Embed Size (px)
Citation preview

Bleeding and Haemostasis
Saman W.Boskani HDD, FIBMS
Maxillofacial Surgeon

1 Beeding

● Its escaping or extravasation of blood contents from blood vessels
Next

● Types: - Arterial - Venous - Capillary
Next

Differences between the types:
Arterial Venous Capillary● Bright red
● Eject out Synchronously
● Its control is difficult
● Avoidable
● Darker blood
● Has steady flow
● Its control is sometimes easier
● Common
● Bright red ●
● Shows as generalized ooze
● Its rapid & controlled much
easier
●Most common than others

Classifications:According to time of haemorrhage:
1. Primary: immediately 2. Reactionary: commonly within first 24
hours 3. Secondary: usually occurs 7-14 days
According to appearance: 1. Revealed (external) 2. Concealed (internal)
Next

Classifications: (cont.)According to size of haemorrhage:
1. Small haemorrhages (petechiae,purpura,ecchymosis)
2. Large or massive haemorrhages (appear as running, clotting or hematomas)
● According to different organs or systems named:
1. Epistaxis, hemoptysis, 2. Hematamesis & melena, 3. Hematuria Next

Compensatory reactions activated by haemorrhage:
➢Vasoconstriction ➢Tachycardia ➢Venoconstriction ➢Tachypnea- increased thoracic pumping ➢Restlessness ➢ Increased movement of intestinal fluid into
capillaries
Next

➢ Increased secretion of norepinephrine &epinephrine
➢ Increased secretion of vasopressin ➢ Increased secretion of glucocorticoid ➢ Increased secretion of renin& aldosterone ➢ Increased secretion of erythropoietin ➢ Increased plasma protien synthesis
Next

Clinical presentation:● Pale ,cold, wet skin ● Restlessness ,anxiety ,change in
conscious level ● Tachycardia ,with normal or even raised
BP at first but later on Hypotension if bleeding cont.
● Deep sighing breathing( air hunger), tachypnea
● Thirst in late stages ● Empty veins ● Shock
Next

Investigations1. Hematological
1. Hb, pcv, blood group 2. Bleeding& clotting studies
2. Radiological studies (including US) 3. Electrolyte, acid- base analysis 4. Blood gas analysis & monitoring 5. Renal function studies after few days 6. Liver function studies
Next

Management● In general managing of a case of
hemorrhage include: I. Primary assessment while resuscitating the
patient I. IV line, fluid, sending blood for group& cross match II. Send for blood if necessary III. Assessing of the amount of blood lost if possible IV. Stopping of bleeding if possible( external) V. CVP measurement
II. Secondary assessment Definitive treatment: including taking the patient to
theatre if indicated
Next

ManagementLocal Haemostasis: 1. Mechanical:
1. Positioning 2. Pressure
1. Finger 2. Hemostat 3. Bandage ,sterile gauze, tourniquet ( better to be avoided)
3. Packing 4. Ligation
2. Thermal 1. Electro cautery 2. Cryogenic surgery
3. Chemical 1. Epinephrine 2. Gel foam, oxycel, fibrin glue 3. Coagulation factors (regardingly )
4. Follow up of the patient
Next

2 hemostasis
Next

Can be define as : ● The process of arresting bleeding by repair
of vessel wall ● Maintaining a balance between
● Coagulation ● Fibrinolysis

Mature clot : is acombination of cross linked fibrin admixed with blood cells
and plasma
Next

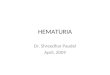
Sub-endothelial matrix
PlateletsHemostatic plug
FibrinEndothelial cell
RBCWBC
WBC

CLOT
Fibrin
Red Blood CellPlatelet
Next

COMPONENTS OF HEMOSTASIS
● Vascular system ● Platelet System ● Coagulation System
Next

Hemostatic Mechanism● 2 phases
● PRIMARY- blood vessel (vascular) and platelet response to injured vessel
● SECONDARY- response of protein coagulation factors to the injury
Next

Vascular phase ● It provide by vasoconstriction due to local
contraction in smooth muscles of vessels by the effect of different stimuli (eg Thromboxane A2 which is a powerful vasoconstrctor) also (Serotonin , bradykinin )
● By this process : 1-reduces blood loss 2-prevents clot from washing out
Next

Platelet Phase
● Also platelet plays a great role as an injury to vascular walls ; expose endothelial collagen to which platelet adhere ,& this required vWf which is producing in the Sub-endothelium , it binds to Glycoprotein in the surface of platelets

● This phase pass through : 1- platelet adhesion 2-platelet activation 3-platelet aggregation
Next

Coagulation ● It is a stepwise pathway , which is stimulated
by platelet phase , ● The resultant system known as coagulation
cascade which consist of two paralleling routes (Intrinsic & Extrinsic pathways )
Next

Coagulation ● Intrinsic Pathway : all its components are found in blood so
its activated by exposure to negatively charged foreign substance
the Intrinsic Pathway include factors VIII , IX , XI , XII
Next

Coagulation ● Extrinsic pathway: refer to extrinsic because the factors that
activate it (tissue factor) is normally outside the vascular space and is exposed to vascular space only after damage to vascular endothelium
Extrinsic Pathway include factor ( III , VII )
Next

Coagulation ● Both intrinsic and extrinsic pathways connect
to forming common pathway ● Common pathway include factors I ,II , III ,X
Next

Contact Tissue Factor + VII
XIIIa
XIII
Thrombin
Fibrin (strong)
Fibrinogen Fibrin (weak)
IXXI
XIaIXa
XaVa
XIIaProthrombin
TF-VIIa
(Prothrombinase)
PL
PL(Tenase)
VIIIaPL
X
Intrinsic Pathway
HKa
Extrinsic Pathway
Common Pathway
TF Pathway
Coagulation Pathways
Protein C, Protein S, Antithrombin III

Important Note
● vWF which synthesized by vascular endothelial and attaches to both platelet receptors and collagen sp.
Next

Important Note
● BT : primary hemostasis ● PT : Extrinsic pathway ● PTT : Intrinsic pathway ● TT : Common pathway
Next

Important Note
● Some time case of vWF disease mistaken for hemophiliac case because the level of factor VIII are commonly low in vW disease because vWF acts as carrier protein for factor VIII
● but with normal PT ,PTT
Next

Important Note
● Bleeding time : reflects the time required to form the platelet
plug (primary hemostasis ) so it reflects platelet function rather than coagulation cascade
Next

Important Note
● Aspirin inhibits platelet function by irreversibly inhibiting the enzyme
cyclo-oxygenase which is normally function to synthesize thromboxane A2 ,
TXA2 normally acts to stimulate platelet aggregation and constriction of blood vessels
so aspirin lead to prolonging Bleeding Time Next

Important Note
● Heparin activates anti-thrombin III (ATIII) which is a potent inhibitor of factor II thrombin as well as some other factor in intrinsic pathway , it prolong PTT , no PT except in high dose ,
● it not affect BT because it not affect platelet function
It can be antagonized by protamine
Next

Important Note
● Warfarin inhibit the production of Vit. K dependant clotting factors X IX VII II so it affects common and extrinsic pathways and so it affects PT rather than PTT .
● Its effect can be antagonized by administering Vit K or fresh frozen plasma
Next

Important Note
● Desmopressin acetate DDAVP is useful in many case of bleeding disorder because it induces the hepatic production of plasma clotting factors , and it stimulate the release the vWF from the endothelial cells
Next

FibrinolysisPlasminogen
Plasmin
Fibrin, fibrinogen
ActivationExtrinsic: t-PA, urokinase
Intrinsic: factor XIIa, HMWK, kallikreinExogenous: streptokinase
Fibrin, fibrinogen degradation products Next

Fibrinolysis● Mechanism of action of tissue palsmogen
activator its enzyme that activate plasma enzyme plasmogen by converting it to active form plasmin and plasmin is an enzyme that protolytically cleave fibrin strands thereby degrading fibrin clots like streptokinase and urokinase
Next

References
● Baily & Love Short practice of surgery ● Textbook of General & Oral Surgery ● Clinician’s manual OMF surgery ● Internet articles

Thanks

![Teske - Anaemia [Compatibiliteitsmodus] · • bleeding (petechiae, ecchymoses, melena, hematuria, hematomas) • fever • splenomegaly Additional Clinical Symptoms: Anaemia Non-Regenerative](https://img.pdfslide.us/doc/110x75/5c8c870a09d3f2804e8c0316/teske-anaemia-compatibiliteitsmodus-bleeding-petechiae-ecchymoses.jpg)