Embed Size (px)
Citation preview

Sarah Wovcha, J.D., M.P.H.
American Association for Community
Dental Programs Symposium
Fort Worth, TX
April 25, 2014

Funded by MCHB and HRSA
Integrate comprehensive oral health services
into an existing school-based health center
(SBHC); within Schools, Head Start Centers and
Community Centers
Increase access to oral health care
Assure delivery of quality education and preventive
and restorative care
Targeted to children and adolescents from
underserved populations, immigrant and refugee
community, and at-risk for oral disease.

Mission:
Children's Dental Services is dedicated to improving the oral health of children from families with low incomes by providing accessible treatment and education to our diverse community.

Began in 1919 as a women’s charity that
supported the provision of oral health care
services to orphans living in Minneapolis
Became the first provider of Head Start-
based oral health care in the United States in
the 1960s
Quadrupled in size since 2000 due to lack of
access to affordable dental care for low-
income children and families
Is currently the single largest provider of on-
site oral health care in Minnesota schools and
Head Start programs

Children from birth to
age 21
Pregnant women with
low incomes
Individuals with low
incomes, the uninsured,
and the under-insured
Individuals with special
health care needs
Individuals who are
chemical and alcohol
dependent
Homeless individuals
and families
Members of the
gay/lesbian/bisexual/tr
ansgender community
Racial and ethnic
individuals including
those from East Africa,
Central and South
America, Southeast
Asia, and Native
American communities

Outreach
Oral health education
Preventive oral health
care (prophylaxis,
fluoride, sealants)
Restorative care
(restorations, extractions,
pulpotomies, stainless
steel crowns, and root
canals)
Hospital care, if needed

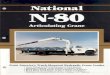
25%24%
22%
14%
10%
5%
0%
5%
10%
15%
20%
25%
30%
Somali/East
Africa
Latino African America Caucasian Hmong American Indian


Language fluency: CDS staff
speak over 16 different
languages and hail from 20
countries
Representing cultures
served: Understanding the
cultural norms, religious
needs and diets of target
communities staff create
culturally targeted and
translated curriculum for
care in school-based settings

Children and pregnant women go without needed services
Insurance Status
Shortage of
Providers
Language Barriers

Providing portable oral health care services
at SBHCs, Schools, Community Centers and
Head Start Centers
Decreasing multiple barriers affecting
families’ with low incomes access to oral
health care
Serving as a model for delivery of school-
based oral health care services for other
Minnesota cities

Minneapolis: 65.8% of residents are of a race or ethnicity other than
European American
69% of students are enrolled in free and reduced lunch
program
Family income is <185% of federal poverty guidelines
Edison High School (where CDS provides Care)
89.1% of students are of a race or ethnicity other than
European American 61.1%: African American
16.7%: Hispanic American
8.5%: Asian American
2.8%: American Indian
92.4% are enrolled in free and reduced lunch program

Engaging Refugee and Immigrant
Communities
Staff is representative of refugee and
immigrant community
Multiple languages offered
Provide care in a location
where trust is established
Reduce economic barriers

“One important means to
promote oral health in
diverse populations is to
develop a workforce that
is both culturally and
linguistically competent,
as well as one that is as
culturally diverse as the
American population.”
Garcia R, Cadoret C, Henshaw M. 2007. Multicultural issues in oral health. Dental Clinics of North
America 52(2):319–332.
Patients feel comfort and trust in staff who:
• Understand from where they come
• Understand their cultural norms and language

CDS acknowledges the
need to speak the same
language as their patients
Staff offer verbal and
written communication in:
Somali
Spanish
Hmong
Karen
Oromo

Clinical settings can
be intimidating
Families know and
trust in the
education system
No additional
transportation
requiredCDS provides on-site
care in elementary
schools

Number of African-born residents in MN
increased by 580% between 1990 and 2000
By 2002, ~9,000 immigrants arrived in MN
directly from various African nations.
13% of MN’s foreign-born residents are from
Africa.
Most came as refugees from Liberia, Somalia,
and the Sudan.
Recent immigrants arriving from Nigeria,
Ethiopia, and Eritrea.

MN has the largest population of Somali
residents in the U.S.
Most Somalis live in the Minneapolis metro
area. Fewer numbers live in Rochester,
Owantonna, and other suburban and greater
MN communities.
Nearly 1/3 of student who speak Somali at
home attend Minneapolis public schools.
Somalis immigrants are diverse; coming
from urban, coastal, agricultural and/or
nomadic regions.

“Children in non-English-primary-language
households are significantly more likely than
children in English-primary-language
households to be poor (42% vs 13%)”.
CDS Offers:
Coordinated assistance for families applying for
Medical Assistance
Certified MNCAA agents can assist families and submit
insurance application on behalf of eligible families
Flores G, Tomany-Korman SC. 2008. The language spoken at home and disparities in medical and dental health, access to
care, and use of services in US children. Pediatrics 121(6):e1703–1714.

60% of students served by
CDS are African, including
those who self-identify as
East African.
East African immigrants do
not place high importance
on oral health and
preventive health.*
* Obeng CS. 2008. Dental care issues for African immigrant families of preschoolers. Early Childhood
Research and Practice 10(2).
Dental checkups are not the cultural norm
Caries is not considered a health issue

Impact of refugee camps
Poor diet
Limited or no access to oral health care
History of torture
Effective oral health practices that are
not the norm in the U.S. (e.g., brushing
with the miswak)

Lack access to preventive and
restorative oral health care
Inadequate or no interpretative
services in dental care settings
Unfamiliar with the dangers of
western diet on oral health (e.g., high
sugar in food and drink)
Potentially unfamiliar with tooth
brushing and flossing

Flores G, Tomany-Korman SC. 2008. The language spoken at home
and disparities in medical and dental health, access to care, and
use of services in US children. Pediatrics 121(6):e1703–1714.
Garcia R, Cadoret C, Henshaw M. 2007. Multicultural issues in oral
health. Dental Clinics of North America 52(2):319–332.
Obeng CS. 2008. Dental care issues for African immigrant families
of preschoolers. Early Childhood Research and Practice 10(2).
Minneapolis Public Schools. 2010–2011. Report of the Annual
Racial/Ethnic Count of MPS Students for the 2009–2010 Year.
Minneapolis, MN: Minneapolis Public Schools
Minneapolis Public Schools. 2010–2011. Minnesota Department of
Education Count for Compensatory Revenue—Meal Participation.
Minneapolis, MN: Minneapolis Public Schools.
Minneapolis Department of Health & Family Support. 2011.
Students Enrolled in Seven Minneapolis High Schools.

Sarah Wovcha, J.D., M.P.H.
Executive Director
In-House Counsel
Children’s Dental Services
(612) 636-1577






















![Search to Distill: Pearls Are Everywhere but Not the Eyes · Teachers Student1 Student2 Comparison EfficientNet-B7 [35] 65.8% 66.6% student1](https://img.pdfslide.us/doc/110x75/600f274218556073a7770037/search-to-distill-pearls-are-everywhere-but-not-the-eyes-teachers-student1-student2.jpg)




