Embed Size (px)
Citation preview

undergo motility and pH testing; (3) Pts found to have EoE would be treated with fluticasone.Allergy testing or immunotherapy treatments were not included; (4) For pts undergoingendoscopy (EGD) w/o Bx, EoE would be missed. Results: Assuming base case probabilities(Table 1), the EGD w/o Bx arm cost $643 and was associated with 0.953 QALYs. The EGDwith Bx arm cost $853 and was associated with 0.957 QALYs. The resulting incrementalcost-effectiveness ratio (ICER) was $52,500 per QALY for the EGD with Bx arm. Tornedoanalysis demonstrated that the results were sensitive to the following variables in descendingorder of influence: cost of EGD with Bx, cost of EGD w/o Bx, probability of EoE in pts withand w/o dysphagia, and symptom resolution on fluticasone. In one-way sensitivity analysis,the ICER exceeded $100K when the probability of EoE in pts w/o dysphagia was 3% orless, or if symptom resolution on fluticasone was 67% or less. The ICER for the EGD withBx arm exceeded $100K when the cost > $700. Conclusions: Upper endoscopy with Bx forEoE appears to be a cost-effective approach when the probability of EoE in pts with refractoryGERD exceeds 3%.Table 1. Model Probabilities
S1090
Celiac Sprue and Eosinophilic Esophagitis: Are Duodenal Biopsies Enough?Jessica B. Johnson, Kathryn R. Byrne, Kathleen K. Boynton, Douglas G. Adler, KathrynPeterson
Background: Recent pediatric studies postulate an association between celiac sprue andeosinophilic esophagitis (EoE), suggesting an increased prevalence of celiac disease in childrenwith EoE. No data have been published regarding the prevalence, detection or impact ofceliac disease in adults with EoE. Aims: To estimate the prevalence of gluten sensitivity inadults with EoE. To determine the diagnostic yield of small bowel biopsies in identifyinggluten sensitivity in EoE patients. To determine whether the addition of celiac serologytesting to small bowel biopsy increases detection of gluten sensitivity in EOE patients. Toreport on the relationship between treatment of gluten sensitivity with dietary avoidanceand resolution of symptoms and pathologic findings of EoE. Methods: A retrospective chartreview was done on all patients diagnosed with EoE from Jan to Oct, 2009. Data gatheredincluded sex, age, duodenal biopsy pathology, tissue transglutaminase IgA antibody (TTG)positivity, esophageal eosinophil counts, and EGD findings. Duodenal biopsy findings werecorrelated with TTG results. Gross and microscopic EGD changes with institution of gluten-free diet were recorded.Results: 29 EoE patients were identified who had both duodenalbiopsies (6 total biopsies) and TTG antibodies performed. The average age of patients was37.4 years (std 10.9), and 13/29 (45%) were female. Gluten sensitivity was identified in 4/29 (13.8%) patients either by biopsy or TTG. Interestingly, 3 of the 4 patients had evidenceof celiac on TTG testing alone (range of TTG 22-250,ref positive = 19) while demonstratingnormal duodenal biopsies, and 1 patient had Marsh 1 changes on a duodenal biopsy withnormal TTG antibody. IgE levels were not substantially different between possible celiacpatients and nonceliac EoE patients (138+/-198 and 248+/-458). 3 patients followed a gluten-free diet. Upon repeat testing of 2 patients, EoE symptoms and histologic findings hadresolved after adopting a gluten-free diet. A gluten-free diet also resulted in improvementin nonspecific abdominal symptoms in 3 patients. Conclusion: Similar to pediatric studies,our data suggest celiac sprue is commonly found in the adult population with EoE. Diagnosismay be challenging, as gluten intolerance may be present on TTG testing despite normalduodenal biopsies in EoE patients. Furthermore, this study suggests that gluten-free dietscan offer relief of abdominal and esophageal symptoms in patients with EoE. Consequently,TTG testing may further direct clinical care for patients with EoE and should be consideredin the setting of normal duodenal biopsies.
S1091
Clinical Presentation of 4905 Adults With Histopathologic Diagnosis ofEosinophilic EsophagitisRobert C. Kapel, Robert M. Genta
Background & Aims: Many studies have demonstrated the varied clinical presentations ofeosinophilic esophagitis (EoE) in both adults and children. The aim of this study was toexamine the presenting symptoms of EoE, by age and gender, in a large group of adultoutpatients meeting the histopathologic criteria for this diagnosis. Methods: We utilizedthe Caris Diagnostics Database of gastrointestinal biopsy specimens from community-basedoutpatient freestanding endoscopy centers in 42 states, DC, and PR. We analyzed thepathology reports for all esophageal biopsy specimens submitted to Caris Diagnostics fromJanuary 2007 through June 2009. We extracted demographic, clinical and endoscopic datafrom all unique patients, 18 years or older, who had an initial histopathologic diagnosis ofEoE “pattern of injury” (>20 eosinophils per high-power field). We excluded patients whopresented with a previous diagnosis of EoE, and those who had insufficient clinical data.Results: During the study period 179,685 patients had esophageal biopsies (median age56 years; 47.6% male); a histopathologic diagnosis of EoE was made in 5,522 patients(3.1%; median age 43; 65.2% male, OR 2.09 95%CI 1.97-2.21). Of the 4,905 patients whomet the inclusion criteria, 1,887 were aged 18 to 39 (67.4% male), 2,227 were 40 to 59(65.3%), and 791 were 60 or older (60.8%). The frequencies of GERD (41%, 40%, 40% -in groups of increasing age, respectively); chest pain (4%, 3%, 3%); and food impaction(1.2%, 0.7%, 0.5%) were similar across age groups. Dysphagia was less frequent in theoldest group (55%) than in the younger groups (59% and 61%; p<0.001). Dyspepsia/
S-177 AGA Abstracts
epigastric pain weremore frequent in the youngest patients (24% vs. 18% and 17%; p<0.001),as were nausea/vomiting (6.6% vs. 2.4% and 1.7%; p<0.001). Women had significantlygreater frequency of dyspepsia (23.4% vs. 14.4%;p<0.001), nausea/vomiting (5.7% vs. 2.9%;p<0.001), and chest pain (4.2% v 2.8%; p=0.013). Men had more frequent dysphagia (62.9%vs. 52.9%; p<0.001). GERD was equally frequent in men and women. Conclusions: Amongadult patients undergoing elective upper endoscopy, dysphagia and GERD were the mostcommon presenting symptoms resulting in the histopathologic diagnosis of EoE. Dysphagia,nausea and dyspepsia decreased with age. The rate of food impaction was low in this patientpopulation (non-emergency room setting) and its frequency was slightly higher in men.Conversely, dyspepsia, nausea and chest pain were more common presentations in women.Over 40% of adult patients presented without dysphagia. These observations may strengthenour recognition of the varied presentations of EoE in adults.
S1092
Food Allergen Restricted Diet in the Treatment of Paediatric EosinophilicEsophagitisRichard Muir, Peter Lewindon, Looi C. Ee, Geoffrey D. Withers
Introduction Treatment of Eosinophilic Oesophagitis (EO) in children remains challenging.Elemental diet is the gold standard but use is limited by palatability and long term compliance.Kagawalla's paper reported significant improvement on standard 6 food elimination diet in74% of patients (<10 eosinophils/HPF). Aims of the study were to assess the efficacy of 6food elimination diet for 6 weeks in children with EO and the role of allergy testing. MethodsEligibility criteria included children with either a new diagnosis of EO (>15 eos/HPF) orpreviously diagnosed and on stable treatment for the prior three months. Patients withhistological evidence of other gastrointestinal diseases (except GOR) were excluded. SkinPrick Testing (SPT) for food and inhalant allergens using standard extracts was undertakenand Atopy Patch Testing (APT) for egg, dairy, corn, soy, wheat, chicken and beef. Patientscommenced a diet excluding cow's milk protein, soy, egg, corn, wheat, seafood, peanutsand tree nuts for 6 weeks. At completion, repeat medical assessment including Endoscopywith biopsy was performed. Results 14 patients were enrolled and 13 patients completedthe study protocol at time of presentation. Mean age 9 (1-15 years); 11 males and 2 females.Incidence of other atopic disorders requiring treatment was 10/13 (76%) and coexistenttopical steroid therapy for EO was 4/13 (30%). On SPT, 7/13 (53%) had positive results(wheal >3mm) with all 7 demonstrating sensitivity to aeroallergens and 2/7 to food allergens.On APT, 10/13 (77%) had positive results, the most common soy (6), cow's milk, egg andcorn (5). At conclusion of diet 3/13 had complete histological remission, 2/13 significanthistological improvement (3-10 eos/HPF), 2 partial histological response (>50% reductioneos/HPF), 6 were non-responders. Mean eosinophil count dropped from 47.3 to 30 perHPF. All patients reported subjective improvement in symptoms Conclusion 53% of patientshad positive histological response rate (RR) to the exclusion diet, 38% showing eithersignificant histological response or entering remission. This histological RR was disappointingversus Kagawalla's RR 74%. Reasons for a lower RR in our study include possible reducedcompliance with prescribed diet and older study population. 53% study population displayedsensitivity to aeroallergens consistent with the observation of increasing aeroallergen sensitiv-ity with age. Conclusions from our allergen tests are difficult with small sample population,but there was no clear correlation between positive SPT, APT and response to diet.
S1093
Significant Esophageal Eosinophilia and Typical Endoscopic Features areHighly but Not Exclusively Specific for Eosinofilic EsophagitisJan Martinek, Alice Strosova, Katerina Kostalova, Tuckova Inna, Petr Hrabal, Filip Zavada,Stepan Suchanek, Magdalena Stefanova, Miroslav Zavoral
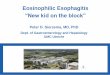
Background: Eosinophilic esophagitis (EE) is an emerging disease with typical clinical,endoscopic and histo-pathological features. However, some studies suggested that esophagealeosinofilia is not a specific finding for EE. Also endoscopic features of EE (rings, furrows)are considered non-specific. Aim: The aim of our study was to assess the prevalence ofesophageal eosiniophilia in a cohort of patients undergoing upper gastrointestinal endoscopy.Methods: A single center prospective study. All patients fulfilling inclusion criteria andagreeing with the participation in the study underwent an upper GI endoscopy includingbiopsies taken from distal (5 cm above the Z-line) and proximal esophagus. In patients withreflux esophagitis samples were also obtained from the Z-line. The presence and the countof of eosinophils were assessed by two experienced pathologists. Results: 2256 biopsies from332 patients were analyzed. Eosinophils in the esophageal mucosa were detected in 22(6.7%) patients. Considering both clinical and histopathological features, EE was diagnosedin 19 patients (5.7%). Among them, in 16 patients the number of eosinophils was higherthan 15/HPF and in 14 patients was higher than 20/HPF. In the remaining 3 patients withsuspected EE, the number of eosinophils was bellow 15/HPF. In two patients without EE(one with achalasia and one with Barrett esophagus), the number of eosinophils reachedhigh levels (20 and 72/HPF). Dysphagia or food impaction was present in 18 (95%) of thepatients with EE, atopy/allergy in 12 (63%) and typical reflux symptoms in 14 (73.7%).Thirteen patients with EE (68%) responded completely or partially to the acid suppressivetherapy. The frequency of esophageal eosinophilia in particular endoscopic findings is shownin the Table. Sensitivity, specificity, PPV and NPV of typical endoscopic features (rings,furrows) for diagnosing EE were 72.3%; 96.5%; 98.1% and 59.2%. Conclusions: Significantesophageal eosinophilia is a rare finding among patients with reflux esophagitis, Barrettesophagus or achalasia. On the other hand some patients with clear clinical and endoscopicfeatures of EE do not reach a required number of eosinophils/HPF. Endoscopic findings ofrings and/or furrows are moderately sensitive and highly specific for diagnosing of EE.Finally, our results suggest that gastroesophageal reflux plays a role in the development of EE.
AG
AA
bst
ract
s

AG
AA
bst
ract
s
* p< 0.001 vs. all remaining; ** p< 0.001 vs. all remaining
S1094
Limited Accuracy of Upper GI Studies in the Diagnosis of EosinophilicEsophagitis in AdultsNelson Moy, Frank H. Miller, Ikuo Hirano
INTRODUCTION: Endoscopy (EGD) has high sensitivity and specificity in the diagnosisof eosinophilic esophagitis (EoE). Prior case series in EoE have detected abnormalities onupper GI studies (UGI) but the sensitivity of these findings is unknown. AIM: Evaluate theaccuracy of UGI in the diagnosis of EoE and compare UGI findings with EGD features.METHODS: A single center adult EoE database identified patients (pts) with prior UGI.Initial UGI reports, EGD data and unblinded, re-evaluation of UGI images by a senior GIradiologist were compared. RESULTS: From 419 EoE pts, 59 (14%) pts with UGI wereanalyzed. EoE pts with UGI included 36 males with mean age of 40 years. UGI indicationsincluded: dysphagia (80%), known diagnosis of EoE (15%) and miscellaneous (abdominalpain and anemia;5%). Mean time between UGI and EGD was 56 days, excluding 13 ptswith > 1.5 years between studies. Initial UGI results were classified into 5 categories:normal (15%), findings characteristic of EoE (rings/furrows/exudates; 0%), findings possiblyconsistent with EoE (stricture/barium tablet retention; 36%), features consistent with GERD(28%), and miscellaneous (hiatal hernia/Schatzki ring/tertiary contractions; 20%). EGDdetected characteristic EoE abnormalities in 85% of pts. On re-evaluation of UGI studiesby a radiologist, the detection rate of EoE features improved; however the sensitivity forrings and furrows was lower than EGD (Figure, *p<0.05). UGI re-evaluation demonstrated:normal (4%), characteristics of EoE (41%), possibly consistent with EoE (13%), GERD(26%), and miscellaneous (15%). Strictures were detected by UGI in 47% compared with28% by EGD (NS). CONCLUSIONS: While commonly used as a diagnostic test for dys-phagia, UGI studies have limited sensitivity for the diagnosis of EoE in adults. Characteristicfeatures of rings and furrows are better detected on EGD than UGI. Radiologist's awarenessof EoE increases the diagnostic yield of UGI detection of EoE features.
S1095
Massive Upper GI Bleed Due to an Iliac Artery-Enteric FistulaChristopher P. Farrell, Robert J. Bailey, Eric Russell, Melissa Morgan, Gary Newman
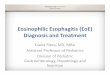
48 year old male with a history of renal transplants in ‘02 and '03 and a pancreatic transplantin '02 presented to the ER following an episode of syncope and melena. An EGD wasperformed on the 1st day and was completely normal. On the morning prior to having acolonoscopy, the patient became unresponsive and hypotensive. A bedside EGD was per-formed, showing a large amount of fresh blood and clot in the 2nd and 3rd portions of theduodenum. The active site of bleeding was unable to be identified and the patient was sentto interventional radiology (IR) on blood products and vasopressor support. Angiographyillustrated no evidence of active bleeding in the celiac artery, SMA, or IMA distributions.The patient produced an increasing amount of blood from his mouth, and also passed a2cm piece of tissue from his oral cavity. IR evaluated the patient's aortic arch and descendingaorta, with no extravasation of dye seen. A repeat EGD was performed in IR, once againshowing a large amount of fresh blood and clot extending to the 4th portion of the duodenum.The endoscope was x-rayed while in the duodenum and found to be much lower in thepelvis than normal. Repeat angiography was performed in the lower vasculature and dyeextravasation was isolated from the right iliac artery into the small bowel.(Fig 1) A stentwas placed which stopped the bleeding. The patient had required an immense amount ofblood products and unfortunately went into pulseless electrical activity following the repairand passed away. The tissue expelled from his mouth was consistent with a pseudoaneurysm,indicating an iliac artery-enteric fistula as the cause of the patient's profound GI bleed.
S-178AGA Abstracts
Figure 1
S1096
Glasgow Blatchford Score as an Effective Triage Tool for Identifying PatientsWith Severe Upper Gastrointestinal Bleeding With High Mortality RiskLee-Guan Lim, Khek Yu Ho, Huak Y. Chan, Pui Li Teoh, Christopher J. Khor, AndreaRajnakova, Li Lin Lim, Khay Guan Yeoh
Background: Guidelines recommend endoscopy within 24 hours for most patients withupper gastrointestinal bleed (UGIB), and emergency endoscopy for high risk patients, asubgroup still not clearly defined. Objectives:(1)Validate Glasgow Blatchford score(GBS) andadmission Rockall score(ARS) in the study population for accuracy in predicting all-causein-hospital mortality and composite outcomes; (2) Identify the high-risk group with greaterall-cause in-hospital mortality. Design and patients: All adult patients presenting with UGIBat National University Health System, Singapore from January 2007 to June 2008, wereenrolled. Presentation-to-endoscopy-time (PET) was defined as time between presentationfor UGIB to time of gastroscopy. Data was prospectively collected. Main outcome measureswere:(1) all-cause in-hospital mortality; (2)composite outcome of re-bleed, all-cause in-hospital mortality or need for intervention in UGIB. Results: 1008 patients (68.3% male;72.7% Chinese) with a median age of 61 (IQR 48-74) years were included. All-cause in-hospital mortality was 6.4%. There was re-bleed in 8%, surgery in 0.5%, endoscopic treatmentin 31%, blood transfusion in 43%. Area under receiver-operating characteristics curve forGBS and ARS were 0.90 and 0.69 for predicting composite outcome, and 0.82 and 0.79for predicting all-cause in-hospital mortality, respectively, with best cut-off at GBS≥8.Patients with GBS≥8 had greater mortality (12.8% vs 2.3%, p<0.001), more compositeoutcome (89.7% vs 29.3%, p<0.001), more variceal bleed (12.1% vs 4.3%, p<0.001), andmore peptic ulcers (54.8% vs 27.9%, p<0.001). Of 69 patients with GBS of 0, none requiredblood transfusion or surgery, none experienced re-bleed or death, and 2 required endoscopictreatment. Of 301 patients with ARS of 0, 1 died, 9 had re-bleeding, 67 received bloodtransfusion, 54 underwent endoscopic treatment, and 1 required surgery. For patients withGBS≥8, the all-cause inhospital mortality was higher when PET>1 hour when comparedto PET<1 hour (14% vs 5%, p=0.037), and when PET>2 hours when compared to PET<2hours (15% vs 5%, p=0.031). For patients with GBS≥8, there was no significant differencein all-cause inhospital mortality between patients with PET above or below 3, 4, 5, 6, 7, 8,12 and 24 hours, respectively. For patients with GBS<8, there was no significant differencein all-cause inhospital mortality between patients with PET of above or below 1, 2, 3, 4, 5,6, 7, 8, 12 and 24 hours, respectively. Conclusions: GBS outperformed admission Rockallscore in predicting mortality from UGIB. GBS≥8 was associated with greater mortality, andGBS of 0 was associated with good outcome.
S1097
Weekend Effect on Patients With a Nonvariceal Upper GastrointestinalHemorrhage (NVUGIH): Experience in a Single Teaching HospitalPedro Almela, Rosario Anton, Alicia G. Bolos, Marta Bañuls, Joan Tosca, Marta M. Bosca,Rosana Villagrasa, Javier Lizarraga, Alejandro Rodriguez, Jesus M. Santiago, AdolfoBenages
It has been postulated that the patients with acute NVUGIH attended during the weekendhave worse evolution (weekend effect). Objetive: To analyze the weekend effect on themortality in patients with NVUGIH attended in a teaching hospital. Patients and Methods:Prospective study with inclusion of 832 consecutive patients with NVUGIH (2005-2008).All patients were controlled by an identical diagnostic-therapeutic protocol with endoscopy(<24 hrs. post-admission). Patients were subdivided in two groups: A) admission in weekend/holydays and B) admission in weekdays. First, we must demonstrate that between bothgroups of patients do not are significant differences in variables (sex, age, comorbility, timeof evolution of the gastrointestinal hemorrhage, hemodynamic state at admission, endoscopic