Embed Size (px)
Citation preview

Sarah Armstrong, MDDirector, Healthy Lifestyles Program
North Carolina School Community Health Alliance Conference
December 14, 2009
The Childhood Obesity The Childhood Obesity Epidemic:Epidemic:How we got here, what it means for a child’s health, and How we got here, what it means for a child’s health, and what you can dowhat you can do

All Rights Reserved, Duke Medicine 2007
Name that FoodENRICHED FLOUR (WHEAT FLOUR, NIACINAMIDE, REDUCED IRON, THIAMIN MONONITRATE [VITAMIN B1], RIBOFLAVIN [VITAMIN B2], FOLIC ACID), CORN SYRUP, HIGH FRUCTOSE CORN SYRUP, DEXTROSE, VEGETABLE OIL (SOYBEAN, COTTONSEED AND HYDROGENATED COTTONSEED OIL† WITH TBHQ AND CITRIC ACID FOR FRESHNESS), SUGAR, CRACKER MEAL, CONTAINS TWO PERCENT OR LESS OF WHEAT STARCH, SALT, DRIED STRAWBERRIES, DRIED APPLES, DRIED PEARS, CORNSTARCH, LEAVENING (BAKING SODA, SODIUM ACID PYROPHOSPHATE, MONOCALCIUM PHOSPHATE), CITRIC ACID, MILLED CORN, MODIFIED WHEAT STARCH, GELATIN, CARAMEL COLOR, PARTIALLY HYDROGENATED SOYBEAN AND/OR COTTONSEED OIL†, MODIFIED CORN STARCH, XANTHAN GUM, SOY LECITHIN, COLOR ADDED, NIACINAMIDE, REDUCED IRON, RED #40, VITAMIN A PALMITATE, YELLOW #6, PYRIDOXINE HYDROCHLORIDE (VITAMIN B6), RIBOFLAVIN (VITAMIN B2), THIAMIN HYDROCHLORIDE (VITAMIN B1), FOLIC ACID, TURMERIC COLOR, BLUE #1.†LESS THAN 0.5g TRANS FAT PER SERVING

All Rights Reserved, Duke Medicine 2007
600 calories per package (2 pop tarts)
38 grams of sugar
“No” trans fat
POP TARTS

All Rights Reserved, Duke Medicine 2007
Obesity Trends Worldwide

All Rights Reserved, Duke Medicine 2007
South East Asia & Pacific RegionNauru 78%Tonga 70%Samoa 63%Niue 46%French Polynesia 44%
AfricaSeychelles 28%South Africa 28%Ghana 20% Mauritania 19%Cameroon (urban) 14%
South Central AmericaPanama 36%Paraguay 36%Peru (urban) 23%Chile (urban) 23%Dominican Republic 18%
North AmericaUSA 33%Barbados 31%Mexico 29%St Lucia 28%Bahamas 28%
Eastern MediterraneanJordan 60%Qatar 45%Saudi Arabia 44%Palestine 43%Lebanon 38%
European RegionAlbania 36%Malta 35%Turkey 29%Slovakia 28%Czech Republic 26%
% Obese
0-9.9%
10-14.9%
15-19.9%
20-24.9%
25-29.9%
≥30%
Self Reported data

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 1985
No Data <10% 10%–14%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 1986
No Data <10% 10%–14%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 1987
No Data <10% 10%–14%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 1988
No Data <10% 10%–14%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 1989
No Data <10% 10%–14%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 1990
No Data <10% 10%–14%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 1991
No Data <10% 10%–14% 15%–19%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 1992
No Data <10% 10%–14% 15%–19%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 1993
No Data <10% 10%–14% 15%–19%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 1994
No Data <10% 10%–14% 15%–19%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 1995
No Data <10% 10%–14% 15%–19%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 1996
No Data <10% 10%–14% 15%–19%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 1997
No Data <10% 10%–14% 15%–19% ≥20%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 1998
No Data <10% 10%–14% 15%–19% ≥20%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 1999
No Data <10% 10%–14% 15%–19% ≥20%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 2000
No Data <10% 10%–14% 15%–19% ≥20%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 2001
No Data <10% 10%–14% 15%–19% 20%–24% ≥25%

All Rights Reserved, Duke Medicine 2007
No Data <10% 10%–14% 15%–19% 20%–24% ≥25%
Obesity Trends* Among U.S. AdultsBRFSS, 2002

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 2003
No Data <10% 10%–14% 15%–19% 20%–24% ≥25%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 2004
No Data <10% 10%–14% 15%–19% 20%–24% ≥25%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 2005
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%

All Rights Reserved, Duke Medicine 2007
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
Obesity Trends* Among U.S. AdultsBRFSS, 2006

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 2007
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%

All Rights Reserved, Duke Medicine 2007
Obesity Trends* Among U.S. AdultsBRFSS, 2008 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%

All Rights Reserved, Duke Medicine 2007
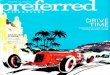
1999
Obesity Trends* Among U.S. AdultsBRFSS, 1990, 1999, 2008
2008
1990
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%

All Rights Reserved, Duke Medicine 2007

All Rights Reserved, Duke Medicine 2007

All Rights Reserved, Duke Medicine 2007
Turning the corner on childhood obesity…

All Rights Reserved, Duke Medicine 2007
03-04 N=2,15903-04 N=981
0
5
10
15
20
25
1963-651966-70
1971-741976-80
1988-9499-00
01-0203-04
US 6-11 yr
US 12-19 yr
NHANES data sources: Ogden et al. Prevalence and Trends in Overweight Among US Children and Adolescents, 1999-2000. JAMA 2002;288(14):1728-1732. Ogden et al. Prevalence of Overweight and Obesity in the United States, 1999-2004. JAMA 2006;295(13):1549-1555.
19.019.520.020.521.021.522.0
2004 2005 2006 2007
AR grades K-6AR grades 7-12
The Arkansas “Experiment:” Act 1220 (2006)

All Rights Reserved, Duke Medicine 2007
ADULT BMI
• Weight (kg) / Height (cm) squared
• Between 18 and 25 is normal
• Between 25 and 30 is “overweight”
• Above 30 is “obese”
http://heartline.in/images/diabetes_BMI_chart.gif

All Rights Reserved, Duke Medicine 2007
Pediatric BMI
-same calculation
-read as percentile
-BMI correlates with risk for disease
-shift paradigm from weight loss to weight maintenance

All Rights Reserved, Duke Medicine 2007
For example, a five year old girl with BMI of 20kg/m2 who maintains her weight but increases her height normally will get into the “green zone” by age 8.
The same girl, if she gains weight slowly, and continues to gain height, will get into the “green zone” by age 10.

All Rights Reserved, Duke Medicine 2007

All Rights Reserved, Duke Medicine 2007
Source: Mokdad et al., Diabetes Care 2000;23:1278-83; J Am Med Assoc 2001;286:10.
Diabetes Trends* Among Adults in the U.S
1990 1995
2001

All Rights Reserved, Duke Medicine 2007
“Pre-Diabetes” or “Insulin Resistance Syndrome”

All Rights Reserved, Duke Medicine 2007
Polycystic Ovarian Syndrome“PCOS”

All Rights Reserved, Duke Medicine 2007
Childhood Hypertension

All Rights Reserved, Duke Medicine 2007
Children and Cholesterol

All Rights Reserved, Duke Medicine 2007
Fatty Liver Disease
“Non-alcoholic steatohepatitis”

All Rights Reserved, Duke Medicine 2007
Osteoarthritis
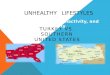
Percent of total daily calories from soda, juice, and milk
0
2
4
6
8
10
12
14
1977 2001
SodaJuiceSoda + JuiceMilk
Neilsen SJ, Popkin BM. Changes in beerage intake between 1977 and 2001. American Journal of Preventive Medicine. 2004; 27(3):205-210.

All Rights Reserved, Duke Medicine 2007
Blount’s Disease“Pathologic tibia varum”

All Rights Reserved, Duke Medicine 2007
Childhood depression
• Quality of life for obese children lower than that for children with cancer
• Bullying, teasing, social isolation and inability to participate in active or social events may contribute
• Rates of depression and anxiety are 2-3 times higher in obese adolescents than in normal weight teens.
Reference: Barlow et al, Pediatrics (s): 2007

All Rights Reserved, Duke Medicine 2007
Economic Update
• Direct medical costs: >9% of all US health expenditures
• Estimated direct and indirect costs: $117 billion in 2000 now estimated at $130 billion per year
• Expenditures expected to increase as obese children become obese adults with chronic illnesses

All Rights Reserved, Duke Medicine 2007

All Rights Reserved, Duke Medicine 2007
PREVENTION, ASSESSMENT AND TREATMENT MESSAGE
• 5 fresh fruits/veggies a day• 3 structured family meals • 2 hours or less of screen time• 1 hour of physical activity a day• “Almost none” sugar-sweetened beverages

All Rights Reserved, Duke Medicine 2007
5 Fruits & VegetablesGoal 5 or more servings/day (1/2 cup = 1 serving) USDA recommends 9 servings/day.
Why eat fruits and vegetables? • Low in calories• High in fiber (fiber goal: age + 5)• Improve satiety• Rich in vitamins and minerals• Natural toothbrushes
Model of Eating Competence:1. No clean plate club rules2. Parent feeding responsibility3. Child feeding responsibility Ellyn Satter, Child of Mine

All Rights Reserved, Duke Medicine 2007
3 Structured Meals
Family guidance: • Eat at the table, at home, with the TV off.• Offer a variety of foods-protein, grain, vegetable, fruit, and reduced
fat milk or water – but no short order cooking!• Create positive meal atmosphere
Skipping breakfast is strongly associatedwith obesity. Eating breakfast is protectiveagainst developing obesity.• Fruit and string cheese• Granola bar and yogurt• Cheese and crackers• Peanut butter toast• Cereal (<9g sugar) and milk• Instant breakfast drink
Barlow et al, Pediatrics, 2007

All Rights Reserved, Duke Medicine 2007
Creative Labeling
Children Under 8 cannot distinguish commercials from reality
No regulation on health claims on box, only Nutrition Label is regulated
“fortified with 8 essential vitamins and iron”

All Rights Reserved, Duke Medicine 2007
Disney and Obesity

All Rights Reserved, Duke Medicine 2007
“Healthy Plate”American Diabetes Association
American Cancer Institute

All Rights Reserved, Duke Medicine 2007
0% 20% 40% 60% 80% 100%
2 Hours or less of TV/media timePercent of 8-18 year-olds with each mediumPercent of 8-18 year-olds with each medium in their bedroomin their bedroom::
TelevisionTelevision
Internet accessInternet access
VCR/DVD playerVCR/DVD player
Video game consoleVideo game console
68%68%
20%20%
49%49%
Cable/satellite TVCable/satellite TV
ComputerComputer
37%37%
31%31%
20%20%
54%54%
Premium cable channelsPremium cable channels
Source: Kaiser Family Foundation, Generation M: Media in the Lives of 8-18 Year-Olds, March 2005: kff.org

All Rights Reserved, Duke Medicine 2007
TV Rules: Parent’s Role Percent of all 8-18 year-olds who say they have:
TV rules that TV rules that are enforced are enforced
“most” of time“most” of time
26%26%53%53%
20%20%
TV rules that TV rules that are are enforcedenforced some, a little some, a little
or neveror never
No rulesNo rulesabout TVabout TV
Source: Kaiser Family Foundation, Generation M: Media in the Lives of 8-18 Year-Olds, March 2005: kff.org

All Rights Reserved, Duke Medicine 2007
Household Media Environment Percent of 8-18 year-olds living in homes where:
TV is “usually” TV is “usually” on during on during
mealsmeals
63%63%
36%36%
TV not usually TV not usually left on during left on during
mealsmeals
Source: Kaiser Family Foundation, Generation M: Media in the Lives of 8-18 Year-Olds, March 2005: kff.org

All Rights Reserved, Duke Medicine 2007
1: Or more hour of active time
At least one hour of outdoor time per day associated with decreased rates of obesity and chronic illness
National survey data indicate that 20% of US children 8 to 16 years of age reported 2 or fewer bouts of vigorous physical activity per week
Decreased school activity time as compared with 10 years ago.
Perceived neighborhood safety important determinant in child’s outdoor play time.
Built environment and access to safe play a critical concern.
Anderson et al. Relationship of physical activity and television watching with body weight and level of fatness among children: results from the Third National Health andNutrition Examination Survey. JAMA. 1998;279:938–942

All Rights Reserved, Duke Medicine 2007
Almost none: Sweetened Beverages
Liquid calories:12 oz. soda= 150 calories 10 tsp sugar12 oz. Kool Aid= 150 calories 10 tsp sugar
• Generally non-nutritive • Replaces source of calcium- needs 500-1300 mg/day
- Peak calcium needs in adolescence for bone density- Vitamin D
• Interferes with appetite for other healthful foods, especially in young children.
• Caffeine content-stimulant, restlessness, interferes with sleep

All Rights Reserved, Duke Medicine 2007
Fruit drinks/fruit punch
• Calories per 12 oz serving?– 171
• Teaspoons of sugar?– 15
Overall 60% increase in the risk of becoming
obese with each additional can of sugar
sweetened drink consumed

All Rights Reserved, Duke Medicine 2007
What about 100% fruit juice?
Recommendations
1. None for children under 1
2. Ages 1-7, 4-6 ounces/day
3. Ages 7 and up, no more than 12 ounces/day

All Rights Reserved, Duke Medicine 2007

All Rights Reserved, Duke Medicine 2007
Acceptance and Behavioral Control as Determinants of Parenting Style
Parenting Style
High Acceptance Low Acceptance
High Control Authoritative Authoritarian
Low Control Indulgent Disengaged
Adapted from Chassin et al, J Pediatric Psychology 2005

All Rights Reserved, Duke Medicine 2007
Age-Appropriate Family Focus
Breastfeeding
Rules and structure“Feeding responsibility”
Rules and structureRole modeling
Role modelingSupport of teenEncouraging good peer
influenceEllyn Satter, Child of Mine

All Rights Reserved, Duke Medicine 2007
CLINICAL CARE The Healthy Lifestyles Program
RESEARCH
EDUCATION
ADVOCACY
HEALTHY LIFESTYLES

All Rights Reserved, Duke Medicine 2007
Risk Reduction:BMI Stabilization
1015
2025
3035
-12 -6 0 6
Time, months
Healthy Lifestyles
BM
I, kg
/m2
N=10; random cohort sample

All Rights Reserved, Duke Medicine 2007
Risk Reduction: BMI in Cohort
0
5
10
15
20
25
30
35
OW Obese SevereObesity
BaselinePost-HLP
Nu
mb
er
of
Pati
en
ts

All Rights Reserved, Duke Medicine 2007
Body Fat Percent
30
32
34
36
38
40
42
44
BF%
BaselinePost-HLP
Perc
en
til
e

All Rights Reserved, Duke Medicine 2007
Initial Cohort Results
Variable* Initial Last
Weight (kg) 74.9 76.2
BMI 32.5 32.2
Z-score 5.2 5.1
Co-Morbidities 3.8 2.4
* Mean Values
Mean time from initial to last visit was 7.4 months

All Rights Reserved, Duke Medicine 2007
Changes in Blood Pressure:Cohort Patients
Blood Pressure Initial Visit Last Visit
Normal 11 20
Pre-hypertension 5 5
Stage 1 Hypertension 8 7
Stage 2 Hypertension 10 2
Total 34 34

All Rights Reserved, Duke Medicine 2007
Pediatric and Adolescent Lifestyle Survey Results:Cohort Patients
0
5
10
15
20
25
30
35
PALS Score
StartPost-HLP

All Rights Reserved, Duke Medicine 2007
Mood and Feeling Questionnaire: Cohort Patients
• Score of 10 or greater indicates depression.
• 8 patients had an initial score of 10 or greater– 6 (75%) of these
patients score returned to normal
– No patient with an initial score <10 had a score of > 10 at last visit
0
1
2
3
4
5
6
7
MFQ Score
StartPost-HLP

All Rights Reserved, Duke Medicine 2007

All Rights Reserved, Duke Medicine 2007
• http://www.eatsmartmovemorenc.com/• http://pediatrics.duke.edu/modules/
ctr_ped_cendo_svc/index.php?id=1• http://kidshealth.org/• http://www.bam.gov/• http://win.niddk.nih.gov/publications/child.htm
Resources

Thank you
Sarah Armstrong
Director, Healthy Lifestyles
Duke Children’s Primary Care
December 14, 2009