Embed Size (px)
Citation preview

Eur. J. Psychiat. Vol. 27, N.° 3, (206-224)2013
Keywords: Attention-deficit/hyperactivity disorder;Adult; European; Atomoxetine.
Safety and Tolerability of AtomoxetineHydrochloride in a Long-Term, Placebo-ControlledRandomized Withdrawal Study in Europeanand Non-European Adults with Attention-Deficit/Hyperactivity Disorder
Angelo Camporeale, MD*Himanshu Upadhyaya, MBBS, MS*J. Antoni Ramos-Quiroga, MD, PhD**,***David Williams, MS****Yoko Tanaka, PhD*Jeannine R. Lane, PhD****Rodrigo Escobar, MD*Paula Trzepacz, MD*Albert J Allen, MD, PhD*
* Lilly Research Laboratories, Lilly CorporateCenter, Indianapolis, USA
** Department of Psychiatry, HospitalUniversitari Vall dʼHebron, CIBERSAM,Barcelona, Spain
*** Department of Psychiatry and LegalMedicine, Universitat Autònoma deBarcelona, Bellaterra, Spain
**** inVentiv Health Clinical,Indianapolis, USA
USA
SPAIN
ABSTRACT – Background and Objectives: Safety and tolerability of atomoxetine were stud-ied in the largest double-blind, placebo-controlled, randomised withdrawal trial of atomoxe-tine (80 or 100 mg/day) in adults with attention-deficit/hyperactivity disorder (ADHD).
Methods: Patients (N = 2017), 18 to 50 years of age, with ADHD were enrolled from18 countries. Patients who responded to atomoxetine during a 12-week open-label treat-ment phase and maintained that response during a 12-week double-blind maintenancephase were randomised to atomoxetine (N = 266) or placebo (N = 258) for 25 weeks ofdouble-blind treatment. Treatment differences were compared for serious adverse events(AEs), treatment-emergent AEs (TEAEs), discontinuation due to AEs, vital signs, bodyweight, and electrocardiograms.

SAFETY OF ATOMOXETINE IN ADULTS WITH ADHD 207
Introduction
There have been major advances in thetreatment and understanding of attention-deficit/hyperactivity (ADHD) during the lastdecade1-6. Yet despite this growing under-standing, ADHD in adults is currently un-derdiagnosed in many European countries,leading to ineffective treatment and highercosts of illness7.
Of the multiple pharmacotherapeutic op-tions for treatment of ADHD in adults8-15, thestimulants methylphenidate and dexamphet-amine are the most widely used in Europe7;however, they are only approved in somecountries. Although efficacy and safety ofthese stimulants are well-established, asmany as 30% of patients have inadequate re-sponse, tolerability problems (e.g., sleep dis-turbance) or contraindicated comorbidities(e.g., schizophrenia, hyperthyroidism, car-diac arrhythmias, angina pectoris, and glau-coma)16,17. Additionally, even with extended-release formulations, the stimulants remain
limited in their duration of effect, and theabuse liability may lead to reluctance to usethem16,17. Hence, treatment should be se-lected according to patient need for lasting ef-ficacy, comorbidity profile, and risk of abuseof prescription medications.
Atomoxetine hydrochloride, a selectivenorepinephrine reuptake inhibitor, is a non-stimulant medication approved to treatADHD in adults in North America and sev-eral other countries17. Because of its demon-strated efficacy, limited spectrum of adverseeffects, and absence of abuse potential, ato-moxetine may aid in treating patients withADHD. Indeed, multiple studies in chil-dren18-23 and adults8,10,11,24,25 have shownthat atomoxetine has an acceptable safetyprofile, with most adverse events (AEs) hav-ing low-to-moderate severity, which diminishover the first month of treatment. To extendthese findings, the long-term safety and effi-cacy of atomoxetine in adults with ADHDwere examined in a double-blind, placebo-controlled randomized withdrawal study. Pa-
Results: During the 25-week double-blind treatment phase, discontinuations due to AEswere similar between atomoxetine and placebo (3.4% vs. 1.9%; P = .418). The percentageof patients experiencing ≥1 TEAE(s) was significantly higher for atomoxetine than placebo(47.0% vs. 37.6%; P = .034), but there were no significant differences for any individualTEAE. Diastolic blood pressure (-0.1 vs. -2.3 mmHg), heart rate (-1.4 vs. -5.3 bpm), andweight (-0.2 vs. 1.1 kg) were significantly different between atomoxetine and placebo (P<.001). There were no significant differences between atomoxetine and placebo in the fre-quencies of patients showing an increase from baseline >30 ms in Fridericia’s QT correc-tion (QTcF; 1.4% vs. 2.6%) or Bazett’s QT correction (QTcB; 2.8% vs. 2.6%). During theentire study, no patient had a QTcF or QTcB >500 ms, or an increase from baseline >60 ms.
Conclusions: This study demonstrated that atomoxetine exhibited an acceptable safetyprofile in adults with ADHD after 1 year of treatment, and no clinically meaningful safe-ty-related rebound effects were observed following abrupt discontinuation after 24 weeksof treatment.
Received: 14 August 2012Revised: 28 March 2013Accepted: 17 April 2013

208 ANGELO CAMPOREALE ET AL.
tients who responded to atomoxetine duringa 12-week open-label treatment phase andmaintained that response during a 12-weekdouble-blind maintenance phase were ran-domized to an additional 25 weeks of atom-oxetine or placebo during a double-blind ran-domized withdrawal phase. The efficacyresults from this trial, reported in Upadhyayaet al.26, demonstrated substantial treatmentresponses to atomoxetine during the 12 weekopen-label and 12-week double-blind main-tenance periods as measured by a ≥30% con-tinuous reduction from baseline in Conners’Adult Attention-Deficit/Hyperactivity Dis-order Rating Scale (CAARS)-InvestigatorScreening Version (CAARS-Inv:SV)27 totalscore and a rating ≤3 (minimally ill) on theClinical Global Impression ADHD-Severity(CGI-ADHD-S)28. In the 25-week random-ized withdrawal phase that followed, theseauthors showed that atomoxetine was able toeffectively control ADHD symptoms asdemonstrated by a significantly greater pro-portion of atomoxetine- than placebo-treatedpatients maintaining their treatment re-sponses. In this paper, we report the 24-weekprerandomisation and 25-week postran-domisation safety results from this trial.
Method
Participants
This study was conducted at 152 centers in18 countries throughout Asia, North America,South America, and Europe. Eligible patientswere age 18 to 50 years and met the Diag-nostic and Statistical Manual of Mental Dis-orders, Fourth Edition Text Revision™(DSM-IV-TR) criteria for current and child-hood ADHD as assessed by the Conners’Adult ADHD Diagnostic Interview for DSM-IV27; had a score of ≥2 on at least 6 items of
either the inattentive or hyperactive core sub-scales of the CAARS-Inv:SV27 and of theCAARS-Observer Screening Version (CAARS-O:SV) with adult ADHD prompts for cur-rent symptoms27; and had a score of ≥20 onCAARS-Inv:SV 18-item total ADHD symp-tom score. Patients were also required to havea CGI-ADHD-S28 rating of ≥4 (moderatelyill) at Visits 1 and 2. The CGI-ADHD-S wasrated on a 7-point scale with 1 meaning “nor-mal, not at all ill” to 7 meaning “among themost extremely ill patients”.
Patients who met DSM-IV-TR diagnosticcriteria for any history of bipolar disorder,current major depression, a current anxietydisorder (including generalised anxiety dis-order, panic disorder, or social phobia), orany history of a psychotic disorder were ex-cluded from the study. Patients who were cur-rently using alcohol, drugs of abuse, or anyprescribed or over-the-counter medication ina manner that the investigator considered in-dicative of chronic abuse or who met DSM-IV-TR criteria for alcohol or other substancedependence were also excluded. Additionaldetails about the inclusion and exclusion cri-teria are provided in Upadhyaya et al26.
An informed consent document approvedby an Ethical Review Board or similar bodywas signed by the patient and/or representa-tive and deemed appropriate, according tolocal laws and regulations. The study wasconducted in accordance with the Declarationof Helsinki and the applicable laws and reg-ulations of the study countries and regions.
Study Design
In this study, a randomised, double-blind,maintenance of response (randomised with-drawal) design was implemented to test thehypothesis that atomoxetine (80 or 100 mg/day) was superior to placebo in maintaining

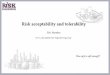
a satisfactory response at the end of double-blind treatment in adult outpatients withADHD. The study design was made up of 3study periods and is illustrated in Figure 1.
The first study period was a screening/washout phase. The second study period wasa 12-week open-label atomoxetine-treatmentphase (Visits 2 to 7 [Weeks 0 to 12]). Duringthis study period, patients received open-la-bel atomoxetine at a starting dose of 40 mg/day(Visit 2 [Week 0]) after completion of all as-sessments, with titration to a target dose of 80or 100 mg/day (depending on tolerability)by Visit 6 (Week 8). This dose was main-tained up to Visit 7 (Week 12). At Week 12,patients were classified as responders if theyhad a ≥30% reduction in their baseline (Visit2) CAARS-Inv:SV total score, and a CGI-ADHD-S score ≤3 (minimally ill). These cri-teria are commonly used in ADHD studiesand provide a clinically meaningful level ofimprovement24,29.
The third study period began with a 12-week (Visits 7 to 11 [Weeks 12 to 24]) dou-ble-blind maintenance phase with atomoxe-tine (80 or 100 mg/day). Only atomoxetineresponders were allowed to enter this studyperiod; non-responders were discontinuedfrom the study. During this study period, ato-moxetine responders were required to con-tinuously maintain their initial treatment re-sponses for 3 months after assessment at Visit7 (Week 12) and through assessment at Visit11 (Week 24), except for 1 excursion. An“excursion” was a brief shift in the patient’ssymptoms or behavior that did not affect thecore ADHD symptoms, but was reflected inthe patient’s overall CGI-ADHD-S score. Anexcursion was defined as a change (worsen-ing) in the CGI-ADHD-S ≤1 point from thepatient’s Visit 7 score, not to exceed a scoreof 4 (moderately ill) and a CAARS-Inv:SVtotal ADHD symptom score that still met the
response criterion (reduction ≥30% in thebaseline [Visit 2] score).
The last portion of the third study periodwas a 25-week double-blind, randomizedwithdrawal phase in which atomoxetine re-sponders who were able to maintain theirtreatment responses were randomized in a1:1 ratio to atomoxetine (80 or 100 mg/day)or placebo. During this study period, patientsmust have continuously met the response cri-teria for 25 weeks, after assessment at Visit11 (Week 24) and through assessment at Visit18 (Week 49), except for a total of 2 excur-sions. Patients were allowed 1 excursion af-ter assessment at Week 24 and through as-sessment at Week 37 (13 weeks) and anotherexcursion after assessment at Week 37 andthrough assessment at Week 49 (12 weeks).Patients were not permitted to have excur-sions at 2 consecutive visits. To be considereda relapser, patients must have had 2 consec-utive visits with a CGI-ADHD-S score ≥4points and a return to ≥80% of the patient’sbaseline (Visit 2) CAARS-Inv:SV total scoreafter Visit 11 (Week 24). If, at any singlevisit, a patient showed evidence of a return ofsymptoms that met the severity criteria and,because of worsening symptoms, was un-willing to remain in the study or did not re-turn for a second visit, the patient was alsoconsidered to have relapsed and was discon-tinued from the study.
Safety Assessments
Safety measures recorded at every visit in-cluded spontaneously reported AEs, weight,and sitting blood pressure (BP) and heart rate(HR). Treatment-emergent AEs (TEAEs)were defined as events that first occurred orworsened after study entry, as compared withthe maximum severity at or before randomi-sation. Serious AEs (SAEs) were defined asany AE that met one of the following criteria:
SAFETY OF ATOMOXETINE IN ADULTS WITH ADHD 209

death; initial or prolonged inpatient hospi-talisation; a life-threatening experience (i.e.,immediate risk of dying); persistent or sig-nificant disability/incapacitation; congenitalanomaly/birth defect; or an event consideredsignificant by the investigator for any otherreason. All SAEs and TEAEs were reportedaccording to the Medical Dictionary for Reg-ulatory Activities (MedDRA), Version 14.
Sitting vital signs were measured at everyvisit. Investigators at each clinical trial sitewere instructed to measure sitting BP twiceat each visit with at least 5 minutes in betweeneach measurement, and report the mean of the2 measurements. Treatment-emergent abnor-mally high systolic BP (SBP) was defined as
an increase ≥20 mmHg from baseline to avalue ≥160 mmHg, and abnormally low wasdefined as a decrease ≥20 mmHg from base-line to a value ≤90 mmHg. Abnormally highdiastolic BP (DBP) was defined as an in-crease ≥10 mmHg from baseline to a value≥100 mmHg, and abnormally low was de-fined as a decrease ≥10 mmHg from baselineto a value ≤50 mmHg. Abnormally high HRwas defined as an increase ≥15 bpm frombaseline to a value >120 bpm, and abnor-mally low was defined as a decrease ≥15 bpmfrom baseline to a value <50 bpm.
Weight was measured at baseline (screen-ing), Visit 7, Visit 15, and the final study visit.Treatment-emergent abnormal weight gain
210 ANGELO CAMPOREALE ET AL.
Figure 1. Illustration of study design.
Abbreviations: ATX = atomoxetine; PBO = placebo; Wks = weeks.

was defined as ≥7% increase from baseline.Abnormal weight loss was defined as ≥7%decrease from baseline. An electrocardiogram(ECG) was collected at baseline (Visit 1 or be-tween Visit 1 and Visit 2), Visit 7, and the fi-nal study visit (including early termination).Standard laboratory tests, including chem-istry, hematology, and urinalysis panels, werecollected at baseline. Other laboratory testssuch as a urine drug screen, thyroid functiontest, and pregnancy tests (urine and serum),were completed at baseline. Follow-up labo-ratory measurements were not planned, andonly conducted at the discretion of the localinvestigator. Therefore, analyses of labora-tory data are not presented.
Prior to administration of study drug atVisit 2 and at each subsequent visit, suicidal-ity was evaluated by a study physician usingthe Columbia Suicide-Severity Rating Scale(C-SSRS)30. Additional safety measures in-cluded the Hamilton Anxiety Rating Scale–14items (HAMA)31,32 and the Hamilton De-pression Rating Scale–17 items (HAMD-17)33,34, which were collected at baseline,Visit 7, and the final study visit.
Statistical Analyses
Safety analyses were performed on thesafety analysis set, which included data fromall patients receiving at least 1 dose of thestudy drug according to the treatment the pa-tients actually received. Safety data were an-alyzed prerandomisation (open-label treat-ment period combined with the double-blindmaintenance period [i.e., 24 weeks atomox-etine]) and postrandomisation (double-blindrandomised withdrawal period [i.e., 25 weeksatomoxetine or placebo]). For the 24-weekprerandomisation analyses, baseline was con-sidered the last available observation of Vis-its 1 and 2. For the 25-week, double-blindpostrandomisation analyses, baseline was
considered the last measurement obtained onor before the randomisation visit. Exposure tostudy drug was summarized prerandomisa-tion and postrandomisation.
Categorical variables were summarized.Postrandomisation treatment differenceswere compared with Fisher’s exact test. Forpredefined abnormalities, only patients witha normal baseline value were included in theanalysis. Post hoc analyses of the incidenceand persistence of the most common AEswere performed postrandomisation.
Wilcoxon signed-ranked tests were usedto assess within-group changes from base-line for continuous variables. Postrandomisa-tion treatment differences for these measureswere analyzed using an analysis of covariancemodel with the terms treatment, investigator,and baseline; however, the HAMA andHAMD-17 were analyzed using an analysisof variance model with the terms for treatmentand investigator. For early dropout patients,endpoint was imputed using the last-observa-tion-carried-forward approach. Chan ges frombaseline in QT corrections were performedusing the Bazett’s (QTcB) and Fridericia’s(QTcF) QT corrections.
All tests were 2-sided and conducted at the0.05 alpha level. All statistical analyses wereperformed using SAS, version 9.1 (SAS In-stitute, Inc, Cary, NC). These analyses wereperformed on an intent-to-treat basis.
Results
Patient Disposition, Demographics,and Discontinuation
Of the 2534 patients screened, 2017 wereenrolled into the study and 517 failed screen-ing. Of the 2017 enrolled patients, 1493 dis-continued prerandomisation (open-label ato-
SAFETY OF ATOMOXETINE IN ADULTS WITH ADHD 211

moxetine and double-blind maintenance pe-riods combined) for reasons such as AEs(17.3%), response maintenance criteria notmet (16.0%), subject decision (12.1%), pro-tocol violation (11.4%), and lost to follow-up(7.4%), lack of efficacy (6.0%), critical re-lapse (2.8 %), physician decision (0.5 %),missing (0.2 %), sponsor criteria not met (0.1%), and entry criteria not met (0.1 %). In to-tal, 524 patients, who met the response main-tenance criteria at Visit 11 were randomizedto atomoxetine (N = 266) or placebo (N =258). Of these, 184 (69.2%) atomoxetine-treated and 165 (64.0%) placebo-treated pa-tients completed the study.
Prerandomisation, 2011 patients received≥1 dose of atomoxetine (mean exposure =105.2 days). Mean exposure to atomoxetinepostrandomisation was 158.9 days. Most pa-tients were White and male (Table 1; seeUpadhyaya et al.26 for additional patientcharacteristics). Postrandomisation, patientdemographics were similar between the treat-ments (Table 1).
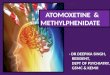
Figure 2 shows AEs leading to discontin-uation reported with ≥0.5% frequency pre-randomisation. Postrandomisation reasonsfor discontinuation were similar between ato-moxetine and placebo with the exceptions oflack of efficacy (1.1% vs. 4.3%; P = .031)and response maintenance criteria not beingmet (0.0% vs. 1.9%; P = .028). Overall inci-dence of discontinuations due to an AE wassimilar between atomoxetine and placebo(3.4% vs. 1.9% P = .418), and no single AEwas predominant (depression and myocardialinfarction were 0.4% vs. 0.4%; depressedmood, ejaculation disorder, erectile dysfunc-tion, hyperhidrosis, hypertension, nausea,and oral disorder were 0.4% vs. 0.0%; breastdisorder, tremor, and weight increased were0.0% vs. 0.4%).
Serious Adverse Events
Twenty-nine of 2011 (1.4%) patients ex-perienced 35 SAEs prerandomisation. Six6
patients each experienced 2 SAEs and 23 pa-tients each experienced a single SAE. Themost common SAE was accidental overdoseof study drug (0.2%). Of the 35 SAEs, 8were judged by the investigator to be treat-ment-related (alcohol abuse and 2 events ofrestlessness in 1 patient; haemorrhage andheadache in 1 patient; bradykinesia, suicidalideation; palpitations; and auditory halluci-nation). All 5 patients who experienced theseSAEs discontinued from the study.
Of the 524 randomized patients, there wasno significant difference in the incidence ofSAEs between atomoxetine and placebo(2.6% vs. 1.6%; P = .55). Seven patients re-ceiving atomoxetine each experienced a sin-gle SAE and 4 patients receiving placeboeach experienced a single SAE. Of the 11SAEs, 1 (myocardial infarction) experiencedby a placebo-treated patient was judged bythe investigator to be related to study treat-ment; the patient discontinued from the study.
One death (reported as suspected myocar-dial infarction by the principal investigator atthe study site) occurred at Visit 14 in a malepatient. There is no confirmation of the di-agnosis; it is unknown at the time of this re-port if an autopsy was conducted. The patientreceived open-label atomoxetine at Visits 2and 3 (40 mg/day), Visit 4 (80 mg/day), andfrom Visits 5 to 6 (100 mg/day). From Visits7 to 14, the patient continued to receiveblinded atomoxetine (100 mg/day). The in-vestigator was unable to assess the related-ness between this event and blinded studydrug, open-label atomoxetine, or protocolprocedures. The patient had a partial block ofthe right bundle branch (heart) as seen by theinvestigator in the ECG at the time of en-rollment and in a second ECG performed
212 ANGELO CAMPOREALE ET AL.

SAFETY OF ATOMOXETINE IN ADULTS WITH ADHD 213Ta
ble
1Pa
tient
Dem
ogra
phic
s
25 W
eeks
Dou
ble-
Blin
d T
reat
men
t
Var
iabl
e 24
Wee
ks A
TX
Tre
atm
ent
AT
XPB
OTo
tal
N =
201
7N
= 2
66N
= 2
58N
-524
P
Sex
Fem
ale,
n (
%)
833
(41.
3)11
5 (4
3.2)
103
(39.
9)21
8 (4
1.6)
.478
a
Mal
e, n
(%
) 11
84 (
58.7
)15
1 (5
6.8)
155
(60.
1)30
6 (5
8.4)
Age
Mea
n, y
ear
(SD
) 33
.2 (
9.1)
33.7
(9.
5)32
.4 (
9.2)
33.1
(9.
4).1
18b
Ran
ge, y
ear
18-5
118
-51
18-5
118
-51
Phy
sica
l Cha
ract
eris
tics
Wei
ght
Mea
n, k
g (S
D)
79.0
(18
.7)
79.6
(18
.9)
78.9
(17
.1)
79.3
(18
.0)
.663
b
Bod
y M
ass
Inde
x
Mea
n, k
g/m
E2
(SD
)26
.4 (
5.6)
26.8
(5.
9)26
.3 (
5.3)
26.5
(5.
6).2
96b
Eth
nici
ty, n
(%
)
Whi
te
1765
(87
.5)
229
(86.
1)22
0 (8
5.3)
449
(85.
7).3
72a
His
pani
c 15
9 (7
.9)
31 (
11.7
)27
(10
.5)
58 (
11.1
)
Afr
ican
56
(2.
8)4
(1.5
)7
(2.7
)11
(2.
1)
Nat
ive
Am
eric
an
6 (0
.3)
0 (0
.0)
0 (0
.0)
0 (0
.0)
Eas
t Asi
an
14 (
0.7)
2 (0
.8)
1 (0
.4)
3 (0
.6)
Wes
t Asi
an
15 (
0.7)
0 (0
.0)
3 (1
.2)
3 (0
.6)
Mis
sing
2
(0.1
)0
(0.0
)0
(0.0
)0
(0.0
)
Abb
reva
tions
: AT
X =
ato
mox
etin
e; n
= n
umbe
r of
pat
ient
s in
age
sub
grou
p; N
= to
tal n
umbe
r of
pat
ient
s in
eac
h tr
eatm
ent g
roup
; PB
O =
pla
cebo
; SD
= s
tan-
dard
dev
iatio
n.a
P-v
alue
is f
rom
Fis
her’
s ex
act t
est.
bP
-val
ue is
fro
m t-
test
.

during the study; however, a cardiologist con-sidered these ECGs to be normal. No ECG re-sults before enrollment were available. Thepatient had normal BP and HR at the begin-ning and throughout the trial. Before treat-ment, cholesterol level was 6.92 mmol/L (ref-erence range = 3.88-6.83) and creatinephosphokinase was 249 U/L (reference range= 18-198). There was no history of smoking,substance abuse, angina, myocardial infarc-tion, arrhythmia, hypercholesterolemia, orcardiovascular disease. The patient was nottaking cardiovascular medications; however,it was not reported if the patient was takingother concomitant medications.
Treatment-Emergent AdverseEvents
Approximately 80% of patients experi-enced ≥1 TEAE prerandomisation. Eventsreported with ≥5% incidence are shown inTable 2. Of the 2011 patients in the safetysample, 1614 reported a TEAE. Of these,30.4%, 38.0%, and 11.8% reported a maxi-mum severity of mild, moderate, and severe,respectively. One patient reported “more se-vere than baseline.” Nausea, reported by27.4% of patients, was the most frequentTEAE; only, 2.4% of all patients discontin-ued because of nausea (Figure 2). Thisequates to a discontinuation rate of 8.7% inpatients experiencing nausea during atom-oxetine treatment.
214 ANGELO CAMPOREALE ET AL.
Figure 2. Adverse events leading to discontinuation in ≥0.5% of patients during the first 24 weeks of atomoxetinetreatment before randomisation (N = 2011). The white bar represents the percentage of total patients treated with
atomoxetine reporting each adverse event; solid portions represent the percentage of total patients treatedwith atomoxetine that discontinued because of the adverse event. Abbreviations: AE = adverse event.

SAFETY OF ATOMOXETINE IN ADULTS WITH ADHD 215
Postrandomisation, approximately 42.4%of patients experienced ≥1 TEAE(s), withthe overall incidence of patients being sig-nificantly higher for atomoxetine thanplacebo (Table 2; P = .034); however, no sig-nificant differences were observed for any in-dividual TEAE in any system organ class. Ofthe 524 randomized patients, 222 had aTEAE. Of these, 17.7%, 19.7%, and 4.4% re-ported a maximum severity of mild, moder-ate, and severe, respectively. Three patientsreported “more severe than baseline.” Posthoc summaries of the weekly incidence of themost common TEAEs showed few new oc-currences of each respective TEAE for anygiven week. Persistence of TEAEs was nu-merically higher in atomoxetine vs. placebofor nausea, dry mouth, fatigue, hyperhidrosis,dizziness, and nasopharyngitis. It should benoted, however, for TEAEs such as fatigue,all 19 persistent occurrences took place in asingle patient. Likewise, for dry mouth, all 17persistent occurrences were for 3 patients.
Vital Signs and Body Weight
Prerandomisation, increases from baselinein SBP, DBP, and HR were significant, aswere decreases from baseline for body massindex (BMI) and weight (Table 3; P <0.001each). Frequencies of treatment-emergent ab-normal high and low vital signs were as fol-lows: SBP (1.3% and 0.7%), DBP (2.9% and0.6%), and HR (0.5% and 0.2%). Only 1.7%and 5.2% of patients had abnormal weightgain or loss, respectively. The number (%) ofpatients with cardiac or weight-related TEAEsleading to discontinuation was small (tachy-cardia [0.4%], hypertension [0.3%], palpita-tions [0.1%], decreased appetite [0.1%], andBP increased [0.0%; 1 in 2011 patients]).
After discontinuation of atomoxetine (dur-ing the double-blind randomized withdrawal
phase), patients on placebo showed a statisti-cally significantly larger reduction in DBPand HR compared to patients who continuedtaking atomoxetine (Table 3; P <0.001 foreach). The reductions in BMI and weight foratomoxetine were significantly different fromthe elevations observed for placebo (P <0.001for each). Treatment-emergent abnormal lowor high changes in SBP and DBP, HR, andweight were not significantly different be-tween treatments. The number (%) of patientswith cardiac or weight-related TEAEs leadingto discontinuation was small for atomoxetine(hypertension [0.4%] myocardial infarction[0.4%]) and for placebo (myocardial infarc-tion [0.4%] and weight gain [0.4%]).
Electrocardiograms
Prerandomisation changes in QTcB,QTcF, uncorrected QT, PR, QRS, and HR areshown in Table 4. No patient had a QTcF orQTcB >500 ms. Increases from baseline inQTcF and QTcB >30 ms were observed in2.1% and 13.7% of patients, respectively. Nopatient showed an increase from baseline inQTcF and QTcB >60 ms. There was no shiftto prolonged QTcB and QTcF (>500 ms) forpatients with normal ECG parameters atbaseline. For patients with borderline para-meters at baseline, there was no shift to pro-longed QTcB or QTcF (>500 ms).
Postrandomisation changes in QTcB,QTcF, uncorrected QT, PR, QRS, and HR areshown in Table 4. No patient had a QTcF orQTcB >500 ms. There were no significantdifferences between atomoxetine and placeboin the frequencies of patients showing an in-crease from baseline in QTcF (1.4% vs.2.6%) or QTcB (2.8% vs. 2.6%) >30 ms. Nopatients showed an increase from baseline inQTcF or QTcB >60 ms. There was no shift toprolonged QTcB or QTcF for patients with

216 ANGELO CAMPOREALE ET AL.
Tabl
e 2
Inci
denc
e of
Mos
t Com
mon
Tre
atm
ent-
Em
erge
nt A
dver
se E
vent
s by
Pre
ferr
ed T
erm
24 W
eeks
AT
X T
reat
men
t25
Wee
ks D
oubl
e-B
lind
Tre
atm
ent T
otal
Med
DR
A P
refe
rred
Ter
mA
TX
N =
201
1A
TX
N =
266
PBO
N =
258
Tota
l Pat
ient
sP
b
Inci
denc
eIn
cide
nce
Pers
iste
ncea
Inci
denc
ePe
rsis
tenc
ea
N (
%)
N (
%)
NN
(%
)N
Patie
nts
with
≥ 1
TE
AE
1614
(80
.3)
125
(47.
0)–
97 (
37.6
)–
222
(42.
4).0
34
Nau
sea
552
(27.
5)6
(2.3
)c19
3 (1
.2)d
79
(1.7
).5
04
Hea
dach
e34
8 (1
7.3)
13 (
4.9)
e12
11 (
4.3)
f22
24 (
4.6)
.835
Dry
Mou
th34
2 (1
7.0)
3 (1
.1)g
182
(0.8
)h10
5 (1
.0)
1.00
Dec
reas
ed a
ppet
ite29
4 (1
4.6)
1 (0
.4)i
11
(0.4
)j3
2 (0
.4)
1.00
Fatig
ue26
2 (1
3.0)
1 (0
.4)k
193
(1.2
)l17
4 (0
.8)
.366
Hyp
erhi
dros
is18
0 (9
.0)
2 (0
.8)m
200
(0.0
)0
2 (0
.4)
.499
Inso
mni
a17
7 (8
.8)
3 (1
.1)n
181
(0.4
)o26
4 (0
.8)
.624
Diz
zine
ss17
0 (8
.5)
1 (0
.4)p
172
(0.8
)q0
3 (0
.6)
.619
Nas
opha
ryng
itis
137
(6.8
)18
(6.
8)r
2913
(5.
0)s
1431
(5.
9).4
61
Som
nole
nce
112
(5.6
)1
(0.4
)t0
1 (0
.4)u
62
(0.4
)1.
00
Abb
revi
atio
ns: A
TX
= a
tom
oxet
ine;
Med
DR
A =
Med
ical
Dic
tiona
ry f
or R
egul
ator
y A
ctiv
ities
; N =
tota
l num
ber
of p
atie
nts
in e
ach
trea
tmen
t gro
up; n
= n
um-
ber
of o
ccur
renc
es; P
BO
= p
lace
bo; T
EA
E =
trea
tmen
t-em
erge
nt a
dver
se e
vent
.

SAFETY OF ATOMOXETINE IN ADULTS WITH ADHD 217
aPe
rsis
tenc
e of
TE
AE
doe
s no
t inc
lude
new
occ
urre
nce
of T
EA
E (
inci
denc
e).
bP
-val
ue f
or in
cide
nce
duri
ng d
oubl
e-bl
ind
trea
tmen
t.c
Inci
denc
e (n
[%])
of
naus
ea in
AT
X g
roup
at W
eeks
26,
27,
45,
and
51
was
1(0
.4)
each
wee
k, a
nd f
or W
eek
31 w
as 2
(0.8
).d
Inci
denc
e (n
[%])
of
naus
ea in
PB
O g
roup
at W
eeks
26,
37,
and
44
was
1(0
.4)
each
wee
k.e
Inci
denc
e (n
[%])
of
head
ache
in A
TX
gro
up a
t Wee
ks 2
8, 3
0, 3
3, 3
6, 3
8, 3
9, 4
1-43
, 46,
and
Wee
k 49
was
1(0
.4)
each
wee
k; W
eek
44 it
was
2(0
.8).
fIn
cide
nce
(n[%
]) o
f he
adac
he in
PB
O g
roup
at W
eeks
25,
26,
32,
41,
45,
and
51
was
1(0
.4)
each
wee
k; W
eek
29 it
was
3(1
.2)
and
Wee
k 33
it w
as 2
(0.8
).g
Inci
denc
e (n
[%])
of
dry
mou
th in
AT
X g
roup
at W
eeks
25,
32,
and
46
was
1(0
.4)
each
wee
k.h
Inci
denc
e (n
[%])
of
dry
mou
th in
PB
O g
roup
at W
eeks
34
and
40 1
(0.4
) ea
ch w
eek.
iIn
cide
nce
(n[%
]) o
f de
crea
sed
appe
tite
in A
TX
gro
up a
t Wee
k 33
was
1(0
.4).
jIn
cide
nce
(n[%
]) o
f de
crea
sed
appe
tite
in P
BO
gro
up a
t Wee
k 28
was
1(0
.4).
kIn
cide
nce
(n[%
]) o
f fa
tigue
in A
TX
gro
up a
t Wee
k 31
was
1(0
.4).
lIn
cide
nce
(n[%
]) o
f fa
tigue
in P
BO
gro
up a
t Wee
ks 3
5, 4
3, a
nd 5
0 w
as 1
(0.4
) ea
ch w
eek.
mIn
cide
nce
(n[%
]) o
f hy
perh
idro
sis
in A
TX
gro
up a
t Wee
k 35
was
2(0
.8).
nIn
cide
nce
(n[%
]) o
f in
som
nia
in A
TX
gro
up a
t Wee
ks 3
8, 3
9 an
d 48
was
1(0
.4)
each
wee
k.o
Inci
denc
e (n
[%])
of
inso
mni
a in
PB
O g
roup
at W
eek
25 w
as 1
(0.4
).p
Inci
denc
e (n
[%])
of
dizz
ines
s in
AT
X g
roup
at W
eek
34 w
as 1
(0.4
).q
Inci
denc
e (n
[%])
of
dizz
ines
s in
PB
O g
roup
at W
eeks
31
and
50 w
as 1
(0.4
) ea
ch w
eek.
rIn
cide
nce
(n[%
]) o
f na
soph
aryn
gitis
in A
TX
gro
up a
t Wee
ks 2
7, 2
9, 3
4, 3
7, 4
0, 4
1, 4
5, 4
6, 4
8, a
nd 5
0 w
as 1
(0.4
) ea
ch w
eek;
Wee
ks 2
6 an
d 28
it w
as 2
(0.8
)ea
ch w
eek,
and
Wee
k 33
it w
as 4
(1.5
).s
Inci
denc
e (n
[%])
of
naso
phar
yngi
tis in
PB
O g
roup
at W
eeks
25,
27,
28,
32,
35,
37,
38,
40,
41,
45,
50,
was
1(0
.4)
each
wee
k; W
eek
33 it
was
2(0
.8).
tIn
cide
nce
(n[%
]) o
f so
mno
lenc
e in
AT
X g
roup
at W
eek
50 w
as 1
(0.4
).u
Inci
denc
e (n
[%])
of
som
nole
nce
in P
BO
gro
up a
t Wee
k 34
was
1(0
.4).

218 ANGELO CAMPOREALE ET AL.
Tabl
e 3
Mea
n C
hang
e Fr
om B
asel
ine
to E
ndpo
int i
n V
ital S
igns
and
Phy
sica
l Cha
ract
eris
tics
24 W
eeks
AT
X T
reat
men
t (N
= 2
011)
25 W
eeks
Dou
ble-
Blin
d T
reat
men
t
Mea
sure
AT
X (
N =
266
)PB
O (
N =
258
)
Bas
elin
eaΔ
to E
ndpo
int
Pb
Bas
elin
ecΔ
to E
ndpo
int
Bas
elin
ecΔ
to E
ndpo
int
Pd
Mea
n (S
D)
LSM
ean
(SE
)M
ean
(SD
)L
SMea
n(S
E)
Mea
n (S
D)
LSM
ean
(SE
)
Vita
l Sig
ns
SBP
120.
2 (1
1.5)
1.3
(0.3
)<
.001
122.
0 (1
1.4)
-0.7
(0.
7)12
1.1
(12.
1)-0
.9 (
0.7)
.825
DB
P75
.7 (
8.9)
1.6
(0.3
)<
.001
77.9
(8.
8)-0
.1 (
0.5)
78.0
(8.
8)-2
.3 (
0.5)
<.0
01
HR
73.1
(10
.0)
5.4
(0.3
)<
.001
79.7
(11
.2)
-1.4
(0.
6)79
.1 (
11.4
)-5
.3 (
0.6)
<.0
01
Phys
ical
Cha
ract
eris
tics
Bod
y W
eigh
t79
.2 (
18.9
)-0
.8 (
0.1)
<.0
0178
.9 (
18.5
)-0
.2 (
0.3)
77.5
(16
.4)
1.1
(0.3
)<
.001
BM
I26
.4 (
5.7)
-0.3
(0.
0)<
.001
26.6
(5.
8)-0
.1 (
0.1)
25.9
(5.
2)0.
4 (0
.1)
<.0
01
Abb
revi
atio
ns: A
TX
= a
tom
oxet
ine;
BM
I =
bod
y m
ass
inde
x; D
BP
= d
iast
olic
blo
od p
ress
ure;
HR
= h
eart
rat
e; N
= to
tal n
umbe
r of
pat
ient
s in
eac
h tr
eatm
ent
grou
p; P
BO
= p
lace
bo; S
BP
= s
ysto
lic b
lood
pre
ssur
e; S
D =
sta
ndar
d de
viat
ion;
SE
= s
tand
ard
erro
r.
aPr
eran
dom
isat
ion
base
line
was
con
side
red
the
last
ava
ilabl
e ob
serv
atio
n of
Vis
its 1
and
2.
bP
-val
ues
are
from
Wilc
oxon
’s s
igne
d-ra
nk te
st.
cPo
stra
ndom
isat
ion
base
line
was
con
side
red
the
last
mea
sure
men
t obt
aine
d on
or
befo
re th
e ra
ndom
isat
ion
visi
t (V
isit
11).
dP
-val
ues
are
from
Typ
e 3
sum
s of
squ
ares
ana
lysi
s of
cov
aria
nce
mod
el: C
hang
e =
trea
tmen
t+po
oled
inve
stig
ator
+ba
selin
e (c
ontin
uous
cov
aria
te o
f ba
selin
evi
tal s
ign)
.

SAFETY OF ATOMOXETINE IN ADULTS WITH ADHD 219
Tabl
e 4
Mea
n C
hang
e Fr
om B
asel
ine
to E
ndpo
int i
n E
lect
roca
rdio
gram
Par
amet
ers
24 W
eeks
AT
X T
reat
men
t (N
= 2
011)
25 W
eeks
Dou
ble-
Blin
d T
reat
men
t
Mea
sure
AT
X (
N =
266
)PB
O (
N =
258
)
Bas
elin
eaΔ
to E
ndpo
int
Pb
Bas
elin
ecΔ
to E
ndpo
int
Bas
elin
ecΔ
to E
ndpo
int
Pd
Mea
n (S
D)
LSM
ean
(SE
)M
ean
(SD
)L
SMea
n(S
E)
Mea
n (S
D)
LSM
ean
(SE
)
QT
cB40
7.0
(21.
1)8.
2 (0
.6)
<.0
0141
7.1
(19.
8)-1
.6 (
1.2)
417.
4 (1
7.8)
-5.9
(1.
3).0
07
QT
cF40
0.6
(17.
5)-0
.1 (
0.5)
.011
400.
4 (1
7.0)
0.8
(1.0
)39
9.2
(15.
8)2.
3 (1
.0)
.207
QT
(un
corr
ecte
d)38
9.0
(26.
3)
-15.
4 (0
.8)
<.0
0136
9.9
(26.
3)5.
4 (1
.7)
366.
0 (2
6.8)
17.2
(1.
8)<
.001
PR15
2.5
(20.
2)-4
.2 (
0.4)
<.0
0114
6.6
(19.
1)0.
2 (0
.8)
147.
9 (1
9.2)
4.1
(0.9
)<
.001
QR
S93
.5 (
9.3)
-0.4
(0.
2).0
4393
.4 (
9.3)
-0.5
(0.
5)92
.2 (
8.9)
0.7
(0.5
).0
68
HR
66.7
(10
.6)
8.7
(0.4
)<
.001
77.3
(12
.0)
-2.6
(0.
8)79
.3 (
12.4
)-9
.1 (
0.8)
<.0
01
Abb
revi
atio
ns: A
TX
= a
tom
oxet
ine;
HR
= h
eart
rat
e; L
SMea
n =
leas
t-sq
uare
s m
ean;
N=
tota
l num
ber
of p
atie
nts
in e
ach
trea
tmen
t gro
up; P
BO
= p
lace
bo;
QT
cB =
Baz
ett’s
QT
cor
rect
ion;
QT
cF =
Fri
deri
cia’
s Q
T c
orre
ctio
n; S
D =
sta
ndar
d de
viat
ion;
SE
= s
tand
ard
erro
r.
aPr
eran
dom
isat
ion
base
line
was
con
side
red
the
last
ava
ilabl
e ob
serv
atio
n of
Vis
its 1
and
2.
bP
-val
ues
are
from
Wilc
oxon
’s s
igne
d-ra
nk te
st.
cPo
stra
ndom
isat
ion
base
line
was
con
side
red
the
last
mea
sure
men
t obt
aine
d on
or
befo
re th
e ra
ndom
isat
ion
visi
t (V
isit
11).
dP
-val
ues
are
from
Typ
e 3
sum
s of
squ
ares
ana
lysi
s of
cov
aria
nce
mod
el: C
hang
e =
trea
tmen
t+po
oled
inve
stig
ator
+ba
selin
e.

normal ECG parameters at baseline. For pa-tients with borderline parameters at baseline,there was no shift to prolonged QTcB orQTcF (>500 ms).
Columbia Suicide-Severity RatingScale and Suicide-Related Events
Prerandomisation, 56 of 2011 (2.8%) pa-tients reported suicide-related events as so-licited by the C-SSRS: 55 (2.7%) reportedsuicidal ideation and 2 (0.1%) reported suici-dal behaviors, both of which were nonfatal sui-cide attempts. One single patient reported bothsuicidal ideation and behaviors. A subset (35of 56) of patients reported a suicide-relatedevent that was a new occurrence followingenrollment or an event which worsened afterenrollment. Only 10 (0.5%) patients, how-ever, experienced an unsolicited TEAE ofsuicide ideation; 3 were SAEs, 2 of which ledto study discontinuation. There were 135(6.7%) patients who showed an improvementin suicidal ideation at endpoint relative tobaseline.
The relative postrandomisation frequen-cies of suicide-related events, as solicited bythe C-SSRS, were not significantly differentbetween atomoxetine and placebo (6 of 266[2.3%] vs. 3 of 258 [1.2%]; P = 0.504). Ofthe 6 atomoxetine-treated patients, 4 reportedexperiencing suicidal ideation, 1 reported ex-periencing suicidal behavior, and 1 reportedexperiencing both suicidal ideation and be-havior. Of the 3 placebo-treated patients re-porting suicide-related events, all 3 reportedexperiencing suicidal ideation and none re-ported experiencing suicidal behavior. Sixatomoxetine-treated patients and 2 placebo-treated patients reported a suicide-relatedevent that was a new occurrence followingenrollment or an event which worsened afterenrollment; however, there were no unso-licited TEAEs, SAEs, or discontinuations due
to a suicide-related event. The relative fre-quencies of these new/worsened occurrencessolicited via the C-SSRS were not signifi-cantly different between treatments.
Hamilton Anxiety Rating Scale-14Items and Depression RatingScale-17 Items
Prerandomisation changes from baseline inthe HAMA and HAMD-17 total scores (-0.8and -0.3) were statistically significant, butthe differences were too small to be clinicallyrelevant. Postrandomisation changes frombaseline in the HAMA and HAMD-17 totalscores were not significantly different be-tween treatments.
Discussion
This study extends the findings of previousstudies of atomoxetine in adults8,10,11,24,25 byproviding evidence of the long-term safety ofatomoxetine in the largest (to our knowl-edge) clinical trial of an ADHD medication(pediatric or adult) performed to date. Thedata demonstrate that atomoxetine, at thetherapeutic dose studied, has an acceptablesafety profile in a large international, multi-center sample of adult patients with ADHD.Adverse events reported at the highest rateoccurred during the first 24 weeks of atom-oxetine treatment (12-week open label and12-week double-blind maintenance periods),when significant amelioration of ADHDsymptoms was reported by Upadhyaya etal.26 to have occurred. These results wereconsistent with other short-term10,11,24,25 andlong-term studies8 of atomoxetine in adults.
Nausea was the most frequent TEAE andthe main reason for discontinuation preran-
220 ANGELO CAMPOREALE ET AL.

domisation; however, approximately 91.3%of patients who experienced nausea with ato-moxetine remained in the study. This is likelythe result of the typical characteristics ofnausea; it occurred early in treatment, wasusually mild or moderate, and tended to re-solve rapidly in most patients. To that extent,all TEAEs appeared earlier in treatment, asshown by higher prerandomisation incidencerates relative to lower postrandomisationrates; the majority were mild or moderate inseverity. A single death occurred during theclinical trial; this death was reported as sus-pected myocardial infarction by the principalinvestigator at the study site. The right-bun-dle branch block and baseline creatine phos-phokinase and cholesterol values are not sub-stantial risk factors for myocardial infarctionin a 38-year-old male. Myocardial infarctionwould actually seem rather unlikely to bethe cause of death and no conclusions can bedrawn regarding possible causality.
Safety and tolerability are critical featuresin the profile of an ADHD medication. Manypatients are required to take ADHD medica-tion chronically. As a result, the nature of AEsoften weighs heavily in patients risk-benefitassessment and may lead to noncomplianceand/or discontinuation. In the current study,prerandomisation rates of discontinuationdue to each respective AE were relativelylow, and the impact of these TEAEs on initialpatient compliance and overall tolerabilitywas modest relative to other long-term stud-ies of atomoxetine with similar dosing sched-ules8. Prerandomisation rates of discontinu-ation were somewhat higher, however, thanthose observed in short-term studies of ato-moxetine, in which doses were adjustedbased on tolerability10. During double-blindtreatment, no single AE reported as reason fordiscontinuation was significantly differentbetween treatments. The implication of theseresults is that education regarding the non-
progressive and transient nature of commonTEAEs in clinical practice is important andmay increase the number of patients that con-tinue atomoxetine treatment.
Many ADHD medications have potentialadverse cardiovascular effects including in-creases in BP and HR35. In the current study,increases in BP and HR observed after 24weeks of atomoxetine treatment were con-sistent with a noradrenergically mediated in-crease in autonomic tone, but for most pa-tients these increases were modest andasymptomatic. Indeed, less than 0.5% of pa-tients discontinued atomoxetine due to treat-ment-emergent hypertension or tachycardia.These results are comparable with those inmost short-term studies of atomoxetine in chil-dren18-20 and adults10,29,35,36. In patients re-ceiving atomoxetine for an additional 25weeks of double-blind treatment, BP and HRslightly declined relative to baseline at ran-domisation (Week 11). The declines in atom-oxetine-treated patients, however, were sig-nificantly smaller than the declines observed inplacebo-treated patients, whose BP and HR atendpoint returned to prerandomisation base-line values. The small percentages of treat-ment-emergent abnormally high or low BPand HR were not significantly different be-tween the treatments. These results collec-tively extend the findings from previous stud-ies, which have shown that increases in BP andHR usually occur within the first 2 months af-ter atomoxetine treatment and are less likely tooccur after 6 months of treatment10,18.
All ECG changes in the current study wereexpected based on HR changes and did notsuggest an arrhythmogenic potential for ato-moxetine. Mean change to endpoint for allECG parameters was unremarkable includingthose for QT corrections. The observed cat-egorical changes for QT corrections werealso within acceptable limits. Taken together,these BP and ECG results did not identify
SAFETY OF ATOMOXETINE IN ADULTS WITH ADHD 221

any significant cardiovascular risks in thisadult population after up to 1 year of treat-ment with atomoxetine beyond those alreadyknown; clinicians should consider the currentprescribing information on cardiovascularrisks for atomoxetine, and evaluate and mon-itor each individual patient accordingly37.
Atomoxetine has been associated withweight loss during treatment in children18-20
and adults8,29. In the current study, bodyweight decreased after 24 weeks of atomox-etine treatment, but appeared to plateau afteran additional 25 weeks of treatment, despitesignificant differences at the 25-week timepoint between atomoxetine and placebo. Thedifference from placebo may have been mag-nified by a rebound in weight gain in thoserandomized to placebo; however, only 1placebo-treated patient discontinued duringdouble-blind treatment due to weight gain.These results are comparable with results ofa long-term study of atomoxetine in adults8
and are consistent with findings in children38.
Patients with ADHD are at greater risk forsuicidal behavior than the general public39.Whether this increased risk is due to the im-pulsivity inherent in ADHD, other comorbidpsychiatric illnesses, or to other factors thathave yet to be identified is unknown. No pa-tient in atomoxetine ADHD trials has com-mitted suicide, and high rates of suicideideation in both children and adults are un-common. However, small, but significantlyhigher rates of suicidal ideation have been re-ported in a pediatric ADHD populationtreated with atomoxetine vs. placebo40. In thecurrent study, CSSR-S results from double-blind treatment did not suggest a link be-tween atomoxetine and suicidality; therewere no significant differences between treat-ments, and no randomized patient discontin-
ued due to a suicide-related event. Further-more, there were no significant differences be-tween treatments in the HAMD and HAMA,supporting the hypothesis that atomoxetinedid not negatively impact depression or anx-iety, respectively.
Several factors limit the interpretation ofthe data presented here. No comparisons withother drugs were included. The ability togeneralize these results to typical outpatientsis somewhat limited, as patients in this studyhad relatively fewer comorbid medical con-ditions and concomitant medications thantheir general outpatient counterparts. Fur-thermore, the low rate of AEs and discontin-uations during double-blind treatment may beartifacts of the fact that all patients in thedouble-blind treatment phase of this studyhad been treated with atomoxetine for 24weeks before randomisation. Indeed, thesedata only describe a subpopulation that re-sponded to atomoxetine and were compliantwith the lengthy study protocol schedule.
This study demonstrated that atomoxetineexhibited an acceptable safety profile inadults with ADHD during 24 weeks of treat-ment and during an additional 25 weeks ofdouble-blind treatment in the largest clinicaltrial of ADHD in adults to date. No clinicallymeaningful rebound effects related to safetywere seen after abrupt discontinuation of ato-moxetine, suggesting that patients do notneed to be tapered when discontinuing treat-ment. Patients and their physicians will needto balance the value of an individual’s treat-ment against the risk and management of po-tential side effects. Individuals that achieve anacceptable level of improvement in ADHDsymptoms and atomoxetine tolerability arethose who should consider continued medicaltreatment.
222 ANGELO CAMPOREALE ET AL.

References
1. Biederman J, Spencer T. Attention-deficit/hyperactiv-ity disorder (ADHD) as a noradrenergic disorder. Biol Psy-chiatry 1999; 46(9): 1234-1242.
2. Faraone SV, Biederman J. Neurobiology of attention-deficit hyperactivity disorder. Biol Psychiatry 1998; 44(10):951-958.
3. Zametkin AJ, Liotta W. The neurobiology of attention-deficit/hyperactivity disorder. J Clin Psychiatry 1998;59(Suppl 7): 17-23.
4. Barkley RA, Fischer M, Smallish L, Fletcher K. Thepersistence of attention deficit/hyperactivity disorder intoyoung adulthood as a function of reporting source and defi-nition of disorder. J Abnorm Psychol 2002; 111(2): 279-289.
5. Mannuzza S, Klein RG, Moulton JL 3rd. Persistenceof attention-deficit/hyperactivity disorder into adulthood:what have we learned from the prospective follow-up stud-ies? J Atten Disord 2003; 7(2): 93-100.
6. Adler L, Cohen J. Diagnosis and evaluation of adultswith attention-deficit/hyperactivity disorder. Psychiatr ClinNorth Am 2004; 27(2): 187-201.
7. Kooij SJ, Bejerot S, Blackwell A, Caci H, Casas-Brugué M, Carpentier PJ, et al. European consensus state-ment on diagnosis and treatment of adult ADHD: the Euro-pean network adult ADHD. BMC Psychiatry 2010; 10:67.
8. Adler LA, Spencer T, Brown TE, Holdnack J, SaylorK, Schuh K, et al. Once-daily atomoxetine for adult atten-tion-deficit/hyperactivity disorder: a 6-month, double-blindtrial. J Clin Psychopharmacol 2009; 29(1): 44-50.
9. Biederman J, Mick E, Surman C, Doyle R, Hammer-ness P, Kotarski M, et al. A randomized, 3-phase, 34-week,double-blind, long-term efficacy study of osmotic-releaseoral system methylphenidate in adults with attention-deficit/hyperactivity disorder. J Clin Psychopharmacol 2010; 30(5):549-553.
10. Michelson D, Adler L, Spencer T, Reimherr FW,West SA, Allen AJ, et al. Atomoxetine in adults with ADHD:two randomized, placebo-controlled studies. Biol Psychia-try 2003; 53(2): 112-120.
11. Spencer T, Biederman J, Wilens T, Prince J, Hatch M,Jones J, et al. Effectiveness and tolerability of tomoxetine inadults with attention deficit hyperactivity disorder. Am J Psy-chiatry 1998; 155(5): 693-695.
12. Spencer T, Biederman J, Wilens T, Doyle R, SurmanC, Prince J, et al. A large, double-blind, randomized clini-cal trial of methylphenidate in the treatment of adults withattention deficit/hyperactivity disorder. Biol Psychiatry2005; 57(5): 456-463.
13. Bouffard R, Hechtman L, Minde K, Iaboni-Kassab F.The efficacy of 2 different dosages of methylphenidate intreating adults with attention-deficit hyperactivity disorder.Can J Psychiatry 2003; 48(8): 546-554.
14. Kooij JJ, Burger H, Boonstra AM, Van der Linden PD,Kalma LE, Buitelaar JK. Efficacy and safety of methylphe -nidate in 45 adults with attentiondeficit/hyperactivity dis-order. A randomized placebo-controlled double-blind cross-over trial. Psychol Med 2004; 34(6): 973-982.
15. Medori R, Ramos-Quiroga JA, Casas M, Kooij JJ,Niemelä A, Trott GE, et al. A randomized, placebo-con-trolled trial of three fixed dosages of prolonged-releaseOROS methylphenidate in adults with attention-deficit/hy-peractivity disorder. Biol Psychiatry 2008; 63(10): 981-989.
16. Himpel S, Banaschewski T, Heise CA, RothenbergerA. The safety of non-stimulant agents for the treatment of at-tention-deficit hyperactivity disorder. Expert Opin Drug Saf2005; 4(2): 311-321.
17. Vaughan B, Fegert J, Kratochvil CJ. Update on ato-moxetine in the treatment of attention-deficit/hyperactivitydisorder. Expert Opin Pharmacother 2009; 10(4): 669-676.
18. Kelsey DK, Sumner CR, Casat CD, Coury DL, Quin-tana H, Saylor KE, et al. Once-daily atomoxetine treatmentfor children with attention-deficit/hyperactivity disorder,including an assessment of evening and morning behavior:a double-blind, placebo-controlled trial. Pediatrics 2004;114(1): e1-e8.
19. Michelson D, Faries D, Wernicke J, Kelsey D,Kendrick K, Sallee FR, et al. Atomoxetine ADHD StudyGroup. Atomoxetine in the treatment of children and ado-lescents with attention-deficit/hyperactivity disorder: a ran-domized, placebo-controlled, dose-response study. Pedi-atrics 2001; 108(5): E83.
20. Michelson D, Allen AJ, Busner J, Casat C, Dunn D,Kratochvil C, et al. Once-daily atomoxetine treatment forchildren and adolescents with attention deficit hyperactivitydisorder: a randomized, placebo-controlled study. Am JPsychiatry 2002; 159(11): 1896-901.
21. Michelson D, Buitelaar JK, Danckaerts M, GillbergC, Spencer TJ, Zuddas A, et al. Relapse prevention in pedi-atric patients with ADHD treated with atomoxetine: a ran-domized, double-blind, placebo-controlled study. J Am AcadChild Adolesc Psychiatry 2004; 43(7): 896-904.
22. Newcorn JH, Michelson D, Kratochvil CJ, Allen AJ,Ruff DD, Moore RJ. Atomoxetine Low-dose Study Group.Low-dose atomoxetine for maintenance treatment of atten-tion-deficit/hyperactivity disorder. Pediatrics 2006; 118(6):e1701-e1706.
23. Spencer T, Heiligenstein JH, Biederman J, FariesDE, Kratochvil CJ, Conners CK, et al. Results from 2 proof-of-concept, placebo-controlled studies of atomoxetine in
SAFETY OF ATOMOXETINE IN ADULTS WITH ADHD 223

children with attention-deficit/hyperactivity disorder. J ClinPsychiatry 2002; 63(12): 1140-1147.
24. Wilens TE, Adler LA, Weiss MD, Michelson D,Ramsey JL, Moore RJ, et al. Atomoxetine treatment ofadults with ADHD and comorbid alcohol use disorders.Drug Alcohol Depend 2008; 96(1-2): 145-154.
25. Adler LA, Liebowitz M, Kronenberger W, Qiao M,Rubin R, Hollandbeck M, et al. Atomoxetine treatment inadults with attention-deficit/hyperactivity disorder and co-morbid social anxiety disorder. Depress Anxiety 2009;26(3): 212-221.
26. Upadhyaya H, Ramos-Quiroga JA, Adler JA, Wi -lliams D, Tanaka Y, Lane JR, et al. Maintenance of Responseafter Open-Label Treatment with Atomoxetine Hydrochlo-ride in International European and Non-European AdultOutpatients with Attention-Deficit/Hyperactivity Disorder:A Placebo-Controlled, Randomised Withdrawal Study. Eur.J Psychiat. Submitted 2012.
27. Conners CK, Erhardt D, Sparrow E. Conners’ AdultADHD Rating Scales (CAARS). North Tonawanda: Multi-Health Systems, Inc.; 1999.
28. Guy W. ECDEU Assessment Manual for Psy-chopharmacology, Revised. Bethesda, MD: US Departmentof Health, Education, and Welfare; 1976.
29. Adler LA, Wilens T, Zhang S, Dittmann RW, D’SouzaDN, Schuh L, et al. Atomoxetine treatment outcomes in ado-lescents and young adults with attention-deficit/hyperac-tivity disorder: results from a post hoc, pooled analysis.Clin Ther 2012; 34(2): 363-373.
30. Posner K, Oquendo MA, Gould M, Stanley B, DaviesM. Columbia Classification Algorithm of Suicide Assess-ment (C-CASA): classification of suicidal events in theFDA’s pediatric suicidal risk analysis of antidepressants. AmJ Psychiatry 2007; 164(7): 1035-1043.
31. Hamilton M. The assessment of anxiety states by rat-ing. Br J Med Psychol 1959; 32(1): 50-55.
32. Riskind JH, Beck AT, Brown G, Steer RA. Taking themeasure of anxiety and depression. Validity of the recon-structed Hamilton scales. J Nerv Ment Dis 1987; 175(8):474-479.
33. Hamilton M. A rating scale for depression. J NeurolNeurosurg Psychiatry 1960; 23: 56-62.
34. Hamilton M. Development of a rating scale for pri-mary depressive illness. Br J Soc Clin Psychol 1967; 6(4):278-296.
35. Stiefel G, Besag FM. Cardiovascular effects ofmethylphenidate, amphetamines and atomoxetine in thetreatment of attention-deficit hyperactivity disorder. DrugSaf 2010; 33(10): 821-842.
36. Simpson D, Plosker GL. Atomoxetine: a review of itsuse in adults with attention deficit hyperactivity disorder.Drugs 2004; 64(2):205-222.
37. Strattera (atomoxetine hydrochloride) [package in-sert]. Indianapolis: Eli Lilly and Company; 2011.
38. Spencer TJ, Kratochvil CJ, Sangal RB, Saylor KE,Bailey CE, Dunn DW, et al. Effects of atomoxetine ongrowth in children with attention-deficit/hyperactivity dis-order following up to five years of treatment. J Child Ado-lesc Psychopharmacol 2007; 17(5): 689-700.
39. Impey M, Heun R. Completed suicide, ideation andattempt in attention deficit hyperactivity disorder. Acta Psy-chiatr Scand 2012; 125(2): 93-102.
40. Bangs ME, Tauscher-Wisniewski S, Polzer J, ZhangS, Acharya N, Desaiah D, et al. Meta-analysis of suicide-re-lated behavior events in patients treated with atomoxetine.J Am Acad Child Adolesc Psychiatry 2008; 47(2): 209-218.
Corresponding author:Himanshu Upadhyaya, MBBS, MSSenior Medical AdvisorADAP Team, Neuroscience PlatformEli Lilly & CoLilly Corp. Center, D/C 6112Indianapolis, IN 46285Phone: 317-655-3516Fax: 713-592-0916
224 ANGELO CAMPOREALE ET AL.