Embed Size (px)
DESCRIPTION
Mediators of Race Effects on Risk of Potentially Avoidable Maternity Complications among Medicaid-insured Mothers. Sarah B. Laditka, Ph.D James N. Laditka, D.A., Ph.D. Janice C. Probst, Ph.D. Background and Theory . PAMCs, a population-based health care indicator - PowerPoint PPT Presentation
Citation preview

South CarolinaRural Health Research Center
At the Heart of Public Health Policy
Mediators of Race Effects on Risk of Potentially Avoidable Maternity Complications among Medicaid-insured Mothers
Sarah B. Laditka, Ph.D James N. Laditka, D.A., Ph.D.
Janice C. Probst, Ph.D.

Rural Health Research CenterSouth Carolina
Background and Theory PAMCs, a population-based health care indicator
Builds on epidemiological work of 1970s identifying "sentinel" conditions, which signal problems with medical care access or quality (Rutstein et al. 1976)
Extends health services research of 1980s and 1990s on Ambulatory Care Sensitive (ACS) conditions or "preventable hospitalization" (Billings et al. 1993, 1996; Bindman et al. 1995)
Assumptions of both ACSs and PAMCs Timely access to ambulatory health care can reduce
risks of certain medical complications Large hospital discharge data sets can be used for
assessment

Rural Health Research CenterSouth Carolina
PAMC: Definition and Example
PAMCs defined based on preventability through timely access to primary and prenatal care of reasonable quality, and through healthy behaviors often promoted by prenatal care.
Most PAMCs defined by a combination of primary and secondary diagnoses using ICD-9-CM codes; selected by panel of obstetricians and health services researchers.
Example: a delivery hospitalization with a substance abuse diagnosis and a complication known to be associated with substance abuse
Premature Rupture of Membranes Intrauterine Growth Restriction

Rural Health Research CenterSouth Carolina
Preliminary Research I Used 1997 Nationwide Inpatient Sample (NIS):
Generated working PAMC list Examined PAMC construct and face validity
Used 1988 National Maternal and Infant Health Survey (NMIHS):
Examined associations among Adequacy of Prenatal Care Utilization index (APNCU), healthy behaviors, and PAMC risk
PAMC citation: Laditka, S.B., J.N. Laditka, M.P. Mastanduno, M.R. Lauria, T.C. Foster. "Potentially Avoidable Maternity Complications: An Indicator of Access to Primary and Prenatal Care during Pregnancy." Women and Health (41(3) In Press).

Rural Health Research CenterSouth Carolina
Evidence of Preventability, NMIHS
Rating on Adequacy of Prenatal Care Utilization Index (APNCU):
“Adequate” compared to “Inadequate”:
Odds Ratio 0.43 (95% CI: 0.23~0.81, p<0.01)
“Intermediate” compared to “Inadequate”:
Odds Ratio 0.53 (95% CI: 0.29~0.97, p<0.05)

Rural Health Research CenterSouth Carolina
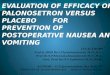
NIS Multivariate Results, DeliveriesControls: sociodemographics, comorbidities, health system & area, hospital characteristics, state effects
0.0
0.3
0.6
0.9
1.2
1.5
AfricanAmerican
Hispanic AsianOdd
s Rat
io &
95%
CI
Compared to Non-Hispanic Whites, All p < 0.0001

Rural Health Research CenterSouth Carolina
Preliminary Research II Used 2000 Nationwide Inpatient Sample (NIS):
Examined access to health care during pregnancy for mothers insured by Medicaid.
Investigated PAMC risks among rural and urban hospital deliveries for groups of mothers defined by race or ethnicity, calculating PAMC rates, logistic regression.
PAMC citation: Laditka, S.B., J.N. Laditka, K.J. Bennett, J.C. Probst (2005). "Delivery Complications Associated with Prenatal Care Access for Medicaid-Insured Mothers in Rural and Urban Hospitals." Journal of Rural Health 21(2), 158-166.

Rural Health Research CenterSouth Carolina
NIS Rural Urban Results
In rural hospitals, African Americans had higher PAMC risk than whites (OR 1.72, CI 1.26-2.36).
In urban hospitals, PAMC risk was not significantly higher for African Americans.
In urban hospitals, odds of a PAMC for Hispanics and Asians were about half of those of whites.
Suggested, policymakers should work to reduce PAMC risks for African American women in rural areas insured by Medicaid.

Rural Health Research CenterSouth Carolina
Present Study: Research Objectives Examine risks of potentially preventable pregnancy
complications Investigate individual-level factors associated with
these risks. Describe differences by race/ethnicity, using state-
level data from South Carolina, and the Potentially Avoidable Maternity Complication (PAMC) indicator.
PAMC indicator identifies pregnancy outcomes associated with access to prenatal care of reasonable quality.

Rural Health Research CenterSouth Carolina
Present Study: Data & Methods Hospital discharge data for SC for 2000, linked to
participant demographic and provider data from South Carolina Medicaid files.
Year 2000 Area Resource File. 26,866 delivery hospital discharges for Medicaid
insured women in South Carolina, 2000. Calculated PAMC rates, compared prevalence of
unadjusted risk factors among black, Hispanic, and white mothers; reference group was whites.
Multilevel logistic analyses. Analyses for ages 10-17 and 18+.

Rural Health Research CenterSouth Carolina
Ages 18+, Percent Distribution
Black HispanicNon-HWhite
Had a PAMC at delivery 3.92 + 1.85 * 3.43Education, < 8 years 2.89 * 10.37 *** 2.35Marital status, single 77.14 *** 41.48 *** 51.48Income below poverty 85.37 *** 65.34 *** 76.11Disabled 2.54 *** 0.00 ** 1.42Diabetes 1.14 *** 0.43 0.58Hypertension 1.47 *** 0.14 * 0.96Obesity 1.67 * 0.43 * 1.33Rural Resident 16.96 *** 15.48 14.48
+p<.1, *p<.05, **p<.01, ***p<.001

Rural Health Research CenterSouth Carolina
Multilevel, Selected Results, Ages11-17Adjusted for Individual, Area, and Hospital Factors
Parameter Odds Ratio LB UB
Black 2.26 1.41 3.62 ***
Hispanic 3.29 1.06 10.25 *
Rural Resident 4.02 1.34 12.02 *
+p<.1, *p<.05, **p<.01, ***p<.001

Rural Health Research CenterSouth Carolina
Multilevel, Selected Results, 18+Adjusted for Individual, Area, and Hospital Factors
+p<.1, *p<.05, **p<.01, ***p<.001
Parameter Odds Ratio LB UB
Black 1.01 0.86 1.19Hispanic 0.51 0.29 0.91 *Marital status, single 1.54 1.24 1.92 ***Diabetes 2.4 1.51 3.82 ***Rural resident 1.83 1.19 2.83 **

Rural Health Research CenterSouth Carolina
Results, Black Women For ages 10-17, PAMC risks were greater for blacks than whites in
unadjusted and adjusted results. For ages 18+, adjusted risks for blacks did not differ from whites. Black mothers 18+ had higher risks than whites: single or
disabled, in poverty or rural county, diabetes or hypertension. Adjusted results for blacks should be interpreted with caution: do
not suggest blacks are no more likely to have PAMCs than whites. Suggest PAMC risks for blacks and whites are indistinguishable when other measured risk factors are controlled.
Black women in South Carolina, as a group, are more likely to experience PAMCs than whites, because they are much more likely to have many notable risk factors.

Rural Health Research CenterSouth Carolina
Results, Hispanic Women For young mothers, PAMC rates did not differ significantly
between Hispanics and whites in unadjusted analyses, which may be attributable small number of Hispanics (n=62), as the occurrence of PAMC diagnoses was a relatively high 6.5%.
In adjusted analysis, Hispanics 10-17 had higher odds for a PAMC.
For those 18+, unadjusted PAMC rates were lower for Hispanics.
Hispanics had lower PAMC risks in multivariate analysis. Several individual-level risk factors were less prevalent in
Hispanics than whites, e.g., being single, having asthma, hypertension, diabetes and obesity.

Rural Health Research CenterSouth Carolina
Results, All Women
Mothers in rural areas had significant higher risks of having a PAMC, both in the bivariate and adjusted results.
Among those age 18+, diabetes emerged as substantial and significant PAMC risk in adjusted analyses; highlights importance of managing diabetes during pregnancy.

Rural Health Research CenterSouth Carolina
Limitations
Among Hispanics, sample size of young mothers small.
Cannot identify how long each mother was enrolled in Medicaid prior to pregnancy. Conducted an analysis of sensitivity to
number of months of pregnancy covered by Medicaid; results did not differ meaningfully.
Cross-sectional analysis.

Rural Health Research CenterSouth Carolina
Policy and Practice Implications I Practitioners should focus prenatal care efforts on
minorities among younger pregnant women. Practitioners should stress treatment of diabetes for
women of all races Rural residence is a major risk factor for PAMCs:
highlights South Carolina’s and nation’s continuing difficulty with ensuring an adequate supply of health care practitioners in rural areas. Policy strategies: increase support of rural residency training;
develop designation for practitioners similar to the Critical Access Hospital program to promote retention of practitioners in rural areas.

Rural Health Research CenterSouth Carolina
Policy and Practice Implications II Policymakers and practitioners should target known risk h
underlying greater PAMC risks for minority women. Medicaid providers should focus on reducing
avoidable morbidity among blacks, rural residents, and young Hispanics.
Healthy Start programs, community health centers, and rural health clinics may be useful for addressing pregnancy risks associated with poverty, single marital status, and chronic disease.
In rural areas, poor, disabled, and single pregnant women may benefit from transportation and other forms of proactive support to attend prenatal care.

Rural Health Research CenterSouth Carolina
~ Thank You ~
Sarah B. Laditka, Ph.D James N. Laditka, D.A., Ph.D.
Janice C. Probst, Ph.D.
Study supported by Grant 6 UIC RH 00045-04, U.S. Office of Rural Health Policy, Health Resources Services Administration
Mediators of Race Effects on Risk of Potentially Avoidable Maternity Complications among
Medicaid-insured Mothers












![[Bavly d.a.] corporate_governance_and_accountabili(book_fi.org)](https://img.pdfslide.us/doc/110x75/548bfd34b479599f408b497c/bavly-da-corporategovernanceandaccountabilibookfiorg.jpg)














