Embed Size (px)
Citation preview
Save the Date!
2013 ANNUAL MEETING OF
THE AANS/CNS SECTION ONDISORDERS OF THE SPINE AND
PERIPHERAL NERVES
March 6 - 9, 2013JW Marriott Desert Ridge
Phoenix, Arizona
Abstract Center Opens May 16, 2012
28th Annual Meeting of the AANS/CNS Section on Disorders of the Spine and Peripheral NervesSpine and Nerve Surgery in the Era ofExcellence: Will You Measure Up?
Scientific Program
March 7-10, 2012Walt Disney World Swan and Dolphin
Orlando, Florida
We Welcome the Spine Section of the Brazilian Neurosurgical Association –2012 International Society
28thA
nnual Meeting of the A
ANS/CN
S Section on Disorders of the Spine and Peripheral N
erves SCIEN
TIFIC PROGRA
M
PROGRAM AT-A-GLANCE
WEDNESDAYMARCH 7, 2012
8:00 AM – 6:00 PMRegistrationNorthern Hemisphere Foyer
1:30 – 5:30 PMPediatric CraniocervicalSociety Meeting Oceanic 1
Special Course I – Neurosurgical Spine:Business and CompensationNorthern Hemisphere A1
Special Course II – Cases and Complications with the MastersNorthern Hemisphere A2
Special Course III – SpinalDeformityNorthern Hemisphere A3
Special Course IV – AdvancedMIS Techniques/ManagingMIS ComplicationsAmericas Seminar
Special Course V –Management of PerioperativePain, PerioperativeComplicationsAsia 3
Special Course VI – Brazil:Spine Surgery in Brazil – in conjunction with the Spine Section of BrazilianNeurosurgical AssociationAsia 4
Special Course VII – Updateson Spine Trauma, Spinal CordInjury, and Cervical SpineTrauma GuidelinesNorthern Hemisphere A4
6:00 – 8:00 PMOpening ReceptionCabana Deck at the Pool
THURSDAYMARCH 8, 2012
6:00 AM – 6:00 PMRegistrationNorthern Hemisphere Foyer
6:30 – 6:55 AMContinental BreakfastSouthern Hemisphere Foyer
Case PresentationsSouthern Hemisphere I-III
7:00 – 9:30 AMScientific Session ISouthern Hemisphere I-III
9:00 AM – 7:00 PMExhibit Hall and PosterViewingNorthern Hemisphere B-E
9:30 – 10:15 AMBeverage Break and What’s New Session INorthern Hemisphere B-E
10:15 AM – 12:30 PMOral PlatformPresentations ISouthern Hemisphere I-III
12:30 – 1:25 PMLunch and What’s NewSession IINorthern Hemisphere B-E
1:30 – 3:00 PMScientific Session II David Cahill MemorialControversies I: In-DepthDebatesSouthern Hemisphere I-III
3:00 – 3:45 PMBeverage Break and What’s New Session IIINorthern Hemisphere B-E
3:45 – 5:15 PMOral Poster Presentations I & IISouthern Hemisphere I-III andAmericas Seminar
5:15 – 6:45 PMReception in the Exhibit HallNorthern Hemisphere B-E
FRIDAYMARCH 9, 2012
6:00 AM – 5:00 PMRegistrationNorthern Hemisphere Foyer
6:30 – 6:55 AMContinental BreakfastSouthern Hemisphere Foyer Case PresentationsSouthern Hemisphere I-III7:00 – 9:00 AMScientific Session IIISouthern Hemisphere I-III9:00 – 9:20 AMMayfield AwardsSouthern Hemisphere I-III9:00 AM – 2:00 PMExhibit Hall and PosterViewingNorthern Hemisphere B-E9:30 – 10:15 AMBeverage Break and What’s New Session IVNorthern Hemisphere B-E10:15 AM – 12:15 PMOral PlatformPresentations IISouthern Hemisphere I-III12:15 – 12:30 PMAnnual Business MeetingSouthern Hemisphere I-III12:30 – 1:25 PMLunch in the Exhibit HallNorthern Hemisphere B-E12:30 – 2:30 PMLuncheon Symposium I –Revision Spine SurgeryNorthern Hemisphere A4Luncheon Symposium II –Spine TumorsNorthern Hemisphere A3Luncheon Symposium III –Cranial-Cervical JunctionNorthern Hemisphere A2Luncheon Symposium IV –Update of Lumbar SpineGuidelinesNorthern Hemisphere A1Luncheon Symposium V –Lateral RetroperitonealInterbody Fusion:Technique and OutcomesAmericas Seminar1:30 – 5:30 PMSpecial Course VIII –Peripheral Nerve Exposuresand Nerve RepairTechniquesAsia 3Special Course IX –AOSpine: Aging Spine Asia 4
SATURDAYMARCH 10, 2012
6:00 AM – 12:30 PMRegistrationNorthern Hemisphere Foyer
6:30 – 6:55 AMContinental BreakfastSouthern Hemisphere FoyerCase PresentationsSouthern Hemisphere I-III
7:00 – 8:20 AMScientific Session IV – OralPoster Presentations IIISouthern Hemisphere I-III
8:20 – 10:10 AMDavid Cahill MemorialControversies II: Spine and Peripheral NerveRapid FireSouthern Hemisphere I-III
10:10 – 10:40 AMBeverage Break Southern Hemisphere Foyer
10:40 – 11:00 AMFellowship and Clinical TrialAward UpdatesSouthern Hemisphere I-III
11:00 AM – 12:30 PMOral Posters Presentations IVSouthern Hemisphere I-III
to These Companies for Providingan Educational Grant in Supportof the 2012 Annual Meeting!
NEUROSURGICAL EDUCATION AMBASSADOR:
NEUROSURGICAL LEADERSHIP AMBASSADOR:
FUTURE OF NEUROSURGERY AMBASSADOR:
RESIDENT EDUCATION PARTNER:
ANNUAL MEETING SUPPORTERS:
as of February 10, 2012
SpecialThanks
TM
CNS11322_12DSPN_SP_Cover_Cover 2/22/12 2:00 AM Page 2
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 1
PURPOSE OF THE SPINE AND PERIPHERALNERVES SECTION
To foster the use of spinal neurosurgical methods for thetreatment of diseases of the spinal neural elements, the spineand peripheral nerves. To advance spinal neurosurgery andrelated sciences, improve patient care, support meaningfulbasic and clinical research, provide leadership in under -graduate and graduate continuing education, and promoteadministrative facilities necessary to achieve these goals.
PREVIOUS MEETINGS2011 Phoenix, Arizona2010 Orlando, Florida2009 Phoenix, Arizona2008 Lake Buena Vista, Florida2007 Phoenix, Arizona2006 Lake Buena Vista, Florida2005 Phoenix, Arizona2004 San Diego, California2003 Wesley Chapel, Florida2002 Lake Buena Vista, Florida2001 Phoenix, Arizona2000 Rancho Mirage, California1999 Lake Buena Vista, Florida1998 Rancho Mirage, California1997 Newport Beach, California1996 Lake Buena Vista, Florida1995 Phoenix, Arizona1994 Fort Lauderdale, Florida1993 Tucson, Arizona1992 Miami, Florida1991 Rancho Mirage, California1990 Captiva Island, Florida1989 Cancun, Mexico1988 Phoenix, Arizona1987 Boca Raton, Florida1986 San Diego, California1985 Greenleaf, Florida
YOUR OPINION IS PIVOTAL!A link to the online evaluations will be sent to the e-mailaddress that you used to register for the meeting. Links to theevaluation system will also be online at www.spinesection.org.You will be able to login with either your last name and the e-mail address where the link was sent or your Annual Meetingbadge number and your last name.
After logging in, simply follow the links to Claim Credits. Eachsession evaluation will be listed on this page. You will also beable to submit a request for CME credits at the same timethough submission of evaluations is not mandatory to receiveCME credit.
Your feedback is critical in helping the AANS/CNS Section onDisorders of the Spine and Peripheral Nerves plan futureeducation and Annual Meetings.
TABLE OF CONTENTS
Program At–A–Glance Inside Cover
Welcome 2
2012 Annual Meeting Committees 2
Chairman’s Biography 3
Awards and Fellowships 4
CME and General Information 11
Current and Past Officers 12
Past Program Committees 14
Disclosure Listing 16
Meeting Agenda 22
Wednesday, March 7 22
Thursday, March 8 25
Friday, March 9 29
Saturday, March 10 34
Exhibitor Information 38
Oral Platform Abstracts 42
Awards Program Abstracts 48
Oral Poster Abstracts 49
Digital Poster Abstracts 69
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES2
Dear Colleague:
On behalf of the AANS/CNS Section on Disorders of the Spine and PeripheralNerves Executive Committee, Annual Meeting Committee and MeritoriousAward Recipient, we welcome you to the Walt Disney World Swan and Dolphinfor the 2012 Annual Meeting, Spine Surgery in the Era of Excellence: Will YouMeasure Up?
Our expert faculty, dynamic scientific program and more than 200 scientificabstracts provide you with the latest advances in spine and peripheral nervesurgery as well as the information you need to advance your practice andultimately improve patient care. Our informative Scientific Sessions offercomplication management and avoidance strategies while exploring how wedefine and achieve excellence in spine and peripheral nerve surgery. Ourextensive program also features two David Cahill Memorial ControversiesSessions with master spine specialists debating their perspectives on criticalissues including, black disc disease, asymptomatic schwannoma and more.Additionally, with nine Special Courses and five luncheon symposia, thismeeting provides the optional education necessary for you to achieve excellencein your daily practice. Through didactic lectures, interactive case presentationsand discussion, these optional courses will enhance your overall meetingexperience.
The Exhibit Hall features the latest developments and advances in spine andperipheral nerve surgery with more than 60 exhibitors displaying their latestproducts and services in neurosurgical and orthopedic technology. Visit withyour corporate partners on Thursday and Friday during complimentary beveragebreaks, Lunch in the Exhibit Hall and What’s New sessions to hear the latestinformation to enhance and improve your practice.
In addition to the outstanding education available, you will experience valuablenetworking events throughout the week including the Opening Reception onWednesday evening and Reception in the Exhibit Hall on Thursday afternoon.Residents and young neurosurgeons will have the opportunity to hear a specialpresentation from Dr. Gerald E. Rodts, Jr. during the Young Neurosurgeons’Dinner on Friday evening.
We thank you again for joining us in Orlando for the 2012 Annual Meeting andhope you will take time to experience the magic that only can be found at theWalt Disney World Swan and Dolphin.
Sincerely,
WELCOME
2012 ANNUAL MEETINGCOMMITTEES
Annual Meeting ChairpersonDaryl R. Fourney
Scientific Program ChairpersonMarjorie C. Wang
Exhibits Committee Michael Y. Wang, ChairpersonAdam S. KanterDaniel M. SciubbaDaniel Hoh
2012 Scientific Abstract Review andScientific Advisory Committee Peter D. AngevineAllan J. BelzbergAli BydonJohn ChiDean ChouSanjay S. DhallDaryl R. Fourney Aruna GanjuJames S. HarropLangston T. HollyPatrick C. HsiehJohn J. KnightlyShekar N. KurpadFrank LaMarcaDaniel C. LuMichael MartinMatthew J. McGirtDavid O. OkonkwoSrinivas K. PrasadCharles A. SansurMeic H. SchmidtJustin S. SmithRobert J. SpinnerMichael P. SteinmetzAndrea L. StrayerWale SulaimanEve C. TsaiMarjorie C. WangChristopher E. WolflaJean-Paul WolinskyLynda Jun-San Yang
2012 Poster Awards and GradingCommitteeSanjay S. DhallAdam S. KanterJohn J. KnightlySrinivas K. Prasad
Christopher E. Wolfa, MD, FAANSChairperson
Marjorie C. Wang, MD, MPHScientific Program Chairperson
Daryl R. Fourney, MDAnnual Meeting Chairperson
Christopher E. Wolfla, MD, FAANS
Christopher E. Wolfla, MD, FAANS, graduated with High Honors from IndianaUniversity, Bloomington, and received his medical degree from Indiana University
School of Medicine. He completed his Neurosurgery residency at Indiana University
Medical Center under the direction of Drs. Robert L. Campbell and Paul B. Nelson.
After residency, Dr. Wolfla completed a Fellowship in Spinal Neurosurgery at the
Medical College of Wisconsin under the direction of Drs. Sanford J. Larson and Dennis
J. Maiman. Upon completion, he joined the faculty of the University of Oklahoma Health
Sciences Center, Department of Neurosurgery, where he held the Greenberg Endowed
Chair. In 2005, Dr. Wolfla returned to the Department of Neurosurgery at the Medical
College of Wisconsin. He is currently Professor of Neurosurgery and Residency
Program Director.
Dr. Wolfla has an active clinical practice centered on spinal neurosurgery. He has
authored more than 35 scientific articles and chapters in medical texts. His research
interests have focused on spine biomechanics and spinal cord physiology. Dr. Wolfla
is a member of Phi Beta Kappa, Alpha Omega Alpha and Beta Theta Pi.
Dr. Wolfla has served on the Executive Committee of the Congress of Neurological
Surgeons since 2000 and has held the offices of Member-at-Large, Education Committee
Chair, Scientific Program Chair, Annual Meeting Chair, Secretary, Vice President, and
President-Elect. In addition, Dr. Wolfla has served on the Executive Committee of the
AANS/CNS Joint Section on Disorders of the Spine and Peripheral Nerves, where he has
held the offices of Member-at-Large, Treasurer, and Chair-Elect. He is the current
Section Chair.
Dr. Wolfla has a wide variety of hobbies and outside interests. He is married to Catherine
Slocum Wolfla. Together they live in Brookfield, Wisconsin and have two children –
Andrew (18) and Julie (13).
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 3
CHAIRMAN’S BIOGRAPHY
PRESIDENTIAL ADDRESSMy Biases
THURSDAY, MARCH 8 u 8:50 AM
Dennis J. Maiman, MD, PhD2012 Meritorious Service AwardRecipient
Dennis J. Maiman, MD, PhD, was bornon July 26, 1953, in Milwaukee,Wisconsin. He attended the University ofWisconsin, Milwaukee and then theMedical College of Wisconsin (MCW),graduating in 1977. He carried out hisneurosurgical residency at the MedicalCollege of Wisconsin under thedirectorship of Sanford J. Larson, MD,PhD. He subsequently completed afellowship in spinal surgery and spinalcord injury. He was appointed AssistantProfessor of Neurological Surgery in
1984. He was also appointed Chief of Spinal Cord Injury at the VA Medical Center, andin 1986 was the Founding Medical Director of the Spinal Cord Injury Center at FroedtertHospital. Simultaneously, he obtained a PhD in Biomedical Engineering from MarquetteUniversity (1985) and was promoted to Associate Professor in 1986. In 1992 he waspromoted to Full Professor and became Director of the Spine Fellowship Program. Hewas also instrumental in the creation of SpineCare, a transdisciplinary evidence-basednonoperative program, which has since grown to four sites.
In March 2009, he became Professor and Chairman of the Department of NeurologicalSurgery and was awarded the Sanford J. Larson Professorship in the Department ofNeurosurgery/MCW in 2011. He was also the Director of Clinical Neuroscience for theMedical College of Wisconsin and Froedtert Hospital until 2011. He is a member of themajor neurosurgical associations as well as NASS and the Cervical Spine ResearchSociety. He has been an ad hoc reviewer for multiple neurosurgical and spine journalsand multiple grant review boards.
His research interests have been in the areas of biomechanics of the spine andpathophysiology of spinal cord injury, and its treatment. His predominant clinical interestis in spinal disorders and spinal cord injury. His bibliography includes 140 papers and co-authorship of Surgery of the Adult Lumbar Spine.
He has been married to Donna (nee Ziger) Maiman since 1976. Together they have fourchildren, and ten grandchildren. Off campus interests include study of Jewish law,shooting, the eternal search for the trophy Muskie, piano, and a rabid passion forbicycling.
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES4
MERITORIOUS SERVICE AWARD
Meritorious Service AwardRecipients 1990 – 20112011 Paul R. Cooper2010 Regis W. Haid, Jr. 2009 Paul C. McCormick2008 Ronald I. Apfelbaum2007 David L. Kelly, Jr.2006 John A. Jane, Sr.2005 Ulrich Batzdorf2004 Russell W. Hardy, Jr.2003 Edward C. Benzel2002 No Award Presented2001 Stewart B. Dunsker2000 Arnold H. Menezes1999 Volker K. H. Sonntag1998 Russell L. Travis1997 David G. Kline1996 No Award Presented1995 No Award Presented1994 Sanford J. Larson1993 Joseph A. Epstein1992 Charles A. Fager1991 Frank H. Mayfield1990 Ralph B. Cloward
AwardsOn pages 5 – 10 general informationregarding section sponsored researchand fellowship awards is listed. Formore information, visit theAANS/CNS Section on Disorders ofthe Spine and Peripheral Nerves website at www.spinesection.org
Research FundingThe AANS/CNS Section onDisorders of the Spine andPeripheral Nerves has establishedthree Research Grants. Dependingupon the quality of the awardsubmissions, there may be one awardin each category annually.

The Kline Award, sponsored by Integra Foundation, is for either basic or clinical researchrelated to peripheral nerves with funding up to $15,000. This research award is intended toestablish funding for research related to the peripheral nerves, and to provide a means of peerreview for clinical research projects to help improve the quality of the proposal and therefore,enhance competitiveness for National Institutes of Health (NIH) funding. The award is alsomeant to create an annual funding mechanism to establish the AANS/CNS Section on Disordersof the Spine and Peripheral Nerves as a known source for quality clinical research aimed atanswering questions pertaining to the treatment of disorders of the spine and peripheral nerves.
Chetan Bettegowda, MDChetan Bettegowda, MD, grew up in Charlotte, NC and completed his undergraduate studies inBiology and Religion at Duke University. He then entered the MD/PhD program at JohnsHopkins University School of Medicine, where he completed his PhD thesis in the laboratory of Bert Vogelstein. Upon completion of his medical education, Dr. Bettegowda entered theneurosurgery residency program at Johns Hopkins where he is a currently a chief resident. Dr. Bettegowda’s clinical interests are in neurosurgical oncology, including tumors of the brainand spine. His research interests are in the global genetic profiling of central nervous systemtumors and using the knowledge gained from these studies to develop blood based tumorbiomarkers that can be used to follow disease burden.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 5
AWARDS AND FELLOWSHIPS
Ronald I. ApfelbaumResearch Award
David Kline Research Award
The Apfelbaum Award, sponsored by Aesculap, is for either basic or clinical research related tothe spine with funding up to $15,000. This research award is intended to establish funding forresearch related to the spine, and to provide a means of peer review for clinical researchprojects to help improve the quality of the proposal and therefore, enhance competitiveness forNational Institutes of Health (NIH) funding. The award is also meant to create an annualfunding mechanism to establish the AANS/CNS Section on Disorders of the Spine andPeripheral Nerves as a known source for quality clinical research aimed at answering questionspertaining to the treatment of disorders of the spine and peripheral nerves.
Jason Liauw, MDJason Liauw, MD, is a Johns Hopkins Neurosurgery resident pursuing a spine fellowship. Dr. Liauw received his undergraduate degree from Washington University in St. Louis andmedical degree from Stanford University School of Medicine. During his tenure at StanfordUniversity, Dr. Liauw was an American Heart and Stroke Association Fellow under Dr. GarySteinberg. This research award will support his project studying the therapeutic potential ofForteo for augmenting spinal fusion.
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES6
AWARDS AND FELLOWSHIPS
The Larson Award, sponsored by DePuy Spine, is limited to clinical research with funding up to$30,000. This research award is intended to establish funding for clinically relevant researchrelated to the spine and peripheral nerves, and to provide a means of peer review for clinicalresearch projects to help improve the quality of the proposal and therefore, enhancecompetitiveness for National Institutes of Health (NIH) funding. The award is also meant tocreate an annual funding mechanism to establish the AANS/CNS Section on Disorders of theSpine and Peripheral Nerves as a known source for quality clinical research aimed at answeringquestions pertaining to the treatment of disorders of the spine and peripheral nerves.
Daniel C. Lu, MD, PhDDaniel C. Lu, MD, PhD, completed his neurosurgery training at University of California, SanFrancisco and spine fellowship with Dr. Kevin Foley at University of Tennessee. Dr. Lu is afaculty member at University of California, Los Angeles. He directs laboratory research effortsat understanding the molecular basis for conditions affecting the spine. For the Larson Award,Dr. Lu will be conducting a one-year prospective trial in determining the “fingerprint” forsymptomatic disc degeneration by looking at the molecular, radiographic and clinical profile ofdegenerated discs. This will potentially serve as a screening tool to predict success withoperative management and establish the basis for potential therapeutic molecular targets.
The Cahill Fellowship, sponsored by Synthes Spine, is awarded annually to one U.S. orCanadian trained neurosurgical resident to provide supplemental funding for advancededucation and research in disorders of the spine or peripheral nerves in the form of fellowshiptraining away from their parent institution. The amount of the award is $30,000. Applicantsshould be residents in training or ABNS eligible fellows, must provide a letter of acceptancefrom the designated mentor and program, a letter of support from their training programdirector, a description of the proposed fellowship with the educational or research goals, and a current CV.
Mark Mahan, MDMark Mahan, MD, is currently a fifth year resident at the Barrow Neurological Institute inPhoenix, AZ. Born in Tulsa, OK, Mark graduated magna cum laude from Princeton Universityin 1998. He worked in leveraged finance at a major Wall Street bank and then in private equityfor five years after his graduation. Unfulfilled academically, Mark left finance and matriculatedat Columbia University’s College of Physicians and Surgeons, graduating AOA in 2007. Duringresidency at the BNI, Mark has found interest in regenerative peripheral nerve procedures andhas established plans to spend his sixth year pursuing an in-folded fellowship under the directionof Dr. Robert Spinner at the Mayo Clinic and Dr. Justin Brown at UCSD. Mark is researchinghigh resolution magnetic resonance imaging of peripheral nerves, distal nerve transfers forbladder reanimation, and other projects.
Sanford LarsonResearch Award
Cahill Fellowship

MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 7
AWARDS AND FELLOWSHIPS
The Cloward Fellowship, sponsored by Medtronic, is awarded annually to one U.S. or Canadiantrained neurosurgical resident to provide supplemental funding for advanced education andresearch in disorders of the spine or peripheral nerves in the form of fellowship training awayfrom their parent institution. The amount of the award is $30,000. Applicants should be residentsin training or ABNS eligible fellows, must provide a letter of acceptance from the designatedmentor and program, a letter of support from their training program director, a description ofthe proposed fellowship with the educational or research goals, and a current CV.
John E. Ziewacz, MDJohn Ziewacz, MD, is currently chief resident in neurosurgery at the University of Michigan-Ann Arbor. He is a 2005 graduate of the Johns Hopkins University School of Medicine and a2010 graduate of the Harvard School of Public Health with a concentration in Health Policy. Hisresearch time was spent studying surgical safety and outcomes research at the Center forSurgery and Public Health in Boston under Dr. Atul Gawande. He became interested in spinesurgery while working with Drs. Frank LaMarca and Paul Park at the University of Michigan.He will pursue fellowship training at UCSF in July 2012 under the direction of Dr. PraveenMummaneni. He plans to pursue a career in academic spine surgery.
The Crockard International Fellowship, sponsored by DePuy Spine, is awarded annually to a neurosurgical resident or neurosurgeon from outside of the U.S. or Canada to providesupplemental funding for advanced education and research in disorders of the spine in the form of a fellowship experience in the United States or Canada. The amount of each award is $5,000. Applicants must provide a letter of acceptance from the designated mentor andprogram, a letter of support from their training program director if applicable, a description of the proposed fellowship with the educational or research goals, and a current CV.
Andrei N. Kuzmin, MDAndrei N. Kuzmin, MD, is a neurosurgeon at the Chelyabinsk State Clinical Hospital inChelyabinsk, Russia. Dr. Kuzmin finished his residency in neurosurgery at the Urals StateMedical Academy, Department of Neurology and Neurosurgery, Ekaterinburg, Russia in 2007and received his medical degree from Chelyabinsk State Medical Academy in 2002.
Dr. Kuzmin’s clinical interest is the study of modern methods of surgical management ofpatients with complex spine disorders.
Crockard InternationalFellowship
Cloward Fellowship

AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES8
AWARDS AND FELLOWSHIPS
The Sonntag International Fellowship, sponsored by Medtronic, is awarded annually to aneurosurgical resident or neurosurgeon from outside of the U.S. or Canada to providesupplemental funding for advanced education and research in disorders of the spine in the form of a fellowship experience in the United States or Canada. The amount of each award is $5,000. Applicants must provide a letter of acceptance from the designated mentor andprogram, a letter of support from their training program director if applicable, a description of the proposed fellowship with the educational or research goals, and a current CV.
Olaolu C. Akinbo, MBBSOlaolu Charles Akinbo, MBBS, received his medical training at the College of Medicine,University of Lagos, Nigeria where he obtained Bachelor of Medicine and Surgery degrees(MBBS) in 1998. His residency training in Neurosurgery was at the Department of NeurologicalSurgery, University College Hospital (UCH), Ibadan, Nigeria. During his residency, Dr. Akinboconducted research on the Epidemiology of Neurotrauma and Motorcycle Head Injury under thesupervision of Professors M.T. Shokunbi and A.O. Malomo. His interest in spine surgerydeveloped during this time as well. Dr. Akinbo plans to hone his skills further in general andcomplex spinal surgeries under Dr. Praveen V. Mummaneni at the University of California, SanFrancisco through an observational fellowship. The Sonntag International Fellowship award willcontribute towards making this a reality.
Introducing the Regis W. Haid, Jr., MD Adult Deformity Award, sponsored by Globus Medical, anew opportunity made available in 2012 intended for primary neurosurgical investigatorsinterested in clinical research in the field of adult spinal deformity. This research award isintended to provide up to $30,000 in research funding for clinically relevant research related toadult degenerative spinal deformity, and to provide a means of peer review for clinical researchprojects to help improve the quality of the proposal and therefore, enhance competitiveness forNational Institutes of Health (NIH) funding. The award is also meant to create an annualfunding mechanism to establish the AANS/CNS Section on Disorders of the Spine andPeripheral Nerves as a known source for quality clinical research aimed at answering questionspertaining to the treatment of disorders of the spine and peripheral nerves.
Justin S. Smith, MD, PhD, FAANSJustin S. Smith, MD, PhD, FAANS, received his medical degree from Mayo Medical Schooland PhD in Molecular Neuroscience from Mayo Graduate School, both in Rochester,Minnesota. He completed a general surgery internship and neurological surgery residency at theUniversity of California at San Francisco, where he served as Chief Resident in NeurologicalSurgery. Dr. Smith advanced his spine training in two fellowship programs. The first was anadult and pediatric deformity spine fellowship at the University of Virginia jointly sponsored bythe Departments of Neurosurgery and Orthopaedic Surgery. Under the tutelage of Richard G.Fessler, MD, he completed a minimally invasive spine fellowship at Northwestern University inChicago, Illinois. He is currently co-director of the UVA Spine Center, and is an AssistantProfessor of Neurological Surgery at the University of Virginia. Within the Department ofNeurological Surgery, Dr. Smith serves in several leadership roles including Director ofMinimally Invasive Spine Surgery, co-director of Spine Division and co-director of SpineFellowship.
Sonntag InternationalFellowship
Regis W. Haid, Jr., MDAdult Deformity Award
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 9
AWARDS AND FELLOWSHIPS
The Mayfield Awards are presented annually by the AANS/CNS Section on Disorders of theSpine and Peripheral Nerves to the neurosurgical residents or BC/BE fellows in North Americantraining programs who author outstanding manuscripts detailing a laboratory or clinicalinvestigation in the area of spinal or peripheral nerve disorders. This award is also applicableto individuals in DO training programs. The manuscript for this award is presented by attachingrelated information to their abstract during the abstract submission process. Two awards areavailable, one for clinical research and one for basic science research. Each recipient willreceive an honorarium of $2,000 to cover the expenses of attendance at the Annual Meeting ofthe AANS/CNS Section on Disorders of the Spine and Peripheral Nerves. Abstracts to beconsidered for the Mayfield Awards should be identified as such on the Annual Meeting abstractsubmission form and submitted prior to deadline.
Mayfield Award Recipients 1984 – 2011
2011Basic Science: Mohammed F. ShamjiClinical Science: Tyler J. Kenning
2010Basic Science: Wilson Zachary RayClinical Science: Raqeeb Haque
2009Basic Science: Daniel L. MasterClinical Science: Matthew B. Maserati
2008 Basic Science: Ann Margaret ParrClinical Science: Dennis E. Cramer,Matthew M. Kang
2007Basic Science: Sharad RajpalClinical Science: Florian Roser
2006Basic Science: Toshitaka SekiClinical Science: Benson Yang
2005Basic Science: John Y. K. LeeClinical Science: Nicholas H. Post
2004Basic Science: Bryan B. BarnesClinical Science: Michael Y. Wang
2003 No Awards Presented
2002Basic Science: Edward R. SmithClinical Science: Ketan R. Bulsara
2001Basic Science: Ketan R. BulsaraClinical Science: Gordon W. Tang
2000Basic Science: Neill M. WrightClinical Science: Viswanathan Rajaraman
1999Basic Science: Steven CashaClinical Science: Nicholas Theodore
1998 Tord D. Alden1997 Michael A. Morone
1996Basic Science: Paul C. FrancelClinical Science: Paul D. Sawin
1995 Simcha J. Weller1994 Timothy C. Ryken1993Basic Science: Allan D. LeviClinical Science: Gerald F. Tuite
1992 Rajiv Midha1991 Peter G. Gianaris1990 R. John Hurlbert1989 Richard K. Simpson, Jr.1988 No Award Presented1987 John A. Feldenzer1986 No Award Presented1985 Abhijit Guha1984 Mark N. Hadley
J. Bridger Cox, MDJ. Bridger Cox, MD, is currently in his fifth year of his neurosurgical residency at the Universityof Florida, expecting to complete his training in June 2014. Dr. Cox’s clinical interests are inspine surgery, specifically deformity correction and spine tumors. Outside of the operatingroom, Dr. Cox has an interest in socioeconomic and policy issues within neurosurgery.During his research year, Dr. Cox completed a clinical spine year under Dr. Patrick Jacob andDr. Daniel Hoh. Dr. Cox is a member of AOSpine, the Congress of Neurological Surgeons, theAmerican Association of Neurological Surgeons, and the Florida Medical Association.He attended the University of Oklahoma, graduating magna cum laude with a degree in PoliticalScience in 2003. He obtained his medical degree in 2007 at the University of Oklahoma HealthSciences Center in Oklahoma City. Dr. Cox was a member of the men’s varsity golf team at theUniversity of Oklahoma. He is a National Merit Scholar and spent time during undergradstudying at Oxford University in England. He continues to enjoy playing golf, as well ashunting, fishing, and travelling.
Friday, March 9, 9:07 – 9:12 AM119. Decreased Incidence of Venous Thrombo-Embolism After Spine Surgery with EarlyAggressive ChemoprophylaxisJoseph Bridger Cox, Catherine Koepnick, R. Patrick Jacob, Daniel J. Hoh
Mayfield ClinicalScience Award
MayfieldAwards

AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES10
Alexander E. Ropper MDAlexander E. Ropper, MD, received a BA from the University of Pennsylvania and an MD fromTufts University School of Medicine (AOA). He is currently a fifth year resident in neurosurgeryat Brigham and Women’s Hospital and Harvard Medical School. His research at Brigham andWomen’s Hospital and the Boston VA Healthcare System in the laboratories of Yang Teng, MD,PhD focuses on stem cell based restorative therapies for spinal cord injury.
Friday, March 9, 9:00 – 9:05 AM118. Human Mesenchymal Stem Cells Seeded in a Polymer Scaffold: A Novel TreatmentApproach for Spinal Cord InjuryAlexander E. Ropper, Devang Thakor, Inbo Han, Dou Yu, Hariprakash Haragopal, A. John Popp,Yang D. Teng
The Outcomes Committee Award is presented annually by the AANS/CNS Section on Disordersof the Spine and Peripheral Nerves to a neurosurgical resident or BC/BE neurosurgeon in NorthAmerica who authors an outstanding abstract presenting the results of a clinical investigation inthe area of spine or peripheral nerve disorders, that demonstrates sound methodological designand includes evaluation of patient-oriented outcomes as the primary endpoint. The recipient ofthe award will be selected by the members of the AANS/CNS Section on Disorders of the Spineand Peripheral Nerves Outcomes Committee. The award is a gift from The David and JeanWallace Fund. The recipient will receive a $2,000 honorarium to help cover the expenses ofattendance at the AANS/CNS Section on Disorders of the Spine and Peripheral Nerves AnnualMeeting. Abstracts to be considered should be identified on the Annual Meeting abstractsubmission form and submitted prior to the deadline.
Jun Jae Shin, MD, PhDJun Jae Shin, MD, PhD, graduated from the neurosurgery residency at Severance Hospital,Yonsei University College of Medicine, Seoul, Korea. He received his BM degree from YonseiUniversity and MD-PhD degrees from Yonsei University College of Medicine. He completed afellowship at Severance Hospital. He is now performing a research fellowship in NeuroSpineCenter and Research Laboratory with Dr. Jon Park at Stanford University Medical Center.
Friday, March 9, 9:14 – 9:19 AM120. The Relevance of Intramedullary High Signal Intensity and Gadolinium (Gd-DTPA)Enhancement to the Clinical Outcome in Cervical Compressive MyelopathyJun-Jae Shin, Ji Hae Lee, Woo Ho Cho, Jon Park
AWARDS AND FELLOWSHIPS
Mayfield BasicScience Award
2012 OutcomesCommittee Award
2011 AWARD RECEPIENTS
Ronald I. Apfelbaum Research Award – Zachary Adam Smith, MDDavid Kline Research Award – Jacob D. Alant, MBChB, MMED, FRCS(C)
Sanford Larson Research Award – Erica F. Bisson, MDCahill Fellowship – Timothy David Uschold, MDCloward Fellowship –Michael J. Dorsi, MD
Sonntag International Fellowship – Gurpreet Singh Gandhoke, MD Outcomes Committee – Cheerag D. Upadhyaya, MD, MS
CME CREDITThis activity has been planned andimplemented in accordance with theEssential Areas and policies of theAccreditation Council for ContinuingMedical Education through the jointsponsorship of the Congress ofNeurological Surgeons and theAANS/CNS Section on Disorders of theSpine and Peripheral Nerves. The CNS isaccredited by the Accreditation Councilfor Continuing Medical Education(ACCME) to provide continuing medicaleducation for physicians.US Physicians: The CNS designates thislive activity for a maximum of 26.75 AMAPRA Category 1 Credits™. Physiciansshould only claim credit commensuratewith the extent of their participation in theactivity. The same number of AMA PRA Category1 Credits™ awarded will be appliedtoward the Continuing Education Awardin Neurosurgery.*A maximum of 18.75 AMA PRACategory 1 Credits™may be earned forScientific Sessions only.
Physician Assistants/PhysicianExtenders/Nurses and Other AlliedHealth Professionals: Attendees willreceive credits for attendance at thegeneral Scientific Program and for anyoptional events attended. Each physicianassistant/physician extender/nurse/alliedhealth professional should contact his orher individual membership associationand certification board to determine therequirements for accepting credits. Allattendees will receive a Certificate ofAttendance.Additional CME Credits can be earned byattending the following:
Special CoursesAttendees will receive a maximum of four(4) AMA PRA Category 1 Credits™ foreach eligible half-day Special Course.Physicians should only claim creditcommensurate with the extent of theirparticipation in the activity.
Luncheon SymposiaAttendees will receive a maximum of two(2) AMA PRA Category 1 Credits™ foreach eligible Luncheon Symposium.Physicians should only claim creditcommensurate with the extent of theirparticipation in the activity.
PostersPhysicians may claim AMA PRACategory 1 Credit™ directly from theAMA for preparing a poster presentation,
which also includes the published abstracts.Physicians may claim them on their AMAPRA certificate application or applydirectly to the AMA for an AMA PRACategory 1 Credit™ certificate. Physiciansmay claim AMA PRA Category 2 Credit™for viewing scientific posters. Physiciansshould self-claim credit on their AMAPRA certificate application form.
GENERAL INFORMATIONSpeaker Ready RoomThe Speaker Ready Room, located inEurope 3, will be available:Wednesday, March 7 8:00 AM – 6:00 PMThursday, March 8 6:00 AM – 6:00 PMFriday, March 9 6:00 AM – 6:00 PM Saturday, March 10 6:00 AM – 12:30 PM All speakers and abstract presenters shouldvisit the Speaker Ready Room prior totheir presentation. All Scientific SessionFaculty are required to check in at theSpeaker Ready Room 24 hours prior totheir presentation.
Exhibit Hall Northern Hemisphere B-EThursday, March 8 9:00 AM – 7:00 PMFriday, March 9 9:00 AM – 2:00 PM
RegistrationNorthern Hemisphere FoyerWednesday, March 7 8:00 AM – 6:00 PMThursday, March 8 6:00 AM – 6:00 PMFriday, March 9 6:00 AM – 6:00 PMSaturday, March 10 6:00 AM – 12:30 PM
No Smoking PolicySmoking is not permitted at any officialAANS/CNS Section on Disorders of theSpine and Peripheral Nerves AnnualMeeting events. Smoking is alsoprohibited inside and on the grounds ofthe Walt Disney World Swan and Dolphin.
DisclaimerThe material presented at the 2012 AnnualMeeting has been made available by theAANS/CNS Section on Disorders of theSpine and Peripheral Nerves and the CNSfor educational purposes only. Thesematerials are not intended to represent theonly, nor necessarily the best method orprocedure appropriate for the medicalsituations discussed, but rather are intendedto present an approach, view, statement oropinion of the faculty, which may be helpfulto others who face similar situations.All drugs and medical devices used in theUnited States are administered inaccordance with the Food and DrugAdministration (FDA) regulations. Theseregulations vary depending on the risksassociated with the drug or medical
devices compared to products already onthe market, and the scope of the clinicaldata available.Some drugs and medical devicesdemonstrated or described within the printpublications of the AANS/CNS Section ofDisorders of the Spine and PeripheralNerves jointly sponsored by the CNS have FDA clearance for use for specificpurposes or for use only in restrictedresearch settings. The FDA has stated thatit is the responsibility of the physician todetermine the FDA status of each drug ordevice he or she wants to use in compliancewith applicable laws.Neither the content (written or oral) of anycourse, seminar or other presentation inthe program, nor the use of a specificproduct in conjunction therewith, nor theexhibition of any materials by any partiescoincident with the program, should beconstrued as indicating endorsement orapproval of the views presented, theproducts used or the materials exhibitedby the AANS/CNS Section on Disordersof the Spine and Peripheral Nerves jointlysponsored by the CNS, or by itscommittees, commissions or affiliates.
OPENING RECEPTIONWednesday, March 7 6:00 – 8:00 PMCabana Deck at the PoolEnjoy a lavish array of food andrefreshments while reconnecting withcolleagues and meeting new contacts atthe Opening Reception. Take in the magicand wonder of the reception at the WaltDisney World Swan and Dolphin. Eachmedical attendee and spouse/guestregistered for the meeting will receive onecomplimentary ticket. Resort casual attireis recommended.
RECEPTION WITH EXHIBITORSThursday, March 8 5:15 – 6:45 PM Northern Hemishpere B-EJoin us for this special event in the ExhibitHall! Interact with colleagues andcorporate contacts while enjoying pre-dinner cocktails and hors d’oeuvres.Business casual attire is recommended.
YOUNG NEUROSURGEONS’ DINNERFriday, March 9 6:30 PMSouthern Hemisphere VSpecial Presentation by Dr. Gerald E. Rodts, Jr.All residents, fellows and youngneurosurgeons are welcome. RSVP toDePuy Spine, Booth #207.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 11
CME CREDIT AND GENERAL INFORMATION
CURRENT OFFICERSChairpersonChristopher E. Wolfla Chairperson ElectJoseph S. ChengSecretaryPraveen V. MummaneniTreasurerR. John HurlbertImmediate Past ChairpersonZiya L. GokaslanMembers–at–Large Michael GroffEric L. ZagerCharles Kuntz, IV
PAST OFFICERS2010 – 2011ChairpersonZiya L. GokaslanChairperson ElectChristopher E. WolflaSecretaryMichael W. GroffTreasurerR. John HurlbertImmediate Past ChairpersonChristopher I. ShaffreyMembers–at–LargeCharles Kuntz, IVMark R. McLaughlinEric L. Zager
2009 – 2010ChairpersonChristopher I. ShaffreyChairperson ElectZiya L. GokaslanSecretaryMichael W. GroffTreasurerR. John HurlbertImmediate Past ChairpersonDaniel K. ResnickMembers–at–LargeMark R. McLaughlinChristopher E. WolflaEric L. Zager
2008 – 2009ChairpersonDaniel K. ResnickChairperson ElectChristopher I. ShaffreySecretaryMichael W. GroffTreasurerChristopher E. WolflaImmediate Past ChairpersonJoseph T. AlexanderMembers–at–LargeGregory R. TrostMark R. McLaughlinEric L. Zager
2007 – 2008ChairpersonJoseph T. AlexanderChairperson ElectDaniel K. ResnickSecretaryDaniel K. ResnickTreasurerChristopher E. WolflaImmediate Past ChairpersonCharles L. Branch, Jr.Members–at–LargeKevin T. FoleyGregory R. TrostChristopher I. Shaffrey
2006 – 2007ChairpersonCharles L. Branch, Jr.Chairperson ElectJoseph T. AlexanderSecretaryDaniel K. ResnickTreasurerChristopher E. WolflaImmediate Past ChairpersonRobert F. HearyMembers–at–LargeKevin T. FoleyDaniel H. KimGregory R. Trost
2005 – 2006ChairpersonRobert F. HearyChairperson ElectCharles L. Branch, Jr.SecretaryDaniel K. ResnickTreasurerTimothy C. RykenImmediate Past ChairpersonGerald E. Rodts, Jr.Members–at–LargeJoseph T. AlexanderDaniel H. Kim
2004 – 2005ChairpersonGerald E. Rodts, Jr.Chairperson ElectRobert F. HearySecretaryCharles L. Branch, Jr.TreasurerTimothy C. RykenImmediate Past ChairpersonRegis W. Haid, Jr.Members–at–LargeJoseph T. AlexanderRonald I. ApfelbaumDaniel H. Kim
2003 – 2004ChairpersonRegis W. Haid, Jr.Chairperson ElectGerald E. Rodts, Jr.SecretaryCharles L. Branch, Jr.TreasurerTimothy C. RykenImmediate Past ChairpersonNevan G. BaldwinMembers–at–LargeJoseph T. AlexanderRonald I. ApfelbaumRobert F. Heary
2002 – 2003ChairpersonNevan G. BaldwinChairperson ElectRegis W. Haid, Jr.SecretaryCharles L. Branch, Jr.TreasurerGerald E. Rodts, Jr.Immediate Past ChairpersonPaul C. McCormickMembers–at–LargeRonald I. ApfelbaumH. Louis Harkey, IIIRobert F. Heary
2001 – 2002ChairpersonPaul C. McCormickChairperson ElectNevan G. BaldwinTreasurerGerald E. Rodts, Jr.Immediate Past ChairpersonCurtis A. DickmanMembers–at–LargeRonald I. ApfelbaumH. Louis Harkey, IIIRobert F. Heary
2000 – 2001ChairpersonCurtis A. DickmanChairperson ElectPaul C. McCormickSecretaryNevan G. BaldwinTreasurerGerald E. Rodts, Jr.Immediate Past ChairpersonVincent C. TraynelisMembers–at–LargeH. Louis Harkey, IIISrinath SamudralaLloyd Zucker
1999 – 2000ChairpersonVincent C. TraynelisChairperson ElectCurtis A. DickmanSecretaryNevan G. BaldwinTreasurerCurtis A. DickmanImmediate Past ChairpersonStephen M. PapadopoulosMembers–at–LargeCharles L. Branch, Jr.Srinath SamudralaLloyd Zucker
1998 – 1999ChairpersonStephen M. PapadopoulosChairperson ElectVincent C. TraynelisSecretaryVincent C. TraynelisTreasurerCurtis A. DickmanImmediate Past ChairpersonRichard G. FesslerMembers–at–LargeCharles L. Branch, Jr.Mark N. HadleyJohn E. McGillicuddy
1997 – 1998ChairpersonRichard G. FesslerChairperson ElectStephen M. PapadopoulosSecretaryVincent C. TraynelisTreasurerCurtis A. DickmanImmediate Past ChairpersonEdward C. BenzelMembers–at–LargeCharles L. Branch, Jr.Mark N. HadleyJohn E. McGillicuddy
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES12
CURRENT AND PAST OFFICERS 1980-2012
1996 – 1997ChairpersonEdward C. BenzelChairperson ElectRichard G. FesslerSecretaryStephen M. PapadopoulosTreasurerPeter M. KlaraImmediate Past ChairpersonArnold H. MenezesMembers–at–LargeGary L. ReaNancy EpsteinJohn E. McGillicuddyEx–Officio MembersKevin T. FoleyMark N. Hadley
1995 – 1996ChairpersonArnold H. MenezesChairperson ElectEdward C. BenzelSecretaryStephen M. PapadopoulosTreasurerPeter M. KlaraImmediate Past ChairpersonRussell L. TravisMembers–at–LargeNancy EpsteinJohn E. McGillicuddyGary L. ReaEx–Officio MembersKevin T. FoleyMark N. Hadley
1994 – 1995ChairpersonRussell L. TravisChairperson ElectArnold H. MenezesSecretaryStephen M. PapadopoulosTreasurerPeter M. KlaraImmediate Past ChairpersonEdward C. TarlovMembers–at–LargeEdward C. BenzelNancy EpsteinGary L. Rea
1993 – 1994ChairpersonEdward C. TarlovChairperson ElectRussell L. TravisSecretaryArnold H. MenezesTreasurerRussell L. TravisImmediate Past ChairpersonVolker K. H. SonntagMembers–at–LargeEdward C. BenzelGary L. Rea
1992 – 1993ChairpersonVolker K. H. SonntagChairperson ElectEdward C. TarlovSecretaryArnold H. MenezesTreasurerRussell L. TravisMembers–at–LargeDonald J. ProloMelville P. Roberts
1991 – 1992ChairpersonCarole A. MillerChairperson ElectVolker K. H. SonntagSecretaryArnold H. MenezesTreasurerRussell L. TravisMembers–at–LargeDonald J. ProloMelville P. Roberts
1990 – 1991ChairpersonEdward S. ConnollyChairperson ElectCarole A. MillerSecretaryVolker K. H. SonntagTreasurerRussell L. TravisMembers–at–LargeArnold H. MenezesDonald J. Prolo
1989 – 1990ChairpersonEdward S. ConnollyChairperson ElectCarole A. MillerSecretaryVolker K. H. SonntagTreasurerRussell L. TravisMembers–at–LargeArnold H. MenezesDonald J. Prolo
1988 – 1989ChairpersonStewart B. DunskerSecretaryCarole A. MillerTreasurerEdward C. TarlovMembers–at–LargePhanor L. Perot, Jr.Volker K. H. Sonntag
1987 – 1988ChairpersonStewart B. DunskerSecretaryCarole A. MillerTreasurerEdward C. TarlovMembers–at–LargePhanor L. Perot, Jr.Volker K. H. Sonntag
1986 – 1987ChairpersonGeorge W. SypertSecretaryHenry H. SchmidekTreasurerEdward S. ConnollyMember–at–LargeCarole A. Miller
1985 – 1986ChairpersonRussell W. HardySecretaryHenry H. SchmidekTreasurerEdward S. ConnollyMember–at–LargeGeorge W. Sypert
1984 – 1985ChairpersonRussell W. Hardy, Jr.SecretaryStewart B. DunskerTreasurerEdward S. ConnollyMember–at–LargeHenry H. Schmidek
1983 – 1984ChairpersonSanford J. LarsonSecretaryStewart B. DunskerTreasurerEdward S. ConnollyMember–at–LargeHenry H. Schmidek
1982 – 1983ChairpersonSanford J. LarsonSecretaryStewart B. DunskerTreasurerEdward S. ConnollyMember–at–LargeHenry H. Schmidek
1981 – 1982ChairpersonSanford J. LarsonSecretaryStewart B. DunskerTreasurerEdward S. ConnollyMember–at–LargeHenry H. Schmidek
1980 – 1981ChairpersonSanford J. LarsonSecretaryStewart B. DunskerTreasurerEdward S. ConnollyMember–at–LargePhilip R. Weinstein
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 13
CURRENT AND PAST OFFICERS 1980-2012
2010 – 2011Peter D. AngevineCarlos BagleyAli BydonJohn ChiDean ChouSanjay S. DhallDaryl R. FourneyOren N. GottfriedJames S. HarropRobert F. HearyLangston T. HollyPatrick C. HsiehAdam S. KanterDean KarahaliosYevgeniy A. KhavkinFrank LaMarcaMatthew J. McGirtPraveen V. MummaneniIbrahim OmeisDaniel M. SciubbaJustin S. SmithRobert J. SpinnerMichael P. SteinmetzEve C. TsaiJamie S. UllmanMarjorie WangMichael Y. WangTimothy F. WithamJean-Paul WolinskyLynda Jun-SanYang
2009 – 2010Peter D. AngevineDean ChouDomagoj CoricSanjay S. DhallW. Jeffrey EliasDaryl R. FourneyJames S. HarropLangston T. HollyAdam S. KanterFrank LaMarcaPraveen V. MummaneniDavid O. OkonkwoShaun T. O’LearyCharles A. SansurDaniel M. SciubbaNirav K. ShahJustin S. SmithMichael P. SteinmetzEve C. TsaiMichael Y. WangLynda Jun-San Yang
2008 – 2009James P. BurkeJoseph S. ChengIra M. GoldsteinRobert F. Heary Langston T. HollyR. John Hurlbert Ryan Philip JewellCharles Kuntz, IVPaul G. MatzEhud Mendel Eric A. Potts Richard P. Schlenk Daniel M. SciubbaAllen H. ManikerMarjorie C. Wang Michael Y. WangEric L. Zager
2007 – 2008Joseph S. ChengTanvir ChoudriPeter C. GersztenMichael W. GroffZoher GhogawalaRegis W. Haid, Jr.Robert F. HearyR. John HurlbertRobert E. IsaacsMichael G. KaiserLarry T. KhooDaniel H. KimJohn J. KnightlyCharles Kuntz, IVP. Colby MaherAllen H. ManikerPaul G. MatzMark R. McLaughlinEhud MendelRajiv MidhaChad J. MorganPraveen V. MummaneniStephen L. OndraDaniel K. ResnickTimothy C. RykenChristopher I. ShaffreyMichael P. SteinmetzBrian R. SubachGregory R. TrostMichael Y. WangChristopher E. WolfaEric L. Zager
2006 – 2007Sean D. ChristieMichael W. GroffJames S. HarropR. John HurlbertRobert E. IsaacsJohn J. KnightlyCharles Kuntz, IVAllan D. LeviMark R. McLaughlinEhud MendelDaniel K. ResnickLali H.S. SekhonChristopher I. ShaffreyMichael Y. WangChristopher E. WolflaEric L. Zager
2005 – 2006Joseph T. AlexanderJuan C. BartolomeiJay Y. ChunPeter C. GersztenIra M. GoldsteinMichael W. GroffRegis W. Haid, Jr.James S. HarropRobert F. HearyR. John HurlbertMichael G. KaiserJohn J. KnightlyMark R. McLaughlinEhud MendelPraveen V. MummaneniFred NobanDaniel K. ResnickTimothy C. RykenChristopher I. ShaffreyNirav K. ShahBrian R. SubachSagun K. TuliPaul H. YoungEric L. Zager
2004 – 2005Joseph T. AlexanderJuan C. BartolomeiSteven CashaJoseph S. ChengAndrew T. DaileyAnthony K. Frempong–BoaduMichael W. GroffJames D. GuestBernard H. GuiotRegis W. Haid, Jr.James S. Harrop
Robert F. HearyR. John HurlbertRobert E. IsaacsMichael G. KaiserCharles Kuntz, IVMark R. McLaughlinEhud MendelRajiv MidhaJunichi MizunoPraveen V. MummaneniNaresh P. PatelEric A. PottsDaniel K. ResnickGerald E. Rodts, Jr.Gregory R. TrostChristopher I. ShaffreyRobert J. SpinnerEric L. Zager
2003 – 2004Joseph T. AlexanderPaul M. ArnoldAndrew T. DaileyMichael W. GroffRegis W. Haid, Jr.Robert F. HearyMichael G. KaiserCharles Kuntz, IVRajiv MidhaDaniel K. ResnickChristopher I. ShaffreyGregory R. TrostGregory C. Wiggins
2002 – 2003Joseph T. AlexanderEdward C. BenzelEugene A. BonarotiAndrew T. DaileyMichael G. FehlingsMichael W. GroffRegis W. Haid, Jr.Robert F. HearyJamie M. HendersonMichael G. KaiserDaniel H. KimRajiv MidhaPraveen V. MummaneniChristopher G. ParamoreGregory J. PrzybylskiDaniel K. ResnickChristopher I. Shaffrey
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES14
PAST PROGRAM COMMITTEES 1985-2011
2001 – 2002Joseph T. AlexanderMichael W. GroffMichael W. GropperRegis W. Haid, Jr.Robert F. HearyMichael G. KaiserCharles Kuntz, IVRajiv MidhaChristopher G. ParamoreGregory J. PrzybylskiDaniel K. ResnickGerald E. Rodts, Jr.Timothy C. RykenBrian R. Subach
2000 – 2001Joseph T. AlexanderBarry D. BirchMichael G. FehlingsRichard G. FesslerRegis W. Haid, JrH. Louis Harkey, IIIRobert F. HearyR. John HurlbertRajiv MidhaStephen L. OndraChristopher G. ParamoreDaniel K. ResnickGerald E. Rodts, Jr.Timothy C. RykenKenneth S. Yonemura
1999 – 2000Joseph T. AlexanderPaul M. ArnoldNevan G. BaldwinPerry A. BallChristopher H. ComeyBrian G. CuddyMichael G. FehlingsAllan H. FriedmanMitchell R. GropperRegis W. Haid, Jr.Andrea L. HallidayH. Louis Harkey, IIIRobert F. HearyR. John HurlbertJohn J. KnightlyCarl LauryssenAllan D. LeviChristopher G. ParamoreGerald E. Rodts, Jr.William S. RosenbergTimothy C. RykenRobert L. TielVincent C. TraynelisChristopher E. WolflaEric J. WoodardSeth M. Zeidman
1998 – 1999Joseph T. AlexanderNevan G. BaldwinAllan J. BelzbergCharles L. Branch, Jr.Brian G. CuddyRichard G. FesslerMichael G. FehlingsKevin T. FoleyRegis W. Haid, Jr.Andrea L. HallidayH. Louis Harkey, IIINoel I. PerinStephen M. PapadopoulosGerald E. Rodts, Jr.Robert L. Tiel
1997 – 1998Nevan G. BaldwinCharles L. Branch, Jr.Brian G. CuddyRichard G. FesslerH. Louis Harkey, IIIGerald E. Rodts, Jr.
1996 – 1997Ronald I. ApfelbaumPaul M. ArnoldNevan G. BaldwinPerry A. BallAllan J. BelzbergBrian G. CuddyCurtis A. DickmanKevin T. FoleyH. Louis Harkey, IIIJames P. HollowellDavid G. KlinePaul C. McCormickChristopher G. ParamoreNoel I. PerinCharles B. Stillerman
1995 – 1996Nevan G. BaldwinBrian G. CuddyKevin T. FoleyAllan H. FriedmanRegis W. Haid, Jr.H. Louis Harkey, IIIPatrick W. HitchonJames P. HollowellRichard K. OsenbachAllan H. FriedmanNoel I. PerinRobert B. SnowRichard H. TippetsDennis G. Vollmer
1994 – 1995Charles L. Branch, Jr.David W. CahillPaul R. CooperCurtis A. DickmanMichael G. FehlingsRegis W. Haid, Jr.H. Louis Harkey, IIIJames P. HollowellPeter M. KlaraJohn J. KnightlyJohn E. McGillicuddyEugene Rossitch, Jr.Charles B. StillermanVincent C. Traynelis
1993 – 1994David W. CahillCurtis A. DickmanRichard G. FesslerPeter G. GianarisH. Louis Harkey, IIIPaul C. McCormickRuss P. NockelsMoris SenegorVincent C. Traynelis
1992 – 1993Charles L. Branch, Jr.David W. CahillCurtis A. DickmanRichard G. FesslerRegis W. Haid, Jr.Robert J. MartinJohn E. McGillicuddyStephen M. PapadopoulosNoel I. PerinGary L. ReaMoris Senegor
1991 – 1992Bennett BlumenkopfCharles L. Branch, Jr.David W. CahillRichard G. FesslerStephen M. PapadopoulosGary L. Rea
1990 – 1991Joy AprinBenjamin G. BennerLawrence F. BorgesNancy EpsteinEmily D. Friedman
1989 – 1990Bennett BlumenkopfPaul D. DernbachNancy EpsteinEdward C. Tarlov
1988 – 1989John C. GodershyPatrick W. HitchonArnold H. MenezesCarole E. MillerRussell L. Travis
1987 – 1988Melville P. RobertsRichard SaundersVolker K. H. SonntagRussell L. TravisHarold A. Wilkinson
1986 – 1987Joel N. AbromovitzTimothy HarringtonRobert S. HoodVolker K.H. Sonntag
1985 – 1986Stanley J. GoodmanBarth A. GreenJohn F. HoweHector E. JamesRandall W. SmithVolker K.H. SonntagPhilip R. Weinstein
1984 – 1985Barth A. GreenGeorge W. Sypert
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 15
PAST PROGRAM COMMITTEES 1985-2011
Behrooz A. Akbarnia, MDF
Consulting Agreement – DePuy Spine (2);K2M (2); Ellipse (2); NuVasive (2) (3)Other – DePuy Spine (6); K2 M (6);NuVasive (6); Ellipse (6); Journal ofOrthopaedic Science (4); OREF (6);Scoliosis Research Society (7); OREF (7);Growing Spine Foundation (7)Royalty – DePuy Spine (6)
Joseph T. Alexander, MDP, F
Consulting Agreement – Stryker Spine (2)
Christopher P. Ames, MDF
Consulting Agreement – DePuy (2);Medtronic (2); Stryker (2)Royalty – Aesalgs (2); LAWX (2)
Ronald I. Apfelbaum, MDF
Other – Medtronic (6)Royalty – Aesculap (2)
J. Brad Bellotte, MDP
Ownership Interest – InnovativePerformance Technologies, Inc. (8);Vigilance Physician Services, LLC (8)
Edward C. Benzel, MDF
Ownership Interest – AxioMed (8)Royalty – DePuy (6); Elseviere (6)
Deborah L. Benzil, MD, FACS, FAANSF
Honoraria – BrainLab (6)
Sigurd Berven, MDF
Consulting Agreement – Biomet (2);DePuy Spine (2); Medtronic (2)Ownership Interest – Acculif (2)
Shay Bess, MDF
Consulting Agreement – Allosource (6);DePuy Spine (6)Royalty – Pioneer (6)
Mark H. Bilsky, MDF
Royalty – Depuy Spine (2)
Oheneba Boachie-Adjei, MDF
Honoraria – K2M (2); Osteotech (6)Other – DePuy Spine (6)Royalty – DePuy Spine (6); K2M (6)
Christopher Bono, MDF
Consulting Agreement – Harvard ClinicalResearch Institute (2)Royalty – Informa Health Care (6); WolterKluwer (6)
Charles L. Branch, MDF
Consulting Agreement – Medtronic (2)Royalty – Medtronic (6)
Darrel S. Brodke, MDF
Consulting Agreement – Medtronic (2)Ownership Interest – Amedica (6);Pioneer (6); Vertiflex (6)Royalty – Amedica (2); DePuy Spine (2)
Douglas C. Burton, MDF
Consulting Agreement – DePuy Spine (6)Other – DePuy Spine (6)Royalty – DePuy Spine (6)
Ali Bydon, MDP, F
Other – Depuy Spine (6)
Jens Chapman, MDF
Other – Alseres Pharmaceuticals (6);Alseres Pharmaceuticals (6); AOSNA (6);HJ Wyss Foundation (6); Medtronic (6);Stryker (6)
John Chi, MDP, F
Consulting Agreement – Synthes (2)(3)
Theodore J. Choma, MDF
Consulting Agreement – Gentis, Inc (2),Stryker Spine (2)
Dean Chou, MDP, F
Honoraria – Stryker (2)
Domagoj Coric, MDF
Consulting Agreement – Depuy Spine (2);Pioneer Surgical (2); Spinal Motion (2);Spine Wave (2)
Reginald J. Davis, MDF
Consulting Agreement – Vertiflex (2)
Mark B. Dekutoski, MDF
Consulting Agreement – Mayo MedicalVentures/Medtronic (2)Honoraria – AO Foundation (6)Other – Broadwater Associates CMEGroup (6); DePuy (6); Medtronic (6);Stryker (6); Synthes (6)
Vedat Deviren, MDF
Consulting Agreement – NuVasive (2);Stryker (2)Other – Medtronic; Depuy (6); Stryker(6); Synthes (6); Johnson & Johnson (6);NuVasive (6)Royalty – NuVasive (6)
Richard G. Fessler, MDF
Consulting Agreement – Medtronic (2)Honoraria – DePuy (6)Ownership Interest – In QueueInnovations (7)Royalty – DePuy (6); Medtronic (6);Stryker (6)
Kevin T. Foley, MD, FACSP, F
Consulting Agreement – ArthroCare (2);Medtronic (2); NuVasive (2)Intellectual Fees – ArthroCare (6)Ownership Interest – Discgenics (3);TrueVision (3)Royalty – Medtronic (6)
Steven D. Glassman, MDF
Royalty – Medtronic (2)Salary – Norton Health Care (5)
Ziya L. Gokaslan, MDP, F
Honoraria – AO North America (7)Other – AANS (6); AO FoundationLectures (6); AO North AmericaFellowship Funding (6); DePuy (6);AOSpine Research Support (6);Medtronic (6); NREF Fellowship Funding(6); Spinal Kinetics Stock (8); US SpineStock (8)Ownership Interest – Spinal KineticsStock (8)
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES16
DISCLOSURES
The AANS/CNS Section on Disorders of the Spine and Peripheral Nerves and the CNS control thecontent and production of this CME activity and attempt to assure the presentation of balanced,objective information. In accordance with the Standards for Commercial Support established by theAccreditation Council for Continuing Medical Education, anyone in the position to control the contentof the educational activity is asked to disclose any relationship they have with commercial companies.Individuals who have disclosed a relationship* with commercial companies whose products may haverelevance to their participation in the Annual Meeting are listed here.
*Relationship refers to receipt of royalties, consultantship, funding by research grant, receiving honorariafor educational services elsewhere, or any other relationship to a commercial company that providessufficient reason for disclosure.
Key:Faculty = FPlanner = P
Positional Interest Codes:(1) CEO (5) Employee(2) Consultant (6) N/A(3) Director (7) Officer(4) Editorial Board (8) Owner
Michael W. Groff, MD, FACSP, F
Consulting Agreement – EBI SpineBiomet (2); Smith & Nephew (2)Royalty – Depuy Spine (2)
Munish Gupta, MDF
Consulting Agreement – DePuy Spine (2);Lanx (2); Osteotech (2)Honoraria – AO (2)Intellectual Fees – Medtronic (6)Other – FOSA (7)Ownership Interest – Acrotech (6); J&J(6); Pfizer (6); Pioneer (6); Proctor andGamble (6)Royalty – DePuy Spine (6)
Regis W. Haid, MDF
Consulting Agreement – Globus Medical(2); Piedmont Health Care (2)Other – NuVasive (6); Globus Medical(6); Medtronic (6)Ownership Interest – Spine Universe (4)Royalty – Medtronic (6)
James S. Harrop, MD, FACSP, F
Consulting Agreement – DePuy Spine (2)Honoraria – Ethicon (6), Stryker Spine (6)Other – Axiomed (6); Geron (6)
Robert Hart, MDF
Consulting Agreement – DePuy Spine (6)Honoraria – Synthes (6)Other – DePuy Spine (6); Medtronic (6);OREF (6); Spine Connect (6); Synthes (6)Royalty – Seaspine (6)
Robert F. Heary, MDP, F
Consulting Agreement – DePuy Spine (6)Other – Biomet Spine (6); DePuy Spine(6)Royalty – Depuy Spine (6); ThiemeMedical Publishers (6)Royalty – Zimmer Spine (6)
Michael S. Hisey, MDF
Other – Zimmer (6)Royalty – LDR Spine (6); Zimmer (6)
Langston T. Holly, MDF
Consulting Agreement – Medtronic (6)
Richard A. Hostin, MDF
Honoraria – DePuy Spine (6)Other – Axial Biotech (6)
Patrick C. Hsieh, MD, MScP, F
Consulting Agreement – Depuy (2);Medtronic (2)
R. Patrick Jacob, MDF
Consulting Agreement – Synthes Spine (2)
Michael Janssen, MDF
Other – AOSNA (6)
J. Patrick Johnson, MDP
Consulting Agreement – Alphatec (2);Pioneer Medical (2); SpineWave (2)Other – FlexUspine (6)
Iain H. Kalfas, MDP, F
Honoraria – Stryker Spine (6)Royalty – Mako Surgical (6)
Adam S. Kanter, MDP, F
Consulting Agreement – Lanx (2);NuVasive (2)
Dean Karahalios, MDP
Consulting Agreement – Anulax (2); Lanx(7); Medtronic (2)Ownership Interest – Lanx (7)Royalty – Anulax (2); Lanx (7); Medtronic(2)
Eric Klineberg, MDF
Consulting Agreement – Synthes (6)Honoraria – DePuy Spine (6); Stryker(6); Synthes (6)Other – AO (6); OREF (6); Synthes (6)
Branko Kopjar, MDF
Consulting Agreement – Cerapedics, Inc(2); Lanx, Inc. (2); Scient'X (2);SpineMark (2); SpineSmith (6)
Tyler R. Koski, MDF
Consulting Agreement – Medtronic (6)Honoraria – Depuy (6); Stryker (6)
Charles Kuntz, IV, MDP, F
Consulting Agreement – Synthes (2)Other – AOSpine – Research andEducation (6); Synthes (6); Stryker –Research/Education (6)Ownership Interest – Mayfield Clinic (8);CKIV Alignment (8); PrecisionRadiotherapy (8); Priority Consult (8);The Christ Hospital Spine Surgery Center(8)Salary – University of Cincinnati (5)
Frank La Marca, MDP, F
Consulting Agreement – Biomet (6);Globus (6); Lanx (6); Stryker (6)Honoraria – Medtronic (6)
Virginie Lafage, PhDF
Other – Nemaris (7)Ownership Interest – Nemaris (8)
Lawrence LenkeF
Other – Axial Biotech (6); DePuy Spine(6)Royalty – Medtronic (6); Quality MedicalPublishing (6)
John C. Liu, MDF
Consulting Agreement – Medtronic (2)
Matthew McGirt, MDF
Other – Research Grants from DepuySpine (6); Globus Medical (6)
Mark R. McLaughlin, MDF
Consulting Agreement – Spine Wave (6)Ownership Interest – Spine Wave (6)
Stefan A. Mindea, MDF
Consulting Agreement – DePuy (6);Globus (6); Medtronic (6)
Praveen V. Mummaneni, MDP, F
Consulting Agreement – DePuy Spine (2);Medtronic (2)Ownership Interest – 2N LLC (8)Royalty – 2N LLC (Royalty from DePuySpine and QMP Publishers) (8)
Gregory Mundis, MDF
Consulting Agreement – K2M (6);NuVasive (6)Other – DePuy Spine (6)
Eric W. Nottmeier, MDF
Consulting Agreement – MedtronicNavigation (2)Royalty – Globus (2)
Pierce D. Nunley, MDF
Consulting Agreement – LDR Spine (2);Spinal Motion (2)Royalty – K2 Medical Inc. (2)
Michael F. O’Brien, MDF
Consulting Agreement – DePuy Spine (2);Medtronic (2); Osteotech (6)Intellectual Fees – DePuy Spine (6)Ownership Interest – Axial Biotech (6)Royalty – DePuy Spine (6); Medtronic (6)
David O. Okonkwo, MD, PhDP, F
Consulting Agreement – Lanx (2);Medtronic (2)
Mick J. Perez-Cruet, MD MSF
Consulting Agreement – Aesculap (2);Stryker (2); Zimmer Spine (2)Ownership Interest – MI4Spine (1);Spineology (2); Thompson MIS (3)
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 17
DISCLOSURES
Daniel L. Peterson, MDF
Consulting Agreement – OrthoKinematics(6); OsteoMed (6); Stryker (6)Other – LDR Spine (6)
Frank Phillips, MDF
Consulting Agreement – NuVasive (2)
Luiz Pimenta, MDF
Consulting Agreement – NuVasive (2);Zyga Tech (2)
Eric A. Potts, MDP, F
Consulting Agreement – Lanx (2);Medtronic (2)Ownership Interest – Lanx (8)Royalty – Medtronic (6)
Srinivas K. Prasad, MDP, F
Consulting Agreement – Synthes Spine (6)Honoraria – Stryker Spine (6)
Daniel Refai, MDF
Consulting Agreement – Aesculap ImplantSystems (2); Stryker Education (2)
Laurence D. Rhines, MDF
Honoraria – Biomet (2); Medtronic (2);Stryker (2)
W.B. Rodgers, MDF
Consulting Agreement – Exactech (2);NuVasive (2)Ownership Interest – NuVasive (2)Royalty – NuVasive (2)
Gerald E. Rodts, Jr., MDF
Consulting Agreement – Globus Medical,Inc. (2); Medtronic (2); Orthofix, Inc. (2)Other – SpineUniverse.com (3)Royalty – Globus Medical, Inc. (2)
Timothy C. Ryken, MD, MS, FACSF
Consulting Agreement – Eisai (2);Medtronic Inc (2); Merck Inc./Schering-Plough Inc. (2)
Charles A. Sansur, MD, MHScP, F
Consulting Agreement – Medtronic (2);Synthes (2)
Rick Sasso, MDF
Other – Cerapdics (6)Royalty – Medtronic (6)
Frank Schwab, MDF
Consulting Agreement – DePuy Spine (2)Honoraria – Medtronic (6)Other – Medtronic (6); Nemaris (7); SRS (6)Ownership Interest – Nemaris (8)
Daniel M. Sciubba, BS, MDF
Consulting Agreement – Globus (2)Honoraria – Depuy (6); Medtronic (6)
Christopher I. Shaffrey, MD, FACSF
Consulting Agreement – Biomet (6)Honoraria – Depuy (6); Stryker (6)Other – AOSPINE North America (6);Department of Defense (6); Journal ofNeurosurgery (4); National Institutes ofHealth (6); NuVasive (6); Spine (4)Royalty – Medtronic (6)
Jonathan D. Sherman, MDF
Consulting Agreement – Depuy (2);Medtronic (2)
Justin S. Smith, MD, PhDP, F
Consulting Agreement – Axial Biotech(2); Biomet (2); Medtronic SofamorDanek (2)Honoraria – Globus (6)Other – DePuy (6); Medtronic SofamorDanek (6)
Michael P. Steinmetz, MDP, F
Consulting Agreement – Medtronic (2)Honoraria – Biomet Spine (2)
John K. Stokes, MDF
Other – LDR Spine (6)Royalty – Genesys Orthopedics (6)
Antoine Tohmeh, MDF
Consulting Agreement – NuVasive (2)
Vincent C. Traynelis, MDF
Consulting Agreement – Medtronic (2);United HealthCare (2)Other – Globus (6)Royalty – Medtronic (6)
Eve C. Tsai, MD, PhD, FRCSCP, F
Other – BrainLab (6)
Juan S. Uribe, MDF
Consulting Agreement – Medtronic (2);NuVasive (2); Orthofix (2)
Alexander R. Vaccaro, MDF
Consulting Agreement – Gerson LehmanGroup (2); Guidepoint Global (2);Medacorp (2)Ownership Interest – Advanced SpinalIntellectual Properties (6); BonovoOrthopaedics (6); ComputationalBiodynamics (6); Cross Current (6);Cytonics (6); Disc Motion Technology(6); Electrolux (6); Flagship Surgical (6);Flow Pharma (6); Gamma Spine (6);Globus Medical (6); In Vivo (6); K2Medical (6); Location Based Intelligence(6); Neucore (6); Orthovita (6); ParadigmSpine (6); Progressive SpinalTechnologies (6); R.I.S (6); ReplicationMedica (6); Small Bone Innovations (6);Spine Medica (6); Spinology (6); StoutMedical (6); Syndicom (6); Vertiflex (6)Royalty – Aesculap (6); Biomet (6);DePuy (6); Globus Medical (6); K2Medical (6); NuVasive (6); Stryker Spine(6)
Marjorie C. Wang, MD, MPHP, F
Salary – Robert Wood Johnson PhysicianFaculty Scholars Program (6)
Michael Y. Wang, MDP, F
Consulting Agreement – Aesulap Spine(2); Biomet (2);Depuy Spine (2)Ownership Interest – NeuroConsultingSpecialists, LLC (8)
William Charles Welch, MD, FACS, FICSF
Consulting Agreement – Best Doctors (2);Synthes Spine (2); Zimmer Spine (2)Ownership Interest – Pittsburgh StandardSpine (7); Welch Research andDevelopment (8)
Timothy F. Witham, MD, BSP, F
Honoraria – Globus Medical (6); StrykerSpine (6)Other – Integra Life Science (6)
Eric J. Woodard, MDP, F
Honoraria – Depuy Spine (2)Ownership Interest – In Vivo Therapeutics(7)Royalty – Stryker Spine (2)
Lynda Jun-San Yang, MD, PhDP, F
Other – Sparton Corp. (3)
Sangwook Yoon, MDF
Other – AOSNA (6); Biomet (6);OMEGA (6); OREF (6); Phygen (6)Royalty – Nexgen (6); Stryker (6)
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES18
DISCLOSURES
Bizhan Aarabi, MDF
Khalid M. Abbed, MDF
Kalil G. Abdullah, BSF
Hamed AbhariF
Owoicho Adogwa, BS, MPHF
Vijay Agarwal, MDF
Basheal M. Agrawal, MDF
Amro Al Habib, MD, FRCSC, MPHF
Todd AlaminF
Ahmed Mustafa Alaqeel, MDF
Fahad AlbadrF
Abdulrahman AldakkanF
Amro Al-HabibF
Warren J. Alilain, PhDF
Matthew D. Alvin, BAF
Anubhav Gautam Amin, BSF
Beejal Y. Amin, MDF
Richard C. Anderson, MDF
Peter D. Angevine, MDP, F
Aluizio Augusto Arantes, MDF
Paul M. Arnold, MDF
Robert Thomas ArrigoF
Anthony L. Asher, MD, FACSF
Mark Attiah, BSF
Ranjith BabuF
Carlos A. Bagley, MDF
Richard A. Bailey, BS, MHSF
Usha Balmuri, MDF
Robert J. Banco, MDF
Michal BarnaF
Eduardo C. Barreto, MDF
Evan Begun, BSF
Allan J. Belzberg, BSc, MD, FRCS(C)F
Erica Fay Bisson, MDF
Benjamin Blondel, MDF
Claire BlumenthalF
Maxwell Boakye, MDF
Margaret BoltesF
Ricardo V. Botelho, MDF
Cammi Bowman, RN, MSNF
Colten D. Bracken, BSF
Dylan BrittF
Paul A. BroadstoneF
Douglas L. Brockmeyer, MDF
Janice Bynum, CRNFAF
Kevin S. Cahill, MD, PhDF
Eugene Carragee, MDF
Steven Casha, MD, PhDF
Srita Chakka, BAF
Ivan ChengF
Joseph S. Cheng, MD, MSP, F
Brandon G. Chew, MDF
Woo Ho ChoF
Woojin Cho, MD, PhDF
Ephraim W. Church, MDF
Megan Clark, MSF
Michelle J. Clarke, MDF
Thomas C. Coburn, MDF
Jean-Valery Coumans, MDP, F
Daniel E. Couture, MDF
Joseph Bridger Cox, MDF
George Austin CrabillF
Jill Curran, MSF
Andrew T. Dailey, MDF
Fernando L. Dantas, MDF
Stephen J. Dante, MDF
Marcio V. de Carvalho, MDF
Ronald de Lucena Farias, MDF
Geraldo de Sa Carneiro Filho, MDF
Jason DemakakosF
Clinton J. Devin, MDF
Sanjay S. Dhall, MDP, F
Marine Dididze, MD, PhDF
Dalton Dietrich, PhDF
Ian G. Dorward, MDF
Andrea F. Douglas, MDF
Jan W. Duncan, MDF
Kurt M. Eichholz, MDPBenjamin M. Ellingson, PhDF
Samuel Estronza-Ojeda, MDF
Asdrubal Falavigna, PhDF
Daniel Robert Fassett, MDF
Ryan Faught, BSF
Michael G. Fehlings, MD,PhD, FRCSC, FACSF
Douglas S. Fenton, MDF
Joel Finkelstein, MDF
Charles Fisher, MDF
Joanne FordenF
Daryl R. Fourney, MDP, F
John France, MDF
Allan H. Friedman, MDF
Steven E. Gaede, MDF
Aruna Ganju, MDP, F
Marcus J. GatesF
John W. German, MDF
Zoher Ghogawala, MD, FACSP, F
Yazhini Gnanasambanthan, MBBSF
Linda Gonia, MPAF
Oren N. Gottfried, MDF
Barth A. Green, MDF
Joey Kevin Grochmal, MDF
Mari L. Groves, MDF
Betsy H. Grunch, MDF
Yoon Ha, MD, PhDF
Mark N. Hadley, MD, FACSF
Matthew HaleF
Casey H. Halpern, MDF
D. Kojo Hamilton, MDF
Inbo Han, MDF
Amgad S. Hanna, MDF
Hariprakash Haragopal, BTechF
J. Frederick Harrington, MDF
Roger Hartl, MDF
Alexander Hass, MDF
Melanie Hayden, MD, MSF
Sharon Hayden, BSF
Marie-Noelle Hebert-Blouin, MDF
Judd HeidemanF
Joshua E. Heller, MDF
Yuichi Hirose, MD, DScF
Chris Ho, BAF
Daniel J. Hoh, MDF
Jeffrey Holtz, PAF
Brian James Hood, MDF
Wesley Hsu, MDF
R. John Hurlbert, MD, PhDP, F
Namath Syed Hussain, MDF
Tatsushi Inoue, MD, PhDF
Aleksandra IvanovicF
Jeffrey T. Jacob, MDF
Line Jacques, MDF
Amit Jain, BSF
Deeptee JainF
Sara JamesF
Michael Jirjis, BSF
Joseph John Joshua, MSEF
Michael G. Kaiser, MD, FACSP, F
Udaya K. Kakarla, MDF
Samuel KalbF
Spyridon Karadimas, MDF
Isaac KarikariF
Manish K. Kasliwal, MD, MChF
Khaled Kebaish, MDF
Marie Kerr, CCRPF
Adam KhanF
Helene T. Khuong, MD, FRCS(C)F
Kee Duk Kim, MDF
Michel Kliot, MDF
John J. Knightly, MDP, F
Catherine KoepnickF
Linda A. Koester, BSF
Jordan KomisarowF
Daniel R. Kramer, BAF
William E. Krauss, MDF
Ajit A. Krishnaney, MDF
Jan KrylF
Ranjan KumarF
Shigehiko KunoF
Shekar N. Kurpad, MD, PhDP, F
Kwaku A. KyereF
Shivanand P. Lad, MD, PhDF
Jean-Charles Lamy, PhDF
Ilya Laufer, MDF
Ji Hae LeeF
Allan D. Levi, MD, PhD, FACSF
Michael Lim, MDF
Chia-Ying Lin, PhDF
Jennifer Lindstedt, NPF
Daniel C. Lu, MD, PhDP, F
Daniel LubelskiF
Subu N. Magge, MDF
Mark Mahan, MDF
Dennis J. Maiman, MDF
George Malcolmson, BSF
Neil R. Malhotra, MDF
Eileen Maloney-Wilensky, ARNPF
Brook I. Martin, PhD, MPHF
Jonathan Martin, MDF
Michael D. Martin, MDP, F
Marcos Masini, MDF
Eric M. Massicotte, MDF
Keishi Mauro, MDF
Marcus D. Mazur, MDF
John E. McGillicuddy, MDF
Paul J. McMahonF
Angus McWilliamsF
Ankit Indravadan Mehta, MDF
Stephen Mendenhall, BSF
Rajiv Midha, MDF
Brian D. Milligan, MDF
Sohail Mirza, MDF
Peter ModeraF
Urvij Modhia, MDF
Zahra Mohajernejadfard, MDF
Eun Su MoonF
Timothy A. Moore, MDF
Osmar Moraes, MDF
Robin MottackelF
Thomas Mroz, MDF
Marcelo L. Mudo, MDF
Michael Mumert, MDF
Gisela Murray, MDF
Lumine NaF
David M. Neils, MDF
Petr Nesnidal, MDF
Agne NoujokasF
Amy S. Nowacki, PhDF
Timothy Ryan Owens, MDF
John Park, MDF
Jon ParkF
Ki ParkF
Paul Park, MDF
Yoon-Shin ParkF
Scott L. Parker, MDF
Emil Antonio PastranaRamirez, MDF
Akil Patel, MDF
Joseph PerraF
Dmitriy Petrov, BAF
Kenneth Pettine, MDF
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 19
DISCLOSURES
NOTHING TO DISCLOSEIndividuals who have reported they do not have any relationship with commercial companies are listed here.
Mark A. Pichelmann, MDF
Rae PodabinskiF
David W. Polly, MDF
A. John Popp, MDF
Nader Pouratian, MD, PhDF
Gustavo Pradilla, MDF
Matthew R. Quigley, MDF
Shayan Rahman, MDF
Rajesh Reddy, MBBS, FRACSF
Daniel K. Resnick, MDP, F
Juan Christian Ribas Nijkerk, MDF
Alex Riccio, BSF
Daniele Rigamonti, MDF
Gloria E. Rodriguez-Vega, MDF
John David Rolston, MD, PhDF
Alexander E. Ropper, MDF
Michael K. Rosner, MDP, F
Jose M. Rotta, MDF
Fanor Manuel Saavedra, MDF
Rachel Sarabia-Estrada, DVM,PhDF
Kajana SatkunendrarajahF
Dwight Saulle, MDF
Justin K. ScheerF
Terry K. Schiefer, MDF
Brian Schmit, PhDF
James M. Schuster, MDF
J. Sanford Schwartz, MDF
Theodore H. Schwartz, MD, FACSF
David L. Semenoff, MDF
Ericson Sfreddo, MDF
Hamid M. Shah, MDF
Antos ShakhbazauF
David Shau, BSF
Jun-Jae Shin, MD, PhDF
Motoi ShodaF
Brenda A. Sides, MAF
Jerry Silver, PhDF
Frederick A. Simeone, MDF
Marcelo S. Simoes, MDF
Laura Ann Snyder, MDF
Robert J. Spinner, MDP, F
Sherman C. Stein, MDF
James Harris Stephen, MDF
Robert StetsonF
Geoffrey E. Stoker, BSF
Andrea L. Strayer, BSNP, F
Jan StulikF
Brian R. Subach, MDPOlawale Sulaiman, MD, PhD, FRCS(C)P, F
Christopher SwartzF
Steven Takemoto, PhDF
Jessica A. Tang, BSF
Phiroz E. Tarapore, MDF
Yang D. Teng, MD, PhDF
Devang Thakor, PhDF
Khoi Duc Than, MDF
Tracey T. ThanF
Nicholas Theodore, MD, FACSF
Zane ThompsonF
Tarik Tihan, PhDF
Pelu Tran, BSF
Gregory R. Trost, MDP, F
Luis M. Tumialan, MDF
Payman Vahedi, MDF
Heather Vallier, MDF
Steven VanniF
Aditya Vedantam, MDF
Luis M. Vialle, MDF
Frank D. Vrionis, MD, PhDF
Tomas VyskocilF
Huaping Wang, PhDF
Lin Wang, MDF
Philip R. Weinstein, MDF
Robert G. Whitmore, MDF
Peter Witt, MDF
Christopher E. Wolfla, MD, FAANSP, F
Jean-Paul Wolinsky, MDP, F
Cyrus Chi-Ho Wong, MD, BScF
Kirkham Wood, MDF
Victor C. Yang, PhDF
Daniel Yavin, MDF
Dou YuF
Patti L. Zadnik, BAF
Eric L. Zager, MDP, F
Huina ZhangF
Scott ZuckermanF
Corinna ZygourakisF
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES20
NON-FDA APPROVED LISTINGFaculty Presentations Including Non-FDA Approved Investigational Drugs or Devices
Scientific Session I – What’sOn Your Report Card?Daryl R. Fourney
Scientific Session III –Complication Avoidance andManagementPraveen V. MummaneniMichael Y. Wang
David Cahill MemorialControversies II Spine andPeripheral Nerve – Rapid FireJames S. HarropCharles Kuntz, IV
Pediatric CraniocervicalSocietyRichard C.E. Anderson
Special Course II – Cases andComplications with theMastersEdward C. BenzelChristopher I. ShaffreyVincent C. Traynelis
Special Course III – SpinalDeformityCharles KuntzJuan S. Uribe
Special Course IV – AdvancedMIS Techniques/ManagingMIS ComplicationsPraveen V. MummaneniMichael Y. Wang
Special Course VII – Updateson Spine Trauma, Spinal CordInjury, and Cervical SpineTrauma GuidelinesMichael G. Fehlings
Special Course IX – AOSpine:Aging SpineJoseph S. Cheng Theodore J. ChomaChristopher I. ShaffreyAlexander R. Vaccaro
Luncheon Symposium II –Spine TumorsDaryl R. Fourney
Luncheon Symposium III –Cranial-Cervical JunctionRonald I. ApfelbaumTheodore H. Schwartz
Luncheon Symposium IV –Update of Lumbar SpineGuidelinesSanjay S. Dhall
Luncheon Symposium V –Lateral RetroperitonealInterbody Fusion: Techniqueand OutcomesJohn C. LiuJuan S. Uribe
Saturday Case PresentationsAruna Ganju
Oral Platform Presentations II 115: Domagoj Coric116: Domagoj Coric
Oral Poster Presentations I 226: Warren J. Alilain
Oral Poster Presentations II 248: Eric W. Nottmeier
Oral Poster Presentations III 218: Khoi Duc Than240: Antoine Tohmeh243: Daniel Robert Fassett
Oral Poster Presentations IV 245: Maxwell Boakye252: Reginald J. Davis
Digital Posters 317: Luis M. Tumialan328: Luis M. Tumialan334: W.B. Rodgers341: Ira M. Goldstein342: John K. Houten343: Eric W. Nottmeier348: John G. Stark351: Mitchell Hardenbrook364: Kenneth Pettine368: Kenneth Pettine370: Kenneth Pettine372: Mick J. Perez-Cruet387: Kaveh Khajavi391: John G. Stark395: Mick J. Perez-Cruet399: Robert F. Heary425: Robert M. Galler433: Randall W. Porter439: Kingsley O. Abode-Iyamah
DISCLOSURES
The AANS/CNS Section on Disorders of the Spineand Peripheral Nerves gratefully acknowledges
for providing an educational grant in support ofthe 2012 Annual Meeting.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 21
NEUROSURGICAL EDUCATION AMBASSADOR
The AANS/CNS Section on Disorders of the Spineand Peripheral Nerves gratefully acknowledges
for providing an educational grant in support ofthe 2012 Annual Meeting.
NEUROSURGICAL LEADERSHIP AMBASSADOR
WEDNESDAY MARCH 7, 2012
1:30 – 5:30 PMOceanic 1
Pediatric Craniocervical Society $200 includes lunchCourse Director: Douglas L. Brockmeyer Faculty: Richard C.E. Anderson, Daniel Edward Couture, Jonathan MartinCourse Description: This course will serveas a symposium for those with an interestin pediatric craniocervical abnormalitiesand disease. It seeks to examine issuesrelated to management of pediatriccraniocervical disease including surgicaland non-surgical treatment, complicationmanagement, and diseasepathophysiology.Learning Objectives: Upon completion ofthis course, participants should be able to:u Apply appropriate management of complex pediatric craniospinal disorders.
u Utilize appropriate research strategies to further the care of patients with craniospinal disorders.
u Apply the mechanism involved in the pathophysiology and progression of pediatric craniocervical disease.
1:30 – 3:30 PMRoundtable Discussion and Presentations
3:30 – 3:45 PMBreak
3:45 – 5:30 PMRoundtable Discussion and Presentations
1:30 – 5:30 PMNorthern Hemisphere A1Special Course I
Neurosurgical Spine: Business and Compensation (a joint Spine Section and CSNS Special Course)$200 includes lunchCourse Directors: Joseph S. Cheng, John J. KnightlyFaculty: Deborah L. Benzil, DomagojCoric, Matthew McGirt, Michael P. SteinmetzCourse Description: This course willprovide up-to-date information on currentissues in spine coding. Coding scenarioswill be reviewed for the correct coding ofroutine as well as complex spinalprocedures.
Learning Objectives: Upon completion ofthis course, participants should be able to:u Integrate the newest changes in CPTcoding for spine.
u Apply the methodology for correctspine coding.
u Identify specific difficult codingscenarios and bring clarity to thecoding process.
1:30 – 1:45 PMIntroduction Joseph S. Cheng, John J. Knightly
1:45 – 2:15 PM2012 CPT Coding Update Joseph S. Cheng
2:15 – 2:45 PMRevenue Generation: Ancillary Incomeand Operational Efficiency Domagoj Coric
2:45 – 3:15 PMOutcomes Data Collection in theChanging Healthcare Environment:Defining the Quality and Value of yourCare Through Practice Data CollectionMatthew McGirt
3:15 – 3:45 PMWhy Building Quality Into Your PracticeIs Important to Your Bottom LineJohn J. Knightly
3:45 – 4:15 PMMarketing Your Practice: Techniques toGenerate Referrals Deborah L. Benzil
4:15 – 4:45 PMPatient Satisfaction: What Really DrivesPatient PerceptionMichael P. Steinmetz
4:45 – 5:30 PMDiscussion
1:30 – 5:30 PMNorthern Hemisphere A2Special Course II
Cases and Complications withthe Masters$200 includes lunchCourse Directors: Edward C. Benzel, Regis W. Haid, Jr.Faculty: Charles Branch, Richard G. Fessler, Ziya L. Gokaslan,Robert F. Heary, Christopher I. Shaffrey,Vincent C. TraynelisCourse Description: This course will
discuss the evolution in diagnosis andtreatment of spinal disorders, as well asmanagement of complications oftreatment, from the perspective of thosewho have extensively contributed to thatevolution. Attendees will gain wisdomfrom historical knowledge andexperiential narration.Learning Objectives: Upon completion ofthis course, participants should be able to:u To understand and appreciate thegravity of decisions that lead tocomplications.
u To understand and appreciate theunderlying principles that might beused to minimize complications.
u To develop strategies that can be used to deal with surgical complications.
1:30 – 1:35 PMWelcomeEdward C. Benzel, Regis W. Haid, Jr.
1:35 – 1:45 PMCase Presentation: LumbarSpondylolisthesis – What Is Your Choiceof Fusion?Regis W. Haid, Jr.
1:45 – 2:05 PMLumbar Fusion: MIS is the Best WayRichard G. Fessler
2:05 – 2:30 PMLumbar Fusion: Open is the Best WayCharles Branch
2:30 – 2:40 PMWhat Was DoneRegis W. Haid, Jr.
2:40 – 2:50 PM Perspective on MIS for Lumbar FusionEdward C. Benzel
2:50 – 3:00 PMQuestions and Answers
3:00 – 3:25 PMLumbar Spondylolisthesis: Complicationsand Avoidance, Lessons LearnedRobert F. Heary
3:25 – 3:35 PMQuestions and Answers
3:35 – 3:40 PMLessons Learned in Approaching SpinalTumors: Managing Complications. WhoNeeds Surgery, Who Does Not…Ziya L. Gokaslan
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES22
MEETING AGENDA WEDNESDAY
3:40 – 3:50 PMQuestions and Answers
3:50 – 4:20 PMLessons Learned in Thoraco-lumbarDeformity: How to Avoid Too Much orToo LittleChristopher I. Shaffrey
4:20 – 4:30 PMQuestions and Answers
4:30 – 4:50 PM Cervical Kyphosis: Getting it RightVincent C. Traynelis
4:50 – 5:00 PMQuestions and Answers
5:00 – 5:30 PMCases PresentationsCourse Directors and Faculty
1:30 – 5:30 PMNorthern Hemisphere A3Special Course III
Spinal Deformity$200 includes lunchCourse Directors: Praveen V. Mummaneni,Christopher I. ShaffreyFaculty: James S. Harrop, Robert F. Heary,Tyler R. Koski, Charles Kuntz, IV, Frank LaMarca, Juan S. UribeCourse Description: This course willdiscuss adult spinal deformity with afocus on the evaluation, classification, andtreatment options available to this patientpopulation. Non-surgical managementoptions will be noted but emphasis will beplaced on surgical correction principlesand techniques. Complicationmanagement and operative outcomes willbe emphasized.Learning Objectives: Upon completion ofthis course, participants should be able to:u Review indications for non-operativeand operative management of adultspinal deformity surgery
u Review spinopelvic anatomy andbiomechanical parameters related tospinal deformity.
u Review the surgical techniques to re-establish sagittal balance and discusscomplication avoidance/management.
1:30 – 1:45 PMSpinal AlignmentCharles Kuntz, IV
1:45 – 2:00 PMCervical DeformityFrank La Marca
2:00 – 2:15 PMQuestions
2:15 – 2:30 PMTrauma and DeformityJames S. Harrop
2:30 – 2:45 PMPSO and SPOTyler R. Koski
2:45 – 3:00 PMQuestions
3:00 – 3:15 PMWhen Is Less Invasive SurgeryAcceptable for Spinal Deformity?Juan S. Uribe
3:15 – 3:30 PMWhen To Extend Fixation to Sacrum and PelvisRobert F. Heary
3:30 – 3:45 PMQuestions
3:45 – 5:30 PMCase PresentationsPraveen V. Mummaneni, Christopher I. Shaffrey
1:30 – 5:30 PMAmericas SeminarSpecial Course IV
Advanced MISTechniques/Managing MISComplications$200 includes lunchCourse Directors: Langston T. Holly,Michael Y. WangFaculty: Kevin Scott Cahill, Dean Chou,Richard G. Fessler, Kevin T. Foley, Praveen V. Mummaneni, Jonathan D. ShermanCourse Description: This course willdiscuss contemporary data and experiencethrough MIS case-based, interactive,didactic presentations. Faculty willdiscuss their evaluation and treatmentalgorithms regarding minimally invasivevs. open surgical options to maximizecomplication avoidance. Focus will begiven to cases initially treated minimallyinvasively with immediate or subsequentnecessity for open conversion. Topicsinclude advanced percutaneous fixationmethods, fusion options without usingBMP, MIS surgery and its effect onhealthcare costs and utilization, spinesurgery in high performance athletes: theimpact of MIS, minimally invasive
resection of metastatic spinal cord tumorsand the future of MIS surgery.Learning Objectives: Followingcompletion of this special course,participants should be able to: u Relate and implement the indicationsfor minimally invasive spinal surgery.
u Distinguish and apply the techniquesavailable for minimally invasivesurgery.
u Develop strategies for complicationavoidance.
1:30 – 1:45 PMIntroductionLangston T. Holly, Michael Y. Wang
1:45 – 2:15 PMAdvanced Percutaneous FixationMethodsJonathan D. Sherman
2:15 – 2:45 PMFusion Options Without Using BMPPraveen V. Mummaneni
2:45 – 3:15 PMMIS Surgery and Its Effect on HealthcareCosts and UtilizationKevin Scott Cahill
3:15 – 3:30 PMBreak
3:30 – 4:00 PMSpine Surgery in High PerformanceAthletes: The Impact of MISRichard G. Fessler
4:00 – 4:30 PMMinimally Invasive Resection ofMetastatic Spinal Column TumorsDean Chou
4:30 – 5:00 PMThe Future of MIS SurgeryKevin T. Foley
5:00 – 5:30 PMDiscussion
1:30 – 5:30 PMAsia 3
Special Course VManagement of PerioperativePain,PerioperativeComplicationsSpecial Course for Nurses, NursePractitioners and Physician Extenders$110 includes lunchCourse Directors:Michael P. Steinmetz,Andrea L. Strayer, MSN, CNRN, ACNPFaculty: Daniel J. Hoh, Jeffrey R. Holtz, PA,
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 23
WEDNESDAY MEETING AGENDA
AjitA.Krishnaney, JenniferLindstedt,APNP,Gregory R. Trost, Luis TumialanCourse Description:This course willprovide practical, current didacticinformation on perioperative painmanagement issues with particularemphasis on up-to-date practical bedsideand outpatient management strategies.Interactive case presentations will illustratetreatment and care considerations. Expertadvanced practice nurse, physicianassistant, and neurosurgeon faculty willexplore the challenges of caring for thiscomplex patient population.Learning Objectives: Upon completion ofthis course, participants should be able to:u Discuss general postoperative painissues following spinal surgery
u Analyze the indications forpostoperative diagnostic studies inpatients with extraordinary pain issuesfollowing spinal surgery.
u Review care considerations forpostoperative pain remote from thesurgical site (e.g. voiding difficulties,constipation, etc.)
1:30 – 2:00 PMPain Pathophysiology; Spine PainJeffrey R. Holtz, PA
2:00 – 2:20 PMMechanisms of Action for VariousAnalgesics Including Voiding Issues,Constipation PreventionDaniel J. Hoh
2:20 – 2:40 PMNSAIDS, Review, Contraindications,OptionsAjit A. Krishnaney
2:40 – 3:05 PMIV vs. Epidural PCALuis Tumialan
3:05 – 3:30 PMDo Minimal Access Surgical PatientsHave Less Pain?Michael P. Steinmetz
3:30 – 3:45 PMBreak
3:45 – 4:30 PMRed Flags What Studies, When - IncludingCasesGregory R. Trost
4:30 – 5:00 PMMultimodal Therapy Jennifer Lindstedt, APNP
5:00 – 5:30 PMPractice Gap Discussion
1:30 – 5:30 PMAsia 4
Special Course VIBrazil: Spine Surgery in Brazil –in conjunction with the SpineSection of BrazilianNeurosurgical Association$200 includes lunchCourse Directors: Ricardo Viera Botelho,Asdrubal FalavignaFaculty: Aluízio Augusto Arantes, Júnior,Eduardo Barreto, Ronald de Lucena Farias,Geraldo de Sá Carneiro Filho, Marcos Masini, Marcelo Luís Mudo, Luiz Pimenta, Fernando Luiz Rolemberg Dantas, José Marcus Rotta, Osmar José Santos de Moraes, Ericson Sfreddo, Marcelo Simone Simões,Márcio Vinhal de Carvalho Course Description: This course willinvolve a debate presentation format.Brazilian spine neurosurgeons experts willargue their perspectives with regard to themanagement scenarios for spine disorderscases through lectures, interactive casepresentations and discussion. This coursewill provide practical, current didacticinformation on spine disorders withparticular emphasis on surgicalapproaches, stabilization technics,complications avoidance andmanagement, surgical and non–surgicaldecision making and management as wellas discussion on future trends. Learning Objectives: Upon completion ofthis course, participants should be able to:u Analyze the evolution of spinal surgeryin Brazil.
u Recognize some technical nuances ofspinal surgery practiced in Brazil.
u Develop strategies for complicationavoidance and management.
u Describe the evaluation and appropriatemanagement of a number of spinalpathologies including trauma,degenerative disease and neoplasms.
u List the advantage and disadvantage ofspinal surgical techniques.
1:30 – 1:40 PMCurrent Status of Brazilian SpinalSurgery José Marcus Rotta
1:40 – 1:50 PMHow To Manage Basilar InvaginationAssociated with Chiari MalformationGeraldo de Sá Carneiro Filho
1:50 – 2:00 PMSpectrum of CraniocervicalMalformations: Diagnosis and TreatmentRicardo Vieira Botelho
2:00 – 2:10 PMDiscussion
2:10 – 2:20 PMC1-C2 Rheumatoid Arthritis DiseaseFernando Luiz Dantas
2:20 – 2:30 PMCervical Foraminotomy for NerveCompressionMarcos Masini
2:30 – 2:40 PMDiscussion
2:40 – 2:50 PMPosterior Approach for CervicalMyeloradiculopathyAluízio Augusto Arantes, Jr.
2:50 – 3:00 PM Cervical Facet Dislocations: Anterior orPosterior Approach?Ericson Sfreddo
3:00 – 3:15 PMDiscussion
3:15 – 3:35 PMBreak
3:35 – 3:45 PMXLIF for Degenerative ScoliosisLuiz Pimenta
3:45 – 3:55 PMNeuromodulation for Failed BackSurgeryEduardo Barreto
3:55 – 4:05 PMThe Role of the Interspinous DeviceMarcio Vinhal de Carvalho
4:05 – 4:20 PMDiscussion
4:20 – 4:30 PMTreatment and Outcome ofPostoperative Deep Wound InfectionFollowing Lumbar ArthrodesisAsdrubal Falavigna
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES24
MEETING AGENDA WEDNESDAY
4:30 – 4:40 PMEvidence in Lumbar Spine SurgeryOsmar José Santos de Moraes
4:40 – 4:50 PMThoracoscopic Surgery for Thoracic DiscHerniationsMarcelo Luís Mudo
4:50 – 5:00 PMDiscussion
5:00 – 5:10 PM Surgical Treatment for CoccygodinyaRonald de Lucena Farias
5:10 – 5:20 PMPost-traumatic Deformity SurgeryMarcelo Simone Simões
5:20 – 5:30 PMDiscussion
1:30 – 5:30 PMNorthern Hemisphere A4Special Course VII
Updates on Spine Trauma,Spinal Cord Injury, and CervicalSpine Trauma Guidelines$200 includes lunchCourse Directors: James S. Harrop,Michael FehlingsFaculty: Bizhan Aarabi, Steven Casha,Rajesh Reddy, Christopher I. ShaffreyCourse Description: This course willdiscuss updates on the treatment of spinetrauma and spinal cord injury includingcurrent clinical trials. Faculty will discussthe current literature and updates onguidelines, and decision-making andtreatment of pediatric and geriatric spinalcord injury. Learning Objectives: Upon completion ofthis course, participants will be able todiscuss the updated treatment of spinetrauma and spinal cord injury in thecervical and thoracolumbar spine, andamong the pediatric, adult, and geriatricpopulation. Participants will be able toassess the current literature and updatedguidelines for treatment of theseconditions.
1:30 – 1:40 PMIntroductionJames S. Harrop, Michael Fehlings
1:40 – 2:05 PM21-Year-Old Male C5 ASIA A: Timing ofTreatment Michael Fehlings
2:05 – 2:30 PMOccipital-C1 InstabilitySteven Casha
2:30 – 2:55 PM75-Year-Old with Central Cord Injury:When to Operate?Bizhan Aarabi
2:55 – 3:10 PM Break
3:10 – 3:35 PMPediatric SCI – Are They Just LittleAdults?Rajesh Reddy
3:35 – 4:00 PML1 Burst Fracture: Neurointact: Brace orFusionChristopher I. Shaffrey
4:00 – 4:25 PM76-Year-Old with Type II OdontoidFractureJames S. Harrop
4:25 – 5:30 PMCase Presentations – Open ForumAll faculty and audience
THURSDAYMARCH 8, 2012
6:30 – 6:55 AMSouthern Hemisphere Foyer
Continental BreakfastSouthern Hemisphere I-IIICase Presentations
Moderators: Erica Fay Bisson, Patrick C. Hsieh
6:55 – 7:00 AMIntroductory Remarks and MeetingAnnouncementsMarjorie C. Wang
7:00 – 9:30 AMSouthern Hemisphere I-IIIScientific Session I:
What’s On Your Report Card?$200 includes lunchModerators:Marjorie C. Wang, Daryl R. FourneyCourse Description: This session willexplore the definition of quality in spineand nerve surgery, and the ways in whichsurgeons are being measured. Thediscussion will also include currently usedquality measures and the evolution ofthese measures. Speakers will discuss howthese quality measures apply to practice,and some of the challenges in definingand achieving excellence.Learning Objectives:u Appraise quality measures andcommonly used quality metrics withinthe field of neurosurgery and inhealthcare overall.
u Relate the evolution of qualitymeasures and currently used qualitymeasures to practice.
u Recognize the challenges in definingand achieving excellence in spine andnerve surgery.
7:00 – 7:12 AMYou’re Being Measured, Whether YouKnow It or NotJohn J. Knightly
7:12 – 7:24 AMDefining Quality in Spine SurgerySohail Mirza
7:24 – 7:36 AMDefining and Achieving Excellence:Cervical MyelopathyMichael G. Fehlings
OPENING RECEPTIONCabana Deck at the Pool
6:00 – 8:00 PM
Enjoy a lavish array of food andrefreshments while reconnecting withcolleagues and meeting new contactsat the Opening Reception. Take inthe magic and wonder of thereception at the Walt Disney WorldSwan and Dolphin. Each medicalattendee and spouse/guest registeredfor the meeting will receive onecomplimentary ticket. Additionaltickets available for purchase at theevent. Resort casual attire isrecommended.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 25
THURSDAY MEETING AGENDA

7:36 – 7:48 AMDefining and Achieving Excellence:Peripheral NerveJohn E. McGillicuddy
7:48 – 7:54 AMQuestions
7:54 – 8:06 AMDefining and Achieving Excellence:Spinal TumorsZiya L. Gokaslan
8:06 – 8:18 AMDefining and Achieving Excellence:Spinal DeformityChristopher I. Shaffrey
8:18 – 8:35 AMDefining and Achieving Excellence: SpineTrauma – The Cervical Spine GuidelinesMark N. Hadley
8:35 – 8:45 AMAnnouncements
8:45 – 8:50 AMIntroduction of Section ChairmanDaniel K. Resnick
9:05 – 9:10 AMIntroduction of Meritorious ServiceAward Recipient Dennis J. MaimanJoseph S. Cheng
9:25 – 9:30 AMQuestions
10:15 AM – 12:30 PMSouthern Hemisphere I-III
Oral Platform Presentations IModerators: Praveen V. Mummaneni,Daniel K. ResnickDiscussants: Daryl R. Fourney, Zoher Ghogawala, Robert F. Heary, Iain H. Kalfas, Mark N. Hadley, Christopher I. Shaffrey, Gregory R. Trost,Eric L. Zager
10:15 – 10:24 AM106. The Short-Term Effect of Surgery onHealth Related Quality of Life andFunctional Outcome in Patients withMetastatic Epidural Spinal CordCompression (MESCC): Results of theongoing AOSpine North AmericaProspective Multicenter StudyMichael G. Fehlings, Branko Kopjar,Charles Fisher, Laurence D. Rhines, Paul M. Arnold, James M. Schuster,Alexander R. Vaccaro, Ziya L. Gokaslan,Joel Finkelstein, John France, Mark B. Dekutoski
10:24 – 10:27 AMDiscussant: Iain H. Kalfas
10:27 – 10:36 AM100. Characterization of FactorsPredictive of PerioperativeComplications in Adult PatientsUndergoing Complex Multilevel SpinalInstrumentation for Deformity: AConsecutive Series of 160 PatientsIsaac Karikari, Jordan Komisarow, Dylan Britt, Ankit Indravadan Mehta,Betsy H. Grunch, Deeptee Jain, Oren N. Gottfried, Carlos A. Bagley
10:36 – 10:39 AMDiscussant: Christopher I. Shaffrey
10:39 – 10:48 AM101. The Impact of Positive RegionalSagittal Alignment on Outcomes inPosterior Cervical Fusion SurgeryJessica A. Tang, Justin K. Scheer, Justin S. Smith, Vedat Deviren, Shay Bess,Robert Hart, Virginie Lafage, Christopher I. Shaffrey, Frank Schwab,Christopher P. Ames
10:48 – 10:51 AMDiscussant: Gregory R. Trost
10:51 – 11:00 AM102. Complications Following Use ofrhBMP-2 in Anterior Lumbar InterbodyFusion: An Institutional CohortControlled StudyDaniel Lubelski, Kalil G. Abdullah,Matthew D. Alvin, Michael P. Steinmetz,Edward C. Benzel, Thomas Mroz
11:00 – 11:03 AMDiscussant: Daryl R. Fourney
11:03 – 11:16 AMDiscussion
11:16 – 11:25 AM103. Characterization of Myelination bySkin Derived Precursor CellsJoey Kevin Grochmal, Rajiv Midha
11:25 – 11:28 AMDiscussant: Eric L. Zager
11:28 – 11:37 AM104. The Design and Development of the Neuropoint SD Spine Registry forLumbar Discectomy and Single LevelFusion for SpondylolisthesisZoher Ghogawala, Christopher I. Shaffrey,Anthony L. Asher, Neil R. Malhotra, Steven Dante, R. John Hurlbert, Andrea F. Douglas, Subu N. Magge,Praveen V. Mummaneni, Joseph S. Cheng,Justin S. Smith, Michael G. Kaiser, Robert F. Heary, Khalid M. Abbed, Daniel M. Sciubba, Daniel K. Resnick
11:37 – 11:40 AMDiscussant: Daniel K. Resnick
11:40 – 11:49 AM105. Is Surgical Decompression inPatients with Mild Cervical SpondyloticMyelopathy Effective? Results of theProspective, Controlled, MulticenterAOSpine North America CSM StudyMichael G. Fehlings, Branko Kopjar,Sangwook Yoon, Paul M. Arnold, Eric M. Massicotte, Alexander R. Vaccaro,Darrel S. Brodke, Christopher I. Shaffrey,Justin S. Smith, Eric J. Woodard, Robert J. Banco, Jens Chapman, Michael Janssen, Christopher Bono, Rick Sasso, Mark B. Dekutoski, Ziya L. Gokaslan
11:49 – 11:52 AMDiscussant: Robert F. Heary
8:50 – 9:05 AMPresidential Address:My BiasesChristopher E. Wolfla
9:10 – 9:25 AMMeritorious ServiceAward Presentation: TheRoleofBiomechanicsin SurgicalDecisionMakingDennis J. Maiman
9:30 – 10:15 AMNorthern Hemisphere B-E
Beverage Break with Exhibitors
What’s New Session IModerators: Srinivas K. Prasad, Daniel M. Sciubba
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES26
MEETING AGENDA THURSDAY

11:52 AM – 12:01 PM107. Anterior vs. Posterior SurgicalApproaches to Treat Cervical SpondyloticMyelopathy: Outcomes of theProspective Multicenter AOSpine NorthAmerica CSM Study in 278 PatientsMichael G. Fehlings, Branko Kopjar,Sangwook Yoon, Paul M. Arnold, Eric M. Massicotte, Alexander R. Vaccaro,Darrel S. Brodke, Christopher I. Shaffrey,Eric J. Woodard, Robert J. Banco, Jens Chapman, Michael Janssen, Rick Sasso, Christopher Bono, Mark B. Dekutoski, Ziya L. Gokaslan
12:01 – 12:04 PMDiscussant: Zoher Ghogawala
12:04 – 12:13 PM108. The Scope and Impact of Wrong-Level Lumbar Spine Surgery: A Survey ofthe Joint Section on Disorders of theSpine and Peripheral NervesMichael W. Groff, Joshua E. Heller, Eric A. Potts, Praveen V. Mummaneni,Christopher I. Shaffrey, Justin S. Smith
12:13 – 12:16 PMDiscussant:Mark N. Hadley
12:16 – 12:30 PMDiscussion
1:25 – 1:30 PM Southern Hemisphere I-IIIMeeting AnnouncementsMarjorie C. Wang
1:30 – 3:00 PMSouthern Hemisphere I-IIIScientific Session II
David Cahill MemorialControversies I: InDepthDebatesModerators: R. John Hurlbert, Daniel M. SciubbaCourse Description: This Scientific Sessionwill involve in-depth debates oncontroversial clinical topics. Experts willargue their perspectives with regard to themanagement scenarios for difficult spineand peripheral nerve cases.Learning Objectives:On completion of this course, participantsshould be able to:
u Analyze the role of surgery intreatment of black disc disease.
u Discuss the risks and benefits ofperforming a single level anteriorcervical discectomy and fusion at asurgery center versus a hospital.
u Distinguish the risks and benefits ofcervical spine clearance in the obtundedpatient using MRI versus CT imaging.
1:30 – 1:57 PMBlack Disc Disease: Is There a Role for Surgery?Dennis J. Maiman vs. Charles Branch
1:57 – 2:24 PMSingle Level ACDF: My Surgery Center vs.Your HospitalDomagoj Coric vs. Joseph S. Cheng
2:24 – 2:51 PMCervical Spine Clearance in theObtunded Patient: MRI vs. CTDavid O. Okonkwo vs. Vincent C. Traynelis
2:51 – 3:00 PMQuestions and Discussion
3:45 – 5:15 PMSouthern Hemisphere I-III
Oral Poster Presentations I(Concurrent Session)Moderators: Dean Chou, Jean-Valery Coumans
3:45 – 3:50 PM219. Impact of Treatment Complicationson Outcomes in Geriatric Patients withType II Odontoid Fracture: Results fromthe AOSpine North America Multi-CenterGOF Prospective StudyMichael G. Fehlings, Alexander R. Vaccaro,Branko Kopjar, Christopher I. Shaffrey,Jens Chapman, Paul M. Arnold, Ziya L. Gokaslan, Darrel S. Brodke, John France, Sangwook Yoon, Mark B. Dekutoski, Christopher Bono,Rick Sasso
3:50 – 3:55 PM206. The Fate of Type II OdontoidFractures After Posterior AtlantoaxialFusion: Where Does Healing Occur?Michael Mumert, Marcus D. Mazur,Andrew T. Dailey, Meic H. Schmidt, Erica Fay Bisson
3:55 – 4:00 PM205. Functional Outcome Instrumentsused for Cervical SpondyloticMyelopathy: Interscale Correlation andPrediction of Preference-based Qualityof LifeDmitriy Petrov, Robert G. Whitmore, Zoher Ghogawala, J. Sanford Schwartz,Sherman C. Stein
4:00 – 4:05 PM217. What Are the Factors That MayPredict Regain of Independent WalkingAfter Surgery for Patients with AdvancedCervical Spondylotic Myelopathy?Ahmed Mustafa Alaqeel, Amro Al Habib,Abdulrahman Aldakkan, Fahad Albadr
4:05 – 4:10 PM235. Standardized Reporting ofPerioperative Complications FollowingCervical CorpectomyMaxwell Boakye, Robert Thomas Arrigo,Ivan Cheng, Stefan A. Mindea, Eugene Carragee, John Park, Todd Alamin
4:10 – 4:15 PMDiscussion
4:15 – 4:20 PM208. Laminoplasty vs. Laminectomy:Prospective Study in JapanTatsushi Inoue, Shigehiko Kuno, MotoiShoda, Yuichi Hirose
4:20 – 4:25 PM250. Kyphotic Deformities of the CervicalSpineJan Stulik, Petr Nesnidal, Jan Kryl, TomasVyskocil, Michal Barna
4:25 – 4:30 PM254. Diffusion Tensor Imaging:Evaluating the Spinal Cord in AnimalModels and HumansShekar N. Kurpad, Brian Schmit, Aditya Vedantam, Marjorie C. Wang,Benjamin M. Ellingson
12:30 – 1:25 PMNorthern Hemisphere B-ELunch with Exhibitors
What’s New Session IIModerators: John Chi, D. Kojo Hamilton
3:00 – 3:45 PMNorthern Hemisphere B-E
Beverage Break with Exhibitors
What’s New Session IIIModerators:DanielHoh,Stefan A.Mindea
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 27
THURSDAY MEETING AGENDA

4:30 – 4:35 PM214. A Novel Animal Model of CervicalSpondylotic Myelopathy: An Opportunityto Identify New Therapeutic TargetsSpyridon Karadimas, Eun Su Moon,Kajana Satkunendrarajah, Michael G. Fehlings
4:35 – 4:40 PM226. Chondroitinase ABC Treatment andModest Exposure to IntermittentHypoxia Restores HemidiaphragmaticActivity After Cervical Spinal Cord InjuryWarren J. Alilain, Jerry Silver, Megan Clark
4:40 – 4:45 PMDiscussion
4:45 – 4:50 PM256. Diffusion Tensor MRI andMotoneuron Morphometric Changes inCervical Gray Matter After a ThoracicSpinal Cord Injury in the RatShekar N. Kurpad, Brian Schmit, Benjamin M. Ellingson, Robin Mottackel
4:50 – 4:55 PM238. Cervical Spine Clearance in theTraumatically Injured Patient: Is CT ScanSufficent AloneBrandon G. Chew, Matthew R. Quigley,Christopher Swartz
4:55 – 5:00 PM239. The Use of Allograft andRecombinant Human BoneMorphogenetic Protein for InstrumentedAtlanto-axial FusionsBrian James Hood, D. Kojo Hamilton,Justin S. Smith, Marine Dididze,Christopher I. Shaffrey, Allan D. Levi
5:00 – 5:05 PM227. Incidental Durotomy after SpinalSurgery: A Prospective Study in anAcademic InstitutionPaul J. McMahon, Marine Dididze,Allan D. Levi
5:05 – 5:10 PM229. Spinal Ependymomas: AnInstitutional Experience Over 25 Years in 134 PatientsPhiroz E. Tarapore, Peter Modera, Agne Noujokas, Christopher P. Ames,Dean Chou, Praveen V. Mummaneni,Philip R. Weinstein, Tarik Tihan
5:10 – 5:15 PMDiscussion
3:45 – 5:15 PMAmericas Seminar
Oral Poster Presentations II (Concurrent Session)Moderators: John Chi, Justin S. Smith
3:45 – 3:50 PM215. Current Practices for IntraoperativeLocalization of Lumbar Spinal Level: ASurvey of the Joint Section on Disordersof the Spine and Peripheral NervesMichael W. Groff, Joshua E. Heller, Eric A. Potts, Praveen V. Mummaneni,Christopher I. Shaffrey, Justin S. Smith
3:50 – 3:55 PM220. Should Routine ScreeningUltrasonography for Deep VeinThrombosis Be Used in AsymptomaticPatients During Hospitalization forElective Spine Surgery? An Analysis andReview of 587 Consecutive PatientsD. Kojo Hamilton, Akil Patel, Charles A. Sansur
3:55 – 4:00 PM258. Repeat Surgery Following LumbarDecompression for Herniated Disc: TheQuality Implications of Hospital andSurgeon VariationBrook I. Martin
4:00 – 4:05 PM242. Analysis of Readmission Rates AfterSpinal Surgery: Do Underfunded PatientsHave Higher Readmission Rates AfterSpinal Surgery?Daniel Robert Fassett, YazhiniGnanasambanthan, Linda Gonia, Huaping Wang, David M. Neils
4:05 – 4:10 PM216. Rates and Causes of MortalityAssociated with Spine Surgery Based on 108,419 Procedures: A Review of theScoliosis Research Society Morbidity and Mortality DatabaseJustin S. Smith, Dwight Saulle, Christopher P. Ames, Lawrence Lenke,Steven D. Glassman, Paul A. Broadstone,David W. Polly, Jr., Christopher I. Shaffrey
4:10 – 4:15 PMDiscussion
4:15 – 4:20 PM201. Radiographic and Clinical Outcomesof Posterior Column Osteotomies inSpinal Deformity Correction: Analysis of128 PatientsIan G. Dorward, Lawrence Lenke, Geoffrey E. Stoker, Woojin Cho, Linda A. Koester, Brenda A. Sides
4:20 – 4:25 PM203. WITHDRAWN
4:25 – 4:30 PM248. The Effect of RhBMP-2 Dosing onthe Complication and Fusion Rate inPosterior Interbody Fusion UsingPolyetheretherketone (PEEK) Cages.Eric W. Nottmeier, Douglas S. Fenton,Cammi Bowman, Zane Thompson,Matthew Hale
4:30 – 4:35 PM207. Complications with the Use of BMP-2 in Thoracolumbar and Lumbar SpineFusions: A Nine-Year InstitutionalAnalysisDaniel Lubelski, Kalil G. Abdullah,Michael P. Steinmetz, Matthew D. Alvin,Amy S. Nowacki, Srita Chakka, Edward C. Benzel, Thomas Mroz
4:35 – 4:40 PM231. Health-Related Quality of LifeOutcomes with Minimally InvasiveTransforaminal Lumbar Interbody FusionBased on Long-Term Analysis of 318Consecutive PatientsMick J. Perez-Cruet, Namath Syed Hussain, Evan Begun,Joseph John Joshua
4:40 – 4:45 PMDiscussion
4:45 – 4:50 PM210. Fractures of the Ankylosed Spine: A Single Institution ExperienceBrian D. Milligan, Terry K. Schiefer,Colten D. Bracken, Jeffrey T. Jacob,William E. Krauss, Mark A. Pichelmann,Michelle J. Clarke
4:50 – 4:55 PM233. Retrospective, Propensity Score-Matched Cohort Study Examining Timingof Fracture Fixation for TraumaticThoracolumbar FracturesMaxwell Boakye, Robert Thomas Arrigo,Melanie Hayden, Corinna Zygourakis,Shivanand P. Lad
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES28
MEETING AGENDA THURSDAY
4:55 – 5:00 PM225. Spinal Epidural Abscess: ClinicalFeatures and Surgical OutcomesAnubhav Gautam Amin, George Austin Crabill, Gustavo Pradilla,Amit Jain, Michael Lim, Daniele Rigamonti, Wesley Hsu
5:00 – 5:05 PM211. Cost per Quality-adjusted Life YearGained of Revision Lumbar Surgery forAdjacent Segment Disease,Pseudoarthrosis, and Same-levelRecurrent Stenosis: Defining the Value of Surgical InterventionScott L. Parker, David Shau, Stephen Mendenhall, Owoicho Adogwa,Joseph S. Cheng, Clinton J. Devin,Matthew McGirt
5:05 – 5:10 PM202. Factors Influencing Two-yearHealthcare Costs in Patients UndergoingRevision Lumbar Fusion Procedures: AGuide to Where We Should Target OurCost and Quality Improvement InitiativesScott L. Parker, David Shau, Stephen Mendenhall, Matthew McGirt
5:10 – 5:15 PMDiscussion
FRIDAYMARCH 9, 2012
6:30 – 6:55 AMSouthern Hemisphere Foyer
Continental BreakfastSouthern Hemisphere I-IIICase Presentations
Moderators: Eve C. Tsai, Daniel C. Lu
6:55 – 7:00 AMMeeting AnnouncementsMarjorie C. Wang
7:00 – 9:00 AMSouthern Hemisphere I-IIIScientific Session III
Complication Avoidance andManagementModerators: Eric J. Woodard, Michael Y. WangCourse Description: This course willaddress complications encountered inspine and nerve surgery using a case-based format. Management techniquesand complication avoidance strategies willbe discussed. Cases will specificallyaddress ectopic ossification after bonemorphogenetic protein use, junctionalkyphosis, failure of instrumentation in theosteoporotic spine, complicationsassociated with the lateral approach to thespine, esophageal injury, revision ulnarnerve decompression, and “wrong-level”spine surgery.Learning Objectives: Upon completion ofthis course, participants should be able to:u Identify risk factors associated withcomplications of spine and nervesurgery.
u Strategize preoperative techniques andplanning to help avoid complications.
u Incorporate intraoperative andpostoperative management andstrategies to help avoid complicationsand mitigate their effects.
7:00 – 7:03 AMEctopic Ossification After rhBMP Use –Case PresentationD. Kojo Hamilton
7:03 – 7:15 AMComplication Avoidance andManagement: Ectopic Ossification AfterrhBMP UsePraveen V. Mummaneni
7:15 – 7:18 AMJunctional Kyphosis – Case PresentationJustin S. Smith
7:18 – 7:30 AMComplication Avoidance andManagement: Junctional KyphosisTyler Koski
7:30 – 7:33 AMFailure of Instrumentation in theOsteoporotic Spine – Case PresentationDaniel Refai
7:33 – 7:45 AMComplicationAvoidance andManagement: Failure of Instrumentationin the Osteoporotic SpineGregory R. Trost
7:45 – 7:48 AMLateral Approach (XLIF/DLIF) – CasePresentationKhalid M. Abbed
7:48 – 8:00 AMComplication Avoidance andManagement: Lateral Approach(XLIX/DLIF)Adam S. Kanter
8:00 – 8:05 AMDiscussion
8:05 – 8:08 AMEsophageal Injury After ACDF – CasePresentationSrinivas K. Prasad
8:08 – 8:20 AMComplication Avoidance andManagement: Esophageal Injury After ACDFDaryl R. Fourney
8:20 – 8:23 AMRevision Ulnar Nerve Decompression –Case PresentationAmgad Hanna
8:23 – 8:35 AMComplication Avoidance andManagement: Revision Ulnar NerveDecompressionEric L. Zager
8:35 – 8:38 AM“Wrong Level” Spine Surgery – CasePresentationEve C. Tsai
RECEPTION WITHEXHIBITORS
5:15 – 6:45 PM Northern Hemisphere B-E
Join us for this special event in theexhibit hall! Interact with colleaguesand corporate contacts while enjoying pre-dinner cocktails and hors d’oeuvres.Business casual attire is recommended.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 29
FRIDAY MEETING AGENDA

8:38 – 8:50 AMComplication Avoidance andManagement: “Wrong Level” SpineSurgeryMichael W. Groff
8:50 – 9:00 AMQuestions and Discussion
9:00 – 9:20 AMSouthern Hemisphere I-III
Mayfield Award PresentationsModerators: Adam S. Kanter, Daniel M. Sciubba
MAYFIELD BASIC SCIENCEAWARD9:00 – 9:05 AM118. Human Mesenchymal Stem CellsSeeded in a Polymer Scaffold: A NovelTreatment Approach for Spinal CordInjuryAlexander E. Ropper, Devang Thakor, Inbo Han, Dou Yu, Hariprakash Haragopal,A. John Popp, Yang D. Teng
9:05 – 9:07 AMDiscussant: R. John Hurlbert
MAYFIELD CLINICAL SCIENCEAWARD9:07 – 9:12 AM119. Decreased Incidence of VenousThrombo-embolism After Spine Surgerywith Early Aggressive ChemoprophylaxisJoseph Bridger Cox, Catherine Koepnick,R. Patrick Jacob, Daniel J. Hoh
9:12 – 9:14 AMDiscussant:Michael W. Groff
OUTCOMES COMMITTEE AWARD9:14 – 9:19 AM120. The Relevance of IntramedullaryHigh Signal Intensity and Gadolinium(Gd-DTPA) Enhancement to the ClinicalOutcome in Cervical CompressiveMyelopathyJun-Jae Shin, Ji Hae Lee, Woo Ho Cho,Jon Park
9:19 – 9:20 AMDiscussant: Langston T. Holly
9:20 – 9:25 AMNREFRegis W. Haid, Jr.
9:25 – 9:30 AMDiscussion
10:15 AM – 12:15 PMSouthern Hemisphere I-III
Oral Platform Presentations IIModerators: Langston T. Holly, Frank La MarcaDiscussants: Joseph T. Alexander, Peter D. Angevine, Allan J. Belzberg, Erica F. Bisson, Joseph S. Cheng, Shekar Kurpad, Michael K. Rosner,Michael P. Steinmetz, Peter Witt
10:15 – 10:24 AM109. Radiographic Predictors of EarlyFailure Following DecompressionWithout Fusion for Degenerative Grade ILumbar SpondylolisthesisClaire Blumenthal, Jill Curran, Edward C. Benzel, Subu N. Magge, J. Frederick Harrington, Jean-Valery Coumans, Zoher Ghogawala
10:24 – 10:27 AMDiscussant:Michael K. Rosner
10:27 – 10:36 AM110. Functional and Quality of LifeOutcomes in Geriatric Patients with TypeII Odontoid Fracture: One Year Resultsfrom the AOSpine North America Multi-Center GOF Prospective StudyMichael G. Fehlings, Alexander R. Vaccaro, Branko Kopjar, Jens Chapman, Christopher I. Shaffrey,Ziya L. Gokaslan, Paul M. Arnold, Darrel S. Brodke, John France,Sangwook Yoon, Mark B. Dekutoski, Rick Sasso, Christopher Bono
10:36 – 10:39 AMDiscussant: Joseph T. Alexander
10:39 – 10:48 AM111. Posterior Cervical Foraminotomy forCervical Radiculopathy: Symptomatic,Functional and Quality of Life Outcomesin 1085 Cases with Long-term Follow-upEphraim W. Church, Casey H. Halpern,Ryan Faught, Usha Balmuri, Mark Attiah,Sharon Hayden, Marie Kerr, Eileen Maloney-Wilensky, Janice Bynum,Sherman C. Stein, Stephen J. Dante,William Charles Welch, Frederick A. Simeone
10:48 – 10:51 AMDiscussant: Peter D. Angevine
10:51 – 11:00 AM112. The Relative Impact of LumbarSpondylosis on Quality of Life in theUnited States: A Population HealthPerspectiveCyrus Chi-Ho Wong, Scott L. Parker,Marcus J. Gates, Matthew McGirt
11:00 – 11:03 AMDiscussant: Erica F. Bisson
11:03 – 11:09 AMDiscussion
11:09 – 11:18 AM113. Pitfalls of Calculating HospitalReadmission Rates Based Solely onNonvalidated Administrative DatasetsBeejal Y. Amin, Urvij Modhia, Keishi Mauro, Lumine Na, Steven Takemoto, Christopher P. Ames,Vedat Devirin, Dean Chou, Sigurd Berven, Praveen V. Mummaneni
11:18 – 11:21 AMDiscussant: Joseph S. Cheng
11:21 – 11:30 AM114. Modest Systemic Hypothermia inAcute Cervical Spinal Cord Injury: AProspective Case Controlled StudyAllan D. Levi, Barth A. Green, Dalton Dietrich, Steven Vanni, Marine Dididze, Michael Y. Wang
11:30 – 11:33 AMDiscussant: Shekar Kurpad
11:33 – 11:42 AM115. Prospective, Randomized Study ofCervical Arthroplasty and ACDF withLong-Term Follow-up: 76 Patients from a Single Site with Four- to Eight-yearFollow-upDomagoj Coric, Margaret Boltes, Sara James, Judd Heideman
11:42 – 11:45 AMDiscussant: Peter Witt
11:45 – 11:54 AM 116. Prospective Study of Disc Repairwith NuQu Injectable AllogeneicChondrocytesDomagoj Coric, Kenneth Pettine,Margaret Boltes
11:54 – 11:57 AMDiscussant:Michael P. Steinmetz
9:30 – 10:15 AMNorthern Hemisphere B-E
Beverage Break with Exhibitors
What’s New Session IVModerators: Khalid Abbed, Daniel J. Hoh
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES30
MEETING AGENDA FRIDAY
11:57 AM – 12:06 PM117. Skin-derived Precursor CellsEnhance Functional Outcome FollowingNerve RepairHelene T. Khuong, Aleksandra Ivanovic,Antos Shakhbazau, Ranjan Kumar, Joanne Forden, Hamed Abhari, Rajiv Midha
12:06 – 12:09 PMDiscussant: Allan J. Belzberg
12:09 – 12:10 PMDiscussion
12:10 – 12:15 PMN2QODZoher Ghogawala
12:30 – 2:30 PMNorthern Hemisphere A4
Luncheon Symposium IRevision Spine Surgery$200 includes lunchCourse Directors: Iain H. Kalfas, Michael W. GroffFaculty: David O. Okonkwo, Timothy C. RykenCourse Description: This course willprovide state-of-the-art information oncomplication avoidance during revisionspine surgery. Faculty will review theirclinical experience and lessons learned viainteractive case discussions. Learning Objectives: Upon completion ofthis course, participants should be able to:u Explain the management issues uniqueto revision surgery.
u Appraise the common reasons forspinal instrumentation failure.
u Evaluate the management of recurrentspinal conditions such as restenosis andreherniation and apply to practice.
u Integrate strategies for the managementof postoperative deformity and adjacentsegment failure.
12:30 – 12:50 PMRecurrent Lumbar Disc Herniation
David O. Okonkwo12:50 – 1:00 PMQuestions
1:00 – 1:20 PMPost-laminectomy Cervical KyphosisIain H. Kalfas
1:20 – 1:30 PMQuestions
1:30 – 1:50 PMLumbar Adjacent Level Degeneration:Stenosis and InstabilityMichael W. Groff
1:50 – 2:00 PMQuestions
2:00 – 2:20 PMSpinal Instrumentation FailureTimothy C. Ryken
2:20 – 2:30 PMQuestions
12:30 – 2:30 PMNorthern Hemisphere A3
Luncheon Symposium IISpine Tumors$200 includes lunchCourse Directors: Daryl R. Fourney,Laurence D. RhinesFaculty: Dean Chou, Ziya L. Gokaslan, Ilya Laufer, Daniel M. Sciubba, Frank D. VrionisCourse Description:This course will reviewthe natural history andmanagement ofprimary andmetastatic spinal tumors.Radiographic imaging, interventionstrategies and treatment algorithms will bereviewed. Surgical treatment includingapproaches will be discussed. Extensiveinteractive case presentations will illustratetreatment and care considerations andexplore the challenges of caring for thiscomplex patient population.Learning Objectives: Upon completion ofthis course, participants should be able to:u Understand the significance of tumorbiology in considering managementoptions.
u Discuss the indications and techniquesfor management of primary andmetastatic spinal tumors.
u Discuss surgical approaches andtechniques for tumor resection andspinal reconstruction.
12:30 – 12:35 PMWelcome and Introductions
Daryl R. Fourney, Laurence D. Rhines12:35 – 12:55 PMUnknown Primary with Neuro Deficit Ilya Laufer
12:55 – 1:05 PMMechanical Instability from Tumors: Can We Define It?Daryl R. Fourney
1:05 – 1:25 PMSurgical Options: When To Go Anterior,Posterior or Combined Ziya L. Gokaslan
1:25 – 1:40 PMMinimally Invasive Options: Is There a Role? Dean Chou
1:40 – 1:55 PMWhen to ConsiderKyphoplasty/Radiosurgery Frank D. Vrionis
1:55 – 2:10 PMNew Frontiers in Metastatic SpineTumors Daniel M. Sciubba
2:10 – 2:30 PMPrimary Tumors: En Bloc SurgeryFeasibility, Justification?Laurence D. Rhines
12:30 – 2:30 PMNorthern Hemisphere A2
Luncheon Symposium IIICranial-Cervical Junction$200 includes lunchCourse Directors:Michael P. Steinmetz,Jean-Paul WolinskyFaculty: Christopher P. Ames, Ronald I. Apfelbaum, Theodore H. Schwartz, Ziya L. GokaslanCourse Description: This course willdiscuss contemporary data and experiencein treating pathology of the cranial-cervical junction. This course will be in acase-based interactive format withdidactic presentations. Faculty willdiscuss their evaluation and treatmentalgorithms surrounding pathology of theCCJ. The focus will be on understandingthe pathophysiology of various conditionsand how treatment strategies have evolvedwith better understanding of this region.Learning Objectives: Followingcompletion of this course, participantsshould be able to:u Relate how certain pathologic processes
ANNUAL BUSINESS MEETING
12:15 – 12:30 PMSouthern Hemisphere I-III
12:30 – 1:25 PMNorthern Hemisphere B-E
Lunch in the Exhibit Hall
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 31
FRIDAY MEETING AGENDA
affect the cranial-cervical junction.u Distinguish why certain treatmentstrategies are implemented andunderstand the basic surgicaltechniques for specific pathologicprocesses.
u Develop and design complexreconstructions of the cranial-cervicaljunction.
Interactive Panel Discussion
Case Presentations and ModeratorMichael P. Steinmetz
Instrumentation and IntraoperativeReduction TechniquesChristopher P. Ames
Trans-Oral ApproachRonald I. Apfelbaum
Transmandibular Circumglossal ApproachZiya L. Gokaslan
Endoscopic Endo-nasal ApproachTheodore H. Schwartz
Endoscopic Trans-cervical ApproachJean-Paul Wolinsky
12:30 – 2:30 PMNorthern Hemisphere A1
Luncheon Symposium IVUpdate of Lumbar SpineGuidelines$200 includes lunchCourse Directors:Michael G. Kaiser,Daniel K. ResnickFaculty: Sanjay S. Dhall,Zoher Ghogawala, Timothy C. RykenCourse Description: This course willdiscuss the current literature and updateson guidelines for the surgical treatment oflumbar spine degenerative conditions. Learning Objectives: On completion of thiscourse, participants will be able to discussthe updated guidelines, indications, andexpected outcomes for surgical treatmentof lumbar spine degenerative conditions.
12:30 – 12:45 PMIntroduction to Lumbar FusionGuidelines, Justification, Methodology,and Use Timothy Ryken
12:45 – 1:15 PMRadiographic, Functional and EconomicOutcomes in Lumbar Fusion: How ToAssess and What Is Expected?Zoher Ghogawala
1:15 – 1:30 PMCorrelating Radiographic to ClinicalOutcome Sanjay Dhall
1:30 – 2:00 PMFusion for Axial Pain, Deformity, andStenosis: What Is it Justified:Daniel K. Resnick
2:00 – 2:30 PMAdjuncts for Fusion: What Works, When,and for Whom?Michael G. Kaiser
12:30 – 2:30 PMAmericas Seminar
Luncheon Symposium VLateral RetroperitonealInterbody Fusion: Techniqueand Outcomes$200 includes lunchCourse Directors: Regis W. Haid, Jr.,Praveen V. MummaneniFaculty: Juan S. Uribe, Allan D. Levi, John C. Liu, Adam S. KanterCourse Description: This course will focuson the indications, outcomes andcomplications of the lateral retroperitonealtranspsoas fusion technique. Specificlectures will concentrate on anatomy andapproach, literature based outcomes,complication avoidance and management,and clinical pearls. Biomechanics ofstand-alone versus supplementedtechniques will be discussed. Interactionand discussion among participants will beencouraged.Learning Objectives: Upon completion ofthis course, participants should be able to:u Review and discuss indications forlateral thoracolumbar interbodyapproaches and surgery.
u Discuss the complications and theiravoidance in these procedures.
u Review the clinical and radiographicresults in lateral thoracolumbarinterbody fusion procedures.
12:30 – 12:50 PMAnatomic Overview and ApproachAllen D. Levi
12:50 – 1:10 PMComplications: Incidence and AvoidanceJohn C. Liu
1:10 – 1:30 PMStand Alone or Anterior – Posterior: How I ChooseAdam S. Kanter
1:30 – 1:50 PMDeformity Correction with Stand AloneJuan S. Uribe
1:50 – 2:10 PMDeformity Correction with Anterior –PosteriorPraveen V. Mummaneni
2:10 – 2:30 PMDiscussion
1:30 – 5:30 PMAsia 3
Special Course VIIIPeripheral Nerve Exposures andNerve Repair Techniques(Complimentary to Residents)$200 includes lunchCourse Directors: Robert J. Spinner, Linda Jun-San YangFaculty: Allan J. Belzberg, Marie-Noelle Hebert-Blouin, Line Jacques,Michel Kliot, Rajiv Midha, Nader Pouratian, Eric L. ZagerCourse Description: This course willdemonstrate the common exposures toperipheral nerves in the upper extremityand common techniques used forperipheral nerve reconstruction. It istargeted to practicing surgeons, seniorresidents and fellows. Learning Objectives: Upon completion ofthis course, participants should be able to:u Synthesize the pertinent and practicalsurgical anatomy of the brachial plexusand peripheral nerves in the upper limbas related to common nerve injuries,nerve entrapments, and other nervedisorders.
u Distinguish common techniquesutilized in the reconstruction ofperipheral nerves (direct repair,grafting, nerve transfers, and nerveconduits).
This course will prepare residents for written boardexaminations and young neurosurgeons for oralboard examinations.
This course will be presented in an interactive,round-robin format to facilitate small group teachingof peripheral nerve anatomy and exposures as wellas nerve repair techniques.
Nerve Repair Techniques (Direct Repair,Grafting, Nerve Transfers, Conduits)Rajiv Midha
Median and Ulnar NervesRobert J. Spinner
Radial and Musculocutaneous NervesLine Jacques
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES32
MEETING AGENDA FRIDAY
Suprascapular and Axillary NervesMarie-Noelle Hebert-Blouin
Exposures to Nerves in Hip and Thigh(e.g., Sciatic, Femoral, Lateral FemoralCutaneous)Nader Pouratian
Exposures to Nerves in Leg (Knee andBelow – e.g., Tibial Nerve, PeronealNerve)Michel Kliot
Brachial Plexus (Supra andInfraclavicular) Allan J. Belzberg, Linda Jun-San Yang
Common Nerve TransfersEric L. Zager
1:30 – 5:30 PMAsia 4
Special Course IXAOSpine: Aging Spine$200 includes lunchCourse Directors: Darrel S. Brodke, Roger HartlFaculty: Eugene Carragee, Jens R. Chapman, Joseph S. Cheng,Theodore J. Choma, Michael G. Fehlings,Christopher I. Shaffrey, Alexander R. Vaccaro, Luis M. VialleCourse Description: This course willdiscuss contemporary data and experiencein treatment of the aging spine. Facultywill discuss decision-making andtreatment options for odontoid fractures,cervical myelopathy, degenerativescoliosis, osteoporosis, minimally invasiveapproaches in the aging spine, and surgerytrends and healthcare costs in the elderly. Learning Objectives: Upon completion ofthis course, participants should be able to:u The participant should understand thedifferent types of odontoid fracturesand the treatment options withpredicted fusion rates based on recentclinical trials.
u The participant should understand therationale for surgical treatment ofcervical spinal stenosis and myelopathywith pros and cons of anterior vs.posterior and combined approaches.
u The participant should understand thespecial risks of surgical treatment ofspinal disorders in the elderlypopulation and their avoidance andmanagement.
u The participant should understand thetreatment options for degenerativelumbar scoliosis in elderly patients
with pros and cons.u The participant should understandcurrent trends in the surgical treatmentof spinal disorders in the elderlypopulation and be able to discussunderlying reasons and implications.
1:30 – 1:35 PMIntroductionDarrel S. Brodke, Roger Hartl
1:35 – 1:45 PMWhat is AOSpine? Jens R. Chapman
Geriatric Cervical Spine1:45 – 1:50 PMCase Presentation Roger Hartl
1:50 – 2:05 PMDecision-making: Surgical vs. Non-operative Management of Odontoid FracturesJoseph S. Cheng
2:05 – 2:20 PMThe AOSpine Multicenter GOF Study Alexander R. Vaccaro
2:20 – 2:35 PMCervical Myelopathy: Clinical Trials andEvidence-based ManagementMichael G. Fehlings
2:35 – 2:50 PMCase Resolution /Questions /Discussion
The Osteoporotic Spine2:50 – 2:55 PMCase Presentation Darrel S. Brodke
2:55 – 3:10 PMBiomechanics of Fixation in theOsteoporotic SpineTheodore J. Choma
3:10 – 3:25 PMManagement of Complications in theOsteoporotic SpineLuis M. Vialle
3:25 – 3:40 PMCase Resolution/Questions /Discussion
3:40 – 3:50 PMBreak
Thoracolumbar Degeneration /Deformity3:50 – 4:05 PMManagement of ThoracolumbarDeformity in the ElderlyDarrel S. Brodke
4:05 – 4:20 PMMinimally Invasive Approaches in theAging Spine: Pros and Cons Roger Hartl
4:20 – 4:35 PMQuestions/Discussion
Surgery Trends and Health Care Costs inthe Elderly4:35 – 4:55 PMIncreasing Complexity of Surgeries in theElderly: Are We Operating Too Much?Eugene Carragee
4:55 – 5:15 PMResponse: The Role of Surgery in ElderlyPatientsChristopher I. Shaffrey
5:15 – 5:30 PMQuestions / Discussion
YOUNG NEUROSURGEONS’DINNER
6:30 PMSouthern Hemisphere V
All residents, fellows and youngneurosurgeons are encouraged to attendthis event with a special presentationfrom Dr. Gerald E. Rodts, Jr. RSVP to DePuy Spine, Booth #207.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 33
FRIDAY MEETING AGENDA
SATURDAYMARCH 10, 2012
6:30 – 6:55 AMSouthern Hemisphere Foyer
Continental BreakfastSouthern Hemisphere I-IIICase Presentations
Moderators: Aruna Ganju, D. Kojo Hamilton
6:55 – 7:00 AMMeeting AnnouncementsMarjorie C. Wang
7:00 – 8:20 AMSouthern Hemisphere I-IIIScientific Session IV
Oral Poster Presentations IIIModerators:Michael P. Steinmetz, Jean-Paul Wolinsky
7:00 AM – 7:05 AM212. Preoperative Zung Depression Scale Predicts Patient SatisfactionIndependent of Extent of ImprovementAfter Revision Lumbar SurgeryScott L. Parker, Owoicho Adogwa, David Shau, Stephen Mendenhall, Matthew McGirt
7:05 AM – 7:10 AM213. Extent of Preoperative DepressionPredicts Outcome After Revision LumbarSurgery for Adjacent Segment Disease,Recurrent Stenosis, and PseudoarthrosisScott L. Parker, David Shau, Stephen Mendenhall, Owoicho Adogwa,Clinton J. Devin, Matthew McGirt
7:10 AM – 7:15 AM218. Intradiscal Injection of Simvastatinfor Disc Regeneration in a Rat Model ofDegenerative Disc DiseaseKhoi Duc Than, Shayan Rahman, Kwaku A. Kyere, Lin Wang, Tracey T. Than,Adam Khan, Yoon-Shin Park, Ki Park,Victor C. Yang, Frank La Marca, Paul Park,Huina Zhang, Chia-Ying Lin
7:15 AM – 7:20 AM223. Correction of Sagittal MalalignmentFollowing Pedicle SubtractionOsteotomy Improves Cervical LordosisJustin S. Smith, Christopher P. Ames,Virginie Lafage, Eric Klineberg, Frank Schwab, Gregory Mundis, Robert Hart, Shay Bess, Richard A. Hostin,Douglas C. Burton, Munish Gupta, Vedat Deviren, Christopher I. Shaffrey
7:20 AM – 7:25 AM221. The Impact of Different SurgicalStrategies in Achieving Satisfactory Post-Operative Sagittal AlignmentJustin S. Smith, Christopher P. Ames,Virginie Lafage, Frank Schwab, Richard A. Hostin, Robert Hart, Vedat Deviren, Behrooz A. Akbarnia,Jason Demakakos, Khaled Kebaish,Douglas C. Burton, Shay Bess,Christopher I. Shaffrey
7:25 – 7:28 AMDiscussion
7:28 AM – 7:33 AM236. Prediction of Reciprocal Changes inCervical Spine Lordosis After CorrectiveThoracolumbar Deformity SurgeryYoon Ha, Vedat Deviren, Christopher P. Ames
7:33 AM – 7:38 AM240. Minimally Invasive Treatment ofAdult Scoliosis with XLIF: RadiographicOutcomes and Predictors from aProspective Multicenter StudyAntoine Tohmeh, Frank Phillips, W.B. Rodgers
7:38 AM – 7:43 AM234. Minimally-invasive vs. OpenThoracolumbar Fusion: A Hospital-basedMicrocosting AnalysisDaniel R. Kramer, Robert G. Whitmore,James Harris Stephen, Robert Stetson,Angus McWilliams, Sherman C. Stein,Sean Doerfler
7:43 AM – 7:48 AM243. Analysis of Spinal Surgery FusionCosts over a Six-hospital System: HowCan We Explain Dramatic Variances inthe Cost of Surgery Between ProvidersDaniel Robert Fassett, Yazhini Gnanasambanthan, Rae Podabinski, Alexander Hass
7:48 AM – 7:53 AM230. Does Single Dose PreemptiveAmitriptyline or Gabapentin ReduceRemaining Leg Pain After Single LevelLumabr Discectomy? A RandomisedClinical Trial with Placebo ControlPayman Vahedi, Zahra Mohajernejadfard
7:53 – 7:57 AMDiscussion
7:57 AM – 8:02 AM232. Modulation of Spinal Cord ReflexCircuitry by Spinal DC Stimulation inHumansMaxwell Boakye, Robert Thomas Arrigo,Chris Ho, Jean-Charles Lamy
8:02 AM – 8:07 AM237. Characterization of a NovelMetastatic Human BreastAdenocarcinoma Rat Model UsingIntracardiac Injection andBioluminescencePatti L. Zadnik, Rachel Sarabia-Estrada,Mari L. Groves, Ali Bydon, Ziya L. Gokaslan, Jean-Paul Wolinsky,Timothy F. Witham, Daniel M. Sciubba
8:07 AM – 8:12 AM241. WITHDRAWN
8:12 AM – 8:17 AM209. The Distribution of Body Mass as aSignificant Risk Factor for Lumbar SpinalFusion Postoperative InfectionsAnkit Mehta, Ranjith Babu, Isaac Karikari,Betsy H. Grunch, Vijay Agarwal, Timothy Ryan Owens, Allan H. Friedman,Carlos A. Bagley, Oren N. Gottfried
8:17 – 8:20 AMDiscussion
8:20 – 10:10 AMSouthern Hemisphere I-III
Moderators: James S. Harrop, Charles Kuntz, IVCourse Description:This Scientific Session will involvesuccinct debates on controversial clinical topics. Experts will argue theirperspectives with regard to themanagement scenarios for asymptomaticpatients with spine and peripheral nervedisease.Learning Objectives:On completion of this course, participantsshould be able to: u Analyze the role of surgical treatmentof asymptomatic cervical stenosis withcord signal changes.
u Evaluate the role of surgical treatmentof an asymptomatic schwannoma.
u Discuss the risks and benefits oftreatment of a neurologically intactpatient with a thoracic epidural abscessand cord compression.
David Cahill MemorialControversies II: Spine andPeripheral Nerve Rapid Fire
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES34
MEETING AGENDA SATURDAY
u Understand the risks and benefits oftreatment of an asymptomatic unstablegeriatric dens fracture.
8:20 – 8:45 AMAsymptomatic Cervical Stenosis withCord Signal Changes
8:20 – 8:22 AMCase PresentationCharles Sansur
8:22 – 8:30 AMRichard G. Fessler
8:30 – 8:38 AMEdward C. Benzel
8:38 – 8:45 AMDiscussion
8:45 – 9:10 AMAsymptomatic Schwannoma: Peripheral Nerve
8:45 – 8:47 AMCase PresentationOlawale Sulaiman
8:47 – 8:55 AMRobert J. Spinner
8:55 – 9:03 AMLynda J.S. Yang
9:03 – 9:10 AMDiscussion
9:10 – 9:35 AMNeurologically Intact Patient withThoracic Epidural Abscess and CordCompression
9:10 – 9:12 AMCase PresentationCharles Sansur
9:12 – 9:20 AMGerald E. Rodts, Jr.
9:20 – 9:28 AMRobert F. Heary
9:28 – 9:35 AMDiscussion
9:35 – 10:00 AMAsymptomatic Unstable Geriatric Dens Fracture
9:35 – 9:37 AMCase PresentationCharles Sansur
9:37 – 9:45 AMRegis W. Haid, Jr.
9:45 – 9:53 AMMichael G. Fehlings
9:53 – 10:00 AMDiscussion
10:00 – 10:10 AMQuestions
10:40 – 10:45 AMSouthern Hemisphere I-III
Fellowship Awards and UpdatesZoher Ghogawala, Adam S. Kanter, Daniel M. Sciubba
10:45 – 11:00 AMSouthern Hemisphere I-III
Clinical Trial Award Updates
10:45 – 10:50 AMMinimally Invasive vs. Open TLIF forSpondylolisthesisKhalid M. Abbed
10:50 – 10:55 AMCSM – Can Outcome Be Predicted byDiffusion Tensor Imaging?Marjorie C. Wang
10:55 – 11:00 AMA Web-based Registry for ComparativeEffectiveness Research for Back Pain inthe Wisconsin PopulationDaniel K. Resnick
11:00 AM – 12:30 PMSouthern Hemisphere I-III
Oral Poster Presentations IVModerators:Michael D. Martin, Shekar N. Kurpad
11:00 – 11:05 AM244. Anterior vs. Posterior InterbodyFusion: A Comparison of OutcomesMark Mahan, Samuel Kalb, Juan Christian Ribas Nijkerk, Laura Ann Snyder, Udaya K. Kakarla,Nicholas Theodore
11:05 – 11:10 AM245. Utility of Clavien-Dindo andAccordion Classification Systems forPostoperative Complications FollowingSpinal Metastasis SurgeryMaxwell Boakye, Pelu Tran, Robert Thomas Arrigo, Ivan Cheng, Stefan A. Mindea, Eugene Carragee, John Park, Todd Alamin
11:10 – 11:15 AM246. Cost-utility and ComparativeEffectiveness Analyses of Laminectomyvs. Comprehensive Medical Managementfor Lumbar StenosisScott L. Parker, Scott Zuckerman, David Shau, Stephen Mendenhall, Joseph S. Cheng, Clinton J. Devin,Matthew McGirt
11:15 – 11:20 AM228. Cost-utility and ComparativeEffectiveness Analyses of Trans-foraminalLumbar Interbody Fusion (TLIF) vs.Comprehensive Medical Managementfor Lumbar SpondylolisthesisScott L. Parker, Scott Zuckerman, David Shau, Stephen Mendenhall, Joseph S. Cheng, Clinton J. Devin,Matthew McGirt
11:20 – 11:25 AM247. Long-term Outcome of MinimallyInvasive Transforaminal LumbarInterbody Fusion: 5 Years Post-op andBeyondHamid M. Shah, Kevin T. Foley
11:25 – 11:28 AMDiscussion
11:28 – 11:33 AM224. Pedicle Subtraction Osteotomy withExtension of Fusion to the Pelvis: DoesAnterior Interbody Support at L5-S1Improve Sagittal and Pelvic Parameters?Justin S. Smith, Christopher P. Ames,Munish Gupta, Eric Klineberg, Virginie Lafage, Shay Bess, Frank Schwab,Oheneba Boachie-Adjei, Khaled Kebaish,Kirkham Wood, Behrooz A. Akbarnia,Gregory Mundis, Michael F. O’Brien,Richard A. Hostin, Christopher I. Shaffrey
10:10 – 10:40 AMSouthern Hemisphere I-III
Beverage Break
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 35
SATURDAY MEETING AGENDA
11:33 – 11:38 AM222. How the Assessment of Pelvic Tilt,Pelvic Incidence/Lumbar LordosisMismatch and Sagittal Vertical AxisPredicts Disability in Adult SpinalDeformity: A Prospective AnalysisJustin S. Smith, Christopher P. Ames, Frank Schwab, Shay Bess, Benjamin Blondel, Richard A. Hostin,Oheneba Boachie-Adjei, Douglas C. Burton, Behrooz A. Akbarnia,Gregory Mundis, Khaled Kebaish, Robert Hart, Virginie Lafage, Christopher I. Shaffrey
11:38 – 11:43 AM259. Relationship Between EffectiveLordosis and Patient Reported Neck Painand DisabilityAlex Riccio, David L. Semenoff, John W. German
11:43 – 11:48 AM253. Does Recombinant Human BoneMorphogenetic Protein-2 (rhBMP-2)Dose and/or Cage Countersinking DepthAffect the Incidence of Heterotopic BoneFormation in Posterior Interbody Fusion?Eric W. Nottmeier, Cammi Bowman, Zane Thompson, Matthew Hale
11:48 – 11:53 AM257. Comprehensive Assessment of One-year Outcomes After SuboccipitalCraniectomy for Chiari I Malformation in AdultsScott L. Parker, Scott Zuckerman, David Shau, Stephen Mendenhall, Matthew McGirt
11:53 – 11:56 AMDiscussion
11:56 AM – 12:01 PM251. Predictors of Outcome FollowingTraumatic Spinal Cord InjuryDaniel Yavin, Steven Casha, Amro Al-Habib, R. John Hurlbert
12:01 – 12:06 PM249. Diffusion Tensor Imaging Correlateswith Spinal Somatosensory EvokedPotentials After Spinal Cord InjuryShekar N. Kurpad, Brian Schmit, Michael Jirjis
12:06 – 12:11 PM200. Acute Adrenal Insufficiency inCervical Spinal Cord InjuryEmil Antonio Pastrana Ramirez, Fanor Manuel Saavedra, Samuel Estronza-Ojeda, Gisela Murray,John David Rolston, Gloria E. Rodriguez-Vega
12:11 – 12:16 PM255. Early Stabilization of ThoracolumbarInjuries in Polytraumatized PatientsTimothy A. Moore, Michael P. Steinmetz,Heather Vallier
12:16 – 12:21 PM252. Functional Improvement After TotalDisc Arthroplasty at 1 and 2 Levels of theCervical Spine: 36 Month Follow-Up ofan FDA IDE Clinical TrialReginald J. Davis, Steven E. Gaede,Michael S. Hisey, Kee Duk Kim, Pierce D. Nunley, Daniel L. Peterson,John K. Stokes
12:21 – 12:26 PM204. Short-term ComplicationsAssociated with Surgery for High-gradeSpondylolisthesis in Adults and PediatricPatients: A Report from the ScoliosisResearch Society Morbidity andMortality DatabaseManish K. Kasliwal, Justin S. Smith,Christopher I. Shaffrey, Dwight Saulle,Lawrence Lenke, David W. Polly, Jr.,Christopher P. Ames, Joseph Perra
12:26 – 12:30 PMDiscussion
12:30 PMAdjourn
The following companies have provided
an educational grant in support of the
2012 Annual Meeting:
Biomet SpineDePuy Spine
GlobusK2M
Medtronic NuVasive
Spine Wave, Inc.SpineologyStryker SpineSynthes Spine
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES36
MEETING AGENDA SATURDAY
Mobile Meeting Guide Use the Mobile Meeting Guide to search for meeting rooms, sessions, faculty members,exhibit booths, abstracts and more. This supplement to the Scientific Program book allowsyou to conveniently access all the 2012 Annual Meeting offers – right from yourSmartphone or laptop! Log on to http://m.cns.org to access this resource today!
u See who is registered
u Locate meetings and courses
u Browse abstracts and digital posters
u Find out what is happening right now
u And more!
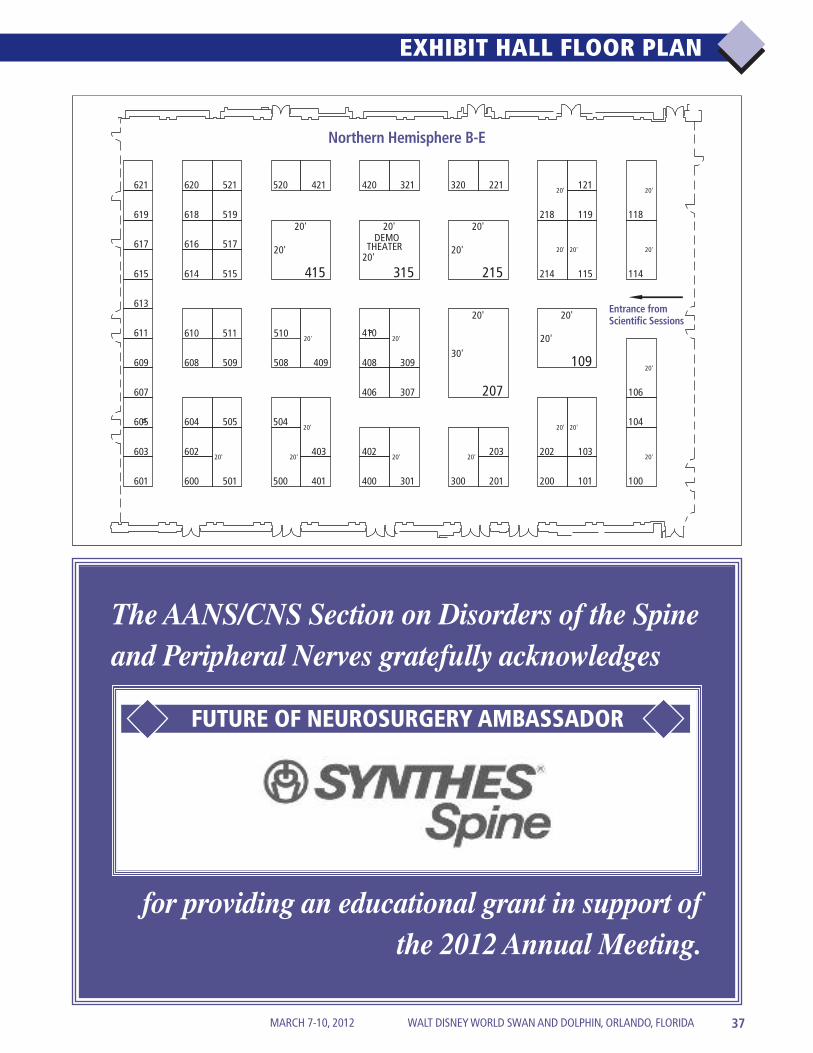
100
20'
101
103
20'104
106
20'109
20'
20'
114
20'
115
20'
118
20'
119
121
200201
202
20'
203
207
20'
30'
214
20'
215
20'
20'
218
20'221
300
20'
301
20'
307
309
20'
315
20'
20'
DEMOTHEATER
320321
400401
402403
20'
406
408
410
415
20'
20'
420421
500
20'
501
20'
504505
509 508 409
515
517
519
520521
600601
602603
604605
607
608
511 510610
609
611
613
614615
616617
618619
620621
20'
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 37
EXHIBIT HALL FLOOR PLAN
The AANS/CNS Section on Disorders of the Spineand Peripheral Nerves gratefully acknowledges
for providing an educational grant in support ofthe 2012 Annual Meeting.
FUTURE OF NEUROSURGERY AMBASSADOR
Entrance from Scientific Sessions
Northern Hemisphere B-E
Advanced Biologics 504 555 Corporate Parkway, Suite 260 Ladera Ranch, CA 92694 800-272-0267 www.advancedbiologics.com
Aesculap Implant Systems 214 3773 Corporate Parkway Center Valley, PA 18034 800-258-1946 www.aesculapimplantsystems.com
Alphatec Spine 415 5818 El Camino Real Carlsbad, CA 92008 760-431-9286 www.alphatecspine.com
Amedica/US Spine 202 1885 West 2100 South Salt Lake City, UT 84119 801-839-3500 www.amedicacorp.com
AOSpine North America 400 1700 Russell Road Paoli, PA 19301 610-993-5131 www.aospine.org
Atlas Spine, Inc. 402 1555 Jupiter Park Drive, Suite 4 Jupiter, FL 33458 561-741-1108 www.atlasspine.com
Baxano, Inc. 511 655 River Oaks Parkway San Jose, CA 95134 408-514-2200 www.baxano.com
Baxter Healthcare Corp. 218 One Baxter Parkway Deerfield, IL 60015 800-423-2090 www.baxterbiosurgery.com
*Biomet Spine & Bone Healing 106Technologies100 Interpace Parkway Parsippany, NJ 07054 973-299-9300 www.biometspine.com
BSN medical 510 5825 Carnegie Boulevard Charlotte, NC 28209 704-554-9933 www.bsnmedical.com
Captiva Spine 420 967 Alternate A1A, Suite #1 Jupiter, FL 33477 877-772-5571 www.captivaspine.com
Centinel Spine, Inc. 119 900 Airport Road, Suite 3B West Chester, PA 19380 484-887-8810 www.centinelspine.com
Congress of 602Neurological Surgeons 10 North Martingale Road, Suite 190Schaumburg, IL 60173847-240-2500www.cns.org
Covidien 508 15 Crosby Drive Bedford, MA 01730 800-722-8772 www.durasealinfo.com
*DePuy Spine 207 325 Paramount Drive Raynham, MA 02767 508-880-8100 www.depuyspine.com
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES38
EXHIBITOR INFORMATION
The Exhibit Hall, located in the NorthernHemisphere B-E, will feature:More than 60 exhibiting companies displaying thelatest neurosurgical technology and equipment,products and services.
Lunch in the Exhibit Hall*: Enjoy a complimentary lunch onThursday and Friday while mingling with your corporatecontacts.
Reception with the Exhibitors: Join us Thursday evening foranother great networking opportunity! Take the time to browsethe aisles of the Exhibit Hall and visit with your corporatecolleagues while enjoying cocktails and hors d’oeuvres.
E–mail Café: Stay in touch with home and the office throughthis complimentary attendee service.
Digital Posters: Browse over 240 abstracts enhanced byphotos and video. The digital format also makes it easy to searchfor abstracts by author or topic.
What’s New Sessions: Join the crowd during daily breaks andThursday lunch as speakers share the latest in cutting-edgeresearch and technology.
Exhibit Hall HoursThursday, March 8 9:00 AM – 7:00 PMFriday, March 9 9:00 AM – 2:00 PM
Beverage Break and What’s New Session HoursThursday, March 8 9:30 – 10:15 AM
12:30 – 1:25 PM*3:00 – 3:45 PM
Friday, March 9 9:30 – 10:15 AM 12:30 – 1:25 PM*
*Lunch in the Exhibit Hall is complimentary to all medicalattendees and guests ages 18 and older.
EXHIBIT HALL NORTHERN HEMISPHERE B-E
Exactech, Inc. 613 2320 NW 66th Court Gainesville, FL 32653 352-377-1140 www.exac.com
Gauthier Biomedical, Inc. 307 1235 North Dakota Drive, Suite G Grafton, WI 53024 262-546-0010 www.gauthierbiomedical.com
*Globus Medical 109 2560 General Armistead Avenue Audubon, PA 19403 610-930-1800 www.globusmedical.com
GS Medical 601 5200 Soquel Avenue, Suite 104 Santa Cruz, CA 95062 831-477-1307 www.gsmedicalusa.com
Industrial Pharmacy 201Management20377 SW Acacia Street Newport Beach, CA 92660 949-777-3100 www.ipmrx.com
Integra Spine 501 311 Enterprise Drive Plainsboro, NJ 08536 609-275-0500 www.integralife.com
Invuity, Inc. 611 39 Stillman Street San Francisco, CA 94107 415-655-2100 www.invuity.com
*K2M, Inc. 114 751 Miller Drive SE Leesburg, VA 20175 703-777-3155 www.k2m.com
KARL STORZ Endoscopy- 605America, Inc. 2151 East Grand Avenue El Segundo, CA 90245 800-421-0837 www.ksea.com
LANX, Inc. 403 310 Interlocken Parkway, Suite 120 Broomfield, CO 80021 303-443-7500 www.lanx.com
LDR 221 13785 Research Boulevard, Suite 200 Austin, TX 78750 512-344-3300 www.ldrspine.com
Life Instrument Corporation 515 91 French Avenue Braintree, MA 02184 781-849-0109 www.lifeinstruments.com
Lilly USA, LLC 408 Lilly Corporate Center Indianapolis, IN 46285 317-651-6557 www.lilly.com
Lippincott Williams and 401Wilkins/WKHTwo Commerce Square2001 Market Street Philadelphia, PA 19103 215-521-8300 www.lww.com
*Medtronic 215 2600 Sofamor Danek Drive Memphis, TN 38132 901-393-3133 www.medtronic.com
MiMedx Group, Inc. 517 60 Chastain Center Boulevard Kennesaw, GA 30144 404-461-9265 www.mimedx.com
Misonix, Inc. 321 1938 New Highway Farmingdale, NY 11735 800-694-9612 www.misonix.com
NeuroMatrix 101 6250 Shiloh Road Alpharetta, GA 30005 800-393-6118 www.neuromatrix.com
New World Rarities, Ltd. 609670 Old Willets Path Hauppauge, NY 11788 800-431-1018 ext. 321www.newworldrarities.com
North American 505Spine Society7075 Veterans Boulevard Burr Ridge, IL 60527 630-230-3600 www.spine.org
NovaBone Products LLC 203 13631 Progress Boulevard, Suite 600 Alachua, FL 32615 386-462-7660 www.novabone.com
Nutech Spine 406 2641 Rocky Ridge Lane Birmingham, AL 35216 205-290-2158 www.nutechmedical.com
*NuVasive, Inc. 115 7475 Lusk Boulevard San Diego, CA 92121 858-909-1800 www.nuvasive.com
Orthofix Spine 300 3451 Plano Parkway Lewisville, TX 75056 214-937-2000 www.orthofix.com
Paradigm Spine 421 505 Park Avenue, 14th Floor New York, NY 10022 212-583-9700 www.paradigmspine.com
Pioneer Surgical 121 9600 Great Hills Trail, Suite 160E Austin, TX 78759 512-372-4355 www.pioneersurgical.com
PMT® Corporation 509 1500 Park Road Chanhassen, MN 55317 952-470-0866 www.pmtcorp.com
Riverside Health System 519 701 Town Center Drive Newport News, VA 23606 757-544-6069 www.riversideonline.com
RTI Biologics, Inc. 520 11621 Research Circle Alachua, FL 32615 386-418-8888 www.rtibiologics.com
Sentient 603 11011 McCormick Road Hunt Valley, MD 21031 410-666-2588 www.sentientmedical.com
Sentio 600 21520 Bridge Street Southfield, MI 48033 248-595-0420 www.sentiommg.com
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 39
EXHIBITOR INFORMATION
SI-Bone, Inc. 607 3055 Olin Ave, Suite 2200 San Jose, CA 95128 408-207-0700 www.si-bone.com
Spinal Elements, Inc. 200 2744 Loker Avenue West, Suite 100 Carlsbad, CA 92010 760-607-0121 www.spinalelements.com
Spine Wave 3093 Enterprise Drive, Suite 210 Shelton, CT 06484 203-944-9494 www.spinewave.com
*Spineology, Inc. 118 7800 3rd Street North, Suite 600 St. Paul, MN 55128 888-377-4633 www.spineology.com
SpineSelect, LLC 104 408 Council Circle (P.O. Box 3660) Tupelo, MS 38801 662-841-7585 www.spineselect.com
SpineView, Inc. 320 48810 Kato Road, Suite 100E Fremont, CA 94538 510-623-1931 www.spineview.com
*Stryker 100 2 Pearl Court Allendale, NJ 07401 866-457-7463 www.stryker.com
Surgitel/General Scientific Corp. 604 77 Enterprise Drive Ann Arbor, MI 48103 734-996-9200 www.surgitel.com
*Synthes Spine 410 1302 Wrights Lane East West Chester, PA 19380 610-719-5000 www.synthes.com
TeDan Surgical Innovations 301 11333 Chimney Rock Road, Suite 180 Houston, TX 77035 713-726-0886 www.tedansurgical.com
TranS1 500301 Government Center Drive Wilmington, NC 28403 910-332-1700 www.trans1.com
ulrich medical USA 610 225 Chesterfield Industrial Boulevard Chesterfield, MO 63005 636-519-0268 www.ulrichmedicalusa.com
Vertebral Technologies, Inc. 509 5909 Baker Road, Suite 550 Minnetonka, MN 55345 952-912-5400 www.vti-spine.com
Zimmer Spine 103 7375 Bush Lake Road Minneapolis, MN 55439-2027 800-665-2614 www.zimmerspine.com
Zyga Technology, Inc. 521 700 10th Avenue South, Suite 20 Minneapolis, MN 55415 612-455-1061 www.zygatech.com
*indicates 2012 Corporate Supporters
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES40
EXHIBITOR INFORMATION
Find the latest research, procedures, productsand services during What’s New sessions!
Join these Exhibitors in the Demonstration Theater for special 10-minute presentations!
THURSDAY, MARCH 89:30 – 10:15 AM
12:30 – 1:25 PM
3:15 – 4:00 PM
FRIDAY, MARCH 99:30 – 10:15 AM
CNS1132_12DSPN_ScientificProgram_Interior_1 2/21/12 6:42 PM Page 40
Complement your neurosurgical experience and education…
…with themostpopular onlinelearning resource for both neuro-surgeons and residents!
SANS Lifelong Learning, offered exclusively through the Congress of Neurological Surgeons,provides subscribers a wide variety of options for learning, including:
l SANS Lifelong Learning General Examinationl SANS: Spinel SANS: Pediatrics l SANS Competenciesl SANS Neurotraumal SANS ABOS
With content that is continually updated, this dynamic learner-driven tool allows you to improve your proficiency in surgical decision making and stay abreast of the latest advances in the field!
• Compare your performance with your peers. • Highlight and bookmark information of interest. • Get a quick overview of your overall performance or a specific analysis by category. • Explore expanded learning links and in-depth critique of each question.
Log on to http://sans.cns.org and start using this essential tool today!
Congress of Neurological Surgeons10 N. Martingale Road, Suite 190, Schaumburg, Illinois 60173
Phone: 847-240-2500 Toll-free: 877-517-1CNS Fax: 847-240-0804 [email protected] www.cns.org
SANS: Spine and SANS ABOS
available for purchase!

100Characterization of FactorsPredictive of PerioperativeComplications in Adult PatientsUndergoing Complex MultilevelSpinal Instrumentation forDeformity: A Consecutive Series of160 PatientsIsaac Karikari, Jordan Komisarow, Dylan Britt, Ankit Indravadan Mehta,Betsy H.Grunch, Deeptee Jain, Oren N. Gottfried, Carlos A. BagleyIntroduction: The emergence of new spinetechniques combined with an agingpopulation has resulted in an increasednumber of complex spineinstrumentations. The specificcomplications in patients undergoing longsegment instrumentations are underreported.Methods: A retrospective review wasperformed on 160 consecutive adultpatients who underwentthoracolumbopelvic fixation for deformitybetween 2004 and 2011. A binary logisticregression model was created to determinethe variables that are associated withincreased perioperative complications.The primary endpoints were overallcomplications, major, and minorcomplications. The variables studiedincluded age, sex, levels of fusion,comorbidity index, fusion to pelvis andestimated blood loss.Results: The mean age was 54.7 years.There were 54 males and 106 females.The mean follow-up was 13.9 months.The mean length of stay was 7.2 days.The mean number of levels fused was 9.2.The average estimated blood loss (EBL)was 1735 ml. The overall rate ofcomplications was 51.9% (i.e. 83 patientshad at least 1 complication). We observed4 deaths in this study. A binary logisticregression analysis revealed fusion topelvis (P = 0.009) and prolonged lengthof stay (P = 0.039)] to be associated withincreased perioperative complication.Age, sex, comorbidity index, levels offusion, osteotomy and EBL did not show
a statistically significant association withincreased complications (P = 0.55, 0.48,0.24, 0.52, 0.45, 0.61, respectively). Theoverall complication rate was 62% and47.3% in the elderly and younger groups,respectively (P = 0.39). Of all thecomplications, respiratory failure,myocardial infarction and intraoperativeCSF leak were found to be significantlyhigher in the elderly group (P = 0.043,0.033, 0.04 respectively).Conclusion: Complication rates in elderlypatients undergoing complex spinalfusions remain high. A continuedassessment of perioperative complicationsand factors predictive of complications arenecessary to ensure safe and favorableoutcomes.
101The Impact of Positive RegionalSagittal Alignment on Outcomes inPosterior Cervical Fusion SurgeryJessica A. Tang, Justin K. Scheer, Justin S. Smith, Vedat Deviren, Shay Bess,Robert Hart, Virginie Lafage, Christopher I. Shaffrey, Frank Schwab,Christopher P. AmesIntroduction: Positive spinal sagittalmalalignment has repeatedly shown tocorrelate with pain and disability inthoracolumbar fusion. This studyevaluated the relationship betweencervical sagittal alignment andpostoperative outcomes for patientsreceiving multi-level cervical fusion.Methods: From 2006-2010, 113 patientsreceived multi-level cervical fusion forcervical stenosis, myelopathy, andkyphosis. Radiographic measurements atintermediate follow-up included: (1) C1-C2 lordosis, (2) C2-C7 lordosis, (3)C2-C7 sagittal vertical axis (C2-C7 SVA),(4) Center of gravity of head SVA (CGH-C7 SVA), and (5) C1-C7 SVA. Healthrelated quality of life measures (HRQOL)included neck disability index (NDI),visual analog pain scale (VAS), and SF-36physical component (PCS) scores.Pearson product-moment correlationcoefficients were calculated between pairsof radiographic measures and HRQOLscores. Improvement in NDI scoresfollowing surgery were evaluated bycategorizing scores into standard intervals:no disability (0-4), mild (5-14), moderate(15-24), severe (35-34), and complete(>34).Results: 80% of patients experienced animprovement of NDI scores or remainedthe same compared to preop. PCS scoresimproved by 22.0 ± 37.5%. Both C2-C7
SVA and CGH-C7 SVA negativelycorrelated with PCS (r = 0.43, P <0.001and r = 0.36, P = 0.005, respectively). C2-C7 SVA positively correlated with NDIscores (r = 0.20, P = 0.036). C1-C2lordosis constituted 76.0 ± 15.8% of totalcervical lordosis (sum of C1-C2 and C2-C7 lordosis). C2-C7 SVA positivelycorrelated with C1-C2 lordosis (r = 0.33,P = 0.0003). For significant correlationsbetween C2-C7 SVA and NDI scores,regression models predicted a thresholdC2-C7 SVA value of approximately40mm, beyond which correlations weremost significant.Conclusion: Positive cervical sagittalmalalignment, measured by C2-C7 SVA,negatively affects HRQOL scoresfollowing multi-level cervical fusion atintermediate follow-up. This is the firststudy to examine the impact that regionalSVA in the cervical spine has uponHRQOL following multi-level cervicalfusion. Our findings demonstrate that,similar to the thoracolumbar spine, theseverity of disability increases withpositive sagittal malalignment followingsurgical reconstruction.
102Complications Following Use ofrhBMP-2 in Anterior LumbarInterbody Fusion: An InstitutionalCohort Controlled StudyDaniel Lubelski, Kalil G. Abdullah,Matthew D. Alvin, Michael P. Steinmetz,Edward C. Benzel, Thomas MrozIntroduction: Recombinant human bonemorphogenetic protein-2 (rhBMP-2) hasbeen increasingly used in spinal fusions.While initial studies extolled the product’simprovement of patients’ outcomes, recentinvestigations have revealed increasedrates of urological complications, as wellas wound infection, pseudoarthrosis, andreoperation, relative to the standard ALIFprocedure.Methods: Using the institutional electronicmedical records, we retrospectivelyreviewed all patients who underwentALIF with and without rhBMP-2 betweenJanuary 2002 and August 2010. Patientdemographic, operative, andoutcome/complication information wascollected.Results: Of the 267 ALIF patients that fitour inclusion criteria, 144 included the useof rhBMP-2 and 123 did not and served asthe control cohort. The mean follow-upwas 20.2 months for the rhBMP-2 groupand 32.5 months for the control group. Nodifference was found regarding the
ORAL PLATFORMABSTRACTS
Thursday and Friday,March 8 and 9 at 10:15 AMSouthern Hemisphere I-III
Nine-minute presentations by theprimary authors are followed by shortdiscussion periods.
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES42
ORAL PLATFORM ABSTRACTS

number of urological complications in therhBMP-2 group vs. the control group (8%vs. 7%, respectively). Only one case ofretrograde ejaculation was identified in therhBMP-2 group, none were found in thecontrol group. The rates ofpseudoarthrosis, radicultis, andreoperation were significantly higher inthe rhBMP-2 group relative to the control(17% vs. 5%, 23% vs. 2%, and 22% vs.5%, respectively).Conclusion: Urological complications andretrograde ejaculation may not be asprevalent as previously reported followingALIF procedures with rhBMP-2. Thehigher rate of pseudoarthrosis, radiculitis,and reoperation confirm previous reportsand should be considered by patient andsurgeon before proceeding to operationswith rhBMP-2.
103Characterization of Myelination bySkin Derived Precursor CellsJoey Kevin Grochmal, Rajiv MidhaIntroduction: Skin derived precursor cells(SKPs) can mimic the phenotypicappearance of Schwann cells whenpredifferentiated in vitro (SKP-SCs). Ourhypothesis is that SKP-SCs can producemorphologically andelectrophysiologically functional myelinas they ensheath axons.Methods:We unilaterally injected 500,000DiI positive, GFP producing SKP-SCsinto the tibial nerves of 10 adult Lewisrats, while the contralateral tibial nervereceived media injection. This was doneone week after a demyelinating bilateraltibial nerve lesion was created using a30ul injection of 12.5ug/mlAdriamycin(1). All animals were followedfor compound motor action potentials(CMAPs) every three days until 60 dayspost-adriamycin. A parallel series ofanimals also included a cohort that insteadreceived GFP labeled Schwann cells(500,000), all of which were sacrificed atday 33 post-adriamycin injury (n =5/group). These animals were analyzedfor EPON morphometry, teased fibreimmunohistochemistry (NaV1.6), as wellas confocal anaysis of 8µm frozensections for axial morphology.Results: The cohort of animals that werefollowed until day 60 demonstrated nosignificant difference between theirrespective return to electrophysiologicalnormalcy. At day 33, however, SKP-SCspromoted a significantly lower G-ratio (P< 0.05) when analyzed against eithermedia or Schwann cell injection in this
model (Epon morphometry, N = 5/group).Teased fibre analysis and spectral confocalanalysis demonstrated strong evidence ofmyelination by SKP-SCs. These cellsformed compact myelin and participatedin mature Node of Ranvier formation.Conclusion: SKP-SCs graft improves tibialnerve remyelination within thisadriamycin injury model. The effect isrobust enough to produce a morphometricdifference in the G-ratios between thetreatment groups at day 33, with the SKP-SC group measuring closest to a normalG-ratio. One plausible mechanism for theimproved morphometry is the direct,compact myelination of axons by SKP-SCs, which was conclusivelydemonstrated.
104The Design and Development of theNeuropoint SD Spine Registry forLumbar Discectomy and Single LevelFusion for SpondylolisthesisZoher Ghogawala, Christopher I. Shaffrey,Anthony L. Asher, Neil R. Malhotra, Steven Dante, R. John Hurlbert, Andrea F. Douglas, Subu N. Magge,Praveen V. Mummaneni, Joseph S. Cheng,Justin S. Smith, Michael G. Kaiser, Robert F. Heary, Khalid M. Abbed, Daniel M. Sciubba, Daniel K. ResnickIntroduction: The aim was to establish amulti-center cooperative research group todemonstrate the feasibility of developing aregistry to assess the efficacy of commonlumbar spinal procedures in actualpractice. Before proceeding withcomparative effectiveness projects, it iscritical to develop an infrastructure withpersonnel that can reliably collect health-related patient-reported outcomes datawith at least 80% compliance.Methods:A prospective, 13-site registrystudy collected data from unselectedpatients undergoing lumbar discectomy orsingle-level fusion for spondylolisthesis.Funding was obtained to enroll 200patients. Subjects completed SF-36 andODI questionnaires pre-operatively, and 3,6, and 12 months post-operatively. Allpatient data were entered into a secureHIPPA compliant internet-based datamanagement platform developed by theNeuropoint Alliance in conjunction withthe AANS.Results: Three investigator meetings wereheld. IRB approval and contracts wererequired at all sites. 211 patients werescreened and 204 were enrolled from 13academic and community sites (mean 16patients/ site) over 1 year (Figure 1).
Mean age: 46.0 years (48% female) forlumbar discectomy (N = 156), 58.3 years(60% female) for lumbarspondylolisthesis (N = 48). Eleven sitesmet enrollment goals (Figure 2). Baselinedata was collected in 99.5% of cases.Complications were assessed at 30 days(96.6% compliance) with 11 (5.4%)reported. Outcomes assessmentcompliance was 90.3% and 88.4% at 3and 6 months, respectively. Overall, therewas 88% compliance with patient-reported outcomes data collection. At 3months, lumbar discectomy and single-level fusion procedures were associatedwith significant improvements in ODI andSF-36 scores (P < 0.001).Conclusion: It is feasible to build a nationalspine registry for the collection of high-quality prospective data to demonstratethe effectiveness of spinal procedures inactual practice. Thirteen sites achieved88% compliance with the collection ofpatient-reported outcomes data over 1year.
105Is Surgical Decompression inPatients with Mild CervicalSpondylotic Myelopathy Effective?Results of the Prospective,Controlled, Multicenter AOSpineNorth America CSM StudyMichael G. Fehlings, Branko Kopjar,Sangwook Yoon, Paul M. Arnold, Eric M. Massicotte, Alexander R. Vaccaro,Darrel S. Brodke, Christopher I. Shaffrey,Justin S. Smith, Eric J. Woodard, Robert J. Banco, Jens Chapman, Michael Janssen, Christopher Bono, Rick Sasso, Mark B. Dekutoski, Ziya L. GokaslanIntroduction: Surgical decompression isstandard for patients with moderate andsevere cervical spondylotic myelopathy(CSM), however, the role of surgery incases of mild CSM remains questioned.We aimed to evaluate the efficacy andsafety of surgical decompression inpatients with mild CSM.Methods: 189 subjects with mild CSM,modified Japanese OrthopaedicAssociation (mJOA) score 12-17, and 79control subjects with moderate CSM,mJOA score 7-11, were enrolled in thisprospective, multi-center study. Theoutcome measures used were mJOA,Nurick Score, Neck Disability Index(NDI), and SF36v2. Measurements weretaken during preoperative and 12 monthpost-surgery assessments. The mild cohortoutcomes were compared to the moderate
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 43
ORAL PLATFORM ABSTRACTS

control group. Complications wereassessed prospectively.Results: Following surgery, patients withmild and moderate CSM showedsignificant improvement in all outcomes.The degree of improvement on theNurick, NDI, and SF36v2 wascomparable in patients with mild andmoderate CSM. Subjects in the mildgroup showed less absolute improvementin their mJOA scores (mean: 2.07, 95%confidence interval: 1.67-2.46) thansubjects with moderate CSM (mean: 4.80,95 % confidence interval: 4.11-5.48). Therate of perioperative neurologicalcomplications was comparable in the mild(3.7%) and moderate (3.8%) groups andlargely reflected transient nerve rootdysfunction. Of note, only one patient(0.4%) experienced permanent decline inspinal cord function.Conclusion: Surgical decompressionimproves outcomes in subjects with mildCSM to an extent comparable toindividuals with moderate CSM. This dataprovides support for surgical interventionin cases of mild CSM.
106The Short-Term Effect of Surgery onHealth Related Quality of Life andFunctional Outcome in Patients withMetastatic Epidural Spinal CordCompression (MESCC): Results of theOngoing AOSpine North AmericaProspective Multicenter StudyMichael G. Fehlings, Branko Kopjar,Charles Fisher, Laurence D. Rhines, Paul M. Arnold, James M. Schuster,Alexander R. Vaccaro, Ziya L. Gokaslan,Joel Finkelstein, John France, Mark B. DekutoskiIntroduction: Studies have providedevidence that in selected patientscombined surgery and radiotherapyprovides the optimal neurologicalrecovery in MESCC patients. However,patients with MESCC have relativelyshort life-expectancy and face numeroushealth challenges. The impact of surgeryon improving quality of life outcomes inthe setting of MESCC is unknown.Methods: 111 surgical patients wereenrolled in a prospective multi-center,cohort study involving 10 sites in NorthAmerica. Outcomes were assessed usingthe pain assessments, ASIA scale, SF-36v2, and EQ-5D.Results:Average age was 58 years, 59percent were males. Common primarysites were lungs (24 percent), prostate (12percent), breast (13 percent), and kidney
(12 percent). 67 percent survived threemonths, only 33 percent survived 12months. The survival was associated withsite of primary cancer. In survivors, theaverage improvement at 3 month was for.23 for EQ5D (P < .01), 19.2 for ODI (P< .01), 2.1 for VAS Pain (P < .01). Also,there was a significant improvement inASIA Impairment grade (P < .01). Thechanges in SF36 PCS and MCS were notsignificant.Conclusion: Surgically treated patientswith MESCC are a diverse group ofpatients with different prognoses. Thesurviving patients experience clinicallyrelevant symptoms improvement andgains in function and utility. Individualswith less than three month life expectancymay be less than ideal candidates forsurgical intervention.
107Anterior vs. Posterior SurgicalApproaches to Treat CervicalSpondylotic Myelopathy: Outcomesof the Prospective MulticenterAOSpine North America CSM Studyin 278 PatientsMichael G. Fehlings, Branko Kopjar,Sangwook Yoon, Paul M. Arnold, Eric M. Massicotte, Alexander R. Vaccaro,Darrel S. Brodke, Christopher I. Shaffrey,Eric J. Woodard, Robert J. Banco, Jens Chapman, Michael Janssen, Rick Sasso, Christopher Bono, Mark B. Dekutoski, Ziya L. GokaslanIntroduction: The optimal surgicalapproach to treat cervical spondyloticmyelopathy (CSM) remains debated withvarying opinions favoring anterior vs.posterior surgical approaches. We presentan analysis of a prospective observationalmulticenter study examining outcomes ofsurgical treatment for CSM.Methods: 278 subjects from 12 clinicalsites in NA received anterior/posterior orcombined surgery at the discretion of thesurgeon. This study focused on subjectswho had either anterior or posteriorsurgery (n = 264, 87% follow-up rate).Outcome measures included the ModifiedJapanese Orthopedic Assessment Scale(mJOA), the Nurick scale, the NeckDisability Index (NDI) and the SF36v2Physical (PCS) and Mental (MCS)Component Scores.Results: 169 patients were treated usinganteriorly (discectomy/corpectomy withinstrumented fusion) 95 receivedposteriorly (either laminectomy (86%)and fusion or laminoplasty (14%)). 42%were female. Anterior surgery cases were
younger (53 ± 11 vs. 63 ± 11 years), hadless severe myelopathy as assessed bymJOA and Nurick scores. There were nobaseline differences in NDI or SF36between the anterior and posterior cases.Anterior cases had on average 3.1vertebral levels operated on compared to5.1 levels in the posterior group (P <.0001). Improvement in the mJOA wassignificantly lower in the anterior groupwhen compared to posterior group (2.47vs. 3.62, respectively, P < .01), althoughthe groups started at different levels ofbaseline impairment. The extent ofimprovement in the Nurick, NDI, SF36v2PCS, SF36v2 MCS scores did not differbetween the anterior and the posteriorgroups.Conclusion: Patients with CSM showsignificant improvements in generic anddisease specific health related outcomemeasures with anterior or posteriorsurgery. Importantly, patients treated withanterior techniques were younger, withless severe impairment and more focalpathology. While there was a greaterimprovement in mJOA scores in posteriorcases, this difference could be accountedfor by differences in baselinecharacteristics.
108The Scope and Impact of Wrong-Level Lumbar Spine Surgery: ASurvey of the Joint Section onDisorders of the Spine andPeripheral NervesMichael W. Groff, Joshua E. Heller, Eric A. Potts, Praveen V. Mummaneni,Christopher I. Shaffrey, Justin S. SmithIntroduction:Wrong-level spine surgerycontinues despite national efforts byregulators and professional societies. Theauthors surveyed the membership of theJoint Section of Spinal Disorders andPeripheral Nerve Diseases (Spine Section)to better understand the scope and impactof wrong-level lumbar spine surgery.Methods:A Spine Section task forcedeveloped a survey on single-level lumbarspine decompression surgery, includingquestions regarding wrong-level lumbarspine surgery. Invitations to complete theweb-based survey were sent to allmembers of the Spine Section.Respondents were assured ofconfidentiality.Results: There were 569 responses from1,045 requests (54%). Almost 50% ofreporting surgeons have performedwrong-level lumbar spine surgery at leastonce, and more than 10% have performed
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES44
ORAL PLATFORM ABSTRACTS

wrong-side lumbar spine surgery at leastonce (see figure). Nearly 20% ofresponding surgeons have been the subjectof at least one medical malpractice caserelating to these errors. In 68% of cases inwhich wrong-level or wrong-side surgerywas performed, this error was discoveredat the time of surgery, and the surgeonproceeded with the correct level/sidesurgery. The error was discoveredimmediately following the procedure in5% of cases and sometime >24 hours afterthe procedure in 27% of cases. Inaddition, almost 90% of surgeons reportedat least one “close call” with regard towrong-level or wrong-side lumbar spinesurgery, including wrong level exposedbut no bony removal (65%), wrong sideexposed but no bony removal (3%), orboth of these events (20%).Conclusion: Existing safety protocols maynot be preventing wrong-level spinesurgery to the extent previously thought.These findings argue for additional studyof wrong-level spine surgery, includingdevelopment of a standardized approachfor level confirmation that can at least beused to facilitate a multi-institutionaleffort to further investigate and mitigatethese errors.
109Radiographic Predictors of EarlyFailure Following DecompressionWithout Fusion for DegenerativeGrade I Lumbar SpondylolisthesisClaire Blumenthal, Jill Curran, Edward C. Benzel, Subu N. Magge, J. Frederick Harrington, Jean-Valery Coumans, Zoher GhogawalaIntroduction: Determining specificradiographic traits that predict earlyfailure following decompression surgerymight guide clinical decision makingregarding the utility of up front fusion inpatients with degenerative grade Ispondylolisthesis.Methods: Patients with grade Idegenerative lumbar spondylolisthesis (3-14 mm) with symptomatic stenosis wereprospectively enrolled from 5 sites fromMay 2002 to September 2009 and treatedwith decompressive laminectomy with orwithout fusion. Patients with mechanicalback pain or with gross motion (>3mm)on flexion-extension lumbar radiographswere excluded. Baseline radiographicvariables measured included amount ofslippage, disc height, facet angle, motionat spondylolisthesis (flexion-extension),and sagittal rotation angle. Data wereanalyzed using univariate and multivariate
forward selection stepwise logisticregression.Results: 106 patients were enrolled, 58were treated with laminectomy withoutfusion and 42/58 patients with completeradiographic data sets were available foranalysis. Re-operation rate was 15/42(35.71%) with mean follow-up of 3 years.Re-operation was performed for paincaused by instability at the index level inall 15 cases. Using multivariate stepwiselogistic regression with a threshold p-value of 0.35, motion at spondylolisthesis,disc height, and facet angle werepredictors of reoperation followingsurgery (Table 1). Facet angle > 50degrees was associated with a 37% rate ofre-operation. Disc height > 6.5 mm wasassociated with a 45 % rate of re-operation. Patients with 3 risk factors forinstability had a 75% rate of re-operation,while patients with no risk factorsinstability had a 0% rate of re-operation(P < 0.05) (Figure 1).Conclusion: Patients with motion atspondylolisthesis, disc height > 6.5 mm,and facet angle > 50 degrees are morelikely to experience instability followingdecompression surgery for grade I lumbarspondylolisthesis. Identification of keysignificant risk factors for instability mightimprove outcomes followingdecompression without fusion surgery.
110Functional and Quality of LifeOutcomes in Geriatric Patients withType II Odontoid Fracture: One YearResults from the AOSpine NorthAmerica Multi-Center GOFProspective StudyMichael G. Fehlings, Alexander R. Vaccaro, Branko Kopjar, Jens Chapman, Christopher I. Shaffrey,Ziya L. Gokaslan, Paul M. Arnold, Darrel S. Brodke, John France, Sangwook Yoon, Mark B. Dekutoski, Rick Sasso, Christopher BonoIntroduction: Odontoid fracturescommonly occur in the elderly andrepresent a management challenge. It isunclear whether surgery or conservativemanagement is the best treatment option.There is a paucity of informationregarding treatment outcomes.Methods:We conducted a prospectivemulti-center cohort study of subjects > 65years old with Type II odontoid fracture at11 sites in North America. Patientsreceived nonoperative or surgicaltreatment at the discretion of the surgicalteam and were followed for 12 months.
Outcomes assessments included the SF36,Neck Disability Index (NDI) and rates ofmortality and complications.Results: 159 subjects were recruited(average age: 80.7 (SD 7.5), 59.8%females) 63.5% were treated operatively(11.9% anterior odontoid screw, 79.2%posterior C1- C2 screw fixation, 6.9%posterior transarticular screw fixation,1.0% Brooks Fusion and 1.0% Occipital-Cervical Fusion). 29 (18.2%) subjectsexpired and 3 subjects withdrew from thestudy. Follow-up was available for 103(79.2%) of 130 eligible, survivingsubjects. The baseline NDI was 21.7 (SD17.2) and SF36v2 PCS was 40.7 (SD10.5). At 12 months, the NDI worsened by7.6 (SD 21.0) points (P < .001) andSF36v2 PCS declined by 1.6 (SD 11.1)points (P = .019). There was a significantdifference in NDI outcomes between thesurgically and the conservatively treatedgroup. The decline in NDI among thesurgical cases was 5.6 points compared to14.7 points in the conservatively treatedgroup (P = .0173). There were nodifferences in the SF36v2 PCS outcomesbetween the treatment groups.Conclusion: In spite of treatment, elderlypatients with type II odontoid fractureexperience significant mortality anddecline in functional outcomes at one yearfollow-up. Our results do suggest thatNDI outcomes may be better in thesurgical group, though the possibility ofselection bias needs to be carefullyconsidered.
111Posterior Cervical Foraminotomy forCervical Radiculopathy:Symptomatic, Functional and Qualityof Life Outcomes in 1085 Cases withLong-term Follow-upEphraim W. Church, Casey H. Halpern,Ryan Faught, Usha Balmuri, Mark Attiah,Sharon Hayden, Marie Kerr, Eileen Maloney-Wilensky, Janice Bynum,Sherman C. Stein, Stephen J. Dante,William Charles Welch, Frederick A. SimeoneIntroduction: The efficacy and safety ofposterior foraminotomy (FOR) forcervical radiculopathy has beendemonstrated in several reports with short-term follow-up. However, there is littledata analyzing the relative effectiveness ofFOR in the treatment of cervicalradiculopathy due to soft disc vs.osteophytic disease. In the present studywe review our experience with FOR forcervical radiculopathy in a large cohort of
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 45
ORAL PLATFORM ABSTRACTS

patients treated at one center with long-term follow-up.Methods:We retrospectively examinedcharts of patients who underwent a total1085 FORs in 1990-2009. A large cohortof these patients participated in astructured telephone interview designed toassess improvement in symptoms andfunction. We assessed post-operativequality of life (QOL) using the EQ-5D. Atotal 338 interviews were completed witha mean follow-up of 10 years.Results:Approximately 90 percent ofinterviewees reported improved pain,weakness or function following FOR, andoutcomes significantly correlated withimproved QOL scores (P < 0.0001). Suchsymptomatic relief allowed 93 percent ofpatients to return to work. The overallcomplication rate was 3.3 percent and therate of recurrent radiculopathy requiringsurgery was 6.2 percent. Neither rate ofcomplications nor that of additionalsurgery correlated with QOL at long-termfollow-up. Soft disc subtypes werecompared to osteophyte disease byoperative report and were associated withsignificantly improved pain, weakness andfunction. The operative report of thesepathologic subtypes was significantlyassociated with the preoperative MRIinterpretation (P < 0.0001).Conclusion: These results suggest thatFOR is a highly effective surgicaltreatment for cervical radiculopathy with alow incidence of complications.Radiculopathy due to soft disc subtypesmay be associated with a better prognosiscompared to osteophytic disease. Thesecommon etiologies for radiculopathy maybe differentiated on preoperative MRIscans, providing an opportunity forsurgeons to predict outcome.
112The Relative Impact of LumbarSpondylosis on Quality of Life in theUnited States: A Population HealthPerspectiveCyrus Chi-Ho Wong, Scott L. Parker,Marcus J. Gates, Matthew McGirtIntroduction: Current cost of healthcare isunsustainable. To improve efficiency,payers are aiming to preferentially supporthigher value care and decrease spendingon disease states with less impact onpopulation health. The relative impactcommon disease states have on quality oflife is poorly understood. In a systematicliterature review, we determined meanquality-adjusted life year (QALY) oflumbar spondylosis vs. other common
chronic disease states and utilize U.S.prevalence rates to determine the relativeimpact (annual U.S. population QALYslost) these common diseases states haveon U.S. population health.Methods: Systematic literature review wasconducted for studies utilizing health stateinstrument(EQ-5D). Studies examiningten common disease states (both surgicaland non-surgical) were included, Table 1.Baseline health state for each disease statewas recorded from the literature. Meanhealth state per disease state wasmultiplied by Center for Disease Controlreported disease prevalence rates todetermine overall annual QALY lost perdisease state in U.S.Results: 137 studies (135,106 patients)met inclusion criteria, Table 1. Lumbarspondylosis patients had cumulative meanEQ-5D of 0.39, Table 2, the lowest QALYamong all disease states examined, Figure1. Lumbar spondylosis, kneeosteoarthritis, COPD, and diabetesmellitus were the most prevalent diseasestates, Table 3. Estimated total annualQALYs lost in the U.S. was greatest forlumbar spondylosis (18,391,456 QALYs),1.34-fold greater than knee osteoarthritis,2.6-fold greater than COPD and diabetes,4.34-fold greater than degenerative hipdisease, Table 3.Conclusion: Lumbar spondylosis wasassociated with the lowest QALY healthstate compared to other common diseasestates. Overall impact on QALYs lost forU.S. population is significantly higher forlumbar spondylosis than disease statesstudied, suggesting degenerative lumbarspinal disorders have a large anddetrimental impact on U.S. population’shealth and quality of life. Healthcarereform initiatives should allocateappropriate resources and spending toaddress this high-impact disease process.
113Pitfalls of Calculating HospitalReadmission Rates Based Solely onNonvalidated AdministrativeDatasetsBeejal Y. Amin, Urvij Modhia, Keishi Mauro, Lumine Na, Steven Takemoto, Christopher P. Ames,Vedat Deviren, Dean Chou, Sigurd Berven, Praveen V. MummaneniIntroduction:Administrative databases areincreasingly being used to establishbenchmarks for quality of care and tocompare performance across peerhospitals. As proposals for AccountableCare Organization are being developed,
readmission rates will be increasinglyscrutinized. The purpose of this study is toassess the accuracy of administrativedatasets and identify independentpredictors of readmission.Methods: Data for 5,854 consecutive spineadmissions to UCSF Medical Center fromJuly 2007- June 2011 was abstracted fromthe University Health-System Consortium(UHC) using the Clinical Database/Resource Manager. Of these admissions,320 cases (5.8%) were rehospitalizedwithin 30 days of the initial dischargedate. We performed an independent chartreview to determine reasons forreadmission and extracted hospitaladministrative data to calculate total anddirect costs. Logistic regression analysiswas used to test the odds of readmissionon categorical variables. The two-samplet-test was used to test the difference oftotal and direct cost between readmissionand non-readmission.Results: The main reasons for readmissionwere infection (46.1%), planned, stagedsurgery (11.6%), and nonoperativemanagement (9.8%). The UHC databaseoverestimated the readmission rate. Basedon our chart review, 50 cases (of the 320total readmissions) were misclassified.Thirty-seven cases (11.6%) were planned,staged procedures and 13 cases (4.1%)were unrelated to the initial admission.When planned, staged readmission casesare excluded, the total cost of readmissionis reduced by 18.2% (P = 0.005). The costvariance is in excess of one milliondollars. Predictors of readmission wereadmission status (P < 0.0001), length ofstay (P = 0.0001), risk of mortality (P <0.0001), and age (P = 0.021).Conclusion: Our findings uncover thepotential pitfalls of calculating hospitalreadmission rates based solely onnonvalidated administrative datasets.Benchmarking algorithms for defining ahospital’s readmission rate must take intoaccount planned, staged surgery andeliminate unrelated reasons forreadmission. Current tools overestimatethe true readmission rate and cost.
114Modest Systemic Hypothermia inAcute Cervical Spinal Cord Injury: AProspective Case Controlled StudyAllan D. Levi, Barth A. Green, Dalton Dietrich, Steven Vanni, Marine Dididze, Michael Y. WangIntroduction: Systemic hypothermiacontinues to show promise in select CNSinjury conditions. We have previously
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES46
ORAL PLATFORM ABSTRACTS

reported our experience (n = 14 pts)[1,2]with modest intravascular hypothermia (T-33 0C) after spinal cord injury (SCI). Wedescribe our extended single centerexperience that now spans over 6 years.Methods:We prospectively acquired dataon 32 patients (mean age 36 years, range18-65) with acute cervical SCI whoreceived intravascular hypothermia withtarget temperature (33 0C) maintained for48 hours. Clinical outcome was assessedby American Spinal injury Associationand International Medical Society ofParaplegia Impairment Scale (AIS). Allpatients initially were complete AIS A onadmission but two converted to AIS B in<12 hours. The majority of patients hadC5-6 lesion (14 and 10 respectively),while 6 had C4 and 2 - C7. 62% ofinjuries were related to motor vehicleaccident or fall.Results: The mean (SEM) time frominjury to initiation of hypothermia was5.95 (0.48) hours (after excluding fourcases due to delayed admission). Thirteenof 32 patients (41%) improved at latestfollow-up (average 11 months): 5converted to AIS B, 3 - to AIS C, 2 to AISD and 1 to AIS E. Complications weremainly respiratory. Five thromboemboliccomplications (15%) were noted - one inan arm vein, one femoral vein, one IVCclot unrelated to the catheter and twopatients developed subsegmentalpulmonary embolus, well managed withanticoagulants. Two deaths (2 and 12months post-treatment) were seen inpatients age 55 and 62 respectively.Conclusion: The AIS conversion rate of41% in 32 complete (AIS A) cervical SCIpatients compares favorably withpreviously published data regarding AISconversion rates in cervical SCI. Theincidence of complications corresponds tocontrol SCI treated in our institutionsupporting concept that systemic coolingafter SCI warrants larger, controlledprospective, randomized study.
115Prospective, Randomized Study ofCervical Arthroplasty and ACDF withLong-Term Follow-up: 76 Patientsfrom a Single Site with Four- toEight-year Follow-upDomagoj Coric, Margaret Boltes, Sara James, Judd HeidemanIntroduction: The purpose of this study isto evaluate the long-term clinical results ofcervical total disc replacement (cTDR)and anterior cervical discectomy andfusion (ACDF) in the treatment of single
level cervical radiculopathy.Methods: The results of two separateprospective, randomized US Food andDrug Administration (FDA)Investigational Device Exemption (IDE)pivotal trials (Bryan Disc and Kineflex|C)from a single investigational site werecombined to evaluate outcomes at long-term follow-up. The primary clinicaloutcome measures included the NeckDisability Index (NDI), visual analogscales (VAS), and neurologic exam.Patients were randomized to cTDR orACDF in two separate studies using theBryan Disc or Kineflex|C artificial discsvs. ACDF using structural allograft and ananterior plate.Results: Results: A total of 76 patientswere enrolled and randomly assigned toeither cTDR (n = 42) or to ACDF (n =34). A total of 63 patients (83%) wereavailable for minimum four-year follow-up (cTDR = 88%, ACDF = 77%). Averagefollow-up was 6 years (72 months) with arange from 48-96 months. Clinicalsuccess: In both the cTDR and ACDFgroups, the mean NDI and VAS scoresimproved significantly by 6 weeks aftersurgery and remained significantlyimproved throughout the minimum 48-month follow-up (P < 0.0001).Radiographic success: The range ofmotion (ROM) in the cTDR groupremained significantly greater than thepre-op mean while the ROM in the ACDFgroup was significantly reduced.Reoperation: The adjacent levelreoperation rate in the cTDR group(4.8%) was not statistically significantlydifferent than the ACDF group (5.9%).The index level reoperation rate in thecTDR group (2.4%) was not statisticallydifferent than the ACDF group (0%).Conclusion: Both cTDR and ACDF groupsshowed excellent clinical outcomes thatwere maintained over long-term follow-up. Both groups showed low index leveland adjacent level reoperation rates. BothcTDR and ACDF appear to be viableoptions for the treatment of single levelcervical radiculopathy.
116Prospective Study of Disc Repairwith NuQu Injectable AllogeneicChondrocytesDomagoj Coric, Kenneth Pettine, Margaret BoltesIntroduction: The purpose of the study wasto evaluate the safety and initial efficacyof the NuQu allogeneic juvenilechondrocyte injection. The NuQu phase I
feasibility study is a single arm,prospective study of disc repair using asingle, outpatient injection of allogeneicchondrocytes for the treatment of patientswith mechanical low back pain (LBP)with single level spondylosis (Pfirrmangrade III-IV) L3-S1.Methods: Patients were evaluated pre-operatively and post-operatively at 1, 3, 6and 12 months. Evaluations includedroutine neurological examinations, MRI,the Oswestry Disability Index (ODI) andpatient self-report visual analog scale painassessments (VAS).Results: Fifteen patients (6 female, 9 male)were enrolled at 2 sites with a mean age of40 years (range 21-48). All 15 (100%)were evaluated at one year follow-up.Levels: L3-4=2, L4-5=1,L5-S1=11. Eachinjection consisted of 1-2 cc (meaninjection=1.4cc) of junvenile chondrocytes(~ 4-5 million chondrocyte cells/cc) withfibrin glue carrier. Mean injection peakpressure=86.5 psi. The mean ODI(baseline = 53, 6 months = 28, P =0.0005), VAS (baseline=6, 6 months=4, P= 0.02) and SF-36 Physical scores(baseline = 35, 6 months = 43, P = 0.005)all improved significantly from baseline.Patient self-report of pain: improved = 8,unchanged = 6, worse = 1. MRI: Nine(60%) of 15 patients showedimprovements in MRI imaging. Highintensity zones (HIZ) consistent withposterior annular tears were present atbaseline in nine patients, eight (89%)showed improvements in MR imaging. Nopatients experienced neurologicaldeterioration. There were no serious andno unexpected adverse events. There wereno observed immunological response tothe chondrocyte injection. Two patients(13%) underwent total disc replacement by12 month follow-up due to persistent LBP.Conclusion: This is the first report of theclinical and radiographic results of cell-based disc repair therapy (injectablejuvenile chondrocytes) in the treatment oflumbar spondylosis with mechanical LBP.The results of this prospective cohort arepromising and warrant furtherinvestigation with a prospective,randomized, double-blinded, placebo-controlled study.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 47
ORAL PLATFORM ABSTRACTS

117Skin-derived Precursor Cells EnhanceFunctional Outcome Following NerveRepairHelene T. Khuong, Aleksandra Ivanovic,Antos Shakhbazau, Ranjan Kumar, Joanne Forden, Hamed Abhari, Rajiv MidhaIntroduction: Although peripheral nervesare known for the capacity to regenerate,outcome following injury remains poor.Previous work has shown that delivery ofskin-derived precursors predifferentiatedinto Schwann cells (SKP-SC) can improvesome measures of axonal regeneration in achronically denervated model of nerveinjury. There is no published data showingfunctional outcome from such a therapy ina model of acute nerve injury.Methods: Eighteen adult male Lewis ratswere trained prior to surgical interventionto cross a previously validated ladder withrungs placed at variable distance. A righttibial nerve section was performed andimmediately repaired in a direct (end-to-end) fashion. One group (n = 5) alsoreceived injection of SKP-SCs (5 X 105cells) 3 mm distally to the repair site whileanother group (n = 5) received injection ofcarrier medium at the same site. Onegroup (n = 5) underwent sham surgeryand one last group (n = 3) had a nerveinjury without repair (see Figure 1). Allrats were tested at defined timepoints overthe 20 weeks following surgery. A slipratio was calculated after gait analysis of 5runs per rat at each timepoint.Results:A baseline slip ratio was similaracross all groups. Immediately aftersurgery, the slip ratio rose similarilyamong all injured animals. Animals inboth positive and negative control groupsperformed as expected. Four weeks aftersurgery, animals treated with SKP-SCsshowed dramatic improvement with amean slip ratio that stayed low for the restof the study. The animals with mediainjection showed a slower improvementthat never matched the level of the treatedgroup. The difference between those twogroups at weeks 5 and 9 was statisticallysignificant. (See Figure 2.)Conclusion: SKP-SCs improve functionaloutcome in an animal model of immediaterepair following nerve injury, with fasterrecovery and better performance on gaitanalysis.
MAYFIELD BASIC SCIENCE AWARD118Human Mesenchymal Stem CellsSeeded in a Polymer Scaffold: ANovel Treatment Approach for SpinalCord InjuryAlexander E. Ropper, Devang Thakor, Inbo Han, Dou Yu, Hariprakash Haragopal,A. John Popp, Yang D. TengIntroduction:We investigated the effects ofhuman mesenchymal stromal stem cells(hMSCs) seeded in poly-lactic-co-glycolicacid (PLGA) scaffold on neurorestorationin rats undergoing thoracic segmentalhemisection spinal cord injury (SCI). Wehypothesized that this treatment, whichutilizes both developmental trophic andhomeostatic properties of hMSCs as wellas the structural stabilization of a PLGAscaffold, would improve sensorimotorrecovery in SCI rats.Methods: Female SD rats received aunilateral T9-10 segmental midlinehemisection. In addition to a lesioncontrol group, biocompatible andbiodegradable PLGA scaffold seeded withbone marrow-derived hMSCs, hMSCsalone or scaffold alone was implanted intothe injury epicenter immediatelyfollowing SCI (n=7/group). Standardizedbehavioral tests were performed at dayone post-injury and weekly thereafter,which was followed by analyses ofhistopathology and cellular/molecularbiology.Results: The scaffold+hMSCs treatmentgroup demonstrated significantlyimproved hind limb locomotion,coordination and spinal reflexes at 4weeks relative to all of the controls.Histochemical evaluation revealed a largervolume of spared gray and white matter inthe scaffold+hMSCs treated spinal cords.Immunocytochemistry of transversesections at and adjacent to the injuryepicenter showed the least scale ofreactive astrogliosis (i.e. GFAPimmunoreactivity) in the treated tissue,indicating that scaffold+hMSCsimplantation engendered a pro-repair
environment in the lesioned parenchyma.Moreover, the treatment reduced levels ofboth chronic inflammation as evidencedby diminished numbers of CD68 andCD11b positive cells around the injurysite and reduced immunoreactivity againstnitrotyrosine, a marker of oxidative injury.Conclusion:We have demonstrated theeffectiveness of a PLGA scaffold+hMSCsbased treatment in improvingsensorimotor function after experimentalSCI. The clinical findings weresubstantiated by histopathologic andcellular/molecular evidence that validatesour hypothesis. Importantly, our datasuggests that the autologous feasibility ofhMSCs plus the biocompatibility ofPLGA may help render CNS traumaoperable under neurosurgical regimensbased on regenerative medicine principles.
MAYFIELD CLINICAL SCIENCE AWARD119Decreased Incidence of VenousThrombo-Embolism After SpineSurgery with Early AggressiveChemoprophylaxisJoseph Bridger Cox, Catherine Koepnick,R. Patrick Jacob, Daniel J. HohIntroduction:Venous thrombo-embolism(VTE) can be a significant complicationafter spine surgery with rates reported ashigh as 2-4%. Institutional practices forVTE prophylaxis are highly variable. In2008, we instituted an aggressive protocolfor early VTE prophylaxis consisting ofcombined compressive devices andsubcutaneous heparin initiated eitherpreoperatively or the day of surgery. Inthis study, we compare our incidence ofVTE in spine surgery patients before andafter initiating this protocol.Methods:An IRB-approved retrospectivereview of spine surgery patients for 2years prior to protocol initiation and for 2years thereafter was conducted. Inclusioncriteria were spine surgery patients ≥18years old and admitted for ≥ 1 day. VTEprophylaxis since 2008 consisted of auniform protocol of heparin 5000 unitssubcutaneously three-times daily, exceptthose >75 years old or <50 kg whounderwent twice-daily dosing. All patientshad sequential compression devices. VTEprophylaxis was administered startingeither preoperatively or the same day ofsurgery and continued throughouthospitalization. Prior to 2008, VTEprophylaxis was variable and providerdependent without any uniform protocol.VTE incidence was identified by ICD-9codes for deep vein thrombosis (DVT)
AWARDS PROGRAMABSTRACTS
Friday, March 9 at 9:00 AMSouthern Hemisphere I-III
A five-minute presentation by theprimary author is followed by a shortdiscussion period.
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES48
AWARDS PROGRAM ABSTRACTS

and pulmonary embolus (PE). Secondarybleeding complications related toanticoagulation were evaluated by CPTcode for postoperative epidural hematoma(EDH) requiring evacuation.Results: Prior to protocol initiation, 1002patients met inclusion criteria: 25 hadDVT (2.50%), 6 had PE (0.60%), 6 hadpostoperative EDH (0.60%). Afterprotocol initiation, 1071 patients metcriteria: 10 had DVT (0.93%), 5 had PE(0.47%), 4 had postoperative EDH(0.37%). This reduction in DVT wasstatistically significant (P = .006). Despiteearly aggressive prophylaxis, there was noincreased incidence of postoperativeEDH, and compared favorably topublished literature.Conclusion:At a high volume tertiarycenter, an aggressive protocol for earlyVTE prophylaxis after spine surgerydecreases VTE incidence withoutassociated increased morbidity.
OUTCOMES COMMITTEE AWARD120The Relevance of IntramedullaryHigh Signal Intensity andGadolinium (Gd-DTPA) Enhancementto the Clinical Outcome in CervicalCompressive MyelopathyJun-Jae Shin, Ji Hae Lee, Woo Ho Cho,Jon ParkIntroduction:We prospectivelyinvestigated whether high intramedullarysignal intensity (SI) and contrast(gadolinium-diethylene-triamine-pentaacetic acid [Gd-DTPA])enhancement in MRI are associated withpostoperative prognosis in cervicalcompressive myelopathy (CCM) patients.Additionally, we investigate the usefulnessof contrast-enhanced MRI in patients withcervical myelopathy.Methods: Seventy-four patients withventral cord compression underwentanterior cervical discectomy and fusion(ACDF) for CCM between March 2006and June 2009. The mean follow-upperiod was 39.7 months (range, 12.7-55.7months). The clinical outcomes weremeasured using Japanese OrthopedicAssociation (JOA) scores. Patients wereclassified into three groups based on theSI change in T2-weighted images (T2WI),T1-weighted images (T1WI), and contrast(Gd-DTPA) enhancement. Group Adisplayed normal intensity on both T2WIand T1WI, group B displayed nointramedullary signal intensityabnormalities on T1WI and high SI onT2WI, and group C displayed no
intramedullary SI abnormalities on T1WI,high SI on T2WI, and an enhancedcontrast(Gd-DTPA) image. By comparingthe preoperative and postoperative signalchange on T2WI, patients with high SIbefore surgery were classified into twogroups after the surgery: reversible group(those whose SI had decreased) andstationary group (those whose SI wasunchanged).Results: The respective postoperative JOAscores and recovery ratios were 16.2 ±0.8/82.4 ± 16.7% for group A, 14.6 ±2.5/69.1 ± 20.8% for group B, and 13.9 ±1.7/57.5 ± 14.0% for group C (P < 0.05).The mean recovery ratio of the reversiblegroup was 75.9 ± 14.3%, which was betterthan that of the stationary group (59.0 ±19.7%) (P <0.05).Conclusion:We found that intramedullarySI change is a poor prognostic factor andthe intramedullary contrast enhancementon preoperative MRI should be viewed asthe worst predictor of surgical outcomesin cervical myelopathy. The regression ofsignal changes in patients withintramedullary high SI before surgeryreflects improved neurological outcomesafter surgery. We consider contrastenhancement and postoperative MRI areuseful for identifying the prognosis ofpatients with poor neurological recovery.
200Acute Adrenal Insufficiency inCervical Spinal Cord InjuryEmil Antonio Pastrana Ramirez, Fanor Manuel Saavedra, Samuel Estronza-Ojeda, Gisela Murray,John David Rolston, Gloria E. Rodriguez-VegaIntroduction:Adequate adrenal response isfundamental for maintenance ofphysiological homeostasis in the setting oftrauma and severe illness. Patients withneurogenic shock are at risk of severeconsequences if adrenal insufficiency isnot rapidly identified and treated.Methods: The medical records of patientsolder than 18 years who were admitted tothe adult neurosurgery service at theUniversity District Hospital due toneurogenic shock following acute cervicalspinal cord injury from January 2004 toDecember 2009 were reviewedretrospectively.Results: One hundred and ninety-ninepatients were admitted with acute cervicalspinal cord injury. 37 patients met the pre-established criteria for neurogenic shock.The incidence of adrenal insufficiency(AI) in patients with neurogenic shockwas 22%. The average random cortisolwas 9.3 µg/dL in patients with AI vs. 29.2µg/dL in Non-AI. The presence of AI waspositively correlated with complicationsand an increase in the risk of intubation (P= 0.01 and P = 0.002). The 30-daymortality rate in patients with AI was 13%compared with the 3% in the Non-AIgroup (P = 0.39).Conclusion:Adrenal insufficiency is apoorly recognized complication inpatients with acute cervical spinal cordinjury and its aggressive treatment is ofutmost importance to avoid furtherneurological injury.
ORAL POSTER ABSTRACTSThursday, March 8
at 3:45 PMSaturday, March 10 at 7:00 AM and 11:00 AM
Southern Hemisphere I-IIIand Americas Seminar
Five-minute presentations by theprimary authors are followed by ashort discussion period. Thurdaysessions are concurrent.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 49
ORAL POSTER ABSTRACTS

201Radiographic and Clinical Outcomesof Posterior Column Osteotomies inSpinal Deformity Correction:Analysis of 128 PatientsIan G. Dorward, Lawrence Lenke, Geoffrey E. Stoker, Woojin Cho, Linda A. Koester, Brenda A. SidesIntroduction: Though posterior columnosteotomies (PCOs Smith-Petersen orPonté) are common, few studies haveevaluated their radiographic and clinicaloutcomes. We present the largest reportedseries of patients with PCOs for spinaldeformity correction.Methods: 128 consecutive adult andpediatric patients underwent PSF withPCOs (75 primary surgeries and 53revisions) with minimum 2-year follow-up. We excluded those with concomitantPSO, VCR, or anterior release/fusion atPCO levels.Results: 128 patients aged 37.6 ± 21 yearsunderwent 518 PCOs (mean 4.0 ± 2.2)with 14.4 ± 3 levels of instrumentation,with 3-year (range 2-6.8) mean follow-up.PCOs were used for kyphosis correctionin 49%, scoliosis correction at the apex ofa curve in 13%, and both in 38%.Kyphosis correction per PCO averaged8.8° ± 7.2, varying with patient age (10.2°for <21 vs. 7.7° for =21, P < 0.0001) andspinal region: TL 11.6° > L 9.4° > MT7.2° > PT 3.6°. Sagittal Cobb for PCOsegments decreased from 30° ± 30 to 8.6°± 22 (P < 0.0001). With PCOs at a curveapex, max coronal Cobb decreased from66° ± 21 to 31° ± 14 (P < 0.0001). EBLaveraged 1419 ± 887mL, correlating withgreater age (P < 0.0001) and moreinstrumented levels (P < 0.0001), but notnumber of PCOs (P = 0.32).Complications occurred in 31 (24.2%)patients, including 4 radiculopathies (noneattributable to PCOs), 5 implant failures,and 4 pseudarthroses (1 at a PCO level).Complications did not correlate withnumber of PCOs (P = 0.5). 6 patientsfailed an intraoperative wake-up test orlost motor evoked potentials (MEPs) dueto overcorrection with PCOs, but nopostoperative deficits occurred. ODIscores improved pre vs. postop (34.4 ± 17vs. 23.6 ± 18, P < 0.0001), as didnormalized SRS-30 scores (63.7 ± 13 vs.76.4 ± 15, P < 0.0001).Conclusion: PCO is a safe and effectivetechnique for posterior spinal deformitycorrection. The number of PCOs did notcorrelate with EBL or complications. Themain technical concern with PCOs wasovercorrection, but intraoperative MEPs
and wakeup tests prevented neurologicdeficits.
202Factors Influencing Two-yearHealthcare Costs in PatientsUndergoing Revision Lumbar FusionProcedures: A Guide to Where WeShould Target Our Cost and QualityImprovement InitiativesScott L. Parker, David Shau, Stephen Mendenhall, Matthew McGirtIntroduction: Failed back surgerysyndrome (FBSS) is technicallychallenging to treat and can be associatedwith tremendous healthcare resourceutilization and cost. There is minimal dataregarding specific factors that significantlycontribute to excessive cost of care.Therefore, we set out to identifyindependent risk factors predictive ofincreasing two-year healthcare costs afterrevision lumbar fusion procedures.Methods: One hundred fifty patientsundergoing revision neural decompressionand instrumented fusion for adjacentsegment disease (n = 50), pseudoarthrosis(n = 47), or same-level recurrent stenosis(n = 53) were included in this study.Patient demographics, co-morbidities, pre-operative health states, and peri-operativecomplications were collected andanalyzed. Two-year back-related medicalresource utilization and direct healthcarecosts were assessed. The independentassociation of all variables to increasingcost was assessed using multivariate linearregression analysis.Results: There was a wide range ($24,935-$63,769) in overall two-year costs forpatients undergoing revision lumbarfusion (mean: $32,915 ± 8,344), Figure 1.Pre-operative variables independentlyassociated with two-year direct healthcarecosts are shown in Table 1. There was a1.1 to 1.2-fold increase in cost for patientsin the greatest vs. lowest quartiles forthese variables, Table 2. Surgical siteinfection (SSI), return to the operatingroom, and spine-related hospital re-admission during the 90-day global healthperiod were independently associated withtwo-year cost, Table 1. Patients in thegreatest vs. lowest quartiles had a 1.7 to1.9-fold increase in cost for thesevariables, Table 2.Conclusion: Costs of revision lumbarfusion can vary widely between patients.While co-morbidities and pre-operativeseverity of disease states contribute to costof care, the primary drivers of excess costinclude peri-operative complications such
as surgical site infection, return to the OR,and re-admission during the global healthperiod. Measures focused on healthservice improvement will be mostsuccessful in reducing the cost of care forpatients undergoing revision lumbarfusion.
203WITHDRAWN
204Short-term ComplicationsAssociated with Surgery for High-grade Spondylolisthesis in Adultsand Pediatric Patients: A Reportfrom the Scoliosis Research SocietyMorbidity and Mortality DatabaseManish K. Kasliwal, Justin S. Smith,Christopher I. Shaffrey, Dwight Saulle,Lawrence Lenke, David W. Polly, Jr.,Christopher P. Ames, Joseph PerraIntroduction: Lack of high level evidencefavoring superiority of one surgicaltechnique over other makes it paramountto recognize the complications whichoften dictate the choice of approach formanagement of HGS. This is aretrospective review of 165 patients withHGS from the M&M index of the SRS toassess complications incidence andidentify factors associated with increasedcomplication rates following surgery forHGS.Methods:All cases of HGS from the SRSM&M database for the year 2007 werereviewed. The data was stratified into 2categories: pediatric (=18 years) andadults (>18 years). Complications wereidentified and analyzed based on gradeand etiology of spondylolisthesis, genderand revision surgery in both the groupsseparately. Occurrence of a newneurological deficit was further analyzedin relation to the grade ofspondylolisthesis, whether directdecompression was performed or not,revision surgery, reduction vs. in situfusion, osteotomy and use ofneuromonitoring.Results:A total of 165 cases of HGS werereported (88 pediatric and 77 adultpatients). There were 49 complications(29.6%) in 41 patients (24.8%) with nodifference in overall number ofcomplications in pediatric vs. adult group.(30% in each) Occurrence of newneurological deficit after surgery was themost common complication seen in 19(11.5 %) patients. (Table 1) Performanceof an osteotomy was associated withhigher chances of development of new
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES50
ORAL POSTER ABSTRACTS

neurological deficits in both adults andpediatric groups (P = 0.02 and 0.012respectively). Though most of the newneurological deficits improved overfollow-up, there was a 10% chance of adeficit being permanent.Conclusion:Awareness of incidence ofoverall complications with influence ofsurgical procedure as shown in this studycan help surgeons select the optimalapproach for HGS.
205Functional Outcome InstrumentsUsed for Cervical SpondyloticMyelopathy: Interscale Correlationand Prediction of Preference-basedQuality of LifeDmitriy Petrov, Robert G. Whitmore, Zoher Ghogawala, J. Sanford Schwartz,Sherman C. SteinIntroduction: Cervical myelopathy is adebilitating disease, greatly impacting thequality of life of the patient. We aim todetermine the correlation betweendifferent functional outcome measuresused in cervical spondylotic myelopathy(CSM) patient assessment and their abilityto predict preference-based quality of life.Methods:CSM patients from seven centersundergoing either anterior or posteriorsurgery were prospectively followed withfive different functional outcomemeasuresover one year. Correlations among scaleswere tested using the Spearman’s rankcorrelation test. The sensitivity andspecificity of each scale for predicting theglobal index of the EuroQol-5D (EQ-5D)was determined, and receiver operatingcharacteristic (ROC) analysis was used tocompare each scale’s ability todiscriminate quality of life (QOL).Results: 106 patients were initiallyenrolled, 103 were operated upon forcervical spondylotic myelopathy andfollowed for one year. Their ages rangedfrom 40 to 82 years (mean 61.9), and61.3% were male. Correlations among thevarious functional outcome instrumentswere all highly significant (P < 0.001),but the degree of correlation variedgreatly. Correlation between the EQ-5Dscale and the Nurick Scale was the least(Spearman’s rho 0.5539), correlation wasthe highest with the Oswestry NDI(Spearman’s rho 0.8306). The OswestryNDI also had the greatest ability todiscriminate favorable from adverse QOLcompared to the other outcomeinstruments (P = 0.023).Conclusion: Preference-based quality oflife instruments, such as the EQ-5D, are
important measures for studying spinaldisorders. Among the various commonlyused outcome instruments for CSM, theOswestry NDI is most predictive ofpreference-based QOL.
206The Fate of Type II OdontoidFractures After PosteriorAtlantoaxial Fusion: Where DoesHealing Occur?Michael Mumert, Marcus D. Mazur,Andrew T. Dailey, Meic H. Schmidt, Erica Fay BissonIntroduction: Odontoid fractures are themost common injury associated with theaxis and account for up to 1/5 of allfractures in the cervical spine. Andersonand D’Alonzo Type II odontoid fractures,the least stable of the three proposedtypes, often require surgical intervention.Range-of-motion sparing treatments are apriority at this level because of itssignificant impact on rotational motion.The goal of this study was to understandthe pattern of healing in patients who hadposterior C1-2 fusion for Type II odontoidfracture.Methods:We retrospectively identifiedpatients who had undergone posteriorscrew fixation and fusion surgery at theatlantoaxial complex for a Type IIodontoid fracture at the University of Utahbetween 1987 and 2011. Techniques forfusion included posterior bone graft witheither a transarticular screw, a C1 lateralmass/C2 pars construct, or a combinationof the two techniques. We collected dataon fusion patterns in patients who hadmore than three months’ follow-up.Results: Sixty-four patients were identifiedthat had posterior cervical instrumentationand fusion for Type II odontoid fractures.Eleven of these patients had fusionevaluation by computed tomography scanmore than three months postoperatively.Ten of eleven patients had fusion acrossthe fracture site. Two patients showedfusion across the C1/2 joint and nine at theposterior graft site. All eleven patients hadat least one site of fusion.Conclusion: Fusion across the fracture siteof a Type II odontoid fracture wasachieved in 91% of patients after internalstabilization via a posterior approach. Thiswould leave the possibility for theoreticalpreservation of rotational movement afterinstrumentation removal if no posteriorbone graft is placed. However, a subset ofpatients does not heal and would best betreated with a combination fixation andposterior fusion.
207Complications with the Use of BMP-2in Thoracolumbar and Lumbar SpineFusions: A Nine-Year InstitutionalAnalysisDaniel Lubelski, Kalil G. Abdullah,Michael P. Steinmetz, Matthew D. Alvin,Amy S. Nowacki, Srita Chakka, Edward C. Benzel, Thomas MrozIntroduction: Bone Morphogenetic Protein(BMP) has been increasingly used inspinal fusions over the past decade. Earlystudies reported that the use of BMP isassociated decreased operative time, bloodloss, and pain scores, as well as improvedfusion rates. Recent investigations haveshown BMP to be associated with variouscomplications occurring at incidencesranging from 0 to 100%.Methods: Using the institutional electronicmedical records, we retrospectivelyreviewed all patients between January2002 and September 2010 that underwentthoracolumbar and lumbar spine fusion.Patient demographic, operative, andoutcome/complication information wascollected.Results: Five hundred forty-seven patientcharts were reviewed with a mean follow-up time of 17 months. Mean age was 58years and mean BMI was 29. Forty-onepercent of patients had undergoneprevious spine surgery, 36% were takingantidepressants, 61% opioid analgesics,and 35% were current smokers. Eightpercent had PLIF operations, 32% TLIF,27% ALIF, and 29% PLF procedures. Noclinically relevant differences in thepatient characteristics and complicationswere identified between the varioussurgical approaches. Adverse outcomesincluded 6% urological complications, 9%wound infections, 10% pseudoarthrosis,19% radiculitis, 15% reoperation, and 1%death. Having undergone a previous spinesurgery was associated with increasedincidence of radiculitis, reoperation, andpseudoarthrosis (P = 0.005, P = 0.0008, P= 0.05, respectively). Being a currentsmoker at the time of operation wasassociated with increased rate ofradiculitis (P = 0.03).Conclusion: The use of BMP is associatedwith high incidence of radiculitis,pseudoarthrosis, and reoperation.Complications do not differ by surgicalapproach, but are more likely in currentsmokers and those with history of spinesurgery. Patients undergoing lumbar spinefusion with BMP have high incidence ofantidepressant use, current smokingstatus, and previous spine surgery and as
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 51
ORAL POSTER ABSTRACTS

such have relatively high complicationrates. Familiarity with possiblecomplications and improved surgicalpatient selection should be prerequisites toproceed with spine fusions with BMP.
208Laminoplasty vs. Laminectomy:Prospective Study in JapanTatsushi Inoue, Shigehiko Kuno, Motoi Shoda, Yuichi HiroseIntroduction: In 2003, Ratliff reported thatthere is no evidence suggesting forlaminoplasty to overcome laminectomy (JNeurosurg (Spine 3) vol. 98). In responseto his report, guideline committee forcervical spondylotic myelopathy byJapanese orthopedic associationconcluded that there had been no quality-certified evidence-based paper suggestingsignificant difference betweenlaminoplasty and laminectomy becauseevery study before was retrospective one.The objective of the present study is tocompare cervical laminectomy withlaminoplasty prospectively regardingneuroradiological findings.Methods: Between 2007 and 2010, 57cases of laminectomy (Group A, M:F =15:42, mean age 68.7) and 26 cases oflaminoplasty (Group B, M:F = 9:17, meanage 61.6) were done at our institution. Thetwo methods for operation were assignedby the day when the patients visited ourhospital without bias for selection.Outpatient clinic opened three times everyweek. One day was for ELAP, the othertwo days were for laminectomy whenposterior decompression was indicated forcervical spondylosis/disc herniation, canalstenosis and OPLL. In laminoplasty, carewas taken to preserve and reconstructposterior element including spinousprocess and supra- and interspinousligament. Radiological follow-upparameters (pre- and postoperativelordotic curve [C2-C7 angle, a] in flexion,neutral and extension positions) werecollected prospectively in a database.Results:Mean postop neutral a was 5.8°and 5.3° in group A and B respectively (P= 0.93). Mean postop flexion a was -16.0°and -0.1° (P = 0.11), mean a loss (preopneutral a postop neutral a) was 8.1° and -0.3° (P = 0.22), mean postop ROM was36.4° and 19.9° (P = 0.057) in group Aand B, respectively. Progressive kyphosisover -20° in postop neutral a was noted in3 cases (5.2%) of group A.Conclusion: There was no significantdifference between laminoplasty andlaminectomy in pre- and postop cervical
alignment, though adequate reconstructionof cervical posterior element followingposterior decompression may help toprevent progressive kyphosis.
209The Distribution of Body Mass as aSignificant Risk Factor for LumbarSpinal Fusion PostoperativeInfectionsAnkit Mehta, Ranjith Babu, Isaac Karikari,Betsy H.Grunch, Vijay Agarwal, Timothy Ryan Owens, Allan H. Friedman,Carlos A. Bagley, Oren N. GottfriedIntroduction: Surgical site infection (SSI)after lumbar spine surgery remains asignificant cause of morbidity. Theliterature demonstrates an increased riskof postoperative infections associated withobesity, diabetes, and multilevel surgeries.The purpose of this study was todetermine the role in body habitus andweight distribution on developing asurgical site infection.Methods:A retrospective review wasperformed on a consecutive cohort of 298adult patients who underwent lumbarspine surgeries between 2006 and 2008 atthe Duke University Medical Center.Previously identified risk factors (i.e.,number of levels, diabetes, body massindex) were collected, as well as thehorizontal distance from the lamina to theskin surface (measured at L4) andthickness of subcutaneous fat at thesurgical site.Results:Among the 298 patients, 24 (8%)had postoperative infections. Of thepreviously identified risk factors, numberof levels P = 0.0078) was found to besignificantly associated with infectionswhereas body mass index (P = 0.16) anddiabetes (P = 0.13) were found to not bestatistically significant. Obesity (BMI > =30) (P = 0.025), skin to lamina distance(P = 0.046) and thickness of thesubcutaneous fat (P = 0.035) were foundto be significant risk factors for SSI.Conclusion: Our findings suggest that inobese patients, the distribution of bodymass is more predictive of SSI than theabsolute BMI and deserves attention inpreoperative evaluation.
210Fractures of the Ankylosed Spine: ASingle Institution ExperienceBrian D. Milligan, Terry K. Schiefer,Colten D. Bracken, Jeffrey T. Jacob,William E. Krauss, Mark A. Pichelmann,Michelle J. ClarkeIntroduction:Vertebral fractures in the
setting of spinal ankylosis may occurfollowing relatively minor trauma and beassociated with significant neurologicmorbidity and/or mortality.Methods:We retrospectively reviewed 72fractures in 65 patients with either diffuseidiopathic skeletal hyperostosis (DISH,30%) or ankylosing spondylitis (AS, 70%)who presented between 1994 and 2010.We recorded demographics,comorbidities, and fracture/treatmentcharacteristics. Neurologic presentationand outcomes were categorized usingASIA grades3 and the modified RankinScale (mRS)1. We utilized univariateanalysis to identify risk factors forneurologic deterioration or poor outcome(mRS 4-6).Results:Most fractures (66%) occurredafter falls of standing height or less andinvolved the cervical (40%), thoracic(40%), and/or lumbosacral (20%) regions.3-column injuries2 were identified in83%. Presentation and diagnosis wereeach delayed by about 1 week in 47% and21% of patients, respectively. Mostfractures were extension (57%) and/ordistraction (71%) injuries. Median SLIC(subaxial cervical fractures)4 and TLIS(thoracolumbar fractures)5 scores were 5(IQR 4.5-7) and 6 (IQR 6-8), respectively.Treatment included operative fusion(67%), percutaneous instrumentation(18%) or external orthosis (32%, of whom55% required subsequent fusion).Neurologic deterioration to a completespinal cord injury (ASIA-A) occurred in 5patients (7%). The presence and severityof neurologic symptoms at presentation,but not age, obesity, polytrauma orfracture treatment choice was predictive ofpoor outcome at 1 year (or last follow-up,P < 0.001). Thirteen patients died withinone year of injury (18%).Conclusion: Spinal fractures in the settingof DISH or AS are frequent after low-energy trauma mechanisms and frequentlyresult in unstable fractures that often failnonoperative treatment. Neurologicdeterioration during the initialhospitalization is not uncommon andmortality within 1 year of the initial injuryis high. Treating physicians and patientsshould be aware that mortality and pooroutcomes might be more common than inthe general trauma population.
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES52
ORAL POSTER ABSTRACTS

211Cost per Quality-adjusted Life YearGained of Revision Lumbar Surgeryfor Adjacent Segment Disease,Pseudoarthrosis, and Same-levelRecurrent Stenosis: Defining theValue of Surgical InterventionScott L. Parker, David Shau, Stephen Mendenhall, Owoicho Adogwa,Joseph S. Cheng, Clinton J. Devin,Matthew McGirtIntroduction: Failed back surgerysyndrome (FBSS) is distressing to patientsand spinal surgeons. While there areseveral studies reporting mixed long-termoutcomes of surgical management ofFBSS, cost-effectiveness of surgery in thispopulation remains unclear. We set out toassess the cost-effectiveness of revisionsurgery for adjacent segment disease(ASD), pseudoarthrosis, and same-levelrecurrent stenosis over a two-year follow-up period.Methods: 150 patients undergoing revisionneural decompression and instrumentedfusion for ASD (n = 50), pseudoarthrosis(n = 47), or same-level recurrent stenosis(n = 53) were included. Two-year totalback-related medical resource utilization,missed work, and health-state values[quality adjusted life years (QALYs)]were assessed. Two-year resource use wasmultiplied by unit costs based onMedicare national allowable paymentamounts (direct cost), patient and care-giver work-day losses were multiplied bythe self-reported gross-of-tax wage rate(indirect cost). Total two-year cost perQALY gained after revision surgery wasassessed.Results: Baseline characteristics providedin Table 1. Pre-operative EQ-5D forpatients with ASD, pseudoarthrosis, andsame-level recurrent stenosis was 0.30 ±0.28, 0.37 ± 0.17, and 0.18 ± 0.22,respectively. Mean cumulative two-yearhealth-state gain for these 3 cohortsfollowing surgery was 0.76, 0.35, and0.84 QALYs, respectively, Figure 1.Mean±SD total (direct+indirect) two-yearcost of surgery following ASD,pseudoarthrosis, and same-level stenosiswas $47,846 ± 32,712, $41,631 ± $9,691,and $49,431 ± 7,583, respectively. Cost-components specified in Table 2. Revisionsurgery for ASD, pseudoarthrosis, andsame-level stenosis was associated withmean two-year cost per QALY gained of$62,955, $118,945, and $58,846.Conclusion: Revision fusion for FBSS wasassociated with significant improvementin quality of life at two years. Surgical
management of ASD and same-levelrecurrent stenosis were cost-effective at$62,955 and $58,846 per QALY gained,respectively. Surgery for pseudoarthrosiswas poorly cost-effective at $118,945 perQALY gained. Our results suggest thatrevision neural decompression and fusionfor FBSS is a valuable treatment option.
212Preoperative Zung Depression ScalePredicts Patient SatisfactionIndependent of Extent ofImprovement After Revision LumbarSurgeryScott L. Parker, Owoicho Adogwa, David Shau, Stephen Mendenhall, Matthew McGirtIntroduction: Patient satisfaction ratingsare increasingly used in healthcare as aproxy for quality and are becoming thefocal point for several qualityimprovement initiatives. Affectivedisorders, such as depression, have beenshown to influence patient reportedoutcomes and self-interpretation of healthstatus. We hypothesize that patientpsychiatric profiles influence reportedsatisfaction with care, independent ofsurgical effectiveness. We assessed thepredictive value of pre-operativedepression on patient satisfactionfollowing revision surgery for same-levelrecurrent stenosis.Methods: Fifty-three patients undergoingrevision neural decompression andinstrumented fusion for same-levelrecurrent stenosis-associated back and legpain were included. Pre-operative Zung-self reported depression score (ZDS),education status, co-morbidities, andpostoperative satisfaction with surgicalcare and outcome was assessed for allpatients. Baseline and two-year VAS-LP,VAS-BP, Oswestry Disability Index(ODI), SF-12 PCS and MCS, as well ashealth-state utility [EuroQol (EQ-5D)]were assessed. Factors associated withpatient satisfaction after surgery wasassessed via multivariate logisticregression analysis.Results: Baseline characteristics presentedin Table 1. Two years after surgery, asignificant improvement was reported inall outcome measures, Table 2.Independent of post-operativeimprovement in pain and disability(surgical effectiveness), increasing pre-operative Zung depression score wassignificantly associated with patientdissatisfaction two-years after revisionlumbar surgery (OR=0.67[CI: 0.38-0.87],
P < 0.001), Table 3. Patients in bottomquartile (least depressed) vs. patients intop quartile (most depressed) of pre-operative Zung scores reported greatersatisfaction with surgical outcome andoverall care experience (94% vs. 6%).Patients with higher levels of education(college graduate or higher) also reportedgreater satisfaction levels (95% vs. 33%)following surgery, Figure 1.Conclusion: Our study suggests thatindependent of surgical effectiveness, theextent of pre-operative depressioninfluence reported patient satisfaction afterrevision lumbar surgery. Qualityimprovement initiatives using patientsatisfaction as a proxy for quality shouldaccount for patients’ baseline depressionas potential confounders.
213Extent of Preoperative DepressionPredicts Outcome After RevisionLumbar Surgery for AdjacentSegment Disease, RecurrentStenosis, and PseudoarthrosisScott L. Parker, David Shau, Stephen Mendenhall, Owoicho Adogwa,Clinton J. Devin, Matthew McGirtIntroduction: Revision surgery for failedback surgery syndrome is technicallychallenging and has been reported to yieldunpredictable outcomes. Recently,affective disorders, such as depression andanxiety, have been considered potentialpredictors of surgical outcomes acrossmany disease states of chronic pain. Thereremains a paucity of studies assessing thepredictive value of baseline depression onoutcomes in the setting of revision spinesurgery. We assessed the predictive valueof pre-operative depression on two-yearpost-operative outcome.Methods: 150 patients undergoing revisionneural decompression and instrumentedfusion for adjacent segment disease (ASD,n = 50), pseudoarthrosis (n = 47), orsame-level recurrent stenosis (n = 53)were included. Pre-operative Zung-selfreported depression score (ZDS) wasassessed for all patients. Pre-operative andtwo-year post-operative back and leg pain(VAS-LP, VAS-BP) and OswestryDisability Index (ODI) were assessed.Association between pre-operative Zungdepression score and two-yearimprovement in disability was assessedvia multivariate regression analysis.Results: Baseline characteristics presentedin Table 1. All patient-reported outcomesassessed were significantly improved attwo-years post-operatively for all 3
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 53
ORAL POSTER ABSTRACTS

cohorts, Table 2. Independent of age,BMI, symptom duration, smoking, co-morbidities, and level of pre-operativepain and disability, increasing pre-operative Zung depression score wassignificantly associated with less two-yearimprovement in disability (ODI) afterrevision surgery for ASD, pseudoarthrosis,and recurrent stenosis, Table 3. Patients inthe top quartile (most depressed) vs.bottom quartile (least depressed) of pre-operative Zung scores experienced 4-foldless mean improvement in ODI two-yearsafter surgery for ASD (P = 0.001), two-fold less mean improvement in ODI forpseudoarthrosis (P = 0.001), and 1.8-foldless mean improvement in ODI for same-level recurrent stenosis (P = 0.001),Figure 1.Conclusion: Extent of pre-operativedepression is an independent predictor offunctional outcome after revision lumbarsurgery for ASD, pseudoarthrosis, andrecurrent stenosis. Future comparativeeffectiveness studies assessing outcomesafter revision lumbar surgery shouldaccount for depression as a potentialconfounder. Zung depressionquestionnaire may help risk stratifypatients presenting for revision lumbarsurgery.
214A Novel Animal Model of CervicalSpondylotic Myelopathy: AnOpportunity to Identify NewTherapeutic TargetsSpyridon Karadimas, Eun Su Moon,Kajana Satkunendrarajah, Michael G. FehlingsIntroduction: In order to validate potentialneuroprotective and neuroregenerativestrategies for cervical spondyloticmyelopathy (CSM), we have developed anovel translationally relevant rat model ofCSM.Methods: Following posterior exposure ofthe cervical spine, the ligamentum flavumis opened at C5-6, C6-7 and progressivecompression (over 10 weeks) wasachieved by introducing a piece ofaromatic polyether with absorbantproperties under the C6 lamina in 10Sprague-Dawley rats. Sham operation wasperformed on 8 animals (controls). Theextent of compression was evaluated usingMRI. Gait patterns were evaluated usingthe automated gait analysis system.Demyelination was assessed by H-E andLuxol Fast. The loss of interneuronal cellsat the site of compression and at thelumbosacral enlargement were measured
by En1(+) and Chx10 (+)immunohistochemistry. Moreover,retrograde labelling of the longdescending propriospinal tract wasperformed by injecting fluorogoldbilaterally at the lumbosacral enlargement(L2-L5). At 10 weeks, the animals weresubjected to in vivo somatosensory andmotor evoked potential recordings (SSEPsand MEPs). ANOVAs were used for thestatistical analysis.Results:MRI quantification at 10 weeksrevealed 50.2% ± 4.8 compression ratio inthe compression group. There was astatistically significant decrease in stridelength, swing speed. Furthermore,statistically significant increases wereobserved in running time, stance phase,four-limb % support, number of steps andbase of support. The normalized graymatter area at the compression epicentrewas decreased compared to controls (5.15± 0.25 vs. 32.04 ± 0.17). Moreover, thenormalized glial scar tissue area at thecompression epicentre was 54.2 ± 1.33.The chronic compression led to decreasesin both SSEP and MEP peak amplitudesand to a decrease in axonal conductioncompared.Conclusion: This model reproduces theneurobehavioural abnormalities, gaitdeficits and the neuropathological featuresof human CSM and hence has thepotential to facilitate discovery of novelclinical translational therapeutic targets.
215Current Practices for IntraoperativeLocalization of Lumbar Spinal Level:A Survey of the Joint Section onDisorders of the Spine andPeripheral NervesMichael W. Groff, Joshua E. Heller, Eric A. Potts, Praveen V. Mummaneni,Christopher I. Shaffrey, Justin S. SmithIntroduction:Methods used by surgeonsfor localization of spinal level have notbeen well studied or standardized. Theauthors surveyed the membership of theJoint Section of Spinal Disorders andPeripheral Nerve Diseases (Spine Section)to better understand current practices forintraoperative localization of lumbarspinal levels.Methods: The Spine Section developed asurvey on single-level lumbar spinedecompression surgery, includingquestions regarding methods to localizethe spinal level. Invitations to completethe web-based survey were sent to allSpine Section members. Respondentswere assured of confidentiality.
Results: There were 569 responses from1,045 requests (54%). Most surgeonseither routinely (74%) or sometimes(11%) obtain preoperative x-ray imagingbefore incision. Approximately one half(56%) of those obtaining preoperativeimaging for localization do so with aradiopaque marker inserted through theskin. Others use a radiopaque marker atthe patient’s side (16%), overlying theplanned incision (14%), or depressed intothe patient’s back without violating theskin (19%). The majority of surgeonsindicated that post-incision imaging forlocalization is obtained either routinelyprior to bone removal (73%) or mostfrequently prior to bone removal butoccasionally after (16%). The mostcommon technique for such imaging wasto place a Penfield #4 or a similarinstrument beneath the lamina (42%) (seefigure). Others use a towel clamp orsimilar instrument attached to a spinousprocess (10%) or place a Penfield #4 orsimilar instrument in the midportion of theincision but not beneath the lamina (10%).The remaining surgeons use acombination of the above or use othermethods.Conclusion: Survey of the Spine Sectionmembership demonstrates that there issubstantial heterogeneity in approachesused to localize operative levels in thelumbar spine. Development ofstandardized approaches for levelconfirmation could facilitate a multi-institutional effort to further investigateoptimal methods for level localization.
216Rates and Causes of MortalityAssociated with Spine Surgery Basedon 108,419 Procedures: A Review ofthe Scoliosis Research SocietyMorbidity and Mortality DatabaseJustin S. Smith, Dwight Saulle, Christopher P. Ames, Lawrence Lenke,Steven D. Glassman, Paul A. Broadstone,David W. Polly, Jr., Christopher I. ShaffreyIntroduction: Despite the best of care, allsurgical procedures have inherent risks ofcomplications, including mortality.Defining these risks is important forpatient counseling and qualityimprovement. The objectives of this studywere to assess rates and causes ofmortality associated with spine surgerybased on a large prospectively collected,multicenter database.Methods: The Scoliosis Research SocietyMorbidity and Mortality database wasqueried for spinal surgery cases
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES54
ORAL POSTER ABSTRACTS

complicated by death from 2004-2007,including pediatric (<21 years) and adult(>21 years) patients. Deaths occurringwithin 60 days and complications within60 days of surgery that resulted in deathwere assessed.Results: 197 mortalities were reportedamong 108,419 cases (1.82 deaths/1,000cases). Based on age (provided for107,517 cases), rates of death/1,000 casesfor adult (n = 82,082) and pediatricpatients (n = 25,432) were 1.99 and 1.26,respectively. Based on primary diagnosis(provided for 107,996 cases), rates ofdeath/1,000 cases were: 0.93 fordegenerative (n = 47,393), 1.82 forscoliosis (n = 26,421), 0.88 forspondylolisthesis (n = 11,421), 5.67 forfracture (n = 6,706), 4.44 for kyphosis (n= 3,600), and 3.29 for other (n = 12,455).The most common causes of mortalityincluded: respiratory/pulmonary (n = 83,including respiratory failure [n = 23],presumed/confirmed pulmonaryembolism [n = 20], and pneumonia [n =9]), cardiac (n = 41, including myocardialinfarction [n = 16] and cardiac arrest [n =13]), sepsis (n = 35), stroke (n = 15), andintraoperative blood loss (n = 8) (Table).Death occurred prior to hospital dischargefor 109 (79%) of 138 deaths for whichthis information was reported. Thespecific post-operative day (POD) ofdeath relative to surgery was reported for94 (48%) cases, and included POD#0 (n =23), POD#1-3 (n = 17), POD#4-14 (n =30), and POD#>14 (n = 24).Conclusion: This study provides rates andcauses of mortality associated with spinesurgery for a broad range of diagnoses andincludes assessments for adult and pediatricpatients. These findings may provevaluable for patient counseling and effortsto improve the safety of patient care.
217What Are the Factors That MayPredict Regain of IndependentWalking After Surgery for Patientswith Advanced Cervical SpondyloticMyelopathy?Ahmed Mustafa Alaqeel, Amro Al Habib,Abdulrahman Aldakkan, Fahad AlbadrIntroduction: Cervical spondyloticmyelopathy (CSM) is a common spinedisease that can be associated withdevastating consequences, one of which isimpairment of walking. Factors that maypredict the ability of walking followingsurgery are not well defined. Studyingpotential predictors of independentwalking in patients with advanced CSM
was our goal. This information isimportant in counseling patients and theirfamilies and planning appropriateresources for rehabilitation.Methods: Retrospective review of CSMpatients with inability to walkindependently (Nurick 4 and 5) whounderwent surgery from 2003-2010. Aneuroradiologist who was blinded to theclinical status reviewed all MRI studies.38% of patients were contacted to updatetheir follow-up status.Results: Forty-eight patients were included(males 83%) with a mean follow-up of24.7 months. Patients with a betterpreoperative neurological status had asignificantly better chance of walkingafter surgery (83.33% for Nurick4 vs.33.33% for Nurick5, P < 0.01).Independent walking after surgery wasless likely in patients with longer signalchange on T2WI MRI study (20.5 mm vs.7.5 mm, P < 0.001) as well as whenstratified to Nurick4 (12.8 mm Vs 7.3mm, P<0.05) and Nurick5 (22.4 mm vs.8.1 mm, P = 0.0001). Additionally,narrow spinal canal width was a predictorfor independent walking (6.3 mm vs. 7.5mm, P < 0.05) as well as for Nurick4alone (4.88 mm vs. 7.53 mm, P < 0.05).Other factors including age, sex, durationof difficulty walking, type of surgicalapproach and the presence of co-morbidities did not predict independentwalking regardless of preoperativeneurological status.Conclusion: In patients with advancedCSM, the better the baseline walking, theless the signal change on MRI, and thewider the spinal canal the better theirability to walk following surgery. Surgeryshould be recommended before patientsprogress into advanced stage whererecovery is less and the need for resourcesis large.
218Intradiscal Injection of Simvastatinfor Disc Regeneration in a Rat Modelof Degenerative Disc DiseaseKhoi Duc Than, Shayan Rahman, Kwaku A. Kyere, Lin Wang, Tracey T. Than,Adam Khan, Yoon-Shin Park, Ki Park,Victor C. Yang, Frank La Marca, Paul Park,Huina Zhang, Chia-Ying LinIntroduction: Degenerative disc disease(DDD) is a common etiology of backpain, and conservative managementoptions are limited. Bone morphogeneticprotein-2 (BMP-2) plays an important rolein the physiology of the intervertebral disc(IVD), and the drug simvastatin is known
to up-regulate the expression of BMP-2.We hypothesized that injection ofsimvastatin into degenerated rat IVDsreverses the process of disc degeneration.Methods: Disc injury was induced in 224rats by needle puncture. After 6 weeks,discs were treated with 2 microliters of:simvastatin (5 mg/ml) in a collagen-basedhydrogel, simvastatin (15 mg/ml) inhydrogel or saline, saline only, orhydrogel only. Rats were sacrificed after2, 4, 8, 12, and 24 weeks. Outcomesmeasures were radiologic, histologic, orgenetic. Magnetic resonance imaging(MRI) was used to calculate the MRIindex. Discs were graded histologicallyaccording to the appearance of theannulus fibrosus (AF), border between theAF and nucleus pulposus (NP), cellularityof the NP, and matrix of the NP. Real-timepolymerase chain reaction was used toquantify gene expression of BMP-2,collagen types I and II, aggrecan, matrixmetalloproteinases-3 and -13, andaggrecan.Results: Radiographic data suggested thatdiscs treated with simvastatin at 5 mg/mlin hydrogel maintained a normal MRIindex at 2-, 4-, and 8-week time points,whereas other treatment groups did not.Histologic data revealed that this groupalso had the best microscopic appearanceat 2 weeks, although this was neitherstatistically significant nor sustained.Genetic data is pending.Conclusion: In a rat model of DDD,simvastatin injected intradiscally in ahydrogel carrier at 5 mg/ml resulted in anormal appearance on MRI through 8weeks. Further data is pending.Simvastatin may result in regeneration ofinjured IVDs via up-regulation of BMP-2,although further work is necessary toidentify the ideal delivery vehicle and dose.
219Impact of Treatment Complicationson Outcomes in Geriatric Patientswith Type II Odontoid Fracture:Results from the AOSpine NorthAmerica Multi-Center GOFProspective StudyMichael G. Fehlings, Alexander R. Vaccaro, Branko Kopjar,Christopher I. Shaffrey, Jens Chapman,Paul M. Arnold, Ziya L. Gokaslan, Darrel S. Brodke, John France, Sangwook Yoon, Mark B. Dekutoski,Christopher Bono, Rick SassoIntroduction: Purpose of this study was toassess the impact of treatmentcomplications on outcomes in geriatric
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 55
ORAL POSTER ABSTRACTS

patients with type II odontoid fractures.Methods: 159 subjects enrolled 65 yearsand older with a Type II odontoid fracturein a prospective multi-center cohort studyat 13 sites in North America. Treatmentcomplications were prospectivelyfollowed using a list of 19 anticipatedcomplications associated with thetreatment of odontoid fractures.Complications not on the list were alsorecorded. Reported events wereadjudicated by a study Adverse EventCommittee. The events were categorizedas treatment complications and treatment-unrelated events.Results: 64.2% of patients were treatedoperatively and 35.8% nonoperatively. 89treatment-related complications reportedamong the 159 subjects. There was atendency towards higher proportion ofsubjects with any complication in thenonoperative cohort compared to theoperative cohort (36.8% and 29.4%,respectively, P = 0.1661). Commoncomplications were dysphagia (11 cases,10.8% in the surgical group and 3 cases,5.3% in the nonoperative group),pneumonia (4 cases, 3.9% in the operativeand 2 cases, 3.5% in the nonoperativegroup), acute airway compromise (5 cases(4.9%) in the operative and 4 cases (7.0%)in the nonoperative group). Nonunionsoccurred in 12 subjects (21.1%) in thenonoperative arm compared with 5 casesin the operative arm (4.9%) (Fisher ExactTest P = .0026). 3 cases of treatment-related deaths, 2 (1.96%) in the operativecohort and 1 case (1.75%) in thenonoperatively group. Analysis iscurrently underway to evaluate the impactof complications on SF-36 and NeckDisability Index and will be available atthe time of the congress.Conclusion: Treatment complications arecommon in geriatric patients with type IIodontoid fractures. There is no evidencethat operative treatment is associated withan increased risk of complications.
220Should Routine ScreeningUltrasonography for Deep VeinThrombosis Be Used inAsymptomatic Patients DuringHospitalization for Elective SpineSurgery? An Analysis and Review of587 Consecutive PatientsD. Kojo Hamilton, Akil Patel, Charles A. SansurIntroduction: Deep Vein Thrombosis(DVT) is a well known complication ofhospitalized neurosurgical patients. The
value of screening ultrasonography forearlier detection of DVT in spinal patientsand the subsequent prevention ofpulmonary complications remains unclear.This is especially true when evaluatingDVT in asymptomatic patientsundergoing spine surgery, who thoughnon plegic or paretic, but due to painand/or deconditioning, have not been verymobile preoperatively. The goal of thisstudy was to determine possible patterns,incidence and risk factors in acquiringDVT in asymptyomatic hospitalized spinesurgery patients who underwent, routineon admission, and weekly, ultrasoundscreening for DVT.Methods:A retrospective review of 587consecutive adult spinal patients whounderwent admission and weeklyultrasound screening at a universityhospital center, over 1 year, wasconducted. All patients received standardmechanical and chemical prophylaxis. Wereviewed patient demographics and highrisk groups.Results: There was a 1.9% overallincidence of DVT in this population.Patients undergoing complex spinalsurgery had a higher subgroup incidencewith further pulmonary complications.Overall, 91% were diagnosed with a DVTwithin 7 days of hospital stay, 0%diagnosed within 8-14 days, and the restwere (9%) diagnosed after 14 days (p-value <0.05).Conclusion: The effectiveness of routineultrasonography screening for DVT maybe most maximized if screening includesan initial admission and immediate post-op study in particularly high risk patients,followed by studies on only symptomaticpatients.
221The Impact of Different SurgicalStrategies in Achieving SatisfactoryPost-Operative Sagittal AlignmentJustin S. Smith, Christopher P. Ames,Virginie Lafage, Frank Schwab, Richard A. Hostin, Robert Hart, Vedat Deviren, Behrooz A. Akbarnia, Jason Demakakos, Khaled Kebaish,Douglas C. Burton, Shay Bess,Christopher I. ShaffreyIntroduction:Adult spinal deformity(ASD) presents a wide range of deformityand clinical patterns. When non-operativecare fails, surgical realignment usingosteotomies is often pursued to achieveimproved alignment and function. Reportshave identified key radiographic spino-pelvic parameters associated with
outcomes, including Sagittal Vertical Axis(SVA,<50mm), Pelvic Tilt (PT,<20°) andPelvic Incidence-Lumbar Lordosis (PI-LL, >10°). While objectives of correctionhave been previously described, differentmethods to reach them have not beenreported. This study evaluated if differentstrategies for realignment can lead tosatisfactory post-operative radiographicsagittal alignment.Methods:A multicenter, retrospectiveradiographic analysis of 77 consecutivelyenrolled ASD patients, who underwentpedicle subtraction osteotomy (PSO) andfusion at three different sites. Baseline andpost-operative coronal and lateral full-length radiographic data were obtained.Only patients that underwent a lumbarPSO with a postoperative SVA<50mmwere included in this study. Thispopulation was analyzed for pre-operativedifferences, surgical parameters (degreeand level of PSO resection, and numbersof levels fused) and changes in post-operative radiographic parameters.Results: There were no significantdifferences in terms of pre-operativeradiographic parameters, and in terms ofprimary and revision patients. For thesurgical procedures, site 3 performedlarger PSO resections, 31° vs. 20°,exhibited an increase in thoracic kyphosis(TK) and used shorter fusions than theother sites (UIV=T9 vs. T5). The patientsfrom site 3 were also 10 years older. Therewas no difference in terms of LL changebeyond the PSO resection.Conclusion: Different surgical strategiescan lead to a satisfactory SVA. Onestrategy employed a smaller PSOresection with conservation of TK and ahigher UIV. Another strategy used a largerPSO resection and a shorter fusion, with asignificant increase in TK. Long-termanalysis will be performed to investigatethe impact of different strategies onincidence of proximal TK.
222How the Assessment of Pelvic Tilt,Pelvic Incidence/Lumbar LordosisMismatch and Sagittal Vertical AxisPredicts Disability in Adult SpinalDeformity: A Prospective AnalysisJustin S. Smith, Christopher P. Ames, Frank Schwab, Shay Bess, Benjamin Blondel, Richard A. Hostin,Oheneba Boachie-Adjei, Douglas C. Burton, Behrooz A. Akbarnia,Gregory Mundis, Khaled Kebaish, Robert Hart, Virginie Lafage, Christopher I. Shaffrey
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES56
ORAL POSTER ABSTRACTS

Introduction: Sagittal spinal malalignment(SSM) is commonly defined by increasedsagittal vertical axis (SVA), however, SVAalone may underestimate the severity ofSSM. Spino-pelvic parameters provide amore complete assessment of SSM. Littledata has correlated spino-pelvicparameters with disability. Purpose:evaluate correlations between sagittalspino-pelvic parameters and health relatedquality of life (HRQOL) scores.Methods: Demographic, radiographic, andHRQOL data were obtained from patientsconsecutively enrolled into a multi-center,prospective study evaluating operative(OP) vs. nonoperative (NON) treatmentfor adult spinal deformity (ASD).Inclusion criteria: age >18 years andradiographic diagnosis of ASD (scoliosis>20°, or SVA > 5cm, or pelvic tilt > 25°,or thoracic kyphosis > 60°). Radiographicevaluation: frontal and lateral spino-pelvicmeasurements. HRQOL questionnaires:Oswestry Disability Index (ODI),Scoliosis Research Society Questionnaire(SRS-22r). Radiographic parametersdemonstrating highest correlation withHRQOL values were evaluated todetermine a disability threshold ofODI=40.Results: 492 consecutive ASD patients(mean age 51.9 years, SD 16.8) wereenrolled. Patients treated OP (n = 178)were older (55 vs. 50.1 years, P < 0.05),had greater SVA (5.5 vs. 1.7cm, P <0.05), greater pelvic tilt (PT, 22° vs. 11°, P< 0.05) and greater pelvic incidence/lumbar lordosis mismatch (PI-LL, 12.2 vs.4.3, P < 0.05) than NON (n = 314). OPdemonstrated greater disability on allHRQOL measures compared to NON(ODI =41.4 vs. 23.9, P < 0.05, SRS total= 2.9 vs. 3.5, P < 0.05). Pearson analysisdemonstrated PT, SVA, and PI-LLcorrelated most strongly with disabilityfor both OP and NON patients (P <0.001). Linear regression modelsdemonstrated threshold radiographicspino-pelvic parameters for ODI = 40included: PT = 22° (r = 0.38), SVA = 46mm (r = 0.47), PI-LL = 11 (r = 0.45).Conclusion: SSM is a disabling condition.Prospective analysis of consecutivelyenrolled ASD patients demonstrated PTand PI-LL combined with SVA predictpatient disability and provide a guide forpatient assessment. Threshold values forsevere disability included: PT = 22°, SVA= 46mm, and PI-LL = 11°.
223Correction of Sagittal MalalignmentFollowing Pedicle SubtractionOsteotomy Improves CervicalLordosisJustin S. Smith, Christopher P. Ames,Virginie Lafage, Eric Klineberg, Frank Schwab, Gregory Mundis, Robert Hart, Shay Bess, Richard A. Hostin,Douglas C. Burton, Munish Gupta, Vedat Deviren, Christopher I. ShaffreyIntroduction: Numerous methods exist thatpredict spinal alignment following pediclesubtraction osteotomy (PSO). Alignmentwithin fused spinal segments iscontrollable by the surgeon, however,alignment changes in segments outside thefusion (reciprocal changes) areunpredictable and can negatively impactpostoperative alignment. Reciprocalchanges have been reported for thethoracic and lumbar spine. Cervicalreciprocal changes have not been defined.Methods:Adult spinal deformity (ASD)patients treated with PSO for sagittalspinal malalignment (SSM) wereevaluated using a multicenter PSOdatabase. Inclusion criteria: age >18 years,preoperative sagittal vertical axis (SVA)>50mm, cervical lordosis (CL, C2-C7Cobb) >15°. Radiographic measuresincluded regional and global spino-pelvicparameters. Regional measures of spinalinclination (cervical, thoracic, lumbar)were based on best-fit linearapproximation of the vertebral bodycentroids.Results: 29 patients treated with 29 PSOs(26 lumbar, 3 thoracic) met inclusioncriteria. PSO levels ranged from T7-L5(most common level = L3, n = 12). Meancorrection at PSO site was 26.5°, meanSVA improved from 134mm to 50mm (P< 0.001). CL decreased (29.1° to 21.4°, P< 0.001) and thoracic inclination (TI)decreased (23.7° to 11.0°, P < 0.001)following PSO. Cervical inclinationremained unchanged (preoperative =13.3°, postoperative = 14.3°, P = 0.554).T1 slope decreased following PSO (-36.9°to -31.8°, P = 0.006). Pearson correlationanalysis demonstrated strong correlationbetween postoperative changes in SVAand TI (r = 0.82, P < 0.001) and moderatecorrelation between postoperative changesin TI and cervical lordosis (r = 0.39, P =0.042). Postoperative change in CL didnot correlate with change in SVA (r =0.18, P = 0.342).Conclusion: Cervical hyperlordosis is acompensatory mechanism utilized bypatients with SSM to maintain horizontal
gaze. SSM correction following PSOgenerates spontaneous decrease andrelaxation of CL Favorable reciprocalchanges in cervical alignment followingPSO correlated with change in TI. TIalignment changes following PSOcorrelated strongly with SVA.
224Pedicle Subtraction Osteotomy withExtension of Fusion to the Pelvis:Does Anterior Interbody Support atL5-S1 Improve Sagittal and PelvicParameters?Justin S. Smith, Christopher P. Ames,Munish Gupta, Eric Klineberg, Virginie Lafage, Shay Bess, Frank Schwab,Oheneba Boachie-Adjei, Khaled Kebaish,Kirkham Wood, Behrooz A. Akbarnia,Gregory Mundis, Michael F. O’Brien,Richard A. Hostin, Christopher I. ShaffreyIntroduction: Lumbar pedicle subtractionosteotomy (LPSO) improves lumbarlordosis (LL), sagittal vertical axis (SVA),and spino-pelvic alignment (SPA).Reports have indicated that interbodyfusion at the L5-S1 improves arthrodesisrates at the lumbosacral junction, however,the contribution of L5-S1 interbodyprocedure toward sagittal alignmentcorrection when performing LPSO isunknown.Methods:Multi-center, retrospective,radiographic analysis of adult spinaldeformity (ASD) patients undergoingLPSO with fusion to the sacro-pelvis forsagittal spinal malalignment (SSM) usinga prospective collected database. Inclusioncriteria: age >18 years, pre andpostoperative spine radiographspermitting spino-pelvic parametermeasurement. Exclusion criteria: post-traumatic, infectious, neuromuscular ortumor associated spinal deformities.Patients evaluated according to type ofinterbody fusion performed at L5-S1(anterior approach= ALIF, posteriorapproach=T/PLIF, no interbody= NONE).ALIF patients divided into timing of theALIF procedure: prior to (ALIFpre) orafter (ALIFpost) the LPSO procedure.Radiographic analysis included coronaland sagittal spino-pelvic parameters anddegree of focal PSO correction.Results: 105 patients were treated withLPSO with fusion to the sacro-pelvis, ofwhich 77 patients met inclusion criteria.Interbody procedures included: NONE, n= 32, T/PLIF, n = 15, ALIFpre, n = 19,ALIFpost, n = 11. Mean preoperativeradiographic parameters, correction of andpostoperative values for SVA, L5-S1
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 57
ORAL POSTER ABSTRACTS

angle, lumbar lordosis and PSO anglewere similar for all treatment groups(ANOVA<0.05). T/PILF had greaterpostoperative pelvic tilt (PT) thanALIFpost (29.4° vs. 17.1°and P = 0.014),however PT correction was similar for allgroups.Conclusion:Anterior interbody graft at L5-S1 has been reported to enhance fusionrates at the lumbosacral junction despitehigher reported complication rates. Therewas, however, no added benefit of ALIFvs. TLIF with respect to sagittal SPAcorrection when performing LPSO andfusion to the sacro-pelvis. Further researchis needed to evaluate long-term outcomesto determine the ideal interbody approachat L5-S1 when performing LPSO.
225Spinal Epidural Abscess: ClinicalFeatures and Surgical OutcomesAnubhav Gautam Amin, George Austin Crabill, Gustavo Pradilla,Amit Jain, Michael Lim, Daniele Rigamonti, Wesley HsuIntroduction:We reviewed our institution’sexperience with spinal epidural abscess(SEA) to assess the clinical presentationand surgical outcomes of SEA.Methods:Medical records were reviewedfor 42 patients who were admitted with adiagnosis of SEA and underwent surgicaldecompression at the Johns HopkinsHospital between 1997 and 2009.Results: The median patient age was 53(range, 39-82). Thirty-three (79%)patients were male. The most prevalentcomorbidities were: diabetes (18, 43%),IV drug use (15, 36%), and obesity (10,24%). Eleven (26%) patients had previousspine surgery. Three (7%) patients wereon dialysis. Only two (5%) patients hadno identifiable risk factor or etiology. Themost prevalent presenting symptomswere: back pain (40, 95%), motor deficit(30, 71%), fever (14, 33%), urinary/bowelincontinence (15, 36%), and sensorydeficit (13, 31%). The SEA was located:14 (33%) cervical, 17 (40%) thoracic, 15(36%) lumbar, and 1 (2%) sacral. SEAwas located anteriorly in 27 (64%) cases,posteriorly in 14 (33%) cases, andcircumferential in 1 (2%) case. Associatedvertebral osteomyelitis and discitis werefound in 29 (69%) and 25 (60%) cases,respectively. All patients underwentsurgical evacuation and decompression.Instrumentation was used in 29 (69%)patients. Motor outcomes improved in80% of patients. 45% of patients wereable to ambulate independently and 36%
of patients were able to ambulate withassistance. 14% of patients had prolongedurinary incontinence. There were 5 (12%)cases of recurrent abscess formation thatrequired subsequent surgical intervention.There were no cases of death secondary toabscess formation or surgical intervention.There was no significant difference inimprovement of motor symptoms foranterior vs. posterior location of SEA.There was no significant difference inincidence of SEA recurrence forinstrumentation vs. non-instrumentation.Conclusion: Surgical evacuation andinstrumentation for spinal epiduralabscess can result in symptomaticrecovery with minimal recurrence ormorbidity. Spontaneous epidural abscessrequiring surgical intervention in patientswithout an identifiable risk factor oretiology was rare in this series.
226Chondroitinase ABC Treatment andModest Exposure to IntermittentHypoxia RestoresHemidiaphragmatic Activity AfterCervical Spinal Cord InjuryWarren J. Alilain, Jerry Silver, Megan ClarkIntroduction:Most spinal cord injuries(SCI) occur at the cervical level. This isdevastating because the phrenic motorneurons, which innervate the diaphragm,are located at this level. As a result, thoseafflicted with a cervical SCI usually havecomplications in breathing and can bedependent on a mechanical ventilator inorder to survive. To study thesecomplications and ways to restorerespiratory motor activity, our laboratoryutilizes the lateral C2 hemisection (C2H)model of SCI. C2H severs the bulbospinalinputs to the phrenic nucleus andparalyses the ipsilateral hemidiaphragmwhile sparing the crossed phrenicpathway, which serves as a potentialanatomical substratum for respiratoryplasticity. Following C2H, there is adramatic upregulation of the chondroitinsulfate proteoglycan (CSPG) containingperineuronal net (PNN) around theipsilateral phrenic motor neurons. CSPGsand the PNN severely inhibit plasticityand axonal regeneration, and thereby themeans to restore function. ChondroitinaseABC (ChABC) can digest these inhibitorymatrix molecules and we have shown thatwith enzyme administration alone, there isa modest return of hemidiaphragm activityafter C2H. In other models of SCI,combining ChABC treatment with task-
specific training can profoundly improvelimb function. We hypothesized thatcombining ChABC treatment with amodest exposure to intermittent hypoxia(IH), which can strongly drive respiratorymotor plasticity (at higher exposuretimes), will further promote recovery.Methods: Rats received a C2H along withChABC or vehicle control. One weeklater, these animals were exposed to IHfor one hour per day for five days. On thelast day of exposure, diaphragm activitywas assessed.Results:We show that this combinationtreatment of ChABC and modest IHexposure can induce robust respiratorymotor function after C2H. Animals thatreceived IH with no ChABC displayedlittle to no recovery.Conclusion: Taken together, these resultsshow that ChABC treatment combinedwith an IH regimen that is far moretolerable to the animal can stronglyaugment recovery of respiratory motorfunction after SCI.
227Incidental Durotomy After SpinalSurgery: A Prospective Study in anAcademic InstitutionPaul J. McMahon, Marine Dididze, Allan D. LeviIntroduction: Incidental Durotomies (IDs)are an unfortunate but anticipatedpotential complication of spinal surgery.We prospectively surveyed the frequencyof IDs of a single spine surgeon andanalyzed major risk factors as well as theimpact on long term patient outcomes.Methods:We conducted a prospectivereview of elective spinal surgery over a15-year period. Any surgery involvingperipheral nerve only, intraduralprocedures or dural tears due to traumawere excluded. The incidence wascategorized by surgery type includingprimary surgery, revision surgery, etc.Incidence was also examined in thecontext of years of physician experienceand training. Furthermore, the incidenceand type of sequelae were examined forthose patients experiencing an ID.Results: Out of 3,000 total elective spinalsurgery cases, 3.5% (104) experienced anID. The incidence of IDs (3.3%) duringminimally invasive procedures wassimilar, but no patients experienced longterm sequelae. The incidence duringrevision surgery was higher (6.5%). Therewas marked difference in incidencebetween cervical (1.3%) andthoracolumbar (5.1%) cases. The
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES58
ORAL POSTER ABSTRACTS

incidence was lower for cases involvinginstrumentation (2.4%). When physiciantraining was examined, residentsaccounted for 49% of all IDs, whilefellows accounted for 26% and theattending 25%. Of all the cases thatinvolved an ID, 7.7% of patients went onto experience a neurologic deficit, and6.8% experienced a failure of dural repair.The risk of failed dural repair increased 3xin the setting of revision surgery.Conclusion:We established a baselineincidence for durotomy after spine surgeryincluding procedure type, clarifiedcontributing factors and examined thelong-term effects on patient outcomes.
228Cost-utility and ComparativeEffectiveness Analyses of Trans-foraminal Lumbar Interbody Fusion(TLIF) vs. Comprehensive MedicalManagement for LumbarSpondylolisthesisScott L. Parker, Scott Zuckerman, David Shau, Stephen Mendenhall, Joseph S. Cheng, Clinton J. Devin,Matthew McGirtIntroduction: The SPORT trial suggestedthat lumbar fusion was efficacious butNOT cost-effective for the treatment oflumbar spondylolisthesis. However, suchrandomized controlled trials inherentlycontrol and standardize medical resourceutilization and cost. Furthermore, mid-trialcrossover of medicine non-responderssignificantly inflates the utility of medicalmanagement, further biasing cost-utilityanalysis (CUA). We performed acomparative effectiveness and CUA ofTLIF vs. medical management for lumbarspondylolisthesis utilizing a prospectivesingle-center multidisciplinary spinecenter registry in a real-world practicesetting.Methods: Eighty patients withdegenerative lumbar spondylolisthesismanaged at a single institution’sMultidisciplinary Spine Center wereentered into a prospective registry. Surgicalmanagement consisted of trans-foraminallumbar interbody fusion (TLIF), whilecomprehensive medical managementincluded spinal steroid injections, physicaltherapy, oral medications, and variousother therapies. Two-year patient-reportedoutcomes (PRO), back-related medicalresource utilization, and work-day losseswere prospectively assessed via phoneinterview and used to calculate Medicarefee-based direct cost and indirect costsfrom occupation loss. Difference in mean
total two-year cost per QALY gained wasassessed as incremental cost-effectivenessratio (ICER).Results:Baseline characteristics of eachcohort presented in Table 1. TLIF resultedin significant (P< 0.001) two-yearimprovement in all outcomemeasures,while comprehensivemedicalmanagementfailed to provide significant improvement,Figure 1. Two-year gain in QALYwassignificantly greater after TLIF (0.43QALYgained) vs. medical management(0.06QALYgained), Figure 2. Total two-year cost was significantly greater for TLIF($36,836) vs. medical management($8,762), Table 2. The cost per QALYgained for surgery vs.medicalmanagement(ICER)was $75,876, Figure 3.Conclusion: In this prospectivemultidisciplinary registry, lumbar fusionvs. medical management was shown to becost-effective and provide greater two-year improvement in pain, disability, andquality of life. The findings from this real-world practice setting may moreaccurately reflect the true value andeffectiveness of surgical vs. medical carefor degenerative spondylolisthesis.
229Spinal Ependymomas: AnInstitutional Experience Over 25Years in 134 PatientsPhiroz E. Tarapore, Peter Modera, Agne Noujokas, Christopher P. Ames,Dean Chou, Praveen V. Mummaneni,Philip R. Weinstein, Tarik TihanIntroduction: Ependymomas of all gradescomprise approximately 40% of primaryintraspinal tumors. This study examineswhether progression free survival (PFS) isinfluenced by histological grade or extentof resection, and analyzes usage andeffectiveness of postoperative adjuvantradiotherapy.Methods:We have performed aretrospective review of 352 consecutiveintraspinal tumors treated at our institutionbetween 1985 and 2010 All patients withsufficient pathology material and clinicalinformation were included in the study,134 patients with ependymomas wereidentified.Results: There were 85 male and 49female patients with ages from 10 to 79(median 41) years at the time of surgery.Thirty were grade I, 101 were grade II,and 3 were grade III. Follow-up rangedfrom 3 months to 20 years. Kaplan Meieranalysis of PFS demonstrated a mean of 6years for grade I, 14.9 years for grade II,and 3.7 years for grade III (P < .001). The
rate of gross total resection was 77% forgrade I tumors, 68% for grade II tumors,and 33% for grade III tumors. In grade Iependymomas, mean PFS was 6.8 yearswith subtotal resection and 6.3 years withgross total resection (P < .74). In grade IIependymomas, mean PFS was 11.2 yearswith subtotal resection and 17.8 yearswith gross total resection (P < .01).Adjuvant radiotherapy was given in 29%of cases overall (79% of patients who hadsubtotal resection, and 14% of patientswho underwent gross total resection (P <.001)). PFS of patients undergoingsubtotal resection of grade I or II diseasewas not significantly changed by adjuvantradiotherapy (P < .36).Conclusion: There appears to be a shorterPFS in grade I ependymoma than in gradeII. Extent of resection does not appear toaffect PFS in grade I ependymoma, but itdoes in grade II.
230Does Single Dose PreemptiveAmitriptyline or Gabapentin ReduceRemaining Leg Pain After SingleLevel Lumabr Discectomy? ARandomised Clinical Trial withPlacebo ControlPayman Vahedi, Zahra MohajernejadfardIntroduction: Remaining leg pain makesthe outcome in lumbar discectomyunfavorable. Long time sciatica facilitatescentral sensitization, which is responsiblefor the maintenance of pain even after theoptimal surgery. Pre-emptive drugseffective on neuropathic pain mightinterrupt this process via their possiblesynergy with opioids. The aim of presentstudy was to assess the effect ofamitriptyline and gabapentin to reducepostoperative pain scores and morphineconsumption after single level lumbarlaminectomy and discectomy.Methods: Over one year, patients with adecision for single level lumbarlaminectomy and discectomy wererandomly assigned into three groups, eachreceived similar capsules containingamitriptyline, gabapentin or matchingplacebo 2 hours before surgery. Sameanesthetic protocol was performed. Onlypatients with postoperative leg painremained in the study. Visual analoguescale and morphine consumption werecompared at 6 hours intervals up to 24hours. The results were analyzed bySPSS.V.13 and Chi Square andIndependent T.test were used for thestatistical analysis. The groups wererevealed after the accomplishment of the
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 59
ORAL POSTER ABSTRACTS

statistical analysis.Results: Pain was significantly reduced ineach group at each time intervals (P value< 0.001). In comparison to the placebo,the amitriptyline group had a significantlylower pain score by the end of 24 hours (PValue = 0.047), however the gabapentingroup showed no statistically significantdifference (PValue = 0.190). Morphineconsumption was not different statisticallybetween the groups (PValue = 0.132,0.087 respectively).Conclusion: The treatment of remainingleg pain should be considered prior to thesurgery. While preemptive amitriptyline iseffective to reduce remaining leg painafter lumbar discectomies, gabapentinworks no better than placebo.
231Health-Related Quality of LifeOutcomes with Minimally InvasiveTransforaminal Lumbar InterbodyFusion Based on Long-Term Analysisof 318 Consecutive PatientsMick J. Perez-Cruet, Namath Syed Hussain, Evan Begun,Joseph John JoshuaIntroduction: Long-term prospectiveoutcomes in patients undergoingminimally-invasive spinal fusion fordebilitating back pain has not been well-studied.Methods: 318 patients (mean age 63 years,range 19-94) who underwent MITLIFwere followed for 7 years. Patientspresented with spondylolisthesis (n = 236,74%), and degenerative disc disease (n =82, 26%). Health care quality of lifemeasures studied were Visual AnalogScale (VAS), Oswestry Disability Index(ODI), and Short Form-36 (SF36). Otheroutcomes analyzed included pre-operativeco-morbidities, age, bone quality, andcomplications.Results: 196 females and 122 males weretreated. Levels fused included L1-2 (n = 3,1%), L2-3 (n = 19, 6%), L3-4 (n = 34,11%), L4-5 (n = 163, 51%), L5-S1 (n =89, 28%), or multi-level instrumentation(n = 10, 3%). Estimated blood loss andhospital stay were 128.4 mL and 4.37days. VAS scores decreased significantlystarting at 6 weeks post-op. ODI scoresdeclined from 44.1 preoperatively to 28.1(P < .05) at one year, and 30.4 (P < .05)at 2-7 year period. SF36 physicalcomponent scores (PCS) increased from30.3 preoperatively to 39.6 (P < .05) atone year, and 38.7 (P < .05) at 2-7 yearperiod. SF36 mental component scores(MCS) increased from 43.7 preoperatively
to 48.5 (P < .05) at one year, and 49.1 (P < .05) at 2-7 year period. Re-operationrate for adjacent level disease was lessthen 2% over the 7 year period.Conclusion: This study presents a largelong-term prospective outcomes analysisof MITLIF revealing statisticallysignificant outcome improvements out toseven years. MITLIF resulted in a highrate of spinal fusion and very low rate ofadjacent segment disease requiring re-operation. These results highlight theimportance of focused surgery andattention to proper indications whenselecting patients.
232Modulation of Spinal Cord ReflexCircuitry by Spinal DC Stimulation inHumansMaxwell Boakye, Robert Thomas Arrigo,Chris Ho, Jean-Charles LamyIntroduction: Transcranial direct currentstimulation (tDCS) of the human motorcortex induces changes in excitabilitywithin cortical and spinal circuits whichoccur during and after the stimulation.Recently, transcutaneous spinal directcurrent stimulation (tsDCS) has beenshown to modulate spinal conductionproperties, as assessed by somatosensory-evoked potentials, and trans-synapticproperties of the spinal neurons. The goalof this project is to examine the ability ofspinal direct current stimulation to induceplasticity of spinal H-reflexes.Methods: To further explore tsDCS-induced plastic changes in spinalexcitability, we examined, in a double-blind crossover randomized study, thestimulus-response curves of the Soleus Hreflex before, during, at current offset and15 minutes after anodal, cathodal andsham tsDCS delivered at Th11 level(2.5mA, 15min, 0.071mA/cm2,0.064C/cm2) in 17 healthy subjects.Results:Anodal tsDCS induced aprogressive leftward shift of therecruitment curve of the soleus H reflexduring the stimulation, the effectspersisted for at least 15 minutes aftercurrent offset. In contrast, both cathodaland sham tsDCS had no significanteffects. Our results confirm that tsDCScan be a useful, non-invasive tool toinduce long-lasting plastic changes inspinal circuitry.Conclusion: Increased spinal excitabilityafter anodal tsDCS may have potential forspinal neuromodulation in patients withcentral nervous system pain or injury.
233Retrospective, Propensity Score-Matched Cohort Study ExaminingTiming of Fracture Fixation forTraumatic Thoracolumbar FracturesMaxwell Boakye, Robert Thomas Arrigo,Melanie Hayden, Corinna Zygourakis,Shivanand P. LadIntroduction: The timing of surgery inpatients with thoracolumbar fractures,with or without spinal cord injury, remainscontroversial. The goal of this study wasto determine the importance of the timingof surgery on complications and resourceutilization following fixation forthoracolumbar fracture.Methods: In this retrospective cohortstudy, the 2003 through 2008 CaliforniaInpatient Databases were searched forpatients receiving fixation forthoracolumbar fractures. Patients wereclassified as having early (within 72hours) or late (beyond 72 hours) surgery.Propensity score modeling was used toproduce a matched cohort balanced onage, comorbidity, trauma severity, andother factors. Complications, mortality,length of stay, and hospital charges wereassessed. Multivariate logistic regressionwas used to determine the impact ofdelayed surgery on in-hospitalcomplications after balancing andcontrolling for other important factors.Results: Early surgery (<72 hours) fortraumatic thoracolumbar fractures wasassociated with a significantly loweroverall complication rate (includingcardiac, thromboembolic, and respiratorycomplications) and decreased hospitalstay. In-hospital charges were significantlylower ($38,120 difference) in the earlysurgery group. Multivariate analysisidentified time to surgery as the strongestpredictor of in-hospital complications,although age, medical comorbidities, andinjury severity score were alsoindependently associated with increasedcomplications.Conclusion:We reinforce the beneficialimpact of early spinal surgery (prior to 72hours) in traumatic thoracolumbarfractures to reduce in-hospitalcomplications, hospital stay, and resourceutilization. These results provide furthersupport to the emerging literature andprofessional consensus regarding theimportance of early thoracolumbar spinestabilization to improve patient outcomesand limit hospitalization costs.
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES60
ORAL POSTER ABSTRACTS

234Minimally-invasive vs. OpenThoracolumbar Fusion: A Hospital-based Microcosting AnalysisDaniel R. Kramer, Robert G. Whitmore,James Harris Stephen, Robert Stetson,Angus McWilliams, Sherman C. Stein,Sean DoerflerIntroduction: To compare upfront,downstream, and total costs of minimally-invasive thoracolumbar spinal fusion(MIS) compared to open spine techniques(OS) from a hospital-based perspective.Methods: Patients underwent either OS orMIS thoracolumbar fusion fordegenerative spinal pathology at ourinstitution. Actual costs for eachcomponent of the index hospitalization(upfront) and for 9 months postoperatively(downstream) were collected from thehealth system financial databases by costcenter. A multivariable regression wasperformed with cost as the dependentvariable and the following as independentvariables: number of levels operated on,OR time, length of stay (LOS), estimatedblood loss (EBL), age, gender, andethnicity.Results: 79 patients were included in theanalysis: 66 for OS and 13 for MIS. MISpatients had a significantly shorter LOS(4.7 days, ± SD 3.6 days vs. 7.3 days, ±SD 5.1 days, P = 0.035) and lessintraoperative EBL (381.7 ml, ± SD 290.8mL vs. 722.3 ml, ± SD 844.8 ml, P =0.012) compared to OS patients. MISprocedures were associated withsignificantly less upfront costs than OSprocedures ($32,119.86, ± SD $11,802.25vs. $43,047.98, ± SD $20504.35, P =.013). No difference was found betweenthe OS and MIS groups for downstreamor total costs (P = 0.966 and P = 0.240respectively). Regression analysis showedthat MIS upfront costs, when corrected for all independent variables, were stillsignificantly less than OS surgery (P = 0.05).Conclusion: Upfront total costs for MISare significantly less than those for OSthoracolumbar fusion, despite the greateractual cost of surgical implants. Thelargest driver of cost savings for MISprocedures is a shortened LOS. However,the 9-month downstream and total costswere not significantly different betweenthe two types of surgery.
235Standardized Reporting ofPerioperative ComplicationsFollowing Cervical CorpectomyMaxwell Boakye, Robert Thomas Arrigo,Ivan Cheng, Stefan A. Mindea, Eugene Carragee, John Park, Todd AlaminIntroduction: Corpectomy with fusion isroutinely used to decompress and stabilizethe degenerative cervical spine but carrieswith it significant perioperativecomplication risk. Non-standardizedcomplications reporting in the literaturehas made comparison of cervicalcorpectomy with alternative proceduresdifficult. This study is the first to presentthe 30-day complication rate followingcervical corpectomy for degenerativespine disorders using standardizedcomplications reporting systems.Methods: Chart review was performed onsixty-two patients receiving corpectomyfor degenerative cervical spine disease atStanford Hospital between 2003 and2010. Two competing complicationsseverity grading systems (Clavien-Dindo1, Table 1, Accordion2, Table 2)were applied.Results: The mean (SD) age at surgerywas 61 (±13) years. Within 30 days ofsurgery, 18 patients (29.0%) developedone or more complications regardless ofthe grading system used. Both assignednine patients (14.5%) the lowest possiblegrade, and three out of four patients thesecond lowest grade, with the fourthpatient having been treated in an ICU(Clavien-Dindo Grade IV) for pneumonia(Accordion Grade 2. ModerateComplication). A single death (1.6%) wastreated similarly in both systems. Theremaining four patients with more severecomplications were sorted differently(Tables 3 and 4). Finally, three patients(4.8%) had a permanent disability (twocases of dysphagia, one chronic pain)following surgery.Conclusion: The literature on anteriorcervical corpectomy cites a significantmorbidity burden but comparing resultsacross studies or against competingprocedures is complicated by a lack ofreliability, bias, and missing severity data.Routine use of a standardizedcomplication severity grading system willimprove surgical outcomes reportingwhich in-turn supports evidence-basedmedicine, facilitates comparisons withinand between studies, and may improvesurgical decision making and informedconsent. While both standardized systemshave their advantages, the Accordion
system has a built-in intuitive set ofquantitative descriptions of categories aswell as a better means of handlingdisability, an important outcome followingspine surgery.
236Prediction of Reciprocal Changes inCervical Spine Lordosis AfterCorrective Thoracolumbar DeformitySurgeryYoon Ha, Vedat Deviren, Christopher P. AmesIntroduction: To document changes invalues for parameters of cervical sagittalspine balance in before and afterdeformity surgery and find thepreoperative parameters affecting thepostoperative cervical spine alignment.Methods: The study included 49 adultpatients treated for thoracolumbar spinaldeformity. Full-length standing films wereavailable for all subjects. Position of C7plumbline relative to sacrum was assessedas C7 sagittal vertical axis (SVA).Thisstudy was divided into two parts. First, toidentify the reciprocal changespostoperatively, we compare cervicalspine parameters in two distinct groups.Low C7 SVA (n = 21) group includespatient’s C7 SVA below 6Cm and high C7SVA group (n = 21) is defined C7 SVAover 9Cm. Comparisons on the basis ofC7 SVA were performed using student t-test. Second, to predict postoperativecervical lordosis, we studied correlationbetween postoperative cervical lordosiswith preoperative spine and pelvicparameters. Multilinear models with astepwise condition were used to assess therelationship between postoperativecervical lordosis and preoperativeparameters including sagittal spinalparameters and surgical plans (C7 SVA to0 Cm, PT to 25 degrees).Results: In high C7 SVA group, compareto low C7 SVA group, demonstratedhigher preoperative cervical lordosisangles (T1, C0-2, C1-2 angles). In low C7SVA group, mean preoperative C0-C1,C1-C2 and C2-C7 angles weresignificantly increased afterthoracic/lumbar deformity correction. Onthe other hand, high C7 SVA groupdecreased T1 and C2-7 anglespostoperatively. Multiple linear regressionanalysis led to formula for the relationshipbetween postoperative cervical lordosisand preoperative parameters (R = 0.808,adjust R2 = 0.619, parameters using preoppelvic tilt plan, preop C7 SVA plan, preopC2-7 angle and preopT1 angle).
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 61
ORAL POSTER ABSTRACTS

Conclusion: This study provides theevidence that cervical lordosis hasreciprocal changes accommodating theshifting of global spine balance.Preoperative parameters in global spinebalance and surgical plans could predictpostoperative cervical spine sagittalalignment.
237Characterization of a NovelMetastatic Human BreastAdenocarcinoma Rat Model UsingIntracardiac Injection andBioluminescencePatti L. Zadnik, Rachel Sarabia-Estrada,Mari L. Groves, Ali Bydon, Ziya L. Gokaslan, Jean-Paul Wolinsky,Timothy F. Witham, Daniel M. SciubbaIntroduction: Previous animal models ofmetastatic spine disease rely on placementof tumor directly into the spine followedby functional and histological assessment.In order to more accurately reflect humanpathophysiology, we developed a ratmodel of human breast adenocarcinomathat reliably metastasizes to the spinefollowing intracardiac injection of tumorcells. In addition, by tagging the cells withLuciferase and GFP, tumor growth can beimaged non-invasively.Methods: Six four-week-old femaleathymic nude rats were injected with100,000 HTB-26 cells (ATCC) into theleft ventricle. Bioluminescence imagingwas performed at day 3, 11 and 34. Group1 was submitted for CT imaging. Group 2was sacrificed and the spine dissected forhistology. Group 3 had spine tumor cellsdissociated for cell culture. Fluorescencemicroscopy was performed to analyzeGFP signal.Results: Bioluminescence/CT Imaging. Byday 34, the rats demonstratedbioluminescence signals in the spine(Figure 1). Small animal CT imagingconfirmed the presence of an osteolyticlesion (Figure 2). Clinical signs ofneurologic compromise. On day 38, allbioluminescence positive ratsdemonstrated paresis. Dissection revealedosteolytic bone lesions as shown on CT(Figure 3 a,b). Cell culture. Osteolytictumor was removed from the vertebralbody and posterior elements and platedfor culture. On day 3, cells exhibited GFPsignaling, confirming their identity asHTB-26 cells (Figure 4).Conclusion:We have created a reliableanimal model of metastasis of a humanbreast cancer line to the spine withsubsequent characterization of the lesion
via bioluminescence, CT imaging andhistology. We were able to recover theoriginal cells from a metastatic spinelesion, as evidenced by GFP expression inour metastatic lesion. This novel modelmore accurately represents the humancondition, and thus experimental therapiesmay transfer more readily to the patientwith metastatic spine disease.
238Cervical Spine Clearance in theTraumatically Injured Patient: Is CTScan Sufficent AloneBrandon G. Chew, Matthew R. Quigley,Christopher SwartzIntroduction: Clearance of the cervicalspine in the trauma patient remains acontentious issue. Although some haveadvocated for the use of CT scanningalone, this has been criticized, amongother things, for the absence of a gold-standard comparator-namely MRI.Methods:A retrospective review of aprospectively collected trauma databasefor all patients admitted January 2004 –January 2011 to a level one trauma centerwho had a cervical CT interpreted by aboard certified radiologist, as beingwithout evidence of acute traumatic injuryand a cervical MR obtained during thesame hospital admission.Results: There were 1004 patientsreviewed, of which 614 were male,average age overall of 47 years. Thirty-nine patients ultimately underwent (29anterior/10 posterior) cervical surgicalprocedures (5 delayed), for central cordsyndrome (21), quadraparesis (9) ordiscogenic radicular pain (9). None had anunstable cervical spine. The MR wasinterpreted as normal in 645, evidencingligamentous injury alone in 125 andshowing non-specific degenerativechanges in the rest. Of the 125ligamentous injuries, 59 haddocumentation of clearance (22 clinical,37 with F/E X-rays), 5 died prior toclearance and one was transferred toanother facility prior to clearance. Nopatient with ligamentous injury on MRwas documented to require any surgicalprocedure nor orthosis.Conclusion: In this large population oftraumatically injured patients with normalcervical CT scans, MR was useful solelyto guide surgical procedures alreadydetermined by clinical presentation. Theappearance of ligamentous injury alone onMR was a common occurrence (12.5%)but never predicted occult cervicalinstability.
239The Use of Allograft andRecombinant Human BoneMorphogenetic Protein forInstrumented Atlanto-axial FusionsBrian James Hood, D. Kojo Hamilton,Justin S. Smith, Marine Dididze,Christopher I. Shaffrey, Allan D. LeviIntroduction: Fusing the atlantoaxialcomplex has long been a challenge tosurgeons. Iliac crest is the historical goldstandard for bone grafting but isassociated with significant patientmorbidity. Hillard et al. reported a fusionrate of 88.9% using iliac crest allograft vs.96.7% using autologous iliac crest bonefor C1-2 fusion.Methods:We reviewed our experienceusing allograft bone, rhBMP2 and rigidscrew fixation of C1-2. A retrospectivechart and film review of a senior surgeonwas performed at the University of Miami(24 patients) and University of Virginia,Charlottesville (28 patients) between 2004and 2011 and examined for fusion ratesand complications. In 28 patients,corticocancellous allograft pieces werelaid along decorticated bone after a C2neurectomy. In 24 patients unicortical iliaccrest allograft was precision cut to fitbetween the C1 lamina and C2 spinousprocess. The mean amount of rhBHMP2used for all cases was 4.5 mg (2.2 mg-12mg).Results: There were 25 female and 27male patients ranging in age from 6 to 92years with a mean age of 65.8 years.Operative indications include trauma(56%), degenerative (23%), rheumatoidarthritis (15%), congenital (4%), andsynovial cyst (2%). The mean follow-upwas 22.5 months (range 1-55 months). 52fusions were performed. 46 patientsachieved a minimum 3 month follow-up.100% achieved fusion: 41/46 Lenke A,5/46 Lenke B. Patients not reaching 3months all appeared to be progressing tofusion. Complications including sustainedtachycardia, pneumonia, DVT,shock/respiratory failure, and bilateralhand numbness occurred in 5 patients(9.6%) and were unrelated to the use ofrhBMP2.Conclusion: The use of small amounts ofrhBMP2 added to allograft in addition torigid screw fixation is safe and highlyeffective means of promoting a solidfusion of the atlantoaxial complex andspares the patient the morbidity of iliaccrest harvest.
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES62
ORAL POSTER ABSTRACTS

240Minimally Invasive Treatment ofAdult Scoliosis with XLIF:Radiographic Outcomes andPredictors from a ProspectiveMulticenter StudyAntoine Tohmeh, Frank Phillips, W.B. RodgersIntroduction: This report summarizes theearly radiographic outcomes of XLIF forthe treatment of adult scoliosis.Methods: 107 patients were treated foradult scoliosis with XLIF. Radiographsand clinical outcomes were collectedpreoperatively and at 0.5, 3, 6, 12, and 24months. This report details results up to 3months as the study progresses.Radiographic measures include lumbarlordosis (L1-S1), Cobb, devicesubsidence/migration, anterior/posteriordisc height, listhesis, and coronal/sagittalbalance. To minimize radiographicmagnification all linear measures werecollected as a ratio of a reference endplateor vertebral body height, and reported as apercentage change.Results:Measures were collected from 93patients (74.2% female, 11.1% smokers)48-87 years old treated at 280 levels fromT11-L5. Up to 6 levels were treated.Supplemental fixation included: bilateralpedicle screws (59.3%), unilateral pediclescrews (23.3%), and anterolateral plating(4.4%), 16.1% of levels were stand-alone.Radiographic measures are reported inTable 1. At baseline, 42 patients werehypolordotic (>-40°) with an averagelumbar lordosis of -24.74° (range: 0 to -40°). Hypolordosis in these patients wascorrected to an average of -38.2° at post-op (P < 0.001). Cobb angle was correctedby 40% from baseline to post-op (P <0.001). Spondylo/retrolisthesis wasreduced from an average baselinemagnitude of 7.3% to a post-opmagnitude of 6.0% (P = 0.002). Allcorrections were maintained at 3 months(P > 0.05). Coronal Cobb correction wasaffected by supplemental fixation (P =0.002), with the greatest correctionsachieved in patients with bilateral pediclefixation and the least achieved in patientswith no supplemental fixation (11.7° vs.<1°). Subsidence was 26.2% at 3 monthswith the highest rate of subsidence insegments with no supplemental fixation(55.6%). No segments required revisionfor subsidence. There were no reports ofmigration.Conclusion: XLIF in the treatment of adultscoliosis, reduces coronal and sagittalplane deformity. Supplemental fixation
optimized deformity correction andreduced subsidence.
241WITHDRAWN
242Analysis of Readmission Rates AfterSpinal Surgery: Do UnderfundedPatients Have Higher ReadmissionRates After Spinal Surgery?Daniel Robert Fassett, Yazhini Gnanasambanthan, Linda Gonia,Huaping Wang, David M. NeilsIntroduction:With “pay for performance”initiatives gaining popularity, insurers andhospitals are scrutinizing a number ofquality measures including the 30-dayreadmission rate. Factors responsible forvariablility in the rate of 30-dayreadmission are not fully understood, butsocioeconomic factors may be aconfounding variable. Academic medicalcenters, which care for a larger proportionof underfunded patients, may have higher30-day readmission rates because ofpatient socioeconomic factors such aslower employment or under/uninsuredstatus.Methods: Our readmission data afterspinal surgery was reviewed for 3275consecutive surgeries from October 2007to June 2011. The patients were dividedinto four groups based on insurance status(A =commercial & managed-care, B=Medicaid, C= Medicare, and D = Self-pay& Charity). The data was analyzed usingChi-square test, Kruskal-Wallis test andmultiple logistic regression test. The two-tailed P < 0.05 was considered forstatistical significance. All statisticalanalyzes was performed using SAS 9.1.3. Results: There were 192 (5.86%) 30-dayreadmissions with the followingpercentages found for each group: A =4.8%, B = 3.8%, C = 8.1%, and D =6.14%. The results revealed that group C(Medicare) had significantly morereadmissions than group A (P = 0.0006)and B (P = 0.0069). After adjusting forage, sex, residential area (rural, suburbanor urban), severity of illness and risk ofmortality, there was no difference inreadmission rates between groups.Regression analysis revealed that severityof illness correlated with increased risk forreadmission.Conclusion: Our analysis indicates thatunderinsured patients (Medicaid andCharity) do not have a higher rate for 30-day readmission. Medicare patients have ahigher rate for readmission due to
increased severity of illness in this groupof patients. This study underscores theimportance of adjusting for severity ofillness when comparing 30-dayreadmission rates between individualproviders.
243Analysis of Spinal Surgery FusionCosts over a Six-Hospital System:How Can We Explain DramaticVariances in the Cost of SurgeryBetween ProvidersDaniel Robert Fassett, Yazhini Gnanasambanthan, Rae Podabinski, Alexander HassIntroduction: There has been significantproduct development in spinal technology.Numerous products/additives are nowavailable for use in spinal fusions, leadingto increasing amounts being used. As aresult, the cost of spinal fusion hasincreased dramatically. In many situations,there is limited clinical data supporting thecost effectiveness of these products.Methods:Analysis of cost for spinalfusion procedures was performed over asix hospital healthcare system (November2008 to April 2009). Single-level posteriorfusions with and without interbodyarthrodesis were analyzed including costsfor spinal instrumentation, interbodyimplants, biologics, and other additives.Mean cost for every surgeon operatingwithin the hospital system was analyzed.Results: Eighteen surgeons (11neurosurgeons, 7 orthopedic) performedposterior lumbar fusions over this timeperiod. There were 97 single-levelposterior fusions with interbody (PFwI)and 33 single-level posterior fusionswithout interbody arthrodesis (PF). Therange of surgical costs for PFwI was$7,550 to $23,824 with an overall meancost of $11,564. Ten surgeons performedPFwI with mean costs for individualproviders ranging from $7,750 -$21,543(178% difference). The overall mean costfor PF was $7,213 with a range from$4,550 to $16,305. Fifteen surgeonsperformed PF with mean costs forindividual providers ranging from $4,450-$16,305 (266% difference). Variances incosts between providers were primarilydue to use of biologics and bone graftsubstitutes. There were no differences inthe mean cost between eitherneurosurgeons and orthopedic surgeons orhospital-employed and private-practicesurgeons.Conclusion: This indicates that there issignificant variance in the cost of
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 63
ORAL POSTER ABSTRACTS

equivalent surgical procedures betweensurgeons. This is largely explained withthe indiscriminate use of biologics andbone graft substitutes. In our currenthealth care economic environment,procedural costs should be scrutinized.Our analysis underscores the need forprotocol development for the use ofbiologics and bone graft substitutes.
244Anterior vs. Posterior InterbodyFusion: A Comparison of OutcomesMark Mahan, Samuel Kalb, Juan Christian Ribas Nijkerk, Laura Ann Snyder, Udaya K. Kakarla,Nicholas TheodoreIntroduction: Choosing the mostappropriate approach for lumbar fusiondepends on individual symptoms andanatomy. Multiple studies havedemonstrated good results with both ALIFand PLIF procedures independently. Thisstudy compares outcome between patientswho received ALIF and PLIF.Methods: 775 patients who underwentlumbar fusion using either ALIF or PLIFtechniques were reviewed. 37 cases werelost to follow up. 500 patients receivedPLIF and 238 received ALIF. Patientsurgical outcomes were evaluated basedon complications, symptomaticimprovement, hospitalized days and Prolooutcome scores.Results: The average length of follow-upfor PLIF patients was similar to that ofALIF patients: 11.8 months and 11.5months, respectively. ALIF patients had a12.1% (29/238) rate of cumulativecomplications. The average economical,functional and total Prolo scores for thisgroup were 4.26, 3.66, and 7.92. PLIFpatients had a 5% (25/500) rate ofcumulative complications. The averageeconomical, functional and total Proloscores for PLIF were 4.07, 4.04, and 8.11.Patients with L3 to L5 disc disease weremore likely to undergo PLIF (P =<0.001). Post-operative complications wassignificantly higher in ALIF group (P =<0.001). Hospital stay was longer in thePLIF group compared to ALIF (P =0.005). PLIF patients showed bettersymptomatic improvement at threemonths follow-up (P = <0.001) and Prolofunctional score (P = <0.001).Nostatistical difference was seen in Prolototal score between ALIF and PLIFpatients. PLIF showed superior overalloutcomes only at L3-L4 level whencompared to ALIF (P = 0.008).Conclusion:ALIF and PLIF have shown to
be safe treatment procedures with lowcomplications rates. PLIF appears to havebetter short term symptomatic outcomeand fewer complications compared toanterior approach. Overall outcomes weresimilar between them. It seems that PLIFis more suitable in L3 to L5 cases,possibly secondary to increased difficultyin performing anterior surgery in superiorlevels.
245Utility of Clavien-Dindo andAccordion Classification Systems forPostoperative ComplicationsFollowing Spinal Metastasis SurgeryMaxwell Boakye, Pelu Tran, Robert Thomas Arrigo, Ivan Cheng, Stefan A. Mindea, Eugene Carragee, John Park, Todd AlaminIntroduction: Surgical intervention forspinal metastases is an extensiveprocedure with extended recovery timesand high rate of morbidity. Yet, aconsistent method of classification andquantification of complications does notexist. In this study, we analyzed theapplicability of the Clavien-Dindo andContracted Accordion classificationsystem on a cohort of 200 patientsoperated on for spinal metastases atStanford Hospital between 1999 and2009.Methods: Stanford’s STRIDE databasewas used to perform a retrospective chartanalysis on 200 patients who had beenoperated on for spinal metastases between1999 and 2009 at Stanford. 30-daycomplications were graded by level ofintervention required, per the Clavien-Dindo and Accordion criteria, andfeasibility and validity of thesecomplication classification systems wereassessed.Results: Under the Clavien-DindoClassification System, 74 patients (37.0%)experienced minor complications and 28patients (14.0%) had major complication.Under the Accordion System, minorcomplications were reported in 58 patients(29.0%), and major complications in 28patients (14.0%). Of the majorcomplications, 8 (4.0%) led to death.Correlation between complication gradeunder the Accordion system and length ofstay was 0.24, vs. 0.22 for the Clavien-Dindo system.Conclusion:Analysis of 30-day spinalmetastasis surgery complicationsclassified via the Accordion and Clavien-Dindo systems provided increasedresolution for complication reporting, and
could be broken down to analyzecomplication severity distribution betweenseveral patient subpopulations. Excludingblood transfusions, the overallcomplication rate was 37.0%, in line withreported complication rates of 15-39%.Classification under the Accordion Systemwas more closely correlated to length ofstay than under Clavien-Dindo.Additionally, overall complication ratereported by the Accordion system moreclosely followed those previously reportedin literature. The use of the Clavien-Dindoor Accordion system for classification ofcomplications is easily applicable tosurgery for spinal metastases and enablesmore precise reporting and analysis ofcomplications.
246Cost-utility and ComparativeEffectiveness Analyses ofLaminectomy vs. ComprehensiveMedical Management for LumbarStenosisScott L. Parker, Scott Zuckerman, David Shau, Stephen Mendenhall, Joseph S. Cheng, Clinton J. Devin,Matthew McGirtIntroduction: The SPORT trial suggestedthat lumbar laminectomy was efficaciousbut only moderately cost-effective for thetreatment of lumbar stenosis. However,such randomized controlled trialsinherently control and standardize medicalresource utilization and cost. Furthermore,mid-trial crossover of medicine non-responders significantly inflates the utilityof medical management, further biasingcost-utility analysis (CUA). We performeda comparative effectiveness and CUA oflaminectomy vs. medical management forlumbar stenosis utilizing a prospectivesingle-center multidisciplinary spinecenter registry in a real-world practicesetting.Methods: Ninety-four patients withlumbar spinal stenosis managed at a singleinstitution’s Multidisciplinary SpineCenter were entered into a prospectiveregistry. Surgical management consistedof laminectomy, while comprehensivemedical management included spinalsteroid injections, physical therapy, oralmedications, and various other therapies.Two-year patient-reported outcomes(PRO), back-related medical resourceutilization, and work-day losses wereprospectively assessed via phoneinterview and used to calculate Medicarefee-based direct cost and indirect costsfrom occupation loss. Difference in mean
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES64
ORAL POSTER ABSTRACTS

total cost per QALY gained was assessedas incremental cost-effectiveness ratio(ICER).Results: Baseline characteristics of eachcohort are presented in Table 1.Laminectomy resulted in significant (P <0.01) two-year improvement in all outcomemeasures, while comprehensive medicalmanagement failed to provide significanteffectiveness, Figure 1. Two-year gain inQALY was significantly greater afterlaminectomy (0.36 QALY gained) vs.medical management (0.10 QALY gained),Figure 2. Total two-year cost wassignificantly greater for laminectomy($24,264) vs. medical management($9,550), Table 2. The cost per QALYgained for surgery vs. medical management(ICER) was $56,592, Figure 3.Conclusion: In this prospective multi-disciplinary registry, lumbar laminectomyvs. medical management was shown to becost-effective and provide greater two-year improvement in pain, disability, andquality of life. The findings from this real-world practice setting may moreaccurately reflect the true value andeffectiveness of surgical vs. medical carefor lumbar stenosis.
247Long-term Outcome of MinimallyInvasive Transforaminal LumbarInterbody Fusion: 5 Years Post-opand BeyondHamid M. Shah, Kevin T. FoleyIntroduction: Several reports havedescribed the efficacy of minimallyinvasive transforaminal lumbar interbodyfusion (MIS-TLIF), but none havedocumented the long-term outcomes ofpatients undergoing this procedure. Thepurpose of this study was to quantifypatient-derived outcomes for MIS-TLIFpatients who were 5 years or more post-operative.Methods:A chart review was performedafter obtaining IRB approval. All patientswho had undergone a single-level MIS-TLIF 5 or more years prior for lumbarspondylolisthesis or spondylosis and forwhom preoperative Oswestry DisabilityIndex (ODI) and visual analog pain scale(VAS) data had been collected wereincluded. These patients were contactedby phone and mail. After informedconsent, they filled out ODI and VASforms and returned them to theinvestigators. The current outcome datawere compared to the preoperativelyderived measures.Results: 55 patients had undergone MIS-
TLIF within the specified time frame[mean 72.6 months (60-90)] and hadpreoperative baseline ODI and VASscores. Of these, 39 (19 male/20 female)patients were successfully contacted andreturned current ODI and VAS scores. Themean cohort age was 63 years (37-80).The mean baseline ODI was 53 (30-100)and mean baseline VAS back and VAS legwere 50 (0-99) and 56 (0-98),respectively. The mean scores at the timeof inquiry for ODI, VAS back, and VASleg were 17(0-60), 12 (0-62), and 16 (0-77), respectively, represent a decrease of36, 38, and 40 points from baseline.Conclusion:Multiple reports havedocumented patient-derived outcome datafollowing MIS-TLIF, none have done sofor patients 5 or more years beyond theirindex procedure. The significantimprovements in disability, back pain, andleg pain seen in the present study implythat MIS-TLIF is capable of producingsustained relief of symptoms andimprovement in patient function. This haspositive implications for the cost-effectiveness of this procedure.
248The Effect of RhBMP-2 Dosing on theComplication and Fusion Rate inPosterior Interbody Fusion UsingPolyetheretherketone (PEEK) CagesEric W. Nottmeier, Douglas S. Fenton,Cammi Bowman, Zane Thompson,Matthew HaleIntroduction: Excellent fusion rates, aswell as complications, have been reportedwith the off-label use of rhBMP-2 inposterior lumbar interbody fusionprocedures.1-5 The authors report thefusion and complication rates in a largecohort of patients undergoing posteriorinterbody fusion using rhBMP-2 at threedifferent dosages.Methods: The charts of 177 consecutivepatients undergoing PLIF or TLIF usingPEEK cages and rhBMP-2 at 234interbody levels were retrospectivelyreviewed. Delivery of rhBMP-2 was viaabsorbable collagen sponges (ACS) in allpatients. All patients had contralateralposterolateral fusion with rhBMP-2 andmorcellized allograft/local autograft.Demineralized bone matrix (DBM) wasused in some patients at the discretion ofthe surgeon. The rhBMP-2 dose used inthe interspace was adjusted twice in this 4cohort secondary to complicationsobserved from rhBMP-2 (Table 1). Allpatients were scheduled for thin-cutcomputed tomographic (CT) scans, which
were graded for fusion by an independentradiologist.Results:Mean follow-up in this study was19 months. Twelve patients undergoinginterbody fusion at 13 levels in this studywere lost to follow-up and no CT wasavailable leaving 221 interbody levels in165 patients to be evaluated.Complications of rhBMP-2 included cystformation behind the cage causingradiculopathy and/or vertebral osteolysis(Fig. 1). The per-level fusion rates inGroups 1, 2, and 3 were 93%, 94%, and93%, respectively. The per-levelcomplication rates in Groups 1, 2, and 3were 17.1%, 9.4%, and 3.4%,respectively.Conclusion: Complications resulting fromthe use of rhBMP-2 in posterior interbodyfusion can be decreased by decreasing thedose of rhBMP-2. In this study, a totaldose of 1.1mg of rhBMP-2 in theinterspace decreased the complication ratewithout a decrease in fusion rate whencompared to higher doses of rhBMP-2used in the interspace.
249Diffusion Tensor Imaging Correlateswith Spinal Somatosensory EvokedPotentials After Spinal Cord InjuryShekar N. Kurpad, Brian Schmit, Michael JirjisIntroduction: Diffusion Tensor Imaging(DTI) is a promising novel MRI basedtechnique for spinal cord tractography.Spinal somatosensory evoked potentials(SpSEPs) have previously been shown todetect and characterize different latencycomponents associated with specificspinal pathways. We have correlated DTIIndex FA and SpSEP in the spinal cordafter varying injury severity .Methods: DTI (FA) and SpSEPs werecollected on 40 female Sprague-Dawleyrats 10 weeks post-injury. 4 groups wereincluded: sham, mild, moderate, andsevere thoracic SCI derived from an NYUimpactor. Animals were imaged in vivousing a 9.4T magnet, and axial diffusionweighted images were collected at a b-value of 500 seconds/mm(2). Average FAvalues were calculated in axial sections ofthe cervical spinal cord with five slicesrepresenting C2-3/C3-4/C4-5/C5-6 andC6-7 respectively. For SpSEPs,stimulation was applied to the sciaticnerve and recording electrodes wereplaced rostral to T5 and T11.Results: In all three injury groups, averageFA values showed a progressivedecreasing trend in a cephalocaudal
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 65
ORAL POSTER ABSTRACTS

direction ranging from 0.69 to 0.59mm(2)/s in FA and correlated with SpSEPamplitude. Severely injured rats showedthe greatest reduction in FA and SpSEPvalues (average of 0.9 decrease in FA)with moderate and mild injured animalsshowing slightly lesser reduction (averageof 0.6 and 0.4 mm(2)/s decrease in FArespectively). FA and SpSEP values in thesevere injury group were significantlydifferent (analysis of variance [ANOVA],P > 0.05) than the other two groups. Nosignificant difference was observedbetween the mild and moderate groups.Conclusion:We have demonstrated thatDTI biomarker FA correlates withSpSEPs after SCI rendering FA a suitablebiomarker for estimating functionalchanges in the spinal cord after varyinginjury severity.
250Kyphotic Deformities of the CervicalSpineJan Stulik, Petr Nesnidal, Jan Kryl, Tomas Vyskocil, Michal BarnaIntroduction: The development of acervical kyphotic deformity can beassociated with a degenerative disease,trauma, tumor, developmental anomalyand also a surgical procedure, both theanterior and posterior surgical approaches.The deformity can also result fromsystemic diseases, such as ankylosingspondylitis or rheumatoid arthritis.Methods: Retrospective analysis of 102patients underwent correction of cervicalkyphosis at our department between May2005 and April 2010, 90 patients wereincluded in this study with an average ageof 56.7 years. In 6 patients kyphosis wascaused by an inveterate injury, in 71 bydegenerative disease, in 6 by rheumatoidarthritis, and 7 due to previous surgery.Surgery was carried out from the anterior,posterior or combined approach. Thesurgical outcome was assessed using theNurick score and Neck Disability Index(NDI), the Visual Analogue Scale (VAS)was used to evaluate pain intensity orparaesthesia.Results: The average NDI value was 25.5before surgery and 14.3 and 14.9 at oneand two years after surgery. The averagepre-operative Nurick score was 0.7, anaverage post-operative value of 0.6 and0,6. The average VAS value for neck andradicular pain was 5.7 pre-operatively, and2.5 and 2.7, respectively. Complete boneunion was achieved at 6 months aftersurgery in 97.8% patients. The averagepre-operative value for the cervical
curvature index (Ishihara) was -13.7,postoperatively was +15.3. The averagepre-operative cervical kyphosis was -14.4degrees, postoperatively was +13.5.Conclusion: The results showed a markedimprovement in the patient’s quality oflife after kyphosis correction, improvedneurological status and an improvedposture seen on radiograms of the cervicalspine. The study also revealed a highernumber of potential complicationsassociated, in particular, with correctiveosteotomy. The best results were achievedwith the combined surgical approach,however, the choice of a surgical methodwas independent on the patient’s clinicalstatus.
251Predictors of Outcome FollowingTraumatic Spinal Cord InjuryDaniel Yavin, Steven Casha,Amro Al-Habib, R. John HurlbertIntroduction:Various determinants ofprognosis following spinal cord injury(SCI) have been proposed. Herein wereport clinical and radiologic featurespredictive of outcomes followingtraumatic SCI.Methods:A post hoc secondary analysiswas performed of outcomes collectedduring a randomized-controlled trialevaluating minocycline in consentingadult patients with traumatic SCI.Outcome measures included the AmericanSpinal Cord Injury Association (ASIA)Impairment Scale (AIS) score, FunctionalIndependence Measure (FIM), LondonHandicap Score (LHS) scale, Short Form36 (SF36), and Spinal Cord IndependenceMeasure (SCIM). Five clinical andradiologic features were evaluated aspredictors of outcome via a multivariateregression.Results: Fifty-two patients were enrolledfrom June, 2004 to August, 2008 andfollowed for a mean duration of 13.5months. Mean patient age was 36.7 years,73% were male, and 67% of injuriesoccurred in the cervical spine. At baselinemean AIS was 129.0. Twelve-month meanAIS, LHS, SF36, and SCIM were 178.5,75.5, 87.3, and 59.8, respectively. Featuresindependently associated with outcomesat 12 months were age (LHS P = 0.05,and SCIM P = 0.03), baseline AIS (AIS P< 0.01, SCIM P < 0.01, LHS P < 0.01),length of parenchymal damage of T2-weighted MR imaging (AIS P = 0.05),maximum canal compromise (LHS P <0.01), and maximal spinal cordcompression (LHS P = 0.02).
Conclusion: Predictors varied withdomains of outcome. Age, baseline AIS,length of parenchymal damage of T2-weighted MR imaging, maximum canalcompromise and maximal spinal cordcompression were predictive of outcomesfollowing traumatic SCI.
252Functional Improvement After TotalDisc Arthroplasty at 1 and 2 Levels ofthe Cervical Spine: 36 Month Follow-Up of an FDA IDE Clinical TrialReginald J. Davis, Steven E. Gaede,Michael S. Hisey, Kee Duk Kim, Pierce D. Nunley, Daniel L. Peterson, John K. StokesIntroduction: Total disc arthroplasty(TDA) is becoming increasingly commonand represents an alternative treatment toACDF for the treatment of symptomaticcervical degenerative disc disease.Methods:A two-arm, randomized,controlled, FDA regulated IDE clinicaltrial to compare treatment of symptomaticcervical DDD at 1 or 2 levels using TDAusing the Mobi-C Cervical Artificial Discto treatment with ACDF was performed at24 clinical sites. A total of 245 patientswere treated at 1-level and 330 at 2-levels.Data were collected through 36 months.Patients were randomized at 2:1 (TDA:ACDF). Neck Disability Index (NDI)score, neurologic outcomes, and VASneck pain are reported through 36 months.Results: The mean NDI and VAS scoresfor the TDA and ACDF groups were notsignificantly different pre-operatively ineither study. Patients in both groups inboth studies showed a significantimprovement in mean NDI and VASscores from baseline at all follow-up timepoints (P < 0.05) and the rates ofneurologic deterioration were very low. Inthe 1-level study the TDA patients had asignificantly better NDI score comparedto ACDF patients at 6 weeks and 3months and significantly better VAS neckpain at 6 weeks (P < 0.05). In the 2-levelstudy the improvement over baseline inNDI was significantly better for TDApatients compared to ACDF patients at alltime points through 36 months andimprovement over baseline in VAS neckpain was also significantly better for TDApatients at 3 and 6 months (P < 0.05).Conclusion: TDA resulted in greaterfunctional improvement and a greaterdecrease in pain early, and similarimprovements throughout the follow-upperiod compared to ACDF for 1-leveltreatment. TDA resulted in significantly
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES66
ORAL POSTER ABSTRACTS

greater functional improvement comparedto ACDF at all follow-up time points andsignificantly less pain at earlier timepoints for 2-level treatment.
253Does Recombinant Human BoneMorphogenetic Protein-2 (rhBMP-2)Dose and/or Cage CountersinkingDepth Affect the Incidence ofHeterotopic Bone Formation inPosterior Interbody Fusion?Eric W. Nottmeier, Cammi Bowman, Zane Thompson, Matthew HaleIntroduction: Heterotopic bone formationhas been reported with the off-label use ofrhBMP-2 in posterior interbody fusionwith and without clinical sequelae.[1-4]The authors report their findings in a largecohort of patients undergoing posteriorinterbody fusion using rhBMP-2 andpolyetheretherketone (PEEK) cages.Methods: The charts and postoperativecomputed tomographic (CT) scans of 165patients undergoing posterior interbodyfusion using PEEK cages and rhBMP-2 at221 interbody levels were reviewed. TherhBMP-2 dose that was used in theinterspace was adjusted twice in thiscohort (Table 1). Heterotopic boneformation in the spinal canal was gradedas less than 5mm or greater than 5mm.Cage countersinking was graded in asimilar fashion. The incidence ofheterotopic bone formation was comparedwithin the rhBMP-2 dosing and cagecountersinking groups, and to the overallincidence of radiculitis/chronic leg pain,by chi-squared tests.Results:Mean follow-up in this study was19 months. Overall results showed thatlower doses of rhBMP-2 weresignificantly related to a lower incidenceheterotopic bone formation (P < .001).Paired group comparisons showed Group1 was significantly different than bothGroup 2 and 3 in the incidence ofheterotopic bone formation (71%, 47%,38%, respectively) (P < .001). Group 2and Group 3 were not significantlydifferent in the incidence of heterotopicbone formation (P > .05). Results alsoshowed a cage depth of less than 5mm, ascompared to greater than 5mm, wasassociated with a significantly higherincidence of heterotopic bone formation(56%, 12%, respectively) (P < .001). Nosignificant increase in the incidence ofradiculitis or chronic leg pain wasobserved in patients with heterotopic boneformation as compared to patients withoutheterotopic bone formation.
Conclusion: The dose of rhBMP-2 andcage countersinking depth can influencethe incidence of heterotopic boneformation in posterior interbody fusion.However, no significant increase in theincidence of radiculitis or chronic leg painexisted in patients exhibiting heterotopicbone formation.
254Diffusion Tensor Imaging: Evaluatingthe Spinal Cord in Animal Modelsand HumansShekar N. Kurpad, Brian Schmit, Aditya Vedantam, Marjorie C. Wang,Benjamin M. EllingsonIntroduction: T2-weighted magneticresonance imaging (MRI) lacks sufficientsensitivity to detect neural injury.Diffusion Tensor Imaging (DTI) is anewer technique that is able to defineaxonal integrity by measuring thediffusion of water molecules. We presentour experience with DTI in studyingspinal cord injury (SCI) in rat models aswell as patients.Methods:We performed DTImeasurements using a 9.4T MR scanneron Sprague-Dawley rats after a moderatecontusion injury at T8 and documentedthe DTI changes as well as histologicalfeatures up to 25 weeks after SCI. Also,we attempted to correlate spinalsomatosensory evoked potentials(SpSEPs) with DTI measurements.Subsequently, we described DTIparameters in human controls and chronicSCI patients.Results: In rat models, the longitudinalapparent diffusion coefficient (lADC) wasreduced throughout the cord up to 25weeks after SCI, while the white matter(WM) fractional anisotropy (FA)decreased and the transverse apparentdiffusion coefficient (tADC) increasedaround the lesion. Histological sectionsshowed progressive cavitation withrostral-caudal spreading that correlatedwith the MD. Early SpSEPs correlatedwith the diffusivity in medial WM tractswhile the late SpSEPs correlated with theMD of the lateral spinothalamic tract. Inhuman controls, while the FA of thewhole cord decreased in the rostral-caudaldirection, MD was relatively constantthroughout the cord. In chronic humanSCI, just as MD, tADC and lADCincreased around the lesion, the FA wasgreatly reduced and was able to accuratelydefine the extent of the lesion.Conclusion: Using rat models, we haveshowed that DTI parameters correlate well
with histological and functional measuresand this has helped us refine this modalityfor human research. DTI is able to providea unique insight into the varied changesassociated with SCI and we expect to seegreater applications of DTI in studyinghuman spinal cord disorders.
255Early Stabilization of ThoracolumbarInjuries in Polytraumatized PatientsTimothy A. Moore, Michael P. Steinmetz,Heather VallierIntroduction: Polytrauma patients oftenpresent with unstable thoraco-lumbarinjuries. While most surgeons feel theseinjuries need to be stabilized, the timing ofsuch an operation remains a topic ofdebate. We present a consecutive series of98 thoraco-lumbar injuries stabilized in anearly or late manner.Methods: Ninety-eight skeletally maturepatients with an Injury Severity Scoregreater than 18 presenting to our Level 1trauma center were retrospectivelyreviewed. There were 79 men and 19women. The average age was 37.3 (18-71)years. The average Injury Severity Score(ISS) was 37.3 (18-50). The “early” groupwas defined as definitive stabilizationwithin 24 hours, 21 patients (21.4%) and“late” group after 24 hours, 77 patients(78.6%). Associated injuries of the chest,abdomen and head were documentedalong with ISS, Abbreviated Injury Scoresand Glasgow Coma Scale. Transfusionrequirements, length of ventilatorassistance, length of ICU stay, and lengthof hospitalization were determined.Complications were reviewed, includingwound infection, pulmonarycomplications (adult respiratory distresssyndrome (ARDS), pneumonia,pulmonary embolism (PE)), renal failure,multiple organ failure (MOF) and deepvenous thrombosis (DVT).Results: The average ISS was 29.1 ± 9.3for the early group and 32.5 ± 11.3 for thelate group (P = 0.001). The late group hadlonger hospital stay and ICU stay. Theearly group had a lower rate of ARDS,pneumonia and sepsis compared to thelate group. Rates of DVT, PE, woundinfection, renal failure, MOF and deathwere not statistically significant betweenthe two groups.Conclusion: In polytraumatized patientswith thoraco-lumbar injuries, prolongedrecumbency has been shown to negativelyimpact pulmonary function. Painreduction achieved by stabilization limitssympathetic discharge and reduce narcotic
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 67
ORAL POSTER ABSTRACTS

consumption causing less pulmonarysuppression. Ninety-eight unstablethoracolumbar injuries in polytraumatizedpatients were reviewed. Patients whounderwent definitive stabilization within24 hours achieved shorter ICU andhospital stays and lower rates ofpulmonary complications than thosetreated greater than 24 hours. We feelsurgical timing should be a multi-disciplinary decision based on thepatient’s physiologic and resuscitationstatus and the extent of the stabilizationprocedure.
256Diffusion Tensor MRI andMotoneuron Morphometric Changesin Cervical Gray Matter After aThoracic Spinal Cord Injury in the RatShekar N. Kurpad, Brian Schmit, Benjamin M. Ellingson, Robin MottackelIntroduction:We investigated the diffusiontensor imaging (DTI) changes in thecervical spinal cord gray matter (GM) as aresult of a thoracic (T8) contusive spinalcord injury (SCI) in the rat.Methods: DTI data from ex vivo rat spinalcords were registered to correspondinghistological slices in uninjured control,and 2, 15 and 25 weeks post injury (n = 5all groups). Animals were perfused with10% formalin, spinal cords excised, post-fixed for 7 days, and imaged using aBruker 9.4T scanner using a standardpulsed gradient spin echo sequence. Afterimaging, samples were dehydrated,blocked in paraffin, sliced axially andstained with eriochrome cyanine R stain,H&E counter-stain, and osmium tetroxidewith toluidine blue. The WM and the GMregions of interest were used to map DTIindices, including fractional anisotropy(FA), longitudinal apparent diffusioncoefficient (lADC) and transverseapparent diffusion coefficient (tADC).Motoneuron size in the ventral GM wascalculated and correlated to the DTIindices in GM.Results: FA values in the dorsal GM ROIwere significantly higher than the ventralGM in controls, 15 and 25 weeks postinjury groups (P < 0.05). lADC in dorsalROI was significantly higher than inventral GM in controls, 15 and 25 weekspost injury (P < 0.05). The FA valuewithin the entire GM at 25 weeks wassignificantly higher than the FA value at 2weeks post injury (P < 0.05) and the FAvalue in controls (P < 0.05). Groupanalysis of the size of the motor neuronsshowed a 9% increase in the motoneuron
size at 2 weeks (P < 0.01) and 42%increase at 25 weeks (P < 0.01) postinjury as compared to controls.Conclusion: These results suggest changesin gray matter structure rostral from acontusion injury can be detected andmonitored using DTI.
257Comprehensive Assessment of One-year Outcomes After SuboccipitalCraniectomy for Chiari IMalformation in AdultsScott L. Parker, Scott Zuckerman, David Shau, Stephen Mendenhall, Matthew McGirtIntroduction: Suboccipital craniectomy isa commonly performed procedure forChiari I malformation, however, to datethere has never been a study tocomprehensively assess the effectivenessof suboccipital craniectomy using patient-reported outcome (PRO) measures. Inlight of this, we set out to assess theeffectiveness of subocciptal craniectomyfor treatment of adult patients with ChiariI malformation utilizing validated patient-reported outcome (PRO) metrics.Methods: Forty-nine adult patientsundergoing suboccipital craniectomy forChiari I malformationwere included in thisstudy. Baseline and one-yearVAS-Head,HeadacheDisability Inventory (HDI),NeckDisability Index (NDI), physical andmental quality of life (SF-12 PCS&MCS), health-state utility [EuroQol (EQ-5D)], time to return towork, andsatisfactionwith surgerywere assessed.Results: Baseline characteristics providedin Table 1. Each of the PROs assessedwere significantly improved (P < 0.01) atone-year post-operatively, Figure 1.Thirty-nine (80%) patients were satisfiedwith their outcome as assessed by the netsatisfaction index. Thirty-five (72%)patients returned to work by one-yearpost-operatively. Median [IQR] time toreturn to work was 12 [6-45] weeks.Conclusion: Surgical management ofChiari I malformation in adults viasuboccipital craniectomy providessignificant and sustained improvement inpain, disability, and quality of life, asassessed by patient-reported outcomes attwo-years post-operatively. This patient-centered assessment suggest thatsuboccipital craniectomy for Chiari Imalformation in adults is a highlyeffective treatment strategy.
258Repeat Surgery Following LumbarDecompression for Herniated Disc:The Quality Implications of Hospitaland Surgeon VariationBrook I. MartinIntroduction: Repeat lumbar spine surgeryis generally an undesirable outcome.Variation in repeat surgery rates may bedue to patient characteristics, diseaseseverity, hospital characteristics, orsurgeon-related factors. However, little isknown about population variation inreoperation rates. To examine hospital andsurgeon variation in reoperation ratesfollowing lumbar herniated disc surgery inrelation to published benchmarks.Retrospective analysis of a dischargeregistry including all nonfederal acute-care hospitals in Washington State from1997- 2007.Methods:We identified adults whoreceived an initial inpatient lumbardecompression for herniated disc. Weperformed generalized linear mixed-effectlogistic regression, controlling for patientcharacteristics and comorbidity, toexamine the variation in reoperation rateswithin 90 days, 1- and 4-years.Results: Our cohort included 29,529patients with a mean age of 47.5 years,61% privately insured, and 15% havingany comorbidity. The age-, sex, insurance,and comorbidity-adjusted mean rate ofreoperation among hospitals was 1.9% at90 days (95%CI 1.2, 3.1), with a rangefrom 1.1% to 3.4%:, 6.4% at 1 year(95%CI 3.9, 10.6) with a range from 2.8%to 12.5%, and 13.8% at 4 years (95%CI8.8, 19.8), with a range from 8.1% to24.5%. The adjusted mean reoperationrates of surgeons were 1.9% at 90-days(95%CI 1.4 - 2.4) with a range from 1.2%to 4.6%), 6.1% at 1-year (95%CI 4.8% -7.7%) with a range from 4.3% to 10.5%),and 13.2% at 4-years (95%CI 11.3% -15.5%) with a range from 10.0% to 19.3%).Multilevel random-effect models suggestedthat variation across surgeons was greaterthan that of hospitals, and that this effectincreased with longer term outcome.Conclusion:We observed a markedvariation in reoperation rates amongsurgeons and among hospitals for aprimary lumbar discectomy, a relativelysimple spinal surgery. Substantialvariation persisted after adjustments forwere made for patient demographics orcomorbidity, suggesting uncertainty aboutindications for repeat surgery, variations inperioperative care, or variations in qualityof care.
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES68
ORAL POSTER ABSTRACTS

259Relationship Between EffectiveLordosis and Patient Reported NeckPain and DisabilityAlex Riccio, David L. Semenoff, John W. GermanIntroduction:Kyphotic spinal curvature isthought to be associated with pooroutcomes following cervical spine surgeryleading some surgeons to suggest that therestoration of kyphosis should be animportant goal of surgery even if moreextensive surgery were to be required. Todate few studies have specificallyevaluated spinal curvature in non-operativepatients with respect to present day clinicaloutcome measures. It is possible thatpatients who present with a straight orkyphotic spine may have a differentbaseline status with respect to neckdisability and pain than those with alordotic curvature.Methods: Fifty patients who underwent anout-patient evaluation for chronic neckpain were included in this study. Allpatients underwent standing lateral x-raysto determine the presence (ELpr) orabsence (ELab) of effective lordosis asdescribed by Gwinn et al (2009) by twoneurosurgery attendings. All patients alsocompleted self-reported outcome measures(NDI, Neck VAS, SF-12 PCS, and SF-12MCS) at the same clinic visit. Correlationbetween the presence or absence of ELand outcome measures was sought.Outcome measures were compared by t-test and reported as mean,SD.Results:After classifying eachx-raywithrespect toELno statistical difference couldbe found in anyoutcomemeasure:NDI(EFpr: 51.87,18.348,EFab: 48.833, 17.538,P=0.57),NeckVAS (EFpr: 5.61,1.87,ELab: 6.07, 2.56,P=0.51), SF-12PCS(ELpr: 28.94, 9.97, ELab: 33.52, 10.12,P=0.15), or SF-12MCS (ELpr: 44.27, 11.18,ELab: 40.41, 9.51,P=0.23).Conclusion: The absence of EL was notassociated with a statistically significantdifference in baseline patient reportedoutcome measures of neck pain ordisability. Spinal curvature may contributelittle to a chronic neck pain patient’soverall perception of neck pain anddisability.
301Management of IncidentalDurotomy in Minimally-InvasiveSpine SurgeryDmitry Ruban, John E. O’TooleIntroduction: Unintended durotomy is oneof the most common complications inspine surgery that may lead to seriouscomplications if not recognized or treatedproperly. There are few reports onmanagement of durotomies incurredduring minimally invasive spine surgery(MISS). The authors describe theirexperience in a series of consecutiveMISS patients with unintendeddurotomies.Methods:All patients who underwentminimally invasive spine surgery by thesenior author from August 2006 toFebruary 2011 were retrospectivelyreviewed and cases with unintendeddurotomies were identified. A case-controlstudy was carried out comparing patientdemographics and perioperative databetween patients with and withoutdurotomy. Surgical technique, including aproposed algorithm for management ofdurotomies, is described.Results: Unintended durotomy occurred in53 out of 563 patients (9.4%). Mean ageat surgery was 60.7 years (range 30-85).Previous surgery at the same level wasperformed in 5 patients (9.4%). Twopatients underwent posterior cervicalsurgery, and 51 patients underwentposterior lumbar surgery. Decompressionalone was performed in 32 cases (60.4%),and fusion was performed in 21 cases(39.6%). Mean follow-up was 310 days,and there were no CSF-cutaneous fistulas,pseudomeningoceles, or othercomplications referable to durotomy ineither group. Risk factors identified fordurotomy included previous operation atthe same level (P = 0.019) and operationin the lumbar spine region (P = 0.001).Conclusion: In our consecutive series of
patients undergoing MISS, an unintendeddurotomy was associated with fewercomplications than previously reported foropen spinal surgery. We propose a simplemanagement algorithm that includes earlymobilization and results in excellentclinical outcomes with no incidence ofpostoperative CSF-cutaneous fistula orother complications.
302Spinal Cord Injury Bypass Techniquewith Nerve Transfers for theRestoration of Hand Function AfterSpinal Cord Injury: Case Report andReview of the LiteratureWilson Zachary Ray, Andrew Yee, Susan E. MackinnonIntroduction: Nerve transfers using anexpendable nearby motor nerve toreinnervate a denervated nerve haveresulted in more rapid and improvedfunctional recovery than traditional nervegraft reconstruction following brachialplexus and distal peripheral nerve injuries.Through our experience with nervetransfers over the last two decades wehave learned that the nerve to thebrachialis muscle is expendable and theanatomical location of the anteriorinterosseous motor group within themedian nerve in the arm. The authorspresent a single case of restorarion ofsome hand function (finger and thumbflexion) following a complete cervicalspinal cord injury using a brachialis toanterior interosseous nerve (AIN) transfer.Methods: Review the presentation, work-up, treatment and outcome of a patientwith a complete cervical SCI injurytreated with nerve transfers for therestoration of hand function.Results:We report the successfulreinnervation of the AIN to restore somefinger and thumb flexion in a patient witha complete cervical SCI twenty-twomonths after injury.Conclusion: The use of nerve transfers mayrepresent a significant breakthroughtoward improved independent function inselect patients with cervical SCIs.Although limited to only a few casereports it appears that the time frame forperforming nerve transfers following aspinal cord injury is longer than with otherperipheral based lesions. Further studieswill be required to assess reliable clinicaloutcomes and optimal timing for surgicalintervention.
DIGITAL POSTER ABSTRACTS
Visit the Digital Poster Center inNorthern Hemisphere B-E to viewthese abstracts in more detail.
Thursday, March 8 from 9:00 AM to 7:00 PM and Friday, March 9 from 9:00 AM to 2:00 PM.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 69
DIGITAL POSTER ABSTRACTS

303Clinical Outcomes FollowingBrachialis to Anterior InterosseousNerve TransferWilson Zachary Ray, Chester Yarbrough,Andrew Yee, Susan E. MackinnonIntroduction: Brachial plexus injuriesrepresent a significant public healthproblem. Most commonly affecting youngmales, these injuries often leaveindividuals with permanent disability.Involvement of the lower truck canproduce deficits ranging from minimalsensory deficits to complete hand motorparalysis. While the advent of nervetransfers has provided a significantadvance in the treatment of brachialplexus injuries, the majority work reportedto date has focused on upper trunkinjuries. The restoration of elbow flexionand shoulder abduction are usually thehighest priority in large brachial plexusreconstructive procedures. The restorationof hand function is usually of lowerpriority, often leaving individuals withlower trunk involvement with significantdisability. While several authors describeddistal nerve transfers for the hand andforearm, outcome series for these transfersare relatively sparse. In this case series theauthors describe their experience withbrachialis to anterior interosseous nerve(AIN) transfer.Methods: Retrospective review of allpatients treated with brachalis to AINnerve transfers at a single institution.Results:All patients recovered at least M3to M4 strength in both flexor digitorumprofundus and flexor pollicis longusfunction. All patients reported markedimprovement in functional ADLs andquality of life.Conclusion: Restoration of hand functionfollowing brachial plexus injuries canmarkedly improve the patient’s subjectivequality of life. We successfully utilized thebrachialis branch to reinnervate FDP andFPL with good clinical results. Whilepatients with isolated lower trunk injuriesremain relatively uncommon, nervetransfers for the restoration of some handfunction should be considered. Furtherstudies will be required to accuratelyassess the long-term benefit of thistransfer
304Incidence of Vertebral Artery Injurywith Traumatic Cervical SpineSubluxationsKamran Parsa, Omid R. Hariri, FaridJamshidian, Dan Miulli, Javed SiddiqiIntroduction: The incidence of vertebralartery injuries in traumatic cervical spinesubluxations has been reported to bevariable, 3%-88% [1-5]. The purpose ofthis study is to investigate the incidence ofvertebral artery injuries at our institution,the second busiest trauma center insouthern California.Methods: Retrospective data collectedfrom our institution’s trauma registry fromJanuary 2000 – June 2011. Search criteria:(1)All traumatic cervical spine fracturespresenting to the emergency room (2)Alltraumatic subluxed cervical spine,(3)Subluxed cervical spine injuries andvertebral artery injuries. Exclusioncriteria: (1)Injury occurring because ofdamage to subclavian artery, (2)Injuryoccurring because of damage to neck softtissue.Results: 852 patients (582 male, 270female) presented with traumatic cervicalspine fractures. 102-(12%) had cervicalspine subluxation injuries. 13 hadsubluxed cervical spine injuries withvertebral artery injuries. This is 1.5% [P <0.01, 95% confidence interval (CI) of0.00-0.02] of all cervical spine fractures,and 12.7% of all traumatically cervicalsubluxation patients. The anatomicalcharacteristics of injury were: 5-(38.4%)involved severe fracture with subluxationresulting in translocated vertebral bodies,5-(38.4%) involved vertebral arteryocclusion secondary to a perched facetand minor subluxation, 2-(15.4%) gunshotwounds associated with fractures andvertebral artery occlusion, 1-(6.6%)vertebral artery dissection associated withsimilar severe fracture and subluxation.According to the Blunt CerebrovascularInjury (BCVI) Grading: 1-(6.6%) Grade V(transection), 9-(69.2%) Grade IV(occluded), 3-(23.1%) Grade II(dissection).Conclusion:At our institution over the past11.5 years, our data suggests a 1.5%incidence of vertebral artery injuriesassociated with traumatic subluxation andfractures. There was no incidence ofvertebral artery injury without a fracture.Compared to the most recent report byMueller et al [5] and other major studies,our results fall below the lowest range of3%. Occlusion (Grade IV) was the mostcommon form of vertebral artery injury.
Thus, in patients with cervical spinesubluxation, vertebral artery injuries arenot relatively frequent.
305Sacral Dural Arteriovenous Fistula:Usefulness of Multidetector-rowCT(MDCT) and Report of 4 CasesTomohiro Murakami, Izumi Koyanagi,Takahisa Kaneko, Satoshi Ookawa, Kei Miyata, Satoshi Iihoshi,Nobuhiro MikuniIntroduction: Sacral dural arteriovenousfistula (dAVF) is a rare entity in spinalarteriovenous malformation. It is wellknown that feeding arteries of this regionare branches of the internal iliac arteries,so it is difficult to detect and identify thesefeeding arteries. The purpose of this studyis to analyze and to evaluate usefulness ofmagnetic resonance (MR) imaging andmultidetector-row CT (MDCT) findings inthe sacral dAVF.Methods: This retrospective studyincluded four cases (three men, onewoman and mean aged 69 years) of sacraldAVF. We assessed the following: clinicalsymptoms, MRI and MDCT findingsfollowed by comparing with spinal digitalsubtraction angiography (DSA) findings.Results: The clinical symptoms weremotor weakness of both lower extremitiesand sensory disturbance in all cases. OnT2-weighted images of all cases, spinalcord had hyperintensity area below Th6level and many flow voids. From theseresults we could diagnose spinal dAVF butit was difficult to detect and identify thefeeding arteries. MDCT revealed dilateddraining vein around the spinal cord in allcases. Especially, dilated venous drainersalong S1 or S2 root or filum terminalefrom sacral bone were indeedcharacteristic findings in the sacral dAVF,which were fed by lateral sacral artery inthree, L5 segmental artery in one. Thesefeeders were identified precisely usingspinal DSA.Conclusion: Clinical symptoms of sacraldAVF had no specific differentciationcompared with other regions dAVF. MRIwas less invasive and useful for analysisof intra-spinal abnormalities but the fieldof view was limited. MDCT was usefulfor the diagnosis of sacral dural AVF, andcould be helpful for the indentification offeeding arteries before spinal DSA.
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES70
DIGITAL POSTER ABSTRACTS

307Carpal Tunnel Surgery: A NovelMethod with Preliminary Results in52 PatientsBruce M. McCormack, Edward F. Eyster,Michael J. Kaplan, William W. Bowen,Stephen Gunther, Jonathan J. LinthicumIntroduction: This is a retrospective reviewof 52 patients with carpal tunnelsyndrome (CTS) treated with theMANOS™ Carpal Tunnel Release device.Methods: The Manos™ Carpal TunnelRelease device is a carpal tunnel bladethat releases the transverse carpal ligamentwith wrist and palm skin punctures assmall as 2.1 mm. A standard disposablenerve stimulator and awake patientprovide feedback as the surgeon navigatesa 14 gauge blunt probe across theundersurface of the ligament from a wriststab wound. The leading tip is insulatedand conducts 2 milliamps. The surgeonconverts the blunt insulated probe into anuninsulated blade by advancing a 17gauge sharp through the palm with athumb activated trigger. The surgeon sawsthe ligament through the two skinpunctures. A validated outcomequestionnaire was used to retroactivelyassess properative symptoms andpostoperative symptoms at three months.Results: Symptom severity and functionalstatus scores were improvedpostoperatively and compare favorably toliterature controls for open andendoscopic surgery at three months. Onepatient required reoperation forincomplete release. There were no tendonor nerve injuries.Conclusion: Preliminary results suggest theManos™ Carpal Tunnel Release device tobe safe and effective.
308Facet Joint Contact Pressure Is NotSignificantly Affected by ProDisc-CDisc Arthroplasty in Sagittal Bending:A Single Level Cadaveric StudyJoel A. Bauman, Nicolas V. Jaumard,Benjamin B. Guarino,Christine L. Weisshaar,Daniel E. Lipschutz, William Charles Welch,Beth A. WinkelsteinIntroduction: Total disc arthroplasty is amotion-preserving spinal procedure thathas been investigated for its impact onspinal motions and adjacent leveldegeneration. However, the effects of discarthroplasty on facet joint biomechanicsremain undefined despite the critical roleof these posterior elements in guiding andlimiting spinal motion. Therefore, thepurpose of this study was to measure the
pressure in the facet joint in cadaverichuman cervical spines subjected to sagittalbending prior to and after implantation ofthe ProDisc-C.Methods: Seven C2-T1 osteoligamentouscadaveric cervical spines wereinstrumented with a transducer to measurethe C5-C6 facet pressure profiles duringphysiologic sagittal bending, before andafter implantation of a ProDisc-C at thatlevel. Rotations of the index segment andglobal cervical spine were also quantified.Results: The mean C5-C6 range of motionsignificantly increased (P = 0.009) from9.6 ± 5.1° in the intact condition to 16.2 ±3.7° after implantation. However, despitesuch changes in rotation, there was nosignificant difference in the facet contactpressure during extension between theintact (64 ± 30 kPa) and implanted (44 ±55 kPa) conditions. Similarly, there wasno difference in facet pressures developedduring flexion.Conclusion:Although implantation of aProDisc-C arthroplasty device at the C5-C6 level increases angular rotations itdoes not significantly alter the local facetpressure at the index level in flexion orextension. Using a technique thatpreserves the capsular ligament, this studyprovides the first direct measurement ofcervical facet pressure in a discarthroplasty condition.
309Clinical Outcomes of UnstableThoracolumbar Burst Fractures:Combined Posterior Short SegmentCorrection Followed byThoracoscopic Corpectomy andFusionWilson Zachary Ray, Khaled M. Krisht,Erica Fay Bisson, Andrew T. Dailey, Meic H. SchmidtIntroduction: The surgical management ofthoracolumbar burst fractures varieswidely among treated clinican. Theauthors review their experience withanterior thoracoscopic corpectomy andshort segment posterior fusion for thetreatment of unstable thoracolumbar burstfractures.Methods:A retrospective chart reviewidentified all patients treated by a singlesurgeon at our institution from 2002 to2009 with anterior thoracoscopiccorpectomy and fusion followed by short-segment posterior fusion for unstablethoracolumbar burst fractures.Demographic data, mechanism of injury,classification of fracture, Cobb angle,American Spinal Injury Association score,
associated injuries, tobacco use, follow-upduration, and radiographic studies were allcollected. Outcomes were assessed forfracture alignment (preoperative,postoperative, and long-term follow-upkyphosis), rate of fusion, neurologicaloutcome, and treatment complications.Results:Thirty-four patients were identified,including 25 with lumbar fractures and 9with thoracic fractures. At a mean follow-upof 19 months, 91% of patients haddemonstrated radiographic evidence offusion and 87% retained the correction oftheir kyphotic deformity. There were threecomplications in the series.Conclusion: Thoracoscopic anteriorcorpectomy with short segment posteriorfusion represents an alternative totraditional open treatment ofthoracolumbar burst fractures. Athoracoscopic approach allows for a short-segment posterior fusion, reducing theloss of adjacent motion segments,minimizes morbidity associated withtraditional open anterior approaches,allows for anterior and posterior columnstabilization, and is associated with a highrate of bony fusion and maintenance ofkyphotic correction.
312Do Porous Tantallum Implants Inducea Radiologically DetectableOsteosintesis? Results from theAnalyses of X-rays and 3D CT ScansObtained in a Series of 83 PLIFProceduresMario Ganau, Franco Ennas, Laura Ganau, Alberto MaleciIntroduction: The high volumetric porosity(70%-80%), low elasticity modulus(3MPa), and high friction characteristicsof porous tantalum metal (PTM) make it abetter conductive material than titanium tobiologic fixation. Several in-vitro studies,although showing differences inexpression levels of bone matrix markersdependent on the age and gender of cell’sdonors, confirmed that PTM is a goodsubstrate for the attachment, growth anddifferentiated function of humanosteoblasts. Indeed, its introduction in themarket of spinal surgery devices hasyielded theroretically better fixationqualities and a so called “gap filling”effect, particularly valuable for patientswith compromised bone foaming abilities(i.e. osteoporosis).Methods: To test, clinically andradiologically, the properties of PTMcages a prospective non-randomised studywas conducted on 83 consecutive patients
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 71
DIGITAL POSTER ABSTRACTS

implanted with PTM cages during PLIFsurgery for degenerative spondylolisthesis,discopathies or segmental stenosis. Everypatient from this cohort was assessed byVAS/ODI test and underwent X-rays/CTscans of the lumbar spine 6 months afterintervention and later on after at least 2years.Results: No migration of implants in aventral/dorsal direction or sideways wasdetected, no implant subsidence in arotation/flexion fashion, nor osteolyticlesions between the cage and adjacentbone were noticed. Evaluation of boneingrowth into the cage was difficult due tothe high X-ray constrast effect of thematerial, nevertheless high qualitybridging fusion lateral to the cages wasseen on 3D CT scan in almost everypatient despite the gender or the age. Theclinical improvement is in agreement withthe stability and fusion achieved.Conclusion:While we can’t confirmclinically any difference in bone ingrowthdependent on the age and gender of thepatients, the good radiological results interms of spinal fusion and absence ofimplant subsidence or complications leadus to conclude that PTM seems an effectivematerial for spinal surgical devices.
313Postoperative Urinary Retention inElective Spinal Surgery PatientsDavid J. Altschul, John K. HoutenIntroduction: Postoperative urinaryretention (POUR) is a common problemin patients undergoing surgery. This studyinvestigates its incidence in patientsundergoing elective spine surgery andattempts to identify significant riskfactors.Methods:All elective spine surgerypatients were monitored for POUR over aconsecutive four-month period. Datacollected included operative dataincluding operative positioning, surgeryduration, fluid administration, and bloodloss as well as patient characteristicsincluding age, sex, and medicalcomorbidities.Results: 131 patients were included in thestudy. 28 of these patients (18.3%)developed POUR. There was nosignificant difference between groups withregard to age, gender, use ofinstrumentation, foley placement, orsurgery duration. Using chi-squaredanalysis, the urinary retention group had ahigher percentage of thoracic/lumbar (P =0.002) and posterior (P = 0.045) positionprocedures. A multivariate analysis
revealed that diabetes (P = 0.01) andvolume of intraoperative fluids (P = 0.05)were significantly different betweengroups, with the odds ratios fordeveloping POUR with intravenous fluids> 2.0 liters was 3.9, having a history ofdiabetes mellitus was 4.2, and having apost-op UTI was 3.4.Conclusion: POUR in elective spinesurgery is common. Patients with diabetesand those receiving more than 2.0 litersintravenous fluids had significantly higherincidence of POUR. Knowledge of theincidence of POUR may be useful inevaluating postoperative spine surgerypatients for cauda equina syndrome fromhematoma insofar as that retention may,without other neurologic signs andsymptoms, be insufficient grounds foremergent imaging.
314The Use of Three-dimensional Image-guidance for Redirecting PedicleScrews in Revision Spinal FusionEric W. Nottmeier, Douglas S. Fenton, Todd Leibowitz, Stephen M. PirrisIntroduction: For patients undergoingrevision spinal surgery, adequateredirection of previously misplacedpedicle screws can be challengingsecondary to the tendency of theredirected screw to follow the cortically-lined tract of the previously misplacedscrew. Additionally, placing a new screwdown a previously misplaced pediclescrew tract can have an unfavorableclinical result in a patient that may havebeen symptomatic from the previouslymisplaced screw. The authors report theirexperience with the use of cone beamcomputed tomography (cbCT)-based,three-dimensional (3D) image guidancefor redirection of pedicle screws inpatients undergoing revision spinal fusionprocedures.Methods: The charts and radiologicalstudies of 20 patients undergoing revisionspinal fusion with redirection of pediclescrews were retrospectively reviewed.Thirty-five pedicle screws were redirectedin these patients using cbCT-based, 3Dimage guidance (Table 1). Five patients inthis cohort had neurologic symptomsrelated to a previously misplaced pediclescrew, none of which were aware that theywere harboring a misplaced pedicle screw.There were 7 redirected pedicle screws inthis study that were not previouslymisplaced, but were close to the medial orinferior border of the pedicle and couldnot be safely upsized. Redirection of new
screws down a different trajectory wasaccomplished with image-guided probes,taps, and screwdrivers (Fig. 1). Anindependent radiologist graded pediclebreach in the screws that were previouslymisplaced, as well as the redirectedscrews using the system described byMirza et al.1Results: No complications occurred in thisstudy as a result of image guidance orredirection of pedicle screws. Four pediclescrews were redirected using an in-out-intechnique and these screws were left outof the breach analysis. No pedicle breachwas noted in the 31 redirected pediclescrews that underwent breach analysis.Conclusion: Redirection of pedicle screwscan be accomplished safely andeffectively with the use of cbCT-based,3D image guidance.
315Stereotactic Navigation with the O-arm for Placement of S2 Alar-IliacScrews in Pelvic-Lumbar FixationWilson Zachary Ray, Erica Fay Bisson,Meic H. Schmidt, Andrew T. DaileyIntroduction: Fixation to the pelvis is acrucial adjunct to many lumbar fusions inorder to avoid L5-S1 pseudoarthrosis.Pelvic fixation is useful for treatment ofkyphoscoliosis, high-gradespondylolisthesis, L5-S1 pseudoarthrosis,sacral tumors, lumbosacral dislocationsand osteomyelitis. The most popularmethod, iliac fixation, has drawbacksincluding hardware prominence, the needfor extensive muscle dissection and theneed for connection devices. As a result,S2 alar-iliac fixation provides a usefulprimary or salvage alternative. Wedescribe our techniques using stereotacticnavigation for screw placement.Methods: Twelve patients had computerassisted S2 alar-iliac fixation over a 12month period. The O-arm ImagingSystem allowed for CT quality multi-planar reconstructions of the pelvis andregistration to a Stealth Treon Stationprovided intraoperative guidance. Sixpatients had a diagnosis of kyphoscoliosis,2 had L5-S1 pseudoarthrosis revision, 2had tumor, 1 had salvage of failed iliacscrews and 1 had distal adjacent segmentdegeneration.Results:All patients had bilateralplacement of the screws with lengthranging from 80-100 mm. All placementswere confirmed with a second multiplanarreconstruction. One screw was moved dueto apparent anterior breach of the ilium.There were no immediate or delayed (4-
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES72
DIGITAL POSTER ABSTRACTS

12 months) neurological or vascularcomplications from screw placement. Thelength of the screws required additionalinstruments including a longer pediclefinder and tap.Conclusion: S2 alar-iliac fixation provideslower profile fixation and often can beperformed without the need forconnection devices. In addition, placing ascrew across two corical surfaces of thesacral alae as well as the cortex of theilium and the thick cortical bone above thesciatic notch should provide superiorbiomechanical fixation. Placement can beachieved without more extensive muscledissection or separate fascial incisions.
316Chiari I Malformation Assessmentwith Intraoperative DopplerUltrasoundBennett Blumenkopf, Alexander Kwong-Tak Yu, Zachary G. Wright, Larry Guraly, Brandon ChewIntroduction: Chiari I malformation is adebilitating disorder resulting fromcerebrospinal fluid (CSF) obstruction atthe level of the foramen magnum. Patientstypically present with headache and lowercranial nerve symptoms. Objectivefindings suggesting obstruction are oftenspeculative, especially when using staticmagnetic resonance imaging (MRI)[ref.1].Cine MRI is useful pre-operatively, but isnot typically available intra-operatively.Ultrasound provides real-time assessment,and Doppler ultrasound assessment offlow [ref.2]. These were evaluatedtogether as a modality to objectivelydetermine the presence of CSFobstruction and flow across the foramenmagnum before and after Chiari Idecompression.Methods: In a series of patientsultrasonography (HDI 5000 ATL with C8-5 8mHz probe) was utilized aftersuboccipital craniectomy with C1laminectomy was performed. Prior to thedural opening, routine ultrasound wasused to assess parenchymal pulsation,whereas, Doppler ultrasound was used todetermine CSF flow at the level of theforamen magnum. Dural expansion usingbovine pericardium was then performed ineach patient. Studies were repeated priorto wound closure.Results: Prior to the dural opening,ultrasound revealed nil to minimalpulsation of the cerebellum and tonsils,Doppler studies showed no CSF flowacross the foramen magnum. After the
duraplasty, routine ultrasound revealedpulsatile neural elements and the Dopplerultrasound clearly depicted flow throughthe decompression and across the foramenmagnum.Conclusion: Doppler ultrasound proved aneffective, easy to use real-time imagingtechnique intraoperatively for theconfirmation of CSF obstruction, and toassure the adequacy of suboccipitaldecompression with the re-establishmentof CSF flow across the foramen magnum,in patients undergoing Chiari Idecompression
317Part II: The Safety and Efficacy of1.05 mg of rh-BMP-2 in MinimallyInvasive Transforaminal LumbarInterbody FusionsLuis M. Tumialan, Frederick F. Marciano,Nicholas TheodoreIntroduction: The recent literature hasreported a significant complication rate inlumbar interbody fusions with rh-BMP-2.The doses in these reports are varied anddoses as high as 12.1 mg in the interbodyspace have been reported. The purpose ofthis report is to review the experience of42 consecutive minimally invasive singlelevel transforaminal lumbar interbodyfusions with 1.05 mg of rh-BMP-2.Methods: The authors prospectivelyfollowed 42 consecutive patients whounderwent a minimally invasive singlelevel transforaminal lumbar interbodyfusion. Preoperative and postoperativevisual analogue scores (VAS), OwestryDisability Index (ODI) and StandardForm-36 (SF-36) were collected. The doseof rh-BMP-2 that was utilized within theinterbody spacer was 1.05 mg. Patientswere monitored for the knowncomplications that have been reported, inparticular, heterotopic bone formation,osteolysis and seroma formation.Results:A total of 42 patients underwent asingle level minimally invasive TLIF.Mean follow-up was 10.8 months. Themean preoperative ODI, VAS and SF-36were: 45.7, 7.2 and 16.7 respectively. Themean postoperative values were 16.4, 3.7and 32.8 respectively. There were nocomplications related to heterotopic boneformation, seroma formation or osteolysisduring the immediate or long termpostoperative period. One patient requireda reoperation for persistent symptomscontralateral to the side of the TLIF. CTand MR imaging of this patient did notreveal any evidence of seroma in thevicinity of the TLIF or heterotopic bone
formation. At six months 36 patients(86%) demonstrated fusion within theinterbody device.Conclusion:A dose of 1.05 mg of rh-BMP-2 is not associated with the variouscomplications reported in the literatureand appears to be sufficient to result inadequate bone formation within theinterbody device. This study reinforces thedose related consequences of thistechnology and also demonstrates thatwhen rh-BMP-2 is used at a low dosecontained within an interbody spacer, itmay be safely used in transforaminalapproaches.
318Should Asymptomatic DegenerativeDiscs Be Included in a Two-levelAnterior Cervical Discectomy andFusion? A Decision AnalysisMaxwell BoakyeIntroduction: The annual incidence ofadjacent segment disease (ASD) rangesfrom 1.5-4% with 10 year estimates ashigh as 25% after anterior cervicaldiscectomy with fusion (ACDF). Theincidence and rate of development of ASDis higher in patients with preexistingasymptomatic adjacent degenerative discs(AADD). A diagnosis of ASD often leadsto additional surgery. Given the risks ofASD and need for additional procedures,the question arises whether AADD’s inpatients with two-level cervical discdisease should be preemptively treatedwith fusion. Decision analysis is a toolthat can aid in surgical decisions in theabsence of randomized controlled studies.The goal of this paper is to perform adecision analysis regarding whether atwo- level ACDF should be performed fora patient with two-level cervical discdisease, of which one level isasymptomatic.Methods: Decision analysis wasperformed using Treeage Pro Suite 2008.Probabilities and utilities of alternativeoutcomes in the decision tree wereassigned based on peer-review literature.Roll-back analysis determined the optimaltreatment. Sensitivity analyses and MonteCarlo simulations were performed toidentify effects of varying modelparameters.Results: Roll-back analysis providedexpected values of 0.92 vs. 0.84 in favorof observation as the optimal decision.Sensitivity analysis identified theprobability of developing ASD and thelikelihood of surgery given a diagnosis ofASD as the most critical parameters
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 73
DIGITAL POSTER ABSTRACTS

influencing the decision. Observation wasthe preferred strategy at all values ofprobability of ASD less than 100%. At aprobability of ASD of 100%, fusion wasthe preferred strategy only when theprobability of surgery for ASD was 66%or greater or the utility assigned tosuccessful nonoperative management was0.84 or less.Conclusion: Observation was the preferredstrategy for management of AADD giventhe probabilities and utilities utilized in thedecision analysis model. The study islimited by unavailability of preciseestimates of the probability ofdevelopment of adjacent segment diseaseand the probability of surgery afterdiagnosis of adjacent segment disease, themost critical factors influencing thedecision. However the conclusions wererobust given wide ranges used for theseparameters in the sensitivity analysis.
319Racial Disparities in ComplicationRates and Resource Utilization AfterSpinal Surgery for Lumbar StenosisMaxwell Boakye, Beatrice UgiliwenezaIntroduction: Recent reviews suggestwidespread racial disparities in surgicalcare. There have been limited studies ofracial disparities in outcomes after spinalsurgery. The goal of this study is tocompare outcomes after surgery forlumbar stenosis between AfricanAmerican (AA) and White patients.Methods:We used the Medicaid databaseof the Thomson Reuter’s MarketScan.African American and Non-HispanicWhite patients who underwent alaminectomy or a fusion as a primaryprocedure for a concurrent primarydiagnosis of lumbar stenosis wereconsidered for the study. We retainedpatients who had at least two years post-operative continuous enrollment. Risk ofpost-operative complications and re-operation were compared usingmultivariate logistic regression, in-hospitaldays and healthcare resources chargeswere compared using generalized linearmodels, and the number of post-operativeall-type outpatient services, EmergencyDepartment outpatient services,prescribed medications were comparedusing negative binomial models. Data pre-processing and statistical analysis wereperformed in SAS 9.2.Results:A cohort of 1263 patients(12.97% AA) was obtained. Four hundredand fifty of them had two years post-operative continuous enrollment. The
average age in this group was 59 years(standard deviation- SD: 12 years) and72.67% were females. One-year, two-yearre-operation rates as well as post-operativehealthcare resources utilization andcharges were statistically similar in bothracial groups. During the indexhospitalization, AA patients hadsignificantly longer hospital stays (mean:5 days, SD: 5 days, vs. mean: 3 days, SD:2 days, p-value < 0.0001) and highercharges (mean: $34,686, SD: $30,551 vs.mean: $25,886, SD: $32,668, p-value =0.0002). also, AA patients hadsignificantly higher wound complicationrates in comparison to White patientsduring the index hospitalization (9.92%vs. 3.13%, OR: 3.13, 95% CI: 1.27-7.72,p-value = 0.013), 30 days (11.45% vs.4.39%, OR: 2.6, 95% CI: 1.16-5.83, p-value = 0.013), after surgery and 90 daysafter surgery (11.45% vs. 5.02%, OR: 2.3,95% CI: 1.05-5.02, p-value = 0.037).Conclusion: During the surgeryhospitalization, the AA race wasassociated with longer stays and highercharges. After surgery for lumbar stenosis,AA patients had higher wound relatedcomplication rates. All other post-operative outcomes were not found to bestatistically different.
320Presacral L5-S1 Interbody Fusion(AxiaLIF) for Obese Patients withLumbosacral Degenerative DiseaseFrederik Pennings, George Malcolmson,John P. WeaverIntroduction: Obesity (BMI>30) is amedical condition that significantlyincreases the morbidity and mortality ofspinal procedures and limits the surgeonsability to perform traditional open fusionprocedures. Therefore, minimally invasivespine procedures that reduce the amountof tissue destruction, blood loss andoperative time may be beneficial for the(morbid) obese patients. An AxiaLIF is anovel minimally invasive presacralapproach to treat symptomaticdegenerative spinal pathologies of thelumbosacral segment. We conducted thisstudy to invesitgate the clinical outcomeand fusion rates in obese patientsundergoing the AxiaLif procedure.Methods: In a prospectively followedstudy population of twenty-six patientsundergoing an AxiaLIF for single levelL5-S1 pathology, eleven patients fulfilledthe criteria of obesity. The VisualAnalogue Score (VAS) and OswestryDisability Index (ODI) were assessed pre-
operatively, at 3, 6, 12 and 24 months aftersurgery. Computer tomography wasobtained at 6 months and 12 months todetermine fusion status. In addition, dataon hospital stay time, operative time,blood loss, complications and reoperationrate were collected.Results: The mean BMI was 37 ± 6 (range30-47). Significant improvement occurredin back pain severity and functionalimpairment. Mean ODI scores improvedfrom 59 ± 16% to 25 ± 15% at 24 months.The mean pain score improved from 74 ±21 pre-operatively to 36 ± 36. The overallradiographic fusion is 82%. However,thetwo non-fused patients had osteoporosis.No surgical complications occurred. Thetotal operative time was 108 ± 13 min, theaverage blood loss was 20 ± 19 cc. Theaverage hospital stay was 37 ± 22 hrs.Conclusion: The AxiaLIF provides a safe,fast and reliable minimally invasivesurgical access to the lumbosacralsegment in morbid obese patients withgood clinical and radiographical outcome.The absence of serious side effects andshort hospital stay will reduce cost oftreatment for this patient population.
321Epidural Tuberculosis Involving theEntire SpineJacob MathewIntroduction: This study is a case reportdescribing the clinical features andradiological presentation of epiduralspinal tuberculosis involving the entirespine and its optimal management. Thisrare clinico-radiological presentation hasnever been reported in the literature.Methods:We discuss an elderly male whodeveloped back pain, rapidly progressingparaparesis and urinary retentionconsequent to L5-S1 spinal tuberculosiswith dissemination of epidural tubercularabscess and granulation tissue to thecervical, thoracic, lumbar and sacralregions. The thoraco-lumbo-sacralpathology was tackled by L5 laminectomyand decompression along with aminimally invasive technique for theepidural extension superiorly andinferiorly. Subsequently he was found tohave clinical and radiological evidence ofextensive cervical extradural compressionwhich required cervical laminectomy.Results:At 9 months follow up with anti-tubercular treatment he had excellentneurological improvement. MRI screeningof the entire spine showed completeresolution of the disease.Conclusion: This report illustrates a rare
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES74
DIGITAL POSTER ABSTRACTS

presentation of spinal TB involving theentire spine which has never been reportedpreviously. We suggest that screening ofthe entire spine should be done in selectcases of spinal TB based onsymptomatology. In spite of the advancedage and complexity of the illness, thispatient could be managed optimally and agood outcome was achieved.
324Kinematic Assay of Multi-LevelAnterior Cervical Discectomy andFusion with Supplementary FacetScrew InstrumentationPatrick Devin Leahy, Kirk C. McGilvray,Jonathan D. Sherman, Vincent C. Traynelis, Eric W. Nottmeier,Vaneet Singh, Brian Murrell, Vikas V. Patel,Christian M. PuttlitzIntroduction: One-level anterior cervicaldiscectomy and fusion (ACDF) operationsdemonstrate high clinical fusion rates(~95%). In contrast, attaining sufficientrigidity to achieve intervertebral fusion inmulti-level ACDF operations isformidable. We hypothesized thattransarticular facet screws would decreaseacute range of motion (ROM) of themulti-level ACDF. A kinematic analysis ofcadaveric cervical spines following athree-level ACDF supplemented withunilateral and bilateral trans-facet screwswas performed to test this hypothesis.Methods: 1.5 N-m moments were appliedto C2-T1 human spines (n=8) in the axialrotation, flexion and extension, and lateralbending directions. Loadings wereimposed on C2 with a robotic actuatorwhile T1 was bound to a force sensingtransducer. A typicalstereophotogrammetric technique assessedintervertebral rotations. Each spine wastested in four surgical forms: 1) Untreated,2) standard multi-level ACDF betweenC4-C7, 3) ACDF including Unilateralfacet screws between C4-C7, and 4)ACDF including Bilateral facet screwsbetween C4-C7 (Figure 1). ACDFhardware was comprised of the 3-levelATLANTIS VISION® anterior cervicalplate with variable-angle screws at themore superior levels, fixed-angle screws atthe caudal level, and VERTE-STACK®PERIMETERTM XS polyetherether ketone (PEEK) spacers. TheTOWNLEYTMTRANSFACETPEDICULAR ScrewFixation System was utilized for facetfixation.Results: ROM declined at the treatedlevels following each operation. The
decrease in ROM relative to the Untreatedcase was 74.9%, 87.7%, and 93.5% forthe ACDF, Unilateral facet fixation, andBilateral facet fixation cohorts,respectively. Bilateral facet fixation wasthe only treatment to consistently furnish astatistically-significant (P < 0.05)decrease in ROM over the standard ACDF(Figure 2).Conclusion: Bilateral facet screwsdemonstrated a significant reduction inacute ROM vs. the standard ACDFoperation. Thus, bilateral facet screwsupplementation may be applicable forimproving ACDF acute stability.
326Axonal Misdirection in a FemoralNerve Neuroma in Continuity InjuryModelJacob D. Alant, Joanne Forden, Rajiv MidhaIntroduction:Management of traumaticneuroma-in-continuity (NIC) posesongoing challenges to peripheral nervesurgeons. Axonal misdirection with non-specific reinnervation, frustratedregeneration and axonal attritionfollowing NIC injuries, are believed to beamong the anatomical substrates thatresult in poor functional recovery andneuropathic pain. We hypothesize thatunlike crush injuries, NIC injuries wouldresult in axonal misdirection similar totransection injuries.Methods:A malleus nipper (MN) wasmodified and calibrated to exert a range ofintense uniform compression forces(Fig.1). Histological NIC features werereproduced in vivo when sub-transectioncompression forces were applied to nerveswith 3-second malleus nippercompression and optimized incombination with simultaneous 50gtraction with a spring scale hooked aroundthe nerves. 42 male Lewis rats wererandomized into one of 7 groups of 6 ratseach for left femoral nerve surgeries(Fig.2). At 28 days, Fast Blue and DiIwere respectively applied distally, to themain motor and sensory divisions of thenerves for retrograde labeling of spinalcord motor neurons. Distal nervesegments were also harvested at this timefor histomorphometry. 13 days later spinalcords and femoral nerves were harvestedfor longitudinal cryostat sectioning,counting of fluorescently labeled neuronsand histological evaluation of injuryzones.Results:Axonal misdirection and motor-neuron counts of the (MN+50g)x2 group
showed statistically significant differencescompared to the sham and crush groups,similar to the transection andtransection+repair groups (Fig.3). Otherresults are still pending.Conclusion: So far our results furthercharacterizes this injury model bydemonstrating a high degree of axonalmisdirection and attrition in severe NICinjuries, consistent with long heldtheories. This NIC model may serve as atool to help us to better understand thepathology of these devastating injuries inorder to catalyze a breakthrough in earlydiagnostic and intervention strategies andultimately lead to improved patientoutcomes.
327Lumbar Spine Annulus Yield MayContribute to InstabilityJamie BaisdenIntroduction: Elevated single cycle orrepeated loading leads to failure of lumbarintervertebral disc fibers. This contributesto increased segmental flexibility,accelerated disc and facet degeneration,and eventual instability. Mechanicalyielding of annular fibers occurs prior toultimate failure and results in decreasedstiffness. This study outlined lumbarannular fiber yield characteristics tohypothesize whether yielding maycontribute to segmental instability.Methods: Intervertebral discs obtainedfrom 5 cadaveric specimens were gradedas mildly degenerated according to anaccepted scale. Specimens obtained froma single annular layer, with all fibersrunning in parallel, were quasi-staticallydistracted to failure in an environmentalchamber simulating in vivo conditions.Axial force and displacement wererecorded and normalized to stress/strainbased on initial specimen dimensions.Results:Mechanical yield occurred priorto ultimate failure in all specimens andwas characterized by a decrease in slopeof the stress-strain curve. Yield andultimate properties were not dependentupon spinal level. Yield occurred at 80%of the stress and 75% of the strain toultimate failure. Post-yield modulus (e.g.,slope of the stress-strain curve betweenyield and ultimate failure) was 54% of theelastic modulus (e.g., slope of the stress-strain curve in the physiologic region).Conclusion:Mechanical yield of annularfibers occurs early in the tissue strainresponse, leaving 20-25% reservestrength/extensibility in the fibers.However, once yielded, fiber stiffness
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 75
DIGITAL POSTER ABSTRACTS

decreased by 46%. This early occurrenceof yield and considerably decreased post-yield stiffness may play a role insegmental instability as it occurs at only75% of the total fiber extensibility andmay add considerable flexibility to thedisc. Normal activities coupled with age-related changes may “push” limitsespecially in specific populations whereinroutine loading of the back occurs andaccelerate degenerative effects to the spinethrough the annulus yield mechanism.
328Part I: Observations on BoneMorphogenetic Protein inTransforaminal Lumbar InterbodyFusionsLuis M. Tumialan, Mark A. Mahan,Frederick F. Marciano, Nicholas TheodoreIntroduction: Ectopic bone formation,radiculopathy, seroma development andosteolysis have been identified in TLIF’swith rhBMP-2. ALIFs with rhBMP-2 inlumbar tapered cages, however, have notexhibited the same pattern ofcomplications.Methods:A retrospective review ofclinical and radiographic data wasperformed on all patients over a three yearperiod who had undergone lumbarinterbody fusion through either atransforaminal or anterior approach withrh-BMP-2. The milligram doses of rh-BMP-2 were correlated withcomplications and outcomes.Results: Thirty-six patients wereretrospectively reviewed over a 3 yearperiod. Delayed radiculopathy, ectopicbone formation and osteolysis were allidentified within the group (4 of 36patients or 11% of the series). A delayedradiculopathy after a transforaminallumbar interbody fusion appears to be theresult of an inflammatory response of rh-BMP-2 interacting with the exposedcancellous bone from the facetectomy.The area of hyperintensity on T2 weightedMR imaging obtained 9-12 weekspostoperatively is highly predictive ofwhere bone deposition will occur. Boneformation has a tendency to form outsidethe collagen sponge and in the presence ofthe rh-BMP-2 solution that is in contactwith the cancellous bone. This findingappears to be dose related. Violation of thecortical endplate and exposure of thecancellous bone appears to be the cause ofosteolysis. None of these complicationswere identified in those patients whounderwent an ALIF with the same orgreater amount of rh-BMP-2.
Conclusion:A lower dose of rh-BMP-2(1.05 mg), eliminating the exposure of rh-BMP-2 solution to the neural elementsand limiting the rh-BMP-2 enhancedsponge to an interbody device to avoid itscompression, collectively minimizes therisk of delayed complications from use ofthis protein. A prospective study applyingthese principles will be subsequentlyreported.
329Pressure Ulcer Prevention DuringProne Position Spinal SurgeryMasahiko Akiyama, Shigekuni Tachibana,Hiroki Ohashi, Satoshi Tani, Toshiaki AbeIntroduction: Prevention of pressure ulcerformation is one of the issues duringprone position spinal surgery. One of themajor causes for pressure ulcer formationis direct compression of patient body tothe operating table. We have tried the besteffort to decompress local pressure sitesusing silicone gel pad, however,epidermolysis or blister formation havebeen occurred in some patients, which ledto be one of major complaints aftersurgery. We have hypothesized that notonly direct compression but frictionbetween patient body and operating tablecould contribute for pressure soreformation. We started to apply babypowder to patient body and silicone gelpad to reduce the friction.Methods: 110 patients, who underwentprone spine surgery, have been appliedthis method since April 2009.Results: No epidermolysis or blisterformation have occurred except onepatient, who suffered from disseminatedpapule due to pre-existing dermatitis, hadminor epidermolysis.Conclusion:Application of baby powder topatient body and silicone gel pad is simpleand effective method to reduce the frictionat local compression sites and to preventpressure ulcer formation during proneposition spinal surgery.
330Simultaneous Direct LateralInterbody Fusion and PosteriorPercutaneous Screw FixationDoniel Drazin, Ali Shirzadi, Michael S. Turner, Beren Tomooka, Srinath Samudrala, Wesley A. King,Terrence T. Kim, J. Patrick JohnsonIntroduction: Lateral interbody lumbarfusion procedures are becoming morecommon for degenerative lumbar diseaserequiring fusion and they are typicallyperformed by repositioning the patient to
complete the second stage of thecircumferential procedure. We havedeveloped a method for performing bothprocedures in a single lateral position.This technique will shorten the length ofsurgery and increase operative efficiencywhile maintaining surgical precision.Methods:We performed a retrospectivechart review of ten patients who underwentboth procedures simultaneously andcompared the outcomes with a controlgroup of ten patients who underwent thelateral interbody fusion and were thenrepositioned for posterior percutaneousscrew fixation. Among the treatedpatients, one patient had a traumaticligamentous injury, one had bilateral parsfractures with instability, one had mobilegrade two spondylolysthesis, and theremaining patients had severe degenerativedisk disease at a single level. Indicationsfor surgery included worsening back painin patients who failed exhaustiveconservative management.Results: Ten patients underwent bothprocedures simultaneously. Avoidingrepositioning, operative time from incisionto closure averaged 130 minutes (vs.control 190 minutes, P = 0.009) andintraoperative blood loss was 108 ml (vs.93 ml, NS). Non-repositioned patientswere hospitalized an average of 4 days(vs. 7 days, NS). There was onecomplication in the control grouprequiring screw repositioning.Conclusion: The lateral interbody fusionand percutaneous pedicle screwprocedures are both readily accomplishedin the lateral decubitous position. In selectpatients with adequate size pedicles,performing simultaneous proceduresoffers an advantage over sequentialsurgery requiring repositioning.Performing the surgeries togetheraccomplished a three column fusion withincreased stability over each procedureperformed alone. Patient outcomes wereexcellent and comparable to proceduresdone in series.
331Iliac Osteotomy to Enhance Exposureof the L4-5 Interspace in Minimally-Invasive Direct Lateral InterbodyFusion: A Cadaveric Feasibility StudyRicardo B.V. Fontes, Vincent C. TraynelisIntroduction: Minimally-invasive directlateral interbody fusion (DLIF) hasemerged as a popular surgical technique ina remarkably short period of time. Wehave found that the iliac crest mayoccasionally prevent access to the L4-5
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES76
DIGITAL POSTER ABSTRACTS

interspace for a DLIF procedure. Wepropose that removal of a minimal amountof ilium may allow for successfulexposure of the L4-5 interspace in thosecases with a “high-riding” iliac crest.Methods: Twenty L4-5 DLIF procedureswere performed on 10 cadavers. L4 5DLIF was successfully completed in13/20 attempts. In the remaining 7 cases,the iliac crest prevented perfect orthogonalaccess to the L4-5 interspace. An iliacosteotomy was performed until the tubularretractors could be perfectly aligned withthe L4-5 interspace and DLIFaccomplished. Pre- and post-osteotomyAP fluoroscopy images were obtained.Working instrument-L5 superior endplateangle and cranio-caudal displacementwere measured, as well as the resectediliac area.Results: Iliac osteotomy enabledcompletion of L4-5 DLIF in the 7remaining cases. Iliac resection wasminimal, an average of 4.92 cm2 of iliacsurface was resected (range, 2.08-8.27cm2) to enable L4-5 access. Adequateworking angles were maintained (average3.3 degrees change post-resection) whilesignificant caudal translation of the tubularsystem was achieved (average 15.7 mm,range 5.2-27.6 mm).Conclusion:A significant fraction ofpatients may have a “high-riding” iliaccrest and that may have had an impact onDLIF series: L4-5 cases are scarce inrelation to the mid-lumbar spine in mostDLIF series. Significant caudaldisplacement of the tubular system wasachieved with minimal iliac osteotomy,ensuring access to the L4-5 interspace inall specimens while maintaining theminimally-invasive philosophy behindDLIF.
332The Minimally Invasive TLIF: Are TwoSurgeons Better than One?Luis M. Tumialan, Frederick F. Marciano,Nicholas TheodoreIntroduction: The very nature of theminimally invasive TLIF requires twoseparate incisions and thereby twoessentially distinct operative sites. Theauthors wished to determine the impact ofa second surgeon in this operation, with aparticular focus on operative time andradiation dose.Methods: The authors retrospectivelyreviewed data from a prospectivelycollected database on minimally invasiveTLIFs. Total fluoroscopy time, radiationdose, operative time, estimated blood loss,
hospital stay and clinical outcomes werecompared between cases performed byone and two surgeons. Statisticalsignificance between the two groups wasevaluated by a paired Student’s t-test.Results: A total of 24 minimally invasiveTLIFs were identified that met criteria forpairing. Indications for surgery includeddegenerative spondylolithesis anddegenerative disc disease. Levels ofsurgery included L3-4, L4-5 and L5-S1.The mean fluoroscopy time, radiationdose and operative times for one surgeonwere 113.54 seconds, 1.26 mGym2, 228minutes respectively, whereas for twosurgeons the mean values were 67seconds, 0.73 mGym2 and 179 minutes.For one surgeon, the mean estimatedblood loss, total hospital stay and clinicaloutcome at 90 days measured by changein preoperative and postoperative OwestryDisability Index (ODI) were asfollows:115 cc, 1.8 days and 28.6,whereas for two surgeons the EBL was118 cc, 1.74 days and 26.4. A pairedStudent’s t-test demonstrated statisticalsignificance in operative times (P =0.000636), radiation dose (P = 0.025) andfluoroscopy times (P = 0.000252). Therewas no statistical significance between thetwo groups with regards to hospital stay,estimated blood loss and clinicaloutcomes.Conclusion: Two surgeons workingsimultaneously in a minimally invasiveTLIF decrease fluoroscopy times, totalradiation dose and total operative timewhen compared to one surgeon. However,this does not appear to impact EBL,hospital stay or clinical outcome. A costeffective analysis to further study this iswarranted.
333Can We Predict AdjacentLigamentous Injury on MRI AfterCervical Spine Fracture?Margaret Carmody, Jeffrey Claridge,Michael Nowak, John J. Como, Michael P. SteinmetzIntroduction: Cervical spine injury is acommon presenting diagnosis to traumacenters. The addition of MR to CTimaging to evaluate for adjacentligamentous injury is often performed,however there is currently no standard asto when this should be done. This studywas undertaken to determine thecharacteristics of soft tissue injuries thatare associated with cervical spine injury,as well as develop guidelines for whenMR imaging should be performed.
Methods: Retrospective analysis of allpatients treated for traumatic cervicalspine injury in a Level I trauma centerfrom 2005 - 2010 was performed. Allpatients had evidence of a cervicalfracture based on CT scan, while asubgroup underwent MRI. Analysis wasthen performed to show relationshipsbetween specific cervical spine fracturetypes, location and neurological status andany associated adjacent ligamentousinjury based on MRI scan.Results: During the study period, 787patients had one or more cervical fracturesidentified on CT scan, 240 of theseunderwent MRI scanning. One hundredthirty-one (56%) had evidence of adjacentligamentous injury. Patients with multiplefractures, multiple fracture types, andpresence of neurologic injury were morelikely to undergo MRI compared to thosethat did not (P < .001). Adjacent softtissue issue was significantly associatedwith the presence of multiple contiguousfactures (P < <0.01), presence of morethan one type of fracture (P < <0.002),and presence of any type of neurologicinjury (P < <0.001).Conclusion: Only 50% of the patients whounderwent MRI following a cervicalfracture actually had evidence of adjacentligamentous injury. Factors that stronglypredicted ajacent injury were multiplecontiguous fractures, multiple fracturetypes and presence of neurolgical deficit.There is significant cost and timeassociated with these scans. Their use inthese patients should be scrutinized fornecessity and overall influence ondecision making.
334Adult Degenerative Scoliosis Treatedby XLIF: Clinical Results of a 24-month Multi-center ProspectiveStudyW.B. Rodgers, Frank M. Phillips, Antoine TohmehIntroduction: Surgical intervention foradult deformity is associated withprolonged recovery periods and a highrisk of complications, particularly in theelderly patient population. This reportsummarizes the longitudinal clinicalresults from a prospective multicenterstudy on the treatment of adultdegenerative scoliosis with the lateralinterbody fusion (XLIF) approach.Methods: 107 patients who underwent theXLIF procedure with or withoutsupplemental fixation for the treatment ofdegenerative scoliosis were enrolled in a
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 77
DIGITAL POSTER ABSTRACTS

prospective multicenter, nonrandomizedIRB-approved observational study ofclinical and radiographic outcomes of theXLIF procedure from 2007-2009.Neurologic evaluation and patient-reported clinical outcomes ODI, VAS,SF-36, and satisfaction were collected atbaseline, 1.5, 3, 6, 12, and 24 months.Results: 79 patients have completed 24-month follow-up. Average patient age was68 years. Mean Charlson co-morbidityscore 0.48. A mean of 4.4 levels weretreated per patient with anterior and/orposterior fixation. Supplemental pediclescrew fixation was used in 75.7% ofpatients. Mean operative time was 178min and median EBL 100-200 mL. Meanhospital stay 3.8 days (2.9 unstaged, 8.1staged). Of 34 motor and 20 and sensorydeficits identified pre-operatively, 26motor and 18 sensory were improved aftersurgery. New and persistent post-surgicalneurologic deficits were identified in 7patients. Clinical outcomes wereimproved (P < 0.05) from baseline to 24months. At 24 months 85% were satisfiedwith their procedure and 85% stated thatthey would repeat their procedure. Majorperioperative complications occurred in13 patients (12.1%). Additionalcomplications to date include 1 posteriorrevision for painful hardware and 1 cagefailure without revision.Conclusion: This prospective studyrepresents the largest report of patientstreated with XLIF for adult scoliosis. Thisstudy supports XLIF as a valuable adjunctin the treatment of adult scoliosis. Despiteadvanced age and co morbidities, datafrom this study reflect promising clinicaloutcomes, low revision rates, and highpatient satisfaction.
335Predictors of Early PostoperativeDischarge Following MinimallyInvasive Lateral Interbody Fusion(MI-LIF)W.B. Rodgers, Edward J. Gerber, Jeffrey A. Lehmen, Jody A. RodgersIntroduction: Extended hospitalizationfollowing spine surgery has been shown toincrease the potential for postoperativecomplications, namely infection, andsubstantially increase costs. In interbodyfusion procedures, namely MI-LIF, whereminimal approach morbidity has beenshown to allow for early postoperativefunctionality and early discharge, thoughpatient characteristics which may predictearly discharge following MI-LIF areheretofore unreported.
Methods: Prospective data on 1033consecutive MI-LIF patients from October2006 through June 2011 were reviewed.Of these, 873 were discharged in <23hours (outpatient), and 160 weredischarged in >23 hours (inpatient).Within the outpatient group, 45 patientswere discharged within 8 hours of surgery(ambulatory). Demographic data werecompared between outpatient andinpatient groups, as well as betweenambulatory and outpatients.Results: Factors impacting early discharge(out- vs. in-patient) were age, gender,smoking, deformity, preop hemoglobin(Hgb) level, preop disc height, number oflevels treated, and fixation type. Mean agefor out- and in-patients was 61.9 and 66.7years, P < 0.001. More males wereoutpatients (88.2%) compared to females(81%), P = 0.012. Smoking was,surprisingly, more frequent in out-compared to in-patients (34.3% and 22%),P = 0.003. Preoperative Hgb and discheight were higher in outpatients (13.8gand 6.3mm) than inpatients (13.1g and5.4mm). More levels treated predictedbeing in patient (P < 0.001), and non-pedicle screw fixation favored outpatientdischarge, P < 0.001. No differences wereseen between out and inpatients in termsof number of comorbidities or having hadprior surgery. Ambulatory patients wereyounger than both out- and in-patients(53.2 years, 62.4 years, and 66.7 years), P< 0.001, had even higher preoperativeHgb (14.4g, 13.7g, and 13.1g), P = 0.001,and preoperative disc height (7.6mm,6.3mm,and 5.4mm, all respectively), P =0.002.Conclusion: These data suggest that factorsincluding but not limited to lower age,elevated preoperative hemoglobin,elevated preoperative disc height at theindex level, having fewer indicated levelswith single-incision fixation may predictearly discharge following MI-LIF.
336Predicting Adjacent SegmentDegeneration After Cervical FusionSurgery: A Novel Grading SystemAlexander E. Ropper, Yang D. Teng,Charles H. ChoIntroduction:Adjacent segmentdegeneration is a common, delayedcomplication of cervical fusion surgery.We evaluated the appearance of discsadjacent to cervical fusions, both beforeand after surgery, to determine ifpreoperative disc appearance was aprognostic factor for subsequent
development of adjacent segmentdegeneration.Methods:We retrospectively reviewedadult patients at a single institution whounderwent any cervical spine fusionprocedure for traumatic fractures,dislocations or ligamentous injury or fordegenerative disc disease, spinal stenosis,ligamentous hypertrophy or foraminalstenosis over ten years. Any patient whosefusion construct contained at least onecervical vertebral body was included. Asimple grading system (grades 0 4) wasdesigned to evaluate intervertebral discappearance on sagittal T2 MRI imaging.Preoperative and postoperative MRIs werereviewed and the adjacent disc(s) weregraded and compared to evaluateprogression of adjacent segmentdegeneration.Results: 190 adjacent cervical discs wereincluded in the analysis. The mean periodfrom surgery to the last reviewable MRIwas 16.3 months (median 10.3 months).Contrary to our hypothesis, the incidenceof progression (to a higher grade)occurred in the same proportion of discsregardless of the preoperative grade. Thepercentage of discs that did not progresswas closely clustered, between 66-69%based on preoperative grade.Conclusion: The grading system describedin this study provides a novel and simplecharacterization of adjacent cervicalintervertebral discs. The data suggest thatpreoperative disc disease visible on MRIwas not a prognostic factor in thedevelopment of adjacent segmentdegeneration. This pilot study can be usedto guide larger scale, prospective researchto define additional predictive imagingfactors for adjacent disc degeneration inpatients about to undergo cervical spinalfusion surgeries. This information can bevaluable to surgeons for planning theextent of cervical fusion constructs.
337Minimally Invasive Lateral InterbodyFusion (MI-LIF) at L4-5 and theProtective Effect of ProphylacticDexamethasoneW.B. Rodgers, Edward J. Gerber, Jeffrey A. Lehmen, Jody A. RodgersIntroduction: It has been reported that MI-LIF procedures performed at the L4-5level have a higher incidence ofpostoperative motor deficits compared toother lumbar segments, and mustoccasionally be aborted to due anatomicconstraintsMethods: In our single-site consecutive
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES78
DIGITAL POSTER ABSTRACTS

series of 1093 MI-LIF patients, 646 (59%)included the L4-5 level. Clinical andradiographic data were prospectivelycollected and reviewed to assess MI-LIFprocedure at the L4-5 level.Results:Age averaged 62.3 years (24-88years). 92.9% had one or morecomorbidities. 33.1% had prior lumbarsurgery. All procedures were successfullycompleted. Hospital stay averaged 1.3days. Average VAS pain scores improvedfrom 8.6 at pre-op to 2.8 at 12 months and2.7 at 24 months follow-up. Lenke fusionscores of 1-2 were present in 96.2% at 6months, and 99.4% at 24 months. Neuralcomplications included 4 (0.6% of allcases, 0.9% of L4-5 cases) transient lowerleg weaknesses (3 quads, 1 anteriortibialis, all resolved within 3 months).After the fourth postoperative motordeficit, we began to administerdexamethasone (10mgIV prior to skinincision) prophylactically in all MI-LIFpatients in whom the L4-5 level was to beapproached. Since the use ofdexamethasone, no additional neuraldeficit developed, a statistically significantdifference (P = 0.0245).Conclusion: The incidence of postoperativemotor deficits following MI-LIF at L4-5 islow. The prophylactic administration ofdexamethasone results in a statisticallysignificant reduction in motor deficits.
338XLIF for Grade II Spondylolisthesis atL4-5: The “Worst Case” ScenarioW.B. Rodgers, Edward J. Gerber, Jeffrey A. Lehmen, Jody A. RodgersIntroduction: The XLIF technique is anMIS alternative to traditional spinal fusion.However, concerns are raised about neuralcomplications with the lateral approach,particularly at the L4-5 level where accessis most difficult due to the lumbar plexus.Significant anterolisthesis at this levelexacerbates this risk. Outcomes from aseries of these “worst case scenario”patients treated with XLIF are reported.Methods: 89 patients with Grade-IIspondylolisthesis at L4-5, with andwithout concomitant stenosis, DDD, post-laminectomy instability, HNP, and/orscoliosis, were treated with XLIF. Clinicaland radiographic data were reviewed toassess comorbidities, surgery details,hospital stay, complications, pain scores,changes in disk height and alignment, andfusion, and satisfaction scores at 24months postop.Results:Ages ranged from 25-91 years(ave 67.4 yrs.). Comorbidities were
common (present in 93%). The L4-5 levelwas accessible in all cases. All casesincluded supplemental posterior fixation.LOS averaged 1.3 days. Complicationsincluded 1 pulmonary embolism requiringanticoagulation, 1 late-term hardwarefailure (screw fracture at 1 year), and onepostop transfusion, one ileus and post-operative atrial fibrillation. No neuraldeficits were noted. In 28 patients at 24months, VAS pain scores improved from8.7 to 2.7. Average disk height improvedfrom 4.6mm at pre-op to 10.3mm post-op,with 1.8mm settling at 24 months. Slipimproved from 10.7mm at pre-op to2.7mm and was maintained at 24 months.Lenke fusion scores averaged 1.9 at 3months, 1.4 at 6 months, and 1.1 at 24months. Eight patients underwent a CTscan at 12 months, all were judged asfused by an independent reviewer. 91% ofpatients were satisfied with the procedureand would do it again.Conclusion: Grade-II spondylolisthesis atL4-5 can be treated successfully with aminimally invasive lateral approach.Results indicate good outcomes, fewcomplications, and high satisfaction evenin the most difficult situation.
340Recapping Laminoplasty for SpinalSurgery Using with Ultrasonic BoneCuretteHidenori MatsuokaIntroduction: The laminoplasty techniqueis the most widely used procedure inspinal surgery. We developed a novelmethod of the recappinghemilaminoplasty in a retrospective studyof the patients with spinal surgicaldisorders. This report describes thesurgical technique and the results of thehemilaminoplasty using with ultrasonicbone curette.The aim of this study was toexamine the safety and effectiveness ofhemilaminoplasty technique in spinalsurgery.Methods: Twenty-nine patients who hadundergone recapping hemilaminoplastywith ultrasonic bone curette for spinaldisease between 2003 and 2010 did notneed spinal canal enlargement after theindradural procedure was completed. Inthis study group, there were 17 men and12 women with a mean age of 47.4(range, 4-74 years). The mean follow-upperiod was 38.4 months (ranged, 5-91months). The mean number of resectedand restored lamina was 1.6. All patientswere observed both neurologically andradiographyically by dynamic plain
radiographs and computed tomography(CT). Bony fusion was evaluated bydynamic plane radiographs based onRay’s criteria and computed tomographyfor 3, 6, 12 months, and then every 12months.Results: Recapping hemilaminoplasty wasdone safety to obtain an enough widerlaminotomy space for an intraduralprocedure preserving posterior elementsincluding spinous process, interspinalligaments, supraspinous ligament andfacet joint. CT confirmed primary bonefusion in the all patients by 6 months aftersurgery. Postoperatively, no majorcomplications such as postoperative spinalcanal stenosis, facet arthrosis, or kyphosiswere reported.Conclusion: Recapping hemilaminoplastyis a useful posterior approach forintraspinal canal procedure preserving theposterior elements. This method allowsanatomical reconstruction of the excisedbone preserving the posterior surroundingtissues.
341Spinal Fusion with Porous TantalumInterbody Cages: Experience in 149CasesIra M. GoldsteinIntroduction: Porous tantalum (trabecularmetal) is a highly porous, osteoconductivescaffold that has been used for numerousbony reconstruction applications since1997. Its compressive strength and elasticmodulus are similar to that of densecancellous bone, serving as amechanically stable graft material withoutthe morbidity of autograft harvest or thepotential for disease transmission ofallograft utilization.Methods:A retrospective chart review of149 patients who underwent interbodyfusion with trabecular metal cages andinstrumentation. Fusion was assessed viathe presence of visible bridging bone orby the absence of motion on flexion-extension Xrays and by the absence ofhardware loosening.Results: 149 patients underwent ACDF (n = 130), TLIF (n = 13), ventralthoracolumbar corpectomy (n = 3), PLIF(n = 2), and ALIF (n = 1) between April2005 and July 2011. Surgical indicationswere degenerative spinal disease (n = 97),trauma (n = 29), osteomyelitis (n = 13),deformity (n = 6), pseudoarthrosis (n = 3),or vertebral neoplasm (n = 1). Follow-upranged from 1 to 36 months. 86 patientshad follow-up of greater than 6 months.Graft expulsion or displacement was seen
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 79
DIGITAL POSTER ABSTRACTS

in no patients. Persistence of infection (inpatients with abscess/osteomyelitis preop)was seen in one patient who developed asuperficial wound dehiscence.Pseudoarthrosis or loss of deformitycorrection was seen in no patients. Visiblebridging bone adjacent to the tantalumcage was seen in most patients withACDF (not corpectomy) or TLIF between6 and 12 months postop. 1-2 mm of cagesubsidence was common. Subsidence wasmore significant with posteriorapproaches.Conclusion: Porous tantalum cages havebeen used in a variety of orthopedicapplications with good success. Tantalumis extremely radioopaque, making CTevaluation difficult. Indirect measures offusion via flexion-extension imaging aswell as the direct visualization of bridgingbone across more limited (less than 10mm) intervertebral spaces allows forassessment of spinal stability.
342O-arm Navigation For Placement ofAtlantoaxial and CervicothoracicJunction Screws: Technique andInitial Clinical ExperienceJohn K. Houten, Gaurav JainIntroduction: Compared with mid-cervicalarea lateral mass screw fixation technique,screw placement at the atlantoaxial leveland cervicothoracic junction isparticularly challenging, as minorimprecision of the trajectory may placethe vertebral artery or spinal cord at risk.Fluoroscopy-guidance does not provide anaxial view to determine the relationship ofthe pedicle wall and spinal canal and theshoulders obscure cervicothoracicjunction visualization. Navigationpreoperative CT scans is limited byinaccuracies from human error in paired-point matching during registration and bychanges in spinal position between thesupine preoperative scan and the proneoperative position. The O-armMultidimensional Surgical ImagingSystem promises to provide superioraccuracy in screw placement byovercoming the limitations of earliernavigation technologies.Methods: Fifteen consecutive patients(Table 1) mean age 56 (8-81) underwentposterior fusion with screw fixation ateither the atlanto-axial or cervicothoracicjunction area using computer-assistednavigation of intraoperative O-armimaging. A tracker was fixed to the 3-pinhead-holder (Figure 1) with an infraredcamera positioned at the head of table.
The bony tract was created with aJamshidi needle with an integratedreflector array. (Figure 1) followed byscrew hole creation using a navigated drillguide. Screws placed in the C1, C2, C7,T1 and T2 were reviewed for accuracy onpostoperative CT scanning or O-armscans.Results: Sixty-eight screws were placed(Table 1), and 66/68 (97%) were entirelywithin the confines of bone. One T2 screwviolated the lateral pedicle cortex 2mmand one T1 screw breached the lateralcortex 5mm. There were no clinicalsymptoms from the pedicle breaches.Conclusion: Initial experience with O-armguided navigation showed good accuracyin cervical and upper thoracic screwfixation. Additional evaluation of thetechnology is warranted, particularly forpatients with difficult surface anatomy oran anomalous course of the vertebralartery.
343The Use of Three-Dimensional ImageGuidance in Subaxial AnteriorCervical Surgery: Technical NoteEric W. Nottmeier, Stephen M. PirrisIntroduction: Three-dimensional (3D)image guidance has been used to navigateposterior cervical spinal anatomy to aid inaccurate instrumentation placement.[1-4]The use of 3D image guidance fornavigating anterior cervical anatomy canbe challenging because of the dynamismin this area of the spine and the difficultyof fixating the image-guided reference arcto the patient. The authors have found 3Dimage guidance helpful in navigating thespinal anatomy in revision anteriorcervical procedures, as well as anteriorcervical procedures involving corpectomyor tumor removal. The technique of 3Dnavigation of the anterior cervical spineutilizing cone based computedtomography (cbCT) is described.Methods: This technique was used in 20patients who underwent anterior cervicalprocedures utilizing cbCT-based, 3Dimage guidance (Table 1). In each case,the patient was placed supine on a shortboard of a radiolucent spine table allowingfor the head to be suspended and fixatedby a skull clamp headholder. Thereference arc of the image-guided systemwas attached to the headholder. Anintraoperative cbCT scan wasaccomplished prior to prepping the patient(Fig. 1). Image guidance was used tomark pertinent anatomical structuresdepending on the case. In corpectomy
cases, the exact midline of the cervicalspine and the borders of the corpectomywere marked. Image guidance was used toguide bone removal and/or locate specificanatomy relevant to the specific casebeing performed.Results: Image guidance was able toreliably locate pertinent anatomicalstructures. No complications resulted fromthe use of image guidance and no vascularinjuries occurred. No patients required arevision anterior surgery.Conclusion: This technical note describesthe setup and technique for the use of 3Dimage guidance in anterior cervicalsurgery. The authors have found 3D imageguidance to be a useful adjunct in revisionanterior cervical procedures, as well asanterior cervical procedures involvingcorpectomy or tumor removal.
344Outcomes in Minimally DisruptiveLateral Interbody Fusion: 24 MonthMinimum Follow-up in 268 PatientsW.B. Rodgers, Edward J. Gerber, Jeffrey A. Lehmen, Jody A. RodgersIntroduction: This study presents thelargest series of patients treated withminimally invasive lateral interbodyfusion (MI-LIF) with long-term outcomesto date.Methods: Prospective treatment,complication, functional outcome, andradiographic data on 1093 consecutiveMI-LIF patients were reviewed. Of these,268 were eligible for and completed 24month follow-up. Patients were 63%female with a mean age of 62.2 years andBMI of 31.3. Baseline comorbiditiesincluded CAD (48%), smoking (31.5%),DM (24.2%), and prior spine surgery(38.3%). The most common primaryindications included stenosis (46.4%),spondylolisthesis (17.7%), and DDD(11.3%). A total of 318 levels were treatedwith MI-LIF and supplemental internalfixation was used in all but 5 (2%) cases.Results: In these 268 patients, 19 (7.1%)complications occurred. Complicationsrelated to the procedure included 3hardware failures (posterior), 1 nerveinjury (quadriceps weakness), 4 vertebralbody (VB) complications, and 1 incisionalhernia. Pain (VAS) improved 65.7% frompre-op to 24 months (8.69 to 2.98,respectively). Disk height improved from6mm pre-op to 10.3mm immediately post-op, settling at 8.9mm at 24 months. Slipwas reduced from 4.5mm pre-op and wascorrected and maintained by 83% through24 months (0.85mm). Mean Lenke fusion
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES80
DIGITAL POSTER ABSTRACTS

at 3, 6, 12, and 24 months progressed from2.03, 1.42, 1.17, to 1.12, respectively. At24 months, 87% of patients were “very” or“somewhat satisfied” with their outcome,81.1% of patients would be “definitely” or“very likely” redo the surgery, and 79.5%were considered excellent or goodoutcomes by the surgeon.Conclusion: These data show satisfactory 2year clinical outcomes in patientsreceiving MI-LIF for degenerative spinalconditions. VAS scores improved, diskheight was restored and maintained, andslip was adequately reduced while patientand surgeon satisfaction scores areencouraging. This study, to date,represents the largest series of long-termoutcomes following MI-LIF.
345Comparison of Resident PhysicianThoracolumbar Pedicle ScrewPlacement Accuracy with Either O-arm Mulitdimensional ImageGuidance or an Open, LateralFluoroscopy TechniqueJohn K. Houten, Adam Lance Sandler,Adesh TandonIntroduction:Minimally invasivetechnique in thoracolumbar fusion surgeryis increasingly popular, and accurateplacement of pedicle screws in theseprocedures necessitates skills beyondthose needed for open, free-hand cases.The introduction of the O-arm systempermits screw placement withoutexamination of surface anatomy orfluoroscopy. The effect of adopting image-guided surgery using the O-arm uponresident training has not been studied. Wecompare the accuracy of open vs. O-armguided pedicle screw placement by novicejunior neurosurgical residents.Methods: Two teams of first and third yearneurosurgical residents placed pediclescrews in TruTrainer spine models usingeither using a percutaneous, O-arm-image-guided technique or a mini-open,lateral-fluoroscopy-guided technique. Allmodels were imaged post-procedure bycone-beam CT scan. Screw placementaccuracy was assessed using a published,four grade scale.Results: In the O-arm group, two of forty(5%) screws breached the pedicle cortexcompared with eleven of forty (27.5%)using lateral fluoroscopic guidance. (P =0.013) There were no grade two or threeperforations using the O-arm comparedwith two grade two and one grade threeperforations with the open, C-armtechnique. There was no difference in
accuracy between first and third yearresidents. Thoracic pedicle perforationoccurred in 8/32 screws, a higher rate thanthe 7/48 seen in the lumbosacral area.Conclusion: Novice neurosurgicalresidents placed pedicle screws withhigher accuracy using O-arm imageguidance compared to a mini-open, lateralfluoroscopy technique. Further study isneeded to understand the implications ofdifferences in the rate of resident masteryof open and imaged-guided pedicle screwplacement techniques.
346Minimally Invasive Lateral InterbodyFusion in the Morbidly ObeseW.B. Rodgers, Edward J. Gerber, Jeffrey A. Lehmen, Jody A. RodgersIntroduction:Minimally invasiveprocedures are challenging in obesepatients whose body habitus may decreasethe accessibility of the spine to theinstruments necessary to perform theseprocedures. The MI-LIF procedure,however, is performed in the lateraldecubitus position, minimizing thedifficulty of the pannus as it falls awayfrom the exposure.Methods: In our single-site prospectiveseries of 1093 MI-LIF patients, 576 wereidentified as obese (BMI>30) and 192 ofthose were morbidly obese (BMI > 38).Comorbidities, surgical details, hospitalstay, complications, pain scores, changesin disk height and alignment, and fusionwere assessed.Results: In all morbidly obese patients, nosurgery could not be successfullycompleted due to body habitus. Theheaviest patient to date weighed 427 lbs(193.7 kgs), the largest BMI was 61.8.Age ranged from 22-83 years.Comorbidities included smoking (34%),prior spine surgery (47%), diabetes (41%),CAD (37%), COPD (3%). 244 levelswere treated in these 192 patients: 150 1-levels, 33 2-levels, 8 3-levels and 14-level, the majority at L4-5. All but 2surgeries included supplemental fixation.There were 3 transfusions and noinfections. Complications included 2 MI’sat 4 and 6 weeks, 3 atrial fibrillation,pneumonia requiring intubation for 5days, one other respiratory distressrequiring re-intubation, one pulmonaryembolism, two posterior hardwarefailure/rod fracture at 6 and 18 months,and one fracture of vertebral osteophytesand a vertebral body fracture at 2 monthsrequiring reoperation. Hospital stayaveraged 1.54 days. From pre-op to 24
month follow-up: disk height increased anaverage 3.0mm, slip decreased an average3.6mm in spondylolisthesis patients, andVAS pain scores decreased from 8.7 preopto 3.1 at 24 mos. Lenke scores were 2.1 at3 months, 1.2 at 12 months, and 1.1 at 24months.Conclusion: Our results demonstrate theusefulness and safety of the MI-LIFtechnique in treating morbidly obesepatients minimally invasively.Complications are minimal, procedurestimely, and outcomes similar to non-obesepatients.
348Clinical Decision Making,Differentiating Disabling SacroiliacPain from Axial Disc BasedExplanationsJohn G. Stark, Chris IdemmiliIntroduction: The sacroiliac joint has beendefined by many authors as a cause ofback and buttock pain. Though thought tobe common, the means of diagnosis andaccurate differential diagnosis has notbeen established.Methods: The sample consists of 67 SIJfusions. Sixty-two cases had pre- andpost-op functional data available forcomparison. Forty-seven out of 62 casesdemonstrated a net functionalimprovement at last follow-up aftersurgery, as reflected on the Million VisualAnalog Scale. Prior to the decision forsurgery, all patients were studied forconfirming clinical findings, injectionresponse, and correlation to clinicalhistory. Elements of the decision makingprocess were ranked in order ofimportance to the final decision forsurgery. ANOVA was performed onfunctional improvement after separatingthe sample into groups by primaryelements of diagnosis.Results: There was a significantimprovement in average Million VASscore (95% confidence interval of 16 to 31points of improvement), yet nostatistically significant association ofoutcome with any individual subset ofclinical findings was found, includinghistory, physical examination, imagingand diagnostic injection.Conclusion: The diagnosis of surgical levelSIJ disease and its qualification forsurgical approach is a complex series ofclose history taking, cautious repeatedphysical examination, and evaluation ofother etiologies which could explain thepatient’s symptoms. The failure of clinicalresponse of lumbar spine surgery to relief
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 81
DIGITAL POSTER ABSTRACTS

of symptoms or improvement, asdemonstrated in the SPORT study, shouldprompt a closer evaluation of the totalityof patient symptoms, and sufficient weight(without overemphasis) to all inclusiveand exclusionary criteria.
349Effect of Machined InterfacetAllografts on in Foraminal Heightand AreaVincent C. Traynelis, Carter S. Gerard, Lee A. Tan, Brian A. O’Shaughnessy, Paul A. AndersonIntroduction:Machined allograft has alarge surface area, provides solid support,and could distract the facets therebyincreasing foraminal space. We tested thehypothesis that machined interfacetallografts increase cervical foraminal area.Methods: The C45, 56, and 67 facets offour fresh adult cadavers were exposedand the identified. The cartilage wasremoved from each facet using curets andrasps. Machined allograft spacers weretamped into the joints. These spacers werein all cases except the C56 and 67 joints inone large cadaver. The spines werescanned with the O-arm before and afterplacement of the spacers. Two individualsmeasured foraminal height and area onobliquely angled sagittal imagesindependently. Averaged measurementsfrom these reviewers were comparedusing the paired t-Test.Results: The Pearson correlation betweenthe two radiographic reviewers was verystrong (r = .971, P = 0.0001) as well asthe Intraclass coefficient (ICC = .907, P = 0.0001). The data are displayed in thetable below. Foraminal height and areawas significantly greater followingplacement of the machined interfacetspacers at all levels.Conclusion: The data confirm thehypothesis that machined interfacetallografts increase cervical foraminalheight and area. Modest distraction of thefacets produced by the machinedinterfacet spacers increases foraminal areaand therefore can indirectly decompressthe exiting nerve root. These grafts shouldprevent foraminal stenosis which mayoccur when placing the initiallynonlordotic spine into lordosis with eitherrepositioning after decompression or withcorrection using instrumentation. This isparticularly important at C45 due to theexquisite sensitivity of the C5 root.Machined interfacet allografts providesolid support and should be expected toheal rapidly since the facets bear axial
load which places the grafts undercompression. These grafts may be a usefuladjunct to the surgical treatment ofcervical spine disease.
350Clinical Outcomes After HardwareRemoval in Patients with aPreviously Instrumented SpineVictor Chang, Mokbel K. ChedidIntroduction: The purpose of this study isto evaluate clinical outcomes in patientswho undergo surgery for hardwareremoval after previous spineinstrumentation. The goal will be to assessthe clinical benefit of such surgery, and topotentially understand what predictorsexist for improved patient outcome afterhardware removal.Methods:A database of all patients whounderwent hardware removal proceduresbetween 2008 and 2010 was created. Age,gender, body mass index (BMI), spinalsegment, primary indication, secondaryindication, number of levels, need foradditional instrumentation, need foradditional decompression, average follow-up, and narcotic freedom at last follow upwere all considered. Chi-square tests, twosample t-tests and Wilcoxon two sampletests were done to compare patient andprocedure characteristics between patientswho were and were not narcotic free.Results: There were 69 patients includedin the following analyses. Of these 69,65% were female and the mean age was61.1 (s.d.=12.2) with a range from 37 to88. The outcome of interest was narcoticfree at last clinic visit, for which 33 (47%)of the patients were (Table 1). Thedifference in rate of narcotic freedom wassignificant, with females having a higherrate than males (58% vs. 29%, P = 0.023).Also, the difference in mean BMI betweenthe two groups of patients was significant,with patients with narcotic freedomhaving a higher mean BMI than patientswithout narcotic freedom (31.5 vs. 28.2, P = 0.024, see table 2). In addition, therewas a trend for age when comparing thetwo groups, with patients with narcoticfreedom having a slightly higher meanage than patients without narcotic freedom(63.7 vs. 58.7, P = 0.086).Conclusion: Hardware removal of spinalinstrumentation can be an effectivetreatment in patients with continued painand narcotic dependence after an initialspinal fusion supplemented withinstrumentation.
351A New Approach to Lateral LumbarInterbody Fusion with One-yearFollow-upMitchell HardenbrookIntroduction: The lateral approach to thelumbar spine for interbody fusion is aversatile and less invasive approach to thespine compared to the anterior approach.However, the current retractor systemshave many limitations. The percutaneousnature of the current systems requires anover-reliance on neuromonitoring tonavigate through the neuroplexus withinthe psoas muscle. Additionally, the bladesand retraction mechanism are radio-denseobscuring fluoroscopic imaging. Thesedeficiencies have lead to well-documentedcomplications that may be avoided withbetter visualization.Methods:A new two-retractor system isutilized to improve the safety profile of thelateral approach. In this approach, aradiolucent, fixed tube is placed throughthe retroperitoneal space and positionedon the surface of the psoas muscle.Underdirect visualization with loupemagnification, the fibers of the psoasmuscle are split in line with the musclefibers. Neural structures can be visualizedand avoided. A second, expendableretractor is then placed through the fixedtube and the psoas muscle is retractedunder direct visualization. A complete andthorough discectomy and placement of animplant can then be safely performed.Results: 22 patients underwent lateralinterbody fusion on 28 levels fordegenerative spondylosis of the spine withone year follow-up. The average age was53 years old (33-73). 20 patientsunderwent surgery at the L4-5 level. APEEK interbody device was used foranterior column support. Posterior fixationwas used in all patients (7 pedicle screws,3 facet screws, 12 interspinous processfixation). Estimated blood loss was 220mlwith average hospital stay of 2.5 days.There were no intra-operativecomplications. VAS before surgery was7.2 and 2.8 at last follow-up. 20 of the 22patients had post-operative CT scansshowing solid fusion. 2 patients refusedthe CT scan. 2 patients required revisionsurgery: one for adjacent segmentdegeneration requiring extention of thefusion, and one with herniated disc at theadjacent segment requiringdecompression.Conclusion: This new retractor systemallowed for safe and reproducible accessto the lumbar spine.
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES82
DIGITAL POSTER ABSTRACTS

352Minimally Invasive Lateral InterbodyFusion (MI-LIF) in SmokersW.B. Rodgers, Edward J. Gerber, Jeffrey A. Lehmen, Jody A. RodgersIntroduction: In a large single-site series ofMI-LIFs, 356 patients smoked at the timeof surgery. Overall clinical andradiographic outcomes and are reported.Methods: In our single-site prospectiveseries of 1093 MI-LIF patients, 356smoked at the time of surgery. Patientdemographics and clinical/radiographicoutcomes were assessed.Results: Patients ranged in age from 22-84years (average 56 years) and were treatedfor a variety of indications. 46% hadprevious spine surgery. 17% had diabetes,34% had CAD, 8% had COPD, and 11%were chronic steroid users. 49% wereobese or morbidly obese. 427 levels weretreated: 296 1-levels, 49 2-levels, and 113-levels. Grafting materials included acomposite of DBM, local bone graft, andbone marrow aspirate (81.5%), a beta-tricalcium phosphate/hydroxyapatite withbone marrow aspirate (6.5%), andallograft cellular bone matrix containingnative mesenchymal stem cells (1.7%).All but two surgeries includedsupplemental fixation, most performed inthe same surgical position. There were noinfections. Complications included 1transfusion, 2 pneumonia, 1 reintubation,1 ileus, 2 urinary retention, 1 atrialfibrillation, 1 endplate fracture (healedwithout intervention), 1 sacral fracture, 3intraoperative hardware failures (replacedwithout incident), 1 osteophyte fracture(required reoperation), 2 compressionfractures (required vertebroplasty), and 1quad weakness (resolved withoutintervention). Hospital stay averaged 1.1days. From pre-op to 24 months post-op,average disk height improved by 2.9mm,average slip improved by 3.6mm, averageVAS pain scores decreased by 5.2 points.Signs of fusion by Lenke scores of 1 or 2were 80% at 3 months, 94% at 6 months,and 98% at 12 months and 98% at 24months – not significantly different fromthe greater non-smoking (624 pts.) cohort(84%, 95%, 97% and 98%, respectively).Conclusion: Our results show nosignificant difference in the clinical andradiographic outcomes between smokersand nonsmokers. MIS fusion approachesmay offset some of the deleterious effectsof smoking on bone healing.
353Optimum Timing of RoutineUltrasound Sonography for DeepVein Thrombosis in AsymptomaticSpine Patients During HospitalAdmission: An Analysis of 591Consecutive PatientsAkil Patel, D. Kojo HamiltonIntroduction: Protocols for the screeningand prevention of Deep Vein Thrombosis(DVT) in neurosurgery are not applieduniversally, particularly when consideringpatients undergoing spinal surgery. Whilethere is data on this topic in the field ofspinal surgery, the overall principles andpractices in regards to spinal patientsremains vague. The idea of screeningultrasonography for earlier detection ofDVT has gained more overall consensus,but the timing of screening continues toremain unclear.Methods:A retrospective review of 591consecutive adult patients, who underwentadmission, as well as weekly ultrasoundscreening at a university hospital center,over 1 year was conducted. Inclusioncriteria included use of chemical andmechanical prophylaxis.Results: There was a 2.5% incidence inthis spinal surgical population. Of thisgroup, 80% were diagnosed with a DVTwithin 7 days of hospital stay, 0%diagnosed within 8-14 days, and the rest(20%) were diagnosed after 14 days ofstay (p-value <0.05). There was a higherincidence of DVT in plegic and pareticpatients, both on admission and duringhospitalizationConclusion: Routine ultrasonographyscreening for DVT should continue to beutilized, as it has shown merit, but theeffectiveness may be most maximized ifscreening includes an initial admissionstudy and also within the first week ofhospital stay. Continued weekly screeningof asymptomatic patients after 14 days inthe hospital is of minor benefit.
354Incidence of Lumbar Spine PedicleBreach Following PercutaneousScrew Fixation: A RadiographicEvaluation of 601 Screws in 151PatientsZachary Adam Smith, Cort D. Lawton,Richard G. FesslerIntroduction: Percutaneous pedicle screwfixation in the lumbar spine continues toincrease in modern neurosurgical practice.Few reports have specifically addressedthe accuracy and safety of this method.The primary objective of this study was to
evaluate the accuracy of fluoroscopicallyguided percutaneous pedicle screwfixation in the lumbar spine.Methods:A total of 151 patients wereevaluated following instrumented single-level or two-level minimally invasiveTLIF (MI-TLIF) with 601 screws placedfor percutaneous fixation. The treatedpatients had an average age of 56.6 (20-85) and there were 192 single-level casesand 22 two-level cases. The levels ofpedicle screw fixation included (Level, ptno.): L1/L2 (1), L2/L3 (2), L3/L4 (33),L4/L5 (101), L5/S1 (46). Radiographicresults were obtained with immediatepost-operative CT scan. Patients werefollowed prospectively to evaluate forclinical outcomes as well as potentialcomplications.Results: In a total 601 instrumentedpedicles, there were 37 pedicle breaches(6.2%). Of these, 22 (3.7%) weresignificant breaches (greater than 3mm).The level of the breached pedicles wereL3 (5/46, 10.2%), L4 (12/201, 7.0%), L5(15/158, 9.5%), S1 (3/47, 3.4%). Theside/location of breach was characterizedas follows: Medial (22), lateral (12),superior (2), and inferior (1). There weretwo symptomatic breaches, bothassociated with a medial breach at the L5pedicle. Both were transient and did notrequire hardware repositioning. Therewere no other complications.Conclusion: Percutaneous pedicle screwfixation in the lumbar spine continues tobe a technique embraced by modernspinal surgeons. The use of intra-operativefluoroscopic guidance is both a clinicallysafe and accurate method forinstrumentation and is of comparableaccuracy to other techniques. Whiletrajectory errors may occur, they are rarelyof clinical significance.
355Comparison of Surgically TreatedAdult and Adolescent Main ThoracicScoliosis Demonstrates Similar AcutePerioperative Outcomes: AProspective, Matched CohortEvaluationJustin S. Smith, Christopher P. Ames, Shay Bess, Burt Yaszay, Breton G. Line,Munish Gupta, Frank Schwab, Baron Lonner, Virginie Lafage, Douglas C. Burton, Behrooz A. Akbarnia,Oheneba Boachie-Adjei, Robert Hart,Richard A. Hostin, Christopher I. ShaffreyIntroduction: Popular belief indicatessurgery for main thoracic (MT) scoliosisduring adolescence provides greater
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 83
DIGITAL POSTER ABSTRACTS

correction, shorter hospitalization andfewer complications compared to adults.Purpose: compare acute (<12 weeks)radiographic and operative data followingposterior spinal fusion (PSF) of MTscoliosis <60° between mature adolescentidiopathic (AIS) and adult idiopathicscoliosis (ADULT) patients.Methods:AIS patients (Risser grade 4-5 atsurgery) consecutively enrolled into aprospective database were matched toADULT patients consecutively enrolledinto a prospective database. All receivedPSF pedicle screw constructs for MTcurve <60°. Matching criteria: MT curvesize, end vertebrae, lumbar curve size, andlumbar curve modifier (A-C).Results:AIS (n = 26, mean age = 15.3)and ADULT (n = 14, mean age = 32.1)had similar preoperative MT (48.8° vs.50.6°) and lumbar curves (31.5° vs.29.9°), lumbar lordosis (60° vs. 54.8°),and spino-pelvic parameters, respectively(P > 0.05). Postoperative MT (14.3° vs.17.1°) and lumbar curves (12.7° vs. 12.4°)were similar for AIS and ADULT,respectively (P > 0.05). MT correction(70.4% vs. 66.6%) and lumbar curvecorrection (60.7% vs. 60.4%) were similarfor AIS and ADULT, respectively (P >0.05). Most common lowest instrumentedvertebra for AIS was T12 and L1 (31%each) and for ADULT was T12 and L1(21% and 36%, respectively). Meannumber PSF levels (9.7 vs. 10.8),posterior osteotomies (2.5 vs. 4), bloodloss (841 vs. 929 ml), blood transfused(335 vs. 206 ml), operative time (269 vs.276 minutes), and hospital stay (5.5 vs.5.6 days) were similar for AIS vs.ADULT, respectively (P > 0.05). Meantotal complications per patient was less forAIS than ADULT (0.2 vs. 0.6,respectively, P < 0.05).Conclusion: Comparison of acute resultsfollowing PSF for MT scoliosis<60°between AIS and ADULT demonstratedsimilar MT correction, number PSFlevels, blood loss, and hospital stay.Complications were uncommon. AIS hadfewer complications than ADULT. Furtherresearch will compare long-termoutcomes.
356Surgical Management of Flexion-Distraction InjuriesAndrew James Grossbach, David Kung,Patrick W. HitchonIntroduction: Flexion-distraction injuriesoccur due to distractive forces causingdisruption of the posterior and middle
spinal columns. These fractures classicallyconsist of a fracture line through theposterior boney elements, however,involvement of the posterior ligamentouscomplex is common. Surgical treatment isoften required for these unstable injuriesbecause the associated ligaments healpoorly and conservative managementoften leads to kyphotic deformity.Methods: Patients with flexion-distractioninjury who were treated between May2003 – December 2010 were prospectivelyfollowed. Asia score and degree ofkyphotic angulation were recorded atadmission, discharge, and follow-up.Minimum follow-up was 60 days.Results:We identified 27 patients, onewho declined surgery. All had injury toposterior ligamentous complex. Theaverage canal compromise was 10% ±21%. All underwent open reduction andposterior instrumentation except 2 whounderwent percutaneous pedicle screwfixation. Seven underwent short segmentinstrumentation. Two lacked sufficientfollow up. Mean follow-up was 14.2months. Average kyphotic angulation was11.3º on admission, 5.9º at discharge, and7.6º at follow-up. Average Asia scoreimproved from 4.3 to 4.5. Averagekyphosis in the short segment fixationgroup was 5.6º on admission, -1.3º atdischarge, and 1.4º at follow-up. Averagekyphosis in the long segment fixationgroup was 12.3º on admission, 8.0º atdischarge, and 9.6º at follow-up. AverageAsia score was 4.43 at both admission andfollow-up in the short segment group, andimproved from 4.37 to 4.58 in the longsegment group. The patient who declinedsurgery has persistent back pain andprogression of kyphosis from 8º to 32º at5 months.Conclusion: For thoracolumbar flexion-distraction injuries, posteriorinstrumentation is favored to correctdeformity and restore stability. Shortsegment instrumentation, one level aboveand below injury, is sufficient to achievethese results. Conservative managementoften leads to kyphotic deformity.
357Recapping Hemilaminoplasty forSpinal Surgical Disorders Using withUltrasonic Bone CuretteHidenori Matsuoka, Yasunobu Itoh, Kazuo WatanabeIntroduction:We developed a novelmethod of the recappinghemilaminoplasty in a retrospective studyof the patients with spinal surgical
disorders. This report describes thesurgical technique and the results of thehemilaminoplasty using with ultrasonicbone curette. The aim of this study was toexamine the safety and effectiveness ofhemilaminoplasty technique in spinalsurgery.Methods: Twenty-nine patients who hadundergone recapping hemilaminoplastywith ultrasonic bone curette for spinalsurgical disorders between 2003 and 2010did not need spinal canal enlargementafter the indradural procedure wascompleted. Ultrasonic bone curette wasused for division of the posterior elements.After resection of the lesion, the excisedlamina was replaced exactly in situ to theiroriginal anatomic position with titaniumplate. In this study group, there were 17men and 12 women with a mean age of47.4 (range, 4-74 years). The meanfollow-up period was 38.4 months(ranged, 5-91 months). The mean follow-up period was 38.4 months (range, 5-91months). All patients were observed bothneurologically and radiographyically bydynamic plain radiographs and computedtomography (CT).Results: The mean number of resected andrestored lamina was 1.7. CT confirmedprimary bone fusion in the all patients by6 months after surgery. Recappinghemilaminoplasty was done safety toobtain an enough wider laminotomy spacefor an intradural procedure preservingposterior elements including spinousprocess, interspinal ligaments,supraspinous ligament and facet joint. Theultrasonic bone curette did not cause anydural lacerations. Intradural procedure,dural reconstruction, and bone recappingwere achieved without majorcomplications such as postoperativecerebrospinal fluid in allpatients.Postoperatively, no majorcomplications such as postoperative spinalcanal stenosis, facet arthrosis, or kyphosiswere reported.Conclusion: Recapping hemilaminoplastyis a useful posterior approach forintraspinal canal procedure preserving theposterior elements. This method allowsanatomical reconstruction of the excisedbone preserving the posterior surroundingtissues.
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES84
DIGITAL POSTER ABSTRACTS

358Does Cervical Spinal Canal StenosisAffect the Neurological OutcomesAfter Spinal Cord Injury WithoutRadiological Evidence of Trauma?Tsuneaki Takao, Takeshi Maeda, Seiji Okada, Keiichirou Shiba, Takayoshi Ueda, Itaru Yugue, Eiji Mori,Osamu Kawano, Hiroaki Sakai, Muneaki Masuda, Tetsuo Hayashi,Yuichirou Morishita, Fumihiko KatohIntroduction: The aim of this study is toevaluate the effect of cervical cordcompression on neurological outcomes forSCIWORA, and discuss the indication oftheir treatments.Methods: 47 patients and 606 controlsubjects of health volunteers wereretrospectively selected. The diameters ofcervical cord were measured at the levelof C2-3 to C7 by MR image. Wecalculated the general incidence rate ofSCIWORA (0.00003). The relative andabsolute risks of spinal canal stenosis onincidence of SCIWORA at the level ofC3-4 were evaluated. We also evaluatedthe relationship between spinal canalstenosis and ASIA impairment scale at thetime of admission and discharge.Results: The diameters for the subjectswith SCIWORA were significantlynarrower than that for the subjects withhealthy volunteers at all levels. Only 6 outof 606 healthy volunteers (1%)demonstrated the evidence of spinal canalstenosis (less than 7mm), however, 24 outof 30 subjects with SCIWORA (80%)demonstrated the evidence of spinal canalstenosis. The relative risk of spinal canalstenosis on incidence of SCIWORA was400 times higher than that of withoutspinal canal stenosis. However, theabsolute risk of spinal canal stenosis was0.0008. There were no significantrelationships between C3-4 corddiameters and ASIA motor scores both atthe time of admission and discharge.Conclusion: There were no significantrelationships between the evidence ofspinal canal stenosis and neurologicaloutcomes for SCIWORA. As SCIWORAis rare trauma, the values between relativeand absolute risks demonstratedremarkable differences. It is important tomake a decision for the indication ofprophylactic operation under considerationof both risks, and prophylactic operationshould be considered in case of highabsolute risk. Our results suggested thatdecompression surgery of canal stenosisin SCIWORA should not berecommended as a prophylactic therapy.
359Posterior Approaches for ThoracicDisc Herniations: Is Anterior SurgeryNecessary? Experience with 24Consecutive CasesRamanan Sivakumaran, Nitin R. PatelIntroduction: The optimal surgicalapproach for thoracic disc herniations isopen to much debate and controversy. Wepresent our experience of the posteriortrans-pedicular and trans-facet pedicle-sparing approaches for all types ofthoracic disc protrusions.Methods: Between 2001 and 2010, thesenior author performed posterior thoracicdiscectomy via a trans-pedicular or trans-facet pedicle sparing approach in 24consecutive patients with 25 symptomaticdisc herniations. Clinical, radiological andoperative data was analysedretrospectively, with follow-up durationranging from 4-36 months. No patientswere lost to follow-up. Twenty-fourpatients {17 women & 7 men} with amean age of 56 years {range 36 - 79}were included. All disc herniations werelocated between T6/7 and T11/12. Pre-operative clinical features includedmyelopathy (n = 17), radicular pain (n =15), axial pain (n = 8), sensory disturbance(n = 13) and bladder dysfunction (n = 13).On pre-operative imaging, and 11 discherniations were calcified (including 3with an intradural component) andfourteen were found to be soft.Results:A total of 26 operations wereperformed on 24 patients with twenty-fivesymptomatic disc herniations. Thiscomprised 16 unilateral and 4 bilateralapproaches performed as a singleprocedure. In addition to these, one patienthad two operations at one level andanother had two procedures for twoseparate levels. Complete spinal corddecompression was achieved in allpatients. Following surgery, 16 patientsreported improvement in myelopathy(84%). Radicular pain improved in 8patients (62%) and axial pain improved in4 patients (50%) post-operatively. Twelvepatients (92%) reported an improvementin bladder dysfunction and sensorydisturbance improved in 9 (69%) patients.No major complications occurred in ourseries and overall, 20 (83%) patientsreported improvement following surgery.Conclusion: In our experience, posteriorapproaches are suitable for all thoracicdiscs including large centrally calcifiedherniations. These approaches have a lowcomplication rate with good clinicaloutcomes.
360BMP-2 Inhibits Tumor Growth ofHuman Renal Cell Carcinoma byInduction of Bone FormationLin Wang, Paul Park, Khoi Duc Than,Shayan Rahman, Frank La Marca, Chia-Ying LinIntroduction: Renal cell carcinoma (RCC)is the fourth most common metastatictumor of the spine. Bone morphogeneticprotein-2 (BMP-2) has been shown tohave inhibitory effect on many tumortypes. However, the effect of BMP-2 onhuman RCC is still unknown.Methods: Human renal carcinoma celllines ACHN and Caki-2 were cultured andinjected with BMP-2 (30 ug/animal) orvehicle control into NOD/SCID mice.After 12 weeks, animals were sacrificedfor evaluation of bone formatiom.Radiographs were obtained using theFaxitron x-ray. For microcomputedtomograpgy (micro-CT) analysis,specimens were scanned on a micro-CTscanner. For histomorphometry,specimens were stained for hematoxylinand eosin (H&E) and Masson’s trichrometo evaluate for collagen type I protein inthe newly formed bone. Sections werestained with von-Kossa staining toidentify the calcification duringosteogenesis in the tumor.Results:All animals receiving low numberof ACHN (1x10^4) and Caki-2 (5x10^4 )cells treated with 30 µg BMP-2 per animalshowed limited tumor growth withsignificant bone formation, whileuntreated cells developed large tumormasses without bone formation inNOD/SCID mice.Conclusion: BMP-2 inhibited tumorgrowth of human renal cell carcinomacells by inducing bone formation. BMP-2may be useful as a novel therapeutic agentfor treatment of renal cell carcinoma.
361Minimally Invasive Spine Surgery: ARealistic Appraisal via Patient SelfReport of OutcomesPhillip G. St. Louis, Daniel Castillo, Tara Batz, Jennifer Clements, Kaity Colon-SanchezIntroduction:Minimally Invasive Surgical(MIS) techniques in the lumbar spineresults in long term improvement infunctional status and pain level.Methods: Ninety-seven patients weretreated with MIS Lumbar Spine Surgeryand followed for an average of 18 months.The average age was 56.06 years andBody Mass Index was 29.41 (overweight
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 85
DIGITAL POSTER ABSTRACTS

by U.S. Dept. of Health and HumanServices). Results were obtained byreview of 1) perioperative data (estimatedblood loss, operative time, length ofhospital stay, postoperative medicationuse, postoperative complications) and 2)validated outcome measurement tools(ODI, SF-36, and patient satisfactionsurveys) completed preoperatively and atfollow-up postoperatively.Results: Patients experienced longeroperative time, shorter hospital stay, andlower narcotic use immediatelypostoperatively, as compared to publishedresults in open procedure studies. Therewere no perioperative transfusions orpostoperative infections observed. Long-term postoperative patient satisfactionsurveys revealed that 61% of patientswere very satisfied with their surgicalexperience and 44% of patients disclosedthat they were taking none or less painmedication postoperatively. Seventy-ninepercent of patients indicated no change oran increase in functional daily activities(95% confidence interval [CI], 0.9, 42.5).Ninety-three percent of patients reportedno change or an improvement in work andphysical activities (95% CI, -11.6, 41.6).Eighty percent of patients reported areduction in pain postoperatively (95% CI,10.3, 45.5). Results of Oswestry DisabilityIndex survey showed that sixty-sevenpercent of patients had improvementpostoperatively as compared topreoperatively (95% CI, 22.1, 14.7).Conclusion: Patients treated with MISspine surgery demonstrated highsatisfaction regarding the surgicalexperience, an improved functional status,and an ability to manage in everyday life.This operative technique results in areduced surgical complication rate in thosepatients that are overweight and obese, asalso a reduced hospital length of stay anddecreased postoperative narcotic use.
362Prospective Study of ClinicalOutcome After Minimally InvasiveTransforaminal Lumbar Inter-bodyFusion (MI-TLIF) for DegenerativeSpondylolisthesis Grades I-IIIManish Singh, Olawale SulaimanIntroduction:Minimally invasivetransforaminal lumbar interbody fusion(MI-TLIF) is a new surgical techniquethat allows for circumferential arthodesiswith adequate decompression of neuralstructure without excessive iatrogenic softtissue/muscle injuries. There are only afew studies that have carefully and
prospectively collected and reportedclinical outcomes in patients withdegenerative spondylolisthesis treatedusing the MI-TLIF technique. Here, wepresent a comprehensive analysis of ourexperience in treating this group ofpatients.Methods:Analysis of preoperative,intraoperative and post-operative clinicaldata was collected on patients undergoingMI-TLIF (40 pts.) and open procedure (10pts.) for degenerative spondylolisthesisgrades I-III. All patients completedOswestry low back pain disability index(ODI) and visual analog pain scale (VAS)pre-operatively and at 6 weeks, 3, 6, 12months and 24 months. Fisher test wasused for association between proceduregroups and complication and student t testwas used for comparison of continuousvariables.Results:Minimum follow-up period was12 months. Average LOS was = 48 hoursfor 1 level and 2-3 days for 2 levels.Average EBL was 100 ml for 1 level,200ml for 2 level. All patients achieved atleast a 10% improvement in their ODIwith mean ODI improving to 36.70 at 6weeks, 26.8 at 6 months and and 23.78 at1 year. We also did a cost compassionanalysis of open vs. MIS-TLIF and fusionrate.Conclusion:MI-TLIF is an effective, cost-effective, less morbid treatment option forsymptomatic spondylolisthesis grades I-III.
363The Appearance of Dural SealantsUnder Magnetic Resonance ImagingPhiroz E. Tarapore, Pratik Mukherjee,Praveen V. Mummaneni, Christopher P. AmesIntroduction: Dural sealants are an adjunctto obtain watertight closure afterintradural procedures. This study aims tocharacterize the appearance on magneticresonance imaging of three commonlyemployed dural sealants: fibrin glue,polyethylene glycol based hydrogel(PEGH), and a bovine serum albumingluteraldehyde polymer (BSAG).Methods: Patients who underwent spinalintradural procedures that included the useof dural sealant during closure wereidentified retrospectively. Post-operativedata was gathered on 15 patients,including complications such aspseudomeningocele formation andinfection, were gathered. The appearanceof dural sealants on follow-up MRI scanswithin 3 days of surgery was analyzed.
Results: Fifteen patients were identified (5with fibrin glue, 5 with PEGH, and 5 withBSAG applied during closure) withappropriately timed post-operative MRIscans. All three substances wereidentifiable based on anatomic locationand imaging characteristics on post-operative MRI in standard T1, T1post-gadolinium, and T2 fast spin echosequences. Definite differentiationbetween cerebrospinal fluid (CSF) andfibrin glue or PEGH was not possible withthe T1-weighted pre- or post-gadoliniumsequence, or with the T2-weighted fastspin echo sequence. Differences inintensity between CSF and BSAG werealso not significant on either T1-weightedsequence, but they were statisticallysignificant on the T2-weighted fast spinecho sequence. All patients had anuneventful post-operative course, and nopatients developed post-operativepseudomeningocele at 30 days.Conclusion:Water-based dural sealantssuch as fibrin glue and PEGH are difficultto differentiate from CSF on standard T1-weighted, T1-weighted post-gadoliniumand T2-weighted fast spin echosequences, while BSAG is easilyrecognized on the T2-weighted fast spinecho sequence. Recognition of water-based sealants therefore requirescommunication between the neurosurgeonand the neuroradiologist to avoid post-operative misidentification.
364Metanalysis of HeterotopicOssification (HO) following CervicalArtificial Disc Replacement (CADR)Kenneth Pettine, Thomas C. CoburnIntroduction:Ascertain the incidence ofHO following CADR and whether thisincidence is influenced by implant type,class of data, or length of follow-up.Methods: Forty-seven articles/abstractswere reviewed on HO following CADR.This information was stratified based onclass of data, severity of HO (McAfeeclassification), length of follow-up andtype of implant.Results: Class I data indicates theincidence of grade-4 HO in ProDisc-C tobe 4% at 24 month and 8% at 48-monthfollow-up, 4% in Kineflex-C at 24months, Bryan not reported. PCM had4.4% incidence of grade-3 or 4 HO at 24month follow-up. Prestige had zeroanterior HO at 2 and 5 year follow-up.Class II data indicates ProDisc-C at four-year follow-up grade-0 - 12%, 1 - 13%, 2- 12%, 3 - 45%, 4 - 18%, Mobi-C disc at
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES86
DIGITAL POSTER ABSTRACTS

two-year follow-up grade-0 - 25%, 1 -9%, 2 - 33%, 3 - 3%, 4 - 6%, M6 at two-year follow-up was 48%. 17.8% of Bryandisc at one-year follow-up had some typeof HO and 6.7 had grade 3 or 4. One classIII paper reported a comparison of threeCADR with an HO incidence of Bryandisc 21%, Mobi-C 52.5% and ProDisc-C71.4%. One class II paper reported on theefficacy of NSAIDs to prevent HO, 64%with HO took no NSAIDs while 60%without HO took NSAIDs. Grade-3 and 4HO in all the FDA IDE studies decreasedrange of motion but did not appear toimpact clinical success. The discrepancyin data between class I, II and III will bediscussed.Conclusion: Implant type, length of follow-up and class of data appear to influencethe reported incidence of HO. There islittle or no data to indicate HO can bedecreased by drugs or surgical technique.
365Adjustment of Suboptimally PlacedLumbar Pedicle Screws DecreasesPull-Out Strength and AltersBiomechanics of the Construct: A Pilot Cadaveric StudyRishi Kumar Wadhwa, Jai D. Thakur, Imad S. Khan, Osama Ahmed, Alan Ogden,Debi P. Mukherjee, Bharat Guthikonda,Anil NandaIntroduction: Lumbar pedicle screws areplaced for internal fixation and help toenhance fusion. Optimal screws aremedially directed, parallel to or pointingto the superior endplate, and penetrate 50-80% of the vertebral body. (1-4)“Suboptimal” pedicle screws can beinadvertently placed within the confines ofthe pedicle and vertebral body but aresometimes replaced to obtain a moreacceptable post-operative image. Wedefine a suboptimal screw to be in thepedicle and body and not violating bone,however not parallel to the superiorendplate. We suspect “cored-out” groovesleft in the bone from the initial screwplacement compromise the integrity of thebone and thus the construct. We testedboth screw pullout strength andbiomechanics of the construct.Methods: DEXA scans and L4-5laminectomies were performed on 4 fresh-frozen cadaveric lumbar spines. Weplaced 2 optimal L4 pedicle screws, 1optimal L5 screw and one suboptimalscrew in L5 (Fig 1a). Axial rotation,flexion/extension and lateral bending weretested and the suboptimal screw wasreplaced optimally (Fig 1b) and retested.
Pullout strength was also performed onthe revised screw and the contralateralscrew.Results: DEXA demonstrated 2 osteopenicand 2 osteoporotic specimen. Using pairedt-test, values for both axial rotation (P =.038) and flexion/extension (P = .036)were significantly decreased in the revisedconstruct. Pullout strengths, with a meandifference of 435 newtons, were alsosignificantly decreased (P = .042) in therevised screws (Fig 2).Conclusion:We found significantdifferences in pullout strength, axialrotation, and flexion/extension in a revisedlumbar pedicle screw construct. Ourrecommendation is to take great care toinitially place screws in an optimalposition. Also, we recommend leaving asuboptimally placed lumbar pedicle screwin. More specimen will likely increase thepower of this pilot study.
366Application of NeuromuscularBlockade and Intraoperative ThreeDimensional Imaging in theReduction of Basilar Invagination:Technical NoteNader S. Dahdaleh, Brian J. Dlouhy,Arnold H. MenezesIntroduction: The treatment of basilarinvagination in the pediatric age group isdependent on the possibility ofpreoperative reduction. Reducible lesionsobviate a ventral decompression andrequire a dorsal only approach forstabilization with or without a suboccipitaldecompression.Methods:We describe a technique ofintraoperative reduction of basilarinvagination with the use of generalanesthesia, and neuromuscular blockadein the presence of crown Halo traction.Using the O-arm a 3D scan is generated inthe sagittal plane to demonstrate thereduction intraoperatively. This techniquewas successful in 6 pediatric patients withbasilar invagination.Results: The average age was 10.8 years,they were followed for a mean period of8.5 months. The patients had mild basilarinvagination or partial reduction inextension on preoperative MRI.Intraoperative reduction was demonstratedin all using the after mentioned techniquewith intraoperative CT. All underwentoccipitocervical fusion and all but oneunderwent a suboccipital decompression.There were no complications to theoperation and all but one reportedimprovement of symptoms on the last post
operative visit. Radiographically allpatients maintained reduction.Conclusion: Intraoperative reduction usingneuromuscular blockade andintraoperative traction is an effectivemethod to further reduce basilarinvagination in the pediatric age group.This is the first reported application ofintraoperative CT imaging using the o-arm in craniocervical surgery todemonstrate in detail successful reduction.
367Spine Surgery at an AmbulatorySurgery CenterKenneth Pettine, Thomas C. CoburnIntroduction: To determine if spine surgerybe safely performed at an ambulatorysurgery center (ASC)?Methods: 710 spine surgeries performed atan ASC from spring 2005 through 2008were prospectively evaluated.Instrumented Spine Surgery: 333 Patients,Anterior Cervical Fusion: 193 Patients,Cervical Artificial Disc: 57 Patients,Lumbar Artificial Disc: 83 Patients, Non-Instrumented Spine Surgery: 377 Patients,Lumbar microdiscectomies and/or nervedecompressions. All cases were evaluatedwith ODI, NDI and VAS. The patientswere evaluated at pre-op, three-month,six-month, one-year and often two-yearfollow-up. Analysis also included minutesin OR, recovery and convalescent centeras well as patient satisfaction and cost.This data will be presented.Results: There were no perioperativecomplications and no unplanned transfersin the ACF group. There was statisticallysignificant improvement in NDI and VASvalues (P < 0.01). Patients who underwentcervical ADR showed statisticallysignificant improvement in NDI and VASat two-year follow-up to a p-value < 0.02.There were no perioperativecomplications and no unplanned transfersin these patients. One lumbar ADR patienthad an unplanned hospital transfer. Therewas a statistically significant improvementin ODI and VAS to a p-value < 0.001 at two-year follow-up. One patient in thenon-instrumented spine surgery group hada perioperative complication. There wereno unplanned transfers to the hospital. Allof the patients undergoing an anteriorcervical fusion, cervical and lumbarartificial disc replacement and non-instrumented lumbar spine surgery werereleased home within 24 hours of theirsurgery. Outside insurance audits indicatea 60% cost savings when performingthese procedures at an ASC vs. a standard
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 87
DIGITAL POSTER ABSTRACTS

hospital setting. Patients reported a 97%satisfaction rate.Conclusion: Prospective analysis of 710spine cases at an ASC indicate anteriorcervical fusion, lumbar nervedecompression, discectomy, lumbar andcervical artificial disc replacements can besafely performed with efficacy at an ASC.
368Cervical Artificial Disc Replacementat an Ambulatory Surgery CenterKenneth Pettine, Thomas C. CoburnIntroduction: The following data will showCervical Artificial Disc Replacements(CADR) can be performed at an ASCwith safety and efficacy.Methods:A total of 224 patients haveundergone cervical ADR at the LovelandSurgery Center. These included fivedifferent types of artificial discs. Elevenpatients received the Kineflex-C, 39patients received the NeoDisc, 21 patientsreceived the ProDisc-C, 10 patientsreceived the Discover and 143 patientsreceived the Prestige.Results: There were 162 patients who hada one-level artificial disc replacement.Fifty-six patients received a two-levelartificial disc replacement, five patientsreceived a three-level artificial discreplacement and one patient a four-levelartificial disc replacement. The averageage of the patients was 45.3 years with aBMI of 27. The ratio of smokers to non-smokers was 1:6. There were a total ofthree re-operations, one patient in 2007,one patient in 2008 and one patient in2009 all underwent revision of the originalimplant. None of these re-operationsoccurred during their initial stay. Theaverage operative time for a one-level discreplacement was 63 minutes, a two-levelprocedure averaged 86 minutes and theaverage operative time for a three-levelprocedure was 100 minutes for an overallaverage of 84 minutes. The average timein the convalescent center was 16 hours.Every patient left within 24 hours with nounplanned transfers to the hospital in anycase. Pre-op NDI went from 54.6 to 23 at2-year follow-up (P < 0.01). Pre-op VASwent from 74 to 28 at 2-year follow-up (P< 0.006).Conclusion: Based on statisticallysignificant improvement in NDI and VASwithout surgical complications, this dataindicates cervical artificial disc surgerycan be safely performed with clinicalefficacy at an ambulatory surgery center.
369Comparison of Surgical OutcomesAfter Cervical Laminoplasty: OpenDoor Technique vs. French DoorTechniqueSun-Ho Lee, Sungjin Kim, Dong-Geun Lee,Eun-Sang Kim, Whan EohIntroduction: Cervical laminoplasty is aneffective method for decompressingmultilevel cervical spinal cordcompressions. The procedures used aremainly classified as Open-door andFrench-door laminoplasty, but it is stillunclear whether laminoplasty techniqueaffects cervical alignment and clinicaloutcomes, including axial symptoms andhealth-related quality of life.The aim ofthis study was to compare the surgicaloutcomes of these two methods ofcervical laminoplasty (Open-doorlaminoplasty and French-doorlaminoplasty).Methods: Fifty-one patients underwentcervical laminoplasty over a 2-year periodfor cervical spondylotic myelopathy,ossification of the posterior longitudinalligament, or both. The following criteriawere evaluated and comparedretrospectively for Open-doorlaminoplasty (Group A) and French-doorlaminoplasty (Group B): Nurick grades,Japanese Orthopedic Association (JOA)scores, Neck disability indices (NDI), andVisual Analog Scale (VAS) scores foraxial neck pain and radiating pain. Forradiological evaluations, changes ofcervical lordotic angles and ranges ofmotion (ROM) were measured at C2-C7.Results: Postoperatively, neurologicalimprovement was 12.5% according to theNurick grade and 28% according to theJOA score in all study subjects. Inparticular, Nurick grade was significantlyimproved in group A (P < 0.05).Furthermore, recovery rates were higherin group A, which achieved rates of 23.5%according to Nurick grade (P < 0.05) and44.4% according to JOA scores (P <0.05). Radiologically, cervical lordoticangle and ROM were more significantlydecreased in group B (P < 0.05). In groupB, there were seven complications,namely, 2 of C5 palsy, 3 wound infections,1 pulmonary thromboembolism, and 1postoperative hematoma, and in group A,there were only two complications, that is,one CSF leakage and one C5 palsy.Conclusion: Though both open-door andFrench-door laminoplasty were found tobe effective for treating cervicalcompressive myelopathy, the open-doortechnique seems to be superior to the
French-door technique with respect toclinical and radiological outcomes andcomplication rates.
370Outpatient Minimally InvasiveLumbar FusionKenneth Pettine, Thomas C. CoburnIntroduction: This abstract describes asurgical technique involving a 3-5cmmidline incision with standard exposure tothe facet joints followed by a bilateralhemi-laminotomy, medial facetectomyand foraminotomy with posterolateralfusion or a complete facetectomy with aTLIF interbody fusion both utilizing theCoflex-F implant.Methods: 90 posterolateral fusions wereperformed, 46 at one level and 44 at twolevels. There were 7 cases performed witha TLIF procedure at one or two levels.Results:Average pre-operative VAS forone level Coflex-F was 7 and ODI of50%. At 6 month follow up VAS was 21(P < 0.001) and ODI was 21 (P < 0.003).The average pre-op VAS for a 2 level was7 with an average ODI of 54. At 6-monthfollow-up the VAS was 21 (P,0.001) andthe ODI was 34 (P < 0.01). The averageoperative time for a one-level procedurewas 42 minutes and a two-level procedureaveraged 73 minutes. Adding a TLIFincreased the operative times an averageof 17 minutes per level. All TLIF fusionswere performed utilizing locally harvestedautogenous graft, BMP and an expandablePEEK implant. The average blood loss fora one-level procedure was 23cc and a two-level procedure was 38cc. The averagefluoroscopy time was three seconds forlocation identification prior to skinincision and post operative implant x-rays.Two cases required more than a 23-hourstay. There were four re-operations. Thesecases will be discussed.Conclusion: This series of cases indicatesperforming a one- or two-level lumbarfusion through a minimal midline incisionusing the Coflex-F implant can besuccessfully performed as an outpatientprocedure. All spine surgeons are familiarwith a midline approach. This procedureincorporates the standard currenttechniques through a small MIS dissect.
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES88
DIGITAL POSTER ABSTRACTS

371The Incidence of Adjacent SegmentDisease Following Thoracic PedicleScrew FixationRobert F. Heary, Nitin Agarwal, Sharanya Mohanty, Osamah J. Choudhry,Reza John Karimi, Antonios MammisIntroduction: Pedicle screw fixation is awidely utilized technique employed forconditions ranging from spine deformitiesto fractures. The use of pedicle screws, asopposed to hooks, in spine deformitysurgeries has demonstrated lowercomplication rates, better three-dimensional correction, better pull-outstrength, and shorter fusion lengths.Traditionally, pedicle screws were used inthe lumbar spine, however, pedicle screwsare being used with increasing frequencyin the thoracic spine, as a more favorablealternative to hooks. While safety concerns,such as the incidence of adjacent segmentdisease (ASD) following cervical andlumbar fusions (30% incidence of ASD)have been reported, these issues have yetto be thoroughly addressed for thethoracic spine.Methods:A retrospective review of aprospectively maintained database wasperformed to determine the incidence ofcomplications for 123 consecutive patients(76 males and 47 females, mean age - 39years), who underwent thoracic pediclescrew fixations over 13 years. Inclusioncriteria were: adults with thoracic pediclefixation. Patients were excluded if:pregnant or lactating, children, andprisoners. By comparing the preoperativeand postoperative radiographic imaging,the occurrence of ASD and disease withinthe surgical construct was determined.Results: Definitive radiographic fusionwas detected in 108 (88%) patients. Sevenincidences of hardware failure and eightlucencies surrounding the screws wereobserved. In total, 1135 thoracic pediclescrews and 233 rods were placed. Thirty-two (26%) patients demonstrated diseasewithin the surgical construct, fifteen(12%) developed ASD, and thirteen (11%)experienced perioperative complications.Mean duration of follow-up was 50months.Conclusion: Radiographic evaluationshowed the use pedicles screws forthoracic fixation to be an effectivestabilization modality. The analysis oflong-term patient outcomes demonstrateda lower incidence of adjacent segmentdisease compared to previously publishedstudies.
372Long-Term Outcomes from IDE Studyof OptiMesh Interbody Fusion DeviceMick J. Perez-CruetIntroduction: OptiMesh interbody fusiondevice is inserted through a small portalthen expands when filled with graftmaterial to conform to the endplates,resulting in a large structural fusionconstruct.Methods:An ongoing prospective,multicenter, IDE study to evaluate safetyand effectiveness of OptiMesh filled withmixture of allograft and autograft to treatsingle level lumbar degenerative discdisease. Phase II randomized trial wasconducted comparing Optimesh to acortical allograft spacer with addedautograft. Pedicle screw constructs addedas fixation. Clinical outcomes measuredusing VAS and ODI. Fusion wasdetermined by independent radiologists.Results:At 11 sites between 7/03 and10/10, 123 patients were implanted withOptiMesh and 33 patients with control.For the OptiMesh group, 107 reached 12months, 85 at 24 months, 41 at 36 months,and 15 at 48 months. Average age 51, 66(54%) female and 57 (46%) male. MeanVAS/ODI scores were 6.8/45.4 pre-op,2.8/33.8 at 6 weeks, 2.5/22.3 at 12months, 2.7/24.1 at 24 months, 2.5/21.4 at36 months, and 2.4/20.2 at 48 months.Fusion rates are 84% at 12 months, 92%at 24 months, 91% at 36 months, and 95%at 48 months. No OptiMesh failures, noloss of graft containment, and noexpulsions. For the control group, 28reached 12 months, 12 at 24 months, 13 at36 months, and 4 at 48 months. Averageage 54 years, 18 (55%) female and 15(45%) male. Mean VAS/ODI scores were7.6/48.7 pre-op, 2.8/35.3 at 6 weeks,3.4/27.0 at 12 months, 3.1/26.3 at 24months, 2.5/18.8 at 36 months, and3.4/17.0 at 48 months. Fusion rates are81% at 12 months, 100% at 24 months,100% and at 36 months.Conclusion: These current study data showthat OptiMesh is safe and effective withclinical and fusion results equivalent toallograft spacer used as interbody fusiondevice with pedicle screw fixation. Thisstudy is ongoing.
373Movement of RetroperitonealStructures with Change in Positionfrom Supine to Lateral DecubitusUsing Magnetic Resonance Imaging(MRI): Implications on the LateralApproach to the Lumbar SpineArmen Deukmedjian, Juan S. Uribe, Elias Dakwar, Tien V. LeIntroduction: In the MIS lateral approachto the lumbar spine, the surgical corridorlies close to peritoneal structures at riskfor injury. Although preoperative imagingis performed supine, the procedure isperformed in the lateral position. Theeffect of positioning on abdominal viscerais unexamined. In this study we measurechanges in location of the aorta, venacava, and kidneys with regards to thespine when moving from supine to lateral.Methods: Lumbar 3T MRI’s wereperformed on 10 volunteers in supine, leftand right decubitus positions. These wereanalyzed, comparing the location of theaorta, vena cava and kidneys at the L1/2,L2/3, and L3/4 disc spaces, going fromsupine to left and right decubitus position.Results: In the right decubitus position, theaorta moves to the right 2.5mm at L1/2,5mm at L2/3 and L3/4, and slightlyanterior, with the greatest displacement of2mm at L1/2. The vena cava moves to theright 5mm and anterior at all levels. Theleft kidney for all patients moved anteriorranging from 0.7-4.7cm and caudal from0.2-2.2cm, while no conclusions weredrawn about the right kidney. In the leftdecubitus position, the aorta shifts to theleft ~1.5mm at all levels with very littleanterior/posterior displacement. At L1/2,there is significant shift of the vena cava1cm to the left, and 1.2cm anterior, and atL2/3 it shifts 5mm anterior and to the left.At L3/4 there is movement 1.5mmleftward and 1mm anterior. The leftkidney moved up to 2cmanterior/posterior, and from 1.4cm caudalto 2.4cm cranial. The right kidney movedanterior up to 4.5cm and from 1.6cmcaudal to 0.5cm cranial.Conclusion:We believe the movements wedescribe of the abdominal viscera with thepatient in lateral position are vital inpreoperative planning for MIS lateraltranspsoas surgery to prevent potentialcomplications.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 89
DIGITAL POSTER ABSTRACTS

374Metanalysis of Class I Results ofAnterior Cervical Decompressionand Fusion with Allograft andPlatingKenneth Pettine, Lukas Eisermann, Thomas C. CoburnIntroduction:What are the clinical resultsof anterior cervical discectomy and fusion(ACDF) with plating? Most spinesurgeons would answer a one-level ACDFhas a 95% fusion rate and 95% excellentclinical results. This perception is basedon class III or class IV data, retrospectivereviews typically performed by a spinefellow or resident on a senior author’ssurgical series.Methods: Class I data from six FDA IDEstudies involving ACDF allograft withplating were reviewed. The studiesinclude: The Prestige (265 patients),ProDisc (103 patients), Bryan (221patients), PCM (185 patients), Kineflex-C(133 patients), and Secure-C (144patients) artificial discs vs. intervertebralallograft with plating. Total number ofpatients included in this metanalysis was1,051. FDA clinical Success was verysimilar in all studies and defined as a 15point or 20% improvement in NDI, noreoperation, and no neurologicdeterioration.Results: The average re-operation rate fora pseudoarthrosis, adjacent leveldegeneration, or index level revision attwo-year follow-up was 9.8% (table oneillustrates individual study results).Clinical success rates at two-year follow-up averaged 68% (table two illustratesindividual study results).Conclusion: Based on a metanalysis of classI data, the results of ACDF with allograftand plating are a 9.8% reoperation rate attwo-year follow-up due to pseudoarthrosis,adjacent level degeneration or revision ofthe index surgical site and a 68% clinicalsuccess. These results emphasize theimportance in differentiating the validity ofinformation gained from class I vs. class IIIand IV data.
375Risk Factors Associated withDevelopment of Post-traumaticSyringomyeliaTaylor J. Abel, Nader S. Dahdaleh, Aaron From, Youssef Karram, Patrick W. HitchonIntroduction: Post-traumaticsyringomyelia (PTS) is an uncommon anddebilitating complication of spinal traumathat results in delayed onset of
neurological deficit. Until the recentadvent of magnetic resonance imaging,PTS was a largely under-recognized entityand clinical research of its risk factors andmechanisms is ongoing. Previous workhas suggested that post-traumaticdeformity leading to decreased residualcanal, increased angulation, andconcomitant blockage of subarachnoidCSF flow leads to PTS.Methods: Reviewing records from 1986 -2010, 22 patients treated for PTS wereidentified. Subsequently, 28 patients witheither flexion-distraction (17 patients) orfracture-dislocation (11 patients) injurieswho did not develop PTS were selected ascontrols. Data was reviewedretrospectively from the medical record.Angulation and residual canal wererecorded when neuro-imaging data wasavailable.Results: PTS patients presented with anaverage Frankel score of 2.4, wheras non-PTS patients presented with an averageFrankel score of 3.5. Majority of non-PTSpatients (96%) underwent surgical fusion,compared to only 40% of PTS patients. Atfollow-up, PTS patients had an averageangulation of 27 degrees and averageresidual canal of 63%. Non-PTS patients,conversely, had an average of 11 degreesof angulation and 71% residual canal.Conclusion: In our hands, PTS isassociated with a greater degree of post-traumatic kyphosis and canal stenosis.Our results suggest that early surgery, byreducing post-traumatic deformity, mayreduce the incidence of PTS. Thesefindings support early surgery forfractures associated with deformity andstenosis to prevent PTS.
376Comparison of ThromboembolicEvents in Open vs. Minimal AccessSurgical Technique in PosteriorSpinal FusionsMichael J. Cirivello, Daniel J. Coughlin,Chris J. Neal, Michael K. RosnerIntroduction: The purpose of the study wasto compare the incidence of pulmonaryembolism (PE) and deep venousthrombosis (DVT) in a patient populationafter receiving lower lumbar (L3 S1)posterior spinal fusion using eitherMinimal Access Surgical Technique(MAST) or open techniques. Additionallythis study evaluated the rate ofhemorrhagic complications related toearly thromboembolismchemoprophylaxis and treatment withheparin or low-molecular-weight heparin.
Methods: 126 Cases of posterior spinalfusion limited only to levels L3-S1 of thesenior author from 2004-2010 wereretrospectively evaluated. The populationwas divided based on technique, MAST(103) and open (23). The type ofchemoprophylaxis administered, rate ofsymptomatic DVT and PE, treatment afterdiagnosis of thromboembolism and theincidence of hemorrhagic complicationsof these two subpopulations weredocumented. The incidence of PEbetween the two subpopulations wasanalyzed using a student t-test to evaluatefor statistical significance.Results:Within the open posterior spinalfusion population, the mean post-operativeday (POD) that chemoprophylaxis wasstarted was 1.13 (3 on DOS, 22 on POD1,2 on POD2-4) with a PE rate of 4.1% (1).Of those patients who underwent fusionusing MAST, the mean POD forchemoprophylaxis was 1.08 (72 on POD1,10 on POD2-4, 18 were not started onDVT prophylaxis) with a PE rate of 2.9%(3). No reports of DVT were documentedwithin either group. There was nosignificant difference in the incidence ofPE using MAST vs. open technique (P =0.36) for L3-S1 posterior spinal fusions.Conclusion: There is no significantdifference in rate of PE or DVT betweensubjects who underwent MAST and openposterior spinal fusions. In addition, theuse of early heparin and low-molecular-weight heparin appear to have acceptablemargins of safety in both the prophylaxisand treatment of thromboembolic diseaseafter posterior spinal fusion.
377Early Chemoprophylaxis in thePrevention and Treatment ofThromboembolism in PosteriorSpinal FusionsMichael J. Cirivello, Daniel J. Coughlin,Chris J. Neal, Michael K. RosnerIntroduction: The purpose of the study wasto identify the incidence of pulmonaryembolism (PE) and deep venousthrombosis (DVT) in a patient populationreceiving early thromboembolismchemoprophylaxis (heparin or lowmolecular weight heparin) after spinalfusion and to evaluate the rate ofhemorrhagic complications in thispopulation related to treatment.Methods: 177 cases of degenerative anddeformity thoracolumbar spinal fusions in2004-2010 of the senior author wereretrospectively evaluated for thetimeframe and type of chemoprophylaxis
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES90
DIGITAL POSTER ABSTRACTS

started, the rate of symptomatic DVT andPE, the treatment after diagnosis ofthromboembolism and the incidence ofhemorrhagic complications.Results: In the study, the mean post-operative day (POD) that chemoprophylaxiswas started was 1.1 (137 on POD1, 16 onPOD2-4, and 21 had no prophylaxisstarted). The PE rate was 5.6% (10), andthere were no DVTs detected. All 10 casesof PE received full anticoagulation afterdiagnosis as early as POD1 with anaverage POD of 2.4. There were nohemorrhagic complications.Conclusion: Heparin and low molecularweight heparin appear to have acceptablemargins of safety in both the prophylaxisand treatment of thromboembolic diseaseafter spinal fusion.
379Less Invasive Surgery ofThoracolumbar FracturesAbdolhamid KhoshabIntroduction:Minimally invasive spinesurgery is growing rapidly. Comparedwith the traditional posterior approachwith long and wide exposure,theminimally invasive approach offerssignificant advantages in treating patientswith spine fractures.Methods: 43 patients (age range, 21-73years) underwent minimally invasivespine surgery ± BKP,and 14 patientsunderwent conventional open surgery. Allpatients underwent pre and postoperativeCT, MRI to analyze the fracture. Bloodloss, postoperative complicationsincluding wound complication, leakage,and haradware malposition, also operativetime, postoperative pain score,postoperative analgesic usage, andrecovery time after surgery were recorded.Results: Blood loss was minimal in the 1stgroup (<40 mL),in the open group rangedfrom 250 to 500 mL. Operative timeranged from 75 to 90 minutes in the 1stgroup and 78 to 100 minutes in the othergroup. Radiation exposure was higher inthe MIS group. No patients in the 1stgroup experienced any postoperativecomplication. In the conventional surgerygroup, 4 patient had a superficial woundinfection. Postoperative VAS wererecorded on postoperative day (1st group:day 1, 5/10, open group: day 1, 6/10).Patients in the MIS group wereambulating 2 to 3 days postoperatively,while in the open group were ambulating3 to 4 days.Conclusion: This system is applicable formost burst fractures. We recommend
using the minimally invasive approach fortreatment of thoracolumbar fractures infresh fractures and in cases that do notrequire excessive force to reduce thefracture. The minimally invasive spinesurgery system decreased intraoperativeblood loss. The procedure is fast, andpatients can ambulate shortly aftersurgery. Analgesics are used lesscompared with the open group. The samecan be said regarding postoperative VASscores. Radiation exposure was higher inthe 1st. group. This could potentially beavoided if and when navigation systemsreplace conventional fluoroscopy. Usingthe MIS system to treat thoracolumbarburst fractures offers many advantagesand could replace conventional opensurgery in most cases.
380International Classification ofDisease Clinical Modification 9Modeling of the Patient ComorbidityScore Predicts Incidence ofPerioperative Complications in aNationwide Inpatient SampleAssessmentRohan Chitale, Peter Campbell, Sanjay Yadla, Robert G. Whitmore,Mitchell Gil Maltenfort, John K. RatliffIntroduction: Our group has developed abasic comorbidity score (CMS) from aprospective study of spine surgerypatients. To validate the CMS, wedeveloped an ICD-CM-9 model of thescore and correlated the score withcomplication incidence in a group ofpatients from the Nationwide InpatientSample (NIS) database. We compared thepredictive value of the score to theCharlson index.Methods:We conducted a retrospectiveassessment of NIS patients undergoingcervical or thoracolumbar spine surgeryfor degenerative pathology. We generatedan ICD-9 coding-based model of ourprospectively derived CMS, categorizingdiagnostic codes to represent relevantcomorbidities. Multivariate models wereperformed to eliminate the leastsignificant variables. ICD-9-CM codingwas used to calculate a Charlsoncomorbidity score for each patient.Accuracy of the CMS was compared tothe Charlson index through use of areceiver operating curve (ROC).Results:A total of 352,535 patientsundergoing 369,454 spine procedures fordegenerative disease were gathered.Hypertension and hyperlipidemia were themost common comorbidities. Cervical
procedures resulted in 8,286complications (4.50%) whilethoracolumbar procedures produced25,118 complications (13.55%).Increasing CMS correlated linearly withincreasing complication incidence (OR1.11, 95% CI 1.10-1.13, P < 0.0001).Logistic regression revealed thatneurological deficit, cardiac conditions,and drug or alcohol use had greatestassociation with complication occurrence.The Charlson index also correlated withcomplication occurrence in both cervical(OR 1.25, 95% CI 1.23-1.27) andthoracolumbar (1.11, 95% CI 1.10-1.12)patient groups. ROC analysis allowed acomparison of accuracy of the indices bycomparing predictive values. The CMSperformed as well as the Charlson indexin predicting complication occurrence inboth cervical and thoracic spine patients.Conclusion: ICD-9 based modelingvalidated that CMS correlates withcomplication occurrence. The CMSperformed as well as the Charlson indexin predicting risk of complication in spinepatients.
381Stable Anteroposterior Diameter ofthe Spinal Canal on Follow-up CTScans After Open Door LaminoplastyBen Z. Roitberg, Melissa StamatesIntroduction: Re-closure of open doorlaminoplasty is a common concern,prompting development of devices to keepthe spinal canal expanded. Addinghardware may add to the cost, time andrisk of the procedure. There is littlequantitative information availableregarding canal diameter stability in opendoor laminoplasty without addinghardware.Methods: This is a retrospective analysisof prospective data from our spineoutcome database. Our open doorlaminoplasty uses two autograft supports,at C4 and C6. Patients have postoperativeCT scans within 48 hours, and then at ± 6months. A researcher who is not part ofthe treatment team measured the A-Pdiameter at each vertebral level at theimmediate post op baseline and at followup.Results: Required imaging was availablein 14 consecutive patients who had a C3-7open door laminoplasty for cervicalmyelopathy, 9 male, 5 female, ages 46-86.Immediate postoperative AP diameter was17.4 (± 0.5)mm at C3, 19.4 ± 0.7 mm atC4, 19.4 ± 0.6 mm at C5, 20.1 ± 0.6 mmat C6, and 20.4 ± 0.5 mm at C7. The 6
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 91
DIGITAL POSTER ABSTRACTS
months follow up demonstrated bonyfusion in all cases. At that time the canaldiameter was 17.4 ± 0.5 mm at C3, 19.6 ±0.6 at C4, 19.7 ±- 0.5 at C5, 20.3 ± 0.6 atC6, and 20.9 ± 0.5 at C7. (NS at all levelsbetween the two time points). There wereno cases of re-closure or any narrowing ofthe canal.Conclusion: Canal diameter wasmaintained both at levels directlysupported by a graft (C4 and C6) andthose not supported (C3, C5, C7). At 6months there was bony fusion and no re-closure of the canal in open doorlaminoplasty with two autografts only andwithout hardware. Fusion occurred in allcases at the time of last CT scan, at thegraft and at the hinge.
382Resistive Capacity of the HumanCervical Spinal Column in CoronalBendingChristopher E. Wolfla, Narayan Yoganandan, John R. Humm,Dennis J. Maiman, Frank A. PintarIntroduction:While studies exist on theclinical biomechanics of the spine underlow magnitude static or quasi-static puremoments, physiologic activities andtraumatic events often induce loads athigher magnitudes and rates. Theobjective of this study is to determine theinjury threshold of the human cervicalcolumn to coronal bending moments atthese higher loading magnitudes and rates.Methods: Data was obtained from testsusing ten human cadavers: eight weretested as intact subjects in sled equipmentat velocities up to 65 km/h, two weresubjected to pure coronal moments usingan electrohydraulic testing device at ratesup to 51.5 rad/s. The head was included inall specimens, allowing the cervicalcolumn to sustain eccentric flexion-compression loading from the preloadedhead mass. Multiaxial accelerometerswere placed on the head to obtain cranialkinematics from which forces andmoments were determined at the occipitalcondyles. The presence of injury wasdetermined by palpation, radiographs,computed tomography, and/or detaileddissection.Results: Sled tests resulted in injuries tothe axis and lower cervical spineassociated with tension and bendingmechanisms. Peak moments up to 62 Nmwere associated with axial tensile forcesup to 2300 N, indicating a complex,combined loading pattern. In contrast,tests using electrohydraulic device
induced pure coronal moments withouttensile forces. At coronal moments of upto 75 Nm, injury to the cervical spine didnot occur.Conclusion: These results indicate that thecervical spine is more susceptible to injuryunder combined loading than under puremoment loading. These results suggestthat the level of pure moment loading (lessthan 10 Nm) often selected in theevaluation of clinical stability of thecervical spine is too low to exercise thecolumn at magnitudes representative ofmany real world activities includingtraumatic loading.
383Outcome and Complications ofAnterior Cervical Discetomy andFusion(ACDF) in Elderly Population: ASingle Surgeon ExperienceAshish Sonig, Imad S. Khan, Jai D. Thakur,Papireddy Bollam, Anil NandaIntroduction: Elderly patients havemultiple co-morbidities and are at theterminal stage of natural history ofdegenerative spine disease. Higherincidence of multiple level disease andprior neck surgeries makes them evenmore vulnerable. Our aim was to analyzethe outcome and complications in suchpatients.Methods:We retrospectively reviewed themedical records of all elderly patients(>65yrs) operated by the senior author. Atotal of 67 consecutive patients underwentACDF for 100 levels from January 1998-December 2010. Nuricks-grade was usedfor outcome analysis and Comorbiditywas assessed by Kaplan-Feinstein index.Data was analyzed using chi square/fisher-exact test and binary logistic regression.Results: The mean age was 70.6 years andF:M ratio was 1.6:1. Mean duration ofsymptoms was 12.2 months, mostcommon presentation was Nuricks-Grade0 (44.8%). KFI was >1 in 28.4% patients,these patients had a significantly longerduration of hospital stay (P = 0.01). C5-6was the most common single level fusionperformed (23.9%, n = 16) and C5-7 wasthe most common multi-level fusion(16.4%, n = 11). Un-instrumented spinefusion was done in 6% cases. Overallcomplications were seen in 13.4%patients, and the most common wasdysphagia (5%). None had root/cordinjury or epidural-hematoma/graftextrusion. Multi-level fusions and re-surgeries were not associated with highercomplication rate. Mean follow-up was10.6 months. Radiological fusion was
achieved in 55 (82.1%) patients and noinstability was detected. There was nostatistical difference in fusion rates on thebasis of gender and level of surgery. 72%patients improved or becameasymptomatic after surgery. Patients withsingle level fusion had statistically betteroutcome compared to multiple fusion (P= 0.04).Conclusion:A high percentage (82.1%) offusion can be achieved in multi/singlelevel surgeries, with overall good-outcome(72%) and minimal complications.Multi-level fusion and increased comorbidityadds to the poor-outcome (P = 0.04) andlonger hospital-stay (P =0.01), thesefactors should always be considered whiledeciding ACDF in the elderly population.
385Six Month Outcomes of iO-FlexSystem Assisted Decompression vs.Traditional Minimally InvasiveDecompression in the Treatment ofLumbar Spinal StenosisRobert E. Isaacs, Scott Tyler BrigemanIntroduction:Although the results ofdecompression from spinal stenosis fromthe SPORT trial were exemplary, concernfor suboptimal long-term results ofstandard decompression techniques hasbeen raised in several studies. From asurgeon’s perspective, there is a potentialtradeoff between inadequatedecompression and iatrogenic instability.The iO-Flex device has been touted as away to potentially decompress under thefacet and through the neural foramenwhile limiting the risk for delayedinstability. Our goal was to examinepatients undergoing decompressionassisted with the Baxano device vs. thoseundergoing traditional MISdecompression.Methods:All patients undergoing lumbardecompression between January 2010 andMarch 2011 were included to ensure theavailability of 6 month data. The Baxanodevice was used if available. Patients weregrouped by surgical technique (Baxanovs. MIS decompression). VAS leg andback pain scores were studied 6 weeksand 6 months postoperatively whenavailable.Results: 10 patients were treated with theBaxano device and 11 patients receivedtraditional MIS decompressions. Thegroups were similar in age (71.5Baxano/74.1 control, P = 0.39), male tofemale ratio (7:3/8:3, P = 0.89), andnumber of levels treated (2.1/1.8, P =0.58), with L4-L5 being the primary level
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES92
DIGITAL POSTER ABSTRACTS

treated. All but 1 patient in each groupreached SCB in leg or back pain 6 weekspostoperatively. At 6 months, though, 89%of those treated with the iO-Flex devicereached SCB in leg pain, compared to60% of those treated with traditional MISdecompressions (P = 0.04). Further,100% of Baxano patients reached SCB inback pain, compared to 80% of the controlgroup (P = 0.08).Conclusion: This small matched cohortshows a greater tendency for improvementin leg and back pain in patients receivinglumbar decompression using the iO-Flexdevice compared to those receiving MISdecompression alone. Patients undergoingdecompression alone showed positiveoutcomes at 6 weeks but deterioratedsome by 6 months. Differences in thenumber of patients reaching leg SCBbetween the groups were statisticallysignificant, those for back SCB showedstrong trends. Larger controlled studiesare needed to determine if this observationcontinues.
386Instrumentation FollowingDecompression for SpinalMetastasesPhilippe A. Mercier, W. Bradley JacobsIntroduction: Decompression andinstrumentation has proven beneficial tothe neurological outcome and quality oflife for selected patients with spinalmetastases. Due to the limited expectedsurvival of this population and the lack ofsuitable local bone graft many physiciansrely on the instrumentation alone tostabilize the vertebral column.Methods:We conducted a retrospectivechart review of patients that hadundergone decompression andinstrumentation for spinal metastateses ina multisurgeon spine practice to measurethe rate of instrumentation failure.Results: Thirty-three patients wereidentified who had surgery within the last4 years. No reports of instrument failurewere identified in the patients in thisseries. Four patients had secondprocedures during which infiltrated bonewas decompressed a second time or newsites of metastases were decompressedand/or instrumented. As expected bonegraft was used in only 12% of patientswhile instrumentation was augmentedwith methylmethacrylate or bone graftsubstitute in 61% while the remainder didnot use any bone graft substitute.Conclusion: This small study suggests thatfailure of spinal instrumentation in
patients with spinal metastases is anuncommon occurrence despite the lack ofbone graft in the constructs use to stabilizethe vertebral column.
387Minimally Disruptive LateralInterbody Fusion in the Treatment ofDegenerative Spondylolisthesis: AProspective Evaluation of Mid-termClinical OutcomesKaveh Khajavi, Alessandria Y. Shen,Anthony HutchisonIntroduction: Over the past decade, non-endoscopic minimally disruptiveapproaches for lumbar interbody fusion(IBF) have gained popularity due tomodern specialized accessinstrumentation and implants which fulfillthe goals of conventional surgery withoutthe associated morbidity. The aim of thisreport is to examine mid-term clinicaloutcomes following a minimallydisruptive, 90° lateral, transpsoasapproach for IBF in degenerativespondylolisthesis patients.Methods: 61 consecutive patients treatedwith extreme lateral interbody fusion(XLIF) for Grade I or II degenerativespondylolisthesis were followed in anIRB-approved, prospective registry(ProSTOS, PhDx) at a single institution inAtlanta, GA. Mean patient age was 67years, 75% were female and 31% hadundergone a previous lumbar surgery. Intotal, 73 levels were treated with 49 (80%)single-level and 12 (20%) 2-level cases.Supplemental fixation was used in 57(93%) cases and 26 (43%) patientsunderwent a direct posteriordecompression. In all cases, rhBMP-2 wasused. Low back (LBP) and leg pain (LP),disability, and quality of life (QOL) weremeasured using VAS, ODI and SF-36(PCS & MCS).Results:Average follow-up was 12.1months. Average ORT, EBL, and LOSwere 205 minutes, 82cc, and 1.31 days,respectively. Complications occurred inthree (5%) patients: one MI, onesuperficial infection in posteriorinstrumentation, and one urinaryretention. Transient approach-relatedthigh/groin was observed in six (10%)cases, all resolving by 3 monthspostoperative. At one year, LBP and LPimproved 78% (8.0 to 1.8) and 70% (7.6to 2.3), respectively (P < 0.001), ODIdecreased 48% from 42% to 23% (P <0.001), SF-36 PCS and MCS improved38% (31.2 to 42.9, P < 0.001) and 21%(43.1 to 52.1, P = 0.003), respectively.
There were no cases of pseudoarthrosis.Conclusion:MIS lateral IBF resulted in ahastened postoperative recovery with alow complication rate and high clinicalefficacy on pain, disability and QOLmeasures, compared to conventionalapproaches.
388The Effect of the Minimally InvasiveLateral Retroperitoneal TranspsoasLumbar Interbody Fusion onSegmental and Regional LumbarLordosisTien Viet Le, Andrew C. Vivas, Elias Dakwar, Ali A. Baaj, Juan S. UribeIntroduction:Minimally invasive spinesurgery is increasingly used to treatmultiple spine pathologies. The minimallyinvasive lateral interbody fusion (MISLIF) via retroperitoneal transpsoasapproach in the lumbar spine can correctcoronal Cobb angles, but the effect onsagittal plane correction is unclear. Ourobjective is to study the effect of MIS LIFon the restoration of segmental andregional lumbar lordosis in patients withdegenerative spine disease.Methods: Thirty-five patients with lumbardegenerative disease who underwent MISLIF without supplemental posteriorinstrumentation using 10° lordoticinterbody cages were studied. The mostrecent postoperative radiograph wascompared to the preoperative radiographfor comparison. Segmental and regionalCobb angles were measured to determinelordosis. Mean disc height changes werealso measured.Results: The mean follow-up period was13.3 months. Fifty total levels were fusedwith a mean of 1.42 levels fused perpatient. Mean segmental Cobb angleincreased from 11.10° to 13.61° (P <0.001), or 22.6%. L2-3 had the greatestproportional increase in segmentallordosis. Mean regional Cobb angleincreased from 52.47° to 53.45° (P =0.392). Mean disc height increased from6.50 mm to 10.04 mm (P < 0.001), or54.5%. There was also a significantincrease at each individual segment.Conclusion:Minimally invasive LIFsignificantly improves segmental lordosisand disc height in the lumbar spine, butnot regional lumbar lordosis. Anteriorlongitudinal ligament sectioning and/orthe addition of a more lordotic implantmay be necessary in cases wheresignificant increases in regional lumbarlordosis is desired.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 93
DIGITAL POSTER ABSTRACTS

389Adult Neural Stem/Progenitor CellResponse to Differentiation FactorsIs Affected by Cell Origin: Impact onTherapeutic ApplicationEve C. Tsai, Matthew Coyle, Ushananthini Shanmugalingam, Harrison Westwick, May Griffith, Xudong CaoIntroduction:Many therapeutic modelshave utilized stem/progenitor cells(NSPCs) from various regions of the bodyfor brain and spinal cord injury repair. Totranslate these models to clinicalapplication, it is essential to determine ifthe controls for the differentiation ofNSPCs are affected by the origin of theNSPCs.Methods:We evaluated adult spinal cord(SC) and subventricular zone (SVZ)NSPC differentiation into neurons,oligodendrocytes and astrocytes withretinoic acid (RA), platelet derived growthfactor (PDGF) and bone morphogenicprotein 4 (BMP-4), respectively. Afterproliferation in culture for seven days,primary neurospheres were plated inconcentrations of RA, PDGF and BMP-4ranging from 0-500 ng/ml. Seven dayspost factor exposure NSPCs were fixedand stained for O4, glial fribrillary acidicprotein (GFAP), ß-III-tubulin (ßIIIT),brain lipid binding protein (BLBP),Nestin, BrdU (pulsed 24hr beforefixation), TUNEL and Hoechst.Percentage of positive cell staining out ofthe total number of cells plated at allconcentrations were obtained andcompared (ANOVA, Tukey’s post hoctest) to control (differentiating factorabsent) conditions.Results: While ßIIIT positive SVZ NSPCsincreased with RA concentrations greaterthan 125ng/ml (P < 0.001), there was noincrease with SC NSPCs. However, withRA concentrations =250 ng/ml anincrease in the proportion of BLBPpositive cells was seen in both SVZ andSC cells compared to control (P < 0.01).Although PDGF increased the number ofO4 positive SVZ NSPCs when it was=500 ng/ml (P < 0.01), PDGF did notincrease the number of O4 positive SCNSPCs. With PDGF concentrations =250ng/ml, there was an increase in thenumber of BrdU positive SVZ NSPCs (P< 0.001). While an increase in theproportion of GFAP positive SVZ NSPCswas seen with BMP-4 concentrations =250 ng/ml (P < 0.001). BMP-4 atconcentrations = 125 ng/ml reduced thenumber of GFAP positive SC NSPCs
(P < 0.001).Conclusion:As factors that inducedifferentiation for SVZ NSPCs may notproduce the same result with SC derivedNSPCs, further work in identifying theappropriate differentiation cues will berequired prior to appropriate therapeuticapplication of NSPCs.
390The Naso-Axial Line: A New Methodof Accurately Predicting the InferiorLimit of the Endoscopic EndonasalApproach to the CraniocervicalJunctionPhilipp R. Aldana, Emanuele La CorteIntroduction: Endoscopic approaches toanterior pathology of the craniocervicaljunction (CVJ) have arisen as alternativesto open approaches. Understanding andpredicting the limits to the endoscopicapproach to CVJ is important in surgicalplanning. The endoscopic endonasalapproach (EEA) is commonly used thuswe sought to develop a method thataccurately predicts the inferior limit ofthis to the CVJ. The method developedwas compared to methods currently usedto predict the same.Methods: Nine fresh-frozen adult cadaverheads were used for anatomicaldissection. Preoperative and postoperativevolumetric computerized tomographicscans were performed to compare thenaso-axial line (NAL) vs. naso-palatine(NPL, or Kassam, line) used to predict theinferior limit of the EEA to the actualextent of surgical dissection.Results:The mean differences between theNAL and the actual inferior surgicalexposure of EEA at C2 cortex (anteriorand posterior) were both 0.3mm.Anatomically, the actual inferior surgicallimit ranged from the dens to the upperhalf of the C2 body, which matched thatpredicted by the NAL. The NPL predictedan inferior EEA limit much lower rangethan the actual - from the lower half of theC2 body to the superior endplate of C3.Using the least-square means (LSM)method to estimate the deviation frompost-surgical measurements, we found nodifference between the NAL and the actualinferior surgical limit (LSM 0, P = 1.0). Incontrast, the NPL predicted a significantlylower EEA limit than the actual surgicallimit (LSM 13.3, P < 0.001).Conclusion: The naso-axial line accuratelypredicts the inferior limit of the EEA,which ranges from the dens to the upperhalf of C2. This new method can be usedin presurgical planning to assess the
suitability of the EEA to craniovertebraljunction pathology.
391Sacroiliac Arthrodesis by MinimalIncision Method: One-Year OutcomesJohn G. Stark, Chris IdemmiliIntroduction: Though fusion has beenadvocated for SIJ pain and disease, noprocedure has received generalacceptance. The purpose of this study is toreport technical outcomes, and short-termfunctional outcomes of patients followingsacroiliac arthrodesis surgery using adistraction-interference technique.Methods: Fifteen patients, severelysymptomatic with SIJ pain, underwent SIJarthrodesis using a combined extra- andpartial intraarticular technique featuring aposterior-midline incision, controlleddistraction/measurement of theextraarticular recess, BMP-2/allograftingof adjacent surfaces, and application of aninterference-fit threaded implant. Patientsample consisted of 4 males and 11females. Mean age was 43 (range 22-65).The Oswestry Disability Index (ODI) andMillion Visual Analog Scale (MVAS)were the primary functional outcomemeasures. Patient self-report ofimprovement, satisfaction, and percentresolution of back and leg pain werecollected.Results: Blood loss averaged 55cc (range10-300cc). Mean hospital stay was 2.2days. Average patient function improvedsignificantly. MVAS scores improved 45.6points (95% confidence interval 30.8 to60.8 points, 43% improvement, P <.0001). ODI scores improved 20 points(95% confidence interval 8.2 to 31.8points, 36% improvement, P < .0001).Patients reported 78% resolution of backpain (95% Confidence interval: 66%-90%) and 86% resolution of leg pain(95% Confidence interval: 77%-96%).Conclusion: Judged by back and leg painrelief, the surgery is promising in allpatients. The SIJ region can be grafted andimplanted by minimal incision methods.Patient satisfaction is high. There were nonerve injuries, displacements, infections,or malpositioned implants. Most patientsshowed significant improvement by threemonths.
392Percutaneous Pedicle Screw Fixationfor Thoracolumbar FracturesNader S. Dahdaleh, Brian J. Dlouhy,Patrick W. HitchonIntroduction: Percutaneous surgery has
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES94
DIGITAL POSTER ABSTRACTS

been gaining popularity in the past 2decades due to its advantages of lessmuscle dissection, faster recovery and lesscomplication rates. In parallel to itsapplication to degenerative spine disease itis also a treatment option forthoracolumbar fractures. We present ourexperience with percutaneous pediclescrew fixation (PPDF) in the treatment ofa variety of thoracolumbar fractures.Methods: This is retrospective study on 13patients who suffered a variety ofthoracolumbar fractures and were treatedwith PPSF at our institution betweenJanuary of 2009 and June 2011. Theirelectronic charts and spine imaging werereviewed. Our indications forpercutaneous fixation for unstable spinefractures include absence of spinal cordcompression, absence of an irreducibledislocation, and a Load sharing score of<6 obviating the need for anterior columnreconstruction.Results: The average age of the group was48.9 years. All but 2 were males. All but 3patients were neurologically normal. 4(30.8%) fractures were thoracic, 7(53.8%) thoracolumbar (T11-L2), and 2(15.4%) were lumbar. Types of fracturewere: 5 (38.5%) flexion distraction, 4(30.8%) burst, 2 (15.4%) extensiondistraction, 1 (7.7%) fracture dislocation,and 1 (7.7%) compression fracture (Figure1). The average follow up was 5.15months. One patient without deficitrequired screw revision for pedicleviolation. All were pain free orcomplained of minimal pain on their lastfollow-up. All fractures were stable ondynamic imaging on the last follow-up.Examples are included in figures 2, and 3.Conclusion: Percutaneous pedicle screwfixation is a treatment option in selectpatients with thoracolumbar spinefractures. The varieties of fractures thatcan be treated encompass flexion andextension distraction injuries, burstfractures, and compression fractures.
393S1-L5 Pedicle Transvertebral FixationRevisitedDavid A. Stidd, Jack H. DunnIntroduction: The surgical goals forsymptomatic moderate- to high-gradelumbosacral spondylolisthesisunresponsive to conservative treatment arearthrodesis, restoration of sagittal balance,and symptom relief. These goals areachieved by multiple surgical techniquesincluding posterior interlaminar fusion,posterolateral fusion, anterior interbody
fusion from a variety of approaches, and acombined circumferential fusion. Pedicletransvertebral screw fixation was firstdescribed in 1994. We present a literaturereview of L5-S1 pedicle transvertebralscrew fixation for spondylolisthesis and acase report.Methods: Case report and literaturereview.Results: Pedicle transvertebral screwfixation was first described in 1994 as asafe, effective method to stabilize thelumbosacral spine with moderate- to high-grade spondylolisthesis (1). Thistechnique establishes a 3-column fixationfrom a single posterior approach withoutplacement of an interbody cage.Transvertebral pedicle screws havemultiple cortical purchases improvingpullout strength and the anteromedialtrajectory of the screws increases fixationstrength by distributing forces over alarger mass of bone rather than the boneonly purchased the screw threads (1). Thefixation strength of pedicle transvertebralscrew fixation of the lumbosacral junctionwas found to be equivalent to a combinedinterbody-pedicle screw fusion andsuperior to traditional pedicle screwfixation alone in a biomechanic analysisof cadaver models(2). Outcomes oftransvertebral fixation were also found tobe equivalent to fixation with TLIFcombined with posterior fixation (3). Atour institution, a 64 year old male with aGrade II isthmic L5-S1 spondylolisthesisthat failed conservative management wastreated with an in situ L3-S1 posteriorpedicle fusion using an L5-S1transvertebral screw. The patient toleratedthe procedure well and his pain issignificantly decreased.Conclusion: Pedicle transvertebral screwfixation is a safe and effective means ofstabilizing moderate- to high-gradespondylolisthesis, minimizingcomplications associated with othertechniques.
395Use of Expandable Interbody Deviceto Restore Disc Height in MinimallyInvasive Spine Fusion SurgeryMick J. Perez-Cruet, Namath Syed Hussain,Joseph John Joshua, Evan BegunIntroduction: Degenerative disc disease isa common, progressive disease processthat leads to disc height loss thatcontributes to foraminal height loss andvarious foraminal impingement painsyndromes. The efficacy of minimallyinvasive spine fusion methods in
improving disc height and reducingsubluxation and its effect on Health-related Quality of Life (HRQL) measureshas not been well studied. The interbodydevice Staxx which is inserted at a heightof 7mm and can expand to 15mm wasevaluated.Methods: 46 consecutive patientsunderwent minimally invasivetransforminal lumbar interbody fusion(MITLIF) between December 2009 andAugust 2011 using the Staxx expandableinterbody device. Preoperative andpostoperative morphometric data(intervertebral height, foraminal height,and degree of subluxation) was collectedbased on plain radiographs. A validatedfull set of Health-related Quality of Life(HRQL) Measures, including VisualAnalog Scale (VAS), Oswestry DisabilityIndex (ODI), and SF-36 were alsocollected preoperatively andpostoperatively.Results: Preoperative disc height increasedfrom 6.7mm (range 2.5 – 12.8mm, SD =2.3mm) to 10.9mm postoperatively (range8.3 – 15mm, SD = 1.6mm, P value <.05).Preoperative foraminal height increasedfrom 20.0mm (range 14.5 – 26.8mm, SD= 4.4mm) to 24.1mm postoperatively(range 15.5 – 32.3mm, SD = 4.6mm, Pvalue <.05). Preoperative subluxationdecreased from 9.9mm (range 4.5 –24.7mm, SD = 5.8mm) down to 4.6mmpostoperatively (range 0 – 7.2mm, SD =2.6mm, P value <.05). Successful fusionwas achieved in >95% of patients basedon postoperative dynamic radiographs at 3month interval. No neurologicalcomplication occurred. Noelectromyographic (EMG) activity wasnoted with implant insertion and discheight restoration. Statistically significantimprovements in VAS, ODI, and SF-36scores were reported starting at 6 weekspost-operatively.Conclusion:MITLIF provides adequatedisc height and foraminal heightrestoration using the Staxx device with aconcomitant reduction of spondylolsithesis.This study validates that this MITLIFapproach improves morphometricparameters that can be correlated withimproved clinical outcomes.
396Sciatic Nerve Palsy Secondary toCompression by HeterotopicOssificationSun Ik Lee, Ilias Nicholas Caralopoulos,John Kimball, Olawale SulaimanIntroduction:We present a patient who
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 95
DIGITAL POSTER ABSTRACTS

developed sciatic nerve palsy fromheterotopic ossification after surgicallyrepaired pelvic fracture and treatmentcourse.Methods:A 35-year-old veteran male whowas hit by a garbage truck and sustained apelvic fracture for which he underwentopen reduction and internal fixation in thesame year and a revision next year. Overthe course of 6 years, he developed rightfoot drop. His preoperative workup whichincluded MRI of lumbar region werenegative. On the EMG/NCS study, it wasdemonstrated that the patient has the rightsciatic neuropathy affecting the peronealdivision above the knee. On the clinicalexam, the motor strength of his rightlower extremity was 5/5 except ankledorsiflexion 3/5, plantar flexion 5/5,eversion 3/5 and inversion 4/5. He alsohad diminished sensation in superficial,deep peroneal nerve distribution and somereduced sensation in the tibial nervedistribution.Results: He underwent exploration of thesciatic nerve from buttock level to upperthigh and heterotopic bone formationcompressing the sciatic nerve wasdecompressed. After the surgery, patient’sneurologic status was unchanged, but hadimmediate improvement in his radicularright leg pain. He underwent localradiation therapy of 7.5 Gy and started onindomethacin treatment.Conclusion: Sciatic nerve entrapment dueto heterotopic osseous formation are rare.Patients with sciatic/peroneal neuropathywith a distant history of trauma/orthopedicsurgery in the adjacent bones need to beinvestigated carefully with proper work-up especially when there is a negativespine MRI or even minor degree of spinepathology demonstrated on MRI that areunlikely to be an etiology of patients’signs and symptoms. There has not beenan established treatment course for thispathology. Post-operative radiationtreatment for prevention of heterotopicossification has been reported withfavorable outcome and could be consideredas an option when it is appropriate.
397Outcome After DecompressionSurgery for the Treatment of ChiariType I MalformationMark Mahan, Samuel Kalb, Luis Perez-Orribo, Ruth E. Bristol,Nicholas TheodoreIntroduction: Decompression of Chiari Imalformations is one of the morecontroversial procedures in neurosurgery.
There is a wide spectrum of symptomsand radiographic findings at presentation,making the decision to proceed withintervention, at times controversial.Similarly, the surgical procedure itself canbe performed in a variety of ways. Ourgoal was to evaluate the outcomes withrespect to symptomatology from a largegroup of surgeons who use diversesurgical techniques.Methods:104 patients who underwentdecompression surgery for the treatment ofsymptomatic Chiari I malformation werereviewed. Factors predicting symptomaticoutcome including clinical presentation,surgical procedure performed, presence orabsence of syringomyelia, previousmedical conditions, and the use ofpostoperative steroid or muscle relaxantsmedications were assessed. Mean follow-up was 10 months.Results: Symptomatic improvement wasevident in the majority of the cases.Patients who initially presented withsyringomyelia showed fewer symptomaticimprovements, however, symptomaticworsening was not associated with thepresence of syrinx. Durotomy wasperformed in 97.1%, arachnoid opening in60.6% with visualization of the fourthventricle in 51.9 % of the patients. Neitherarachnoid opening nor fourth ventriclevisualization affected symptomaticoutcome. Duroplasty was performed in94.2% of the cases, and Chiari plate wasused in 13.4% cases resulting in favorablesymptomatic outcome. The use of post-operative steroid or muscle relaxantmedications did not change the course ofsymptom outcome. Follow-up MRI ofpatients who initially presented withsyringomyelia showed a 62.5%improvement rate.Conclusion: Bony decompression isprobably the most important aspect ofChiari I surgery. Whether or notsyringomyelia responds better to openingof the outlet of the fourth ventricle willrequire a larger study population. Evenwith the variety of surgical techniques in alarge group of surgeons, symptomaticimprovement can be achieved in themajority of patients.
398Occipitocervical Fusion Surgery: ASingle Institution Single SurgeonExperienceMark Mahan, Samuel Kalb, Juan Christian Ribas Nijkerk, Nikolay L. Martirosyan, Nicholas TheodoreIntroduction: The craniovertebral junction
(CVJ) constitutes the most mobile portionof the spinal axis. The complexanatomical properties and kinematicrelationships at this site make it difficult toachieve proper surgical fusion. This studyevaluates outcomes between differentsurgical techniques used foroccipitocervical (OC) fusion.Methods: 70 patients who underwent OCfusion by a single surgeon were reviewed.Surgical outcomes were evaluated usingthe modified Japanese OrthopaedicAssociation scale (mJOA) andpostoperative recovery rate.Results: Indications for surgery includedcongenital malformations, degenerativedisease, rheumatoid arthritis, trauma,infection and tumor. Fusion was mostlyperformed at O-C2, O-C3, and O-C4 .Autograft was installed using rib (50%) oriliac crest (27%). Additional cases werefused using fibular allograft. At follow up,the rate of successful fusion was 97%.Overall complication rates was 12.9 %,2.9 % of which occurred intraoperativelyand 10% during follow up. Patients withcomplications were younger (P = 0.008),predominantly males (P = 0.039) andwith hypertension (P = 0.033). Follow-upcomplications were associated with theindication of surgery, where congenitalmalformations, degenerative disease, andinfection were associated with theincidence of complications (P = <0.001).Also, the higher the number of fusedlevels the higher the complication rate (P= <0.001). Clinical outcomes improvedfrom 14.19 (preoperative) to 16.5(postoperative) with a recovery rate of43%. Postoperative improvement wasassociated with the number of levelsfused, where shorter constructs showedbetter outcomes compared to longerfusions (P = <0.001).Conclusion: CVJ pathology requiringsurgical treatment remains challenging,with an elevated rate of complicationscompare to fusion in other regions of thespine. Many of the problems that lead tothe initial deformity are often the sourceof complications and have to beconsidered in advanced surgical planning.Shorter fusion constructs appear to bebetter tolerated long-term, but may beessential for multiple disease levels orpolysegmental instability.
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES96
DIGITAL POSTER ABSTRACTS

399Analysis of Cervical SagittalAlignment Following Lateral MassScrew-Rod FixationRobert F. Heary, Osamah J. Choudhry,Devesh Jalan, Nitin AgarwalIntroduction: The use of posteriorinstrumentation constructs is wellestablished for performing subaxial cervicalstabilizations/fusions. The importance ofglobal and regional sagittal balance hasbecome increasingly recognized. Usingpreoperative and postoperative imaging,long-term analysis was performed todetermine the effect of posteriorinstrumentation on postoperative cervicalsagittal alignment at long-term follow-up.Methods: Over a period of 6 years, 64consecutive patients (45 males and 19females, mean age- 47 years) underwentcervical lateral mass screw-rod fixation.Plain radiographs, CT scans, and MRimages were analyzed preoperatively toassess sagittal balance (C2-C7).Postoperatively, CT scans and serialradiographs were obtained in all patients.Using two independent observers,changes in sagittal balance weredetermined by comparing the preoperativeand postoperative imaging studies. Aminimum of 6 months follow-up wasobtained in all patients.Results: In total, 455 screws were placedin the cervical spines of 64 patients.Definitive radiographic fusion wasdetected in all 64 (100%) patients. Therewere no incidences of instrumentationfailures or lucencies surrounding anyscrews. The mean preoperative Cobbangle in all patients was -6.2° ± 1.9°. Themean postoperative sagittal angle on latefollow-up imaging was -8.3° ± 1.9°.Patients with preoperative kyphosis (N =23, mean +10.3º) significantly improved(P = .003) their sagittal alignment by 7.7º(to a mean value of +2.6º) while patientswith preoperative lordosis (N = 41, mean -15.4º) maintained their lordosis (to a meanvalue of -14.9º). There were noneuroforaminal, 3 foramen transversarium,and 9 facet joint violations. Mean durationof follow-up was 36.2 months.Conclusion: Radiographic analysis showedlateral mass fixation to be safe andeffective. Certain operative techniquesallowed for substantial deformitycorrection, fusion in all patients, andmaintenance of long-term correction ofdeformity. Lateral mass screw-rod fixationis an effective method for maintaininglordotic cervical alignment and forsignificantly correcting kyphotic deformity.
400Multifactorial Lumbar StenosisTreated Successfully with PrimaryFactor Treatment OnlyDavid A. Ditsworth, Luis LombardiIntroduction:Multifactorial spinalstenosis, whether central, lateral orforaminal, affects millions of Americans.The clinical presentation ranges fromasymptomatic (radiological finding) toneurological claudication and radicularpain. After exhausting conservativemethods of treatment, most surgicalsolutions entail generous bone, ligamentflavum, articular facet and disc removal.This in turn could generate, in a highpercentage of cases, spinal instabilitywhich leads to fusion and possibly tofailed back surgery syndrome. The presentabstract deals with the treatment ofmultifactorial spinal stenosis by treatingone of the factors, the disc, with a focusedlumbar discectomy.Methods: 27 cases were obtained from aretrospective chart review from 2009 up todate. We included cases of patients olderthan 50 years of age with multifactorialspinal stenosis diagnosed by MRI and CTscan, interpreted by independentradiologists. All patients underwent CTscan after discography and were treatedwith a focused lumbar discectomy. Agesranged from 50 to 86, 41% females and59% males. 70 % of patients presentedwith a combination of central, recess andforaminal stenosis, 78% with radicularsymptoms, 11% with lumbago and 11 %with neurological claudication, the latterin combination with radicular presentation.Average follow up was 8 weeks.Results: Utilizing the MacNabb criteria theresults were as follows: 41 % (n = 11)excellent, 52% (n = 14) good and 7% (n =2) Fair with a success rate of 93%. Nocomplications were reported.Conclusion: The treatment of multifactorialspinal stenosis with solely a primaryfactor approach lumbar discectomy is veryeffective and safe. At the same time itdoes not preclude the use of other moreinvasive surgical options should thisapproach be insufficient.
401Analysis of Injury Input Parametersin a Feline Model of Spinal CordInjuryJoseph Battocletti, Christy Stadig, Dennis J. Maiman, Frank A. PintarIntroduction: To evaluate certaintherapeutic effects for Spinal Cord Injury(SCI) researchers have begun with rodent
models. There are very few higher orderspecies models of SCI due to the complexnature of the biological response and thedifficulty in post-injury care. Ourlaboratory has developed a feline model ofSCI that uses a dorsal impact contusionmethod. The purpose of the presentanalysis was to determine a functionaloutcome scale that correlated to themechanical input to the cord.Methods:A weight-drop apparatus wasconstructed that included a rigidly-mounted accelerometer attached to thefree-falling weight. The accelerometersignal was recorded at 12.5 kHz samplingrate using a digital data acquisitionsystem. A laminectomy at the T5-T6levels was done to expose the dorsal cord.The 25-gm weight was dropped onto theexposed cord and the accelerationrecorded. From the accelerometer signalimpact velocity, cord deformation, cordstress and strain, and impact force werecomputed. From the integration of theforce-time trace, force impulse wascomputed. Animals were survived for upto 12 weeks depending on therapeutics. A20-point hindlimb functional ambulationscore similar to the BBB score in rodentswas used to assess outcome. Assessmentswere made at 3-days and 10-days postinjury and equal intervals until sacrifice.The spinal cords were harvested forhistology.Results: Peak acceleration, peak stress,peak strain, and cord deformation, wereweakly correlated (R-squared < 0.2) tofunctional outcome score. The strongestcorrelation with functional outcome scorewas Force Impulse (R-squared = 0.4). Theuniformity of the acceleration signal was asignificant indicator of test-to-testuniformity.Conclusion:A feline model of SCI wasdeveloped to evaluate therapeutic methodsincluding pulsed magnetic fields and stemcell transplant. A functional ambulationscore was developed to assess therapeuticeffectiveness with impulse forcecalculation to assess input.
402Correlation of Foraminal Area andResponse to Cervical Nerve RootInjectionsWilson Zachary Ray, Lubdha Shah, Syed Hasan Akbari, Meic H. Schmidt,Andrew T. Dailey, Erica Fay BissonIntroduction: To analyze whether cervicalneuroforaminal area measured onmagnetic resonance imaging (MRI) canbe used to predict immediate therapeutic
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 97
DIGITAL POSTER ABSTRACTS

responses to cervical nerve root injectionsin patients with cervical radiculopathy.Methods:A retrospective chart reviewidentified 100 consecutive patients treatedat a single tertiary referral center. Datacollected included patient demographics,neuroforaminal area of the symptomaticside and contralateral side, Visual AnalogScore pre- and post-injection, history ofprevious cervical surgery, comorbidities,and history of tobacco use.Results: One hundred consecutive patientswith symptoms of cervical radiculopathywere treated with neuroforaminal nerveroot injections were identified. Immediatesymptomatic improvement of post-injection visual analog scores correlatedwith foraminal areas at least one standarddeviation smaller as compared to thecontralateral control side.Conclusion:Measurement ofneuroforaminal areas may represent auseful pre-procedural technique to predictwhich patients with symptoms of cervicalradiculopathy secondary to foraminalstenosis are likely to respond to selectivenerve root injections. Larger prospectivestudies are needed to verify theseretrospective results and make moremeaningful conclusions regarding otherdemographic predictors.
403Thoracic Chance Fractures:Treatment and Outcomes in theLargest Reported SeriesSanjay S. Dhall, Daniel J. HohIntroduction: Chance fractures aretypically reported in the lumbar spine, andthoracic Chance fractures are very rare. Tothe best of our knowledge, this is thelargest reported series of thoracic chancefractures and their management.Methods:A study at three level 1 traumacenters was performed of patients withtraumatic thoracic Chance fractures.Charts were assessed for clinicalpresentation, treatment modalities,admission and post-treatment neurologicstatus, and complications.Results: Twelve patients were identifiedwith thoracic Chance fractures. Seven ofthe patients were ASIA A (completespinal cord injury), one ASIA C, and fourwere ASIA E (intact). Two patients weremanaged with bracing, nine patientsunderwent posterior instrumentedstabilization, and one patient underwentcombined anterior-posterior stabilization.Half of the patients suffered multiplesevere chest injuries, including aorticdissection and flail chest. One patient died
from these injuries. Two patients hadimproved ASIA scores at discharge, andnone of the patients worsenedpostoperatively.Conclusion: Though thoracic chancefractures are a rare injury, they are a highenergy injury resulting in multiple organtrauma as well as spinal injury. Thoughmany of these patients suffer spinal cordinjury, a significant number can remainneurologically intact or even improve afterspinal cord injury.
404Management and Outcome ofInadvertent Durotomies in LumbarSpine Surgeries for DegenerativeConditionsImad S. Khan, Ashish Sonig, Jai D. Thakur,Prashant Chittiboina, Anil NandaIntroduction: Inadvertent durotomies arerelatively common complications inlumbar surgeries for degenerativeconditions. Our aim was to analyze ourinstitutional experience of managementstrategies to deal with these durotomiesintraoperatively and their outcomes.Methods:We retrospectively reviewed allthe patients with documented durotomiesduring surgery. A total of 50 consecutivepatients had inadvertent intra-operativedurotomies in relevant surgeries fromJanuary 2001 to December 2010.Results: The average age of the patientswas 57.1 years with a 1:1 sex ratio. Themost common procedure wasinstrumented lumbar surgery (35%). Thedurotomy was intraoperatively managedwith suture (silk or nylon) and glue (fibrinor polyethylene-glycol-hydrogel) in 21patients, and suture alone in 17 patients.In 8 patients when no definite durotomywas identified, or its location was notamenable to suturing, glue along withmuscle or fat patch was used. All patientsunderwent an intra-operative valsalvaprocedure to ascertain the completeness ofthe repair. Seventy-six percent of all thepatients were mobilized within 24 hoursof the surgery with no issues, and theaverage length of stay was 3.4 days. Themean follow-up period was 13.1 monthsand only 3 patients (6%) had to be re-explored in the follow-up period due topersistence of CSF leak symptoms. All ofthese patients were found to havepseudomeningoceles which were drainedand the dural defect repaired with silksuture and fibrin glue. There were norecurrences on follow-up. We did not findany significant difference betweendifferent management techniques and
outcomes in our patients.Conclusion:Meticulous attention torepairing lumbar durotomies with suturewith or without glue, and confirming withvalsalva maneuver, has excellent results. Ifno definite durotomy is found, or thelocation is not amenable to suturing, fibringlue along with muscle or fat patch can beused with comparable good results.
405Posterior Less InvasiveDecompression and Stabilization forthe Treatment of MalignantNeoplasms of the Thoraco-lumbarSpine: Perioperative Results and Riskof Hardware FailureAvery Lee Buchholz, Vibhor Krishna, Brian Blaker, Steven Morgan, Bruce M. FrankelIntroduction:Metastatic epidural spinalcord compression (MESCC) is adebilitating complication of cancerresulting in motor or sensory deficits andbowel and bladder incontinence. Whilechemotherapy and radiation are theprimary treatment for MESCC, surgery isindicated for intractable pain, impendingmechanical failure or instability, andneurological deficits. Open surgicaltechniques often cause extensivedissection, increased post operative pain,immobility and longer hospitalizations.Advances in technology and refinement oftechniques in minimally invasive spinesurgery (MIS) may provide effectivedecompression and stabilization in theMESCC patient.Methods:We retrospectively reviewed theperioperative results from a series of 19patients with malignant metastatic spinedisease treated with minimally invasivetechniques of posterior decompressionand stabilization by the senior author.These results are compared to aconsecutive series of similar patientsperformed at our institution by opensurgery.Results: Satisfactory decompression andstabilization was achieved in all patientsthorough one of the three techniques:microtubular laminectomy, transpedicularcorpectomy and constotransversecorpectomy. None of the patientsexperienced procedure relatedneurological deterioration and the deficitsimproved in all cases except those withcomplete spinal cord injury. The meanblood loss was 755 mL. The blood loss ina similar the open cohort was 2500 mL.The length of stay in our MIS series was3.5 days as compared with 9.4 days in
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES98
DIGITAL POSTER ABSTRACTS

patients who underwent open surgery.Conclusion: This case series demonstratesthe feasibility of MIS approach fortreatment of MESCC patients.
406Incidence of and Factors Associatedwith Severe Dysphagia FollowingCircumferential Cervical SpineSurgeryDwight Saulle, Kai-Ming G. Fu, Justin S. Smith, Christopher I. ShaffreyIntroduction: The objective of this studywas to evaluate the incidence andpotential influencing factors of severedysphagia after combined anterior-posterior cervical spine surgeries.Methods:Medical records of 30consecutive patients undergoing same-dayanterior-posterior (AP) cervical spinefusions were retrospectively reviewed,including general assessment ofdemographic, radiographic, and surgicalfactors, and specific assessment ofdysphagia.Results:Mean age was 59.1 (range 36-80),with 17 men and 13 women. Diagnoseswere cervical spondylotic myelopathy(43%), pseudarthrosis with kyphoticdeformity (27%), rheumatoid arthritis(13%), adjacent level disease (10%), andmetastasis (7%). The mean number oflevels fused anteriorly was 3.4 (range = 1-6) and posteriorly was 5.6 (range = 2-8).Fifteen (50%) patients required formalpostoperative swallow evaluation, and 12(40%) had objective evidence ofdysphagia. An NG tube was placed in 9(30%) patients, with 6 (20%) requiringPEG tube placement. Of these six, onewas lost to follow-up and another expiredpostoperatively. The remaining four PEGrecipients had complete resolution ofdysphagia with PEG removal an averageof 6 months after surgery. Patientsrequiring speech evaluation underwentmore levels of anterior exposure (4.1 vs2.7 P = 0.001) and had longer hospitalstays (10.4 vs 5.4 P = 0.001) comparedwith patients not requiring speechevaluation. Factors including duration ofanterior procedure, degree of correctionand preoperative kyphosis did not differsignificantly. Four patients had subjectivecomplaints of dysphagia pre-operatively,with two of these patients ultimatelyreceiving a PEG after surgery.Conclusion: There is a high rate of severedysphagia and PEG tube placementfollowing AP cervical spinereconstructions. A greater number oflevels treated anteriorly was significantly
associated with greater risk ofpostoperative dysphagia. These data mayprove valuable for patient counseling andon-going efforts to improve the safety ofpatient care and suggest that further studyis warranted.
407Posterior Minimally InvasiveDecompression and Stabilization forthe Management of Benign,Intradural, ExtramedullaryNeoplasms of the Thoraco-lumbarSpineVibhor Krishna, Brian Blaker, Avery Lee Buchholz, Steven Morgan, Bruce M. FrankelIntroduction: Benign intraduralextramedullary neoplasms of the thoraco-lumbar spine produce an array ofneurological symptoms that have asignificant impact on quality of life. Therecognized limitations of the ‘open’approach include acceleration ofdegenerative changes, epidural fibrosis,and paraspinal muscle damage. Withrecent advancements in the minimallyinvasive spine (MIS) techniques it can beemployed for the benign neoplasms ofthoraco-lumbar spine.Methods:A retrospective review ofconsecutive patients with benign spinaltumors treated by the senior author withMIS techniques was performed.Results: Gross total resection was achievedin all patients. None of the patientsrequired a conversion to open procedure.Preoperative neurological deficitsimproved in all patients.Conclusion:MIS techniques are feasiblefor resection of small and moderate sizebenign intradural, extramedullary tumorsof the thoraco-lumbar spine.
408The Impact of Sagittal Balance onClinical Outcome FollowingDecompressive Surgery for CervicalSpondylotic MyelopathyRichard Kaplan, Hani Rimlawi Malone,Oscar Flores Medrano, Michael Maurice McDowell, Michael G. KaiserIntroduction: Cervical spondyloticmyelopathy (CSM) is the most commoncause of spinal cord dysfunction inpatients over 55 years of age (1). Inaddition to spinal cord decompression,maintenance of sagittal balance is apotentially important outcome measurethat may be influenced by surgicalapproach (2-4). To better characterize the
importance of this parameter, weinvestigated its association with clinicaloutcome.Methods: The charts of 528 patientsundergoing surgery for CSM at ColumbiaUniversity between 1998 and 2010 wereretrospectively reviewed. Demographicdata, surgical approach, and pre and post-operative clinical and radiographicoutcomes were analyzed. Cervicalalignment was determined by measuringthe C2-C7 lordotic angle from uprightlateral x-rays (5,6). Correlation analysiswith a Pearson two-tailed test was used toinvestigate the relationship betweensagittal balance (pre/post op lordosisangles, as well as angle change) andassessments of clinical outcome utilizingstandard neurological testing.Results: Pre and post-operativeradiographic data was compiled for 55patients. Preliminary analysis did not finda significant correlation between clinicaloutcome and postoperative sagittalbalance (P = 0.45) or change in sagittalbalance (P = 0.33) following surgery.Conclusion: In our initial surgical cohort,we found no significant correlationbetween sagittal balance and clinicaloutcome. We intend to expand this studyas we accrue more patients. Prospectivedata collection is currently underway toincrease sample size and address thepotential relationship between sagittalbalance and postoperative pain, asmeasured by the neck disability index.
409Posterior Less InvasiveDecompression and Stabilization forthe Treatment of Thoraco-lumbarTraumatic Spine FracturesVibhor Krishna, Libby M. Kosnik, Steven Morgan, William A. Vandergrift, III,Bruce M. FrankelIntroduction: The treatment of patientswith traumatic fractures affecting the axialspine, can be approached in a variety ofways, each with its own risks and benefits.In an effort to reduce surgical-relatedpatient morbidity in multiple systeminjured trauma patients, we haveemployed several posterior less-invasivetechniques to decompress and stabilize thethoraco-lumbar spine.Methods:We retrospectively reviewed thecharts of 30 patients treated with one ofthree posterior less invasive methods(MIS) of decompression including: micro-tubular decompressive laminectomy andfacetectomy, microtubular transpedicularpartial or complete corpectomy, or micro-
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 99
DIGITAL POSTER ABSTRACTS

tubular costo-transverse partial orcomplete corpectomy. In these patientsanterior column reconstruction wasperformed, where necessary, by eithertamping fractured bone fragments orperforming VBR cage insertion. Three-column fixation was performed usingpercutaneous pedicle screw insertion andaugmented with PMMA where indicated.The rate of complications, blood loss andhospital length of stay were comparedwith the historical open cohort.Results: The mean age of the patientcohort was 47.5 years (18 males, 13females). A variety of disparatepathologies were treated including AOclassification sub-types: A-3, B, and C,both with and without neurological injury(SCI). There were no cases of newpostoperative neurological deficits, deficitstabilization or improvement was seen inall patients except those presenting with acomplete SCI. The mean number ofsegments fused were 3.8 (Range: 2-8levels). The mean postoperative length ofstay was 6.5 days (Range: 1-28 days). Themean blood loss was 518 cc (Range: 50-2800 cc). There were two cases (6%) ofhardware failure requiring re-operationwithin 6 months postoperatively, and onesuperficial wound infection treated withantibiotics.Conclusion: Posterior less invasivetechniques of decompression andstabilization of the thoraco-lumbar spineshould be considered as a treatment optionfor patients with traumatic fracturesaffecting the axial spine. Length ofhospitalization, blood loss and complicationprofiles compare favorably to historicalcontrols utilizing “open” procedures.
410The Role of Vertebroplasty in AcuteOsteoporotic Vertebral Fractures: AMeta-analysis of Randomized TrialsVibhor Krishna, Yasmeen Rauf, Sarah Denham, Joyce Nicholas, Bruce M. FrankelIntroduction: The role of vertebroplasty inthe treatment of acute osteoportic fracturesremains controversial. Recently, asubgroup analysis from combined patientdata of two large trials was published. Ameta-analysis of these data with two othertrials permitted detection of even smalltreatment effects from vertebroplasty afteracute osteoporotic fractures.Methods:A meta-analysis was performedwith three publications of four trials:INVEST, the Australian trial, VETOS IIand the Netherlands trial. The primary
outcome was improvement in pain scoreson an 11-point visual analogue scale(VAS). An improvement of =3 wasconsidered significant. The cumulativeimprovement in pain score was calculatedusing DerSimonian-Laird (D-L) method.Results: The cumulative resolution in painduring a short-term (less than 3 months)follow-up is 1.15 (-2.48, 0.19) and forlong-term (12 months) is -1.14 (-1.79, -0.49). Both these results are clinicallyinsignificant (improvement in VAS score <3).Conclusion: Both short- and long-termpain relief from vertebroplasty is clinicallyinsignificant for acute osteoporoticfractures. The ongoing randomized trialsshould further investigate the subset ofpatients likely to benefit fromvertebroplasty.
411Surgical Outcome of Extreme LateralInterbody Fusion: A ComparativeRetrospective Study of the Clinicaland Measured Radiological ResultsMarjan Alimi, Christoph Hofstetter,Apostolos Tsiouris, Andrew R. James,Danika Paulo, Eric H. Elowitz, Roger HartlIntroduction: Extreme lateral interbodyfusion (ELIF) is an increasingly populartechnique for anterior fixation of thelumbar spine. More comprehensiveoutcome studies are needed to betterdefine appropriate indications for thistechnique.Methods: Demographic and peri-operativedata of 90 patients who underwent ELIFbetween 2007 and 2011 were collectedretrospectively. For radiographic outcome,pre-op, immediate post-op and follow-upcoronal Cobb angles, disc heights andforaminal heights were measured. Clinicaloutcome was evaluated by OswestryDisability Index and Visual Analog Scalescores.Results: Ninety patients (35 males, 55females) with a mean age of 64 yearsunderwent ELIF surgery. More than halfof the procedures involved a single-leveland the remaining constructs involved 2, 3or 4 levels. Among 156 operated levels,L4/L5 was the most common level,followed by L3/L4, L2/L3, L1/L2. 76.6%of constructs were stabilized by posteriorpedicle screws, 14.4% by lateral platesand 8.9% were stand-alone. Mean time ofsurgery, estimated blood loss, and lengthof hospital stay were 203 ± 94.4 (±SD)minutes, 195 ± 325.7 ml and 4.6 ± 4.9days, respectively. Latest follow-up data
was obtained 12.4 months following theprocedure. Radiographic evaluationrevealed a mean pre-operative coronaldeformity of 7.2 ± 7.40 degrees whichwas reduced to 5.5 ± 5.03 degreespostoperatively. The ELIF procedureresulted in a significant postoperativereduction of deformity (defined asdecrease of > 5 degrees) in 21.6% ofpatients. Moreover, ELIF increasedforaminal height by an average of 3.17mms. Clinical evaluation revealed a meanODI, VAS back, buttock and leg decreaseof 10.73 ± 9.64, 3.78 ± 3.93, 3.57 ± 4.02and 3.83 ± 4.06 points, respectively.84.8% of the patients had a Macnab ofexcellent, good or fair.Conclusion: ELIF is well-toleratedprocedure for instrumentation of thelumbar anterior spinal column. It allowsfor restoration of foraminal height andsome correction of coronal deformity inpatients with symptomatic lumbarspondylosis.
412Preoperative Diagnosis and SurgicalTreatment of Spinal MeningiomasTomohiro Murakami, Izumi Koyanagi,Takahisa Kaneko, Nobuhiro MikuniIntroduction: In spinal meningiomas, themanagement of the dura attachment willbe important to prevent recurrence.Therefore preoperative diagnosis mayplay a role of the surgical strategy. Thepurpose of this study is to analyze thepreoperative diagnosis and determine thesurgical management strategies for spinalmeningiomas in our institute.Methods: This retrospective studyincluded 18 patients (4 men and 14women) between 2002 and 2011 agedmean 57.1 years (range: 22-83 years). Thelevels of tumor were cervical in 8 cases,thoracic in 8 and thoraco-lumbar in 2.Three cases were associated withneurofibromatosis type 2 (NF2).Results:All cases were diagnosed asmeningioma preoperatively andunderwent removal of tumor viahemilaminectomy or laminectomy. Fourtumors were located at the intra- andextradural spaces of upper cervical spine.In two of them, we resected the tumor andalso the dorso-lateral hypertrophic duramater with duraplasty. In othermeningiomas located intradurally, theattached dura was bipolar-coagulatedadequately. Tumors were totally removedin 15 cases, subtotally in 3 cases. Duringthe follow-up period, there was norecurrence of the tumors.
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES100
DIGITAL POSTER ABSTRACTS

Conclusion: Bipolar-coagulation of theattached dura mater is sufficient to preventrecurrence of the intradural spinalmeningioma. For meningiomas showingintra- and extradural extension, surgicalremoval of the hypertrophied dura andduraplasty may be important.
413Spinal Somatosensory EvokedPotentials Correlate with BBB ScoresAfter Spinal Cord Injury of VaryingSeverityShekar N. KurpadIntroduction:We have correlated BBBscores with Spinal somatosensory evokedpotentials (SpSEPs) in the rat after spinalcord injury (SCI). SpSEPs havepreviously been shown to detect andcharacterize different latency componentsassociated with specific spinal pathways.SpSEPs could prove useful inunderstanding spinal cord functionfollowing an injury and provide insightinto course of treatment.Methods: SpSEPs were collected on 40female Sprague-Dawley rats 10 weekspost-injury. 4 groups were included: sham,mild, moderate, and severe thoracic SCIderived from an NYU impactor. SpSEPscharacteristics were correlated with BBBlocomotor scores. Stimulation was appliedto the sciatic nerve to yield SpSEPs.Recording electrodes were placed rostralto T5 and T11. The range of signalamplitude was found as the maximumamplitude-minimum amplitude (D1 = P1-N1) between 10 and 25ms for themid-latency and 25-100 ms for the longlatency (D2 = P2-N2). Finally SpSEPswere correlated to BBB scores.Results: The varying injury severitiesresulted in different SpSEP responses. Theindividual peaks and valleys of the evokedpotential epochs were collected andcompared against the BBB scores.Correlations were noted between theoverall SpSEP amplitude (D1 and D2amplitudes) and the BBB scoring andseverity. D1 time and amplitude weresignificant (P < 0.05), where the D2correlations were not significant.Conclusion: There are characteristicdifferences in SpSEPs between injurieswith different severities and correlate withBBB scores. Overall there was a relationbetween the severity and the mid- or long-latency components.
414Treatment of Herniated Lumbar Discby Sequestrectomy or ConventionalDiscectomyMohammed F. Shamji, Ish Bains, Emma Yong, Garnette R. Sutherland, R. John HurlbertIntroduction: Optimal surgical techniquefor treatment of herniated lumbar discremains uncertain. Advocates ofsequestrectomy cite less perioperativepain and preserved disk architecture,whereas advocates of conventionaldiscectomy cite less frequent reherniation.We investigated perioperative andpostoperative endpoints to evaluate thecomparative success of each procedure.Methods: Consecutive discectomy patientswere treated at a single center by surgeonswith technique to either consistentlyperform sequestrectomy or conventionaldiscectomy. Retrospective collection ofdemographic, radiographic, and outcomesdata provided analysis of each procedure’sefficacy, with particular attention toclinical outcome and reherniation with orwithout need for further operation.Continuous and categorical variables wereanalyzed by ANOVA and Pearsonlikelihood ratio with surgical technique asfactor, at the 0.05 level of significance.Results:Of172patients treated, 74wereunderwent conventional discectomyand98underwent seqeustrectomy, followed formedian6years.Therewerenodifferencesin age, gender, smoking status, and level ofdischerniation (alpha=0.05).Intraoperatively, conventional discectomydidnot associatewith anygreater bloodloss (P=0.90)or longerdurationof surgery(P=0.67), norwith anyperioperativedifference in lengthof stay.Postoperatively,we reoperated for discherniation in14%ofpatients, variableby surgical technique (P<0.01).Amongconventional discectomy,the reoperation ratewas10%(6%same-level, 4%adjacent-level), lower thansequestrectomywith reoperation rate of19%(15%same-level, 4%adjacent-level).In the latter group, a trendof reherniationwasobservedamongsmokers.Conclusion: This cohort of patients withgood long-term follow-up exhibited areoperation rate of 14%, more frequentwith sequestrectomy than conventionaldiscectomy. No significant differencesoccurred with blood loss, surgical time, orhospital length of stay. Clearly, while alarger prospective RCT may moredefinitively answer this question, thisstudy provides substantial support for amore conventional surgical approach.
415Rates of Infection with DynamicStabilization Compared to PosteriorInstrumented FusionIra M. Goldstein, Nitin Agarwal, Antonios Mammis, James Barrese, Lana D. ChristianoIntroduction: Dynamic stabilization offersan adjunct to fusion with motionpreservation. Dynamic stabilizationconstructs include a polycarbonateurethane spacer secured by titaniumpedicle screws, which allows for limitedflexion and extension. In comparison,standard instrumented fusion (IF) consistsof titanium screws and rods/plates, whichdo not allow for motion at the level of thefusion. The reported infection ratefollowing a standard IF ranges from 0.2%-7%.Methods:A retrospective chart review of142 patients who underwent posteriorlumbar stabilization procedures wasconducted. Ten patients received dynamicstabilization and 132 patients had astandard IF. Rates of infection, requiringhardware removal, were comparedbetween the aforementioned groups.Comorbidity scores were assigned to eachpatient, using the Charlson ComorbidityIndex.Results: Of the 132 patients undergoingposterior IF, 3 developed a deep woundinfection requiring removal of hardware(2.3%). Of the 10 patients undergoingdynamic stabilization, 3 developed a deepwound infection (30%) with 2 requiringremoval of hardware (20%), secondary topersistent deep wound infection orosteomyelitis at the pedicle screw sites.There was a significantly increased risk ofdeep wound infection (P < 0.0001) withthe use of dynamic stabilization comparedto standard IF. Comorbidity scoresdemonstrated no difference between thedynamic stabilization and IF groups, but asignificant difference (P < 0.05) wasfound, within the IF group, comparingpatients that did and did not developinfection.Conclusion: Our series demonstrates thatthe infection rate in patients undergoingdynamic stabilization is higher than thatfor instrumented fusion. We postulate thatthe polycarbonate urethane spacer acts asa medium for bacteria, whereas thetitanium screws and rods are smooth,solid, and inert, resulting in a lower risk ofinfection. Future research should include aprospective trial comparing the infectionrates of posterior instrumented fusion tothat of posterior dynamic constructs.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 101
DIGITAL POSTER ABSTRACTS

417DVT Prophylaxis in Primary SpinalCord Tumor ResectionAnubhav Gautam Amin, Harold Wu,Gustavo Pradilla, Amit Jain, George I. Jallo, Ziya L. Gokaslan, Wesley HsuIntroduction: Deep venous thrombosis(DVT) and pulmonary embolism (PE) canoccur after surgical resection of spinalcord tumors. Although postoperativeadministration of subcutaneous heparinhas been shown to decrease the risk ofpostoperative DVT, there is some concernthat this may increase the risk ofpostoperative hemorrhage. We reviewedour institution’s recent experience withspinal cord tumor resection to assess theincidence of DVT/PE.Methods:Medical records were reviewedfor 62 patients who underwent surgicalresection of a primary spinal cord tumor atthe Johns Hopkins Hospital between2006-2009.Results: The median patient age was 48(range, 22-93). Twenty-seven (44%)patients were male. The most prevalentcomorbidities were: hypertension (19%)and hyperlipidemia (11%). Presentingsymptoms included: sensory deficit(76%), back pain (74%), motor deficit(60%), and urinary/bowel incontinence(31%). Tumors were located mostcommonly in the cervical (46.8%) andthoracic (46.8%) spine. Tumors werelocated intradural-extramedullary (29%)and intramedullary (71%). The mostcommon tumor pathologies were:ependymoma (57%), meningioma (26%),and astrocytoma (10%). Post-operatively,all patients wore compression stockingsand intermittent pneumatic compressiondevices. 42 (68%) patients wereadministered heparin subcutaneously(1000U) every 12 hours starting 12-48hours after surgery. The median length ofstay was 5 days. Postoperatively, 81%showed improvement in motor function,68% showed improvement inurinary/bowel incontinence, 65% showedimprovement in back pain, and 62%showed improvement in sensory deficit.There were 12 complications: 4 CSFleaks, 3 surgical site infections, 2 epiduralhematomas requiring surgicalintervention, 2 DVTs, and 1 PE whichresulted in death. There were no instancesof intradural/intraparenchymalhemorrhage requiring surgicalintervention. Of the 3 (4.8%) cases ofDVT/PE complications, two patients didnot receive subcutaneous herparin
postoperatively. Of the 2 (3.2%) cases ofepidural hematomas, one patient was onanticoagulation.Conclusion: DVT/PE after surgicalresection of spinal cord tumors may bemore common than previouslyrecognized. DVT prophylaxis cannot fullyprotect a patient from this complication.Administration of subcutaneous heparindoes not appear to increase the risk ofpostoperative hemorrhaghic complicationsin this patient population.
418Evaluation of Radiographic Evidenceof Interspinous Fusion in VariousConstructs of Minimally InvasiveLumbar SurgeryAmir A. Vokshoor, Arian Esmaili, Sanjay Khurana, Peter Filsinger, Dean WilsonIntroduction: InterSpinous Process (ISP)fixation for fusion has gained recentattraction as a less invasive option forpatients undergoing lumbar fusion surgeryfor the treatment of degenerative discdisease, spondylolisthesis and/or instabilityof the lumbar spine. ISP fixation can beused in a variety of constructs, their actualfusion success rate has yet to bedetermined in a large case series.Methods: 46 patients who underwent ISPfixation over a 48-month period wereevaluated. In patients who underwentlumbar fusion with an ISP fixation device,interspinous fusion (and interbody fusionif applicable), was assessed using post-operative CT imaging obtained between 2and 23 months. These images werereviewed by an independent radiologist toevaluate success of fusion for the ISPspace using the following scale: Grade 1indicates small islands of bone, Grade 2shows larger islands of coalescence withbridging to the surrounding anatomy,Grade 3 indicates some solidincorporation and bridging bone, Grade 4shows solid fusion, with incorporation andobvious stability and maturity. Fusion ofthe intervertebral space was assessedusing the Burkus criteria.Results: 38 patients represented a total of43 lumbar levels with ISP fixation forfusion. 91% of levels demonstratedGrades 4 ISP fusion based on theaforementioned scale. 25 levels (64%)fused posteriorly also had placement of aninterbody cage. 21 of these levels (84%)showed solid interbody fusion (BSF-3).Of the 4 pseudoarthrosed levels, 2 hadadjunct pedicle screw fixation, and 2 wereinterbody and ISP fixation alone. 2 of
these patients underwent re-explorationand explantation due to post-operativepain secondary to fracture of the spinousprocess and/or lamina.Conclusion: ISP fixation is a safe andeffective minimally invasive technique inlumbar fusion surgery and uses a lessinvasive approach than traditional fixation.
419A New Alternative to EstablishReliable Atlanto-Axial (C1-2) FusionJoseph Chia Yu Hsieh, Samer Ghostine,Doniel Drazin, Shoshanna S. Vaynman,Terrence T. Kim, Parham Zarrini, Stephen Scott Scibelli, Scott Schoeb,Srinath Samudrala, Carl Lauryssen,J. Patrick JohnsonIntroduction:Atlanto-axial (C1-2) fusioncan be complicated by (1)pseudoarthroses from insufficient surfacearea for fusion and (2) chronicpostoperative pain from sacrifice of the C2nerve root. This study presents findingsfor a novel surgical technique for C1-2fusion using C1 lateral mass and C2pedicle screw fixation with intra-articulararthrodesis to maximize a surface areaunder direct axial load favored by Wolff’slaw while sparing the C2 nerve.Methods: Retrospective review wasperformed on 29 patients withdocumented C1-2 instability whounderwent the described single stageprocedure from 2001 to 2010 (median age73 years, age range 30-83 years, 18females and 11 males, 9 with smokinghistory). In all cases, patients underwentisolated C1 lateral mass and C2 pediclescrew placement with fluoroscopic orimage guidance and C1-C2 jointpreparation using a high-speed burr withC2 nerve-sparing mobilization.Arthrodesis was completed by packing thejoint cavity with autologous bone alone(15 cases) or supplemented byrecombinant human bone morphogenicprotein (rhBMP) (14 cases). No otherposterior interspinous fusions wereperformed.Results: Radiographic or clinical evidenceof C1-C2 fusion/stability was achieved inall patients at last clinic visit (median of 8months). Median post-operativehospitalization period was 4 days (range1-10 days). Median operative time was138 minutes (range 97-189 minutes).Median estimated blood loss was 300 cc(range 75-1100 cc). In total, 26 of 29(89.6%) patients had minimal or no painat last clinic visit. One patient withdocumented fusion had post-operative
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES102
DIGITAL POSTER ABSTRACTS

occipital headaches from a C1 screwimpinging on the C2 nerve root with painresolving after hardware removal.Conclusion:Atlanto-axial (C1-2) fusionusing C1 lateral mass and C2 pediclescrews with C2-nerve sparing C1-2 intra-articular arthrodesis is a safe and reliabletechnique with high fusion and lowcomplication rates.
420Two-Level Anterior CervicalDiscectomy vs. One-LevelCorpectomy in Cervical Spine:Biomechanical StudyKamran Aghayev, Imam Saleh, Nam Duy Tran, Frank D. VrionisIntroduction: The aim of the study was tocompare the biomechanical behavior ofhuman cervical cadaveric segments in thefollowing conditions: intact, one levelcorpectomy, and two level discectomy.Methods: Seven fresh frozen humancadaveric spines (C3-T1) were used. Theinitial testing was performed on intactspecimens. Pressure transducers wereinserted at C3-C4, and C6-C7 disc spaces.Strain gauges were affixed on facets ofC3-C4 and C6-C7 bilaterally. Pressuretransducer and strain gauge signals wereconditioned and amplified by a signalconditioner and recorded by the servo-hydraulic mechanical testing system.Discectomy was performed at C4-5 andC5- 6 levels, with cage and anterior platereconstruction, followed by C5corpectomy with cage and platereconstruction. The outputs of the pressuretransducers and strain gauges weredetermined for each specimen in thefollowing conditions and order: 1) intact,2) after discectomy and implantation oftwo cages and anterior plate 3) aftercorpectomy and implantation of cage andanterior plate. Calculated responses of theintact and simulated fusions werecompared at each loading condition.Results: Statistical significance (P < .05)reached for both: range of motion andstiffness between the intact/twodiscectomy and corpectomy/twodiscectomy conditions in all movingconditions. In the intact condition bothsuperior and inferior adjacent discs hadthe highest mean intradiscal pressure,followed by corpectomy (P > .05). Thetwo discectomy condition had the lowestmean adjacent disc intradiscal pressuresand statistical significance between theintact and two discectomy conditions wassignificant (P > .05) for superior andinferior intradiscal pressures in flexion-
extension as well as superior intradiscalpressure in axial rotation. For all motionsand conditions peak superior facetmicrostrains were higher than inferior.There were no statistically significantfacet microstrain differences between theintact and simulated fusions.Conclusion: Stiffness and range of motiondata show that two discectomy morestable than corpectomy. Conversely toprevious reports we found that simulatedfusion decreases intradiscal pressure andthere is an inverse relation between thestiffness and intradiscal pressure.
421Intracranial ComplicationsAssociated With Spinal SurgeryMartin Pham, Alexander Tuchman, Andrew Platt, Sara Kingston, Thomas C. Chen, Patrick C. HsiehIntroduction: Though rare, intracranialcomplications have been reported as aresult from spinal surgery. Most if not allof these are a result of intracranialhypotension from CSF leak andhypovolemia.Methods:We conducted a retrospectivereview of all patients who underwentspinal surgery at our institution by twoneurosurgeons from July 2008 to April2011.Results: Our review yielded 484 patientswho underwent spinal surgery for a total of 616 procedures. There were 227 (47%)men and 257 (53%) women. Their meanage was 58.3 years (range 20-90).Intracranial imaging using either CT orMRI were obtained on 22 (3.6%) patientsafter a procedure due to neurologic change.Two patients (0.3%) were found to havebilateral subdural hygromas suggestive ofacute intracranial hypotension. There wereno reports of any hemorrhages, strokes, orother complications of the intracranialcompartment.Conclusion: Intracranial complicationsfrom spinal surgery are a rare event. Wedemonstrate an incidence of 0.3% of totalintracranial pathology, all of which weresubdural hygromas. There were no casesof intracranial hemorrhage and infarction.
422Biomechanical Comparison ofAnterior Cervical SpineInstrumentation Techniques AfterTwo Levels CorpectomyKamran Aghayev, Imam Saleh, Nam Duy Tran, Frank D. VrionisIntroduction: The aim of this study was tocompare the stiffness and range of motionof four cervical spine constructs and theintact condition: three anterior cervicaldiscectomies with three level anteriorplate, one discectomy and one corpectomywith three level anterior plate, two levelscorpectomy with three level anterior plate,two levels corpectomy with anterior plateand posterior fixation.Methods: Eight human cadaveric fresh-frozen cervical spines from C2 T2 wereutilized. Three-dimensional motionanalysis with an optical tracking devicewas used to determine motion followingvarious reconstruction methods. Thespecimens were tested in the followingconditions: 1) intact, 2) segmentalconstruct with discectomies at C4-C5, C5-C6, C6-C7, PEEK interbody cage, andanterior plate 3) segmental construct withdiscectomy at C6-C7, corpectomy of C5,with PEEK interbody graft at discectomylevel and titanium cage at corpectomylevel 4) corpectomy at C5 and C6 withtitanium cage and an anterior cervicalplate and 5) corpectomy at C5 and C6with titanium cage and an anteriorcervical plate and posterior lateral massscrews/rod system from C4 to C7. Allspecimens underwent a pure momentapplication of 2 Nm with regards toflexion extension, lateral bending, andaxial rotation.Results: In all tested motions the statisticalcomparison between intact and the twolevels corpectomy with anterior plate andposterior fixation construct wassignificant. All other comparisons werenot statistically significant except betweenthe three levels discectomy and the twolevel corpectomy in axial rotation.Conclusion: Segmental plate fixation (threelevels discectomy) affords the samestiffness and range of motion ascircumferential fusion in two levelcervical spine corpectomy. This obviatesthe need for staged circumferentialprocedures for multilevel cervicalspondylotic myelopathy. The placement ofposterior instrumentation should bestrongly considered to significantlyimprove the overall stability of thestability after a two level cervicalcorpectomy.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 103
DIGITAL POSTER ABSTRACTS

423High-Grade Traumatic CervicalSubluxation Injuries: TreatmentStrategies and OutcomesSanjay S. Dhall, Daniel J. HohIntroduction: Traumatic high-grade(>50%) cervical subluxations areuncommon spinal injuries, oftenassociated with severe neurologiccompromise. Particularly, traumaticcervical spondyloptosis (>100%subluxation) is rare, with little reported inthe literature regarding treatment andoutcome. To the best of our knowledge,we present the first reported case seriesdescribing management of these complexspinal injuries.Methods:A study at three level 1 traumacenters was performed of patients withtraumatic cervical subluxation >50%.Charts were assessed for clinicalpresentation, treatment modalities,admission and post-treatment neurologicstatus, and complications.Results: Eleven patients with high-gradesubluxation were identified, 7 who had>=100% subluxation. Ages ranged 19 to76 years. High-energy closed spinal injurywas the mechanism in all but one patient.Admission ASIA grade varied (A=4, B=1,C=4, D=1, E=1). Ten patients underwenthalo traction with five (50%) failingclosed reduction. High-dosemethylprednisolone was administered in 4patients. All patients underwent surgicalstabilization ± open reduction: anterioronly (n = 3), posterior only (n = 3),combined anterior-posterior (n = 5). Fourpatients (36.4%) had good post-treatmentneurologic outcome (ASIA D, E), 2 ofwhom improved one ASIA grade. Oneadditional patient remained ASIA B,however, improved in neurologic level ofinjury post-treatment. Complicationsincluded neurologic worsening (n = 1),traction pin-site scalp laceration (n = 2),hardware failure (n = 1), vertebral arteryinjury (n = 1), infection (n = 1), DVT (n =1), death (n = 1).Conclusion: High grade traumatic cervicalsubluxations are complex, unstableinjuries. Remarkably, 45.5% demonstratedgood neurologic outcomes as defined asimprovement in ASIA grade, neurologiclevel of injury, or preservation of goodASIA grade. Pre-operative traction did notsignificantly improve neurologic outcomeand was associated with high failure rateof reduction. Likely due to severity ofthese injuries, there was a high incidenceof related complications. However, giventhe observed potential for neurologic
improvement, we recommend aggressivesurgical reduction and stabilization forthese complex spinal injuries.
424Validation of the SRS-Schwab AdultDeformity ClassificationJustin S. Smith, Christopher I. Shaffrey,Benjamin Ungar, Frank Schwab, Virginie Lafage, Benjamin Blondel, Jacob Buchowski, Jeffrey Coe, Hossein Mehdian, Clifford TribusIntroduction:A classification system foradult spinal deformity (ASD) can serveseveral purposes, including: consistentcharacterization of a clinical entity, a basisfor comparing different treatments, and abasis for recommending treatments. Basedupon a Scoliosis Research Society (SRS)effort, this study seeks to determine if aproposed new ASD classification systemis clear and reliable.Methods: Initiated by the SRS AdultDeformity Committee, this study used aclassification system previously publishedby Schwab and revised to include pelvicparameters. Modifier cutoffs weredetermined using health-related quality oflife data from a multi-center database ofadult deformity patients. 9 readers graded21 pre-marked cases twice each,approximately one week apart. Inter- andintra-rater reliability and inter-rateragreement were determined for the curvetype and each modifier separately. Fleiss’Kappa was used for reliability measures,with values of 0.00-0.20 considered slight,0.21-0.40 fair, 0.41-0.60 moderate, 0.61-0.80 substantial, and 0.81-1.00 almostperfect agreement.Results: Inter-rater Kappa for curve typewas 0.80 and 0.87 for the two readings,respectively, with modifier Kappas of 0.75and 0.86, 0.97 and 0.98, and 0.96 and 0.96for pelvic incidence-lumbar lordosis (PI-LL), pelvic tilt (PT), and sagittal verticalaxis (SVA), respectively. By the secondreading, curve type was identified by allreaders consistently in 66.7%, PI-LL in71.4%, PT in 95.2%, and SVA in 90.5%of cases. Intra-rater Kappa averaged 0.94for Curve Type, 0.88 for PI-LL, 0.97 forPT, and 0.97 for SVA across all readers.Conclusion: Data from this study show thatthere is excellent inter- and intra-raterreliability and inter-rater agreement forcurve type and each modifier. The highdegree of reliability demonstrates thatapplying the SRS-Schwab system is easyand consistent. Greater Kappa values inthe second set of readings alsodemonstrate a learning curve in
application of the classification system.
425PEEK Rods for Stabilization of theLumbar SpineRobert M. GallerIntroduction: Instrumented fixation forspinal surgery has become an increasinglyutilized method to achieve fusion. Withthe rising use of rigid fixation there hasbeen recognition of the development ofproblems with adjacent segments in termsof premature degeneration. The exactmechanism is unclear but it is believedthat the increased stresses on the adjacentsegment to the fused segment in thepresence of hardware provides increasedtension on the elements of the spineleading to degeneration, spondylolisthesisand stenosis. Polyetheretherketone(PEEK) has been used as a biomaterial fororthopedic, and spinal implants. PEEK isa thermoplastic polymer whose chemicalstructure maintains stability attemperatures exceeding 300??C, resistschemical and radiation damage, exhibitsgreater strength per mass than manymetals, and offers compatibility withmany reinforcing agents. PEEK as abiomaterial is fully biocompatible, withnumerous studies documenting minimalsystemic, intracutaneous, andintramuscular toxicity.Methods: This is a retrospective caseseries of the surgical experience of asingle surgeon. 65 cases of patientsimplanted with PEEK rods are reviewed.The CD Horizon Legacy PEEK rodsystem was used in all cases with orwithout the addition of interbody grafting.The interbody grafts were PEEK implantsor Bone.Results: The patients were followed at 1week, 1 month, 3 month and 6-monthintervals. All patients are to be followed atone year with clinical and radiographicevaluation. Fusion mass developed withexcellent clinical results. Complicationrates were comparable to previousexperience and published reports with noevidence of rod breakage in either group.One patient in the PEEK rod group retropulsed a graft after a postoperative fall.This required re-operation.Conclusion: PEEK rods represent a safealternative to Titanium rods forinstrumentation of the lumbar spine.
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES104
DIGITAL POSTER ABSTRACTS

427Outcomes in Surgical Managementfor Adult Degenerative LumbarScoliosis: A Comparison of ThreeDifferent ApproachesAnish A. Patel, Jared Fridley, Ibrahim OmeisIntroduction:Adult degenerative lumbarscoliosis is a complicated spinal disorderin which the optimal managementalgorithm is often not clear in patientswho require surgical intervention. Thepurpose of this study was to review theliterature in order to review the pre- andpost-operative spinal measurements,clinical outcomes, and complicationsbetween three general surgical approachesfor treating this disease: decompressionalone, decompression with short segmentfusion, and decompression with full-curvefusion.Methods: The published literature wasreviewed using manual and electronicsearch techniques. Data includeddemographics, presenting symptoms,Cobb angle, lumbar lordosis, laterallisthesis, sagittal plumb angle, number oflevels decompressed and fused, recovery,post-operative complications, Oswestrydisability index (ODI), and incidence ofrevision surgery.Results: Six relevant publications werefound, reporting on a total of 37 patientsin the decompression alone group, 110patients in the partial fusion group, and190 patients in the long fusion group.Among the three groups, the averagenumber of decompressions was 1.9, 2.5,and 3.1 levels, respectively. There was amean of 3.1 levels fused for the shortfusion group and 5.9 levels for the longfusion group. Pre-operative Cobb angleswas similar for each group (21.1, 21.7,and 23.8 degrees). During theirpostoperative follow up, in thedecompression group, 75% were reportedto have recurrent stenosis and 14%needing revision. In the partial fusiongroup, 36% of patients had adjacentsegment disease and 11% underwentrevision. In the long fusion group, 26%developed adjacent segment disease, with16% needing revision. The averageimprovements in ODI for thedecompression group, partial fusiongroup, and long fusion group were 7.9,11.2, and 11.4, respectively.Conclusion:Although all three approachesshowed good post-operative outcomes,each method also has its own set ofcomplication and revision rates that werelikely influenced by pre-operative
conditions as well as co-morbidities.Likewise, these patients were notrandomized thus leaving selection bias asa significant confounding factor. Thus,more studies are needed to specificallydetermine what pre-operative variablesand range of deviation necessitate aspecific approach.
428Loading Rate Dependency ofThoraco-Lumbar Spine FractureLocation: An Investigation of Traumain Military ScenariosBrian D. Stemper, Jamie Baisden, Narayan Yoganandan, Dennis J. Maiman,Frank A. PintarIntroduction: Diverse injury mechanismsin military environments necessitate thestudy of associated spinal injuries andrelevant clinical biomechanics. Aviatorejections and helicopter crashes havetraditionally constituted the most commonspinal injury modes. However, currentconflicts have demonstrated a prevalenceof underbody blast (UBB) events due toincreased use of improvised explosivedevices. Although all three environmentsinvolve primarily vertical acceleration/deceleration, the differences lie in theloading rate, with helicopter crashes andUBB occurring at higher accelerationsand with greater rates of onset.Methods: This abstract presents ananalysis of clinical, descriptive, andbiomechanical studies in these areas.Results: Ejection-related injuries weredistributed across the entire vertebralcolumn, focused in the mid-thoracicregion and thoraco-lumbar junction.However, helicopter crash and UBB-related injuries were biased toward dorsalregions. Specifically, 38%, 42%, and 2%of ejection injuries occurred in the middlethoracic, throaco-lumbar, and lowerlumbar regions. In contrast, 12%, 52%,and 16% of helicopter crashes affectedthose regions. Likewise, 10%, 52%, and38% of UBB injuries affected the sameregions. Injuries were focused in the mid-thoracic areas for ejection and in themiddle and lower regions of the lumbarspine for higher-rate scenarios.Conclusion: These patterns indicate thatthe primary mode of external loadtransmission, as well as rate at which theloading is applied, affect injurydistributions within the anatomicalstructure. These distributions contrastcivilian populations wherein thethoracolumbar junction is the mostvulnerable region for acute trauma.
Important biomechanical factors affectingtrauma included loading rate, dynamicload level, occupant anthropometry, andposture/alignment with respect to theloading vector at the time of thetransmission of the external load. Thechanging injury patterns resulting incaudal migration for underbody blast androstral migration for ejection loadingsmay have implications in the treatmentregimen.
429Correlation Between Thoracic andThoracolumbar Spinal andNeurological Injuries and MagneticResonance Imaging FindingsDaniel Robert Fassett, Swetha Naroji,Mitchell Gil Maltenfort, Yazhini Gnanasambanthan, Shiveindra Jeyamohan, James S. HarropIntroduction: The objective of this studywas to correlate MRI findings withneurological deficits associated withthoracic spinal cord injuries (SCIs).Methods: The association betweenneurological deficits and MRI findingswas assessed in a case control series ofconsecutive patients who underwentthoracic spine MRI as part of evaluationfor traumatic injuries. Spinal canalcompromise, spinal cord compression,extent of cord edema, and parenchymalhemorrhage were analyzed for correlationwith the presence and degree ofneurological deficits.Results: Seventy-seven patients (51 male,26 female) with a mean age of 34.6 yearswere identified (36 patients withneurological deficits attributable to spinalcord injury (SCI) and 41 patients with noapparent deficits). Canal compromise wasnoted in 51 patients (31 patients greaterthan 25% and 8 greater than 50%compromise). Canal compromise greaterthan 25% had a Positive Predictive Value(PPV) for SCI of = 74.2% and PPV ofgreater than 50% canal compromise was100%. Spinal cord compression had aPPV = 84.6% and a Negative PredictiveValue (NPV) = 92.1%. Spinal cordcompression had a 91.6% sensitivity and85.3% specificity in predicting SCI.Spinal cord edema had a PPV = 92.3%,NPV = 76.4%, Sensitivity = 66.7%, andSpecificity = 95.1%. Eleven patients hadintramedullary hemorrhage and all hadneurological deficits (PPV =100%, NPV =62.1%).Conclusion: This is the first study tocorrelate MRI findings with the presenceof neurological deficits in thoracic spinal
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 105
DIGITAL POSTER ABSTRACTS

injuries. Several findings were associatedwith a high likelihood for neurologicaldeficits with thoracic spinal injury,including (1) >50% spinal canalcompromise, (2) presence of spinal cordcompression, (3) presence of spinal cordedema, and (4) presence of intramedullaryspinal cord hemorrhage. In attempting topredict the absence of SCI, the absence ofspinal cord compression was the bestpredictor of no neurological deficits.
430Trends in the Surgical Treatment ofC2 FracturesAli A. Baaj, Tien V. Le, Fernando L. ValeIntroduction: The second cervical vertebrais the most commonly fractured level incervical spine trauma. With advancementsin surgical technique and technology, wehypothesized that there is an increasingtrend of surgical intervention in cases ofC2 fractures on a national level.Methods: Data were abstracted from theNationwide Inpatient Sample (NIS) forthe years 2005 through 2009. The NIS ismaintained by the Agency for HealthcareResearch and Quality and represents a20% random stratified sample of alldischarges from nonfederal hospitalswithin the United States. Patients with C2fractures that underwent spinal fusionwere identified using the appropriate ICD-9-CM codes. The number of discharges,length of stay (LOS), hospital charges,and total national charges were analyzed.Results: 137,000 records were obtained foranalysis. During this 5-year period, therewas an 18% increase in the number ofadmissions for C2 fractures (24,508 in2005 to 28,837 in 2009), but an 85%increase in the number of spinal fusionsduring the same time period (1,317 in2005 to 2,436 in 2009). Furthermore,there was a 57% increase in the surgicalrate during this 5-year period (5.4% in2005 to 8.5% in 2009). Hospital chargesassociated with spinal fusions for C2fractures increased by 32% but the totalnational bill increased by 145%.Conclusion:Analysis of a nationalhealthcare database confirms ourhypothesis of increased trends of surgicalintervention in the cases of C2 cervicalspine fractures. We believe thatadvancements in spinal technique andtechnology are contributing factors. Giventhe associated increases in costs, however,our efforts to make these interventionsmore cost-effective needs to continue.
431Placement of Thoracic TransvertebralPedicle Screws Using Three-Dimensional Image GuidanceEric W. Nottmeier, Stephen M. PirrisIntroduction: Originally described byAbdu[1], transvertebral pedicle screwshave been used successfully in thetreatment of high-grade L5-S1spondylolisthesis.[2,3] An advantage oftransvertebral pedicle screws is purchaseof multiple cortical layers across twovertebrae, thereby increasing the stabilityof the construct.[4] The use oftransvertebral pedicle screws at spinallevels other than L5-S1 has not beenreported. The authors report their initialexperience with placement of thoracictransvertebral pedicle screws using conebeam computed tomography (cbCT)-based, three-dimensional (3D) imageguidance.Methods: Seven patients underwentplacement of 26 thoracic transvertebralpedicle screws. Image guidance was usedto place the screws across the thoracicpedicle from inferior to superior with thescrew crossing the cortical endplates ofthe disc space above (Figs. 1-2). Anintraoperative cbCT scan was accomplishedin every patient to confirm adequate screwplacement. Screw position and breachwere assessed on intraoperative cbCTscans or postoperative CT scans.Results:A total of 26 transvertebralpedicle screws were placed into thoraciclevels spanning from T1 to T12. Nocomplications resulted frominstrumentation placement or the use ofimage guidance. Additionally, no screwshad to be replaced or repositioned afterintraoperative review of the cbCT scans.Review of intraoperative cbCT andpostoperative CT scans revealed allscrews to be across the superior disc spacewith the tips in the superior vertebral body(Fig. 3). Six pedicle screws were placedusing the in-out-in technique in patientswith narrow pedicles leaving 20 screwsthat underwent breach analysis, none ofwhich was noted to have a breach. Anoticeable increase in insertional torque ofthe transvertebral pedicle screws wereobserved by the authors as compared tostandard pedicle screws that were placedcontralaterally or at other levels in thesame patient.Conclusion: Placement of thoracictransvertebral pedicle screws can beaccomplished safely and accurately withthe use of image guidance. A formalbiomechanical study is planned to
quantify the possible increasedbiomechanical stability to a construct thatthese screws may provide.
432Disseminated MyxopapillaryEpendymomas of LumbosacralSpine: A Preliminary Series of EightCasesPatrick R. Maloney, Jeffrey T. Jacob,Michelle J. Clarke, William E. Krauss,Caterina GianniniIntroduction:Myxopapillaryependymomas (MPEs) account for 13%of all ependymomas with a predilectionfor the lumbosacral region (1,2). Whilegross total resection (GTR) is the goldstandard, patients may have disseminationat presentation, making GTR impractical(3-5).The management followingresection in those with disseminateddisease remains controversial (6,7).Methods: From August 1988 to September2011, nine patients were identified havingundergone treatment for disseminatedMPE at our institution, 8 of whom hadfollow-up greater than 1 year for whichresults were analyzed. All patients hadundergone primary surgical resection ofall visible tumor in the operative bed,however disseminated disease was notedin the lumbosacral cisterns at the time ofthe initial surgery. Patients with simplebiopsies were excluded. Availablesurgical/pathological reports, clinical andradiological outcomes in patients withdisseminated MPEs were reviewed.Results:Average age at pathologicdiagnosis was 29 (range 17-46). Sixpatients (67%) had undergone initialtreatment at an outside institution. All hadevidence of disseminated disease seedingthe cisterns and tracking along thelumbosacral roots at the time of the initialsurgery per operative notes or imaging.Following surgery, 1 patient (11%) wasobserved, 3 patients (33%) receivedupfront radiation, and 5 patients (83%)had progression requiring treatment eitherby radiation (n = 3) or further surgery (n =2). The respective mean and median timeto progression in those who receivedradiation was 89 and 62 months vs. 26and 28 months in those who did notreceive any form of radiation.Collectively, 7 out of 8 patients (88%) hadcontinued progression of diseasefollowing their initial management duringthe follow-up period. The mean andmedian follow-up for the entire cohortwas 128 and 88 months respectively.Conclusion:Management of disseminated
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES106
DIGITAL POSTER ABSTRACTS

MPE remains challenging. Close follow-up with or without adjuvant treatment isadvised.
433Inhibition of Epidural Fibrosis by anHSP20-mimetic (AZX100) in theRabbit Model of Laminectomy: APilot StudyRandall W. Porter, Roger S. Crowther,Mark C. PreulIntroduction:AZX100, a synthetic peptidecomprising a fragment of heat shock-related protein HSP20 conjugated to aprotein transduction domain, inhibitsfibroblast production of pro-fibrotic growthfactors, including connective tissue growthfactor (CTGF).This pharmacologic profileled us to evaluateAZX100 effectiveness onthe severity of epidural fibrosis in the rabbitlaminectomy model.Methods: New Zealand rabbits hadlaminectomies (~ 10 x 15 mm) performedat T4-5, and before closing wereimplanted with osmotic pumps deliveringvehicle (saline) or 5.0, 50.0 or 500 microg of drug per day between days 7-28 post-surgery (n = 3 per group). Two rabbitsreceived laminectomies but were notimplanted with pumps (no intervention).After sacrifice at 28 days, histologicsections were prepared, stained with H &E or trichrome, and evaluated, blinded, bya veterinary pathologist for fibrosis (1),fibroblast and inflammatory cell density(2) and bone regeneration.Results: Drug vehicle and no interventionGroups had similar mean epidural fibrosisscores (3.0 and 2.5, respectively,maximum score = 3). Fig. 1 is arepresentative vehicle controlphotomicrograph showing diffuseadherence of dura mater to scar tissuefilling the laminectomy site. Five and 50micro g/day treated Groups had similarfibrosis scores: 2.3 and 2.7, respectively. Anotable reduction in epidural fibrosis(mean = 0.3) was seen in the 500 micro gper day treatment Group. The differencewas not significant, because of the smallgroup size. Fig. 2, from a 500 micro g/daytreated animal, shows the striking absenceof fibrosis at the dura mater. Nodifferences were seen in scores forfibroblast or inflammatory cell density. Inall specimens, bone regeneration wasnoted as Grade 1 or 2, with no consistentdrug-related effect.Conclusion: These pilot data show thatAZX100 can strikingly reduce epiduralfibrosis in a relevant surgical model, andshould undergo further study.
436The Schwannomatosis InternationalDatabaseAllan J. Belzberg, Amanda Bergner,Jaishri BlakeleyIntroduction: Schwannomatosis is arecently recognized disorder, withdiagnostic criteria first published in 2005.Little is known about the natural history.Given the limited number of patientsidentified with the disorder, this is achallenging undertaking and acollaborative effort is desirable to allowfor pooling of data from multiple centers.Methods: The specific aims of this projectwere: (1) coordinate national andinternational experts in schwannomatosisto formulate key research questions, (2)translate key questions into specific datapoints, (3) design a web-based database tocollect data across international treatmentcenters.Results: A collaboration of internationalschwannomatosis experts from fifteeninstitutions in eight countries wasestablished. The SchwannomatosisInternational Database (SID) wasdesigned and built around core questions.The data points were chosen specificallyto provide adequate information toresearchers while remaining de-identifiedto protect patient confidentiality. Thedatabase is a platform from whichmultiple research endeavors can belaunched, assisting researchers to identifysubjects who might be appropriate fortheir studies. A steering committee hasbeen established for this collaboration andby-laws have been ratified. Individualresearchers with a question in the field ofschwannomatosis can submit a letter ofintent to the SID Steering Committee. Theresearch will be reviewed and, ifapproved, the database will be queried toconnect the researcher with the centersthat manage the patient(s) of interest.Currently, 14 centers are participatingrepresenting 6 countries.Conclusion: This project has increasedcommunication and collaboration withinthe schwannomatosis community ofexperts. It will also facilitate connectionsbetween researchers studyingschwannomatosis and patients wanting toparticipate in research. Suggestions fortrial design and evaluation of relevance tothe schwannomatosis community will beevaluated through the process of steeringcommittee review of letters of intent. Themethodology can be easily adapted toother medical conditions.
437Percutaneous Placement of ThoracicIntra- and Extrapedicular Screws:Clinical and Radiographic ResultsJustice Agyei, John W. GermanIntroduction: Intrapedicular (IP) andextrapedicular (EP) screw placement arerecognized as viable options forstabilization of the thoracic spine. Onlyone small series of percutaneous screwplacement has been published.Methods:A retrospective review wasundertaken of 31 consecutive patients whounderwent thoracic screw placement.Information abstracted from the medicalrecords included: age, sex, height, weight,spinal diagnosis, pre- and post-operativeneurologic status, complications, andoffice follow-up. All patients underwentCT imaging within 48 hours of surgeryand screw placement was assessed.Results are reported as mean ± standarddeviation.Results: Thirty-one consecutive patients(age 48.8 ± 20.5 years, 15 males & 16females, BMI 26.8 ± 8.7) with thoracicand/or thoracolumbar instabilityunderwent placement of percutaneous IPor EP screws between T2 and T12. Theunderlying spinal diagnoses includedtrauma (n = 21), infection (n = 2), cancer(n = 6), and disk herniation (n = 2). Twopatients required further surgery related tothe initial procedure for evacuation of anepidural hematoma (n = 1) anddebridement of a deep wound infection (n= 1). No patient required revision of theirspinal instrumentation. Of the 99 thoracicscrews placed 55.6% were IP and 44.4%were EP. Grading of screw placement wasfollows: IP: grade 1: 61.8%, grade 2:36.4%, and grade 3 1.8%, EP grade 1:63.6%, grade 2: 34.1%, and grade 3 2.3%.The two grade three screws both occurredat T4. One cancer patient developingincreased paraparesis two days aftersurgery but refused further intervention.At last follow-up (8.8 ± 7.6 months) nopatient had clinical or radiologic evidenceof instrumentation failure. Overalloutcomes at last follow-up appearedacceptable for the group including ODI(40.9 ± 21.4), Back VAS (4.1 ± 2.1), SF-12 PCS (34.0 ± 10.5), and SF-12 MCS(44.4 ± 9.0).Conclusion: Both IP and EP screw fixationcan be performed safely using apercutaneous approach to the thoracicspine.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 107
DIGITAL POSTER ABSTRACTS

438Nanosolutions for Spinal Cord Injury,How Far Have We Got?Mario Ganau, Lara Prisco, Francesco Lupidi, Laura Ganau, Roberto Spinelli, Roberto ForoniIntroduction:An estimated 10,000-12,000Spinal Cord Injuries [SCIs] occur everyyear in the US, and 1/4 of a millionAmericans are currently living with SCI.Accounts of SCI and their treatment dateback to ancient times, even though ourpatients have, nowadays as in the past,only little chances of recovery from such adevastating injury. Then, will it bepossible in the future to repair a damagedspinal cord? Probably the solution is onlya matter of research and development.Methods: Understanding the cellular andmolecular mechanisms involved in boththe working and the damaged spinal cordcould point the way to therapies thatmight: 1)prevent secondary damage,2)encourage axons to grow in injuredareas, and 3)reconnect vital neural circuitswithin the spinal cord and CNS. In thisreview we describe the nanotechnologicalresearch strategies pursued in this fieldand their groundbreaking advances todate.Results: Biosynthetic/biodegradableconduits carrying extracellular matrixmolecules or cell lines, and supplementedwith neurotrophic growth factors haveyielded encouraging results inexperimental SCI. Poly-ß-hydroxybutyrate conduits in combinationwith alginate and fibronectin provideneuroprotection for axotomizeddescending neurones. A poly(lactic-co-glycolic acid) scaffold seeded with neuralstem cells has been developed thatpromotes axonal regeneration across thegap. Single-walled carbon nanotubesfunctionalized with polyethylene glycolhave been shown to increase the length ofneurites in vitro, and axons in vivo,without increasing reactive gliosis inexperimental SCI. To recreate the optimalconditions for vehiculation of a stepforward is required, to this regardnanorobots could assist the body in thehealing process by transporting “all that isneeded” from and to the right places at theright time.Conclusion: This review offers a clearoverview concerning thenanotechnologically driven researchstrategies for SCI. The nanosolutionsherein described seem promising to coverthe existing gap between hope and reality.
439Pedicle Guide for Thoracic PedicleScrew PlacementKingsley O. Abode-Iyamah, Luke Stemper,Shane Rachman, Kelly Schneider, Kathryn Sick, Patrick W. HitchonIntroduction: The placement of thoracicpedicle screws is challenging requiringintra-operative imaging. While increasingaccuracy, these modalities increase intra-operative time, radiation to patient,surgeon, and cost. We have designed apedicle screw guide (PSG) for placementof thoracic pedicle screws to potentiallyprovide increased accuracy compared tofree hand screw placement.Methods: Two spines were imaged tomeasure the angle between the long axisof the pedicle and the sagittal plane fromT1-T12. The cortex at the junction of thetransverse process and the superior facetwas penetrated using an awl. The PSGwas used to make a 20 mm pilot hole intothe pedicle along the trajectory calculatedfrom the CT scans. On one side from T1-T12, pedicle screws were placed freehandbased on clinical experience. On the other,pedicle screws were placed using thePSG. After placement of the screws, CTscans were obtained and grading ofmedial violation was recorded. The degreeof violation was recorded for each pedicle(1: no violation, 2: <2mm violation, 3:>2mm violation).Results: Two specimens were used with atotal of 48 pedicles. Of the total 48-pedicle screw there were a total of 11pedicle violations. Of these violations, 3(12.5%) were with the use of PSG, all ofwhich were grade 2. There were 8violations (33%) with the free handtechnique. The percent error from the pre-instrumentation CT trajectory angle was62.3%(±39.5) and 34.3%(±23.3) (P =0.002) for freehand and guide assistedrespectively.Conclusion: Free hand placement ofthoracic pedicle screw challenging due tothe unique anatomy the thoracic spine.While intra-operative imaging techniqueincreases accuracy there is radiation riskto the surgeon. The use of the pedicleguide screw increases accuracy whiledecreasing the risk of radiation.
440Minimal Invasive VertebralAugmentation in Geriatric Patientswith High ComorbidityBasar Atalay, Mehmet Volkan Harput,Kaan Cumhur Yaltirik, Ozge Koner,Ayce AtalayIntroduction: Geriatric population is underrisk for highly morbidVertebralcompression fractures (VBC).The purpose is to determine, levelsinvolved, comorbid factors, and outcomeof treatment of VBC by vertebroplastyand kyphoplasty in geriatric age group.Methods:A total of 32 patients with anaverage age of 76,63 ± 9 years wereenrolled. Traumatic, pathologic orosteoporotic fractures were treated.Patients had undergone Vertebralaugmentation (VA) under sedo-analgesia.Visual analog scales (VAS), percent ofcompression, and Cobb’s were measured.Comorbidity index was calculated. Timeof mobilization post surgery, length ofhospital stay were evaluated.Results: In 68.8% osteoporoticfracture,18.7% pathological fracture, and12.5% traumatic fracture was identified.22 patients (68.8%) had single,10 (31.2%)had multiple level fractures. L1 was themost commonly involved level. 59.4% ofthe patients (n = 19) underwentvertebroplasty, 37.5% (n = 12)kyphoplasty and 3.1% (n = 1) were treatedby both vertebroplasty and kyphoplasty.Mean time of total anesthesia time was68.28 ± 25.05 minutes. 15 (46.9%)patients were immediately mobilisedwithin 12 hours. 17 (53.1%) patients weremobilised between 12 to 24 hours.Preoperative mean VAS was 72.58 ±12.64 postoperative mean VAS was 20.97± 18.14 (P = 0.0001) Preoperative Cobbangle of the compressed segment was9.51 ± 6.57 and the post operative cobbangle was 7.64 ± 5.89 (P = 0.209).Preoperative compression ratio revealed20,55 ± 19,96 % and postoperativecompression ratio was 15.44 ± 17.05 % (P= 0.109). Mean length of stay in thehospital was 1.32 ± 0.67 day. Meanfollow-up time was 18.04 ± 11.69 months.Charlson comorbidity score was 3.06 ±1.8. Mean VAS difference betweenpatients with high and low comorbiditywas similar between groups (P = 0.38).Conclusion:Vertebroplasty andkyphoplasty can be safely done in thegeriatric patient group with multiplecomorbid factors. Even patients with highcomorbidity scores can benefit from theseprocedures. VA procedure is a minimally
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES108
DIGITAL POSTER ABSTRACTS

invase technique and can be performedunder sedoanalgesia combined with localanesthetic infiltration which enables earlymobilization and a short hospital stay.
441Direct Lateral vs. TranspedicularCorpectomy for Spinal MetastasisEmam Saleh, Tsz Lau, Timothy Miller,Frank D. Vrionis, Nam Duy TranIntroduction: Primary or metastasic spinaltumors can cause pain and neurologicdeficit due to spinal instability, spinalmisalignment and/or compression ofneural elements. Surgical management ofvertebral body tumors may includeposterior transpedicular or direct lateral(retropleural or retroperitoneal)approaches. Lateral approaches providedirect access to the anterior or middlecolumns for decompression and/orreconstruction without disruption of theposterior elements. The purpose of thisstudy is to compare the clinical outcomesbetween lateral or posterior approachesfor thoracic and lumbar corpectomy in thecancer population.Methods: Retrospective chart review on 33consecutive patients who had undergonethoracic or lumbar (T5-L4) corpectomyplus instrumentation using expandablecage at our institution between January2010 and August 2011. All patients hadeither primary or metastasis diseasecausing intractable pain, neurologicaldeficits, and/or instability. Patientdemographics, surgical blood loss,surgical duration, complications, length ofhospital stay and functional outcome wereanalyzed.Results: 19 patients underwent a directlateral retropleural or retroperitonealapproaches while 14 patients underwent aposterior transpedicular approach forthoracic or lumbar corpectomy. Theaverage blood loss was 350cc per level forlateral approaches and 660cc per level forposterior approach. The average surgeryduration was 3 hours for lateralapproaches and 3.6 hours for posteriorapproaches. The average length ofhospital stay was shorter for patients thathad undergone lateral approaches (5 vs. 7days). There were no neurologicalcomplications for both groups. Allpatients had improvements in theirfunctional outcomeConclusion: Direct lateral approaches formidthoracic to lumbar spinal malignancyare safe with low complication rates.Intraoperative blood loss, surgicalduration per level and length of hospital
stay are favorable when compared toposterior transpedicular approaches. Forselected patients with anterior and/ormiddle column malignancy, lateralapproach is a feasible option.
442Participant Satisfaction withSimulation of Minimally InvasiveSpine Surgery Using Virtual Realityand HapticsBen Z. Roitberg, P. Pat Banerjee, Christian Luciano, Silvio Rizzi, Ali Alaraj,Sameer Ansari, Prashant Chittiboina,Anand Germanwalla, Leonard I. KranzlerIntroduction: The purpose of this studywas to evaluate participant satisfactionwhile performing a percutaneous spinalprocedure on a head- and hand-trackedhigh-resolution and high-performancevirtual reality and haptic technologyworkstation. We also aim to collect dataon performance and accuracy.Methods: 134 neurosurgery fellows andresidents trained on an ImmersiveTouchsystem (63 on Thoracic 9,10 and 11 and71 on Lumbar 2,3 and 4 virtual models).A virtual Jamshidi needle waspercutaneously inserted into a virtualpatient’s pedicle derived from a computedtomography data set. An entry point onbone surface and a target point withinbone were predetermined by a spineneurosurgeon. Participants were allowedup to five minutes of practice attempts.They were then asked to repeat what theypracticed. Accuracy (average Euclideandistance from predefined entry and targetpoints) was measured for each insertion.Every participant was requested to fill ananonymous form asking whether theywere satisfied with the realism of thesimulation, and if not explain why.Results: 108/134 participants filled thefeedback form, 105 were satisfied and 3were dissatisfied with the realism of thesimulation experience. Those dissatisfiedcited inability to see the image in 3D.There were 268 measured attempts toinsert the virtual needle, 248 successful,and 20 breached bone, 9 out of 126(7.14%) failed in the thoracic group, and11/142 (7.5%) failed in the lumbar group(NS). Mean accuracy score of successfulattempts was 13.83 mm (SD 6.74 mm).Conclusion: Satisfaction with the realismof the simulation is high. We plan a moredetailed questionnaire in future studies.The accuracy of pedicle needle placementachieved by participants using thesimulator is comparable to that reported in recent literature1, further evidence of
simulation realism.
443Characterizing Spine Injuries inRollover CrashesBabak Cohen, Dale Halloway, Waqar Malik, Narayan Yoganandan, Frank A. Pintar, Dennis J. MaimanIntroduction: Rollovers are less than threepercent of motor vehicle crashes, yetaccount for more than 28% of fatalcrashes with more than 10,000 deathsannually. Spine and head injuries are stillthe most prevalent in rollovers. This studyintended to identify the most frequentspine injuries during rollover crashes todelineate patterns associated with certainscenarios.Methods: The US-DOT-NHTSA CrashInjury Research and Engineering Network(CIREN) database was used to studysingle vehicle rollover crashes involvingfront occupant adults. CIREN containsdetailed documentation of both medicaland engineering data for each crash.Arrested rolls or ejected occupants wereexcluded. Variables included gender, BMI,vehicle type, occupant seating position,number of quarter turns, side-slip angle,seatbelt usage, and airbag deployment.The criterion provided 38 cases, 30 hadinjuries between C1 and T2.Results: In both passenger cars and SUVsthe occupant on the far side of the roll hada higher incidence and severity of injuriesthan the near side occupant (17 vs 13).Facet fractures were the most commoninjury type and twice as common in farsided crashes and in cars compared toSUVs. Vertebral lamina fractures wereevenly distributed among occupants, butwere more common in SUVs. Vertebralpedicle fractures were more frequent innear side occupants. Most fractures in theC4 and lower vertebrae were facetfractures, while above C4 were mostlyvertebral body fractures. There was nosignificant correlation between vertebralfractures, surgeries, MAIS scores, side-slip angles, and number of quarter turns.Conclusion: The location of the occupantin the vehicle, type of vehicle, and angleof the roll seem to have significantinfluence on the severity and location ofspine injury in a rollover crash. This studyreinforces the concept that occupantposition with respect to the type of rollinduces differing mechanisms of spineinjury.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 109
DIGITAL POSTER ABSTRACTS

444Parieto-occipito-cervicalInstrumentation and Fusion of aPatient with an Unstable Cranio-cervical Junction After Both aPosterior Fossa Craniectomy andLeft Transcondylar CraniotomyAmandip Singh Gill, Joseph Chia Yu Hsieh,Abhishek Chaturbedi, Daniel S. Yanni,Mark E. Linskey, J. Patrick Johnson, Samer GhostineIntroduction: Skull base surgeries forresection of complexe tumors emphasizebone drilling to minimize brain retraction.Trans-condylar approaches to resectventral foramen meningioma is welldescribed, and is notorious fordestabilizing the cranio-cervical junction.Methods:A 46-year old man with ahistory of a suboccipital craniectomy atage 12 for a posterior fossa astrocytomaresection followed by chemo and radiationtherapy presented to our multi-disciplinarycomplex spine center with severemyelopathy. MRI of his brain revealed alarge 4.4 x 4.3 cm ventral foramenmagnum meningioma extending to the leftjugular tubercle and occipital condyle andinferiorly to C2. The approachnecessitated drilling of greater than 80%of the condyle to properly visualize andresect the tumor.Results:A custom plate-rod system wassecured to the pariental bone via 4bicortical screws. Because of priorradiation to the posterior fossa resulting inatrophy of subcutaneous tissue, the rodswere fashioned closely to the boneintraoperatively over the occipital andmastoid convexities and attached to thebicortical cervical screws.Conclusion:We present a unique techniqueto stabilize the cranio-cervical junction inthe setting of absence of occipital boneand cranio-atlantal instability.
445Minimally Invasive Robotic GuidedPercutaneous Lumbar SpineStabilization and Fusion forTraumatic Lumbar Chance FracturesDaniel S. Yanni, Amandip Singh GillIntroduction:Modern treatment of Chancefractures has entailed open pedicle screwfixation and fusion for instability. Externalbracing required many months of bed-restand strict physical limitations. Recently,percutaneous pedicle screw stabilizationhas allowed for internal bracing, butrequire removal after healing occurred.We present a minimally invasivestabilization and fusion to treat Chance
fractures.Methods:A 22-year-old male status postmotor vehicle collision presented withmultiple solid organ injuries and Chancefractures of both L2 and L3 withligamentous injury at both levels. He wasneurologically intact with severe backpain. Given his active lifestyle andligamentous injury, decision was made toproceed with stabilization and fusion.Results:We chose a minimally-invasiveapproach both for the faster recovery timeas well as the decreased risk of bleeding inthe face of a liver laceration. The Mazorrobot assisted in placing screw trajectoriesacross the fractured pedicles at bothlevels, allowing for precise placement ofhardware. Screws were then compressedto close the fracture gap. A percutaneousfacet/transverse-process reaming devicewas next used to decorticate boneposterolaterally and a funnel-device wasused to spread allograft posterolaterally topromote arthrodesis. The patient wasambulating within 24 hours and wasdischarged within 48 hours. At 6 monthspost-op, patient remains neurologicallyintact without back pain and has returnedto work.Conclusion:We present a technique andcase illustration using robotic guidance forminimally-invasive percutaneousstabilization and fusion of the lumbarspine in the setting of 2 adjacent chancefractures. Such fusions have traditionallybeen accomplished via large openprocedures, bringing with themcommensurate risk and complication.Image-guided percutaneous techniquesoffer the option for internal bracing andfusion with small risk and recovery times.Robotic guidance allows for placement ofscrews accurately through the fracturedsegments.
446Factors That Predict Hospital andSurgical Costs and Recovery Ratesfor Lumbar LaminectomySandya Venugopal, Patricia Zadnik,Camilo A. Molina, Mari L. Groves, Ali Bydon, Ziya L. Gokaslan, Jean-Paul Wolinsky, Timothy F. Witham,Daniel M. SciubbaIntroduction: In the current economicclimate with intense focus on reducinghealthcare costs, a common assumptionamong policy-makers is that surgeons’professional fees form a large proportionof expenditures. Our previous work hasshown that surgeons’ reimbursement issignificantly lower than hospital’s for
lumbar laminectomy. Here we present thepredictors of hospital and surgical costsfor the same cohort of patients.Methods: In this retrospective analysis of76 patients (44 male/32 female) thatunderwent non-instrumented lumbarlaminectomy during 2009-2010 weperformed multiple linear regressionanalyses to look for factors that mightcontribute to the discrepancy in the ratesof cost recovery between the hospital andthe surgeons. We regressed HospitalCost/Collection, Surgeons’ Bill/Collection, as well as Hospital andSurgeons’ Collection Rates (percentage ofcollection to cost) against gender, race,age, laminectomy levels, length ofhospital stay, operating surgeon, type ofinsurance as well as patient co-morbidities.Results: Regardless of insurancestratification, and despite eliminatingpatients with 100% (n = 5) and 0% (n = 5)surgical collection rates, the predictorsremained the same. The most commonpredictor for hospital cost and collectionwas patient length of stay and postoperative complications/comorbities (P <0.001). The biggest predictor for surgeonbilling and collection was the levels oflaminectomy performed (0.004 < P <0.04).Conclusion: The majority of health carecosts associated with the acute stay forlumbar laminectomy are associated withhospital reimbursement as opposed tosurgeon reimbursement. Factorsassociated with higher hospital costsinclude length of stay and postoperativecomplications/comorbidities whilesurgeon costs are associated with size ofsurgery. Evaluation of such cost driversmay improve strategies for increasingefficiency of spine care delivery in theacute setting.
447Spontaneous Regression of LumbarHerniated Disc: Two Case Reportsand Review of the LiteratureKee Duk Kim, Eric S. KimIntroduction: The spontaneous regressionof lumbar disc herniations is a well-documented phenomenon. However, theexact mechanism is still unknown. WithMRI, the size of herniated disc materialmay be determined and the tear in theannulus fibrosis classified. Furthermore,immunophenotypic studies have alsodemonstrated regression by means ofphagocytosis involving angiogenesis.Formation of granulation tissue and
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES110
DIGITAL POSTER ABSTRACTS

vascularization are believed to exhibitperipheral enhancement of herniated discsusing Gd-enhanced MRI. We report twocases of spontaneous regression of lumbarherniated disc and characterize factors thatare favorable for disc regression.Methods:A literature search wasperformed for case reports of lumbarherniated disc regression as well as relatedimaging and immunohistologic studies.Case reports, including two of our own,were analyzed retrospectively for factorsassociated with regression.Results: Rim enhancement was thestrongest positive indicator for a faster rateof resorption [1] while the extent ofnucleus pulposus migration predicted thedegree of resorption[2]. An extruded-typeresulted in regression in almost all cases in100% of cases reviewed by Splendiani etal[3]. Breach of the posterior longitudinalligament induces an immune responseleading to chemokine action anddehydration. Contrastingly, smaller discbulges in which the annulus fibrosus wasintact did not undergo substantialregression.Conclusion: Given that cauda equinasyndrome and motor weakness are absent,conservative treatment may be favorablefor patients presenting with sequestered-or migrated-type disc herniations. Whilethe rate of regression is not yetpredictable, MR imaging is still valuablein classifying the nature of a discherniation and may aid in decision forsurgery.
448Readability of Patient EducationMaterials for Peripheral NeuropathyDavid R. Hansberry, Nitin Agarwal, Robert F. HearyIntroduction: Given the increase in theincidence of diseases, in particulardiabetes, causing peripheral neuropathy, agreater number of people are expected toutilize healthcare oriented patienteducation materials relevant to this diseaseof the peripheral nervous system. Formany, online resources have become aprimary source for information. However,often times online resources inadequatelyconvey essential information, since thelanguage is written above the seventhgrade that the average American cannotunderstand.Methods:We reviewed the U.S. NationalLibrary of Medicine, the National Instituteof Neurological Disorders and Stroke,Neuropathy.org and the Mayo Clinicwebsites to determine their readability on
peripheral neuropathy. All bullet pointsand unnecessary headings were removedfrom the documents and evaluated inMicrosoft Office Word using the FleschReading Ease and Flesch-Kincaid GradeLevel to determine their readability.Results: The Flesch Reading Ease scoresaveraged 40.2 with only the U.S. NationalLibrary of Medicine scoring above 50(76.5). The Flesch-Kincaid Grade Levelscores averaged 11.3. All scores wereabove a ninth grade level except the U.S.National Library of Medicine, which hada score of a fifth grade reading level.Conclusion: Our results indicate that theaverage American would benefit fromreading only the U.S. National Library ofMedicine while most would struggle tofully comprehend the other websites. TheNational Institute of NeurologicalDisorders and Stroke, Neuropathy.org andthe Mayo Clinic websites use languagethat is clearly higher than therecommended level.
449Readability of Patient EducationMaterials for the Secondary DamageFollowing Spinal Cord InjuryNitin Agarwal, David R. Hansberry, Robert F. HearyIntroduction: The use of online materialsby healthcare consumers to accessmedical information presents uniquechallenges. Most Americans have accessto the Internet and frequently turn to it as afirst-line resource. Therefore it isimperative that this information be writtenat a level that the average American canunderstand, which is about a seventhgrade reading level.Methods: The readability of online patienteducation materials was evaluated.Materials provided by the NationalInstitute of Health (NIH) and, inparticular, the National Institute ofNeurological Disorders and Stroke(NINDS) were assessed using the FleschReading Ease and Flesch-Kincaid GradeLevel evaluations with Microsoft OfficeWord software. Unnecessary formattingwas removed and the readability wasevaluated with the Spelling and Grammarfunction.Results: The average Flesch-KincaidGrade Level was 13.6 with no sectionlower than 12.8, indicating that mostAmericans would not be able to fullycomprehend this material. Additionally,the Flesch Reading Ease had an averagevalue of 31.5, a number that also suggestthis language is too complex for the
average American.Conclusion: Results indicate that thelanguage used on materials provided bythe NIH and NINDS are perhaps tooadvanced for the average American.Website revisions might be beneficial forimproved patient education and ultimatelyclinical results.
450Hospital and Surgeon Variation inComplications and Repeat SurgeryFollowing Incident Lumbar Fusionfor Common DegenerativeDiagnosesBrook I. MartinIntroduction: To identify factors thataccount for variation in complication andreoperation rates across hospitals andsurgeons performing lumbar spinal fusionsurgery.Methods: Discharge registry including allnon-federal hospitals in Washington Statefrom 2004-2007. We identified adults (n =5,864) undergoing an initial inpatientlumbar fusion surgery for degenerativeconditions without significantcomorbidity. We identified whether or noteach patient had a subsequent spineoperation or complication within 90 days.Controlling for patient characteristics andcomorbidity, a generalized logisticregression model with hospital andsurgeon random-effects was used toexamine the rates of complications andreoperation.Results: Complications within 90 days ofan initial fusion occurred in 4.8% ofpatients, and 2.2% had a reoperation.Surgeon effects account for 45% of thevariation in hospital complication rates,and 75% of the variation in reoperationrates. Operative features accounted for37% and 19% of the variation insurgeons’ complication and reoperationrates, respectively.Conclusion: To improve the safety oflumbar spinal fusion surgery, qualityimprovement efforts that focus onsurgeons, including their discretionary useof operative features, may be moreimportant than those that target hospitals.
MARCH 7-10, 2012 WALT DISNEY WORLD SWAN AND DOLPHIN, ORLANDO, FLORIDA 111
DIGITAL POSTER ABSTRACTS
AANS/CNS SECTION ON DISORDERS OF THE SPINE AND PERIPHERAL NERVES112
The AANS/CNS Section on Disorders of the Spineand Peripheral Nerves gratefully acknowledges
for providing an educational grant in support ofthe 2012 Annual Meeting.
RESIDENT EDUCATION PARTNER
Mobile Meeting GuideUse the Mobile Meeting Guide to search for meeting rooms, sessions, faculty members,exhibit booths, abstracts and more. This supplement to the Scientific Program book allowsyou to conveniently access all the 2012 Annual Meeting offers – right from yourSmartphone or laptop! Log on to http://m.cns.org to access this resource today!
� See who is registered
� Locate meetings and courses
� Browse abstracts and digital posters
� Find out what is happening right now
� And more!
CNS1132_12DSPN_ScientificProgram_Interior_1 2/21/12 6:46 PM Page 112

PROGRAM AT-A-GLANCE
WEDNESDAYMARCH 7, 2012
8:00 AM – 6:00 PMRegistrationNorthern Hemisphere Foyer
1:30 – 5:30 PMPediatric CraniocervicalSociety Meeting Oceanic 1
Special Course I – Neurosurgical Spine:Business and CompensationNorthern Hemisphere A1
Special Course II – Cases and Complications with the MastersNorthern Hemisphere A2
Special Course III – SpinalDeformityNorthern Hemisphere A3
Special Course IV – AdvancedMIS Techniques/ManagingMIS ComplicationsAmericas Seminar
Special Course V –Management of PerioperativePain, PerioperativeComplicationsAsia 3
Special Course VI – Brazil:Spine Surgery in Brazil – in conjunction with the Spine Section of BrazilianNeurosurgical AssociationAsia 4
Special Course VII – Updateson Spine Trauma, Spinal CordInjury, and Cervical SpineTrauma GuidelinesNorthern Hemisphere A4
6:00 – 8:00 PMOpening ReceptionCabana Deck at the Pool
THURSDAYMARCH 8, 2012
6:00 AM – 6:00 PMRegistrationNorthern Hemisphere Foyer
6:30 – 6:55 AMContinental BreakfastSouthern Hemisphere Foyer
Case PresentationsSouthern Hemisphere I-III
7:00 – 9:30 AMScientific Session ISouthern Hemisphere I-III
9:00 AM – 7:00 PMExhibit Hall and PosterViewingNorthern Hemisphere B-E
9:30 – 10:15 AMBeverage Break and What’s New Session INorthern Hemisphere B-E
10:15 AM – 12:30 PMOral PlatformPresentations ISouthern Hemisphere I-III
12:30 – 1:25 PMLunch and What’s NewSession IINorthern Hemisphere B-E
1:30 – 3:00 PMScientific Session II David Cahill MemorialControversies I: In-DepthDebatesSouthern Hemisphere I-III
3:00 – 3:45 PMBeverage Break and What’s New Session IIINorthern Hemisphere B-E
3:45 – 5:15 PMOral Poster Presentations I & IISouthern Hemisphere I-III andAmericas Seminar
5:15 – 6:45 PMReception in the Exhibit HallNorthern Hemisphere B-E
FRIDAYMARCH 9, 2012
6:00 AM – 5:00 PMRegistrationNorthern Hemisphere Foyer
6:30 – 6:55 AMContinental BreakfastSouthern Hemisphere Foyer Case PresentationsSouthern Hemisphere I-III7:00 – 9:00 AMScientific Session IIISouthern Hemisphere I-III9:00 – 9:20 AMMayfield AwardsSouthern Hemisphere I-III9:00 AM – 2:00 PMExhibit Hall and PosterViewingNorthern Hemisphere B-E9:30 – 10:15 AMBeverage Break and What’s New Session IVNorthern Hemisphere B-E10:15 AM – 12:15 PMOral PlatformPresentations IISouthern Hemisphere I-III12:15 – 12:30 PMAnnual Business MeetingSouthern Hemisphere I-III12:30 – 1:25 PMLunch in the Exhibit HallNorthern Hemisphere B-E12:30 – 2:30 PMLuncheon Symposium I –Revision Spine SurgeryNorthern Hemisphere A4Luncheon Symposium II –Spine TumorsNorthern Hemisphere A3Luncheon Symposium III –Cranial-Cervical JunctionNorthern Hemisphere A2Luncheon Symposium IV –Update of Lumbar SpineGuidelinesNorthern Hemisphere A1Luncheon Symposium V –Lateral RetroperitonealInterbody Fusion:Technique and OutcomesAmericas Seminar1:30 – 5:30 PMSpecial Course VIII –Peripheral Nerve Exposuresand Nerve RepairTechniquesAsia 3Special Course IX –AOSpine: Aging Spine Asia 4
SATURDAYMARCH 10, 2012
6:00 AM – 12:30 PMRegistrationNorthern Hemisphere Foyer
6:30 – 6:55 AMContinental BreakfastSouthern Hemisphere FoyerCase PresentationsSouthern Hemisphere I-III
7:00 – 8:20 AMScientific Session IV – OralPoster Presentations IIISouthern Hemisphere I-III
8:20 – 10:10 AMDavid Cahill MemorialControversies II: Spine and Peripheral NerveRapid FireSouthern Hemisphere I-III
10:10 – 10:40 AMBeverage Break Southern Hemisphere Foyer
10:40 – 11:00 AMFellowship and Clinical TrialAward UpdatesSouthern Hemisphere I-III
11:00 AM – 12:30 PMOral Posters Presentations IVSouthern Hemisphere I-III
to These Companies for Providingan Educational Grant in Supportof the 2012 Annual Meeting!
NEUROSURGICAL EDUCATION AMBASSADOR:
NEUROSURGICAL LEADERSHIP AMBASSADOR:
FUTURE OF NEUROSURGERY AMBASSADOR:
RESIDENT EDUCATION PARTNER:
ANNUAL MEETING SUPPORTERS:
as of February 10, 2012
SpecialThanks
TM
CNS11322_12DSPN_SP_Cover_Cover 2/22/12 2:00 AM Page 2
Save the Date!
2013 ANNUAL MEETING OF
THE AANS/CNS SECTION ONDISORDERS OF THE SPINE AND
PERIPHERAL NERVES
March 6 - 9, 2013JW Marriott Desert Ridge
Phoenix, Arizona
Abstract Center Opens May 16, 2012
28th Annual Meeting of the AANS/CNS Section on Disorders of the Spine and Peripheral NervesSpine and Nerve Surgery in the Era ofExcellence: Will You Measure Up?
Scientific Program
March 7-10, 2012Walt Disney World Swan and Dolphin
Orlando, Florida
We Welcome the Spine Section of the Brazilian Neurosurgical Association –2012 International Society
28thA
nnual Meeting of the A
ANS/CN
S Section on Disorders of the Spine and Peripheral N
erves SCIEN
TIFIC PROGRA
M