Embed Size (px)
Citation preview

San Diego Long Term Care Integration Project
Personal Care Services Workgroup
October 5, 2005
Mrs. C
84 year old woman lives alone CHF, HTN, diabetes, hearing and vision
loss, IADL dependencies 16 medications by 6 MDs Medicare and Medi-Cal beneficiary Only child lives in Chicago
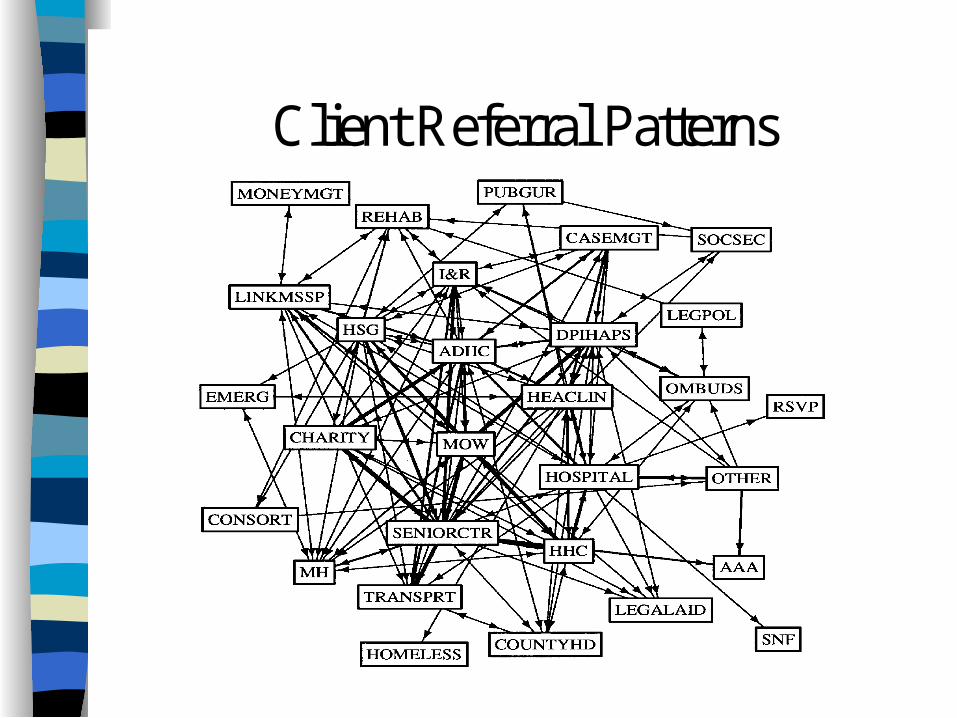
Client Referral Patterns
Journal of the American Geriatrics Society, Feb. 1997
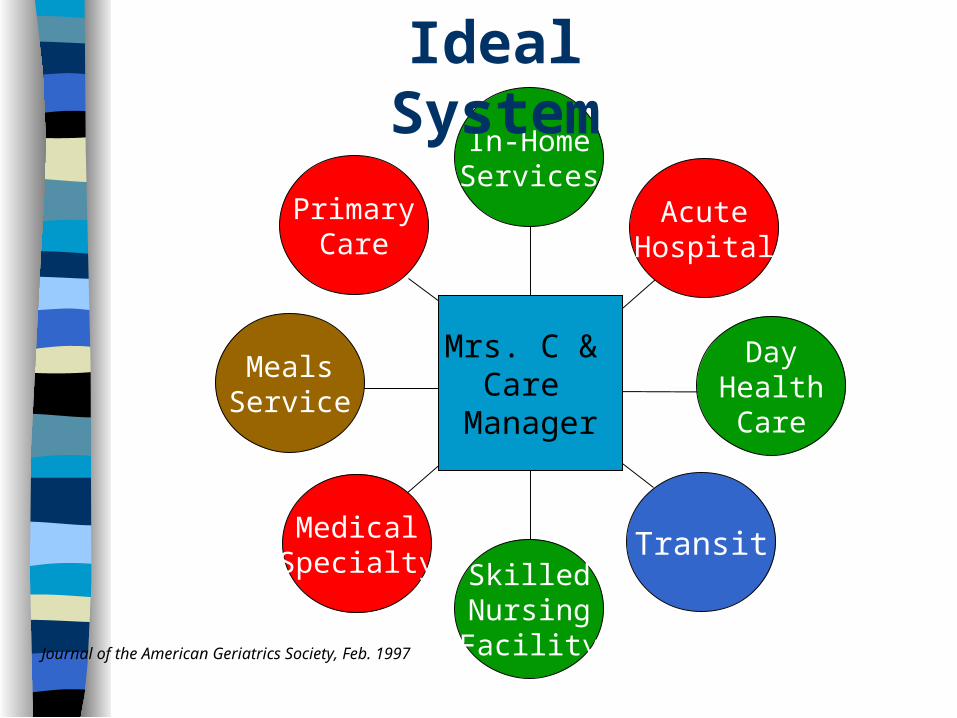
In-HomeServices
DayHealthCare
AcuteHospital
TransitSkilledNursingFacility
MedicalSpecialty
MealsService
PrimaryCare
MRS.C.
Ideal System
Mrs. C & Care
Manager
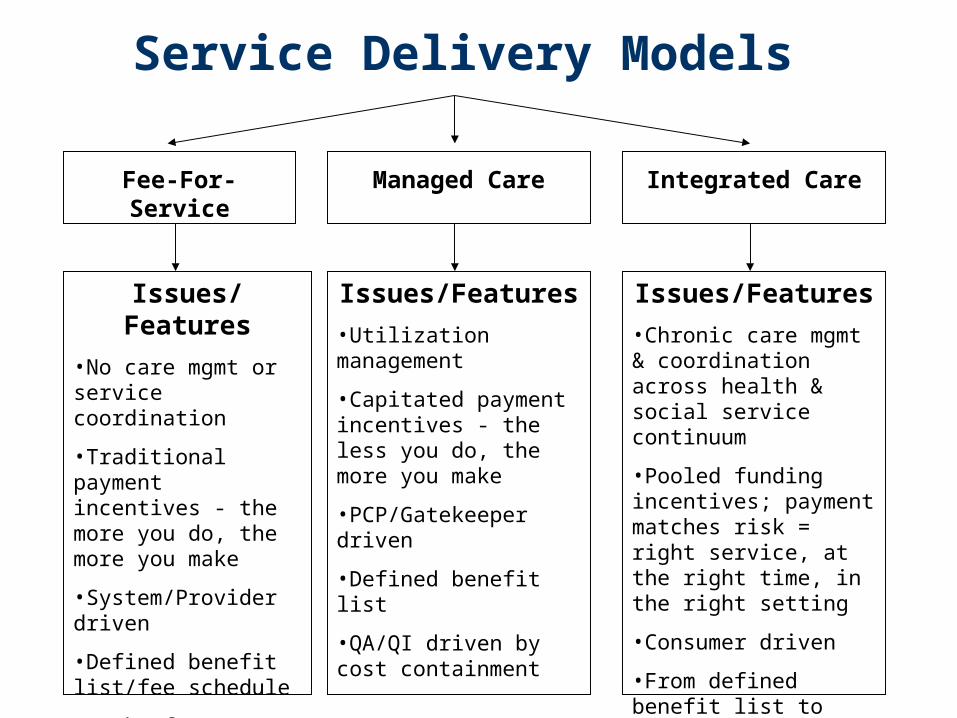
Fee-For-Service Managed Care Integrated Care
Issues/Features
•No care mgmt or service coordination
•Traditional payment incentives - the more you do, the more you make
•System/Provider driven
•Defined benefit list/fee schedule
•Lack of QA/QI measures & oversight
Issues/Features
•Utilization management
•Capitated payment incentives - the less you do, the more you make
•PCP/Gatekeeper driven
•Defined benefit list
•QA/QI driven by cost containment
Issues/Features
•Chronic care mgmt & coordination across health & social service continuum
•Pooled funding incentives; payment matches risk = right service, at the right time, in the right setting
•Consumer driven
•From defined benefit list to what indiv. needs/ prefers
•Comprehensive QA/CQI built into system
Service Delivery Models

LTCIP Strategies
Network of Care (NOC) – Web-based information & communication system
to support the 2 service delivery models below Physician Strategy
– Managed Fee-For-Service initiative to improve chronic care management
Healthy San Diego Plus (HSD+) – Integrated service delivery model that provides the
full continuum of health and social services

Network of Care (NOC) Test/improve existing web-based system &
expand to support 2 service delivery models Funding: AoA, $610,000 over 3 years for
Aging & Disability Resource Center Expand as communication link btw MD,
consumer, caregiver, community providers Develop CQI program/Community Education
Workgroup www.sandiego.networkofcare.org
Physician Strategy Fee-for-service initiative to improve chronic
care management Funding: $142,000 (planning) CA Endowment Partner w/physicians vested in chronic care Develop interest/incentive for support of
HCBC ID care management resources Train on healthy aging, geriatric/chronic
disease protocol, pharmacy, HCBC supports Falls Prevention initiative
Fully Integrated Model
In SD, known as Healthy San Diego Plus (HSD+)
Builds on geographic managed care model for Medi-Cal
Option to mandatory primary & acute enrollment for ABDs
Pooled Medi-Cal (& Medicare for duals) health and supportive service $$
From defined benefit list to what individual needs/prefers
Care manager and member in “hub”

Community Planning Process
From 50 to 700+ key stakeholders over past 6 years: 22,000+ hours
Seeking to improve system of care for consumers and providers
Agreement to use existing providers, assure fair compensation
Planning within state LTCIP authorization (form follows funding)

San Diego County Board of Supervisors&
State Office of Long Term Care
Jean Shepard, DirectorCounty of San Diego, Health & Human Services
Agency, (HHSA)
Advisory Group:Goal: Make final decisions and
recommendations for inclusion in the plan.
Planning Committee:Goal: Guide the LTCIP planning process.
Suspended Workgroups pending need for further action/decision-making
Suspended Workgroups pending need for further action/decision-making
Health Plan Partners Workgroup
Health Plan Partners Workgroup Finance/Data
Workgroup
Finance/DataWorkgroup Options Workgroup
Options Workgroup
Internet• Facilitates
communication• Provides broad public
education
Pamela B. Smith, Project DirectorEvalyn Greb, Project ManagerAging & Independence Services
Lead County Agency
MH & SAWorkgroup
MH & SAWorkgroup
Explore use of the Healthy SanDiego model for potentialService delivery system for LTCIP.
Determine the financialfeasibility of the proposedLTCIP for San Diego County.
Make recommendations to Planning Committee re: inclusion of mentalhealth and substance abuse services in LTCIP.
LTCI Strategies:1) Network of Care2) Physician Strategy3) Healthy San Diego Plus Workgroups:Care Management, Provider NetworkDevelopment, Cultural Responsiveness
Governance-Case Management-Info/Technology-Quality Assurance-Scope of Services-Workforce Issues-Developmental Disabilities-Community Network Development
Community EducationWorkgroup
Community EducationWorkgroup
Explore use of public health education models that promote improved chronic care management for LTCIP
Long Term Care Integration Project
Organizational Chart & Decision Tree
San Diego Stakeholder LTCIP Vision for Elderly & Disabled Develop “system” that:
– provides continuum of health, social and support services that “wrap around consumer” w/prevention & early intervention focus
– pools associated (categorical) funding– is consumer driven and responsive– expands access to/options for care
Stakeholder Vision (continued)
– Fairly compensates all providers w/rate structure developed locally
– Engages MD as pivotal team member– Decreases fragmentation/duplication
w/single point of entry, single plan of care– Improves quality & is budget neutral– Implements Olmstead Decision locally– Maximizes federal and state funding

Legislative Authority
AB 1040 in 1995 (revised in 1998) State Office of LTC:
– provides planning $$ ($873,000 to-date)– provides “Center” resources– provides liaison with other state programs– approves local activity toward LTCI– will assist in procuring federal waivers– (? budget for FY 05-06)

Why change?
To align incentives for optimum care across the continuum
To impact quality of life for aged and disabled, especially high cost users
To respond to demographics that require Medicare to respond to chronic care needs
To shift focus to consumer and outcomes To support consumer desire to “age in place” To respond to Olmstead Decision
Statement of Need Aging Population
– San Diego County to increase significantly• Elderly:14% today; 25-33% by 2030• From 1990 to 2010, 75+ increases by 81%• 85+/minority elderly: fastest growing segments
– 60% of those 65+ will require long term care services at some point
– Those who need service can’t find it– Care is fragmented by regulation!– Providers asked to do more w/less– Medi-Cal Redesign proposes expansion to ABDs

Statement of Need (cont’d) Expenditures
– LTC recipients represent: 25% of Medicaid population, 70% of Medicaid expenditures
• San Diego ABD enrollees/month - 90,000 • 20,000 IHSS consumers• 62% of ABDs are dually eligible (Medi-Medi)• 90% of those 65+ are dually eligible• Projected annual expenditures for Medi-Medi’s
– Medi-Cal: $1.2 B (CY 2005)– Medicare: $.5 B (CY 2005)
– Only 7% of US population currently has private LTC insurance (narrow population can benefit)
– Resources insufficient to meet future demand
From Vision to Service Delivery Model… Explore Healthy San Diego due to:
– Access, education, prevention– Advocacy– Cost-effectiveness– Population-based– Existing infrastructure– Stakeholder-designed, BUT
HSD Currently Does NOT…
Tailor the program for chronic care or aged and disabled persons
Provide “wraparound” services Provide chronic care management on a
population basis Receive adequate reimbursement for
chronic care Have much info on “duals”
LTCIP Workgroups
NEW: Personal Care Services Governance Care Management Information Technology Quality Assurance Scope of Services Health Plans Finance/Data

LTCIP Workgroups
Developmental Disabilities Mental Health & Substance Abuse Community/Provider Network
Development Community & Cultural Responsiveness Community Education

Why should stakeholders get involved? To influence planning and decisions To impact delivery of acute & LTC
needs of individuals (support+services) To recommend how to include personal
care services into the fully integrated model
Current Reality Medi-Cal Redesign and ALTCI
– ABDs to be mandated in Jan. Budget for primary and acute managed care?
– IHSS to be included in ALTCI services– OLTC and health plan CMs
Medicare Modernization Act (SNPs) Mercer Rate-Setting Report Local recommendations for RFSQ
– Provider Network– Care Management– Community & Cultural Responsiveness

Other national LTCI programs
PCS provided according to need Health plan responsible for assessment
and authorization of all but medical svcs Greater # receive in-home care Hours/individual have not increased Co. staff still in PCSP, working for
health plan (higher pay), or new Co.job
Assumptions
Voluntary enrollment beginning July 2007 Eligible population: up to 95,000 Medi-Cal-
only and dually eligible aged, blind and disabled persons, 21yo+
PCS included as a benefit One care manager Single multi-dimensional assessment One Care Plan
LTCIP and Personal Care Services Eliminate duplicate assessments/plans Replaces IHSS regs w/quality indicators CM to assess across all needs and
preferences w/consumer on “team” PCS is one of many plan services available Monitoring/reassessment more frequent Helps provide new incentive for health plans:
stabilize at-risk individuals with home care, avoid inappropriate ER, hospital, SNF use

Personal Care Services Workgroup Goal To forward a recommendation to the
Planning Committee on how to best integrate personal care services into HSD+ in a manner that is consistent with the LTCIP stakeholder vision
How to influence planning?
Next Workgroup meeting: Oct. 19, 1:00-3:00, Pt. Loma Nazarene University, 4007 Camino Del Rio South, SD CA 92108 (Mission Valley area)
Get on LTCIP mailing list for updates Log onto website for background & info:
www.sdcounty.ca.gov/cnty/cntydepts/health/ais/ltc/
Call or e-mail input/ideas: [email protected], 858-495-5428 or [email protected], 858-694-3252





























