Embed Size (px)
Citation preview

Author's Accepted Manuscript
Scapular Notching in Reverse Total ShoulderArthroplasty: Now What?
John P. Taliaferro MD., Lynn A. Crosby MD.
PII: S1045-4527(14)00044-3DOI: http://dx.doi.org/10.1053/j.sart.2014.02.008Reference: YSART50583
To appear in:Semin Arthro
Cite this article as: John P. Taliaferro MD., Lynn A. Crosby MD., Scapular Notching inReverse Total Shoulder Arthroplasty: Now What?,Semin Arthro , http://dx.doi.org/10.1053/j.sart.2014.02.008
This is a PDF file of an unedited manuscript that has been accepted for publication. As aservice to our customers we are providing this early version of the manuscript. Themanuscript will undergo copyediting, typesetting, and review of the resulting galley proofbefore it is published in its final citable form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers that applyto the journal pertain.
www.elsevier.com/locate/enganabound

Scapular Notching in Reverse Total Shoulder Arthroplasty: Now What?
Authors:
1. John P. Taliaferro, MD. Medical College of Georgia, Georgia Regents University, Augusta, GA
2. *Lynn A. Crosby, MD. Department of Orthopaedics, Division of Shoulder Surgery, Medical College of Georgia, Georgia Regents University, Augusta, GA
Department of Orthopaedic Surgery, Medical College of Georgia, Georgia Regents University, 937 15th St. , Augusta, GA. 30912
Institution:
From the Medical College of Georgia, Georgia Regents University.
Address:
*Corresponding Author: Lynn A. Crosby, MD, Department of Orthopaedic Surgery, Georgia Regents University, 937 15th St., Augusta, GA 30912. Email: [email protected]

Abstract:
Scapular notching is a well known complication of reverse total shoulder arthroplasty.
While early reports revealed no ill effects on clinical outcomes, later research has shown
decreased range of motion, decreased strength, lower Constant scores, and higher pain scores. It
appears that lowering the glenosphere on the glenoid decreases contact between the humeral
component and the inferior bony pillar, decreasing the rate and grade of notching. Once notching
occurs after reverse total shoulder arthropasty , it appears that close observation in an
asymptomatic patient is sufficient. Revisions in symptomatic patients require debridement, bone
grafting, and baseplate augments.
Introduction:
Stemming from Kobel's first reverse total shoulder arthroplasty design in 1972, a myriad
of reverse shoulder prosthesis designs have followed since the 1970s [1]. These early implants
were a constrained design, requiring a fixed center of rotation leading to high rates of mechanical
failures, usually on the glenoid side. This lead to their eventual removal from the United States
market in the 1980s. Grammont continued to seek a solution to this mechanical problem, and in
1985 released an inverted version of the constrained prosthesis designs of the 1970s (Fig 1).
Lowering and medializing the center of rotation, Grammont increased the moment arm of the
deltoid and limited the shear forces responsible for the earlier glenoid failures.
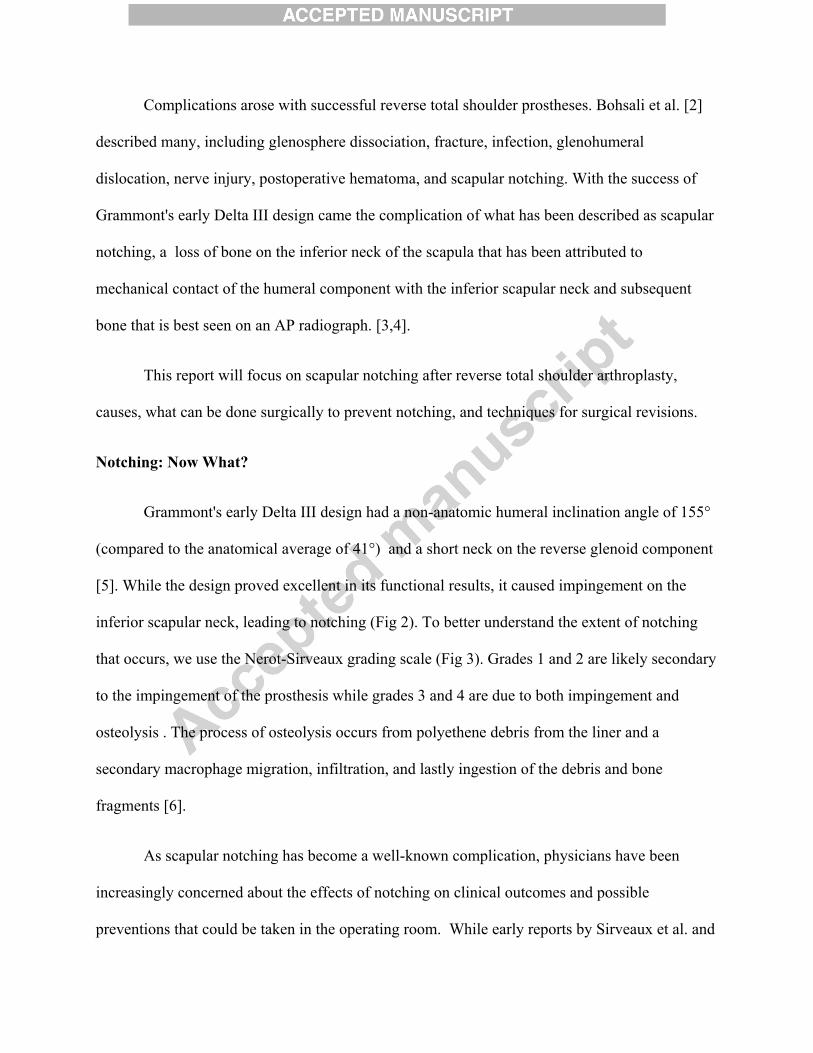
Complications arose with successful reverse total shoulder prostheses. Bohsali et al. [2]
described many, including glenosphere dissociation, fracture, infection, glenohumeral
dislocation, nerve injury, postoperative hematoma, and scapular notching. With the success of
Grammont's early Delta III design came the complication of what has been described as scapular
notching, a loss of bone on the inferior neck of the scapula that has been attributed to
mechanical contact of the humeral component with the inferior scapular neck and subsequent
bone that is best seen on an AP radiograph. [3,4].
This report will focus on scapular notching after reverse total shoulder arthroplasty,
causes, what can be done surgically to prevent notching, and techniques for surgical revisions.
Notching: Now What?
Grammont's early Delta III design had a non-anatomic humeral inclination angle of 155°
(compared to the anatomical average of 41°) and a short neck on the reverse glenoid component
[5]. While the design proved excellent in its functional results, it caused impingement on the
inferior scapular neck, leading to notching (Fig 2). To better understand the extent of notching
that occurs, we use the Nerot-Sirveaux grading scale (Fig 3). Grades 1 and 2 are likely secondary
to the impingement of the prosthesis while grades 3 and 4 are due to both impingement and
osteolysis . The process of osteolysis occurs from polyethene debris from the liner and a
secondary macrophage migration, infiltration, and lastly ingestion of the debris and bone
fragments [6].
As scapular notching has become a well-known complication, physicians have been
increasingly concerned about the effects of notching on clinical outcomes and possible
preventions that could be taken in the operating room. While early reports by Sirveaux et al. and

Werner et al. showed radiographic evidence of notching, neither study found notching
correlating with a lower Constant score or clinical deterioration. [7,8] Simovitch et al.
contradicted these findings. [9] Their report showed that notching occurred rapidly in the first 14
months and finally stabilized around 18 month. This notching did lead to lower Constant scores
and higher pain scores along with decreased range of motion and strength on further clinical
follow-up .
Following the negative outcomes related to scapular notching, the practicing shoulder
surgeon should be concerned with the prevention of poor outcomes. Several strategies have
emerged in an effort to prevent the detrimental effects of notching. One approach would be to
add an inferior tilt to the glenosphere. However, Edwards et al. reported no difference in the rate
of notching between tilted and normal set glenospheres. [10] Another strategy has been to move
the glenosphere inferiorly on the glenoid. Roche et al. led a multicenter study reporting that
lowering the glenosphere had a scapular notching rate of only 9.7% with no grades over 2 (Fig
4). [11] With this knowledge, different prostheses were made that lowered the glenosphere in
the design. However, even the newer designs did not lower the glenosphere sufficiently,
requiring surgeons to secondarily adjust the glenosphere placement on the glenoid to avoid
notching.
Having a lowered glenosphere still does not always prevent advanced glenoid notching,
but slows down the rate of notching substantially [11]. It is known that many patients are noted
to have advanced notching without symptoms. These patients are followed closely and
monitored for advancement of the notching or significant changes in the position of the
components. Once patients become symptomatic or significant shifting has occurred, surgical

intervention is required [12]. Without intervention, the glenoid component will become unstable
with progressive migration of the glenosphere post.
When revisions are required, bone quality may guide treatment options [13]. Using the
Antuna Classification system for glenoid deficiency, the shoulder surgeon is able to classify the
extent and location of the bone deficiency. Bone grafting is possible for repair, but a very
thorough debridement must be performed. With more central erosion of the glenoid, extended
cage glenoid baseplate bridges have been produced in order to allow the peg to extend into native
bone. This design also allows for bone graft to be placed to fill the defect (Fig 5). Some
glenosphere design changes have also been developed for more centrally eroded glenoids that
lateralize the humerus without the need for large bone grafts . This lateral offset may help to
restore the anatomic position of the tuberosities and may decrease the risk of acromial fractures
(Fig 6). Other improvements have been developed to usurp the need for bone graft. These
product designs include superior and posterior augmented metaglenes that fill in these defects
with built up metal continuous with the baseplate that allows for stability in these bone deficient
cases (Fig 7).
Conclusions:
Scapular notching is a well known complication of reverse total shoulder arthroplasty. It
has been shown to negatively affect patient outcomes in range of motion, strength, and pain
scores if progressing to advanced stages. To prevent this complication, lowering of the
glenosphere appears to be the best method to slow notching and improve patient outcomes.
Surgeons must take into consideration that even the use of a lowered prosthesis may not lower
the glenosphere sufficiently, and may have to place the glenosphere additionally lower to
decrease notching. If revision is required, aggressive debridement of all the polyethylene debris,
and either the use of bone grafting or metal augmentation to correct the bone deficient glenoid
may be required. Longer term follow up will be required to determine if these changes in
prosthesis design and the use of augments will make a difference in clinical outcome in the
future.
References
(1) Katz D, O'Toole G, Cogswell L, Sauzieres P, Valenti P. A history of the reverse shoulder
prosthesis. Int J Shoulder Surg. 2007;1:108-13.
(2) Bohsali KI, Wirth MA, Rockwood Jr CA. Complications of total shoulder arthroplasty. J
Bone Joint Surg Am. 2006;88(10):2279-92.
(3) DeWilde L, Mombert M, Van Petegem P, Verdonk R. Revision of shoulder replacement with
a reversed shoulder prosthesis (Delta III): report of five caes. Acta Orthop Belg,
2001;67:348-53
(4) Sirveaux F. Grammont prosthesis in the treatment of shoulder arthroplasties with massive
cuff tear. Multicenter series of 42 cases (in French) Medical doctor thesis Nancy I
University (France, 1997). In: Levigne C, Garret J, Boileau P, Alami G, Favard L,
Walch G. Scapular notching in reverse shoulder arthroplasty: is it important to avoid
it and how? Clin Orthrop Relat Res 469(9):2512-2520, 2011.

(5) Robertson DD, Yuan J, Bigliani LU, Flatow EL, Yamaguchi K. Three-dimensional analysis
of the proximal part of the humerus: relevance to arthroplasty. J Bone Joint Surg Am.
2000;82-A(11):1594-602.
(6) Nicholson G, Strauss E, Sherman S. Scapular notching recognition and strategies to minimize
clinical impact. Clin Orthrop Relat Res. 2011;469(9):2512-2520,2011.
(7) Sirveaux F, Favard L, Oudet D, Huqet D, Walch G, Mole D. Grammont inverted total
shoulder arthroplasty in the treatment of glenohumeral osteoarthritis with massive rupture
of the cuff. J Bone Joint Surg Br. 2004;86-B:388-95.
(8) Werner C, Steinmann P, Gilbart M, Gerber C. Treatment of painful pseudoparesis due to
irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total
shoulder prosthesis. J Bone and Joint Sur Am. 2005;87A:1476-86.
(9) Simovitch RW, Zumstein MA, Lohri E, Helmy n, Gerber C. Predictors of scapular notching
in patients managed with Delta III reverse total shoulder replacement. J Bone Joint Surg
Am. 2007;89(3):588-600.
(10) Edwards TB, Trappery GJ, Riley C, O'Connor DP, Elkhousy HA, Gartsman GM. Inferior
tilt of the glenoid component does not decrease scapular notching in reverse shoulder
arthroplasty: results of a prospective randomized study. J Shoulder Elbow Sur.
2012;21)5):641-6.
(11) Roche C, Wright T, Flurin PH, Grey S, Jones R, Routman H, et al: Scapular notching
radiographic analysis: recommendations for glenoid plate positioning and glenosphere
overhang in male and female patients, Submitted to ORS.

(12) Florie E and Crosby L. Scapular Notching: Danger ahead? Seminars in Arthroplasty. 24
(2013) 24-27.
(13) Antuna SA, Sperling JW, Cofield RH, Rowland CM. Glenoid revision surgery after total
shoulder arthroplasty. J Shoulder Elbow Surg 2001;10:217-24.
Figure Legends
Figure 1- Newest version of Grammont's Delta III Prosthesis (2004)
Figure 2- Grade 4 scapular notching.
Figure 3- Nerot-Sirveaux staging scale for scapular notching.
Figure 4- (A and B) No scapular notching at postoperative time points: 1 week and 23 months with lowering the implanted position of the glenosphere.
Figure 5- Extended Cage Glenoid Plate. The extended cage allows for the bone graft to fill the defect while also extending into native bone.
Figure 6-Lateralized glenospheres. Help to restore anatomic positions of the tuberosities, decreasing the rate of acromial fractures.
Figure 7- Metal solution-augmented baseplates.

Fig 1

Fig 2

Fig 3
Grade 1‐ Confined to the pillars
Grade 2‐ Contact with lower screw
Grade 3‐ Over the lower screw
Grade 4‐ Extended under the baseplate
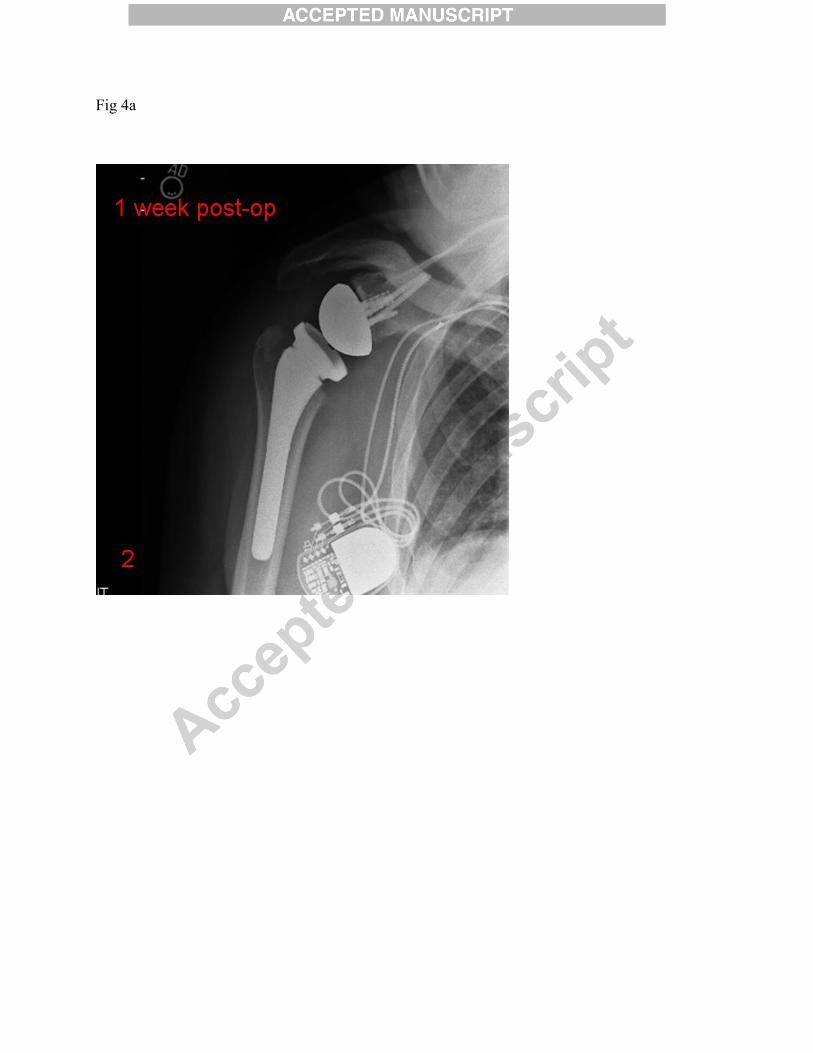
Fig 4a

Fig 4b

Fig 5

Fig 6

Fig 7








![Ann cools 3 scapular rehab [compatibiliteitsmodus]](https://img.pdfslide.us/doc/110x75/556bd7aad8b42ab2138b4af1/ann-cools-3-scapular-rehab-compatibiliteitsmodus.jpg)


















