Embed Size (px)
Citation preview

AG
AA
bst
ract
sSa1860
Transanal Endoscopic Microsurgery: Colorectal Surgeons' Learning CurveRenée M. Barendse, Marcel G. Dijkgraaf, Ursula Rolf, Evelien Dekker, Paul Fockens,Willem A. Bemelman, Eelco J. de Graaf
Introduction. Transanal endoscopic microsurgery (TEM) is a key technique in minimallyinvasive rectal surgery. TEM is technically demanding and various training programs exist.However, the learning curve of colorectal surgeons who commence with TEM is unknown.We aimed to evaluate the outcomes of colorectal surgeons' first series of TEM proceduresand to assess whether outcomes improved with increasing experience. Methods. The first32 TEM procedures of 4 colorectal surgeons, who completed a dedicated TEM trainingprogram, were analyzed. Patient, lesion and procedure characteristics were collected. Proced-ures were ranked chronologically per surgeon. Outcome parameters included conversionrate, postoperative complications, recurrence, procedure time and hospitalization length.Backward multivariate regression analysis was performed to identify independent predictorsof the outcome parameters. Results. Four colorectal surgeons performed 128 procedures(mean patient age 71 ± 12 years, 48% males, ASA classification 1/2/3 in 30%/55%/9%).Rectal lesions (adenoma / carcinoma / other in 76%/20%/4%, 21% recurrent lesions) hada median size of 13 cm2 (interquartile range (IQR) 6-23). Mean distance ab ano was 6.8 ±4.0 cm. Lesions were located on the posterior, anterior, left and right lateral rectal wall in 47%,20%, 19% and 15%. Resections were performed with three-dimensional (3D) stereoscope in94 cases (73%) and 2D in 34 cases; 67% were full thickness and 89% in one piece. Peritonealbreech occurred in 6 cases (5%). 86 resections (67%) were histopathologically radical (R0)and 42 (33%) were irradical or unsure (R1/Rx). Conversion (overall conversion rate 8%)was predicted by lesion size (odds ratio (OR) 1,046 per cm2, 95% confidence interval (CI)1,016 - 1,075). Postoperative complications (14% overall, 12% surgical) were independentlyassociated with peritoneal breech (overall OR 7,133 (95% CI 1,317 - 38,624), surgical OR9,167 (95% CI 1,662 - 50,562)). Recurrence (11%) was independently associated with 3Dvs. 2D instruments (OR 0,123 (95% CI 0,035 - 0,435). Procedure time (median 90 minutes(IQR 60-90)) was dependent upon the individual surgeon (P<.001), lesion size (regressioncoefficient (B) 2,173 (95% CI 1,745 - 2,601)) and peritoneal breech (B 71,075 (95% CI19,939 - 122,211). Hospitalization (median 5 days (IQR 4-7)) was independently associatedwith patient age (B 0,129 (95% CI 0,047 - 0,211)), lesion size (B 0,069 (95% CI 0,019 -0,119)), distance ab ano (B 0,277 (95% CI 0,013 - 0,542)) and peritoneal breech (B 18,137(95% CI 11,659 - 24,615)). Chronological procedure rank did not predict any of theoutcomes. Discussion. Achieved outcomes correspond with previous literature of TEM inan early phase. As increasing experience was not associated with improved outcomes, thelearning curve of TEM may extend beyond 32 cases in colorectal surgeons.
Sa1861
3De - Introducing the 3rd Dimension to Gastrointestinal EndoscopyHelmut Neumann, Michael Vieth, Claudia Günther, Markus F. Neurath
Background: Endoscopy is the gold standard for diagnosis of various gastrointestinal diseases.Nevertheless, image interpretation and handling is often aggravated because current endos-copy-systems only illustrate 2-dimensional (2D) views without any depth perception. 3-dimensional (3D) images contain more cues, especially in order to accurately and efficientlyguide the action. Moreover, in 2D, examiners tend to underestimate distances when per-forming reaching and grasping movements. Aims: To establish the 3rd dimension in gastroin-testinal endoscopy. Material & Methods: First, standard 2D high-resolution and high-defini-tion endoscopic videos were recorded and digitally stored as high-quality frames. Thedata set was then manipulated in real-time with a special video editing software program(CyberLink, Santa Clara, USA) into 3D videos by using stereoscopic 3D conversion. In orderto display 3D-videos HDMI 1.4 enabled 3DTV with active shutter glasses (NVIDIA , SantaClara, USA) and 120Hz frame-sequential 3D LCD display (LG Electronics, Seoul, NorthKorea) was used. Results: 2D-videos were easily converted into 3D-videos in real-time. Usingactive shutter glasses a real 3D experience with depth perception during the endoscopicprocedure was gathered. Thus, planes were visible that, prior to 3D, could only be imagedand reconstructed mentally. 3D experience was feasible without weakening the examiner.3D enabled the evaluation of gastrointestinal masses and abnormalities in a more precisemanner compared to 2D view and gave a totally new experience of the endoscopic procedure.Conclusions: For the first time, the 3rd dimension was exploited to gastrointestinal endos-copy. 3D-endoscopy (3De) extended our current understanding of endoscopy as the newdepth perception now enables the endoscopist to evaluate the mucosal surface much moreprecisely compared to standard 2D view. The utility of 3De is now evaluated in differentpilot studies for diagnosis and characterization of various diseases, including Barrett's eso-phagus and colon polyps.
Sa1862
3-D Histology of the Human Colonic Microstructure, Vasculature, andInnervation With Optical ClearingYuan-An Liu, Shih-Jung Peng, Yuan-Chiang Chung, Shien-Tung Pan, Yung-Chi Hou,Shiue-Cheng Tang
Background & Aims: Three-dimensional (3-D) microscopy of the intestinal microstructure,vasculature, and innervation is important for understanding the physiology and developingscreening and diagnostic tools for intestinal diseases. However, due to the intrinsic opacityof human biopsies, in-depth imaging of the intestinal tissues has been difficult. Particularly,the dispersed neural and vascular networks in space require substantial sensitivity andresolving power in microscopy to detect and distinguish image signals. In this research, weapply optical clearing to prepare transparent colon specimens to simultaneously visualizethe immunolabeled mucosal microstructure, vasculature, and innervation. Methods: Colonictissues were obtained from colectomies carried out for colorectal carcinoma. Samples of thenormal mucosa were taken at least 5 cm apart from the tumor area. We only focused onthe normal tissue in this study. Triple staining of nuclei, CD34 (endothelial marker), andPGP9.5 (pan-neuronal marker) was used to reveal the microstructure, blood vessels, and
S-344AGA Abstracts
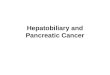
nerves in the mucosa. Optical clearing— use of immersion solution to reduce light scatteringin deep-tissue microscopy (Liu et al., Neurogastroenterol Motil 23:e446, 2011; Smith, NatRev Gastroenterol Hepatol 8:600, 2011) — was applied to prepare transparent colon speci-mens for penetrative confocal microscopy. Afterward, the scanned specimens were retrievedfrom the immersion solution, washed with saline, and then underwent the standard micro-tome-based 2-D immunohistochemistry analysis. Results: Optical clearing led to in-depthimaging, up to 200 μm, of the mucosal microstructure, vasculature, and innervation with highdefinition.We observed organized plexuses of peri-cryptic capillaries and nerves embedded inthe honeycomb structure of the lamina propria. Significantly, the voxel-based 3-D imagedata provided a continuous flow of the anatomic information for panoramic projection anddigital analysis of the vessel and nerve density. In addition, using the vascular morphology,we demonstrate matched tissue information between the 3-D confocal and the standardhematoxylin and eosin (H&E) and immunohistochemistry images. Conclusion: We providea straightforward method to acquire a continuous flow of the anatomic vascular and neuralinformation in situ. This optical method is reversible and can serve as an add-on to thecurrent 2-D histological evaluation of the colorectal biopsies.
(A) Transmitted light micrograph of the optically cleared specimen. (B and C) Penetrativeand 3-D projections of the colonic microstructure (nuclei: gray), vasculature (CD34: red),and innervation (PGP9.5: green) derived from the optically cleared specimen (A). Dimensionof the scanned volume: 460 × 460 × 200 (depth) μm.
Sa1863
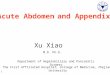
Bio-Texture Modeling Technology of Gastrointestinal Hepatobiliary PancreaticOrgans by Multimaterial 3D Printing SystemMaki Sugimoto
Background 3D printing technologies have been used for manufacturing patient-specificmodels used for planning surgical procedures. However the initial method has been simplyprinted out by one material. Our new technique of bio-texture modeling by multimaterial3D printing system enabled simultaneous jetting of different types of model materials enablingthe simultaneous use of two different rigid materials, two flexible materials, one of eachtype, any combination with transparent material, or two jets of the same material to form3D organ textures and structures. We evaluate an anatomical 3D rapid prototyping modelingof gastrointestinal hepatobiliary pancreatic organs to facilitate planning and execution of themedical and surgical procedure and educational aspects. Metod and result Based on CT andMRI images, regions of interest were segmented using OsiriXMD. After generating an STL-file out of the patient's data set, the 3D printer Connex created a 3D multimaterial organmodel. The patient individual 3D printed models were used to plan and guide the successfulliver resection and orthopedic surgery. The 3D objects using combination of transparentand soft materials allowed creation of translucent medical models that show visceral organsand other details that can be handled, overcome the limitation of the conventional image-guided navigation. The gel-like support material, which is specially designed to supportcomplicated geometries, is easily removed by hand and water jetting. This enabled eachcomposite material to provide specific values of bio-texture in gastrointestinal hepatobiliarypancreatic organs for tensile strength and elongation to break. Discussion These futuristictechnologies provide better gastrointestinal hepatobiliary pancreatic anatomical referencetool as a tailor-made medical and surgical simulation and navigation, and contribute tomedical safety/accuracy, less-invasiveness and improvement of the medical education forstudents and trainees. Conclusion The bio-texture modeling by multimaterial 3D printingsystem combines the advantages of conventional 3D modeling, precise virtual 3D planning,and the possibility of transforming the acquired information into a medical profession.