Embed Size (px)
Citation preview
CODING and BILLINGAm I Being Paid Appropriately?
Sandra M. Nettina, MSN, CRNPPresident, NPAM
Nurse Practitioner, Columbia Medical Practice
CODINGICD-9 International Classification of
DiseasesPublished by United States GovernmentDiagnoses basedAssign codes to your assessment at the highest
level of differentiationCPT Current Procedural Terminology
Copyrighted by American Medical AssociationProcedural rather than disease or disorder
Coding (cont.)ICD-9 codes are used to justify
medical necessity of a serviceCPT codes are used for billingEvaluation and management codes
(E&M) are CPT codes that describe consultations, ER, and office visits
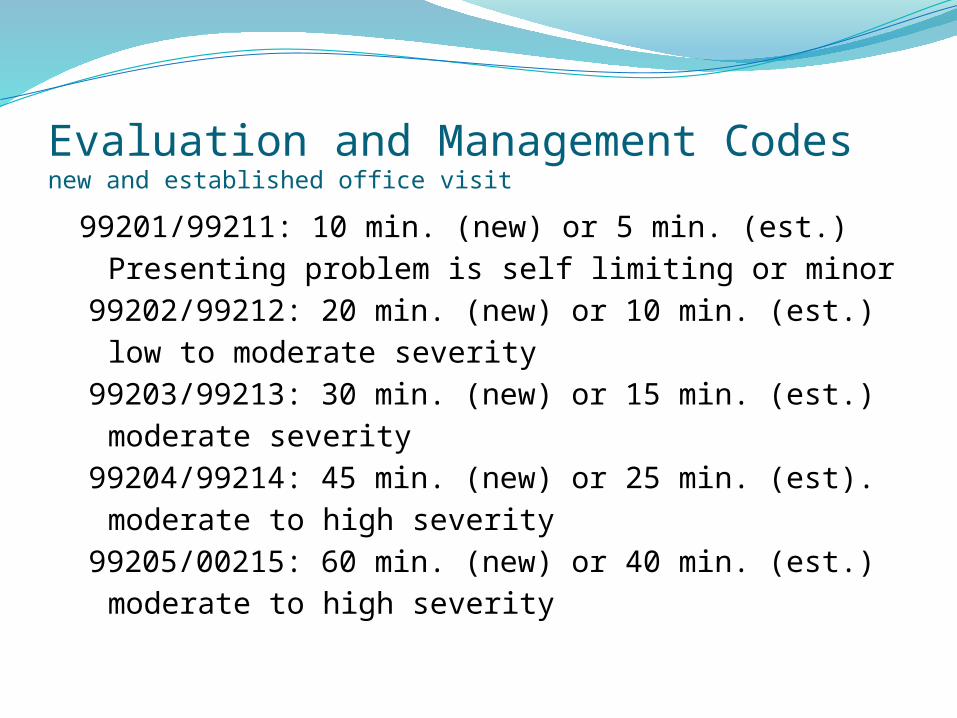
Evaluation and Management Codesnew and established office visit
99201/99211: 10 min. (new) or 5 min. (est.) Presenting problem is self limiting or minor
99202/99212: 20 min. (new) or 10 min. (est.)low to moderate severity
99203/99213: 30 min. (new) or 15 min. (est.)moderate severity
99204/99214: 45 min. (new) or 25 min. (est).moderate to high severity
99205/00215: 60 min. (new) or 40 min. (est.)moderate to high severity
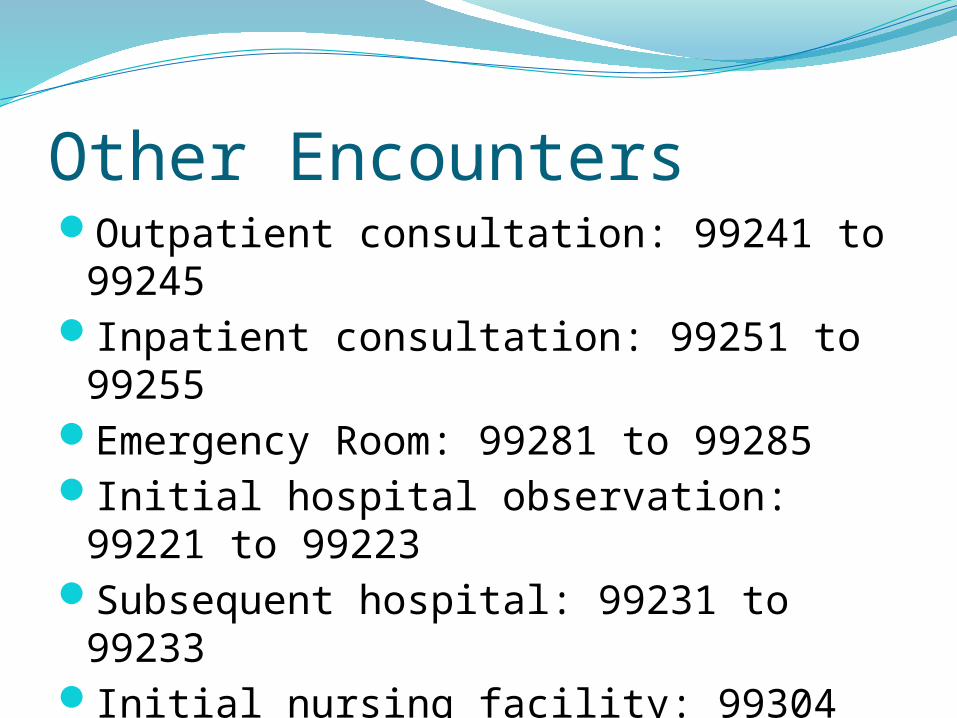
Other EncountersOutpatient consultation: 99241 to
99245 Inpatient consultation: 99251 to 99255Emergency Room: 99281 to 99285Initial hospital observation: 99221 to
99223Subsequent hospital: 99231 to 99233Initial nursing facility: 99304 to 99306Subsequent nursing facility: 99307 to
99310Domiciliary, Rest home, custodial care
Billing
Use E&M codes for Outpatient Visits, Consultations (outpatient and inpatient), ER visits
Calculated by 7 componentsSimilar process for hospital observation, nursing facility, and home care, but will not be discussed
Componentsdetermine E&M coding level—must be documented
Key HistoryExamMedical Decision
Making (MDM)
ContributingCounselingCoordination Nature of
Presenting ProblemTime
HISTORYChief Complaint—required for all level of
visitsHistory of Present Illness (HPI)—brief or
extendedReview of Systems (ROS)—problem focused,
extended, completePast, Family, Social History (PFSH)—
pertinent or completeHow much information is obtained and
documented?
CC and HPIChief complaint is required for all level of
histories: simple statementHPI elements: OLFQQAAT, OLDCART, PQRSTOnset, location, frequency, duration, quality
(character), quantity (severity), aggravating factors, relieving factors (treatments tried), associated factors
REVIEW of SystemsConstitutionalEyesEars, nose, throatCardiac/vascularRespiratoryGIGUMusculoskeletalIntgumentary/breast
NeurologicPsychiatricEndocrineHeme/lymphAllergy/immunology
Past Medical, Family, and Social HistoryPast illnesses, chronic conditions,
surgeries, injuries, hospitalizations, health screening and diagnostic tests
MedicationsRelated family historySocial history—tobacco, alcohol, drugs,
exercise, diet, work, sexual activity
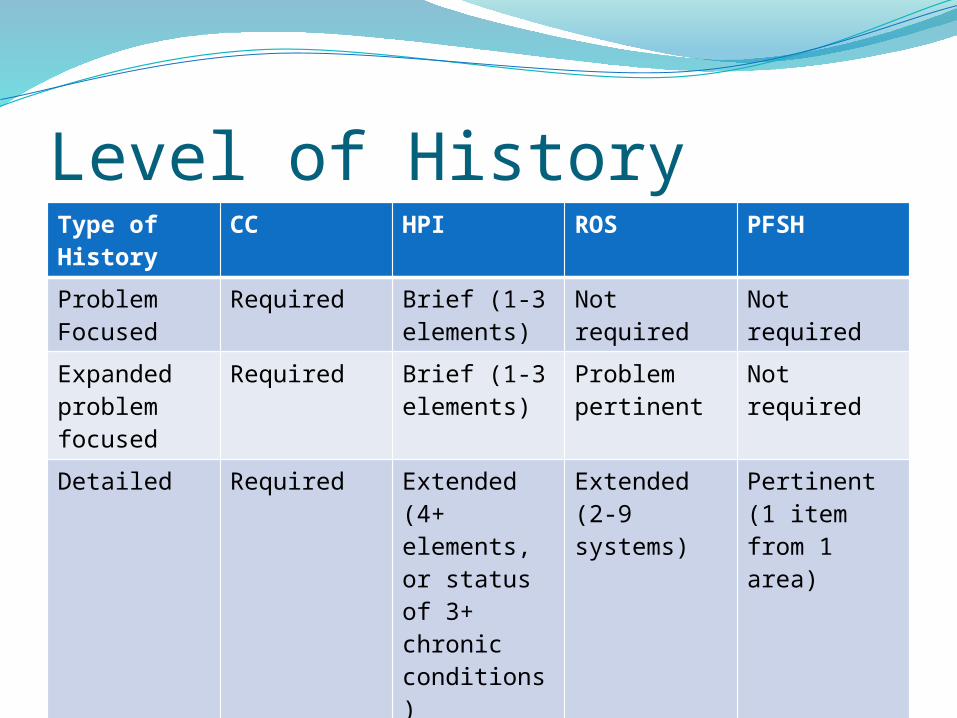
Level of HistoryType of History
CC HPI ROS PFSH
Problem Focused
Required Brief (1-3 elements)
Not required
Not required
Expanded problem focused
Required Brief (1-3 elements)
Problem pertinent
Not required
Detailed Required Extended (4+ elements, or status of 3+ chronic conditions)
Extended (2-9 systems)
Pertinent (1 item from 1 area)
Comprehensive
Required Extended Complete (10+ systems)
Complete (1 item from 2 areas (est.) or 3 areas (new))
Level of History (cont.)Complete ROS—10 or more systems or some
systems with statement “all other systems negative”
Complete PFSH—need 3 for new patients, consultations, hospital observation, initial nursing facility care
Determine the level of history by the column farthest to the left (one poorly documented element can bring the level down).
EXAMBody Area
Head/face, Back/spine, Chest/breast/axilla, Genitalia/groin/buttocks, Abdomen, Neck, Each Extremity
Organ SystemsConstitutional, Eyes, Ears/nose/throat, Cardiovascular, Respiratory, GI, GU, Musculoskeletal, Skin, Neuro, Psych, Heme/lymph/immune
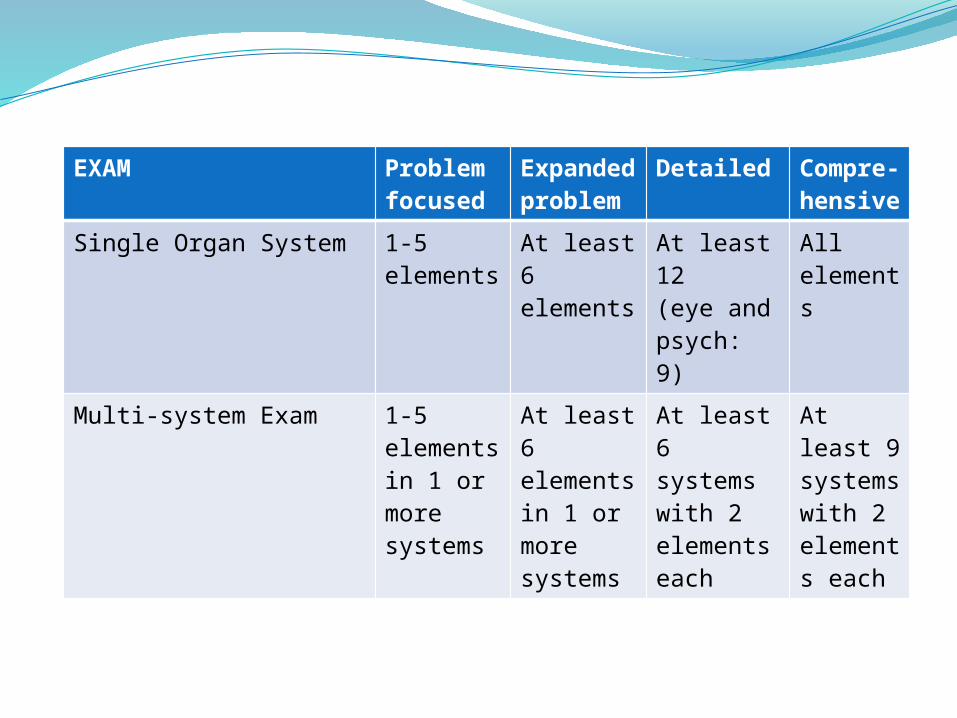
EXAM Problem focused
Expanded problem
Detailed Compre-hensive
Single Organ System 1-5 elements
At least 6elements
At least 12(eye and psych: 9)
All elements
Multi-system Exam 1-5 elements in 1 or more systems
At least 6 elements in 1 or more systems
At least 6 systems with 2 elements each
At least 9 systems with 2 elements each
Medical Decision MakingNumber of diagnoses and treatment
optionsAmount and complexity of data
reviewedRisk of complicationsMorbidity and mortality
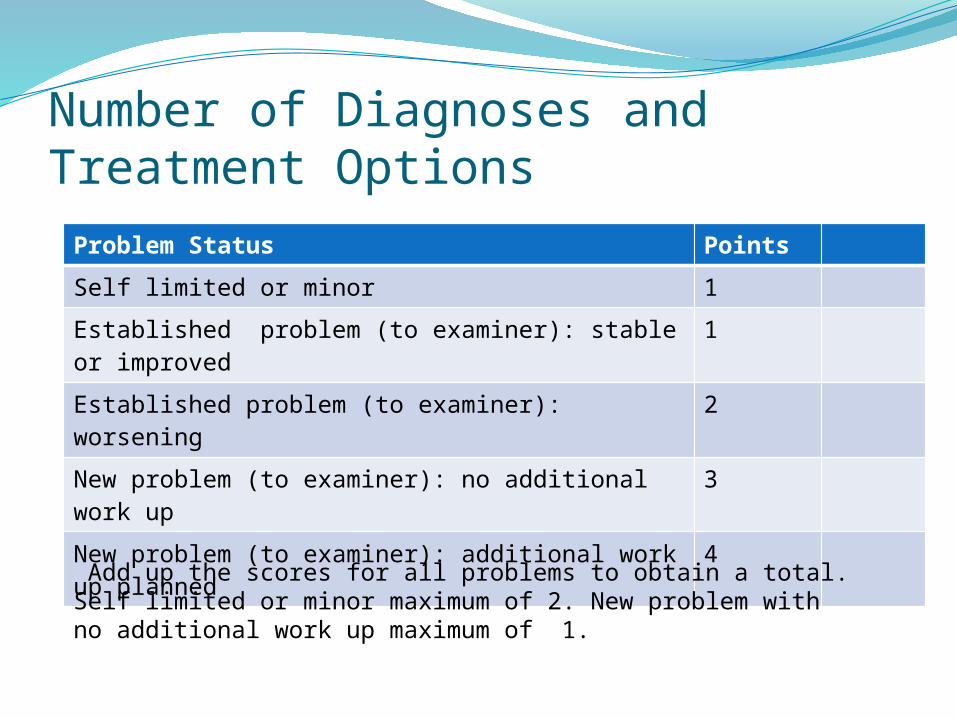
Number of Diagnoses and Treatment Options
Problem Status Points
Self limited or minor 1
Established problem (to examiner): stable or improved
1
Established problem (to examiner): worsening 2
New problem (to examiner): no additional work up
3
New problem (to examiner): additional work up planned
4
Add up the scores for all problems to obtain a total. Self limited or minor maximum of 2. New problem with no additional work up maximum of 1.
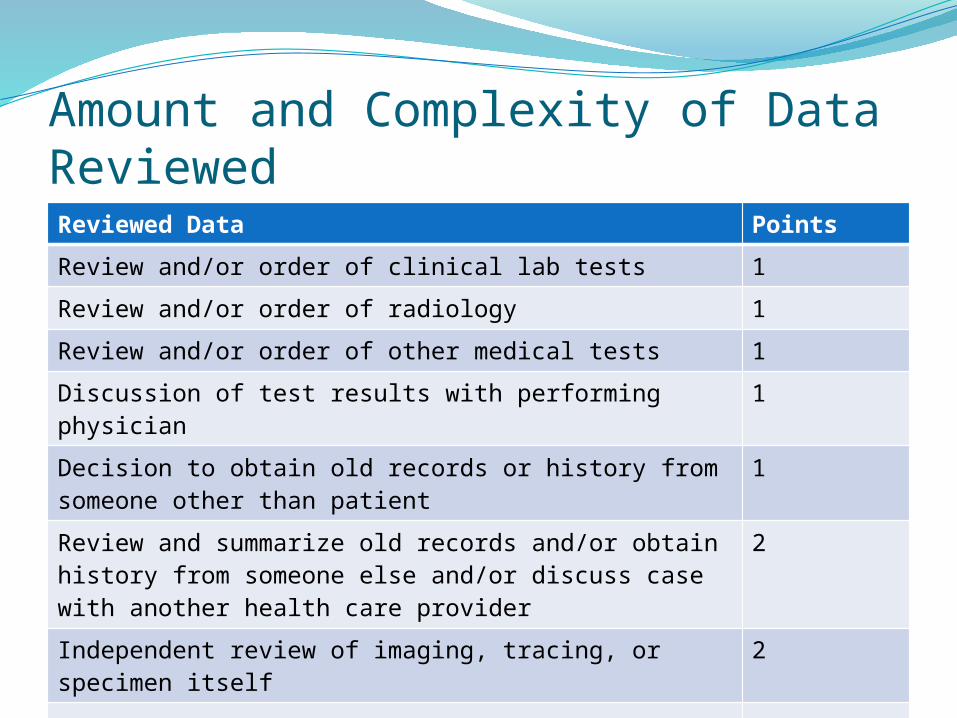
Amount and Complexity of Data ReviewedReviewed Data Points
Review and/or order of clinical lab tests 1
Review and/or order of radiology 1
Review and/or order of other medical tests 1
Discussion of test results with performing physician 1
Decision to obtain old records or history from someone other than patient
1
Review and summarize old records and/or obtain history from someone else and/or discuss case with another health care provider
2
Independent review of imaging, tracing, or specimen itself
2
Total
Risk of Complications, Morbidity/MortalityMinimal—one self-limited or minor problemLow—2 or more self-limited or minor
problems; 1 stable chronic illness; 1 acute, uncomplicated illness
Moderate—1 or more chronic illness with minor exacerbation; 2 or more stable chronic illnesses; undiagnosed new problem with uncertain prognosis; acute illness with systemic symptoms; acute complicated injury
Risk (continued)High
1 or more chronic illnesses with severe exacerbation
Acute or chronic illnesses or injuries that may pose a threat to life or bodily function
An abrupt change in neurologic status
Minimal Risk examplesCold, insect bite, tinea corporisOrder blood work, chest xray, ECGRecommend rest, gargles,
superficial dressing
Low Risk Examples2 or more self limited or minor
problems1 chronic illness that is well
controlledAcute illness such as UTI, simple
sprain, allergic rhinitisPFT, skin biopsy, non-cardiac
imagingOTC meds, physical therapy, minor
surgery without risk factors, IV fluid without additives
Moderate Risk examplesOne or more chronic condition, worseningTwo or more stable chronic conditionsAcute illness with systemic symptoms such as
pylonephritis, pneumoniaAcute complicated injury such as concussionNew problem needing additional work upStress test, endoscopy, cardiovascular
imagingMinor surgery with risk factors, prescription
drugs, closed treatment of fracture
High Risk examplesOne or more chronic illness with severe
exacerbation, abrupt change in neuro statusAcute threatening illnesses such as severe
respiratory distress, acute MI, pulmonary embolus, peritonitis, acute renal failure
Invasive tests with identified risk factorsElective surgery with risk factorsDrug therapy requiring intensive monitoringDecision not to resuscitate or de-escalate
care
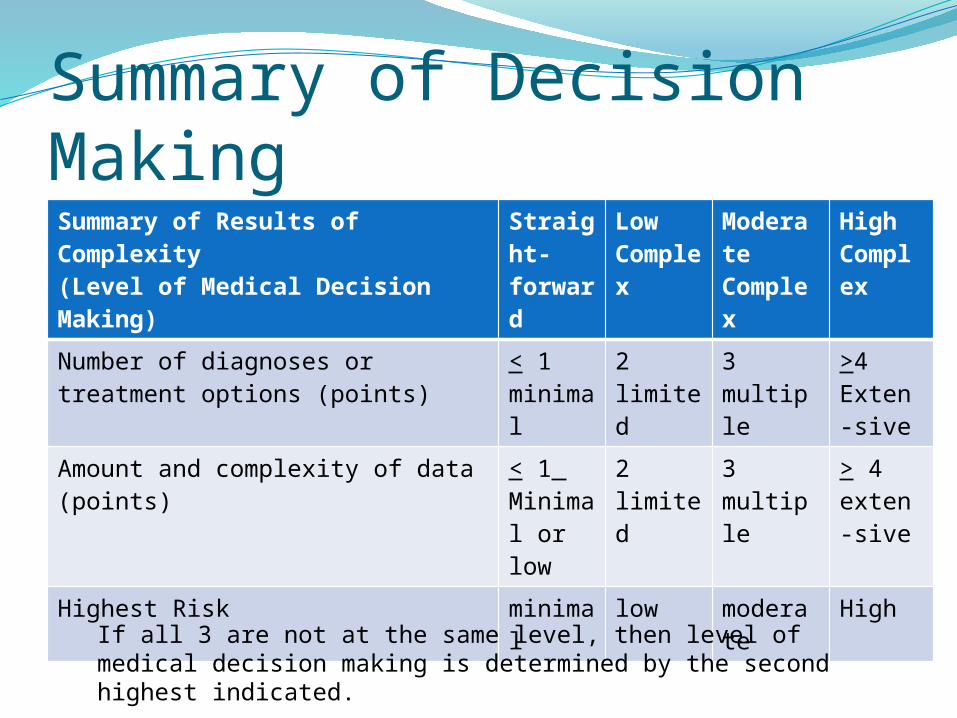
Summary of Decision MakingSummary of Results of Complexity(Level of Medical Decision Making)
Straight-forward
Low Complex
Moderate Complex
High Complex
Number of diagnoses or treatment options (points)
< 1minimal
2limited
3multiple
>4Exten-sive
Amount and complexity of data (points)
< 1 Minimal or low
2limited
3multiple
> 4exten-sive
Highest Risk minimal
low moderate
High
If all 3 are not at the same level, then level of medical decision making is determined by the second highest indicated.
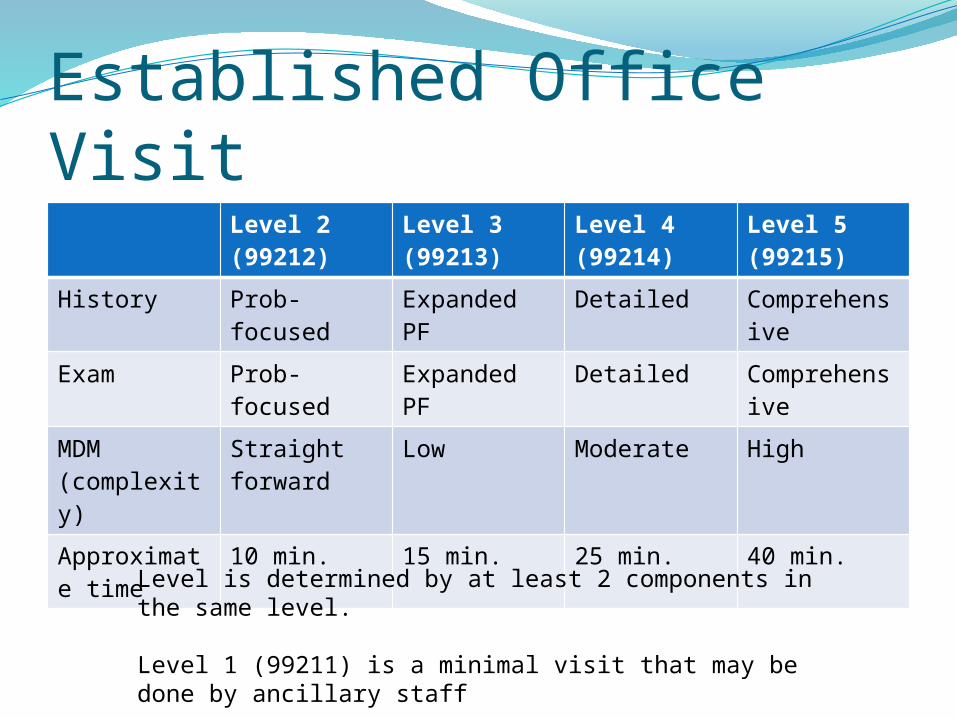
Established Office VisitLevel 2 (99212)
Level 3 (99213)
Level 4 (99214)
Level 5 (99215)
History Prob-focused
Expanded PF
Detailed Comprehensive
Exam Prob-focused
Expanded PF
Detailed Comprehensive
MDM(complexity)
Straight forward
Low Moderate High
Approximate time
10 min. 15 min. 25 min. 40 min.
Level is determined by at least 2 components in the same level.
Level 1 (99211) is a minimal visit that may be done by ancillary staff
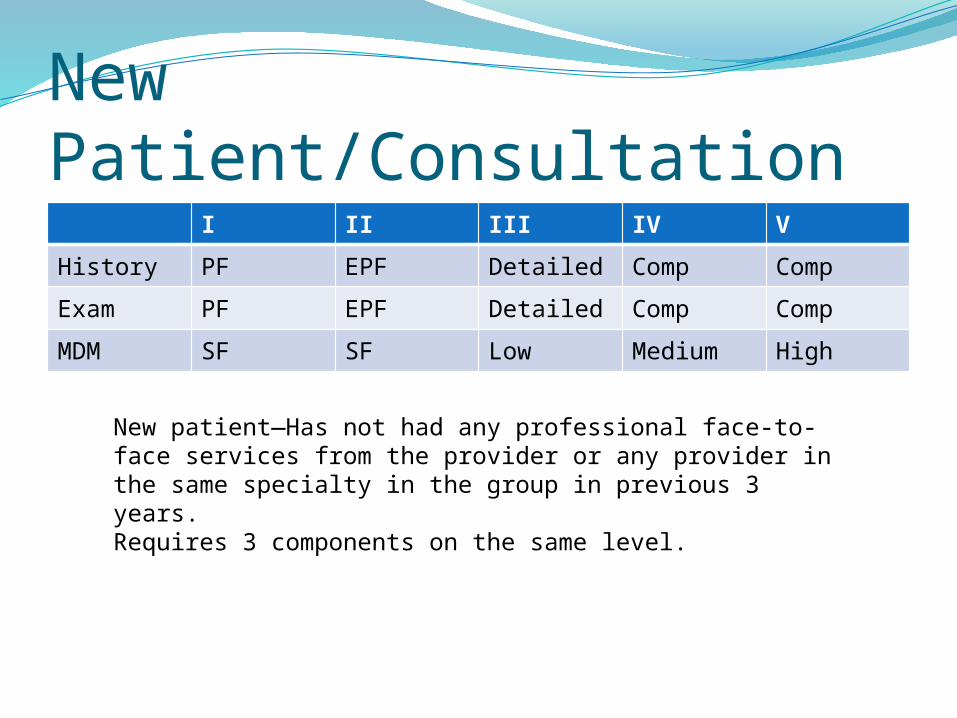
New Patient/ConsultationI II III IV V
History PF EPF Detailed Comp Comp
Exam PF EPF Detailed Comp Comp
MDM SF SF Low Medium High
New patient—Has not had any professional face-to-face services from the provider or any provider in the same specialty in the group in previous 3 years. Requires 3 components on the same level.
Preventative ServicesBy age, coverage and reimbursement are
preset and vary by insuranceMedicare does not cover a routine yearly
physicalWelcome physical in first yearOther preventative services and screenings at
determined intervals Must use appropriate codes
Counseling/Coordination of CareFor an encounter dominated by counseling
about a medical condition or coordination of care, time is a determining factor.For outpatient visit, must be face-to-face timeFor inpatient, can be time on unitTime can be estimatedMust document 3 components: total time, at
least 50% of the visit was spent counseling, nature of the counseling
Incident ToPaid at full physician fee schedule amountNPs and other non-physician providers are
usually allowed at 85%Usually used for follow up of a physician’s
patient following the same plan of care.
Incident To ProvidersAuxiliary personnel: RNs, LPNs, TechniciansNon Physician Providers (NPPs): NP, PA,
CNS, CNM (can supervise auxiliary personnel for payment, except in hospital outpatient departments)
Physical therapists, occupational therapists, clinical social worker
On claim report both name and NPI of initiating physician and supervising physician
RequirementsServices must be furnished in the office (not
hospital)Furnished under direct supervision of a
doctorMust have employment relationship Are integral, although incidental to the
doctor’s services. Commonly rendered without a physician
charge but incur some expense (for dressing change, drug administration)
Direct SupervisionSupervising physician can be any
member of the group Must be present in the office suites
and immediately available.Does not need to speak to or lay
hands on the patient.
Employment RelationshipEmployeeLeased employeeIndependent contractor of physician
or legal entity that employs or contracts physician
Documentation mustIdentify who rendered the serviceIndicate supervision requirement is
metShow physician’s initiation and
continued involvement in treatment plan
Show that care was reasonable and necessary
Show that care was within the scope of practice of NPP
Modifiers25—significant, separate E&M
performed by same provider on same day
24—unrelated E&M done by provider at post operative visit
50—bilateral (pays 150%)51—multiple proceduresDocumentation should show medical
necessity and what was done in addition
Comprehensive Error Rate TestingCMS program monitors accuracy of
claims and paymentsNational error rate is 4.5%Maryland and surrounding states: 4.3%Services associated with errors:
Consults 27% --Established office visits 21%
other outpatient 21%Initial hospital 15% ---Subsequent 13%
Billing and Coding TipDocument every visit using a SOAP note
with subheads and bulleted points for HPI (OLDCART, PQRST), ROS, related past/family/social history, exam by systems, diagnoses, and treatment plan.
You will more easily be able to determine the E&M level, or if you document electronically, a computer program may determine the E&M.
ResourcesCenter for Medicare and Medicaid Services w
ww.CMS.hhs.govwww.cms.hhs.gov/MLNEdWebGuide/25_EMD
OC.aps (Documentation Guidelines)www.cms.hhs.gov/MLNProducts/downloads/19
95dg.pdf (1995 Guidelines)
www.cms.hhs.gov/MLNProducts/downloads/master1.pdf (1997 Guidelines)
www.cms.hhs.gov/manuals (Claims processing)
Resources (cont.)Highmark Medicare Services
www.highmarkmedicareservices.com
www.highmarkmedicareservices.com/faq/partb/index.html (Frequently Asked Questions)
www.highmarkmedicareservices.com/partb/reference/scoresheets.html (E&M score sheets)