-
7/29/2019 SAS Clinical Trails Phase-I
1/70
Design and Analysis of Phase IClinical Trials in Cancer
Therapy
Alex A. AdjeiKatherine Anne Gioia Chair in Cancer
MedicineRoswell Park Cancer InstituteBuffalo, NY
-
7/29/2019 SAS Clinical Trails Phase-I
2/70
Definition
First evaluation of a new cancer therapy inhumans
First-in-human single agent study
Combination of novel agents
Combination novel agent and approved agent
Combination of approved standard agents ?(pilot study ?)
Combination of novel agent and radiationtherapy
Eligible patients usually have refractorysolid tumors of any
type
-
7/29/2019 SAS Clinical Trails Phase-I
3/70
Conventional eligibility criteria- examples:
Advanced solid tumors unresponsive to standardtherapies or for
which there is no known effective
treatment
Performance status (e.g. ECOG 0 or 1)
Adequate organ functions (e.g. ANC, platelets,
Creatinine, AST/ALT, bilirubin)
Specification about prior therapy allowed
Specification about time interval between prior therapy
and initiation of study treatment
No serious uncontrolled medical disorder or active
infection
Phase I Patient Population
-
7/29/2019 SAS Clinical Trails Phase-I
4/70
Agent-specific eligibility criteria - examples:
Restriction to certain patient populationsmust havestrong
scientific rationale
Specific organ functions:
For examplecardiac function restrictions (e.g. QTc <
450-470ms, LVEF > 45%, etc) if preclinical data or prior
clinical data
of similar agents suggest cardiac risks
For exampleno recent (6-12 months) history of acute
MI/unstable angina, cerebrovascular events, venous
thromboembolism; no uncontrolled hypertension; no
significant
proteinuria, for antiangiogenic agents
Prohibited medications if significant risk of interaction
with study drug
Phase I Patient Population
-
7/29/2019 SAS Clinical Trails Phase-I
5/70
A New Agent Merits Clinical Study if
It is biologically plausible that the agent may
have activity in cancer (target seems valid and
agent affects it)
There is reason to expect benefit for patients(preclinical or
other evidence of efficacy)
There is reasonable expectation of safety
(toxicology)
Sufficient data on which to base starting dose
Hirschfeld S, 2004
-
7/29/2019 SAS Clinical Trails Phase-I
6/70
The 3 Basic Tenets Of Phase I Studies
Define a recommended dose : SAFELY (minimum # of serious
toxicities)
EFFICIENTLY (smallest possible # of pts) RELIABLY (high
statistical confidence)
SAFETY TRUMPS EVERYTHINGELSE
-
7/29/2019 SAS Clinical Trails Phase-I
7/70
-
7/29/2019 SAS Clinical Trails Phase-I
8/70
-
7/29/2019 SAS Clinical Trails Phase-I
9/70
At what dose do you start ?
-
7/29/2019 SAS Clinical Trails Phase-I
10/70
Typically a rodent (mouse or rat) and non-rodent(dog or
non-human primate) species
Reality of animal organ specific toxicitiesvery few
predict for human toxicity Myelosuppression and gastrointestinal
toxicity
more predictable
Hepatic and renal toxicitieslarge false positive
Toxicologic parameters
LD10lethal dose in 10% of animals
TDL (toxic dose low)lowest dose that causesany toxicity in
animals
Preclinical Toxicology
-
7/29/2019 SAS Clinical Trails Phase-I
11/70
Phase I Trials : Starting Dose
1/10th of the LD10 in rodents,or
1/3rd of the minimal toxic dose in
large animalsExpressed as mg/m2
These have historically been safedoses
-
7/29/2019 SAS Clinical Trails Phase-I
12/70
Equivalent Surface Area DosageConversion Factors
MOUSE20g
RAT150 g
MONKEY3.0 kg
DOG8 kg
MAN60 kg
Mouse 1 1/6 1/12Rat 2 1 1/7Monkey 4 2 1 3/5 1/3Dog 6 4 5/3 1 Man
12 7 3 2 1
Freireich EJ, et al, Cancer Chemother Rep 50:219-244, 1966
-
7/29/2019 SAS Clinical Trails Phase-I
13/70
What are the endpoints
/ objectives ?
-
7/29/2019 SAS Clinical Trails Phase-I
14/70
Phase I Study Endpoints
Dose, toxicity, pharmacology (efficacy ? )
Classical goals
Identify dose-limiting toxicities (DLTs)Identify the maximally
tolerated dose
(MTD)
Assess pharmacokinetics (drug metabolismand clearance)
Evaluate target modulation
-
7/29/2019 SAS Clinical Trails Phase-I
15/70
Defining Toxicities :NCI Common Toxicity Criteria
Grade 1 = mild
Grade 2 = moderateGrade 3 = severe
Grade 4 = life-threatening
Grade 5 = fatal
-
7/29/2019 SAS Clinical Trails Phase-I
16/70
Dose-Limiting Toxicities (DLT)
Toxicities that, due to their severity or duration,
are considered unacceptable, and limit further
dose escalation
Defined in advance of beginning trial
Classically based on cycle 1 toxicity
Examples:
ANC < 500 for 5 or 7 days
ANC < 500 of any duration with fever
PLT < 10,000 or 25,000
Grade 3 or greater non-hematologic toxicity
Inability to re-treat patient within 2 wks of
scheduledtreatment
-
7/29/2019 SAS Clinical Trails Phase-I
17/70
Definition of DLT is Dynamic
Examples: DLTs in 2008 Diarrhea : grade 3 in spite of adequate
antidiarrheal
therapy (loperamide)
Nausea and vomiting : grade 3 in spite of adequate
anti-emetic prophylaxis and therapy (steroids,
5HT3antagonists)
Hypertension : grade 3 in spite of adequate anti-hypertensive
therapy
Inability to take at least 90% of drug doses in a
cycle(continuous oral meds)
Grade 2 chronic unremitting toxicity
-
7/29/2019 SAS Clinical Trails Phase-I
18/70
Maximally Tolerated Dose(MTD)
Inconsistently defined as either: Dose at which 33% of pts
experience
unacceptable toxicity (DLT in 2 of 3 or 2 of 6)
OR 1 dose level below that
MTD = level @ DLT (in Europe or Japan)
MTD = level below DLT (in US)
6-10 pts treated at the recommended Phase IIdose (MTD or 1 dose
level below)
-
7/29/2019 SAS Clinical Trails Phase-I
19/70
Recap : Trans-AtlanticDifferences in Terminology
Important to note that:
Maximum tolerated dose (MTD):
Usually means recommended dose in US
Usually means dose level above recommendeddose in Europe and
some other jurisdictions
-
7/29/2019 SAS Clinical Trails Phase-I
20/70
How many patients percohort?
-
7/29/2019 SAS Clinical Trails Phase-I
21/70
Patients per Cohort : Guiding
Principles
Minimum needed to provide adequate
toxicity information
Classically 3 patients per cohort In some designs 1 patient per
cohort
until toxicity seen
If correlative studies are a major aim, may
increase up to 6 patients per cohort
-
7/29/2019 SAS Clinical Trails Phase-I
22/70
3 pts
Dose
3 pts
3 pts
3 pts
3 pts
3 ptsRecommended dose
DLT
3 pts+
Eisenhauer et al.
DLT
Phase I Standard 3 + 3 Design
-
7/29/2019 SAS Clinical Trails Phase-I
23/70
How quickly do youescalate?
-
7/29/2019 SAS Clinical Trails Phase-I
24/70
Phase I Trial Design : Dose Escalation
Escalation in decreasing steps (Hansen HH et al.
Cancer Res. 1975)
Attributed to a merchant from Pisa in the 13th century
(Leonardo Bonacci, 1170-1240; aka Fibonacci)
Outlined a number of problems including how many pairs
of rabbits can be produced from a single pair underspecified
conditions? (1, 1, 2, 3, 5, 8, 13, 21, 34, 55, 89,
144..) in a book, Liber abacus
-
7/29/2019 SAS Clinical Trails Phase-I
25/70
Phase I Trials: Dose Escalation
Cohort Dose % Escalation
1 n first dose
2 2 n 100%
3 3.3 n 67%
4 5 n 50%5 7 n 40%
6 and higher 25-33%
The Modified Fibonacci Schedule
-
7/29/2019 SAS Clinical Trails Phase-I
26/70
Cohort Dose Escalation
# of pts w/DLT Action
0/3 Increase to next level
1/3 Accrue 3 more pts at same dose level
1/3 + 0/3 Increase to next dose level
1/3 + 1/3 Stop: recommend previous dose level
1/3 + 2/3 Stop: recommend previous dose level
1/3 + 3/3 Stop: recommend previous dose level
2/3 Stop: recommend previous dose level3/3 Stop: recommend
previous dose level
-
7/29/2019 SAS Clinical Trails Phase-I
27/70
Problems and Pitfalls
-
7/29/2019 SAS Clinical Trails Phase-I
28/70
Phase I Study Assumptions
The higher the dose,
the greater the
likelihood of efficacy
Dose-related acute
toxicity is regarded as
a surrogate for
efficacy The highest safe dose
is the dose most likely
to be efficacious
A B
107
107
106 106
105 105
104 104
103 103
102 102
SURVIA
LFRACTION
c d
DOSE DOSE
y
x
z
w
Slope of line c = y/x = k
Slope of line d = z/w = h
-
7/29/2019 SAS Clinical Trails Phase-I
29/70
Dose-response: Efficacy and
Toxicity
010
20
30
40
50
6070
80
90
100
0.00
1.25
2.00
2.50
3.00
3.50
4.25
4.75
5.50
7.00
Therapeutic
Adverse
M difi d Fib i D
-
7/29/2019 SAS Clinical Trails Phase-I
30/70
Modified Fibonacci DoseEscalation
Problems:
Requires many patients
Takes a long time
May expose a substantial proportion of
patients to low, ineffective doses
Cl i Ph I T i l
-
7/29/2019 SAS Clinical Trails Phase-I
31/70
Classic Phase I TrialsDesign Limitations
Wide confidence intervals
Patients treated at ineffective dosesin first cohorts
High risk of severe toxicities at late
cohorts
-
7/29/2019 SAS Clinical Trails Phase-I
32/70
Classic Phase I Trials
Design LimitationsChronic toxicities usually cannot
be assessedCumulative toxicities usually
cannot be identifiedUncommon toxicities will be
missed
-
7/29/2019 SAS Clinical Trails Phase-I
33/70
Phase I Studies and Infrequent
Toxicities
Probability of NOT observing a serioustoxicity occuring at a
rate of:
Number of patients 10% 20%
1 0.90 0.80
2 0.81 0.64
3 0.73 0.51
6 0.53 0.26
10 0.35 0.11
15 0.21 0.04
Probability of overlooking a toxicity: POT(p) = (1-
p)n; n = sample size,p = true toxicity rate
Al D i
-
7/29/2019 SAS Clinical Trails Phase-I
34/70
Alternate Designs
Starting dose
Number of patients per dose level
Method/rapidity of dose escalation
-
7/29/2019 SAS Clinical Trails Phase-I
35/70
Starting
Dose
(% of LD10)
# of Dose
Levels to
Reach MTD
# of Unsafe
Trials*
n = 21
# of Unsafe
Drugs*
n = 14
10% 7 (4-14) 0 0
20% 5 (3-11) 5 2
30% 3 (2-9) 11 6
Selection of Starting Dose for Phase I Trials:
Retrospective analysis of 21 trials using
modified Fibonacci dose escalation
*Unsafe defined as reaching MTD in 3 dose levels
Eisenhauer et al JCO (18), 2000
I t ti t d l ti
-
7/29/2019 SAS Clinical Trails Phase-I
36/70
Intra-patient dose escalationTreat patients at dose level 1
Dose level 2 is well tolerated and patients
at dose level 1 have no toxicities
Patients at level 1 are escalated to level 2
WHY NOT DO THIS ALWAYS ?
Makes evaluation of chronic toxicitiesdifficult
The proverbial 1 responder at dose level 1
Phase I Trial Design
-
7/29/2019 SAS Clinical Trails Phase-I
37/70
First proposed by Simon et al (J Natl
Cancer Inst 1997)
Several variations exist:
usual is doubling dose in single-patient cohorts
till Grade 2 toxicity
then revert to standard 3+3 design using a 40%
dose escalation
intrapatient dose escalation allowed in somevariations
More rapid initial escalation
Phase I Trial DesignAccelerated Titrated Design (Rule-based)
-
7/29/2019 SAS Clinical Trails Phase-I
38/70
1 pt
Dose
1 pt
1 pt
3 pts
3 pts 3 ptsRecommended dose
DLT
3 pts+ DLT
Accelerated Titrated Design
Accelerated Titrated Design : Phase
-
7/29/2019 SAS Clinical Trails Phase-I
39/70
Accelerated Titrated Design : Phase
I Study of Lonafarnib (SCH66336)
Adjei AA et al, Cancer Research, 2000
Phase I Trial Design
-
7/29/2019 SAS Clinical Trails Phase-I
40/70
Bayesian method
Pre-study probabilities based on preclinical orclinical data of
similar agents
At each dose level, add clinical data to betterestimate the
probability of MTD being reached
Fixed dose levels, so that increments ofescalation are still
conservative
Phase I Trial DesignModified Continual Assessment Method
(MCRM Model-based)
Modified Con
tinual Assessment Method (MCRM
-
7/29/2019 SAS Clinical Trails Phase-I
41/70
Example: Pre-set dose levels of 10, 20, 40, 80, 160,
250, 400 If after each dose level, the statistical model
predicts a MTD higher than the next pre-set doselevel, then dose
escalation is allowed to the next
pre-set dose level
Advantages:
Allows more dose levels to be evaluated with a smaller
number of patientsMore patients treated at or closer to
therapeutic dose
Disadvantages:
Does not save time, not easily implemented if without
access to biostatistician support
Modified Continual Assessment Method (MCRMModel-based)
-
7/29/2019 SAS Clinical Trails Phase-I
42/70
-
7/29/2019 SAS Clinical Trails Phase-I
43/70
EXAMPLE of Probability of DLTs (Bayesian design)
Under-Dosing(This % should be minimal)
Ideal Dosing(This bar should be the highest percentage)
Over-Dosing(This bar should be below 25%)
Excessive Over-Dosing(This bar should be 0%)
7% 60% 30% 3%
44% 52% 4% 0%
Drug at 0.5mg
7% 66% 27% 0%
Drug at 0.75 mg
0% 35% 64% 0%
Drug at 1.0 mg
-
7/29/2019 SAS Clinical Trails Phase-I
44/70
0/3
Posterior summaries for probabilities of DLT (in %)
________________________________________________________________
Dose 0-0.16 0.16-0.33 0.33-0.6 0.6-1 Median Overdose
mg Under- Targeted Over- Excessive DLT rate Control/day dosing
Toxicity dosing toxicity
________________________________________________________________
2.5 95.7 3.3 0.5 0.4 0.0 ok
5 91.1 5.5 3.1 0.4 0.2 ok
10 82.9 9.1 6.7 1.3 1.9 no3
17.5 62.5 17.7 12.5 7.2 8.8 no2,3
25 40.0 21.2 19.3 19.5 22.3 no1-3
35 15.6 19.7 20.4 44.3 53.7 no1-3
45 9.9 12.5 19.9 57.7 73.0 no1-3
60 5.6 10.9 12.0 71.5 86.5 no1-3
75 3.2 7.7 12.7 76.4 92.8 no1-3
100 2.4 3.3 13.3 80.9 96.6 no1-3
__________________________________________________________________1
Escalation to this dose not possible, overdose control
criterion
(P(overdosing or excessive tox)>25%) violated
2 Escalation to this dose not possible, overdose control
criterion
(P(excessive tox)>5%) violated3 Escalation to this dose not
possible, increment >100%
No first cycle DLTs
Bayesian model supports dose escalation in cohort 2 (100%
doseincrement)
Prior and posterior probabilities of DLT (median and 95%-CI)
dose
ProbabilityofDLT
0.0
0.2
0.4
0.6
0.8
1.0
dose
ProbabilityofDLT
0.0
0.2
0.4
0.6
0.8
1.0
2.5 5 10 17.5 25 35 45 60 75 100
-
7/29/2019 SAS Clinical Trails Phase-I
45/70
1/4
Posterior summaries for probabilities of DLT (in %)
________________________________________________________________
Dose 0-0.16 0.16-0.33 0.33-0.6 0.6-1 Median Overdose
mg Under- Targeted Over- Excessive DLT rate Control/day dosing
Toxicity dosing toxicity
________________________________________________________________
2.5 48.1 28.4 16.4 7.1 16.5 no2
5 30.5 31.5 27.5 10.5 26.4 no1,2
10 16.5 23.7 37.3 22.4 38.3 no1-3
17.5 8.8 14.7 41.6 34.9 50.3 no1-3
25 6.1 9.9 37.6 46.4 58.3 no1-3
35 5.6 7.7 29.6 57.1 65.6 no1-3
45 3.7 7.6 24.5 64.1 69.6 no1-3
60 3.3 6.5 18.9 71.2 75.1 no1-3
75 2.4 6.1 15.3 76.1 78.1 no1-3
100 2.4 4.9 13.6 79.1 82.3 no1-3
__________________________________________________________________1
Escalation to this dose not possible, overdose control
criterion
(P(overdosing or excessive tox)>25%) violated
2 Escalation to this dose not possible, overdose
controlcriterion
(P(excessive tox)>5%) violated3 Escalation to this dose not
possible, increment >100%
First cycle DLT in first cohort
Bayesian model does not support dose escalation in cohort 2
Prior and posterior probabilities of DLT (median and 95%-CI)
dose
P
robabilityofDLT
0.0
0.2
0.4
0.6
0.8
1.0
dose
P
robabilityofDLT
0.0
0.2
0.4
0.6
0.8
1.0
2.5 5 10 17.5 25 35 45 60 75 100
Challenges to developing novel non-
-
7/29/2019 SAS Clinical Trails Phase-I
46/70
General requirement for long-term administration:pharmacology
and formulation critical
Difficulty in determining the optimal dose in phase I:
MTD versus OBD
Absent or low-level tumor regression as single
agents:problematic for making go no-go decisions
Need for large randomized trials to definitively assessclinical
benefit: need to maximize chance of success in
phase III
Challenges to developing novel non
classical cytotoxic agents
-
7/29/2019 SAS Clinical Trails Phase-I
47/70
Phase I Trial Design: Non-Cytotoxic Agents
MTD may not be the goal of Phase I sincespecificity of effect
may be lost at MTD
Pharmacologic effect may not equal
biologic effectGoal: identify optimal biologically effective
dose (OBED)
Paradox: requires early development andintegration of (usually
unvalidated)
measures of biologic effect into Phase I
Do we need correlative studies ?
-
7/29/2019 SAS Clinical Trails Phase-I
48/70
Conventional cytotoxic drugs have led to predictable
effects on proliferating tissues (neutropenia,
mucositis, diarrhea), thus enabling dose selection and
confirming mechanisms of action
Targeted biological agents may or may not have
predictable effects on normal tissues and often enterthe clinic
needing evidence/proof of mechanisms in
patients
Do we need correlative studies ?
Do we need correlative studies ?
-
7/29/2019 SAS Clinical Trails Phase-I
49/70
Therefore, biological correlative studies maybe used to derive
the best dose and schedule
of an agent,and
To determine whether the drug is inducing the
intended biological effect in the patient,and
To predict clinical benefit, although this
generally requires testing in large randomized
studies.
Do we need correlative studies ?
Alternative Endpoints
-
7/29/2019 SAS Clinical Trails Phase-I
50/70
Alternative Endpoints
Minimum blood levels/AUC or other
PK measure Inhibition of target
In normal tissue
In tumor tissue
Need enough preclinical evidence tosuggest that the above
are
reasonable endpoints withsufficient clinical promise
Must also pay attention to toxicity
Phase I Trial Design : Non-Cytotoxic
-
7/29/2019 SAS Clinical Trails Phase-I
51/70
Phase I Trial Design : Non Cytotoxic
Agents - Examples
Pre-clinically define target drug
exposureMatrixMetalloproteinase Inhibitors
Define pharmacodynamic endpointBortezomib
(70% of 26S proteasome inhibition in PBMCs)
Use functional imaging as endpointVatalanib
(DCE-MRI)
Use cumulative toxicitiesCI-1040 MEK Inhibitor,800mg TID
intolerable after 3 cycles of therapy
Problem : If drug works, youre a genius. If it
doesnt, youre a goat
V t l ib (PTK/ZK) VEGF R t
-
7/29/2019 SAS Clinical Trails Phase-I
52/70
Adapted from Dvorak H. J Clin Oncol. 2002;20(21):4368-4380.
VEGF-AVEGF-CVEGF-DVEGF-E
VEGF-AVEGF-B
VEGF-CVEGF-D
VEGFR-1/Flt-1 VEGFR-2/KDR VEGFR-3/Flt-4
PTK/ZK PTK/ZK PTK/ZK
Extracellular
Intracellular
Vatalanib (PTK/ZK) : VEGF Receptor
Tyrosine Kinase Inhibitor
PTK/ZK Induced Significant
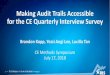
-
7/29/2019 SAS Clinical Trails Phase-I
53/70
Reduction in tumor blood flow through liver metastases
secondary to colorectal cancer at day 2 is significantly
correlated with improved early clinical outcome
PTK/ZK Induced Significant
Reduction in Tumor Blood Flow in
Metastatic Colorectal Cancer by DCE-MRI
Baseline Day 2
Thomas AL, et al. Semin Oncol. 2003;30:32-38.Morgan B, et al. J
Clin Oncol. 2003;21:3955-3964.
-
7/29/2019 SAS Clinical Trails Phase-I
54/70
Morgan B, et al. J Clin Oncol. 2003;21:3955-3964.
MeanbaselineMRIKi,%
160
140
120
100
80
60
40
20
0
020
40
60
80
100
120
140
160
180
200
Progressors
Nonprogressors
AUC 0-24, hrM
260
240
220
200
180
160140
120
100
80
60
4020
0
Dose, mg
Day 28
0
200
400
600
800
1,0
00
1,2
00
1,4
00
1,6
00
1,8
00
2,0
00
2,2
00
AUC0-24,hrM
Using DCE-MRI to Establish theOptimal Therapeutic Dose for
Vatalanib
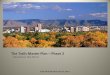
The Conundrum of Optimal Biologic
-
7/29/2019 SAS Clinical Trails Phase-I
55/70
The Conundrum of Optimal BiologicDose : Phase III PTK787/FOLFOX
in CRC
PTK787 1250 mg QD
0
25
50
75
100
0 2 4 6 8 10 12
Time since randomization, months
Progres
sion-freesurviv
al,% PTK/ZK + FOLFOX4
Placebo + FOLFOX4
Phase I Trials of Agent Combinations
-
7/29/2019 SAS Clinical Trails Phase-I
56/70
Initial dose-finding component often needed if you
are planning a new combination for a phase II trial Patients for
dose-finding phase:
Advanced solid tumors (all comers):
Advantage:fast accrual
Disadvantage:may not be representative of your patientpopulation
of interest
Specific patient population (e.g. same as phase IIcohort):
Advantage:population of interest, and early glimpse atantitumor
activity in disease of interest
Disadvantage:slow down accrual especially if
rare/uncommontumors
Phase I Trials of Agent Combinations
Phase I Trials of Agent Combinations
-
7/29/2019 SAS Clinical Trails Phase-I
57/70
Dose escalation:
New drug A + Standard combination BC
Ideally keep standard combo doses and
escalate the new drug (e.g. 1/3, 2/3, full dose)
Need to provide rationale: why add A to BC?
Need to think about overlapping toxicity in
your definition of DLT
Do you need PK assessment to determine if
A, B and C interact with each other?
Phase I Trials of Agent Combinations
How are Phase I Studies
-
7/29/2019 SAS Clinical Trails Phase-I
58/70
How are Phase I Studies
Designed Now ?
31 targeted agents: representative of most
common targets
Reports (papers or abstracts) of completed single
agent phase I trials in non-hematologic
malignancies
57 phase I reports identified
Parulekar and Eisenhauer JNCI July 2004
Agents/Targets
-
7/29/2019 SAS Clinical Trails Phase-I
59/70
Agents/TargetsTarget Agent #Trials
Angiogenesis Endostatin
ZD6474
PTK787
SU6668
SU5416
Bevacizumab
SU11248
3
1
1
3
3
1
1
BCL-2 G3139 2
PKC alpha ISIS 3521 2
raf kinase BAY 43-
9006 ISIS5132
3
3
DNA MTase MG98 2
MEK CI-1040 1
mTOR CCI-779 1
Target Agent #Trials
EGFR/HER2
ZD1839OSI-774
C225
MAB225
EMD7200
EKB569RG83852
trastuzumab
51
1
1
1
11
1
MMP BAY 12-9566
Marimastat
COL-3BMS-275291
3
2
11
Farnesyl
trans-
ferase
BMS-214662
R115777
L778,123
SCH66336
2
3
2
3
Results: Reason for Halting
-
7/29/2019 SAS Clinical Trails Phase-I
60/70
Results: Reason for Halting
Dose EscalationReason No. Trials No. Agents
Toxicity 36 20
PK 7 5
Other:Design (max. planned dose)
Drug Supply
Other phase I results
Active dose
3
4
2
1
3
2
2
1Not stated 4 4
TOTAL 57
Basis for Recommending Phase II Dose
-
7/29/2019 SAS Clinical Trails Phase-I
61/70
Basis for Recommending Phase II Dose
Recommended phase II dose? No. Trials No. Agents
Recommended 50 27
Basis: Toxicity
PK (blood levels)Other trial toxicity
Clinical activity
PBMC findings
Tumor measuresConvenience
35
92
1
1
11
19
72
1
1
11
Not stated 5 5
Not recommended 2 1
Parulekar and Eisenhauer JNCI July 2004
Secondary Information to
-
7/29/2019 SAS Clinical Trails Phase-I
62/70
ySupport Dose Recommendation
No.
TrialsPrimary
Basis
No. Trials Secondary Support From:
Toxicity PK Tumor
measures
Surrogate
measures
Other
Toxicity 35 - 12 2 7 8
PK 9 - - 1 1 3Tumor
measures
1 - - - - -
Surrogate
measures
1 - - - - -
Other 4 2 1 1 -
TOTAL 50 1 12 4 9 11
Other includes: clinical effects, results other trials,
convenience, etc.
Laboratory and Imaging Studies
-
7/29/2019 SAS Clinical Trails Phase-I
63/70
y g g
Total
No. Trials
Primary
Basis ofDose
Supportive
of dose
No
Help
Tumor Tissue 5 1 4 -
Surrogate
Tissue:
PMBC
Skin
Buccal
11
2
2
1
-
-
5
2
2
5
-
-
Imaging 6 - 1 5
15
Parulekar and Eisenhauer JNCI July 2004
Summary Review
-
7/29/2019 SAS Clinical Trails Phase-I
64/70
Summary: ReviewPhase I Trials Targeted Agents
Toxicity
Most common reason to halt escalation and primary
basis for dose recommendation (35/50 trials)
PK (Blood levels) Second most common basis for dose
recommendation (9/50 trials)
Laboratory studies May provide information to support dose
recommendation
Parulekar and Eisenhauer JNCI July 2004
-
7/29/2019 SAS Clinical Trails Phase-I
65/70
Phase I Study - Ethics
Phase I Study Ethics
-
7/29/2019 SAS Clinical Trails Phase-I
66/70
Phase I Study - Ethics
Patient benefit or antitumor activity is not aprimary goal of
the study, but therapeutic intent
is an important feature
Desperate patients cannot make a truly informed
decision
Historically low probability of response in Phase I
trials
< 5% response rate Majority of responses occur within
80%-120% of the
recommended phase II dose
Response Rates and Toxic Deaths in Phase I OncologyTrials
(Horstman et al NEJM 352; 2005)
-
7/29/2019 SAS Clinical Trails Phase-I
67/70
Trial No. ofTrials
# of PtsAssessed
forResponse
OverallResponse Rate*
%
No. ofPatients
Assessed forToxic Events
Deathsfrom Toxic
Eventsno. %
TotalFirst use of an agent inhumans
117 3164 4.8 3498 9 (0.26)
Cytotoxic chemotherapyFirst use of an agent inhumans
43 1298 5.0 1422 7 (0.49)
ImmunomodulatorFirst use of an agent inhumans
16 404 7.4 431 1 (0.23)
Receptor or signaltransductionFirst use of an agent inhumans
27 742 3.8 853 1 (0.12)
AntiangiogenesisFirst use of an agent inhumans
8 200 7.0 228 0
Gene transferFirst use of an agent inhumans
0 0 0 0 0
Vaccine
First use of an agent inhumans
23 520 3.1 564 0
Trials (Horstman et al, NEJM 352; 2005)
-
7/29/2019 SAS Clinical Trails Phase-I
68/70
Phase I Study - Ethics
Investigators have an inherent conflict ofinterest
Funding
Academic promotion
Publicity
Phase I Study Ethics : Partial
-
7/29/2019 SAS Clinical Trails Phase-I
69/70
ySolutions to the Dilemma
Youre the patients physician 1st and a scientist 2nd
Scientific goals should never take precedence overthe patients
best interest
Only pts for whom no life-prolonging or curativetherapy exists
are eligible for Phase I trials
Informed consent is obtained from every patient
No new agent can hit the pharmacy shelveswithout going through
Phase I clinical evaluation
Phase I Clinical Trials - Summary
-
7/29/2019 SAS Clinical Trails Phase-I
70/70
y
Most drugs tend to follow the MTD/DLT
paradigm Alternative designs continue to be explored.
Most times they are more complex.
Correlative studies are increasingly importantin the
comprehensive evaluation of new agents
Patient benefit/wellbeing trumps all the science
Being a good phase I trialist is not as simple asyou may
think