Embed Size (px)
Citation preview
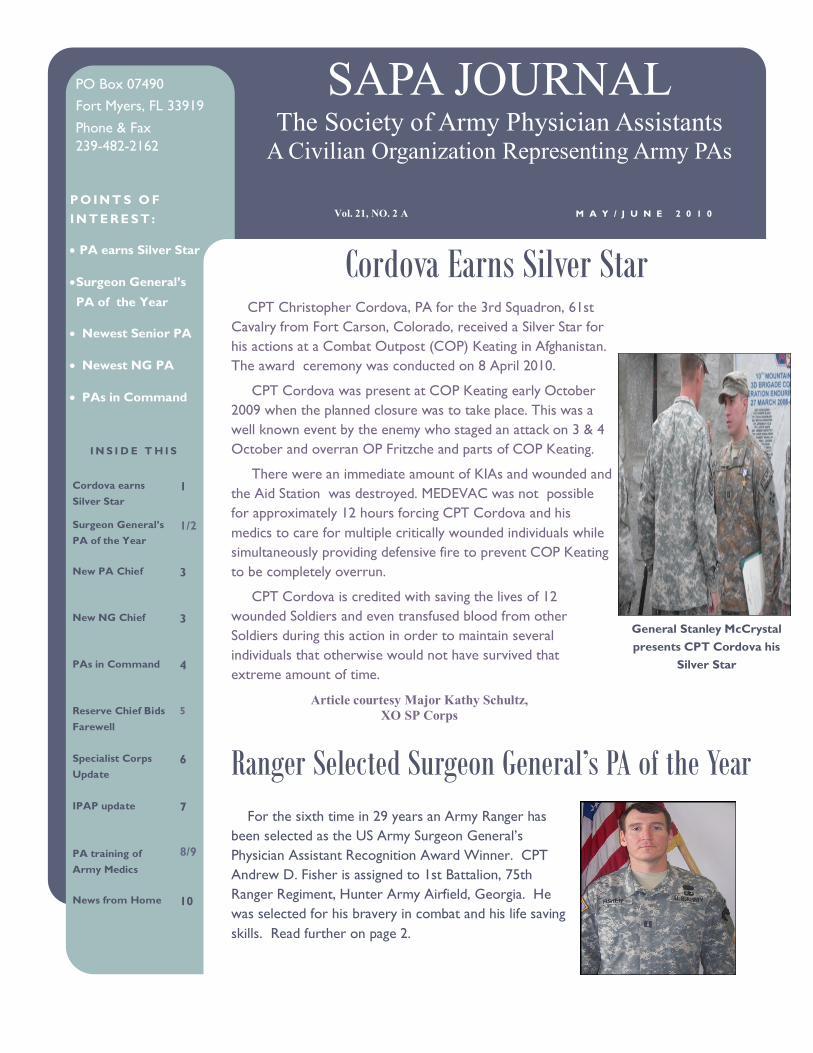
CPT Christopher Cordova, PA for the 3rd Squadron, 61st
Cavalry from Fort Carson, Colorado, received a Silver Star for
his actions at a Combat Outpost (COP) Keating in Afghanistan.
The award ceremony was conducted on 8 April 2010.
CPT Cordova was present at COP Keating early October
2009 when the planned closure was to take place. This was a
well known event by the enemy who staged an attack on 3 & 4
October and overran OP Fritzche and parts of COP Keating.
There were an immediate amount of KIAs and wounded and
the Aid Station was destroyed. MEDEVAC was not possible
for approximately 12 hours forcing CPT Cordova and his
medics to care for multiple critically wounded individuals while
simultaneously providing defensive fire to prevent COP Keating
to be completely overrun.
CPT Cordova is credited with saving the lives of 12
wounded Soldiers and even transfused blood from other
Soldiers during this action in order to maintain several
individuals that otherwise would not have survived that
extreme amount of time.
For the sixth time in 29 years an Army Ranger has
been selected as the US Army Surgeon General’s
Physician Assistant Recognition Award Winner. CPT
Andrew D. Fisher is assigned to 1st Battalion, 75th
Ranger Regiment, Hunter Army Airfield, Georgia. He
was selected for his bravery in combat and his life saving
skills. Read further on page 2.
General Stanley McCrystal
presents CPT Cordova his
Silver Star
Cordova Earns Silver Star
I N S I D E T H I S
Cordova earns
Silver Star
1
Surgeon General’s
PA of the Year
1/2
New PA Chief 3
New NG Chief 3
PAs in Command 4
Reserve Chief Bids
Farewell
5
Specialist Corps
Update
6
IPAP update 7
PA training of
Army Medics
8/9
News from Home 10
Ranger Selected Surgeon General’s PA of the Year
SAPA JOURNAL The Society of Army Physician Assistants
A Civilian Organization Representing Army PAs
M A Y / J U N E 2 0 1 0 Vol. 21, NO. 2 A P O I N T S O F
I N T E R E S T :
PA earns Silver Star
Surgeon General’s
PA of the Year
Newest Senior PA
Newest NG PA
PAs in Command
PO Box 07490
Fort Myers, FL 33919
Phone & Fax
239-482-2162
Article courtesy Major Kathy Schultz,
XO SP Corps

P A G E 2
“CPT Fisher
moved forward
to assist with
clearing the
objective. “
All The Way!
Ranger Receives Award (cont) Below is the nomination information provided to the SP Corps by the 75th Ranger
Regiment.
CPT Fisher distinguished himself throughout the inclusive dates as a Ranger
Physician Assistant who saved numerous lives on the battlefield in Afghanistan and
Iraq, during two separate combat deployments. His lifesaving interventions and
leadership provided during multiple intense firefights are shining examples of what a
Physician Assistant brings to the fight. He not only acted heroically in combat, his
daily performance as a health care provider, leader, and mentor to his medics directly
translates into his battalion having more combat power now and for the foreseeable
future.
On September 30, 2009, while deployed in support of OEF, CPT Fisher was
attached to a Ranger platoon during a raid. During their infiltration the platoon
received effect machine gun fire while sustaining one critically injured Ranger. CPT
Fisher provided lifesaving care and prepared the casualty for evacuation. As the
assault force moved toward the objective, a firefight ensued. The platoon medics
weapon malfunctioned and CPT Fisher moved forward to assist with clearing the
objective. During exfiltration, a Ranger stepped on a pressure plate IED and was
killed instantly. However, 6 Rangers were wounded , four critically. Without regard
for his own safety, CPT Fisher moved to the site and assisted with retrieval of the
wounded. He established a casualty collection point, triaged the wounded, and
performed numerous lifesaving medical interventions. He coordinated movement to
the CSH via tactical aircraft.
On 29 October, CPT Fisher responded to a downed Marine assault helicopter.
He established a CCP and provided lifesaving measures. His actions saved the lives
of 2 crew members. CPT Fisher lives the words of the Ranger Creed and exhibits the
Army Values. His dedication to Rangers and his medics is unsurpassed.
Courtesy 75th Ranger Regiment
S A P A J O U R N A L
New Physician Assistant Chief Announced
P A G E 3 V O L . 2 1 , N O . 2 A
The Surgeon General, has selected LTC John E. Balser to serve as the 6th
Chief of the Physician Assistant Section/Assistant Corps Chief of the Army
Medical Specialist Corps, as well as the Physician Assistant Consultant to the
Surgeon General.
LTC Balser is the commander of the 240th Forward Surgical Team (FST)
(ABN) Fort Bragg, NC, and currently deployed in support of Operation
Enduring Freedom. He succeeds COL Michael A. Robertson, currently the
commander of the 31st Combat Support Hospital, and also deployed in
support of Operation Enduring Freedom. LTC Balser will assume his new re-
sponsibilities no later than 20 July 2010.
LTC Balser has provided a message for distribution to Army PAs.
I am humbled to be chosen the new consultant and Deputy Corps Chief. As a
group, we have the most diverse background of various experiences that we
can bring to bear in support of the Warfighters. We are known as dependable
and willing to do the tough jobs. As a group, we work behind the scenes and
need to continue the outstanding job we do day in and day out providing the
best care we can to the Soldiers we support.
LTC Tanya F. Moore has been named the newest Reserve Component PA Chief.
Below is a brief biography.
LTC Tanya Moore was born in Greensboro, North Carolina. Her father was an Army Officer, thus she moved all
over the United States. She graduated from the University of North Carolina at Greensboro with a BS in Community
Health Education and received her Physician Assistant training at Wake Forest University. She was originally
commissioned a Second Lieutenant in the Signal Corps in 1982. She served as a platoon leader, company executive
officer in Heidelberg Germany and Schwabish Gmund Germany, Company Commander, Assistant S-3 at Fort Bragg,
NC, Training with Industry Hughes Aircraft Company, Fullerton California, and Project Officer at Fort Gordon,
Georgia. LTC Moore left active duty and joined the reserves in 1997. She then served as Executive Officer to the J-5
at US Space Command. She resigned her commission as a Signal Officer in 2000 and was reappointed as a First
Lieutenant in the Army Medical Specialist Corps. Her assignments include IMA to Evans Army Community Hospital,
mobilization as Chief of Military Medicine at DeWitt Army Community Hospital, Fort Belvoir Virginia, and Team
Leader with the 7225th Medical Support Unit in Greenville, South Carolina. Lieutenant Colonel Moore holds a
Bachelor of Science Degree in Community Health Education, Physician Assistant certification from Wake Forest
University, and a Masters of Medical Science in Hospital Medicine and Critical Care from Alderson Broaddus College.
LTC Moore’s awards and decorations include the Bronze Star, the Army Commendation Medal (6th Award), Army
Achievement Medal (4 Oak Leaf Clusters), National Defense Service Medal with Bronze Star, South West Asia Service
Medal with three Bronze Service Stars, Kuwait Liberation Medal (Kuwait), Kuwait Liberation Medal (Saudi Arabia),
Global War on Terrorism Service Ribbon, Armed Forces Reserve Medal with M Device (2nd Award), Overseas Service
Ribbon, Armed Forces Reserve Medal with Ten Year device and the Parachutist Badge. She currently resides in
Greensboro, North Carolina with her husband and her three daughters.
New Reserve Component PA Chief
“ I
represent
all of you
and in
order to
go
forward, I
will need
your
input”
LTC Balser
LTC Balser (black shirt) directing his
FST staff during a trauma event

P A G E 4
COL Piper Bids Farewell COL Frank Piper, Reserve Component PA is retiring after 28 years of service. The
SAPA staff wishes him happiness and prosperity in life and all future endeavors.
Below is a farewell message from the chief.
Having served in this capacity for the past 2 1/2 years, I have enjoyed every
minute. While officially retired, I hope to keep in touch and maintain the friendships
I have been honored to have over the past 28 years of my Army Reserve career.
Frank Piper, MS, MPAS, PA-C
COL (R) USAR
COL Piper has provided a duty description for the Reserve Component PA
Consultant, which is presented below.
His duties and now those of LTC Moore include being a Drilling Individual
Mobilization Augmentee (DIMA) to the PA Corps providing leadership / mentorship
to RC Physician Assistants , and is a liaison between the Army Reserve PAs and the
AC Physician Assistant Consultant to the OTSG. He/she serves as the senior PA RC
representative to the PA Section Chief on all issues related to RC PA manage-
ment The DIMA serves as liaison between RC PAs and RC Corps Chief on all things
affecting 65Ds. Other important duties include establishing and maintaining formal
and informal communications with the RC PA community and the PA Section Chief,
participating in the development and implementation with the SP Strategic Plan and
Balanced Scorecard as appropriate, and in conjunction with SP XO and IMA to the
Chief of the SP Corps maintain a database of mobilized/deployed SP PAs in support of
GWOT, OIF, OEF. He/she also coordinates issues of RC force structure with AC
Chief PA and RC rep at APPD.
S A P A J O U R N A L

P A G E 5
COL Michael A.
Robertson, PA-C,
commander of the
31st Combat Support
Hospital (CSH), Fort
Bliss, TX, has recently
deployed February
2010 in support of
Operation Enduring
Freedom.
COL Michael A. Robertson receiving a
thank you gift from the Commander of an ANA Soldier who had a head injury and was cared for at the Kandahar Regional
Medical Hospital
LTC Balser First PA to Command FST in Combat
COL Robertson First PA to Command CSH in Combat
LTC Balser is the commander of the 240th Forward Surgical Team (FST) (ABN) Fort Bragg, NC, and currently deployed in
support of Operation Enduring Freedom. He
succeeds COL Michael A. Robertson, currently the commander of the 31st
Combat Support Hospital, and also deployed in support
of Operation Enduring Freedom.
S A P A J O U R N A L
COL Robertson and staff visit
Kandahar Regional Medical Hospital
LTC Balser (third from left) and his Forward Surgical Team
Iron Majors
P A G E 6 V O L U M E 1 , I S S U E 1
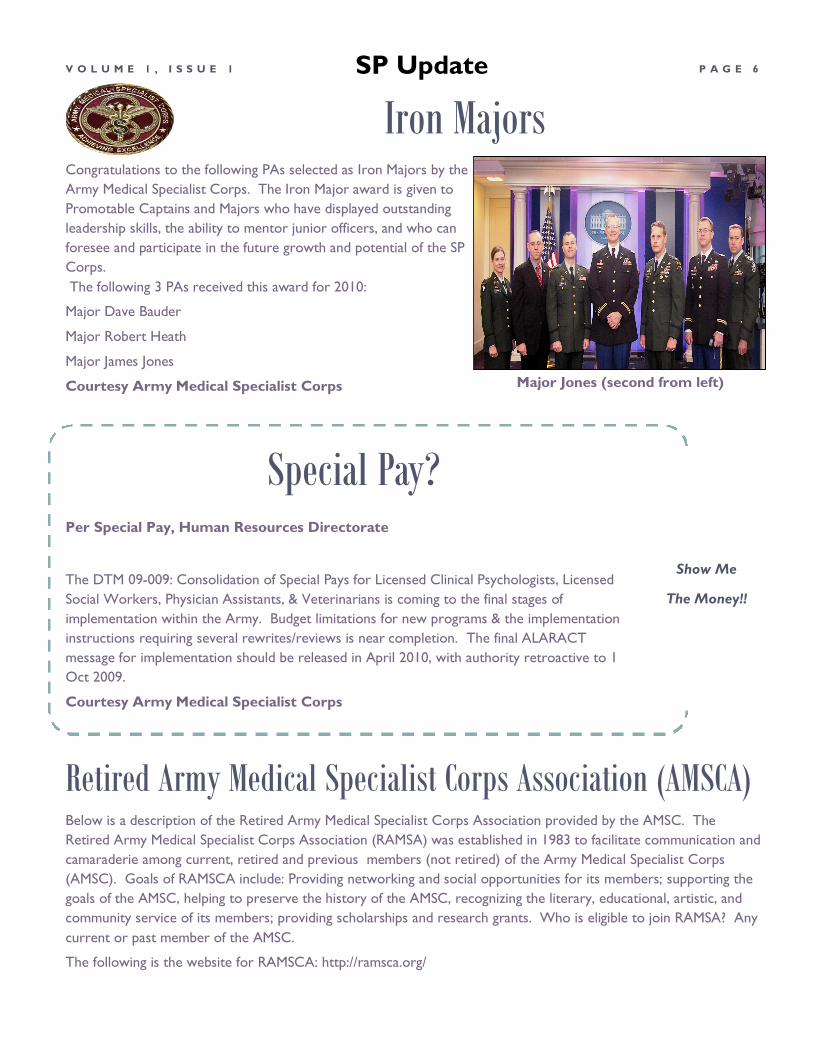
Congratulations to the following PAs selected as Iron Majors by the
Army Medical Specialist Corps. The Iron Major award is given to
Promotable Captains and Majors who have displayed outstanding
leadership skills, the ability to mentor junior officers, and who can
foresee and participate in the future growth and potential of the SP
Corps.
The following 3 PAs received this award for 2010:
Major Dave Bauder
Major Robert Heath
Major James Jones
Courtesy Army Medical Specialist Corps
Below is a description of the Retired Army Medical Specialist Corps Association provided by the AMSC. The
Retired Army Medical Specialist Corps Association (RAMSA) was established in 1983 to facilitate communication and
camaraderie among current, retired and previous members (not retired) of the Army Medical Specialist Corps
(AMSC). Goals of RAMSCA include: Providing networking and social opportunities for its members; supporting the
goals of the AMSC, helping to preserve the history of the AMSC, recognizing the literary, educational, artistic, and
community service of its members; providing scholarships and research grants. Who is eligible to join RAMSA? Any
current or past member of the AMSC.
The following is the website for RAMSCA: http://ramsca.org/
Per Special Pay, Human Resources Directorate
The DTM 09-009: Consolidation of Special Pays for Licensed Clinical Psychologists, Licensed
Social Workers, Physician Assistants, & Veterinarians is coming to the final stages of
implementation within the Army. Budget limitations for new programs & the implementation
instructions requiring several rewrites/reviews is near completion. The final ALARACT
message for implementation should be released in April 2010, with authority retroactive to 1
Oct 2009.
Courtesy Army Medical Specialist Corps
Special Pay?
Retired Army Medical Specialist Corps Association (AMSCA)
Show Me
The Money!!
SP Update
Major Jones (second from left)
P A G E 7
”our next move was
to extend the
length of the
program from 24 to
29 months.”
Interservice Physician Assistant Program Update
Update from the Interservice Physician Assistant Program
For those of you have not visited the “Schoolhouse” in a few years, there are some big
changes at the IPAP. We have dramatically increased the size of the program, which has
resulted in several changes. In 2007, the Army, Navy, Air Force and Coast Guard all came
to us stating they needed increased graduates. The increased need came from the wartime
demand and the fantastic job the PAs were doing down range. Of course, PA excellence
on the battlefield comes as no surprise to you.
We gained approval from the Health Care Interservice Training Advisory Board (HC
ITAB) that oversees our multiservice program to expand class sizes from 60 to 80
students, an increase of 60 more students starting the program each year. In order to do
this, we needed larger classrooms and laboratory space. By the end of 2008, we had two
new classrooms that seated 100 students. We also had three additional rooms with exam
tables, and oto-ophthalmoscopes to train 100 students at a time. Each of the three lab
rooms also had a Smart board at the end to allow video and interactive web utilization.
The staff has also grown. We now have 14 Army, 5 Air Force, 3 Navy, 1 Coast Guard and
6 civilian faculty. Maria Charles has many more PAs to keep in line now. This expansion
preparation was accomplished during 2008 and in January, 2009, we started training 123
RA, 30 ARNG, 9 USAR, 37 USAF, 29 USN and 4 USCG students. These classes are
spread out over three trimesters, just as before. We have not changed the curriculum,
though we have added more labs to many of the classes that emphasize problem based
learning as opposed to pure didactic (PowerPoint) instruction.
Our next move will be to extend the length of the program from 24 to 29 months.
Medical education has increased at a tremendous rate. Most all civilian PA programs now
average 29 months in length. Our faculty took a critical look at our curriculum and
determined that 33 credits per semester or 100 semester hours in one year was too
much, too fast. Rather than cut back on any classes, we proposed to HC ITAB that we
add another semester to the first year that allows the coursework to be spread out. We
also proposed adding another month to the clinical phase to accommodate increased
hospital education requirements and provides time for leave during the second year.
Students will have more study time and not just prepare each day for the next test. Also,
in a time where military families are stressed by wartime missions (60% of our students are
OIF/OEF veterans) we need to allow more time for maintaining the family. The HC ITAB
members approved the extension to 29 months on March 26th, 2010. The change also
means that as we continue to start a class every four months, we will end up with four
classes at FSH for Phase 1. The AMEDDC&S will now have to prepare a fourth classroom.
Other work must be done, but for the most part the only visible changes will be students
attending four semesters with a shortened day of classes and more study time.
COL William Tozier,
Director IPAP
S A P A J O U R N A L
Training and Sustaining 68Ws: The Physician Assistants Role
P A G E 8 V O L U M E 1 , I S S U E 1
The backbone of Army Medicine, particularly in a deployed environment, is the 68W Health Care Specialist. These
combat medics are trained in a 16 week training program at Fort Sam Houston. The Department of Combat Medic
Training trains approximately 8000 68W students per year in this course. Students are taught over 140 different
critical skills during this training program. They begin with six weeks of Emergency Medical Technician-Basic training,
and must successfully complete the National Registry of Emergency Medical Technicians-Basic examination. Following
the EMT portion of the course the students then enter the Tactical Medicine portion of the course. These 10 weeks of
training begin with the basic understanding of how the environment differs in a tactical situation versus a civilian
scenario.
Medics are given numerous lectures to understand the knowledge basis of the MOS. However, the primary focus is on
learning and becoming proficient in the many hands-on skills required to save lives on the battlefield. Consequently,
with a limited number of military instructors we must ensure that each student has been trained and validated on each
of the skills needed to save lives in combat. Being trained during Initial Entry Training does not make these individuals
proficient in these skills over time. It will require additional training in their unit to fully grasp and maintain their skills. I
recall the days when all of my medics were tasked out to perform jobs and details that were not medical in nature.
Many hours spent in the motor pool did not make these individuals more competent and confident in their medical
skills. It becomes imperative that the unit medical officer continue this training and validation of skills as time goes by
and the medic migrates away from the learning environment and more towards the general life of a garrison Soldier.
This brings me to my next point. Over the past 5-6 years we have seen a trend for the enlisted medic to have to take
on more roles of an independent practitioner. That lone medic with a forward platoon on a Contingency Operating
Base, the sole medic in support of an isolated artillery battery, or the transition team medic who is the sole provider
for his team is sometimes the only medical provider in the area. This is not a role the 68W is trained for. In addition to
providing life saving care for traumatic injuries they have the day to day function of the “Doc” for routine sick call
problems. How do they develop these skills? We used to have Medical Proficiency Training (MPT) where the medics
would spend 60-90 days at the hospital or clinic to gain additional medical knowledge that they were not getting in the
battalion. However, I don’t believe this program still exists, and if it does, the limited scope of practice of the 68W in a
MTF precludes them from being fully utilized and learning new Primary Care skills.
Most unit medical officers (Physician Assistants) are assigned to a maneuver or support battalion. While in garrison,
they are frequently required or tasked to work in the Troop Medical Clinic or one of the Family Medicine Clinics on
post. While this is technically a MEDDAC function they frequently utilize division assets for the bulk of troop medicine.
So if the battalion medical officer is at the TMC seeing patients, how are the unit medics getting trained? Not only do
they need to sustain their trauma skills, but how do they learn the skills necessary to provide routine sickcall to
Soldiers in their unit? The unit leadership must realize this valuable asset is being supplanted to support other organi-
zations which is detrimental to the battalion. Command leaders from the Battalion, Brigade, and even the Division
Surgeon must weigh in and insure the medical assets organic to the maneuver units are available to provide training and
guidance to unit medical assets. If the unit has an organic battalion aid station or medical company, then the medics
must work with the PA or MD in the unit area to learn the necessary fundamentals to understand an independent type
of practice and know when someone is really ill and needs evacuation, or has a minor illness they can take care of.
The Department of Combat Medic Training provides a week long program in “Limited Primary Care”. The students
LTC (Retired) Don Parsons

P A G E 9
“The long tradition of
enlisted medics
progressing up
through the ranks and
eventually applying
for and being
selected for PA school
has gone the way of
the dinosaur.”
Combat Medic Training (continued) get classes on medical documentation, EENT disorders, abdominal disorders, respiratory
disorders, MS disorders, and even some dermatology. However, this is really just the basics.
Providing care in the unit area gives the medic the ability to work with the unit medical officer
and observe his technique. Classes by the unit medical officer on different disorders, history
taking, and physical exam techniques are all areas medics need work on. If the medical officer
does not provide this training then a lot more Soldiers will enter the evacuation channels. In my
last field assignment I was the PA in a Field Artillery Battalion. We had a small area in the base-
ment of the barracks where we conducted sickcall every day. I did not have an office but
worked among the several cubicles we had to see patients in (This was in the days before
ALTHA). The medics would get the chart with vital signs recorded and start the subjective and
objective part of the exam. I would come by and consult with the medics on what they had
asked and recorded in the way of physical findings. We would then go into a little more depth
of history and physical exam so they could observe how I conducted a history and physical.
This way they learned to perform these skills themselves. We went over a treatment plan to
include medications and disposition of the Soldier so that they started to develop some
capabilities and confidence in their skills. This paid big dividends when we deployed or even
went to the field. I didn’t have to see every sore throat or knee pain, unless the medic had
some question about the patient that they were not comfortable with. Today many of the unit
PA’s are too busy in the MEDDAC clinic to train their medics. They seldom give classes on
medication, or the proper way to examine a knee. How then do we expect these medics to
develop skills to provide care to the Soldiers in their unit?
I understand all about JACHO and the regulations that govern patient care. However, in a
deployed environment the unit medical officer cannot be everywhere that the Soldiers are.
Who is going to take care of them if they get injured or ill? The medic who is out there with
them will have that responsibility, and it is our job to train them to be able to provide capable
and competent care in any situation. Battalion PAs must schedule time in their unit to train their
medics, and validate their skills; this should be reinforced by both the Brigade Surgeon and the
Division PA and Surgeon.
The long time tradition of enlisted medics progressing up through the ranks and eventually
applying for and being selected to PA school has gone the way of the dinosaur. Today the
selectees are primarily officers from backgrounds other than medical, and they do not have the
same tradition of ensuring the enlisted medics are fully trained to care for Soldiers in an isolated
assignment. In fact, many of these candidates have never performed the functions of a medic. It
is time for PAs to relook at the training and sustainment of the enlisted medic. Unit medical
officers must make this a priority in their already busy daily schedule. The medical platoon
leader needs to ensure his personnel are getting the training they need to sustain their skills.
Without this continued training and sustainment these fine Soldiers will not be able to reach
their full potential. LTC (R) Donald Parsons is the former director IPAP.
S A P A J O U R N A L
News from Home
P A G E 1 0 V O L U M E 1 , I S S U E 1
Retirements
Promotion/Recognition
Special events/Occasions/Training
This section is under construction
and requires input from SAPA
members.
SAPA OFFICERS SOCIETY OF ARMY PHYSICIAN ASSISTANTS
P O Box 07490, FT. MYERS, FL 33919-6402
Phone and Fax - 239-482-2162
Executive Director: Harold E. Slusher, PA-C
Address and phone as above, e-mail - [email protected]
SAPA Web Page: http://www.sapa.org (Webmaster: Orie Potter)
PRESIDENT Stephen W. Ward, PA-C
email: [email protected]
PRESIDENT ELECT Sherry Womack, Major, SP, PA-C
IMMEDIATE PAST PRESIDENT Pat Malone PA-C
SECRETARY Karen McMillan, PA-C
email: [email protected]
TREASURER James L.C. Miller, PA-C
e-mail - [email protected]
DIRECTOR, ACTIVE DUTY ARMY PAs Theresa Martin, Capt., SP, U.S. Army
DIRECTOR, US ARMY NATIONAL GUARD PAS Nolan Wright, Capt., Texas State Army National Guard
e-mail:
DIRECTOR, US ARMY RESERVE PAS LTC (R) Frank Piper, Jr., PA-C
e-mail; [email protected]
MEMBERSHIP DIRECTOR Paul Lowe, PA-C
EMAIL: [email protected]
SAPA CONFERENCE STAFF CONFERENCE COORDINATOR: Bob Potter, PA-C
PO Box 623
2Monmouth, IL 61462
SAPA Voice Line: 309-734-5446
Fax: 309-734-4489
e-mail: [email protected]
CONFERENCE REGISTRAR: Bob Potter, PA-C Info for Bob Potter same as immediately above
ASST. CONFERNECE COORDINATOR: David M. Paulson, PA-C
e-mail: [email protected] CO-REGISTRAR: Judy Potter
DECORUM AND MORALE: Nicole Potter
e-mail: [email protected] SALES AND MARKETING: Stephen Ward, PA-C,
Bob Egbert, PAC, Tom Matherly, PA-C
MODERATORS/AUDIO/VISUAL: LCDR Irwin Fish, PA-C
SAPA JOURNAL STAFF Editor: Major John F. Detro, MPAS, PA-C
email: [email protected]
COMMITTEES SCHOLARSHIPS/AWARDS
LTC-R Donald Parsons, PA-C (Chair) COL -R Sherry Morrey, PA-C CW4-R Marvin W. Cole, PA-C
LTC Donald Black, SP, PA-C POC for Captain Sean P. Grimes
Physician Assistant Educational Scholarship Award)
email: [email protected]
SAPA HISTORIAN William Long, PA-C
MINORITY AFFAIRS Karen McMillan, PA-C
PUBLIC EDUCATION Harold E. Slusher, PA-C
PROFESSIONAL WELLNESS Michael Champion, PA-C
LEGISLATIVE AFFAIRS Harold E. Slusher, PA-C
DELEGATES TO AAPA HOUSE OF DELEGATES Pat Malone, PA-C (Chief Delegate)
Stephen W. Ward, PA-C
ACADEMY LIASON COL Pauline Gross, SP, PA-C
e-mail: [email protected]
COMMUNICATIONS/ELECTRONICS Stephen Ward, PA-C
Irvin Fish, PA-C
Bob Potter, PA-C
The SAPA Journal staff and SAPA Board of Directors encourages membership participation in this publication. Feel free to use this
forum to present your views on any topic you desire. The publication of clinical articles on any subject is also solicited, however, to reduce
our workload, we do request articles be presented typed, double-spaced format, and on CD, Microsoft Word format. The editor
reserves the right of final acceptance of articles as well as the right to serialize articles which are too lengthy to be included in a single issue.
Articles will be accepted via email.
The SAPA Journal is the official publication of the Society of Army Physician Assistants. The views and opinions expressed herein are not
necessarily those of the editors, SAPA, the SAPA Board of Directors or the Department of the Army unless explicitly expressed as such.
This is not an official Army Publication.





























