Embed Size (px)
DESCRIPTION
Scarf sign. Put the child in a supine position and hold one of the infant’s hands. Try to put it around the neck as far as possible around the opposite shoulder. Observe how far the elbow goes across the body. In a floppy infant, the elbow easily crosses the midline. Pull to sit: - PowerPoint PPT Presentation
Citation preview
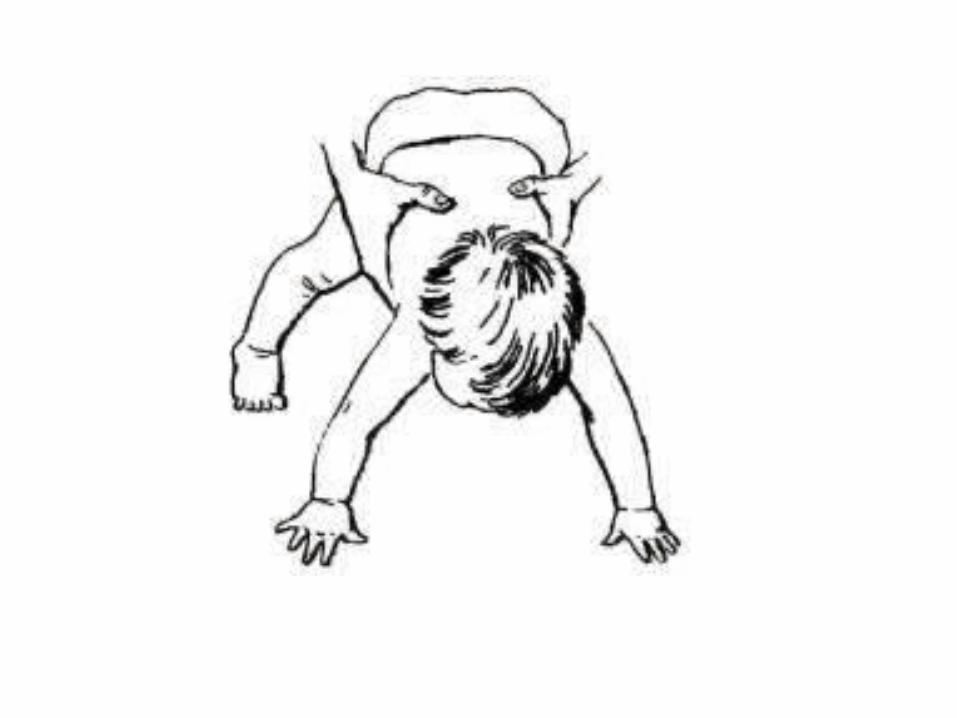




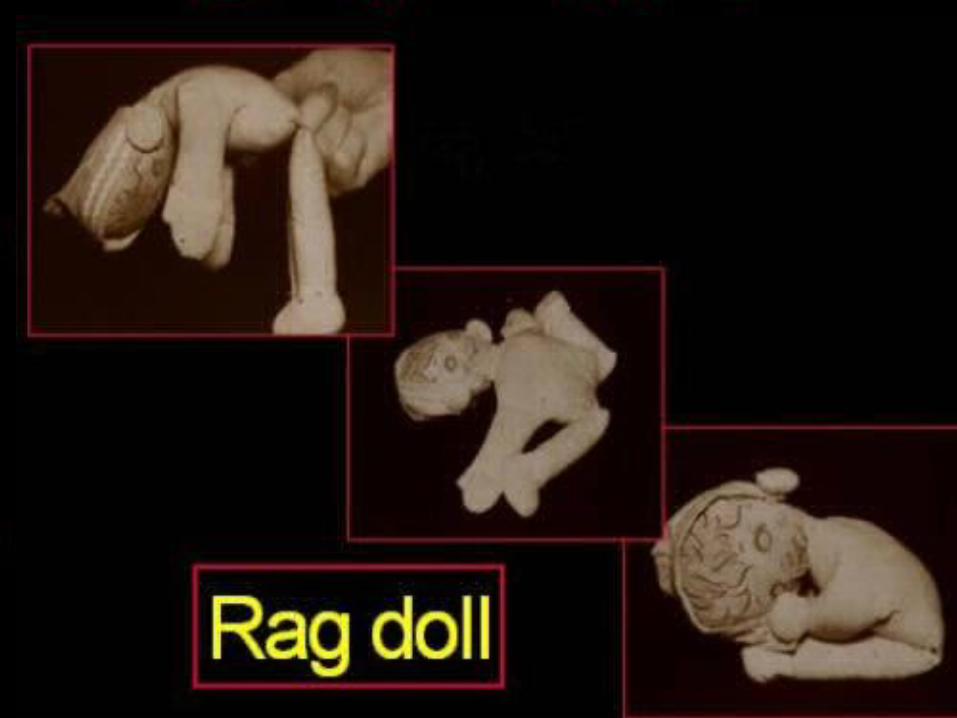
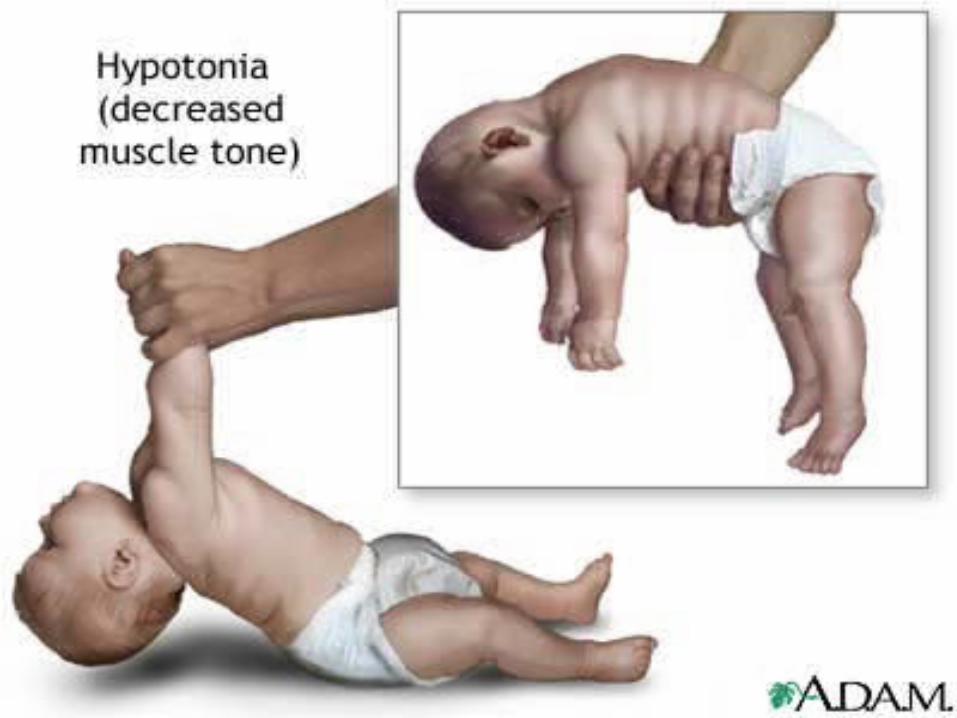
Scarf sign
Put the child in a supine position and hold one of the infant’s hands. Try to put it around the neck as far as possible around the opposite shoulder. Observe how far the elbow goes across the body. In a floppy infant, the elbow
easily crosses the midline .
Pull to sit:When pulled up from the supine to the sitting position, the head of the baby lags.
Causes of Floppy Infant Syndrome1. Central nervous system
Perinatal asphyxia, neonatal, encephalopathy, kernicterus, cerebral palsy (atonic type), intracranial hemorrhage, chromosomal anomalies including down syndrome and inborn errors of metabolism e.g., aminocidurias, mucopolysaccharidosis and cerebral lipidosis.
2. Spinal cord lesionsAnterior horn cell disease – werdnig Hoffman spinal muscular atrophy, poliomyelitis.
3. Peripheral nervousAcute polyneuropathy, familial dysautonomia, congenital sensory neuropathy.
4. Myoneural junctionNeonatal myasthenia gravis, infantile botulism, following antibiotic therapy.
5. Muscles
Muscular dystrophies, congenital myotonic dystrophies, congenital myopathies (including central core disease and nemalin myopathy), polymyositis, glycogen storage disease (pompe’s), and arthrogryposis multiplex congenital.
6. Miscellaneous
Protein energy malnutrition, rickets, prader willi syndrome, malabsorption syndromes, Ehler-Danlos syndrome, cutis laxa, cretinism.
• Radiology • Head CT • Head MRI • Electromyogram (EMG) • Nerve Conduction Studies • Serum electrolytes • Serum Calcium • Serum Glucose
• Creatine Phosphokinase (CPK) • Toxic scan• Blood Culture • Lumbar Puncture with Cerebrospinal Fluid Examination • Thyroid Function Tests • Labs: Test as indicated • Toxicology screen • Serum Ammonia and Venous pH – Serum amino acids – Urine amino acids and organic acid
• Karyotype • TORCH Virus Screening
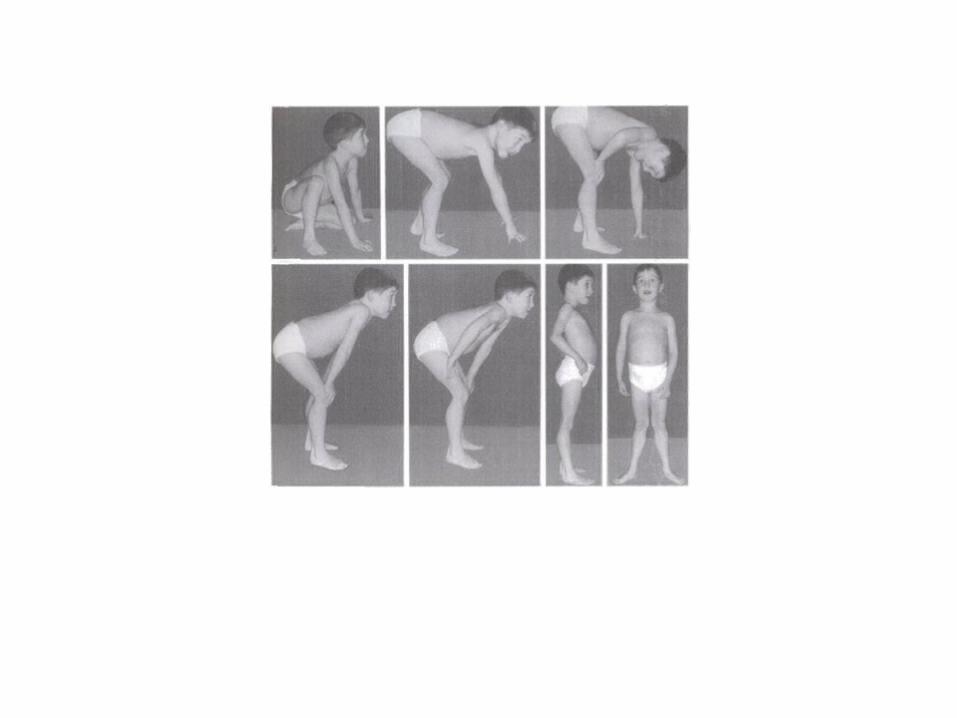
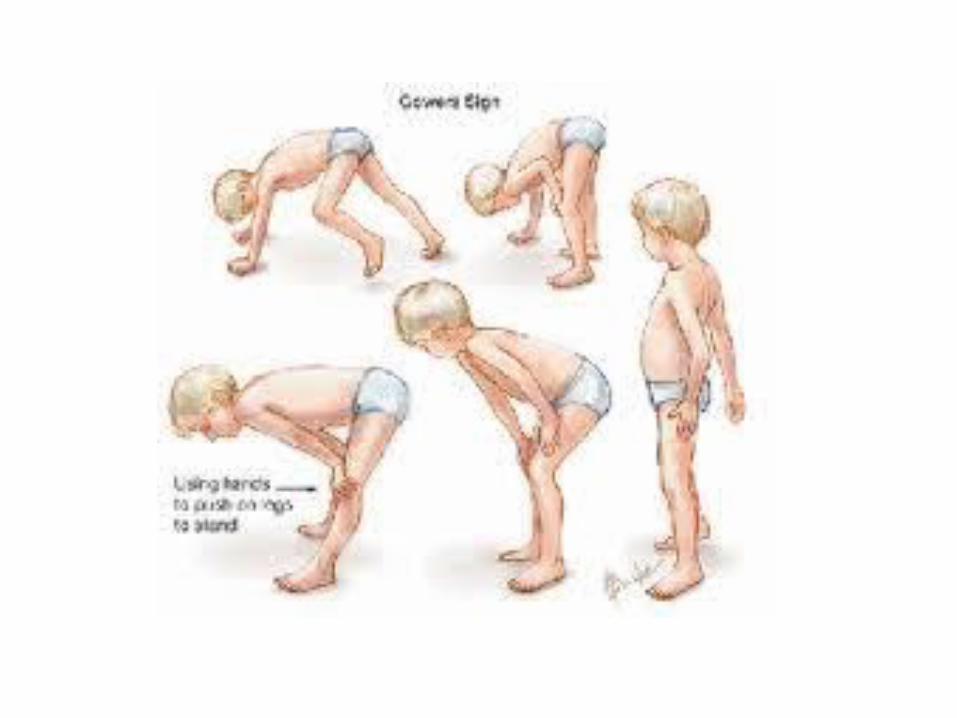

Duchenne Muscular Dystrophy
INVOLVEMENT
• Anterior horn cells• Poliomyelitis• Acute transverse myelitis
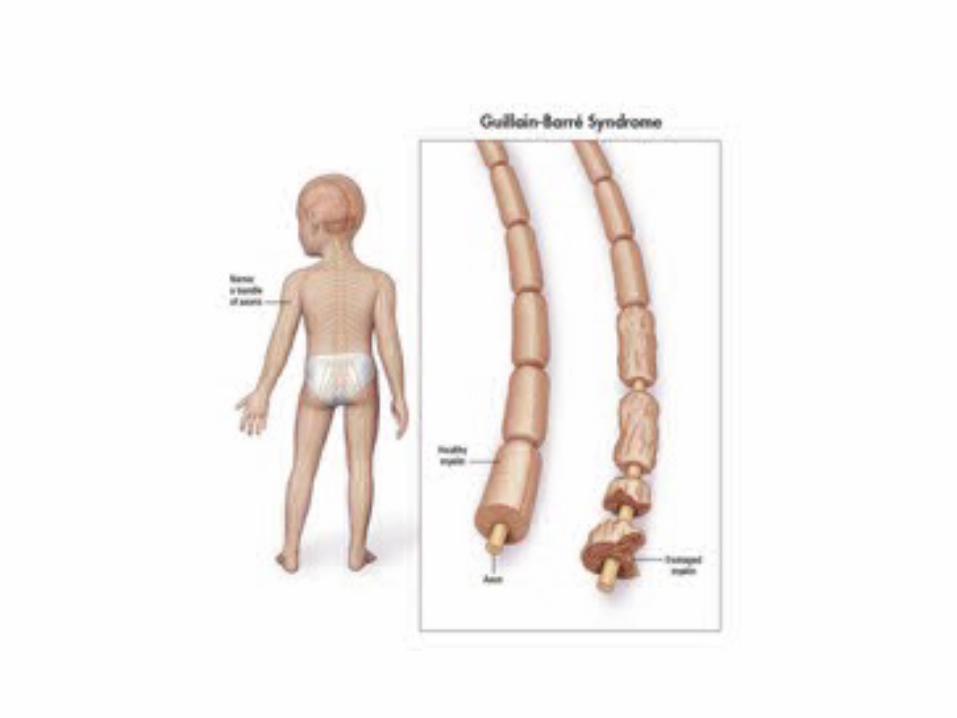
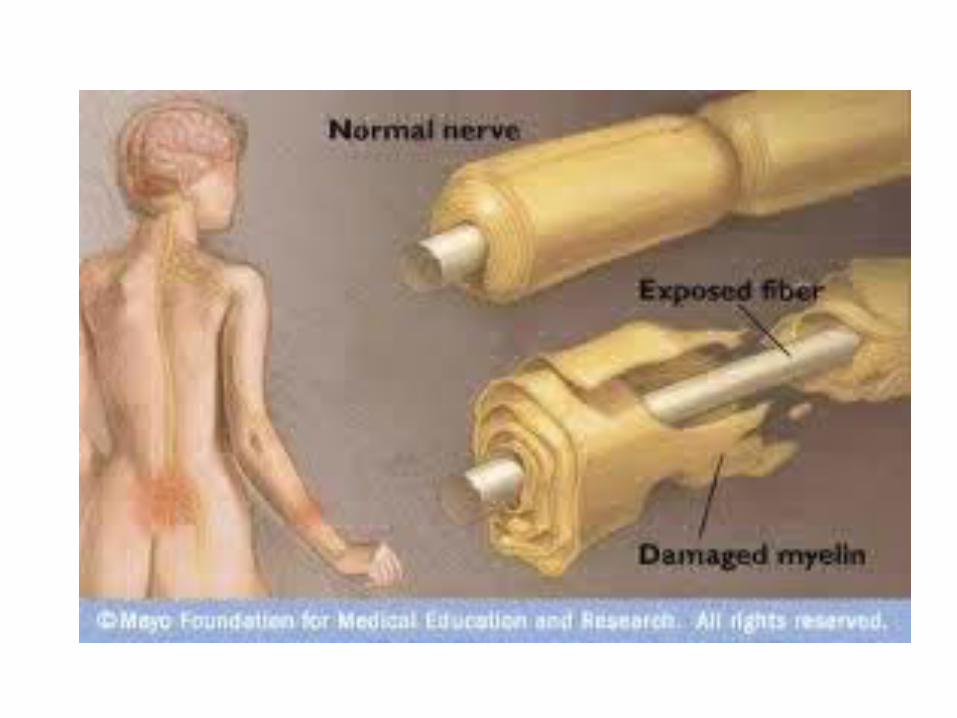
• Nerve fibres• Postinfectious polyneuropathy (GBS syndrome)• Toxins----diphtheria, porphyria
INVOLVEMENT
• Neuromuscular junction• Tick toxin• Botulinum toxin
• Metabolic causes• Periodic paralysis
• Muscular disease• Myositis
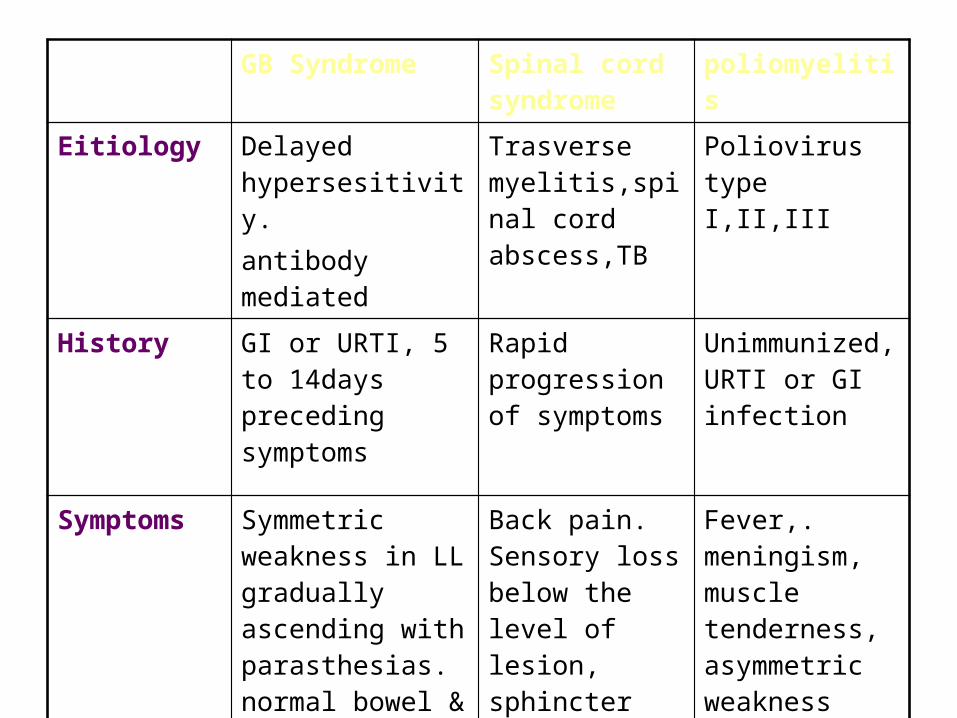
GB Syndrome Spinal cord syndrome
poliomyelitis
Eitiology Delayed hypersesitivity.antibody mediated
Trasverse myelitis,spinal cord abscess,TB
Poliovirus type I,II,III
History GI or URTI, 5 to 14days preceding symptoms
Rapid progression of symptoms
Unimmunized, URTI or GI infection
Symptoms Symmetric weakness in LL gradually ascending with parasthesias. normal bowel & bladder function
Back pain. Sensory loss below the level of lesion, sphincter problems
Fever,. meningism, muscle tenderness, asymmetric weakness
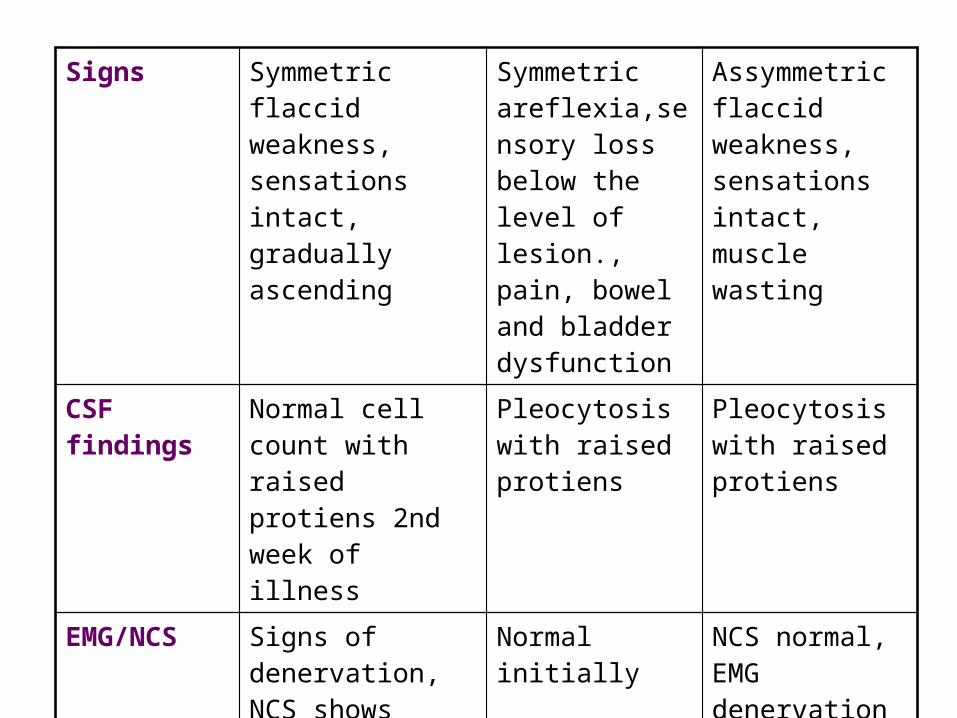
Signs Symmetric flaccid weakness, sensations intact, gradually ascending
Symmetric areflexia,sensory loss below the level of lesion., pain, bowel and bladder dysfunction
Assymmetric flaccid weakness, sensations intact, muscle wasting
CSF findings Normal cell count with raised protiens 2nd week of illness
Pleocytosis with raised protiens
Pleocytosis with raised protiens
EMG/NCS Signs of denervation, NCS shows delayed conduction
Normal initially NCS normal, EMG denervation later
Course and prognosis
Recovery in majority within 12 months
Depends on eitiology
Permanent disability in 1% cases