-
8/19/2019 Scapular Positioning in Overhead Athletes With and
Without Shoulder
1/10
Scapular positioning in overhead athletes with and without
shoulderpain: a case–control study
F. Struyf 1,2, J. Nijs1,2, J. De Graeve1, S. Mottram3, R.
Meeusen2
1Division of Musculoskeletal Physiotherapy, Department of Health
Sciences, Artesis University College Antwerp, Antwerp,
Belgium,2Department of Human Physiology, Faculty of Physical
Education and Physiotherapy, Vrije Universiteit Brussel, Brussels,
Belgium,3Kinetic Control International, Ludlow,
UK Corresponding author: Filip Struyf, PT, Campus HIKE, Dept
G, Artesis University College Antwerp, Van Aertselaerstraat 31,2170
Merksem, Belgium. Tel: 132 36 418 265, E-mail:
[email protected]
Accepted for publication 27 January 2010
Abnormalities of scapular positioning are considered im-portant
risk factors for developing shoulder disorders. Thisstudy analyses
the scapular positioning pattern in a group of overhead
athletes with and without shoulder pain. In a multi-center blinded
case–control study, 36 shoulder pain athletes(19 men, 17 women),
were compared with 36 unimpairedathletes free of shoulder pain,
matched for gender, age, handdominance and body mass index. The
blinded assessorperformed visual observation, the measurement of
the dis-
tance between the acromion and the table, inclinometry andthe
kinetic medial rotation test for dynamic scapular controlin random
order. Athletes with shoulder pain demonstratescapular asymmetry in
the sagittal plane, observed visuallyas anterior tilting on the
painful side. Athletes with shoulderpain show a lack of scapular
motor control on their painfulside in contrast to their pain-free
side. No scapular position-ing or motor control differences were
found in athletes withor without shoulder pain.
Narrowing of the subacromial space might increasethe risk for
developing shoulder pain, and be a factorin shoulder impingement
syndrome. Abnormal scap-ular positioning has previously been
related to this
excessive narrowing of the acromiohumeral distance(Brossmann et
al., 1996; He ´ bert et al., 2002).Changes in scapular
positioning are considered im-portant risk factors for developing
shoulder disor-ders such as shoulder impingement syndrome,shoulder
instability as well as post-operativeshoulder complaints, neck pain
and cervicogenicheadache (Host, 1995; Paletta et al., 1997;
Schmitt& Snyder-Mackler, 1999; Ludewig & Cook,
2000;He ´ bert et al., 2002; Lewis et al., 2002; Van Wilgenet
al., 2003; Endo et al., 2004; Van Wilgen, 2004;Cools et al., 2005;
Von Eisenhart-Rothe et al., 2005;McClure et al., 2006). In
addition, a recent studysuggests that reducing the scapular
mobility (non-specific) directly reduces the acromiohumeral
dis-tance and therefore increases the risk for
subacromialimpingement (Atalar et al., 2009).
Normally, humeral elevation is accompanied byscapular upward
rotation and posterior tilting, gle-nohumeral external rotation,
clavicular retraction,elevation and posterior axial rotation
(Ludewig &Cook, 2000; McClure et al., 2001; Borsa et al.,
2003;Ebaugh et al., 2006; Ludewig et al., 2009). Contro-versy
exists on the pattern of internal or external
scapular rotation during humeral elevation (McClureet al., 2001;
Ebaugh et al., 2006; Ludewig et al.,2009). In addition, scapular
upward rotation appearsto be greater in the scapular plane than in
the sagittal
plane (Borsa et al., 2003). In contrast to pain-freeshoulders,
patients with various shoulder disordersdemonstrate altered
scapular positioning patterns(Lukasiewicz et al., 1999; Ludewig
& Cook, 2000;He ´ bert et al., 2002; Borstad &
Ludewig, 2005;McClure et al., 2006; Ludewig et al., 2009).
Excessivescapular internal rotation, a decrease in scapularupward
rotation and a decrease of posterior scapulartilting are closely
associated with shoulder impinge-ment syndrome (Solem-Bertoft et
al., 1993; Ludewig& Cook, 2000; He ´ bert et al., 2002;
Endo et al., 2004;Lukasiewicz et al., 2009). However, some
studiesmention more upward rotation in patients withshoulder pain
(Von Eisenhart-Rothe et al., 2005;McClure et al., 2006).
While the complex kinematic behavior of thescapula and shoulder
has been studied extensively(McKenna et al., 2004), these full
three-dimensionalmotion tracking systems are costly and not
readilyavailable for clinical practice. Additionally, the ques-tion
remains whether there are clinical tools that areable to
demonstrate the same findings. Thereforethere is a need for valid
and reliable measures thathave strong clinical utility. A
literature review con-
Scand J Med Sci Sports 2011: 21: 809–818 & 2010
John Wiley & Sons A/S
doi: 10.1111/j.1600-0838.2010.01115.x
809
mailto:[email protected]:[email protected]
-
8/19/2019 Scapular Positioning in Overhead Athletes With and
Without Shoulder
2/10
cluded that clinical assessment strategies for
scapularpositioning are available but require further study
of their clinimetric properties (Nijs et al., 2007).
Researchers have suggested that shortening of thepectoralis
minor, a decrease in activity of the serratusanterior muscle and an
increase of activity of theupper trapezius muscle may affect
scapular position-ing in terms of winging, anteriorly tilting and
a
reduced scapular upward rotation. (Ludewig &Cook, 2000;
Borstad & Ludewig, 2005; Cools et al.,2003) It has also been
shown that subjects with shortpectoralis minor muscle length
demonstrate similarscapular kinematics as subjects with shoulder
impin-gement syndrome (Lukasiewicz et al., 1999; Ludewig& Cook,
2000; Borstad & Ludewig, 2005; Smithet al., 2006).
Likewise, muscle imbalance results in an abnormalforce
contribution around the shoulder, which couldlead to pain and
pathology (Comerford & Mottram,2001). It is noted clinically
that patients presentingwith upper extremity dysfunction,
frequently demon-strate poor scapular control (Mottram, 1997;
Mor-rissey et al., 2008). Consequently, abnormal scapularmovement
and muscle function has been shown to berelated to shoulder
impingement syndrome (Luka-siewicz et al., 1999; Ludewig &
Cook, 2000). Noprevious study examined the ability of a
muscularmotor control test in discriminating people with orwithout
shoulder pain. In addition, the kinetic med-ial rotation test
(KMRT) aims at observing move-ment faults at the scapula and
glenohumeral jointassociated with glenohumeral medial
rotation(Comerford & Mottram, 2001; Mottram, 2003).
This test has been developed by observation of patients
together with research results relatingshoulder girdle movement
(Comerford & Mottram,2001; Morrissey et al., 2008).
The specific purpose for this study was to analyzethe scapular
positioning pattern: scapular upwardrotation, forward shoulder
posture, tilting, wingingand scapular motor control in a group of
athleteswith shoulder pain relative to a group of athleteswithout
symptoms. Second, inter-individual differ-ences are subject to this
research.
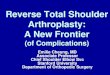
Materials and methodsStudy design
Scapular positioning and dynamic scapular control wereassessed
in a case–control study in 153 voluntary overheadathletes (Fig. 1).
Before assessment, a variety of sportsassociations agreed to
participate in the study. Subsequently,athletes that were present
at training, were asked to participatein the study. All athletes
agreed to participate and filled in awritten informed consent. The
assessor was blinded for thepresence of shoulder disorders among
the participants. Aftermeasuring the athlete’s weight and height,
the clinical assess-ment was performed in random order: observation
of forward
tilt and winging, measurement of forward shoulder posture(the
acromial distance), the measurement of scapular upwardrotation
(inclinometry) and the assessment of scapulardynamic control (the
KMRT). Scapular positioning of bothshoulders was assessed. After
the assessment protocol, thestudy participants with shoulder pain
were asked to fill inthe shoulder disability questionnaire (SDQ).
Finally, theywere interviewed to collect relevant demographic
information(age, gender and hand dominance). Height and weight
weremeasured using a measurement tape and a digital scale(Exacta,
Nassau, Germany). The study protocol was reviewedand approved by
the local medical ethics committee.
Before the study, the assessor (holder of a bachelor degreein
physiotherapy) underwent a 4-h training session. The
training session was used to instruct the assessor in
performingan accurate measurement of scapular positioning and
scapulardynamic control including pilot testing on healthy
athletes.The assessor was trained by two highly experienced
phy-siotherapists. All participants received an information
leafletand provided written informed consent. The male athleteswere
tested with their trunk bare. Female athletes wore asports bra or a
halter-top so that the scapula remained visibleand shoulder
movements were not hampered by clothing.Previous study concluded
that palpation was a valid methodto find the location of the
scapula, so all reference points usedduring the inclinometry and
acromial distance were palpated(Karduna et al., 2001; Lewis et al.,
2002).
Athlete recruitment
Seventy-two athletes (38 men, 34 women), 18–60 years of age[mean
standard deviation (SD), 33 11 years] wereincluded in this study.
Thirty-six shoulder pain athletes (19men, 17 women) were compared
with 36 unimpaired athletesfree of shoulder pain, matched for
gender, age, hand dom-inance and body mass index. Among the 36
athletes withshoulder pain, 35 painful shoulders were on the
dominant side.The mean shoulder disability score (SDQ) was 35.8
13.5.No significant differences were noted in height, age,
weight,hand dominance or duration of overhead activities
betweenboth groups. Table 1 shows the descriptive characteristics
of the athletes.
117 athletes without
shoulder pain
36 athletes with shoulder
pain
36 athletes matched for
age, gender, hand
dominance and Body
Mass Index.
Blinded clinical
assessment
Shoulder pain?YES NO
153 athletes voluntary
rectruited
Fig. 1. Flow chart of the study design; case vs control.
Struyf et al.
810
-
8/19/2019 Scapular Positioning in Overhead Athletes With and
Without Shoulder
3/10
A total number of 306 shoulders were examined from 153overhead
athletes who were recruited from a variety of
sportsassociations.
Because of possible differences in scapular positioningbetween
adults and children, study participants had to be atleast 18 years
of age to be included in the study (Dayanidhiet al., 2005; Struyf
F, Nijs J, Horsten S, Mottram S, Meeusen R,unpublished
observation). In addition, athletes had to parti-cipate in an
overhead sport at least once a week and had to beable to perform at
least 1401 of humeral abduction in thecoronal plane. This
range of shoulder abduction was measuredby use of an inclinometer,
using a standardized and reliable
protocol (Green et al., 1998). Sufficient reliability of
themeasurement of scapular upward rotation (by means of
twoinclinometers) was only attained for subjects performing 1401of
humeral abduction or more (Watson et al., 2005). Theexclusion
criteria for all athletes were a history of injury orsurgery to the
shoulder complex, upper thorax, upper backand humerus in the past
year.
Outcome measures
Visual observation for tilting and winging
Firstly, the scapular was observed to identify the
restingposition. Secondly, observation of scapular positioning
during
humeral movement was noted to assess the kinematicalrhythm
between glenohumeral abduction and scapular up-ward rotation.
The observations were performed with the athlete standingand
instructed to stay relaxed. Because high-heeled shoes caninfluence
posture and consequently scapular positioning, weasked the athletes
to stand barefoot. Only artificial lightingfrom above was used, in
order to reduce the altering effect of natural light on the
body. The scapula was observed in restingposture and during active
unloaded movement. The athletewas observed from dorsal (frontal
plane) and lateral (sagittalplane). During scapular observation at
rest, we observed allparticipants bilaterally in three positions:
static with botharms relaxed (thumbs facing forward), hands placed
on
ipsilateral hips (thumbs facing backward) and arms in 901
of humeral abduction in the frontal plane (thumbs facing
up).Scapular positioning was deemed impaired when (1) theinferior
angle of the scapula becomes prominent dorsally(the axis of
rotation is in the horizontal plane – tilting);(2) the entire
medial border of the scapula becomes prominentdorsally (the axis of
rotation is vertically and in the frontalplane – winging). If one
(or more) of the criteria listed positive,we judged scapular
positioning as impaired (score5 1), if noneof the criteria satisfy,
we judged scapular positioning asnormal (score5 0). Next, the
athlete performed active move-ment (unloaded) in standing posture.
We asked them to
perform bilateral shoulder abduction (0–1801) in the
frontalplane. The same criteria as above were used.
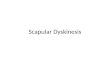
Forward shoulder posture (acromial distance)
The acromial distance is the measurement of the acromion tothe
table in supine, intended to measure forward shoulderposture.
The measurement of the distance between the posteriorborder of
the acromion and the table was performed in supine.In this
position, the assessor measured the distance betweenthe most
posterior aspect of the posterior border of theacromion and the
table bilaterally [measured vertically witha sliding calliper –
Manutant (Manutan nv, Brussels,Belgium), accuracy 0.03 mm].
Next, the assessor repeatedthis procedure with the athlete actively
retracting bothshoulders while keeping the thorax fixed against the
table.The data collected during this measurement were adjusted
bydividing by the body length, which resulted in a score enteredas
cm/cm. Each position was measured once (Fig. 2).
Scapular upward rotation (Inclinometry)
One gravity referenced inclinometer (Plurimeter-V, La
Con-version, Switzerland; accuracy to 11) (Green et al., 1998)
wasused to measure humeral elevation, and a second inclinometerwas
used to measure upward rotation of the scapula.
Thegravity-referenced inclinometer is calibrated on the basis
of
Table 1. Descriptive characteristics of the athletes
Athletes with shoulderpain (n 5 36)
Athletes without shoulderpain (n 5 36)
Age (years)Mean 33.4 33.1SD 11.3 10.9Range 18–60 18–56
Gender
Male 19 (52.8%) 19 (52.8%)Female 17 (47.2%) 17 (47.2%)Height
(cm)
Mean 176.9 178.2SD 10.5 9.8Range 156–194 158–195
Duration of contiguous overhead activities (years)Mean 12.8
11.9SD 8.8 9.5Range 1–35 1–37
Type of sportTennis 9 (25%) 9 (25%)Volleyball 16 (44%) 12
(33%)Baseball 2 (6%) 1 (3%)Badminton 7 (19%) 10 (28%)Handball 2
(6%) 4 (11%)
Fig. 2. Measurement of forward shoulder posture
(acromialdistance).
Scapular positioning in overhead athletes
811
-
8/19/2019 Scapular Positioning in Overhead Athletes With and
Without Shoulder
4/10
gravity. The starting position of the movement to be measuredis
therefore fixed, minimizing placement error. All athleteswere
assessed in a relaxed, standing (barefoot) position.Scapular upward
rotation was measured during total shoulderabduction using a
standardized reliable protocol as describedby Green et al.
(1998).
Athletes were asked to perform full extension at the
elbow,neutral wrist position and with the thumb leading.
Theinclinometer is attached perpendicular to the humerus, justunder
the deltoid insertion using a Velcro tape. Athletes were
then asked to move both arms into abduction and to stop at451,
901, 1351 and at full range of humeral abduction (Fig. 3).At
each of these positions, the degree of upward rotation of the
scapula was measured using the second inclinometer. Thiswas
achieved by manually aligning the base of the inclin-ometer along
the spine of the scapula. Additionally, wecreated four phases of
humeral elevation: phase I (restingposition to 451), phase II
(45–901), phase III (90–1351) andphase IV (1351 to end
range). Only positions that can bemeasured reliably with the
Plurimeter-V inclinometer wereincluded in this study. For
standardization, each athlete getsone test-rehearsal before the
test was performed.
Scapular motor control (KMRT)
The athlete is supine with the humerus abducted to 901, theelbow
flexed 901 and the humerus in 301 of
horizontalabduction (hand to the ceiling with the humerus in the
planeof the scapula). All angles were measured by using
aninclinometer. The athlete is taught to perform medial rotationat
the glenohumeral joint while keeping the scapula still in
itsneutral position. This test is scored positive when
scapularforward tilt, downward rotation or elevation occurs (Fig.
4).The KMRT is performed until 601. Normative research datasuggest
that during medial rotation to 601, in non-painfulshoulders the
glenoid does not anterior translate 44 mm, andthe scapula
does not translate 46 mm (Morrissey et al., 2008).Accuracy of
palpation is critical to the test. Recent studyconcluded that this
manual landmark identification can be
tracked accurately by palpation (Morrissey et al., 2008).For
this experiment, test scoring was twofold: first, this test
is scored positive (score5 1) when the assessor feels that
thescapula forward tilts or elevation occurs (A-list).
Second,difficulties in breathing, performing difficulties, unable
toperform 601 medial rotation, glenohumeral anterior
transla-
tion, fatigue, the need of external feedback and externalsupport
are also scored (score5 1 if present – B-list) (Comer-ford &
Mottram, 2001). Finally, this gives rise to a total scoreon a
117-points scale (Table 2). We state the scapula to have alack of
motor control when the score is 1 on the A-list, 43 onthe
B-list or both. For standardization, each athlete gets
onetest-rehearsal before the test was performed.
SDQ
The SDQ covers 16 items to evaluate functional statusdisability
in athletes with shoulder disorders and is suggestedto be
responsive and ready for use in clinical trials andlongitudinal
studies (Van der Windt et al., 1998; Van derHeijden et al., 2000).
All 16 items describe a possible pain-provocation during the last
24 h of the athletes daily activities.The questionnaire is
completed with yes, no or not applicable.It is scored by the
summation of all yes-answers, divided by allanswered questions (yes
or no) and subsequently multiplied by100. This results in a score
between 0 (no disabilities) to 100(very disabled). In this study,
the Dutch version of the SDQwas used.
Reliability of outcome measures
Previous study on the inter-tester reliability of
scapularobservation conclude that the observation at rest and
duringmovement is a clinically applicable tool for assessing
patternsof scapular positioning and movement (McClure et al.,
2009;Struyf et al., 2009). The k values for the
observation of tiltingand winging at rest were 0.48 and 0.42,
during unloadedmovement 0.52 and 0.78 (Struyf et al., 2009).
Validity of thescapular dyskinesis test was demonstrated (Tate et
al., 2009).The measurement of the acromial distance was found
reliable(both relaxed and during retraction, ICCs40.88) (Nijs et
al.,2005) and is suggested to be indicative for pectoralis
minormuscle length (Borstad & Ludewig, 2005). Overall,
measure-ment of upward rotation by means of analogue
inclinometersreached very good intrarater reliability (ICC5 0.88)
(Watson
et al., 2005). The KMRT has been validated against
dynamicultrasound (Morrissey, 2005). However, reliability data for
theKMRT are currently lacking. Cross-sectional comparisonshowed
similar overall validity and patient acceptability asthe UK version
(Paul et al., 2004). Participants of that cross-sectional
comparison rated the Dutch version of the SDQ as
Fig. 3. Measurement of scapular upward rotation with
twoinclinometers.
Fig. 4. Measurement of scapular motor control using theKMRT.
Struyf et al.
812
-
8/19/2019 Scapular Positioning in Overhead Athletes With and
Without Shoulder
5/10
best for the relevance to their shoulder problem (Paul et
al.,2004).
Statistical analysis
Means, standard deviations and ranges were calculated for
allmeasured and normalized data. A one-sample
Kolmogorov– Smirnov goodness-of-fit test was used to identify
normaldistribution. The athletes’ painful shoulder is always
com-
pared with the same side in the pain-free group. An
indepen-dent-samples t-test was used when analyzing the
differencebetween the athletes with and without shoulder disorders
forthe inclinometry and acromion–table (AT) distance.
Forcomparisons between the painful and pain-free shoulderwithin the
athletes with shoulder pain group, the pairedsample t-test
and the chi-square test were used for theparametric and
non-parametric data, respectively. The chi-square test was used to
identify differences for the outcome of the KMRT and
observation protocol. The Pearson andSpearman correlations were
computed for examining associa-tions between the scores of the SDQ,
demographic featuresand the clinical measures and between the
clinical measuresmutually. Because the body length correlated with
the mea-surement of the distance between the posterior border of
the
acromion and the table, the data were adjusted for the
bodylength, creating an acromial distance index (i.e. the outcome
of the measurement of the distance between the posterior
borderof the acromion and the table was divided by the body
lengthin cm and multiplied by 100). The scapulohumeral rhythm
wascalculated by dividing the total humeral elevation by
thescapular upward rotation. Groups were matched for age,gender and
BMI without the knowledge of other outcomemeasures. Data were
analyzed using SPSS version 12.0, forWindows (SPSS Inc., Chicago,
Illinois, USA). The poweranalysis was performed using SigmaStat 3.1
(Systat SoftwareInc., San Jose, California, USA). Except for the
power
analysis, data were analyzed using SPSS version 12.0, forWindows
(SPSS Inc.).
ResultsVisual observation for tilting and winging
The observation protocol for scapular tilting andwinging did not
show significant differences between
the athletes with and without shoulder pain. Table 3shows all
observations for present or absent tiltingand winging. Within the
group of athletes withshoulder pain, tilting was found to be more
presenton the painful side (12/36; 33%) then on the pain-freeside
(8/36; 22%) (Po0.01). Winging was found tomore present on the
pain-free side (5/36; 14%) thanon the painful side (4/36; 11%)
(Po0.01). No differ-ences were seen between men and women.
Forward shoulder posture (acromial distance)
The athletes with shoulder pain presented with amean AT-distance
of 83.6 28 mm at rest and53.8 22 mm during bilateral retraction.
The ath-letes without shoulder pain presented with a
meanAT-distance of 84.9 25 mm at rest and54.6 22 mm during
bilateral retraction. Table 4shows the results of the AT distance
index [correctedfor BL (cm) 100] between athletes with and
with-out shoulder pain. No significant differences werefound
between groups or between men and women.Within subgroup analysis
did not show any signifi-cant differences in the AT-distance
index.
Scapular upward rotation (inclinometry)
When comparing scapular upward rotation betweenthe two groups
using two inclinometers, no signifi-cant differences were found.
Table 5 shows the resultsof the upward scapular rotation during
humeralelevation in both groups. No significant differenceswere
found between men and women. However,when analyzing the women only,
the athletes withshoulder pain did show a significant loss of
upwardrotation (351) compared with the pain-free women
(421
) (P5
0.049).
Table 2. 117-point scale for scoring the kinetic medial rotation
test
Correct pattern ScoreA-list(0 or 1)
Efficiency ScoreB-list(0 or 1)
Compensationscapular
Difficulty breathing
Difficult to performNo movementpossible (601)FatigueExtra
feedback neededExternal support neededGlenohumeralcompensation
Sum /1 /7
Table 3. Observation of winging and tilting of the scapula
between case and control
Observation Athletes with shoulder pain
Painful side (A) Pain-free side (B) A-matched side B-matched
side
Winging Present 4 (11%) 5 (14%) 5 (14%) 5 (14%)Absent 32 (89%)
31 (86%) 31 (86%) 31 (86%)
Tilting Present 12 (33%) 8 (22%) 10 (27%) 6 (17%)Absent 24 (67%)
28 (78%) 26 (72%) 30 (83%)
Scapular positioning in overhead athletes
813
-
8/19/2019 Scapular Positioning in Overhead Athletes With and
Without Shoulder
6/10
Scapular motor control (KMRT)
Table 6 shows the positive KMRT scores in bothathletes with and
without shoulder pain.
No significant difference was found betweengroups. Within the
shoulder pain group, 77%(n5 10) of the positive MRT scores were on
thepainful side, in contrast to 23% (n5 3) on the pain-free side
(P5 0.017). No significant differences were
noted between the left or right shoulder within thepain-free
subgroup (data not shown). No significantdifferences were observed
between men and women.
Discussion
This case–control study highlights several interestingaspects of
the clinical evaluation of scapular posi-tioning and scapular motor
control. Although theclinical assessment protocol was not able to
identifystatistically significant differences in scapular posi-
tioning or motor control between athletes with orwithout
shoulder pain, there appear to be somesignificant differences
between the athletes sympto-matic and asymptomatic shoulder.
Visual observation for tilting and winging
First, tilting appears to be more present on thepainful side and
winging on the asymptomatic side.This finding reinforces earlier
research in which it hasbeen shown that subjects with a protracted
scapula(or short pectoralis minor muscle length) demon-strate
similar scapular positioning as subjects withshoulder impingement
syndrome (Solem-Bertoft
et al., 1993; Lukasiewicz et al., 1999; Ludewig &Cook, 2000;
Borstad & Ludewig, 2005). In addition,both tilting and
AT-distance are suggested to beindicative for pectoralis minor
muscle length (Borsaet al., 2003; Nijs et al., 2005). Scapular
asymmetry inthe sagittal plane (increased scapular tilting)
waspreviously seen in patients with the shoulder impin-gement
syndrome between their asymptomatic andsymptomatic shoulders
(Lukasiewicz et al., 1999).However, when comparing dominant vs
non-domi-nant shoulder, these differences significantly
reoccur.This reinforces the results from a recent study in
healthy overhead athletes, which concluded that thedominant-side
scapula was more anteriorly tiltedthan the non-dominant-side
scapula (Oyama et al.,2008). We need to recognize that scapular
asymmetry
Table 4. Measurement of forward shoulder posture (acromial
distance index) corrected with body length
Case vs control N Mean [(cm/BL) 100] SD
[(cm/BL) 100] Power
AT distance (relaxed) Pain-free athletes 36 4.77 1.45
0.863Athletes with shoulder pain 35 4.70 1.54
AT distance (retracted) Pain-free athletes 36 3.07 1.20
0.913Athletes with shoulder pain 35 3.04 1.26
SD, standard deviation; AT, acromion–table.
Table 5. Scapular upward rotation (inclinometry) during humeral
elevation between the different groups
Case vs control N Mean (1) SD (1) Power
Scapular upward rotation at rest Pain-free athletes 36
7.72 6.68 0.662Athletes with shoulder pain 36 8.53 7.00
Scapular upward rotation at 451 humeral abduction Pain-free
athletes 36 3.08 7.39 0.721Athletes with shoulder pain 36
3.75 7.27
Scapular upward rotation at 901 humeral abduction Pain-free
athletes 36 9.08 7.37 0.94Athletes with shoulder pain 36 8.94
9.15
Scapular upward rotation at 1351 humeral abduction
Pain-free athletes 36 24.64 8.90 0.67Athletes with shoulder pain 36
23.61 9.25
Maximal scapular upward rotation Pain-free athletes 36 39.44
10.46 0.53Athletes with shoulder pain 36 37.22 9.68
Ratio phase 1 Pain-free athletes 36 16.13 15.19 0.99Athletes
with shoulder pain 36 16.15 1.83
Ratio phase 2 Pain-free athletes 36 5.35 5.51 0.91Athletes with
shoulder pain 36 5.55 8.37
Ratio phase 3 Pain-free athletes 36 3.41 1.57 0.51Athletes with
shoulder pain 36 4.29 3.77
Ratio phase 4 Pain-free athletes 36 4.96 8.56 0.58Athletes with
shoulder pain 36 3.78 4.91
Overall gh/st ratio Pain-free athletes 36 3.66 0.82 0.59Athletes
with shoulder pain 36 3.81 0.99
SD, standard deviation.
Struyf et al.
814
-
8/19/2019 Scapular Positioning in Overhead Athletes With and
Without Shoulder
7/10
in healthy overhead athletes often occurs. However,as tilting is
related to shoulder impingement syn-drome, we suggest assessing the
scapula for thisasymmetry is needed in order to create a
baselineevaluation of the athlete.
Forward shoulder posture (acromial distance)
The AT-distance measurements are put into perspec-tive with the
body length. Our results are in line withthe normative data
presented in a previous study onthe AT-distances relative to the
body length in 105healthy subjects (Struyf F, Nijs J, Horsten S,
Mot-tram S, Meeusen R, unpublished observation).Adults presented
with a mean AT-distance (correctedto BL) of 4.12 cm/cm and 2.67
cm/cm for the relaxedand retracted position, respectively, while
the presentstudy showed a mean AT-distance of 4.77cm/cm and3.07
cm/cm. When we address non-relative distances,our results are
slightly higher than a previous studyin patients with shoulder
pain. Nijs et al., (2005)reported a mean (relaxed) AT-distance of
7.2 vs4.6 cm during retraction. Our results are approxi-
mately 1.0 cm larger, which could be due to the studypopulation.
More specific, Nijs and colleagues im-plemented a sample of
convenience of 29 patients,mainly recruited in private practices
for physicaltherapy, while our study included overhead
athlete’s.The repetitive movements performed by overheadathletes
may increase the AT-distance and hencetrigger forward shoulder
posture. This might increasethe risk for developing shoulder
disorders amongoverhead athletes.
Scapular upward rotation (inclinometry)
Third, inclinometry for measuring scapular upwardrotation did
not reveal any significant differencesbetween both groups or
between the symptomaticand asymptomatic shoulder. These
observations arein line with previous studies (Lukasiewicz et al.,
1999;Graichen et al., 2001; He ´ bert et al., 2002).
Assuggested by Lukasiewicz et al. (1999), this couldbe caused by
the faulty use of neuromuscular strate-gies in both shoulders.
Compared with the study of McClure et al. (2001), our athletes
with shoulder painattained lower degrees of scapular upward
rotation
[mean (SD)5 37.21 (9.71) vs 501 (4.81) in
theMcClure’s study]. Although overhead athletes con-stantly perform
activities which require sufficientupward scapular rotation, they
demonstrate lessupward rotation. Although the athletes
withoutshoulder pain did not report any pain, these resultsmight
indicate that they are at increased risk fordeveloping shoulder
problems.
Controversy still exists about the overall ratio
of glenohumeral to scapulothoracic (gh/st) movement(Freedman
& Munro, 1966; Poppen & Walker, 1976;McQuade & Smidt,
1998; Johnson et al., 2001). First,most studies assume a 01
starting position of thehumerus, whereas others actually measure
the restingposition. Second, differences in measurement techni-ques
and methodology can create a wide range of reported ratios.
Finally, the comparison across dif-ferent studies is difficult due
to inter-individualvariability. The mean ratio of glenohumeral to
sca-pulothoracic motion in the athletes with shoulderpain was 3.8:1
in our study vs 1.7:1 (McClure et al.,2001) and 2.1:1 (Graichen et
al., 2001) in otherstudies. The study of McClure implemented
healthysubjects, whereas Graichen also examined patientswith
shoulder impingement syndrome. Previous re-search in patients with
atraumatic shoulder instabil-ity demonstrate similar results with
an increasedratio in the patient group (Von Eisenhart-Rotheet al.,
2005). The implementation of subjects withshoulder pain appears to
increase the gh/st ratio.
No significant differences were noted between menand women.
Surprisingly, when analyzing womenonly, the athletes with shoulder
pain showed a
significant loss of upward rotation in comparisonto pain-free
women. In contrast, earlier research of 160 healthy men and
women did not find anysignificant differences between men and women
onshoulder posture variations (Raine & Twomey,1997). One
explanation for this discrepancy couldbe the influence of shoulder
pain. Based on theseobservations, it is postulated that shoulder
painmanifests differently in men and women. Furtherstudy is
required to examine this issue.
Scapular motor control (KMRT)
Finally, this study also addressed scapular motorcontrol. The
KMRT did not show significant differ-ences between both groups, but
there were some strongsignificant differences between the painful
shoulderand the pain-free shoulder within the athletes withshoulder
pain subgroup. More than three-quarters of the impaired
subgroup demonstrated with positivescores on their symptomatic
side. However, poorscapular motor control was prevalent among
theathletes without shoulder disorders as well, possibleexplaining
the lack of significant differences in motor
Table 6. Positive KMRT scores
Pain-free athletes Athletes withshoulder pain
10/36 (28%) 13/36 (26%)
On painful side: 10/36
On pain-free side: 3/36P 50.017
Scapular positioning in overhead athletes
815
-
8/19/2019 Scapular Positioning in Overhead Athletes With and
Without Shoulder
8/10
control between the two groups. The athletes withoutshoulder
disorders are all performing overhead activ-ities and have
therefore an increased risk for develop-ing shoulder disorders. In
addition, the KMRT wasvalidated in a sample of convenience of
normal sub-
jects (Morrissey et al., 2008). However, baseball
pitch-ers, tennis and handball players have been repeatedlyfound to
have an increased range of external rotation
with a corresponding decreased range of internalrotation in
their throwing shoulder compared withthe contralateral shoulder
when assessed at 901 of abduction (Borsa et al., 2008).
This could have causedextra positive scores on the KMRT in both
case andcontrol group. Likewise, this could have increased
theside-to-side differences.
Except for the KMRT and the visual observationduring humeral
elevation, an important limitation of this study is that in
the main outcome measures onlystatically held positions were used
rather than dy-namic motion. Statically held positions may
notrepresent functional movement patterns. Secondly,no
identification of the type of shoulder disorder wasperformed in
this study. Pain, as the only inclusioncriteria, may neglect
relevant differences between thevarious shoulder disorders. More
specifically, themost frequently seen shoulder pathologies are
ac-companied with different scapular motion patterns(Ludewig et
al., 2009). While patients with shoulderimpingement syndrome,
rotator cuff diseases orglenohumeral joint instability are
accompanied witha reduced scapular upward rotation, patients
withadhesive capsulitis show an increase in upward rota-tion.
Additionally, patients with shoulder impinge-
ment syndrome or rotator cuff diseases can show lessposterior
tilting, while no evidence for this alterationis found in patients
with other shoulder pathologies.Future study should include
differentiation of shoulder pathologies.
As the athletes age ranged from 18 to 60 years, it ispossible
that age differences alter scapular position-ing and motor control.
Although no differences inscapular positioning were noted between
unimpairedadults, clinicians should be aware of the
decreasingmuscular system during aging. Since the scapularmuscular
system is the major contributor to scapularpositioning, differences
in scapular positioning and
motor control in adults may exist (Dayanidhi et al.,2005; Nijs
et al., 2005).
The majority of researchers in the field applyexpensive and
specialized equipment for assessingscapular positioning. In
contrast, the results obtainedin this study were all gathered with
clinical tests.Although three-dimensional electromagnetic track-ing
systems allow us to increase scapular assessment
accuracy, the use of these measurement tools in theclinic are
limited. However, our methods of measur-ing scapular motion should
be validated againstaccurate motion analysis. Finally, the findings
fromthis study can only be generalized to
inter-individualdifferences in athletes who compete in
overheadsports.
Perspectives
This study puts extra emphasis on the clinical eva-luation of
overhead athletes with various shoulderdisorders. Scapular
asymmetry in the sagittal plane,observed visually as tilting and a
lack of scapularmotor control are highly related to the
athletes’shoulder pain. Both observation of tilting and theKMRT are
therefore suggested to be discriminativein distinguishing
symptomatic and asymptomaticshoulders. Future research needs to be
directed tounravelling the basic mechanisms that control
thescapular motion and study the effects of varioustreatment
methods in patients with a variety of shoulder
pathologies.
Key words: scapula, athletes, clinical, assessment,
pain.
Acknowledgements
This study was financially supported by a research grant(G826)
provided by the Department of Health Sciences,Artesis University
College Antwerp, Antwerp, Belgium.
We certify that no party having a direct interest in theresults
of the research supporting this article has or will confera benefit
on us or on any organization with which we areassociated.
The study protocol was reviewed and approved by themedical
ethics committee of the University Hospital Brussels(2006/137).
References
Atalar H, Yilmaz C, Polat O, Selek H,
Uras I, Yanik B. Restricted scapular
mobility during arm abduction:
implications for impingement
syndrome. Acta Orthop Belgica 2009:
75: 19–24.
Borsa PA, Laudner KG, Sauers EL.
Mobility and stability adaptations in
the shoulder of the overhead athlete: a
theoretical and evidence-based
perspective. Sports Med 2008: 38: 17–
36.
Borsa PA, Timmons MK, Sauers EL.
Scapular-positioning patterns during
humeral elevation in unimpaired
shoulders. J Athl Train 2003: 38: 12–17.
Borstad JD, Ludewig PM. The effect
of long versus short pectoralis
Struyf et al.
816
-
8/19/2019 Scapular Positioning in Overhead Athletes With and
Without Shoulder
9/10
minor resting length on scapular
kinematics in healthy individuals.
J Orthop Sports Phys Ther 2005: 35:
227–238.
Brossmann J, Preidler KW, Pedowitz RA,
White LM, Trudell D, Resnick D.
Shoulder impingement syndrome:
influence of shoulder position
on rotator cuff impingement –
an anatomic study. Am Roentgen
Ray Soc 1996: 167: 1511–1515.Comerford MJ, Mottram SL.
Movement
and stability dysfunction –
contemporary developments. Man
Ther 2001: 6: 15–26.
Cools AM, Witvrouw EE, Declercq GA,
Danneels LA, Cambier DC. Scapular
muscle recruitment patterns: trapezius
muscle latency with and without
impingement symptoms. Am J Sports
Med 2003: 31: 542–549.
Cools AM, Witvrouw EE, Declercq GA,
Vanderstraeten GG, Cambier DC.
Evaluation of isokinetic force
production and associated muscle
activity in the scapular rotators duringa protraction–retraction
movement in
overhead athletes with impingement
symptoms. Br J Sports Med 2005: 38:
64–68.
Dayanidhi S, Orlin M, Kozin S, Duff S,
Karduna A. Scapular kinematics
during humeral elevation in adults and
children. Clin Biomech 2005: 20:
600–606.
Ebaugh DD, McClure PW, Karduna AR.
Effects of shoulder muscle fatigue
caused by repetitive overhead activities
on scapulothoracic and glenohumeral
kinematics. J Electromyo Kinesiol
2006: 16: 224–235.
Endo K, Yukata K, Yasui N. Influence of
age on scapulo-thoracic orientation.
Clin Biomech 2004: 19: 1009–1013.
Freedman L, Munro RR. Abduction of
the arm in the scapular plane: scapular
and glenohumeral movements. J Bone
Joint Surg 1966: 48: 1503–1510.
Graichen H, Stammberger T, Bone ´ l H,
Wiedemann E, Englmeier K-H, Reiser
M, Eckstein F. Three-dimensional
analysis of shoulder girdle and
supraspinatus motion patterns in
patients with impingement syndrome. J
Orthop Res 2001: 19: 1192–1198.
Green S, Buchbinder R, Forbes A,
Bellamy N. Standardized protocol for
measurement of range of movement
of the shoulder using the Plurimeter-V
inclinometer and assessment
of its intrarater and interrater
reliability. Arthr Care Res 1998: 11:
43–52.
He ´ bert LJ, Moffet H, McFadyen BJ,
Dionne CE. Scapular behaviour
shoulder impingement syndrome.
Arch Phys Med Rehabil 2002: 83:
60–69.
Host HH. Scapular taping in the
treatment of anterior shoulder
impingement. Phys Ther 1995: 75:
803–812.
Johnson MP, McClure PW, Karduna
AR. New method to assess scapular
upward rotation in subjects with
shoulder pathology. J Orthop Sports
Phys Ther 2001: 31: 81–89.
Karduna RA, McClure PW, Michener
LA, Sennet B. Dynamic measurementof three-dimensional
scapular
kinematics, a validation study. J
Biomech Eng 2001: 123: 184–190.
Lewis J, Green A, Reichard Z, Wright C.
Scapular position: the validity of skin
surface palpation. Man Ther 2002: 7:
26–30.
Ludewig PM, Cook TM. Alterations in
shoulder kinematics and associated
muscle activity in people with
symptoms of shoulder impingement.
Phys Ther 2000: 80: 276–291.
Ludewig PM, Phadke V, Braman JP,
Hassett DR, Cieminski CJ, LaPrade
RF. Motion of the shoulder complexduring multiplanar humeral
elevation.
J Bone Joint Surg Am 2009: 91: 378–
389, doi: 10.2106/JBJS.G.01483.
Lukasiewicz AC, McClure P, Michener L,
Pratt N, Sennet B. Comparison of
3-dimensional scapular position and
orientation between subjects with and
without shoulder impingement. J
Orthop Sports Phys Ther 1999: 29:
574–586.
McClure P, Tate AR, Kareha S, Irwin D,
Zlupko E. A clinical method for
identifying scapular dyskinesis, part 1:
reliability. J Athl Training 2009: 44:
160–164.
McClure PW, Michener LA, Karduna
AR. Shoulder function and 3-
dimensional scapular kinematics in
people with and without shoulder
impingement syndrome. Phys Ther
2006: 86: 1075–1090.
McClure PW, Michener LA, Sennett BJ,
Karduna AR. Direct 3-dimensional
measurement of scapular kinematics
during dynamic movements in vivo.
J Shoulder Elbow Surg 2001: 10:
269–277.
McKenna L, Cunningham J, Straker L.
Inter-tester reliability of scapular
position in junior elite swimmers. Phys
Ther Sports 2004: 5: 146–155.
McQuade KJ, Smidt GL. Dynamic
scapulohumeral rhythm: the effect of
external resistance during elevation of
the arm in the scapular plane. J Orthop
Sports Phys Ther 1998: 27: 125–133.
Morrissey D. 2005. The development of
the kinetic medial rotation test of the
shoulder. PhD Thesis, University of
London.
Morrissey D, Morrissey MC, Driver W,
King JB, Woledge RC. Manual
landmark identification and tracking
during the medial rotation test of the
shoulder: an accuracy study using
three-dimensional ultrasound and
motion analysis measures. Man Ther
2008: 13: 529–535.
Mottram S. Dynamic stability of the
scapula. Man Ther 1997: 2: 123–131.
Mottram S. Dynamic stability of the
scapula1postscript in Beeton. Man
Ther Masterclasses Periph Joints 2003:Chapter 1: 3–17.
Nijs J, Roussel N, Struyf F, Mottram S,
Meeusen R. Clinical assessment of
scapular positioning in patients with
shoulder pain: state of the art. J Manip
Phys Ther 2007: 30: 69–75.
Nijs J, Roussel N, Vermuelen K,
Souvereyns G. Scapular positioning in
patients with shoulder pain: a study
examining the reliability and clinical
importance of 3 clinical tests. Arch
Phys Med Rehabil 2005: 86: 1349–1355.
Oyama S, Myers JB, Wassinger CA, Ricci
RD, Lephart SM. Asymmetric resting
scapular posture in healthy overheadathletes. J Athl Train 2008:
43:
565–570.
Paletta GA, Warner JJP, Warren RF,
Deutsch A, Altchek DW. Shoulder
kinematics with two-plane x-ray
evaluation in patients in anterior
instability or rotator cuff tearing.
J Shoulder Elbow Surg 1997: 6: 516–527.
Paul A, Lewis M, Shadforth MF, Croft
PR, Van den Windt DAWM, Hay EM.
A comparison of four shoulder-specific
questionnaires in primary care. Ann
Rheum Dis 2004: 63: 1293–1299.
Poppen NK, Walker PS. Normal and
abnormal motion of the shoulder.
J Bone Joint Surg 1976: 58: 195–201.
Raine S, Twomey LT. Head and
shoulder posture variations in 160
asymptomatic women and men. Arch
Phys Med Rehabil 1997: 78:
1215–1223.
Schmitt L, Snyder-Mackler L. Role of
scapular stabilizers in etiology and
treatment of impingement syndrome.
J Orthop Sports Phys Ther 1999: 29:
31–38.
Smith J, Dietrich CT, Kotajarvi BR,
Kaufman KR. The effect of scapular
protraction on isometric shoulder
rotation strength in normal subjects.
J Shoulder Elbow Surg 2006: 15:
339–343.
Solem-Bertoft E, Thuomas K,
Westenberg C. The influence of
scapular retraction and protraction on
the width of the subacromial space.
Clin Orthop 1993: 296: 99–103.
Struyf F, Nijs J, De Coninck K, Giunta
M, Mottram S, Meeusen R. Clinical
assessment of scapular positioning in
musicians: an inter-tester reliability
study. J Athl Train 2009: 44: 519–526.
Scapular positioning in overhead athletes
817
http://localhost/var/www/apps/conversion/tmp/scratch_5/10.2106/JBJS.G.01483http://localhost/var/www/apps/conversion/tmp/scratch_5/10.2106/JBJS.G.01483
-
8/19/2019 Scapular Positioning in Overhead Athletes With and
Without Shoulder
10/10
Tate AR, McClure P, Kareha S, Irwin D,
Barbe MF. A clinical method for
identifying scapular dyskinesis, part 2:
validity. J Athl Train 2009: 44: 165–173.
Van der Heijden GJMG, Leffers P,
Bouter LM. Shoulder disability
questionnaire design and respon-
siveness of a functional status measure.
J Clin Epidem 2000: 53: 29–38.
Van der Windt DAWM, van der Heijden
GJMG, de Winter AF, Koes BW,Deville ´ W, Bouter LM.
The
responsiveness of the shoulder
disability questionnaire. Ann Rheum
Dis 1998: 57: 82–87.
van Wilgen CP. 2004. Morbidity
after neck dissection in head and
neck cancer patients. A study
describing shoulder and neck
complaints, and quality of life. PhD
thesis, Rijksuniversiteit Groningen,
10–11.
van Wilgen CP, Dijkstra PU, van der
Laan BFAM, Plukker JT, RoodenburgJLN. Shoulder complaints after
neck
dissection; is the spinal accessory nerve
involved? Br J Oral Maxillofacial Surg
2003: 41: 7–11.
Von Eisenhart-Rothe R, Matsen FA,
Eckstein F, Graichen H.
Pathomechanics in atraumatic
shoulder instability: scapular
positioning correlates with humeral
head centering. Clin Orthop Relat Res
2005: 433: 82–89.
Watson L, Balster SM, Finch C, Dalziel
R. Measurement of scapula upwardrotation: a reliable clinical
procedure.
Br J Sports Med 2005: 39: 599–603.
Struyf et al.
818