Period Poverty in context of women on road: A study in New
Delhi
Sasmita Swain and Rituparna Dey
School of Rural Development,
Tata Institute of Social Sciences, Tuljapur – 413601,
Maharshtra
ABSTRACT
Present research article aims at examining the concept of
“Period Poverty” with special reference to women living on road and
proposing possible interventions for improving condition. A
qualitative research study was carried out in Delhi. In-depth
interview of various stakeholders i.e.; women on road,
gynaecologist, and NGO members were taken using semi structured
interview guides. The responses were transcribed verbatim. Field
notes of the group and individual interviews were also taken. The
data was analysed using the Rigorous and accelerated data Reduction
(RADaR) technique. The findings indicate women on road faces the
issues of privacy, lack of toilets and water, security, lack of
scientific knowledge, and adoption of unhygienic menstrual
materials. Based on the responses of various stake holders an
intervention model is suggested.
(Key words: Period poverty, menstruation, women on road,
menstrual hygiene, stigma)
Background
The incident of homelessness is one of the most unpleasant
outlines of urban poverty and social susceptibility, an obstructive
display of the failure of governance and the state’s pledge to a
welfare state. It is catastrophic and deplorable in a civilized
society and independent India that a huge percentage of our poor
are deprived and homeless. No one choose to become homeless it is a
forced situation. The census of India 2011 defines “houseless
household” as, “households who do not live in buildings or census
houses but live in the open on roadside, pavements, in Hume pipes,
under flyovers & staircases, or in the open in places of
worship, mandaps, railway platforms, etc.”
Increased harsh socio-economic conditions have resulted in a
large increase in the rates of street homelessness in the large
cities of India. As per the Census of 2011, India hosts more than
1.7 million homeless people, of which 938,384 are residing in urban
areas. However the accuracy of these figures is questioned by civil
society organizations. As per their estimation at least one per
cent of the urban population of India is homeless. If we assume
this claim to be true, at least 3 million people of the urban India
are homeless. Civil society estimates at any given point of time
the number of homeless in the capital city of Delhi alone, stands
around 150,000- 200000 of which at least 10,000 are women (Source:
Housing and land rights network).
When the incidents of homelessness infringe the most primary
human rights for all populace, women who live on the streets
undergo the most brutal forms of violence and abuse. Women living
on road are not only prone to various kinds of physical and
psychological abuse but also forced to live a much undignified
life. The resource scarcity limits them from having healthy food,
hygienic living condition, safe drinking water, privacy, safety and
security. Owing to their biological difference they face even more
difficulty; one such biological process which every woman
experiences is menstruation. Menstruation, even though a natural
biological process, is socially coloured by the patriarchal society
in different ways. It is associated with stigma, taboos,
prejudices, stereotypes and even in some cases discrimination.
Every women experience a different psychophysical state during this
period, but for women living on road lack of private space; lack of
toilet facility and water; lack of money to purchase menstrual
hygiene products makes this monthly occurrence even more
difficult.
Studies undertaken across different settings in India examining
the usage of menstrual hygiene products and health awareness
related to menstruation highlights two strong trends. First,
compared to urban area both the usage of menstrual hygiene products
and health awareness is much lower in rural areas of India. Among
the studied population in urban areas the usage of sanitary pads
has been reported to include between 50 and 90 percent
(Bharathalakshmi et al., 2014; Thakre et al., 2011) which drops to
0 to 65 percent in rural areas (Kamath et al., 2013; Shah et al.,
2013). Second, sanitary pads usage rate in urban slums is much
lower than the average urban usage rates roughly equates to the
usage rate of rural areas. In Delhi slums and resettlement colonies
it is 2.9 to 28 percent (Baridalyne & Reddaiah, 2004; Garg et
al., 2001). These trends reflect the extreme inequality amongst
different population with regard to menstrual hygiene management
(MHM) and emphasises the dire need of having health, hygiene and
sanitation programmes for the rural and urban poor. These study
findings primarily suggest that any intervention plan aiming to
improve MHM in India, has to give priority to rural areas and urban
slums.
METHOD
The study design used narrative inquiry. Narrative inquiry is a
qualitative methodology which focuses on studying and understanding
the individuals experiences (Creswell, 2007; Firkins, Twist,
Solomons, & Keville, 2019; Rance, Gray, & Hopwood, 2017).
In-depth interviews were used to “gather, analyses and interpret
stories people tell about their lives” (Marshall & Rossman,
2011, p.151).
Study Setting
Present study was carried out in New Delhi, an urban district of
National Capital of India, Delhi. The areas of New Delhi chosen for
the study were Sadarjung, IIT Gate; Ber Sarai, Sadar Bazar,
Pahargunj, Cannught place; New Delhi Railway station & Sarojini
Nagar.
Sampling & Recruitment
For the study two categories of participants were selected i.e.;
medical doctors and woman living on road. For selecting the
research participants a purposive sampling method was used.
Purposive sampling is used to identify and select information
related to the event of interest (Creswell 2007; Palinkas et al.,
2015). Women who are living and dependent on road for earning their
livelihood were selected. Pre menarche and post menopause women are
excluded from the study. The medical practitioners who have
specialized knowledge in gynaecology and have a minimum experience
of 7 years medical practice were selected.
Table 1. Participants’ Characteristics (n= 30)
Women on road
Medical doctor
n1=30
n2=5
Marital status
Occupation
Sex
Specialization
Married=24
Unmarried=6
Begging=22
Balloon seller=4
Others=4
Male=01
Female=04
Gynaecologist=5
Age(in years)
<15
15-24
25-34
35-44
45-54
n (%)
3 (10)
6 (20)
10 (33.33)
7 (23.33)
4 (13.33)
Year of practice
<10
10-20
21-30
n (%)
1 (20%)
2 (40%)
2 (40%)
Total=(n1+n2)=30+5=35
Participants
The study includes total 35 respondents, of which 30 were women
living on road and 5 are medical doctors. Women living on road were
interviewed to understand the issues they face during menstruation;
the way they manage with it; and the expectation they have from
Government. Five respondents were medical doctors, whose interviews
were taken to understand the short term and long term heath effects
of unhygienic menstrual practices. Detail Demographic
characteristics of participants are provided in Table 1.
Data Collection
As the study was related to a not much discussed topic, women
were very hesitant to talk about it. The interviews were taken with
consent of the participants in their place, according to their
availability. Though the interview took place over seven weeks
period, initial rapport building phase only took nearly three weeks
time. In a day 1 to 3 interviews were done depending on the
availability of respondents, with a mean length of 112 minutes.
Data was collected using in depth interview method. In addition to
the verbatim, audio recordings were taken with the prior permission
of the respondents. The researcher conducted the interviews in the
local language so as to keep the true essence of the experiences
expressed by the respondents. Then transcriptions were made and
translated by the researcher. To make it more accurate comparisons
between the transcriptions and the field notes of the researchers’
were also made.
Data Analysis
Data were analyzed using “rigorous and accelerated data
reduction” (RADaR) technique. The RADaR technique is an approach to
coding and analyzing qualitative data (Fernald & Duclos, 2005;
Guest & MacQueen, 2008; Watkins, 2012; Watkins &Gioia,
2015). The data was analysed in four steps. First all the data
collected from in-depth interview were transcribed and formatted in
a uniform format. Next the uniformly formatted transcripts are
placed into an all-inclusive data table created in Microsoft Excel
which includes transcript number, question, participant’s response,
key words, code, notes and theme. Next the data from the all
inclusive data table, the data not directly related to research
question was reduced and from more open codes focused codes derived
and then they are clubbed into concepts and then themes. The
intervention strategies were developed based on the final phase
data table.
Homelessness and period poverty
Period poverty refers to the inability to afford sanitary
products; lack of access to sanitation facility and water; and lack
of proper knowledge and adequate awareness about menstruation. The
concept of period poverty emerged in UK after researching on the
conditions that teenage girls and woman go through during their
periods on road. According to a recent research of Children Charity
Plan International UK, almost one in ten girls in UK aged between
14-21 were not able to afford rather buy any of the period products
because of their financial constrain. One of the causes of period
poverty might be poverty in its broad terms but other reasons may
include the social and cultural dynamics of the society that
results into inaccessibility of the period products. According to
the UN reports globally 1.2 billion women do not have access to the
basic hygiene and sanitation. The report also highlights that in
South Asia most of the schools fell short of the WHO standards of
one toilet for every 25 girls. Though menstrual hygiene is
recognised by UN as a global public health and human right issue,
still 1.2 billion women lack access to basic sanitation and hygiene
all over the globe (The Hindu, May28, 2018).
As per the report of International Federation of Gynaecology and
Obstetrics (FIGO) titled “Month after month: period Poverty” each
month nearly 500 million girls and women are living in period
poverty. The cost of purchasing sanitary napkin every month is a
major constraint for many women across both high and low resource
setting. An estimated one in ten young women has been unable to
afford protection for their period all over the globe, nearly 12
percent have been forced to manage with ineffective, unhygienic and
unsafe devices (FIGO, 22.02.2019).
1. Unhygienic menstrual practices
Women living in underserved areas menstruation can become the
most trepidation time of the month. Because of lack of
accessibility to sanitary products due to the financial constraint
women can end up adopting unhygienic means to absorb menstrual flow
which may leads to infectious and life threatening diseases. A
study conducted in urban resettlement colon of Delhi reported that
86 per cent of women are not psychologically prepared for
menstruation. 60 per cent women use home-made absorbents made from
dirty cloth and three-fourth of them are unaware of the health
consequences of using dirty cloth (Baridalyne & Reddaiah,
2004). The condition of menstruation is almost alike in most
countries where women use twigs or leaves or cut out mattresses,
papers, mud, used bandages, unclean cloths collected from dustbins
to use as pads for soaking blood.
“My mother gave two clothes so I used to rewash it and use it,
but sometimes during the rainy seasons or winters when the clothes
would not dry I used to use the same clothes with “Leaves” to soak
the blood flow. Still it was very difficult and at times, I would
even have bloodstains on my clothes.” “Ek baar hum subha uthkar
dekhe ki hamari poore kaprde me khoon laga hai aur jahan hum sote
the wahan bhi khoon laga hua tha”
Women who are living on nearer to hospital areas reported using
bandages as it is easily available to them. But this practice
involves a huge health risk as in many cases these bandages may be
contaminated.
“I used to use cloth and still use cloth and now to soak more
blood I even use torn and thrown away bandages as well.”
She collects the thrown bandages from the hospital dustbins and
uses it during her menstruation. Inability to purchase safe and
hygienic menstrual products forces females living on road to adopt
such unhygienic and life threatening means to deal with menstrual
blood. Women living in tents with no doors, just a curtain which
separates the outer world from the inner, poorly lit and unclean
with lack of access to water end up being in a pool of health
issues that could have been avoided if hygienic conditions were
being maintained.
It is not that all women living on road are ignorant about the
health hazards of such unhygienic practices but they are unable to
overcome the environmental and financial constraints and feel
helpless. Staying in a place on road which itself is not hygienic,
and having no access to basic minimum of life like water, private
place, money it is very hard to maintain hygiene during
menstruation.
“It’s very difficult to maintain cleanliness around but whatever
little I can, like washing everyday when water is available I do,
apart from this extra I can’t afford to do. I use public toilets
and hospital toilets to change and wash myself. “
2. Menstrual Hygiene and health
Menstruation is a normal biological procedure, which an
adolescence girl and women passes through during their life.
According to medical science during this period a women need to
keep her private parts clean and change the menstrual products
(cloth, pad, tampon etc) at regular interval. Medical doctors
opines that during this time it is essential to maintaining
cleanliness and use hygienic menstrual observant for preventing any
infection.
“Amid monthly cycles it is critical to deal with the individual
cleanliness, measures like Hand washing when heading off to the
toilet is a daily schedule however it ought to likewise be entirely
pursued to diminish the chances of disease beside The sanitary pad
ought to be changed every now and again, not over 6 hours one
single pad ought to be utilized and it is constantly desirable to
use sanitary pads which are accessible in the market. In any case,
on the off chance that it isn't workable for a lady to obtain them
for individual reasons, he can at any rate pick a clean cloth. The
fabric ought to be appropriately washed and dried before it is
utilized for this reason.”
Inadequate menstrual hygiene can have potential health
consequences like increased risk of reproductive and urinary tract
infections (Howard et al., 2016; Das et al., 2015; Anand et al.,
2015). Unhygienic practice during menstruation can adversely affect
women health in some cases lead to life threatening health hazards
if not addressed on time. Poor menstrual hygiene can cause from
mild uneasiness to vaginal diseases.
“Awful smell is a typical after effect of unhygienic menstrual
propensities. Change your pad three to four times each day. Indeed,
even gathered body secretions can cause uneasiness. An unreasonably
clammy pad can harbour microorganisms and cause contamination.
This, thus, can cause urinary tract and vaginal diseases. It's an
extremely basic issue and pretty much every other ladies have
encountered it a few or the other time. The fundamental explanation
behind the rashes shaped amid your periods is not changing your
sanitary napkins every now and again enough. The modern edge
napkins utilize a decent measure of plastic and other material not
all around inviting to your skin. Additionally, utilizing a napkin
for more than 46 hrs can make the blood cause contamination in its
environment, causing skin rashes and aggravation.”
In practice, young girls and women in India and across the globe
who are staying on road it is a luxurious dream, as they lack the
required resources; knowledge, money, private place, medicine, and
clean water.
When asked to the respondents whether they face any health
problems they only told about the inconvenience, discomfort, rashes
near the private place, itching, sometimes burning issues. Most of
them are not aware of any long term consequences of unhygienic
practices.
“I get rashes using clothes and papers, I want free pads”
3. Menstruation a reason of early Marriage
Menstruation in many communities is perceived as a symbol of
“Womanhood” presuming that the girl is now ready to get married and
bare a child. However, in practical terms girls do not become
physically or emotionally ready to take up challenges like marriage
and motherhood until adulthood. As per a report released by United
Nations Population Fund (UNFPA) in 2013, nearly 7.3 million girls
give birth to child before attaining 18 years of age. Teen
pregnancy (pregnancy before 20 year) leads to childbirth
complications, high risk of postpartum depression, denied of right
to education and health, affects their income-earning potentials
and is locked into a poverty syndrome (Ghose, & John, 2017).
Studies have shown that parents often fear that schools can turn
into hostile environments for their daughters after they attend
their puberty. They can be subjected to sexual violence or
harassment by their peers or teachers or the school staff or the
bystanders on the road and hence, they need to be married just
after the puberty. However, this can differ across several ethnic
groups having their own rules and perception regarding Menstruation
and Early Marriage. However, mostly in rural India people do
associate Menstruation with marriage so that girls remain inside
the boundaries and shackles of Patriarchy and are out of the reach
from the outside world. Marriage brings lots of responsibilities
and restrictions for women so if it happens very early when a
person is not mentally and physically prepared, it is not a very
pleasant experience. When preparedness for marriage is based on
occurrence of menstruation rather than on personal choice and
mental preparedness it becomes a burden and perceived as a negative
event of life. Menstruation is considered as the attainment of
womanhood in many cultures and girls are married off once they
attain their menarche, this develops a negative attitude among
women towards menstruation. Most of the respondents held
menstruation as a cause for their plight situation as many of them
migrated after marriage from village to the cities and landed on
roads:
“I didn’t like menstruation because I was married off that very
year and I didn’t expect that coming my way. I knew I would be
married but not so early. So this is the only reason I don’t like
my periods. After I got married I had to work so hard cooking,
washing, taking care of my in laws, children and the extended
family members. And after we moved from Begusarai my village in
Bihar to Delhi the city life has made it worse”
The association of menstruation with restrictions, ritualistic
practices, religion, womanhood and marriage makes a simple
biological process into a complex socio cultural phenomenon.
4. Menstruation and the pressure to keep silence
Medically menstruation is defined as the process of discharging
(through the vagina) blood and other materials from the lining of
the uterus at about four week interval from puberty until
menopause. This lasts for 3-5 days. Menstrual blood is just like
another type of human excretes which flows out every month. But in
almost all cultures the menstrual blood is stigmatized as impure
and dirty. Not only the women body which housed this biological
event is stigmatized but also the women as an individual is
stigmatized during this monthly occurrence and is treated in a
discriminatory and undignified way:
“mujhe esa lagta hai ki logo ko mujhe aur bura bhals bolne ka
mauka mil jata hai jab unko galti se ye pata chalata hai ki mujhe
mahina ho raha he”
“Sometimes I do feel disrespectful when people come to know I am
menstruating they do have a different discriminating gaze, as if I
have done some murder or something”
Woman feels lot of pressure to keep it as a secret so that
others cannot notice that she is on her period. The stigma attached
to this makes it not to be discussed open, and arrested in the arm
of a dark silence.
The clutch of stigma surrounding menstruation is so strong that
even women living on road with all forms of scarcity are not free
from it. Some respondents reported explicitly that they are not
subject to any stigma but when asked why, the answer their feeling
of stigmatized or not is dependent on bystander:
“I don’t know I have never experienced so can’t say, mostly
people don’t know when I am having periods. Jab unko pata hi nahi
hota tho kya hi bolenge”.
Even though she reported that she didn’t experience it directly,
her response does indicate that, such experience of her is
conditioned upon the bystanders ignorance about her menstruation
status at the given point of time. As hiding her periods does not
attract the bystanders gaze or comments, she feels that stigma is
being absent, the again stresses that menstruation should be kept
hidden.
5. Age old silence leading to inadequacy of knowledge
According to 2011 census estimates 10% of Indian population are
female adolescents aged 10-19 years which means roughly 120 million
are girls. A systematic review of Indian studies estimates that
most of the girls have inadequate knowledge at the time of
menarche. Barely half (48%) of adolescent girls in India are aware
of menarche before their first menstruation. (Eijk et al., 2016).
Nearly 71 percent of adolescent girls are unaware of menstruation
till menarche and 70 percent of mothers who have menstruating
daughters consider menstruation as dirty (A 2014 report by the NGO
‘Dasra’ titled Spot On!)
This inadequacy of knowledge results in a state of confusion,
fear and anxiety among adolescent girls on the attainment of
menarche. Mother, school teacher, health workers, other lady
relatives, friends and peers who pass on the information regarding
menstruation to adolescent girls, also sometimes don’t have
scientific knowledge regarding menstruation. In their mind the
construct “menstruation” is coloured with stigma and taboos, a
secret of girl’s life which is not supposed to be discussed openly.
Rather than a scientific understanding of menstruation; the
illogical rituals, socio-cultural taboos, shame, fear, anxiety and
narrow understanding of menstruation passes from one generation to
another. Most women have internalised the silence and without
questioning accept the illogical ritualistic prescription concerned
with menstruation. Over emphasis on menstruation as a sign of
attainment of womanhood somewhere underscores its psychophysical
and social impact on an adolescent’s life. In many cases the
physical discomfort and pain is seen as a normal part of
menstruation and girls indulge in self medication which later may
lead to health complications.
Menstruation that is almost made into a forbidden word by the
society has had a strong impact on the psyche of the girls as well.
Since for so long this ‘False Notion’ has been around that the
women have actually started believing that Menstruation is
something that should be talked about in hushed tones. A woman’s
first period can be quite confusing and scary because of the deep
rooted taboos attached culminating her normal biological cycle into
a harrowing process. Mothers are mostly expected to talk about
menstruation with their daughter but the menstrual taboos are so
deep seated that even mother hesitate to ‘Break the Silence’ on
menstruation and let their daughters know all about it at the time
of menarche. Here the researcher would like to quote one of the
respondents who went through a similar experience since she did not
have any idea regarding Menstruation.
“I had no idea about periods so I was dead scared, for the first
day I did not tell anyone out of the fear that I am going to die.
Next day when my mother noticed my blood stained salwar she then
got to know and I told her everything.”
Dr. Rani Bang, in her book “Putting Women First: Women and
Health in Rural Community” quoted that in the rural communities of
India women have very little or most of the time no knowledge about
menstruation. This situation occurs because they have no one to
educate or counsel them regarding this biological process of their
body. Mothers in rural India refrain from going into this
discussion since they are ashamed of the fact that they menstruate
and consider themselves impure according to the male dominated
society. Therefore, to break such patriarchal taboos one need to
look beyond and break the glass ceiling that prevents individuals
to have an opinion of their own. Association of period or
menstruation with religion or culture has given rise to the
societal taboos around it and which are so strong in itself that
even women most of the time abide by it saying it is necessary for
the well being of the society. Women are therefore, made to believe
this illogical patriarchal concept where they would demean
themselves upholding the rituals beyond everything. In the society
these discriminatory practices are normalised in the name of
culture and tradition. Women themselves also has internalized these
things and incorporated in their life without questioning.
“Nothing more just a little Puja ceremony was done in the house
and I was separated from everyone for 14 days. Although my periods
got over within eight days but I was not allowed to enter the
house, it was only after 14 days that I was allowed to enter. This
continued for one year until I got married, after marriage, I used
to move out myself when periods hit.”
“Nothing as such, just there were few restrictions like I was
not allowed to touch the pickle or meethai or I was not allowed to
enter the temple or ‘Tulsi mandap’. All these rituals I think are
very necessary and important.”
This internalization process inhibits adolescents to discuss
about the health, hygiene, and psychological issues concerning it,
because of this they even hesitate to ask for sanitary products to
the parents, which later compromises their health and feeling of
psychological comfort.
6. Notion of “impurity” root for discrimination
Menstrual discrimination has always been there since ages where
in women are discriminated upon because of their biological process
necessary for the creation of the future generation. Being referred
to as “that time of the month” or “the curse” these euphuisms
clearly up holds the fact that Menstruations has always been looked
down upon and portrayed as a “Dirty Secret” of a woman’s life. In
many cultures women are separated from their family during the few
days of menstruation where in they are meant to sleep outside their
house or in huts which is far from their house. This kind of
discriminatory behaviour has been going on for ages in the name of
Culture and Religion, where in women are not only forbidden to
enter the house but also forbidden to enter public places like the
temple. Research studies also reveal poor sanitation facility in
schools and non-accessibility to quality sanitary products can be
associated with lower enrolment in schools, absenteeism, and
dropout. A report titled Spot On! Published by the NGO ‘Dasra’ in
the year 1014 reports that every year nearly 23 million girls
dropout of school due to lack of proper menstrual hygiene
management facilities such as, availability of sanitary napkins and
logical awareness of menstruation. Such situation can
systematically exclude girls and women from availing the life
changing opportunities like education. Ultimately, without adequate
support or MHM, the health, wellbeing and safety of women and girls
are threatened.
All women residing on the road are not born on road many of them
are migrated from rural areas to the metropolitan city. Some women
interviewed, shared their experience regarding the discrimination
they faced in their home.
As one respondent said:
“I was asked not to touch the temple or even come in front of
the temple; I was not allowed to touch any of my family members. I
was told that I was “DIRTY” and hence, after I get clean I can come
back to a normal life. I was also not allowed to touch the flowers
because they said if I touch the flowers it would not blossom and
would die”
Answering to the question do you practice these rituals now? She
reported
“Now there is no house, no basic facility is there, so I don’t
practice these things”.
Another respondent said:
“I was asked to not touch the Quran and not offer ‘Namaz’ during
those days, when I attained periods during Ramadan time I was told
by my mother to stop fasting and to complete those remaining fast
on some other days when I am not menstruating.”
“I was asked to not enter the kitchen or the temple, I was also
asked to wash my own things. Rituals as such were not performed,
only a little puja was done by my mother. I was also asked to stay
outside of the house until the period gets over, I personally did
not like this because rest of my family was inside only I was the
one who was outside and I was also not allowed to talk to
someone.”
It indicates how discrimination creeps in right from the
beginning when a girl attains her puberty and it continues on for
the rest of her life.
One of the respondents who were the member of the NGO shared her
experience about how isolated she felt during her monthly menstrual
cycle.
“Experiencing childhood in a home where I wasn't permitted to
contact anything aside from the bed sheet on my bed and the
utensils in which I ate amid my menstrual cycle. On the third day
of my menstrual cycle my mom would demand that I bathe, in the wake
of guaranteeing that my bed sheet and my utensils are washed or
given in laundry separately. Since I would revolt in most
occasions, she would wash them herself and afterward clean up. The
tenets on washing up – 'the ritual bath' were additionally set
down...”
The Voices
Most of the women shared their desire to have sanitary napkins
during menstruation so that the blood gets soaked without getting
spilled on the cloth and also they can feel clean and comfortable;
and move around without any fear and anxiety. The second most
important need that should be addressed by the government or the
NGOS’s working for women according to the respondents is to ensure
safe places where in a menstruating woman can go and change her pad
and wash herself, get properly cleaned up so that she could remain
hygienic during this time. The third need of women on road is to
get free medicine for menstrual cramps and other menstrual related
diseases so they can carry out their daily activities, without any
hassle. As one of the respondent expressed her wishes
“No water; no pads; no medicines; no privacy are the
difficulties that I face. I wish to have a safe place to clean
myself; and get medicines and Pads for free”
Most of the women participated in the study expressed that their
voices need to be heard by the concerned authorities; (Government,
NGOs, low cost pad making private organizations) and positively
addressed. This will enable them in managing their menstruation in
a dignified way even in the general poverty condition they are
into.
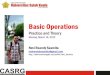
(Multi stakeholder Model(Period Poverty))
(Maintenance of the Facilities)
(Pad Vending Machine ) (NGO) (Stakeholders) (Awareness)
(Funding) (Adoption of the Localities) (CSR Organization)
(Community Organization ) (Awareness) (Networks) (Monitoring and
Evaluation) (Free Woman Health Camps) (Public Toilet ) (Government
(Ministry of Health and Family Welfare)) (Adoption of the Ideas)
(Dissemination of Information) (Participation ) (Text) (Women on
the Road)
(Bridging the Gaps)
(Free Woman Health Camps)
Source: Primary data
Multi Stakeholder Model
The proposed Multi stakeholder Model would work towards
eliminating the issue of period poverty faced by women who live on
road in the streets of New Delhi. The model will begin by
construction of toilets for women with the help of government and
CSR funding. These funds would be allocated not only for
construction of toilets for women but also for purchasing the
sanitary and toiletry products that would be kept inside the
toilets for the women to use. The toilets have to be constructed in
areas where the concentration of women living on the streets is
higher so that they avail the benefits. For this the NGO’s and the
government can conduct a survey and find out the concentration in
each area of New Delhi and then decide accordingly where to
construct the toilets. For this Geographical Information System
(GIS) software can be used. For the first year the toilets would be
accessible to all women irrespective of any category but after
completion of one year the use of toilets have to be restricted
only to women who live on road. For enabling them to use the
toilets a “Smart Card” has to be issued to women who live on road
after carrying out a detail need assessment. Inserting the smart
cards in machines they can easily get their sanitary products which
other women can’t.
NGOs can help in carrying out awareness programmes regarding the
toilets and they have to try to de-stigmatize menstruation as a
whole by organizing speeches from different NGO’s working on
menstruation. The trainers providing awareness has to be
periodically trained in capacity building so that they can carry
out their duty in an efficient manner. The Government also has to
arrange health camps and free health checkups along with free
medicine and this work can be jointly done with the CSR as well.
Therefore, Multi stakeholder Model would be based on Public Private
Partnership, where in the government, Civil society and CSR will
together for solving the issues of the women on road and letting
them to live a life of dignity.
Roles and responsibility of different stakeholders as proposed
in the model:
1) The Ministry of Health and Family Welfare (MoHFW):
· Work as the nodal agency.
· Construct toilets.
· Install pad vending machines in those toilets.
· Regular maintenance of those machines and the toilets.
· Conducting free checkups for the women on road and provide
medicines.
· Monitor and evaluate the results of the services after the
first year.
2) Women on road:
· Understand the concept and avail the services.
· Accept the concept and fully participate in the movement.
· Won the system and services provided.
· Disseminate the information.
3) Corporate Social Responsibility:
· Adopting the localities in which they work and constructing
toilets in their own locality.
· Arranging free health checkups.
· Providing funds for free sanitary and toiletry products.
· Creating awareness.
4) Non Government Organization (NGO):
· The NGO’s will begin by analyzing the gaps and thereby
bridging the same.
· The NGO’s will also be involved in community organization and
mobilization.
· Free health camps and awareness programmes will also be
carried out by the NGOs.
· NGO’s will also help in networking with other agencies.
Conclusion
Every human being has a right to live with dignity irrespective
of their sex and place of living. When a woman is feeling unsafe,
uncomfortable, restricted, helpless, disrespectful, discriminated,
blamed, ridiculed only because her body looks and behaves in a
different way than it is a high time to ask ourselves the question,
are we civilized?. It is high time to break the vicious cycle of
ignorance, overcome the environmental constraints and create an
enabling condition where women can lead a healthy life. Creation of
enabling environment requires efforts and involvement of all
stakeholders i.e.; women, family, community, civil society,
corporate and Government. Women living on road in big cities depend
on public facilities like toilets, water, footpaths, and shelter
homes for urban homeless for their sustenance. So it is the
responsibility of Government to create such facilities. Women
living on road in general and women in particular are exposed to a
variety of unhygienic condition and various forms of abuse. Though
they live under a highly vulnerable situation with potential health
risks, their ability to mitigate such risks and deal with it is
almost negligence. So it is very essential to organise free health
camps and avail free medicines for the homeless people.
References
1. Anand, E., Singh, J., Unisa, S.(2015). Menstrual hygiene
practices and its association with reproductive tract infections
and abnormal vaginal discharge among women in India. Sexual &
Reproductive HealthCare, 6, 249-254. doi:10.1016/j.
srhc.2015.06.001
2. Creswell, J. W. (2007). Qualitative inquiry and research
design: Choosing among five approaches (3rd ed.). Los Angeles:
SAGE.
3. Firkins, A., Twist, J., Solomons, W., & Keville, S.
(2019).Cutting ties with Pro-Ana: Anarrative inquiry concerning the
experiences of Pro-Ana disengagement from six former site users.
Qualitative Health Research, 29, 1461-1473.
Doi:10.1177/1049732319830425.
4. Fernald, D. H., & Duclos, C. W. (2005). Enhance your
team-based qualitative research. Annals of Family Medicine, 3,
360–364.
5. Ghose, S. & John, L. B. (2017). Adolescent pregnancy: an
overview. International Journal of Reproduction, Contraception,
Obstetrics and Gynaecology, 6(10),
4197-4203.doi:http://dx.doi.org/10.18203/2320-1770.ijrcog2017-4203
6. Guest, G., & MacQueen, K. M. (2008). Handbook for
team-based qualitative research. Walnut Creek, CA: AltaMira
Press
7. Watkins, D. C. (2012). Qualitative research: The importance
of conducting research that doesn’t ‘count’. Health Promotion
Practice, 13, 153–158.
8. Watkins, D. C., & Gioia, D. (2015). Mixed methods
research. Pocket Guides to Social Work Research Methods Series. New
York, NY: Oxford University Press
9. Office of the Registrar General & Census Commissioner
India, Ministry of Home Affairs, Government of India. Census in
India. 2017. Available: http://censusindia.gov.in.
10. Van Eijk, A .M., Sivakami, M.,, Thakkar, M.B., Bauman, A.,
Laserson, K.F., Coates S., Phillips,P.A.(2016). Menstrual hygiene
management among adolescent girls in India: a systematic review and
meta-analysis. BMJ Open. 2016;6:e010290. doi:
10.1136/bmjopen-2015-010290. [PMC free article] [PubMed]
[CrossRef] [Google Scholar]
11. Garg, S., Sharma, N., & Sahay, R. (2001). Socio-Cultural
Aspects of Menstruation in an Urban Slum in Delhi, India.
Reproductive Health Matters, 9(17), 16-25.
12. Barathalakshmi J, Govindarajan P, Ethirajan N, John William
Felix A. 2014. Knowledge and Practice of Menstrual Hygiene among
School Going Adolescent Girls. National Journal of Research in
Community Medecine 3(2): 138–142.
13. Baridalyne N, Reddaiah V. 2004. Menstruation Knowledge,
Beliefs and Practices of Women in the Reproductive age Group
Residing in an Urban Resettlement Colony of Delhi. Health and
Population; Perspectives and Issues 27(1): 9–16.
14. Kamath R, Ghosh D, Lena A, Chandrasekaran V. 2013. A Study
on Knowledge and Practices Regarding Menstrual Hygiene Among Rural
and Urban Adolescent Girls in Udupi Taluk, Manipal, India. Global
Journal of Medicine and Public Health 4(2): 1–9
15. Shah S, Nair R, Shah P, Modi D, Desai S, Desai L. 2013.
Improving Quality of Life with new Menstrual Hygiene Practices
Among Adolescent Tribal Girls in Rural Gujarat, India. Reproductive
Health Matters 21(41): 205–213.
16. Thakre S, Thakre S, Reddy M, Rathi N, Pathak K, Ughade S.
2011. Menstrual Hygiene: Knowledge and Practice Among Adolescent
School Girls of Saoner, Nagpur District. Journal of Clinical and
Diagnostic Research 5(5): 1027–1033.
17. SUPRIYA GARIKIPATI1* and CAMILLE BOUDOT2 TO PAD OR NOT TO
PAD: TOWARDS BETTER SANITARY CARE FOR WOMEN IN INDIAN SLUMS Journal
of International Development J. Int. Dev. 29, 32–51 (2017)
Published online in Wiley Online Library (wileyonlinelibrary.com)
DOI: 10.1002/jid.3266
18. Phillips-Howard PA, Nyothach E, Ter Kuile FO, Omoto J,
Wang D, Zeh C, et al. Menstrual cups and sanitary pads to reduce
school attrition, and sexually transmitted and reproductive tract
infections: a cluster randomised controlled feasibility study in
rural Western Kenya. BMJ Open. 2016;6:e013229. doi:
10.1136/bmjopen-2016-013229. [PMC free article] [PubMed]
[CrossRef] [Google Scholar]
19. Das P, Baker KK, Dutta A, Swain T, Sahoo S, Das BS, et al.
Menstrual hygiene practices, WASH access and the risk of urogenital
infection in women from Odisha, India. PLoS
One. 2015;10:e0130777. doi:
10.1371/journal.pone.0130777. [PMC free article] [PubMed]
[CrossRef] [Google Scholar]
20. “Menstrual hygiene practices, WASH Access and the risk of
urogenital infection in women from Odisha. Inida. Padma Das, Kelly
K. Baker, Ambarish Dutta, Tapoja Swain, Sunita Sahoo, Bhabani
Sankar Das, Bijay Panda, Arati Nayak, Mary Bara, Bibiana Bilung,
Pravas Ranjan Mishra, Pinaki Panigrahi, Sandy Cairncross, Belen
Torondel
PLoS One. 2015; 10(6): e0130777. Published online
2015 Jun 30. doi: 10.1371/journal.pone.0130777
21. Adolescent pregnancy: an overview Seetesh Ghose*, Lopamudra
B. John International Journal of Reproduction, Contraception,
Obstetrics and Gynecology Ghose S et al. Int J Reprod Contracept
Obstet Gynecol. 2017 Oct;6(10):4197-4203 www.ijrcog.org DOI:
http://dx.doi.org/10.18203/2320-1770.ijrcog20174393
22. Marshall, C., & Rossman, G. B. (2011). Designing
Qualitative Research (5th ed.). Thousand Oaks, CA: Sage
Publications.
23. Palinkas, L.A., Horwitz,S.M., Green,C.A., Wisdom, J.P.,Duan,
N.,& Hoagwood, K. (2015). Purposeful sampling for qualitative
data collection and analysis in mixed method implementation
research. Administration and Policy in Mental Health, 42, 533-544.
Doi:10.1007/s10488-013-0528-y
24. Health and Population Perspectives and Issues 27 (1): 9-16,
2004 MENSTRUATION: KNOWLEDGE, BELIEFS AND PRACTICES OF WOMEN IN THE
REPRODUCTIVE AGE GROUP RESIDING IN AN URBAN RESETTLEMENT COLONY OF
DELHI N. Baridalyne & V.P. Reddaiah
25. Daphne C. Watkins, (2017). “Rapid and rigorous Qualitative
Data Analysis: The “RADaR” Technique for Applied Research”.
International Journal of Qualitative Methods Volume 16: 1-9
(sagepub.com/journalsPermissions.nav DOI:
10.1177/1609406917712131
26. Land Right network, New Delhi
(https://www.hlrn.org.in/homelessness)
27. Pacha.A.(2018)Is India suffering from ‘period poverty’?.The
Hindu
(https://www.thehindu.com/sci-tech/health/is-india-suffering-from-period-poverty/article24011206.ece
28. International Federation of Gynaecology and Obstetrics
(2019) “Month after month: Period Poverty
29. The state of world population 2013, United Nations
Population Fund