med Sample Qs
18/39
Updated 17-Aug-2012
Question 18
A 47-year-old man presented with an acutely painful right ankle,
shivering and mild fever.He was unable to bear weight. He had no
history of joint problems but was takingtreatment for
hypertension.
On examination, his temperature was 37.4C. He was overweight and
had a swollen rightankle with erythema over the joint.
What is the most important investigation?
A blood cultureB joint fluid examinationC serum C-reactive
proteinD serum urateE X-ray of ankle
-
7/29/2019 Sce Acute Med Sample Qs
19/39
Updated 17-Aug-2012
Question 19
A 24-year-old woman was admitted complaining of feeling unwell.
She had returned from a2-month tour of Malaysia the previous week.
She complained of a severe headache, whichwas worse behind the
eyes, and sore muscles, especially in her back, arms and legs.
She
had also had an intermittent fever for 3 days. She had no past
medical history of note, andher only medication was the combined
oral contraceptive.
On examination, she was suntanned, with a temperature of 38.5C,
a pulse of 76 beatsper minute and a blood pressure of 95/60 mmHg.
She had some palpable lymph nodes inthe axillae and inguinal
regions, but no other abnormality was detected.
Investigations:
haemoglobin 144 g/L (115165)
white cell count 1.8 109/L (4.011.0)
neutrophil count 0.6 109/L (1.57.0)
lymphocyte count 0.9 109/L (1.54.0)
monocyte count 0.4 109/L (
-
7/29/2019 Sce Acute Med Sample Qs
20/39
Updated 17-Aug-2012
Question 20
A 48-year-old man presented with a short history of fever,
headache and confusion. Hehad a history of type 2 diabetes
mellitus.
On examination, his temperature was 40.1C, his pulse was 103
beats per minute and hisblood pressure was 87/52 mmHg. His Glasgow
coma score was 9. His neck was stiff andhe had photophobia.
A CT scan of head was normal. He was given intravenous
fluids.
Investigations:
cerebrospinal fluid:total protein 1.80 g/L (0.150.45)glucose 1.9
mmol/L (3.34.4)
cell count 2100/L (5)lymphocyte count 100/L (3)neutrophil count
2000/L (0)Gram stain negative
In addition to cefotaxime, what is the most appropriate
treatment?
A aciclovirB amphotericinC chloramphenicolD dexamethasoneE
vancomycin
-
7/29/2019 Sce Acute Med Sample Qs
21/39
Updated 17-Aug-2012
Question 21
A 40-year-old man was brought to the emergency department by his
friends. He wasthought to have ingested an unknown medication in a
suicide attempt.
On examination, he was disorientated in time. His temperature
was 39.3C, his pulse was100 beats per minute and irregular, his
blood pressure was 120/85 mmHg and hisrespiratory rate was 22
breaths per minute. His skin was flushed and dry. On
physicalexamination, he was noted to have dilated pupils and muscle
twitching. There was noapparent neurological abnormality.
Investigations:
arterial blood gases, breathing air:PO2 12.0 kPa (11.312.6)PCO2
4.1 kPa (4.76.0)
pH 7.36 (7.357.45)H+ 44 nmol/L (3545)bicarbonate 27 mmol/L
(2129)oxygen saturation 96% (9498)
ECG sinus tachycardiaPR interval 145 ms (120200)QRS complex 128
ms (40120)
Ingestion of what substance is most likely to have resulted in
these findings?
A citalopramB dosulepinC ethyl alcoholD lithium citrateE
venlafaxine
-
7/29/2019 Sce Acute Med Sample Qs
22/39
Updated 17-Aug-2012
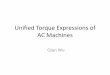
Question 22
A 74-year-old woman was admitted to hospital at 04.00 h, having
suddenly woken fromsleep with a feeling of severe anxiety,
breathlessness and suffocation. She felt she hadneeded to sit
upright in bed and had become extremely breathless very rapidly.
She had
not suffered chest pain. She had a history of an uncomplicated
anterior myocardialinfarction 6 years previously. Hypertension had
been diagnosed 10 years previously, andshe had occasional angina
when walking up a hill on a cold day. She had mild asthma, butwas
taking no regular treatment. Her treatment included aspirin,
simvastatin, furosemide,ramipril and amlodipine. She needed to use
a nitrate spray only once or twice a month.
On examination, she was apyrexial. She had oedema of both lower
limbs to her knees.Her pulse was 35 beats per minute and irregular,
and her blood pressure was 86/48mmHg. Her jugular venous pressure
was elevated to the level of her earlobes while sittingat 45
degrees. There was a gallop rhythm on auscultation of the heart,
and crackles wereheard at both lung bases.
Investigations:
haemoglobin 109 g/L (115165)
serum sodium 129 mmol/L (137144)serum potassium 7.2 mmol/L
(3.54.9)serum urea 14.9 mmol/L (2.57.0)serum creatinine 168 mol/L
(60110)
ECG see images a and b
Image a
-
7/29/2019 Sce Acute Med Sample Qs
23/39
Updated 17-Aug-2012
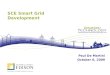
Image b
What is the most appropriate initial treatment?
A intravenous atropineB intravenous calciumC intravenous
dobutamineD intravenous insulin and glucoseE nebulised
salbutamol
-
7/29/2019 Sce Acute Med Sample Qs
24/39
Updated 17-Aug-2012
Question 23
A 62-year-old man presented with chest pain. A few minutes after
arrival he suffered acardiopulmonary arrest. Basic life support was
started without delay. After 2 minutes ofchest compressions the
cardiac rhythm was as shown (see image). Defibrillation was
attempted but there was no change in the rhythm. After a further
2 minutes of basic lifesupport there was still no palpable carotid
pulse and no change in rhythm. One furthershock was delivered
without beneficial effect. A further 2 minutes of basic life
support wasperformed. The cardiac monitor showed that the rhythm
was unchanged and there wasstill no carotid pulse.
What is the most appropriate intervention?
A further shockB intravenous adrenaline (epinephrine)C
intravenous amiodaroneD intravenous magnesium sulphateE intravenous
sodium bicarbonate 8.4%
-
7/29/2019 Sce Acute Med Sample Qs
25/39
Updated 17-Aug-2012
Question 24
A 19-year-old man was brought to hospital after collapsing
during a national marathonrace. He had enjoyed good health in the
past. There was no family history of suddencardiac death.
Attempts to resuscitate him failed. Post-mortem examination
revealed the cause of death.
What is the most likely cause of death?
A anomalous coronary arteryB aortic stenosisC arrhythmogenic
right ventricular dysplasiaD hypertrophic obstructive
cardiomyopathyE ischaemic heart disease
-
7/29/2019 Sce Acute Med Sample Qs
26/39
Updated 17-Aug-2012
Question 25
A 23-year-old man presented to the acute medicine unit at 20.00
h with a 2-week history ofexcessive thirst, urinary frequency and
some weight loss. His general practitioner hadfound his random
blood glucose to be 25.0 mmol/L.
On examination, his pulse was 80 beats per minute and his blood
pressure was 120/70mmHg. He had normal skin turgor and capillary
refill. His abdomen was soft, and nottender. His body mass index
was 22 kg/m2 (1825). Urinalysis showed ketones 1+.
Investigations:
serum sodium 143 mmol/L (137144)serum potassium 4.2 mmol/L
(3.54.9)serum bicarbonate 22 mmol/L (2028)serum urea 5.2 mmol/L
(2.57.0)
serum creatinine 75 mol/L (60110)random plasma glucose 26.0
mmol/L
What is the most appropriate next management step?
A intravenous insulin and admit for observationB long-acting
insulin and admit for observationC long-acting insulin and
discharge for review next dayD short-acting insulin and admit for
observationE short-acting insulin and discharge for review next
day
-
7/29/2019 Sce Acute Med Sample Qs
27/39
Updated 17-Aug-2012
Question 26
A 72-year-old man presented after having vomited bright-red
blood the previous day. Hehad no significant medical history and
was taking no regular medication. He was a smokerand admitted to
consuming roughly 20 units of alcohol per week.
On examination, his pulse was 105 beats per minute, his blood
pressure was 110/65mmHg, his heart sounds were normal and his chest
was clear. His abdomen was soft butmildly tender.
Investigations:
haemoglobin 101 g/L (130180)MCV 102 fL (8096)
serum sodium 134 mmol/L (137144)
serum potassium 4.1 mmol/L (3.54.9)serum urea 8.1 mmol/L
(2.57.0)serum creatinine 85 mol/L (60110)
Upper gastrointestinal endoscopy the next morning showed a
gastric ulcer with adherentblood clot.
What is the likelihood of a further significant bleed?
A 7%B 14%C 25%D 35%E 55%
-
7/29/2019 Sce Acute Med Sample Qs
28/39
Updated 17-Aug-2012
Question 27
A 48-year-old man presented with vomiting followed by streaks of
haematemesis. He hadbeen self-medicating with diclofenac for
abdominal pain.
On examination, his pulse was 120 beats per minute and
irregularly irregular, and hisblood pressure was 140/60 mmHg. The
abdomen was mildly distended. Dullness over theliver was reduced.
Bowel sounds were present.
Investigations:
haemoglobin 160 g/L (130180)
white cell count 14.4 109/L (4.011.0)
serum sodium 145 mmol/L (137144)serum potassium 3.5 mmol/L
(3.54.9)
serum chloride 104 mmol/L (95107)serum bicarbonate 20 mmol/L
(2028)serum urea 12.0 mmol/L (2.57.0)serum creatinine 110 mol/L
(60110)
X-ray of abdomen see image
What is the most likely diagnosis?
A drug-induced gastritisB ischaemic bowelC MalloryWeiss tearD
perforated viscusE volvulus
-
7/29/2019 Sce Acute Med Sample Qs
29/39
Updated 17-Aug-2012
Question 28
A 48-year-old man developed breathlessness, non-productive cough
and fever with chillswithin 6 hours of starting a blood transfusion
(on the second unit). He had been admittedwith gastrointestinal
bleeding as a result of peptic ulcer disease. He had no
significant
medical history.
On examination, his temperature was 37.8C, his pulse was 100
beats per minute andregular, his blood pressure was 90/70 mmHg and
his respiratory rate was 30 breaths perminute. His oxygen
saturation breathing maximal high-flow oxygen was 85%.
Investigations:
ECG sinus tachycardia; 100 beats perminute
chest X-ray bilateral nodular infiltrates with batswing
pattern
The transfusion was discontinued.
What is the most appropriate next step in management?
A intravenous chlorphenamineB intravenous furosemideC
intravenous hydrocortisoneD mechanical ventilationE non-invasive
ventilation
-
7/29/2019 Sce Acute Med Sample Qs
30/39
Updated 17-Aug-2012
Question 29
A 20-year-old woman was admitted with a 2-day history of
headache, photophobia andfever. There were no other symptoms and
she had no other medical history. Onexamination, she had signs of
meningism. She was alert, her vital signs were normal and
there was no papilloedema. A lumbar puncture was planned.
What is the most appropriate type of needle to use?
A 16G Quinckes (bevelled) needleB 18G Quinckes (bevelled)
needleC 18G Sprotte (atraumatic) needleD 22G Quinckes (bevelled)
needleE 22G Sprotte (atraumatic) needle
-
7/29/2019 Sce Acute Med Sample Qs
31/39
Updated 17-Aug-2012
Question 30
A 58-year-old man was admitted with a history of occipital
headache of sudden onsetassociated with nausea, vomiting, vertigo,
double vision and slurred speech.
On examination, he was confused and had mild dysarthria. There
was no neck stiffness.He had normal tone and power in his limbs
with normal reflexes. Sensation seemednormal but was hard to assess
because of his confusion.
Investigations:
unenhanced CT scan of head see image
What is the most appropriate interpretation of the scan
appearance?
A basilar artery thrombosisB cerebral infarctionC lacunar
infarct
D no abnormalityE subarachnoid haemorrhage
-
7/29/2019 Sce Acute Med Sample Qs
32/39
Updated 17-Aug-2012
Question 31
A 43-year-old man was admitted with a 4-day history of
progressive leg weakness andpoorly localised lower back pain.
On examination, he had reduced tone in both lower limbs, with
grade 4 power of flexionand extension of hips and knees
bilaterally, and grade 3 power of foot dorsiflexion andplantar
flexion bilaterally. His deep tendon reflexes in the lower limbs
were absent, and theplantar responses were flexor. There was loss
of all modalities of sensation in both feet ina stocking
distribution. Examination of the upper limbs was normal.
What respiratory function variable is it most important to
measure regularly?
A forced expiratory volume in 1 s
B oxygen saturation
C peak expiratory flow
D respiratory rate
E vital capacity
-
7/29/2019 Sce Acute Med Sample Qs
33/39
Updated 17-Aug-2012
Question 32
A 32-year-old woman was referred with a 3-week history of a
left-sided headache. Thishad not interfered with her life until the
previous 2 days when she had also developedslight nausea and some
weakness of her right hand.
On examination, she looked well and her temperature was 36.8C.
Her pulse was 68 beatsper minute and her blood pressure was 135/75
mmHg. Cranial nerve examination wasnormal and there was no
papilloedema. Power in her right arm was grade 4/5. Her rightbiceps
reflex was brisker than the left, and there was reflex spread.
Sensation was normal.
Investigations:
MR scan of brain (T2 weighted) see image
What is the most appropriate diagnostic investigation?
A blood cultureB HIV testC open biopsyD PETCT scanE toxoplasma
serology
-
7/29/2019 Sce Acute Med Sample Qs
34/39
Updated 17-Aug-2012
Question 33
A 60-year-old woman was admitted with deterioration in her renal
function. She had ahistory of type 2 diabetes mellitus,
hypertension and chronic kidney disease stage 3a, withan estimated
glomerular filtration rate (MDRD) of 4560 mL/min (>60). She was
taking
perindopril for hypertension, and had recently started taking
celecoxib for osteoarthritis.
What best describes the mechanism of her celecoxib-induced
deterioration in renalfunction?
A hypersensitivity reactionB inhibition of afferent arteriole
vasodilatationC interstitial nephritisD renal parenchymal
infarctionE renal tubular acidosis
-
7/29/2019 Sce Acute Med Sample Qs
35/39
Updated 17-Aug-2012
Question 34
A 68-year-old man with chronic obstructive pulmonary disease
presented with a 24-hourhistory of increased wheeze and
breathlessness. He was treated with nebulisedsalbutamol 2.5 mg and
ipratropium 500 micrograms, oral prednisolone 30 mg and 28%
oxygen via a Venturi mask.
On examination, his pulse was 84 beats per minute and his blood
pressure was 146/88mmHg. His respiratory rate was 24 breaths per
minute. He had polyphonic wheezethroughout both lung fields.
Investigations:
chest X-ray hyperexpanded lungs consistentwith emphysema; no
consolidation orpulmonary oedema
arterial blood gases, 1 h after admission, breathing FiO2
0.28:PO2 7.4 kPaPCO2 7.1 kPa (4.76.0)pH 7.28 (7.357.45)H+ 53 nmol/L
(3545)bicarbonate 24 mmol/L (2129)oxygen saturation 84%
What is the most appropriate next step in management?
A bilevel positive airway pressure ventilationB increase oxygen
to FiO2 0.35C intravenous aminophyllineD intravenous
hydrocortisoneE reduce oxygen to FiO2 0.24
-
7/29/2019 Sce Acute Med Sample Qs
36/39
Updated 17-Aug-2012
Question 35
A 74-year-old woman was admitted with an exacerbation of chronic
obstructive pulmonarydisease. She had been admitted three times in
the previous 9 months. She was using asalbutamol inhaler.
On examination, her oxygen saturation was 94% (9498) breathing
air.
What change in her management is most likely to reduce the
number of furtherexacerbations?
A addition of tiotropium bromideB long-term domiciliary oxygenC
long-term low-dose prednisoloneD pneumococcal vaccineE regular
nebulised salbutamol
-
7/29/2019 Sce Acute Med Sample Qs
37/39
Updated 17-Aug-2012
Question 36
A discussion took place on how to improve the management of
patients presenting withdiabetic ketoacidosis and development of a
diabetic ketoacidosis care bundle wassuggested.
What best describes a care bundle?
A a checklist of medical and nursing interventions designed to
ensure all steps arecompleted
B a series of processes that must be completed to ensure patient
safetyC a small group of evidence-based processes that, when
performed collectively, improve
outcomesD a small group of interventions that define minimum
care standardsE steps in patient management that must be completed
sequentially within a defined timeperiod
-
7/29/2019 Sce Acute Med Sample Qs
38/39
Updated 17-Aug-2012
Question 37
A 65-year-old woman presented with an acute stroke with aphasia
and flaccid paralysis ofthe left side. She had a history of heart
failure. On examination, her oxygen saturation was94% (9498)
breathing air.
What is the most appropriate treatment?
A 2 L oxygen via nasal cannulaeB 5 L oxygen via simple face
maskC 15 L oxygen via reservoir bag maskD 28% oxygen via Venturi
maskE no additional oxygenF
-
7/29/2019 Sce Acute Med Sample Qs
39/39
Answers:
1 E2 E3 B
4 D5 A6 A7 C8 A9 D10 D11 E12. D13 C14 B
15 A16 C17 A18 B19 E20 D21 B22 B23 A24 D25 C26 B27 D28 D29 E30
A31 E32 C33 B34 A35 A
36 C37 E