Embed Size (px)
Citation preview
1
Module on Childhood Diarrhea
Part 4 – Sanitation and HygienePart 4 Sanitation and Hygiene----------------------------------------------------
Mduduzi Mbuya, PhDZVITAMBO Study Group
April 20, 20101
Sanitation & Hygiene:Designing an intervention in rural Zimbabwe
Introduction to Global Health
April 20, 2010
Mduduzi Mbuya
ZVITAMBO Study Group
Lecture roadmap
• Global trends in sanitation• The scale of the challenge• Implications
• Climbing the sanitation ladderClimbing the sanitation ladder• Sanitation ladder?• How is the world doing?
• Basic considerations in sanitation intervention
• Designing a sanitation and hygiene intervention in Zimbabwe
The scale of the challenge
• 2.6 billion people – four in ten people in the world – do not use improved sanitation
• 884 million people do not use improved sources of drinkingimproved sources of drinking water
• Every day, diarrhoeal disease kills 5,000 children.
• Every week, it kills 42,000 people.
• Every one of these deaths is tragic – and preventable.
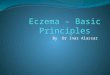
The global picture
Total Sanitation Coverage 2006
Less than 50%50 – 75%76 – 90%91 – 100%No or Insufficient data
Sources: World Health Organization and United Nations Children's Fund Joint Monitoring Programme on Water Supply and Sanitation (JMP). Progress on Drinking Water and Sanitation: special focus on sanitation. UNICEF, New York, and WHO, Geneva, 2008.
The good news
• Coverage in the developing world has increased from 41% to 53% (1990 -> 2006)
⇒1.1 billion people gained access!
• Coverage in South-eastern and Eastern Asia increased 17%Coverage in South eastern and Eastern Asia increased 17%
• Many countries are making rapid progress, despite initial low coverage and rapid population growth:
– Vietnam: 47 percent of the population gained access to sanitation (1990-2006).
– Philippines: 43%; Pakistan: 40%; Benin: 30%; Cameroon and Mali: 29%
Sources: World Health Organization and United Nations Children's Fund Joint Monitoring Programme on Water Supply and Sanitation (JMP). Progress on Drinking Water and Sanitation: special focus on sanitation. UNICEF, New York, and WHO, Geneva, 2008.
2
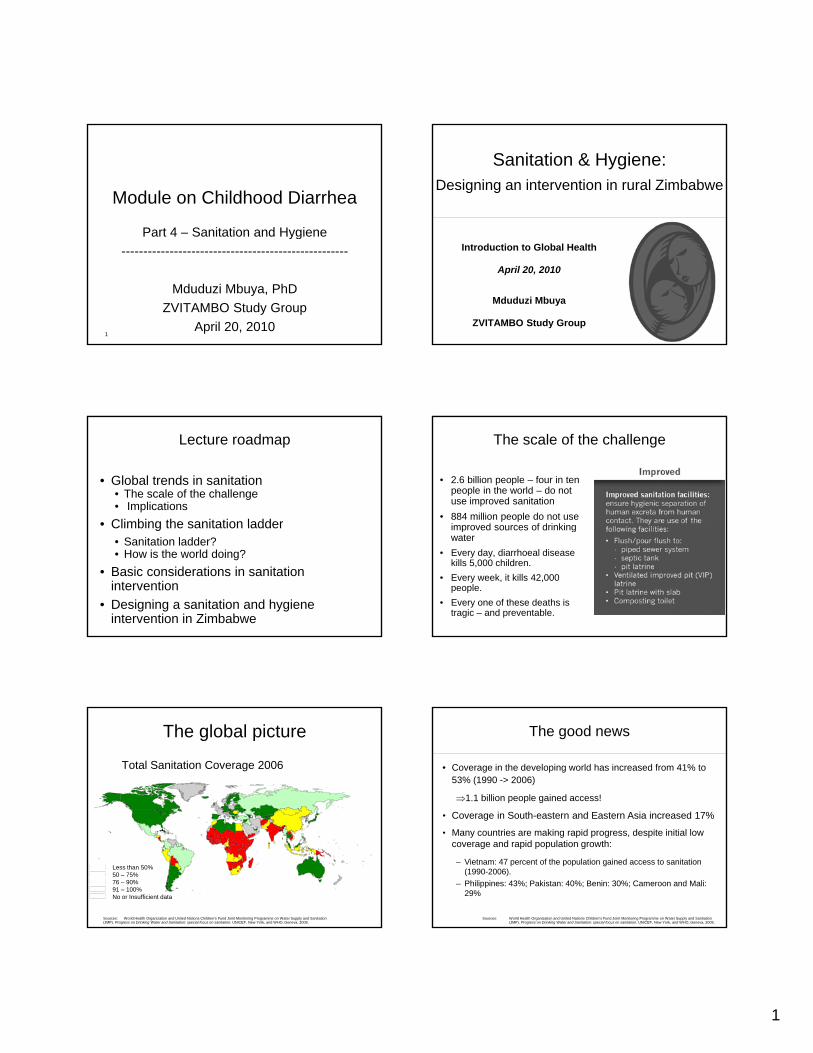
The bad news
• Sub-Saharan Africa recorded least progress – only 5%: from 26 (1990) to 31 percent (2006).
• Southern Asia recorded moderate progress – 12 percent: from 21% (1990) to 33% (2006).21% (1990) to 33% (2006).
• The majority of people without sanitation live in Asia (70%) and Sub-Saharan Africa (22 %).
• The world is not on track to meet the MDG sanitation target. At the current rate, we will miss the target by over 700 million people.
Sources: World Health Organization and United Nations Children's Fund Joint Monitoring Programme on Water Supply and Sanitation (JMP). Progress on Drinking Water and Sanitation: special focus on sanitation. UNICEF, New York, and WHO, Geneva, 2008. WHO & Unicef JMP, 2010.
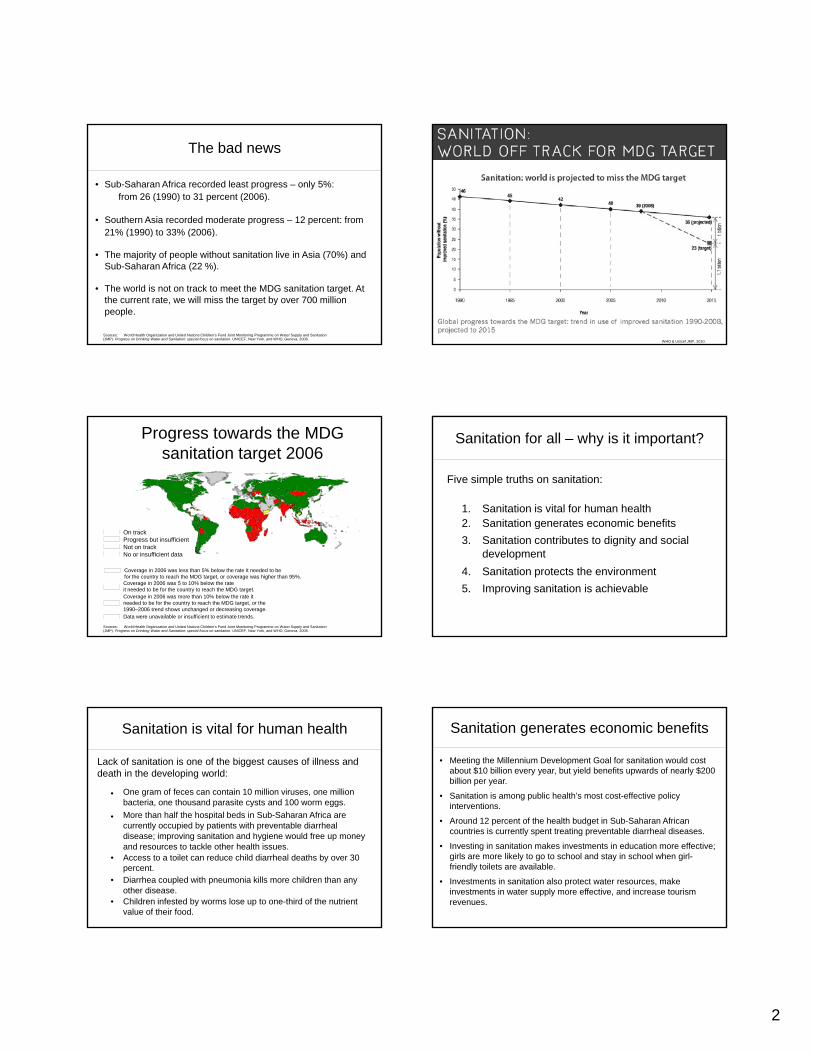
Progress towards the MDG sanitation target 2006
On trackProgress but insufficientNot on trackNo or insufficient data
Coverage in 2006 was less than 5% below the rate it needed to be for the country to reach the MDG target, or coverage was higher than 95%.Coverage in 2006 was 5 to 10% below the rate it needed to be for the country to reach the MDG target.Coverage in 2006 was more than 10% below the rate it needed to be for the country to reach the MDG target, or the 1990–2006 trend shows unchanged or decreasing coverage.Data were unavailable or insufficient to estimate trends.
Sources: World Health Organization and United Nations Children's Fund Joint Monitoring Programme on Water Supply and Sanitation (JMP). Progress on Drinking Water and Sanitation: special focus on sanitation. UNICEF, New York, and WHO, Geneva, 2008.
Sanitation for all – why is it important?
Five simple truths on sanitation:
1. Sanitation is vital for human health2. Sanitation generates economic benefits2. Sanitation generates economic benefits3. Sanitation contributes to dignity and social
development4. Sanitation protects the environment5. Improving sanitation is achievable
Sanitation is vital for human health
Lack of sanitation is one of the biggest causes of illness and death in the developing world:
One gram of feces can contain 10 million viruses, one million bacteria, one thousand parasite cysts and 100 worm eggs.More than half the hospital beds in Sub-Saharan Africa areMore than half the hospital beds in Sub Saharan Africa are currently occupied by patients with preventable diarrheal disease; improving sanitation and hygiene would free up money and resources to tackle other health issues.
• Access to a toilet can reduce child diarrheal deaths by over 30 percent.
• Diarrhea coupled with pneumonia kills more children than any other disease.
• Children infested by worms lose up to one-third of the nutrient value of their food.
Sanitation generates economic benefits
• Meeting the Millennium Development Goal for sanitation would cost about $10 billion every year, but yield benefits upwards of nearly $200 billion per year.
• Sanitation is among public health’s most cost-effective policy interventions.
A d 12 t f th h lth b d t i S b S h Af i• Around 12 percent of the health budget in Sub-Saharan African countries is currently spent treating preventable diarrheal diseases.
• Investing in sanitation makes investments in education more effective; girls are more likely to go to school and stay in school when girl-friendly toilets are available.
• Investments in sanitation also protect water resources, make investments in water supply more effective, and increase tourism revenues.
3
Sanitation contributes to dignity and social development
• 1.2 billion people defecate in the open, exposing themselves to ridicule, shame; and, for women and girls, the risk of attack.
• Within thirty years, UN-Habitat estimates that one in three people in the world will live in a slum. Without adequate sanitation, they will live surrounded by human filth.
Sanitation protects the environment
Investments in sanitation protect vital natural resources, keep rivers and coastal seas clean, and reduce degradation of productive land and fisheries:
• Worldwide, every year more than 200 million tonnes of , y yhuman waste and vast quantities of solid waste and wastewater remain untreated.
• In Southeast Asia 13 million tons of feces are released to inland water sources each year, along with 122 million m3 of urine and 11 billion m3 of gray water.
The sanitation ladder The sanitation ladder
The sanitation ladder
Proportion using an improved, shared or unimproved sanitation facility or practicing open defecation, by MDG region, in 1990 and 2008
Designing a sanitation and hygiene intervention in Zimbabwe
Pop: 12.5 million~ 70% rural
2008: 25% OD, 7% Unimproved, 24% Shared, 44% Improved
4
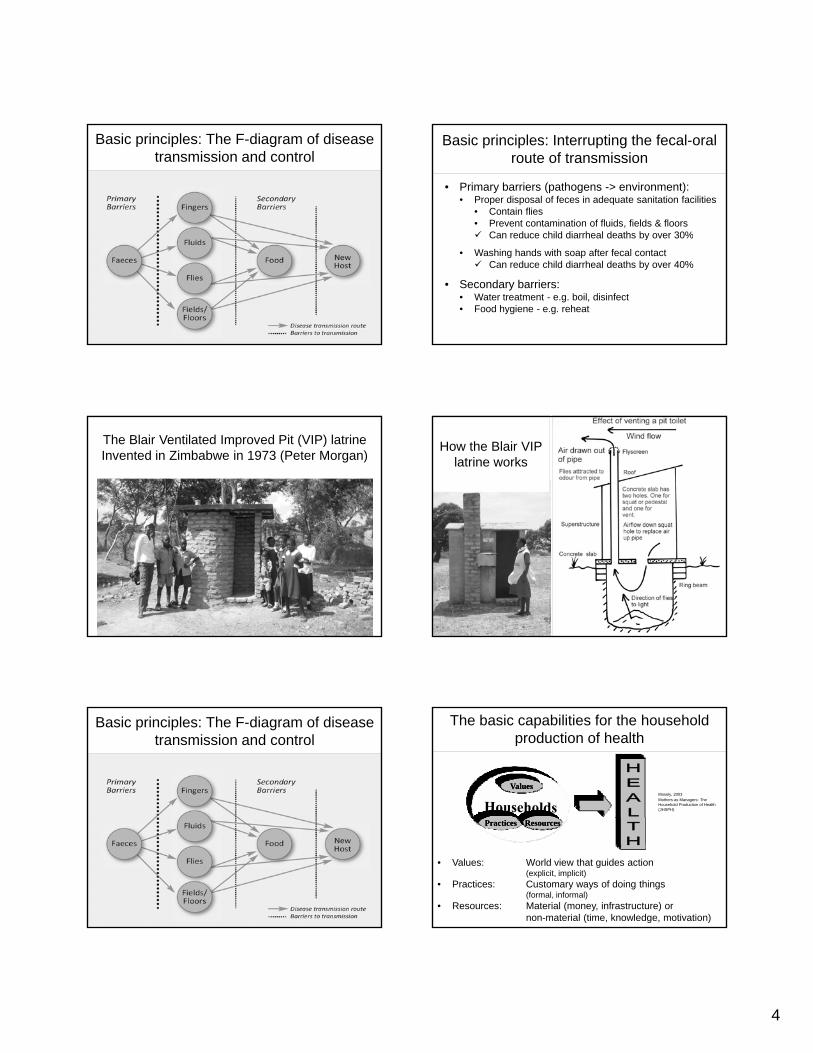
Basic principles: The F-diagram of disease transmission and control
Basic principles: Interrupting the fecal-oral route of transmission
• Primary barriers (pathogens -> environment):• Proper disposal of feces in adequate sanitation facilities
• Contain flies• Prevent contamination of fluids, fields & floors
Can reduce child diarrheal deaths by over 30%Can reduce child diarrheal deaths by over 30%
• Washing hands with soap after fecal contactCan reduce child diarrheal deaths by over 40%
• Secondary barriers: • Water treatment - e.g. boil, disinfect• Food hygiene - e.g. reheat
The Blair Ventilated Improved Pit (VIP) latrineInvented in Zimbabwe in 1973 (Peter Morgan)
How the Blair VIP latrine works
Basic principles: The F-diagram of disease transmission and control
ValuesValues
The basic capabilities for the household production of health
Mosely, 2003Mothers as Managers: The Household Production of Health(JHSPH)
PracticesPractices ResourcesResources
• Values: World view that guides action(explicit, implicit)
• Practices: Customary ways of doing things(formal, informal)
• Resources: Material (money, infrastructure) or non-material (time, knowledge, motivation)
5
Hygiene and Sanitation Formative Research
• Chirumanzu district, Zimbabwe• Mostly rural
• Sanitation coverage ~ g30%
• Water coverage ~ 80%
Research aim and objectives
• To inform the development of a hygiene and sanitation intervention• Document current practices
Di l f fDisposal of fecesHandwashing, particularly after fecal contactWater use and treatment
• Document constraints to improved practices• Pilot improved sanitation and hygiene
practices
Methods: Exploration
• 21 households• With child 0-18 mos• Mother = primary respondent
• Direct observations: • Living environment -
cleanliness sanitary facilitiescleanliness, sanitary facilities• Key behaviors (water
handling, handwashing, fecal contact)
• Observation checklists• ~3 hours
• In-depth Interviews with caregiver• Detailed narrative report• ~1 hour
Methods: Trials of Improved Practices (TIPs)
(Dickin, Griffiths & Piwoz, 1997)
• Consultative research approach• Adaptation of recommendations to suit context• Understand motivations and constraints to behavior change
StSteps1. Problem identification through exploratory research (e.g.
observation and interviews)2. Prioritization of problems3. Counseling/negotiation on new/improved practices for
trial 4. Review of progress in implementing (trying and adopting)
new/improved behaviors5. Development of messages and delivery mechanisms
Sanitation
• BEFORE TIPS:• 4 owned a toilet
• All without wanted one• Lacked resources to construct one
• 1 used a neighbor’s toilet• 15 OD• 6 discarding water from washing baby
nappies in pit or field
Disposal of Stool
• Adult stool “more offensive” than baby stool• Baby stool less infectious, smaller, easier on the
eyes…“Once baby poo dissolves in water, it is not very infectious; one can just throw the dirty water in the open”j y p
• Sometimes difficult to find a place to OD• Few bushy areas in some villages
• Burying stools is difficult because the ground is hard
• Using the bush impinges on one’s dignity• Main reason to have toilet is reduce diarrhea, esp
cholera
6
Disposal of Stool
• Animal stool not frequently or consistently disposed of• Most homesteads are
t f d d tinot fenced - domestic animals can access the clean living areas
•Chickens in particular roam free•Cow dung used to polish hut floors
Improved Practices Identified for Trial:Disposal of Human and Animal Feces
Ideal• Dispose all human feces and dirty nappy water in toilet at
all times. If no toilet, bury stool.• Corral domestic animals or keep them away from clean
area of the yardy
Specific recommendations• Designate a hoe for burying stool and store at an
accessible place• Corral animals outside clean section of the yard• Remove animal stools promptly and bury them in rubbish
pit or field
Sanitation
• AFTER TIPS:• 7/14 without toilet constructed a temporary toilet• 2/14 preparing to construct (dug pit, burned bricks)• 1/14 now using neighbor’s toilet• 5 designated a hoe for stool burial• 2 refused to bury (“its embarassing to carry a hoe” ….”pigs
dig up the buried poo so its not worth burying”
• The concept of a temporary toilet was new.
• “All the individual holes we have been digging to bury stool could have mounted up to digging a temporary toilet had I known of the concept earlier.”
7
• One month after TIPS, 20 additional families that were not in the TIPs study but lived near a TIPs family had also built a temporary toilet.
More amazing to us:
p y
Handwashing
• BEFORE TIPS:• 19/21 washing in still water especially when alone• 11/21 use “run-to-waste” when someone can pour for
them• 14 were using soap• 6 used soap or ash• 5 used no rubbing agent
However, from observation:
Potential handwashing events Potential handwashing events
8
Handwashing
• 76% of households (16/21) had at least some soap• Used for:
•Washing dishes (12/16)Laundry (7/16)•Laundry (7/16)
•Bathing (7/16)•Handwashing (4/16)
• Use by children is minimal/restricted (valuable commodity)
• Handwashing before eating is considered a must• Wide preference NOT to use soap before eating
• Mothers often poured water for everyone else, then washed in still water
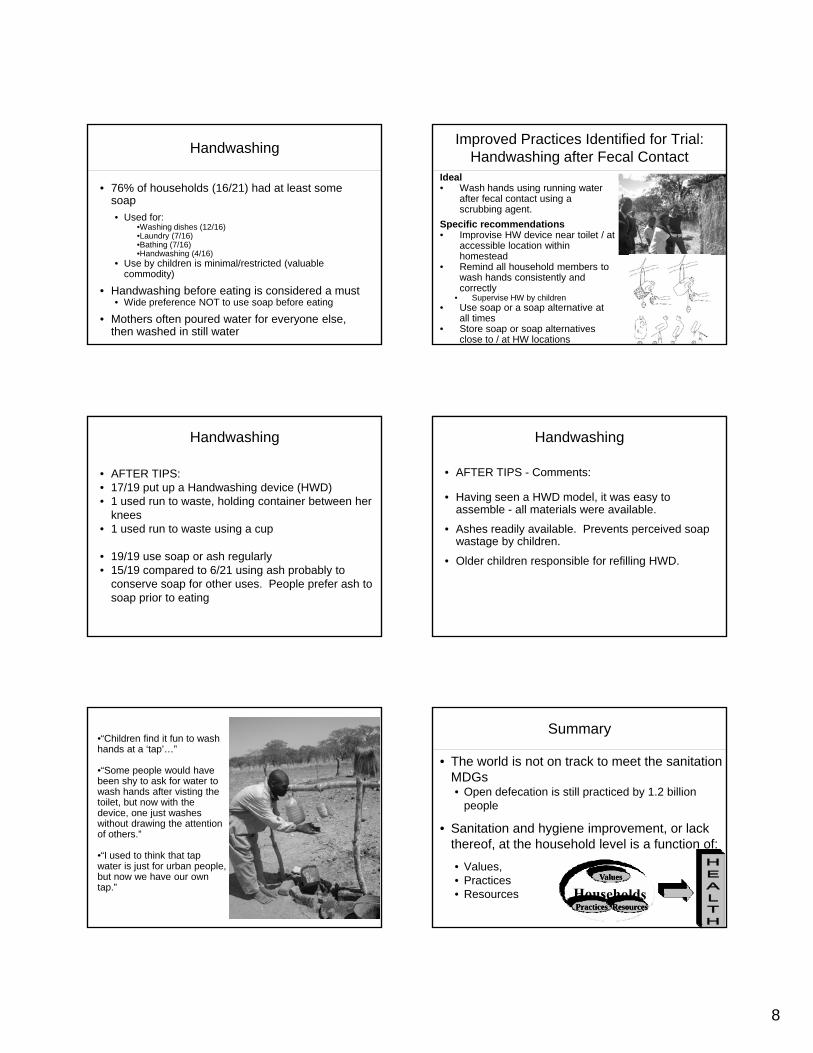
Improved Practices Identified for Trial:Handwashing after Fecal Contact
Ideal• Wash hands using running water
after fecal contact using a scrubbing agent.
Specific recommendations• Improvise HW device near toilet / at• Improvise HW device near toilet / at
accessible location within homestead
• Remind all household members to wash hands consistently and correctly
• Supervise HW by children• Use soap or a soap alternative at
all times• Store soap or soap alternatives
close to / at HW locations
Handwashing
• AFTER TIPS:• 17/19 put up a Handwashing device (HWD)• 1 used run to waste, holding container between her
knees1 d t t i• 1 used run to waste using a cup
• 19/19 use soap or ash regularly• 15/19 compared to 6/21 using ash probably to
conserve soap for other uses. People prefer ash to soap prior to eating
Handwashing
• AFTER TIPS - Comments:
• Having seen a HWD model, it was easy to assemble - all materials were available.
A h dil il bl P t i d• Ashes readily available. Prevents perceived soap wastage by children.
• Older children responsible for refilling HWD.
•“Children find it fun to wash hands at a ‘tap’…”
•“Some people would have been shy to ask for water to wash hands after visting the toilet, but now with the device, one just washes jwithout drawing the attention of others.”
•“I used to think that tap water is just for urban people, but now we have our own tap.”
Summary
• The world is not on track to meet the sanitation MDGs• Open defecation is still practiced by 1.2 billion
people
• Sanitation and hygiene improvement, or lack thereof, at the household level is a function of:
• Values,• Practices • Resources
ValuesValues
PracticesPractices ResourcesResources

9
Summary
• Explorative study can reveal the sociocultural construction of health behaviors:• Values:
• Would like to have a toilet• Cleanliness held in high esteem• Privacy (stigma around toilet use)• Patriarchal systems; status based
• Resources• Know of the benefits of sanitation and hygiene• Lack money to construct “ideal” toilets• Motivated to prevent disease
• Practices:• Make rational decisions
• Specific targeted messages with demonstration, as appropriate, can be used to negotiate incremental or large-scale change in S&H behavior
Thank you!! Siyabonga!! Tatenda!!