Embed Size (px)
Citation preview

250
started. Due to the extended half I fe of fluoxetlne and its active metabohte norfluoxetine, that washout may take weeks to even a couple of months For this reason, clinicants may wish to give smaller doses of nefazodone when starting nefazodone before fluoxetine has completely washed ou t This issue is a common problem when switching from fluoxetine to other drugs due to the extended half-life and its propensity for causing drug-drug interactions.
In contrast to fluoxetlne and paroxettne, nefazodone does not inhibit the P450 enzyme, CYP 2D6. However, it does inhibit the P450 enzyme CYP 3A3/4, as does the SSRI, f luvoxamme, and to a lesser extent, the SSRI, f luoxet ine Due to the shorter half-life of nefazodone, thereis no prolonged carryover of the effect on this enzyme unlike the case wtth f luoxet ine Armed with this knowledge, the physician can anticipate the potential for specific types of pharmacokinetlc drug-drug interactions and make appropnate dose adjustments to avoid adverse consequences
Nefazodone is also metabolized by CYP 3A3/4. Analogous to the situation with paroxetine and fiuoxetine, th~s fact explatns why nefazoaone shows nonlinear pharmacokinetics ( i e . its inhibits the P450 enzyme which is responsible for its metabol ism]
Nefazodone represents a antidepressant option which is distinct from other classes, It has clinically meaningful advantages over its earlier prede- cessor, trazodone, while preserving many of the features of that drug w h c h clinicians found desirable. Ongoing research and the increase in clinical experience m clinical practice wil! further define its role as an potion in the treatment of patients with major oepresston.
SAT-2-3 j Modern approach in the treatment of anxiety ]
associated with depression M.B. Keller. Brown Umversl~ Oepartment Psychiatry and Human Behavior, 345 B/ackstone Bfvd, Providence, R/, USA
Depressive and anxiety disorders are illnesses which have a high hfetlme prevalence, 8% and 15% respectively (Regier et al, 1988). Un~polar de- pression has a 6% lifetime prevalence while the prevalence rate for all depressive disorders is between 8% to 10% at a minimum. Each of these disorders have also been found to have a high rate of chronic~ty anti re- currence. It has become increasingly apparent over the past decade that within episodes of depression, anx~etysymptoms often exist Whether or net this phenomenon tndicates two separate, but comorbid illnesses or if the presence of anxiety symptoms is part of the course of depression is of particular significance for diagnosis and t reatment
This presentation will focus on the ~ssues of differential d~agnosis, includ- ing physical and emotional manifestations of the illness. The consequences of comorbid anxiety on depression can be very serious from social and phys ical disability to suicidal ideation and behavior. Anxtetv has been found to be a predictor of suicide in depressed patients and since anxiety symptoms respond to intervenbon, they can also serve as an indication of type ef treatment
Antidepressant should be used w~th anxiety or pamc symptoms when the depression is severe or recurrent, in studies compar,ng TCAs SSRIs and MAOIs, the latter two Nave been found to be more effective than TCAs, in treating depression with anxiety (Liebowitz et al. 1988; Davidson et al, 1987; Robinson etal , 1985; Quitkln et al, 1988: Stewart et al, 1993). Most importantly, it must be understood that comerbid depression and anxiety occurs more frequently than not, and the prognosis is worse than with either illness a lone
For over a decade research and ciincal oOservation have shown that patients with both depresston and anxiety have a significant likelihood of experiencing relapse, recurrence, chronicity, and residual "subsyndromar' symptoms between full-criteria episodes of illness. In addition, it has been found that there is considerable overlap of these two orewously considered distinct disorders Because successful treatment depends on the disor- der diagnosed, both the diagnosis and ~reatment of comorb~d anxiety and depression is crucial to the outcome
Regardless of which disorder came first or which may be seconoarytothe other, rt appears that patients exhibiting comorbid anxiety and depression are more significantly impaired than patients suffering from either illness alone (Clancy et al, 1978, Dealy et al, 1981, Van Valkenberg et al, 1984) Research shows that patients with major depression and coexisting panic disorder display more psychological and social impairment and have more anxiety and somatic problems (Lesser et al, 1988, Dube et al, 1985, Grun haus et al, 1986) These patients are also at higher nsk for suicide attempts (Johnson et al. 1990) The majority of patients with a depressive disorder also have anxiety symptoms and approximately one quarter of patients with an anxiety disorder have depresswe symptoms
SAT-2 New perspectives in the management of depression
The effects of nefazodone on sleep profiles in depression
R Armitage. Department of Psychiatry The University of Texas Southwestern Medica/ Center at Dal/as. TX,, USA
Major depressive disorders (MDDs) are associated with a variety of sleep disturbances that include insomnia, short latency to the first rapid eye movement (REM) period, decreased restorative, slow-wave sleep, multiple awakenings throughout the night, and increased light sleep. It is estimated that 90% of depressed inpattents suffer from sleep disturbance [1]. Patients with MDD also show a disruption in circadian (24 hour) and ultradian (90 minute) rhythms in sleep electroencephalograms (EEGs), nocturnal temper- ature and neuroendocrine function [2].
Most antidepressants, including tricyclics (TCAs} and selective serotonin reuptake inhibitors (SSRIs), act as potent REM sleep suppressors, increas- ing the latency to REM and decreasing the total amount of REM sleep. Several researchers have suggested that antidepressant efficacy is linked to REM sleep suppression [3-5], But, SSRIs, in particular fluoxetine, have been shown to increase arousals and fragment sleep about baseline levels m patients with MDD [6].
The sleep effects of nefazodone, a 5-HT 2 antagonist that also inhibits serotonin reuptake, differ from SS RIs and TCAs. Nefazodone improves sleep disturbance in patients with MDD, decreasing the number of arousals and like Stage 1 sleep. Nefazodone also has remarkably little effect on REM sleep. The improvement in sleep architecture has been reported in both open-trial studies and double-bind comparisons of nefazodone with fiu- oxetine [7] Data will be presented from several studies of the effects of nefazodone on sleep architecture in depression.
Results indicate that nefazedone is an efficacious antidepressant asso- ciated with significant improvement in both obiective and subjective sleep measures. These findings also suggest that the antidepressant efficacy of nefazodone is not tied to REM sleep suppression.
References II1 Kupfer, DJ.; Foster, G.E; Reid, L; Thompson, K.S; Weiss, B; EEG sleep changes as
predictors in depression Am. J PsychiatH, 1987; 133: 622426. 12] Armitage, R Microarchitectural findings m sleep EEG in depression: Diagnostic im-
plications Bio; Psychiatry 1995: 37: 72-84. 13] Vogel, GW Evidence for REM sleep depnvation as the mechanism of action of an-
tidepressant drugs Prog Neuropsychopharmacol Biol Psychiatry 1983; 7:343-349 14} Vogel, GW; Buffenstein, A.; Minter, K ; Hennessey, A; Drug effects on REM sleep
and on endogenous depression Neurosci Biobehav Rev 1990; 14:49-63 [5} Kupfer, D.J.; Spiker, D,G.; Cable, PA.; Ned, J.E; Ulrich, R ; Shaw, D.H. Sleep and treat-
ment prediction in endogenous depression Am J Psychiatry 1981; 138: 429-433. {6} Hendrickse, WA ; Roffwarg, HP; Grannemann, B.D.; Orsulak, RJ.: Armitage, R ;
Cain. JW: Battaglia, J; Dehus, J.R: Rush, AJ. The effects of fluoxetine on the polysomnogram of depressed outpatients A pilot study. Neuropsycho pharmacol- ogy 1994: 10(2): 85 9 t
[7] Armltage, R ; Rush, A.J; Trivedi, M.; Cain, J ; Roffwarg, HP The effects of nefa- zodone on sleep architechture in depression Neuropsychopharmacology 1994; 10: 123-127
I SAT-2-51 Sexual dysfunction and other tolerability In the management of depression
David Baldwin. Faculty of Medicine, University of Southampton, Southampton. UK.
Complaints of sexual dysfunction by patients taking psychotrophic medica- tion. But, before the reported adverse effect can be ascribed to a particular drug, many other causes of possible dysfunction have to be considered. A rage of factors require evaluation, including the features of the psychiatric disorder, the presence and intensity of any co-morbid psychiatric or physical illness, and the concomitant use of other drug treatments.
Psychotrophic drugs may have adverse effects on any part of the normal pattern and sequence of sexual response latrogenic sexual dysfunction may therefore include the reduction of sexual desire, the impairment or disturbance of physiological arousal, and the loss. delay or alteration of orgasm.
The adverse effects of psychotrophie drugs on sexual function may re- sult from a range of different pathophysioiogical mechanisms. Within the central nervous system, non-specific effects such as sedation may result in a general decrease in the level of sexual interest and activity, and specific effects on particular neurotransmitters may lead to circumscribed impair- ments of sexual arousal or function. Actions on neurotransmitters within the autonomic nervous system may also lead to altered pattern of sexual response. Furthermore, many drugs have direct or indirect effects on the regulation of hormonal activity,
SAT-3 Mechanism of action of venlafaxine." clinical and preclinical insights 251
The management of sexual dysfunction associated w,th psychotrop~c drugs should start with a detaded assessment of the reported adverse event and its possible causes, fol lowed by a range of treatment approaches, including psychological and behavioural strategies. Pharmacological ap- proaches include the partial or complete withdrawal of medication, substi- tution of the implicated drug with an alternative compound, and the use of adjunctive pharmacological t reatments
SAT-2-6 j S l e e p and n e u r o e n d o c r i n e prof i les in depress ion and mania
R Linkowski, J. Mendlewicz Department of Psychzato4, Free Umvers/ty of Brussels, Belgium
The study of neuroendocrine abnormaiities in malor mental ilqness such as the unipolar and bipolar affective syndromes, qas been the focus of interest in the past few years The neuroendocrme "window" into the brain has been considered as a fruitful and promising approach to the study of mental disorders, as suggested by studies of some neuroendocrine challenge tests in depression that demonstrated their potential use as a biological markers The modern approach to hormonal dynamics focuses on the c~rcadian and pulsatiLe profiles that truly represent physiological modulat ion
From the fundamental point of view, such studies performed using a frequent sampling interval over the 24-hour cycle aim to cladfy the control and significance of the temporal sleep and wake fluctuations of neuroen docrine system activities Furthermore. these 24-hour studies are extremelv important in evaluating the characteristics of the biological time-keeping m man and to test possible hypotheses about chronobiological disturbances in neuropsychiatric disorders. Twenty four heypersecretion of cortisol, d~ urnal hypersecretlon of growth hormone, and normal 24-hour levels pro lactin have been reported m careful ch'onooiologlcal studies of depressec patients, along with sleep recordings n addition, a nocturnal qulescePt period, and a subsequent increase toward the mormng maximum, have been consistently found ir" a subset of depressed patients suffering from endogenous depression. A~ter successful treatment w!th antidepressants most of these abnormalities (w~th the exception of those found in the prolactin study) tend to correct
The normalization of the timing of hormoPal secretion was accompanied by a correction of sleep abnormalities and m particular, a lengthening o ~ the REM latencies Normalization of corhaol secretion was associated w~th a decrease in the magnitude of episodic cortisoi pulses whereas normal ization of growth hormone secretion was due to a diminished number of secretory pulses In conclusion, a disorder o~ circadian time-keeping seems to characterize acute episodes of major endogenous depression in some patients This abnormality was well as the associated increases m the adrenocorticotropic and somatotropie actw~tles seems to be state-, rather than trait dependent
The simultaneous study of seep and secretory rhyth'~s of ACTH, cort~so~ prolactm and GH in patients with major endogenous depression has thus provided strong ewdence for the hypcthes~s that the circadian clock ~.~, phase-advanced in the acute oepressive state However, a study of a group of manic patients has indicated that abnormal circadian timing may also be observed in mania In contrast, in schizophren,a, we have shown that there is not alteration of the circadian coqtrol o~ neuroendocrine secretions bu: the elevation of prolactin secret~or associale(l with earl;, sleep is decreased
SAT-3 Mechanism of action of venlafaxine: clinical and preclinical insights
ISAT-3-11 Precl in ical /c l in ica l aspects of in teract ions be tween serotonin and norep inephr ine
R Blier. Neufobio/og~ca/Psychiatry Umt, McGdl Un/vers~ty, Morttrea/, Ouebec, Canada
Several antidepressant treatments enhance serotonin (5-HT) neurotransm,s sion, and it is generally accepted that these drugs exert their therapec.tic effect via this system This hypothes~s~s supported by two lines of climcal evidence: 1} all selective 5-HT reuptake inh~bitors (SSRIs), despite several being of different chemical famdles are effective ,n major depression, and 2) inhibition of 5-HT synthesis in depressed patients m remission fol low ing antidepressant drug treatment producesa relapse Thenorepinephrine (NE) system is also thought to be revolved in the antidepressant response, at least in the response obtained w,th certain drugs In particular, severai
tncyclic ant4depressant (TCA) drugs potently block the reuptake of NE. In addition, the ( - ) enantiomer of maprotiline, which is reactive on the NE transporter, ts not an antidepressant, whereas the (+) enantiomer potently blocks the NE transporter and is effective in major depression. Furthermore, Jong-term administration of TCA drugs in laboratory animals enhances the responsiveness of postsynaptic alpha-adrenergic receptors located in the bra~n regions involved in mediating some depressive symptoms.
There are two reports suggesting that a more robust and perhaps more rapid antidepressant effect occurs when combining an SSRI with a TCA selective for the NE reuptake process. This putatively more pronounced effect could result f rom a synergistic action on the 5-HT and the NE sys- t ems On the one hand, the SSRI enhances 5-HT neurotransmission by increasing the efficacy of 5-HT terminals, as a result of a desensitization of cell oody and terminal 5-HT autoreceptors which normally exert a neg- ative feedback role on 5-HT neurons. On the other hand, the NE reuptake inhibitor would enhance NE neurotransmission by augmenting NE release. indeed, it was documented in our laboratory that long-term administra- tion of desipramme increases NE release even fol lowing elimination of this TCA Considenng that, for neurons in several brain regions, the effect of mlcrolontophoretically applied 5-HT and NE is the same on firing activity, an enhancement of both 5-HT and NE release could produce a synergistic effect on such target neurons.
Venlafaxine is a novel antidepressant drug which is a potent 5-HT reuptake b ccker that also inhibits the NE reuptake process, Its 5-HT/NE potency ratio , sabou t4 to 1 t can thus be speculated that. at doses m the upper recom- mended range, venlafaxine mimics the pharmacological condition obtained when giving an SSRI with an NE reuptake blocker such as desipramine. This could account for the putatively faster onset of action of venlafaxine when ~t ~s rapidly titrated up to its maximal recommended dose, This possible dual effect of venlafaxine on the 5-HT and NE reuptake processes could also account for its therapeutic effect in SSRI-resistant depressed patients. Stud,es are ongoing in our research unit to address these issues.
i SAT-3-21 P h a r m a c o t h e r a p e u t i c prof i le of ven la fax ine
S H Preskorn Department of Psychiatry and BehavioralSciences, Umvers/ty of Kansas School of Medicine, Wichita, Kansas, USA
The factors that must be considered when selecting an antidepressant can be summar zed by STEPS: Safety, Tolerability, Efficacy, Payment {eg, cost-effectweness) and -simphcitly of use. Efficacy includes overall efficacy, unique spectrum of activity, rate of onset of action, and efficacy as mainte- nance and prophylactic treatment. Safety and tolerability include short- and ong-term safety and pharmacokinetlcs and pharmacodynamic interactions.
Sm-p iclty of use refers to the convenience of the dosage regimen, need for dosage titration, and necessity for therapeutic drug monitoring.
Venlafaxme is a member of a new class of antidepressants called serotonm-noradrenahne reuptake inhibitor (SNRI). Drugs m the SNRI class nhlbtt the neuronal uptake of serotonm and noradrenaline, but are struc-
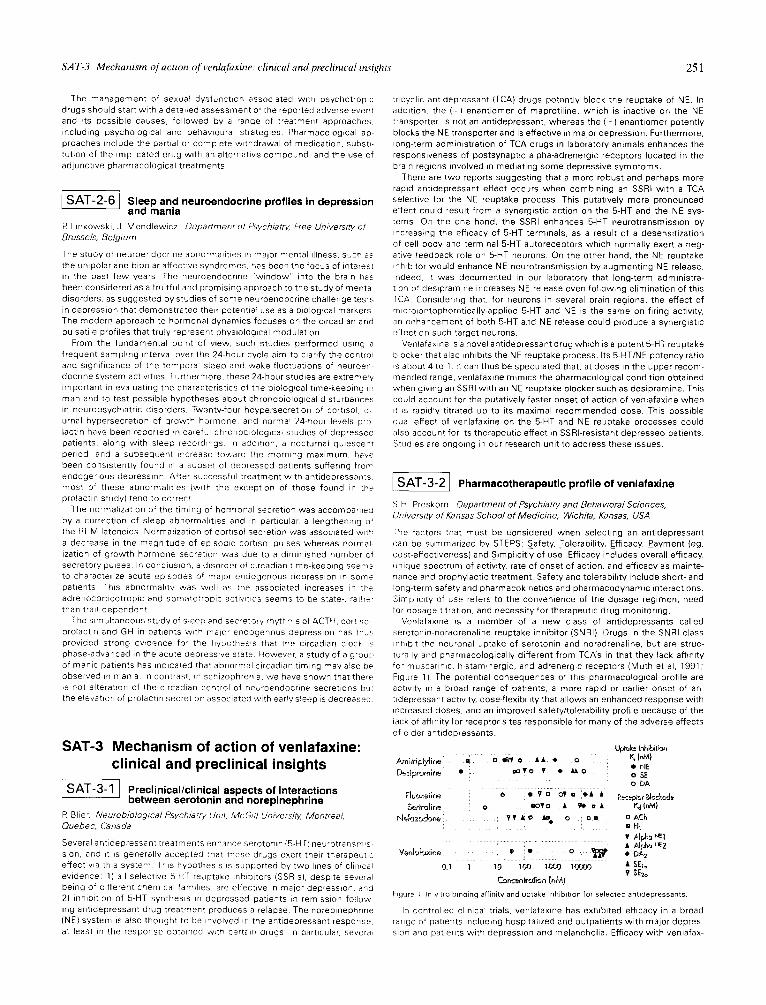
tura ly and pharmacologically different from TCA's in that they lack affinity formuscanmc hlstammergic, andadrenergrcreceptors(Muth etal , 1991; Figure 1) The potential consequences of this pharmacological profile are actwity m a broad range of patients, a more rapid or earlier onset of an- tidepressant act wry, dose-flexibi ity that allows an enhanced response with increased doses, and an improved safety/tolerabil ty profile because of the iack of affinity for receptor s~tes responsible for many of the adverse effects of o der antidepressants.
t~.#u~ Inhi~i,-~l ~1n;tnp~y~irle i [ ] ~ ' e • • • o K.i (r~}
• i'lE ~)~-~ premlrne • ~ • 0 ¥ • ~ 0 0 SE
ODA
-,~erir,3~ir,e o I o f o • ~ = • tt~ (r~} N.,~Jz~dore_ • • &o ~ o []= []ACh
la H t .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . • p-],,~,= ~
Ver,k.;ksxi,-;e • • o ~ . ~ • OAt
0.1 1 ' 1 0 ........ lt~'JJ lt.~0 lOOf3tj • SE]o v $Ezo
Cor,__-~tro~bn (~,M)
F gure I n v,tro b,na~ng affinity and uptake nhlbUlon for selected antidepressants.
h contro lee cl n ca1 trials, venlafaxine has exhibited efficacy in a broad range of patents nc ludmghospi tahzedandoutpat tentswkthmajordepres- s~on a,-d patients w~th depression and melancholia. Efficacy with venlafax-