Embed Size (px)
Citation preview

CONGRESS OF THE UNITED STATESCONGRESSIONAL BUDGET OFFICE
s T


AN ANALYSIS OFTHE MANAGED COMPETITION ACT
The Congress of the United StatesCongressional Budget Office

NOTES
Numbers in the text and tables of this report may not add to totals because ofrounding.
Cover photo by The Stock Shop, Inc./MediChrome.

Preface
T he Congressional Budget Office (CBO) has prepared this analysis of the ManagedCompetition Act of 1993 in response to several Congressional requests. Thereport summarizes the main provisions of the proposal, examines how they relate
to the key features necessary to achieve the full potential of the managed competitionapproach, and estimates the proposal's effects on national health expenditures and thefederal budget. The report also examines the proposal's impact on the economy and otherconsiderations affecting its design and implementation.
Many staff members in several of CBO's divisions contributed to the analysiscontained in this report. Paul Van de Water coordinated the analysis and the preparationof the report. Linda Bilheimer was responsible for the Summary and Chapter 5, Paul Vande Water for Chapters 1 and 3, Leonard Burman and Sandra Christensen for Chapter 2,and Douglas Hamilton for Chapter 4.
In the Budget Analysis Division, under the supervision of C.G. Nuckols, Paul Vande Water, and Charles Seagrave, contributors were Paul Cullinan, Alan Fairbank, ScottHarrison, Jean Hearne, Lori Housman, Lisa Layman, Jeffrey Lemieux, Patrick Purcell, andConnie Takata. In the Health and Human Resources Division, under the supervision ofNancy Gordon and Linda Bilheimer, contributors were B.K. Atrostic, Carol Frost, CarlaPedone, Constance Rhind, Murray Ross, and Cori Uccello. In the MacroeconomicAnalysis Division, under the supervision of Robert Dennis and Douglas Hamilton,Douglas Elmendorf made important contributions. In the Tax Analysis Division, underthe supervision of Rosemary Marcuss, contributors were David Weiner and RobertonWilliams. Gail Del Balzo, CBO's General Counsel, also contributed.
CBO would like to acknowledge the significant contribution of the staff of the JointCommittee on Taxation, particularly Bernard Schmitt, Ron Jeremias, Thomas Koerner,Pamela Moomau, Michael Udell, Laura Wheeler, and Judy Xanthopoulos. MichaelO'Grady of the Congressional Research Service also provided invaluable assistance.
Paul L. Houts supervised the editing and production of the report. Major portionswere edited by Paul L. Houts, Sherry Snyder, and Leah Mazade. Jeanne Burke, SharonCorbin-Jallow, Dorothy Kornegay, and Linda Lewis assisted in the typing. ChristianSpoor provided editorial assistance during production. With the assistance of MartinaWojak-Piotrow, Kathryn Quattrone prepared the study for final publication.
Robert D. ReischauerDirector
April 1994


Contents
ONE
TWO
THREE
SUMMARY
OVERVIEW OF THE MANAGEDCOMPETITION ACT
Managed Competition 7Assistance to Low-Income People 4Other Provisions 5
THE PROPOSAL'S ADHERENCE TOTHE KEY FEATURES OF THE MANAGEDCOMPETITION APPROACH
Regional Health Plan PurchasingCooperatives 8
Universal Access to Insurance 8Standard Benefit Packages and
Comparative Information 9Nonoverlapping Networks
of Providers 9Risk-Adjusted Payments to
Health Plans 10Limits on the Amount of Tax-
Sheltered Insurance Premiums 10Assumed Effects of the Proposal
on the Growth of HealthCare Costs 13
FINANCIAL IMPACT OF THE PROPOSAL
Determining the Standard BenefitPackage 75
Estimating Health InsurancePremiums 17
How the Proposal Would AffectHealth Insurance Coverageand National Health Expenditures 19
How the Proposal Would Affectthe Budget 21
IX
15

vi AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
FOUR
FIVE
APPENDIX
THE ECONOMIC EFFECTS OF THEMANAGED COMPETITION ACT
The Effect of Insurance Reformson the Labor Market 27
Benefits of Subsidies toLow-Income People 28
Incentives Inherent in theSubsidy System 30
OTHER CONSIDERATIONS
Determining Eligibility forSubsidies 40
The Consequences of Shortfallsin Payments for Low-IncomeEnrollees 42
The Tension Between CoveredBenefits and the Proposed Systemof Subsidies 45
Effects of the Proposal onEmployers and Employeesin Certain Firms 46
Effect of Cost-Sharing Provisionsand Alternative BenefitPackages on AHPs of DifferentTypes 47
Role of the Health CareStandards Commission 48
Conclusion 49
Illustrative Effects of Shortfallsin Federal Subsidies andPremiums Under the ManagedCompetition Act 51
21
39

CONTENTS
TABLES
2-1. Employees' Incentive to Purchase MoreExpensive Health Insurance UnderPresent Law, a Tax Cap, and No TaxExclusion 13
3-1. Health Insurance Coverage Under theManaged Competition Act 20
3-2. Projections of National HealthExpenditures Under the ManagedCompetition Act 21
3-3. Estimated Budgetary Effects of theManaged Competition Act 22
4-1. Projected Poverty Guidelines,U.S. Average, by Family Type, 1995 28
4-2. The Effect of the Managed CompetitionAct on the Number of Uninsured,by Income Category, 1996 29
4-3. Take-Home Pay for Additional Hours ofWork: A Comprehensive Standard BenefitPackage Under the Managed Competition Act 34
4-4. Take-Home Pay for Additional Hours ofWork: A Limited Standard BenefitPackage Under the Managed Competition Act 35
A-l. Shortfalls in Federal Subsidies foran AHP Charging the Reference Premium 52
A-2. Shortfalls in Premiums and FederalSubsidies for an AHP Charging MoreThan the Reference Premium 53

viii AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
FIGURES
4-1. Effective Marginal Tax Rates onCompensation in 1995: A ComprehensiveStandard Benefit Package Under theManaged Competition Act 36
4-2. Effective Marginal Tax Rates onCompensation in 1995: A LimitedStandard Benefit Package Under theManaged Competition Act 37

Summary
T he Managed Competition Act of 1993 en-deavors to slow the growth of health carecosts and expand access to health insurance
by strengthening competitive forces in health caremarkets and providing people with better access toaffordable coverage. It would restructure healthinsurance markets, provide people with strong in-centives to purchase health insurance prudently, andsubsidize health insurance for low-income people.
The proposal would make health insuranceavailable to all but would not establish universalcoverage. Individuals would not have to obtaincoverage if they did not choose to do so, and em-ployers would only have to offer—not pay for—cov-erage for their workers. Even without individual oremployer mandates, the number of uninsured peoplewould drop significantly under the proposal.
The major vehicle for reorganizing the healthcare marketplace would be regional health planpurchasing cooperatives (HPPCs). Through them,employees of small firms (generally those with 100or fewer employees) and individuals with no attach-ment to the labor force would purchase coverage.(Medicare's coverage would, however, be essen-tially unchanged.) The HPPC would offer thosepeople a choice of accountable health plans (AHPs),which would provide a standard benefit package.AHPs would have to meet strict requirements re-garding open enrollment, limits on exclusions forpreexisting conditions, and modified communityrating—allowing each AHP's premiums to vary onlyby age and the type of enrollment (individual, indi-vidual and spouse, individual and one child, andindividual and family).
Firms with more than 100 employees wouldalso have to offer their employees the opportunity topurchase coverage from an AHP. They could ac-complish this either by self-insuring—that is, settingup their own AHPs-or by purchasing coveragefrom an AHP offered in the non-HPPC marketplace.They could not participate in a HPPC, however,unless they were located in states that took advan-tage of the option to raise the maximum size offirms that must participate in a HPPC.
The proposal would make changes in the taxcode, some of which would promote more wide-spread insurance coverage while others would dis-courage the purchase of generous policies. Premi-ums paid to AHPs would be tax deductible up tothe "reference premium11—that is, the premium forthe lowest-cost plan offered through the HPPC thatcovered at least a specified proportion of eligibleenrollees. The deduction would encourage peopleto purchase health insurance: under current law, theself-employed and people purchasing individualpolicies generally do not qualify for tax subsidies.Because premiums in excess of the reference pre-mium would not be deductible, employers would beencouraged to limit their contributions for healthinsurance premiums, and consumers motivated toselect lower-cost health plans.
Under the proposal, the Medicaid programwould end, and a broad system of federal subsidieswould enable low-income people to purchase acutecare coverage from AHPs. States would assumeresponsibility for the long-term care component ofMedicaid, with most of them benefiting from thenew division of responsibilities with the federalgovernment.

x AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
Subsidies for premiums and cost sharing wouldbe available for everyone with income below 200percent of the poverty level. (The only exceptionswould be Medicare beneficiaries for whom subsidieswould mirror current Medicaid benefits for duallyeligible enrollees and "qualified Medicare beneficia-ries.") Those at or below 100 percent of the pov-erty level would be fully subsidized for the refer-ence premium. The premium subsidies would bephased out between 100 percent and 200 percent ofthe poverty level By contrast, the subsidies forcost sharing would be the same throughout theentire income range up to 200 percent of the pov-erty level; no one in this group would have to paymore than nominal cost-sharing amounts. Individu-als with income below 100 percent of the povertylevel would also be eligible to receive a package ofwraparound benefits—additional benefits that wouldnot be part of the standard benefit package.
Spending on the subsidies would be limited tothe amounts generated by proposed reductions incurrent health care programs, revenue changes, andprefunding of retiree health benefits for the PostalService. Low-income participants would not berequired to pay more if insufficient funds wereavailable to fund the subsidies fully; rather, AHPswould have to absorb the shortfalls.
A new federal agency, the Health Care Stan-dards Commission, would oversee the health caresystem and design the uniform benefit package. Itwould establish broad principles and standards forthe system and would also undertake such day-to-day activities as determining eligibility for subsidiesand registering AHPs. The commission's responsi-bilities would be far-reaching and would generallytranscend those of state and local governments inthe health care arena.
Managed Competition
The managed competition approach, which providesthe basis for this proposal, remains largely untried.Advocates of the approach believe it has the poten-tial to slow the rate of growth of health spending,but estimates of the magnitude of such effects arehighly speculative. When the Congressional Budget
Office (CBO) examined this issue in a 1993 study,it concluded that the capacity of any particularmanaged competition proposal to control costswould depend on the degree to which it includedthe following eight features:
o Regional purchasing cooperatives that wouldoversee a restructured health insurance market;
o Universal access to health insurance with com-munity rating of premiums and limited restric-tions on coverage;
o Universal health insurance coverage;
o A standard package of benefits for all healthplans;
o Comparative information on the price and thequality of all health plans;
o Health plans with almost no overlap in theirnetworks of providers;
o Effective mechanisms to adjust the premiumspaid to health plans for the health risks of theirenrollees; and
o Limits on the amount of health insurance premi-ums that people could shelter from taxes set atthe cost of the least expensive plan.
The Managed Competition Act includes all or partof seven of these features. It would not, however,require universal coverage, even though the numberof uninsured people would certainly fall. Whetheran effective risk-adjustment mechanism could bedeveloped is uncertain, but that problem besetsmany health care proposals—not this one alone. Theproposal would also be in closer accord with theeight conditions if all of the population had to pur-chase health insurance through HPPCs and ifHPPCs were given more power to negotiate withhealth plans.
CBO believes that the proposal incorporates thekey attributes of managed competition sufficientlywell that—over time—significant savings wouldresult from both the more competitive market envi-ronment and the enrollment of more people in effec-

SUMMARY
tively managed plans. The magnitude of thesesavings, however, remains largely a matter of specu-lation. Presumably, the effect on the growth rate ofnational health expenditures (NHE) would dependon the benefits included in the standard package.The more comprehensive the package, the larger theproportion of NHE that would be under the man-aged competition system and, hence, subject to itscost-reducing incentives. For the purpose of its costestimates, CBO assumed that increasing enrollmentin effectively managed plans would slow the growthin costs of AHPs by 0.6 percentage point per yearfor the first five years. In addition, competitiveforces would dampen the rate of growth of costs ofAHPs by increasing amounts over the projectionperiod, thereby reducing the annual rate of growthby 1 percentage point after 2004.
Financial Impact ofthe Proposal
As with other proposals to restructure the healthcare system fundamentally, estimates of the effectsof this proposal on national health expenditures andon the federal budget are highly uncertain. In addi-tion to the lack of evidence about the effects ofmanaged competition per se, the proposal leavesmany important details-such as the standard benefitpackage-unspecified.
In preparing its cost estimates, therefore, CBOhad to make a number of assumptions about theeffectiveness of managed competition and the un-specified dimensions of the proposal. The estimatesare extremely sensitive to these assumptions, themost important of which relate to the standard bene-fit package. In general, a more comprehensivebenefit package would result in a higher premium,which would~in turn-translate into higher budget-ary costs and national health expenditures. Al-though a more limited benefit package would have alower premium, it would probably have little effecton the number of people with insurance. Morelimited standard benefits would, however, raise theafter-tax costs of insurance for people who currentlyhave more comprehensive policies, many of whomwould probably purchase supplementary coverageout of after-tax income. As a result, they would
probably become more prudent purchasers of healthinsurance.
Because of the uncertainty regarding the benefitpackage, CBO estimated the financial effects of theproposal under two illustrative alternatives. Thefirst is the comprehensive benefit package proposedin the Administration's Health Security Act. Thesecond is a benefit package costing 20 percent lessthan the first; it would have limited hospital cover-age and would not cover prescription drugs, dentalcare, mental health, and preventive services. CBOconcluded that, for differing reasons, neither alterna-tive would be feasible without further adjustmentsto the proposal.
Under the more comprehensive alternative, thenumber of uninsured people would drop by almost40 percent in 1996 (from 39 million to 24 million),with less than 10 percent of the population remain-ing uninsured thereafter. National health expendi-tures would rise above CBO's baseline initially--reflecting the increase in the number of people withinsurance—but would fall below the baseline oncethe effects of managed competition, more enroll-ment in managed care, and cuts in the Medicareprogram began to be felt. By 2004, NHE would be$30 billion (or about 1V4 percent) below the base-line.
Under this alternative, spending on subsidieswould far exceed the funds designated for them;between 1996 and 2000, the average annual short-fall would be over 30 percent of the subsidies forpremiums for non-Medicare enrollees. Although theproposal would require health plans to absorb short-falls in subsidies, shortfalls of that magnitude couldcause turmoil in HPPC markets. To avoid thatpossibility, the subsidies would have to be close toor fully funded. Consequently, some other featuresof the proposal would have to change if one wishedto maintain a comprehensive benefit package. Pos-sible options include reducing the generosity of thesubsidies or augmenting the pool of resources avail-able to fund the subsidies by cutting other pro-grams, raising taxes, or allowing the budget deficitto increase.
Under the less comprehensive benefit package,the number of uninsured people would be about the

xii AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
same as under the first alternative. As before, na-tional health expenditures would rise in the earlyyears—but by less than under the comprehensivealternative—and then fall below CBO's baseline.
Even though the premium would be 20 percentlower under the second alternative, the resourcesavailable under the proposal would be insufficient tofund the premium subsidies fully. Rather than cutback the already Spartan benefit package further,CBO chose to modify the proposal's subsidyscheme to permit full funding of the subsidies with-out exceeding the funds available in the subsidypool. For the purposes of this illustration, CBOassumed that the cost-sharing subsidies for peoplewith income between 100 percent and 200 percentof the poverty level would be dropped. With thatadditional assumption, the subsidies would befunded in full or nearly so after 1997.
Effects of the Proposalon the Economy
By ensuring that people could purchase health insur-ance at community rates regardless of their healthstatus, the proposed restructuring of the health in-surance market would improve certain aspects oflabor markets. For example, it would assure work-ers who have health insurance through their jobsthat they could continue to obtain coverage if theychanged jobs or left the labor force. Insofar assome workers hesitate to change jobs because of thepossibility of losing their health insurance, the prob-lem of "job lock" would be reduced. Moreover,some workers might choose to retire early if theyknew they could still obtain health insurance.
The subsidies for premiums and cost sharingwould greatly reduce the number of people withoutcoverage and would be very beneficial for low-income workers. But such workers would receivethe full benefit of the proposed subsidy system onlyif their employers did not pay for insurance and,consequently, low-income workers would haveincentives to work for employers that did not payfor insurance. If the employer of a low-wageworker contributed some amount toward insurancecoverage, the subsidy would be reduced dollar for
dollar under the proposal. In addition, the worker'swage would be lower than it would be if the em-ployer did not contribute because employers shiftthe costs of such contributions back onto workersthrough reduced cash wages.
These effects would be particularly pronouncedfor workers with employment-based insurance andincome close to the poverty level; they could earnconsiderably more if their employers no longer paidfor coverage and subsidies would pay for most oftheir health insurance. By contrast, higher-incomeworkers, who would not be eligible for subsidies,would probably prefer that their employers pay forinsurance rather than pay them higher cash wages inorder to avoid the payroll taxes they would pay onhigher wages.
A less desirable consequence of the proposedsystem of subsidies is that it could discourage somepeople with incomes between 100 percent and 200percent of the poverty level from working more.People with income in the range in which the subsi-dies were phased out would have to pay more forhealth insurance as their income rose. Some work-ers in this income range already face high effectivemarginal tax rates because of the phaseout of theearned income tax credit and the payment of incomeand payroll taxes. The phaseout of the subsidies forpremiums would impose an additional marginal levyon workers of 15 percentage points to 30 percentagepoints, depending on their family type and the com-prehensiveness of the benefit package.
Low-income families would also lose valuablebenefits abruptly if their income rose to the point atwhich they lost eligibility for cost-sharing subsidies.(That income level would be 200 percent of povertyunder the proposal as written, or 100 percent ofpoverty under CBO's second alternative with lim-ited benefits.) Since there would be no graduatedphaseout of those subsidies, a large "cliff1 effectwould result: below the income cutoff, peoplewould have full cost-sharing benefits-worth anaverage of approximately $1,400 for a family offour in 1995-and above that income level theywould not have any. A similar "cliff would occurwhen people's income reached 100 percent of thepoverty level and they lost their eligibility for wrap-around benefits. The amount they would lose

SUMMARY xin
would depend on the benefits covered by the stan-dard benefit package—the more generous the cover-age the less would be included in the wraparoundbenefits. Thus, under the comprehensive benefitpackage, the wraparound benefits would be worthan average of $600 for a family of four in 1995;under the less generous alternative, they would beworth $2,900.
The problem of high effective marginal tax ratesfor people affected by the phaseout of subsidies isnot unique to this proposal. Unfortunately, alterna-tive solutions—such as reducing subsidies or phasingthem out over a wider income range-would gener-ate other problems. Smaller subsidies would requirelow-income people to pay a higher percentage oftheir health care costs; a slower phaseout wouldincrease federal subsidy payments and cause work-ers at higher income levels to face disincentives foradditional work.
How Shortfalls in PaymentsWould Affect AHPs andInsurance Markets
Certain features of the proposal might produce unin-tended consequences, lengthen the time needed forimplementation, or limit the effectiveness of theproposal. Some of those features could be modifiedquite easily. Modifying others might prove moredifficult.
One particularly problematic feature of theproposal is the large shortfalls that could faceAHPs. If the funding designated for subsidies wasinsufficient to pay them in full, the federal govern-ment would reduce the proportion of the premiumsubsidies it paid and the AHPs would have to ab-sorb the difference. They could not require low-income enrollees to pay more.
Shortfalls in premiums paid to health planscould also occur with full funding of the federalsubsidies because the maximum federal subsidycould not exceed the reference premium for theHPPC. Low-income enrollees who chose AHPswith premiums higher than that amount would have
to pay only a portion of the difference; the planswould have to absorb the shortfall. Some plansmight also experience shortfalls in subsidies for costsharing because those payments would not be re-lated to the actual use of services by a plan's low-income enrollees.
To ensure that shortfalls in payments would notdisproportionately affect AHPs enrolling large num-bers of low-income people, the proposal wouldestablish an interplan reconciliation process for low-income assistance. The scheme would require allAHPs, including self-insured plans, to participate ina nationwide system to distribute shortfalls in pre-miums and cost sharing equitably among healthplans. This process would be extremely compli-cated; its feasibility is doubtful. Yet, without aneffective mechanism, premiums in the HPPC couldbe highly unstable.
Instability of premiums would be a consequenceof both the uncertainty plans would face in settingpremiums and their probable responses to shortfalls.Although health plans could adapt to some uncer-tainties, as they do today, the proposed approach forshifting shortfalls in payments to plans would re-quire them to deal concurrently with many un-known, interdependent variables in determining theirpremiums. As a result, the process would be excep-tionally difficult. Moreover, there would be noguarantee that the uncertainties would lessen overtime.
AHPs could respond to shortfalls in payments invarious ways. But the responses and their impactswould generally be greater within HPPCs than out-side them because low-income people would consti-tute a much higher proportion of the HPPC popula-tion. In the short term, AHPs might lower pay-ments to providers or reduce the quantity or qualityof the services they provided. In the longer term-when AHPs had the opportunity to do so—theywould almost certainly raise their premiums. Plansfacing strong competitive pressures might withdrawfrom the market altogether.
Because enrollment in AHPs would be volun-tary, some people whose premiums were not heavilysubsidized might drop their insurance coverage ifpremiums rose significantly. Healthy people who

xiv AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
felt the least need for coverage would be the mostlikely to withdraw in those circumstances. The lossof healthier people would cause the average risklevel of enrollees in the HPPC to rise, placing fur-ther upward pressure on premiums. An upwardspiral of premiums in the HPPC might result.
In the absence of an effective distribution pro-cess, extremely high shortfalls in payments couldrapidly undermine insurance markets. For example,under the comprehensive benefit package assumedin CBO's first alternative, the shortfalls in premiumsubsidies would be so large that the HPPC systemmight collapse if AHPs had to absorb them.
Conclusion
The Managed Competition Act would significantlyreduce the number of people lacking health insur-ance, but—because key elements of the proposal areunspecified—its effects on the budget, the economy,and health insurance markets are uncertain. Al-though several features of the proposal as written
might impair its effectiveness or prove difficult toimplement, the majority of them could probably beaddressed quite easily through minor modifications.
More controversial are those elements of theproposal that both reflect its underlying philosophyand might also limit its feasibility. For example,allowing enrollment in AHPs to be voluntary andrestricting the size of firms that could participate inthe HPPC would have the potential to produceunstable premiums—especially if the federal subsi-dies were not fully funded. Moreover, withoutadditional revenues or spending cuts, deficit neutral-ity would be difficult to reconcile with a compre-hensive benefit package and full funding of thesubsidies.
Such problems present difficult choices andtrade-offs. The most immediate question, however,concerns the issues that should be resolved now aspart of the proposal versus those that should be leftto the Health Care Standards Commission, othergovernment agencies, or the Congress to decide inthe future.

Chapter One
Overview of theManaged Competition Act
T he Managed Competition Act of 1993 seeksto slow the growth of health costs and ex-pand health insurance coverage by adopting
the managed competition approach to health carefinancing.1 This approach, which was developed bya group of experts in health policy known as theJackson Hole Group, emphasizes motivating con-sumers, insurers, and providers to be more cost-conscious, and it tries to imbue the health caresystem with the efficiency, flexibility, and innova-tion of competitive markets, without the undesirableoutcomes of the present system. It leaves muchdecisionmaking decentralized. Managed competi-tion also pursues expanded access to health insur-ance coverage, partly because that is an objective inits own right and partly because shrinking the poolof uninsured people would enhance the effectivenessof other changes designed to contain costs.2
The Managed Competition Act would regulatethe health insurance market to make insurance moreavailable and affordable, but it would not requireeither employers or individuals to purchase insur-ance. Various incentives would encourage healthcare providers, insurers, and consumers to focusmore on the cost and quality of care; the govern-
H.R. 3222 was introduced by Congressman Jim Cooper and has57 current cosponsors. A similar Senate bill, S. 1579, was intro-duced by Senator John Breaux and has three cosponsors. For ananalysis of an earlier version of the bill, see "Estimates of HealthCare Proposals from the 102nd Congress," CBO Paper (July1993), Chapter 5.
See Congressional Budget Office, Managed Competition and ItsPotential to Reduce Health Spending (May 1993).
ment, though, would not limit insurance premiums,reimbursement rates, or total spending for health.
The proposal would create a system of man-aged competition consisting of a federal Health CareStandards Commission, regional health plan pur-chasing cooperatives (HPPCs), and a large numberof accountable health plans (AHPs). It would repealMedicaid and establish a new federal program thatwould help low-income people purchase healthinsurance coverage from an accountable health plan.Other provisions are designed to improve access tohealth care in rural and other underserved areas,expand preventive health programs, establish uni-form standards for malpractice claims, and simplifythe administration of health insurance. For the mostpart, the system of managed competition created bythe proposal would not affect the Medicare programor private medigap health insurance policies.
Managed Competition
Managed competition is intended to encouragehealth insurers and health care providers to competeby offering high-quality, low-cost care and not byrisk selecting-that is, by attempting to cover onlythe healthiest individuals. Under the proposal, aHealth Care Standards Commission would overseethe health insurance market and establish a standardbenefit package and other criteria for accountablehealth plans. Changes in the tax code wouldstrongly encourage the use of accountable healthplans. Regional health plan purchasing cooperativeswould allow individuals and small groups to pur-

2 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
chase health insurance on much the same terms aslarge groups. Firms would be required to offerhealth insurance to their employees but would notbe required to pay for it. People eligible for Medi-care would continue to receive health benefitsthrough that program and would not participate inaccountable health plans.
Health Care Standards Commission
A new federal Health Care Standards Commissionwould be created to oversee the system of managedcompetition. The commission would specify auniform set of health insurance benefits, and thecommission's recommendations would go into effectunless overturned by a joint resolution of the Con-gress. These recommendations would supersedestate laws requiring insurers to cover specific healthcare services. The commission would establishuniform cost-sharing requirements for all healthplans, but no cost sharing would be allowed forclinical preventive health services. The commissionwould set these cost-sharing requirements to ensurethat the use of health care services by the currentlyinsured would not increase. It would also establishstandards for reporting prices, health outcomes, andmeasures of consumer satisfaction. Plans that metthe commission's standards would be registered asaccountable health plans.
The commission would also play a substantialrole in the ongoing operation of the health caresystem. It would determine the eligibility of low-income families for subsidies, distribute subsidies tohealth plans on behalf of eligible families, ensurethat any shortfalls in subsidies for premiums wereshared equitably among AHPs, set up a methodol-ogy for allocating risks among health plans withineach HPPC, coordinate the payment of premiums tohealth plans when employees resided outside theiremployer's HPPC area, provide for the auditing ofhealth plans, monitor the reinsurance market forhealth plans, ensure that enrollees were protectedagainst the potential insolvency of their health plan,establish standards for a national health data system,and conduct various analyses of health care expen-ditures and use. By 1997, the commission wouldalso submit to the Congress recommendations forachieving universal health insurance coverage, in-
cluding one regarding an individual mandate topurchase health insurance.
Accountable Health Plans
Accountable health plans would provide healthcoverage in a variety of ways. Some, such ashealth maintenance organizations, might offer healthinsurance and health care as a single product. Oth-ers might provide indemnity insurance benefits.AHPs would be of two types-closed and open.Closed plans generally would be limited to employ-ees of firms employing more than 100 people, par-ticipants in plans established under a collectivebargaining agreement prior to September 1993, andstudents enrolled in a university or college. Closedplans would be required to offer health insurance toall members of the relevant group and would not beoffered through a health plan purchasing coopera-tive. Open plans would be required to accept alleligible applicants and would be available onlythrough a HPPC.
AHPs would be prohibited from basing premi-ums on a person's health status or previous claimsbut could differentiate among demographic groups.The Health Care Standards Commission wouldestablish premium classes based on type of enroll-ment and age. The proposal provides for four typesof enrollment—individual, individual and spouse,individual and one child, and individual and family;the age groups would be established by the commis-sion. In general, each open AHP would establish astandard premium for its plan in each HPPC inwhich it was offered. The premium charged foreach class would equal the standard premium multi-plied by a premium class factor, which the commis-sion would determine. Closed AHPs would alsoestablish a standard premium, but they could basepremiums only on type of enrollment and coulddisregard the adjustment for age. Closed AHPswould also be allowed, but not required, to establishcommon premiums for two or more HPPC areas.
An accountable health plan could offer morebenefits than the standard package, but these itemswould have to be offered and priced separately fromthe uniform benefit package. No AHP or otherinsurer could offer benefits that duplicated those in

CHAPTER ONE OVERVIEW OF THE MANAGED COMPETITION ACT 3
the standard package or reduce cost sharing belowthe uniform amounts established by the commission.
Accountable health plans would face extensiverequirements for reporting information, which wouldhave to be collected and transmitted to the HealthCare Standards Commission or the local HPPC instandardized formats. Plans would have to provideinformation on their preventive health activities,outcomes of treatments, and consumer satisfaction.Moreover, plans would be taxed for failing to com-ply with these requirements and would be prohibitedfrom paying providers who failed to report therequired information. AHPs would also have to payseveral taxes and assessments, including taxes onpremiums to finance graduate medical education andassessments to equalize the burden of any shortfallsin subsidies for premiums for low-income families.
All open AHPs that are health maintenanceorganizations (HMOs) would have to become Medi-care risk contractors—that is, if Medicare beneficia-ries chose to enroll, the plans would have to provideservices for a predetermined periodic payment fromMedicare and would not be reimbursed separatelyfor each service provided. All other AHPs (includ-ing closed plans) would be required to make com-pensating payments if the Health Care StandardsCommission found that Medicare risk contractingput open HMO plans at a disadvantage.
Changes in the tax code would strongly encour-age the use of accountable health plans. The pro-posal would limit the tax deductibility of healthinsurance spending to the "reference premium rate,"which is the lowest premium for the individual'spremium class charged by an open AHP enrolling asignificant percentage of eligible individuals in thelocal HPPC. A 35 percent excise tax would beimposed on employers' payments for health insur-ance or a self-insured plan above the referencepremium, as well as on all payments to plans thatwere not AHPs.3 Individuals (both employed andself-employed) could take an income tax deduction
H.R. 3222 and S. 1579 would set the excise tax rate at 34 percent,the top tax rate on corporate income in effect when the bills weredrafted. The sponsors have told CBO that they intend the excisetax rate to equal the current top corporate tax rate, which wasraised to 35 percent in the Omnibus Budget Reconciliation Act of1993.
for premiums paid to an accountable health plan,but the individual and the employer could togetherdeduct no more than the reference premium. Unlikethe present deduction for medical expenses, the pro-posed deduction for premiums would be available toall individual taxpayers, even if they did not itemizetheir deductions or their medical expenses did notexceed 7.5 percent of adjusted gross income.
Health Plan Purchasing Cooperatives
Each state would set up health plan purchasing co-operatives through which individuals and smallbusinesses would have access to health insurancecoverage. Except for those individuals working forbusinesses with more than 100 employees, everyonewould generally be required to purchase their ac-countable health plan through the HPPC to receive atax deduction. States would have the flexibility tomake larger firms participate in the HPPC, as longas no more than half of the employees in the statewould be eligible to purchase insurance throughHPPCs. Each HPPC would cover an exclusive geo-graphic area~an entire state, a portion of a state, oran interstate region. Once a year, a HPPC wouldoffer each eligible individual the option of enrollingin any one of the open AHPs available in its area.This open enrollment period would have to last atleast 30 days. During this period, the HPPC wouldprovide standardized information on each open plan,including data on price, quality of care, and con-sumer satisfaction. The HPPC could also collectand disseminate information on the quality of careprovided by closed AHPs in its area; if the HPPCdid not do so, the Health Care Standards Commis-sion would perform this task.
The HPPC would collect all premiums fromindividual purchasers and small businesses anddistribute them to the open AHPs. Small businesseswould have to enter into an agreement with thelocal HPPC, furnish the appropriate HPPC with thename and address of each employee, and providefor the payroll deduction of an individual's pre-mium; employers would not be required to enrolltheir employees in a plan or contribute to the costof coverage. Using a procedure to be established bythe Health Care Standards Commission, the HPPCwould pay relatively more to open AHPs that en-

4 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
rolled high-risk individuals and less to AHPs withlow-risk enrollees. The proposal provides for noadjustment of risks among HPPCs or between openand closed AHPs. The expenses of the HPPCwould be financed by a surcharge on premiums forinsurance bought through the HPPC. HPPCs wouldbe prohibited from any actions that affected premi-ums, the reimbursement of providers, or the perfor-mance of AHPs.
Like small firms, large firms (in general, thosewith more than 100 employees) would be requiredto provide an accountable health plan in which theiremployees could enroll and to provide for the pay-roll deduction of premiums. Unlike small busi-nesses, large firms could not offer a plan throughthe local HPPC, but rather would have to contractdirectly with a plan offered outside the HPPC orestablish a self-insured plan. Insurers offeringAHPs in the non-HPPC marketplace would not berequired to charge large firms the same rate chargedenrollees in the HPPC or the same rate chargedemployees of other large firms. Thus, the cost ofthe least expensive AHP available to a large firmmight exceed the reference premium. In such situa-tions, employers would be required to contribute totheir employees' coverage. They would have to paythe difference between the lowest available premiumand the reference premium to ensure that their em-ployees could obtain coverage at no more than thereference rate.
Because people would always have access tohealth insurance coverage, either through the localHPPC or their employer, the proposal would repealthe so-called COBRA requirement for continuationcoverage. Currently, the Consolidated OmnibusBudget Reconciliation Act of 1985 (COBRA) re-quires that employers providing health insuranceand with 20 or more employees must allow partici-pants and other beneficiaries to purchase continuingcoverage for at least 18 months after coveragewould otherwise cease-for example, because of jobloss, death, or divorce.
Assistance to Low-Income PeopleThe Managed Competition Act would repeal Medic-aid and establish a new program to assist many
more low-income people with the costs of healthcare. The federal government would provide subsi-dies for health insurance premiums, cost-sharing re-quirements, and certain benefits commonly coveredunder Medicaid that were not part of the standardbenefit package. Medicare beneficiaries would beeligible for similar subsidies. The Health CareStandards Commission would be responsible fortaking applications for low-income assistance, veri-fying the information provided, computing theamount of assistance, and distributing subsidies tohealth plans on behalf of eligible families. Thesubsidies and other budgetary costs would be fi-nanced by repealing Medicaid, limiting the deduct-ibility of health insurance expenses for employers,reducing certain payments under Medicare, andmaking other changes in taxes and spending.
Subsidies for Premiumsand Cost Sharing
For people not eligible for Medicare, the subsidy oftheir premium would be based on the referencepremium-the premium for the least expensive AHPenrolling a significant number of people in theHPPC. In general, those with adjusted gross in-come up to 100 percent of the poverty level (ad-justed for the state's cost of living) would be eligi-ble for a federal subsidy equal to the referencepremium. The subsidy would be phased out forpeople with incomes between 100 percent and 200percent of the state-adjusted poverty level. Recip-ients of Aid to Families with Dependent Children orSupplemental Security Income would be deemed tobe poor for the purpose of computing subsidies. Anemployer's payments for health insurance on behalfof an individual would reduce the amount of thefederal subsidy dollar for dollar. Medicare benefi-ciaries with income below 120 percent of the pov-erty level would receive a full subsidy of their pre-mium for Medicare's Supplementary Medical Insur-ance~currently $493 a year.
Low-income people who chose to enroll inAHPs charging more than the reference premiumwould receive a reduction in their premium, but thisreduction would be absorbed by other participants inthe plan and not financed by the government. Peo-ple with incomes up to 110 percent of povertywould pay only 10 percent of the difference be-tween their plan's premium and the reference pre-

CHAPTER ONE OVERVIEW OF THE MANAGED COMPETITION ACT 5
mium. This reduction in premiums would bephased out for people with incomes between 110percent and 200 percent of poverty.
All non-Medicare enrollees with income below200 percent of the poverty level would be requiredto pay only nominal cost-sharing amounts, as cur-rently defined for the Medicaid program. Healthplans would be reimbursed by the federal govern-ment for these cost-sharing subsidies based on thenumber and type of low-income people in the plan,not on the amount of services they used. Medicarebeneficiaries with income below 100 percent ofpoverty would be exempt from all cost-sharingrequirements. In this case, Medicare would payproviders the full amount allowed, and the HospitalInsurance Trust Fund would receive an appropria-tion to pay for the subsidies.
For individuals with family income below 100percent of poverty, a wraparound benefit wouldcover certain items commonly covered under Med-icaid, including prescription drugs, eyeglasses, andhearing aids. Specifically excluded would be long-term care services and services included in thestandard benefit package. Because prescriptiondrugs would most likely be covered in the standardbenefit package, the prescription drug coverage inthe package of wraparound benefits would primarilyassist poor Medicare beneficiaries.
States would no longer be responsible for cover-ing acute care for the former Medicaid population.They would, however, assume full responsibility forlong-term care. This trade would provide substan-tial fiscal relief to most states. Moreover, states inwhich state and federal spending on long-term careexceeds the state's share of Medicaid would receivetemporary federal financial assistance, which wouldbe phased out over four years.
Financing
Several changes in taxes and spending would fi-nance the assistance to low-income people, theexpanded deductibility of health insurance premiumsfor employees and the self-employed, and othersmaller costs associated with program expansions.
The proposal would cap the deductibility of healthinsurance expenses for employers, reduce paymentsto providers under Medicare, phase out Medicare'sdisproportionate share payments to hospitals, in-crease Medicare premiums for upper-income benefi-ciaries, require the Postal Service to prefund itsretiree health benefits, and repeal Medicaid.
The proposal is intended to produce no increasein the federal budget deficit. If the savings fellshort of covering the new federal costs, the proposalwould scale back the amount of premium assistanceprovided to low-income people not eligible forMedicare. Under those circumstances, AHPs couldnot increase the premiums charged low-incomepeople but would have to absorb the shortfall infederal payments by increasing premiums, reducingpayments to providers, or other means. Alterna-tively, the Health Care Standards Commission couldtailor the standard benefit package to fit the avail-able funding, additional spending cuts could bemade, or additional revenues provided.
To ensure that AHPs enrolling large numbers oflow-income people were not disproportionatelyburdened by any shortfall in federal subsidies ofpremiums, the Health Care Standards Commissionwould establish a system to ensure the equitabledistribution of the shortfall among health plans.This same reconciliation process would also be usedto equalize reductions in premiums and cost sharing.
Other Provisions
The proposal also contains provisions relating tohealth care services in underserved areas, graduatemedical education, preventive health services, medi-cal malpractice, and administrative simplification.
The proposal would improve access to healthcare in rural and other underserved areas by allow-ing HPPCs to require AHPs in the HPPC to servesuch areas, promoting the development of AHPs inrural areas, authorizing additional funds for migrantand community health centers, and establishing anew system of Medicare payments for rural emer-gency access care hospitals.

6 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
Title III of the bill would alter the system offederal funding for medical education. It wouldestablish a National Medical Education Fund, to befinanced by a levy of 1 percent on the premiums ofall AHPs and by payments from Medicare. TheHealth Care Standards Commission would approveprograms for training medical residents and wouldpay each approved program out of the fund. Thecurrent medical education payments under Medicarewould be repealed. The proposal would also in-crease funding for training midlevel practitioners,the National Health Service Corps, and area healtheducation centers.
Title IV would expand preventive health ser-vices. It would increase authorizations for severalpublic health programs, including immunizationagainst vaccine-preventable diseases, prevention oflead poisoning, prevention of breast and cervicalcancer, health information and health promotion,and the Preventive Health Services Block Grant. Itwould also expand Medicare to cover screening forcolon and breast cancer, vaccination against influ-
enza and tetanus-diphtheria, and well-child care fordisabled children eligible for Medicare. The addi-tional preventive services provided under Medicarewould be financed by an increase in the premiumpaid by Medicare beneficiaries for SupplementaryMedical Insurance.
Title V would establish uniform federal stan-dards for malpractice claims, including limitingclaims for noneconomic damages and reducing longstatutes of limitations. It would also authorizegrants to states to develop systems of resolvingmalpractice disputes other than through court pro-ceedings and to develop medical practice guidelines.
Title VI would attempt to reduce the administra-tive costs of health insurance. Initially, the HealthCare Standards Commission would establish goalsfor standardizing claims forms and electronic trans-mission of data. If the goals were not met, thecommission would set standards and requirementsfor health plans.

Chapter Two
The Proposal's Adherence to the Key Featuresof the Managed Competition Approach
T he managed competition approach seeks toimprove access to health insurance and torestrain the growth of health care costs by
making consumers, insurers, and providers moreconscious of cost. Such an approach would createpurchasing cooperatives to improve access to afford-able insurance for individuals and small groups. Itwould also increase insurers' incentives to competeon the basis of price and quality instead of byavoiding high-risk enrollees. The extent to whichany managed competition proposal could achievethe full potential of this approach depends, in largemeasure, on the degree to which the proposal incor-porates the following eight key features.1
o Regional health plan purchasing cooperatives(HPPCs) would oversee a restructured insurancemarket, with the objective of fostering competi-tion among insurers on the basis of price andquality instead of by seeking to exclude high-risk enrollees.
o Access to insurance would be universal and onan essentially equal basis, accomplished byopen-enrollment periods, community-rated pre-miums, and limited restrictions on coverage, toavoid current insurance practices that have madeinsurance unavailable to many individuals andsmall groups. (Under community rating, premi-ums vary only by type of enrollment and some-times by the age or sex of the enrollee.)
These features were identified and discussed in greater detail inCongressional Budget Office, Managed Competition and Its Po-tential to Reduce Health Spending (May 1993).
o Insurance coverage would be universal, to avoidthe shifting of costs for the uninsured to insuredgroups.
o All plans would offer a standard benefit pack-age, to minimize nonprice differences so thatconsumers could more easily compare plansbased on price.
o The HPPCs would provide comparable informa-tion on both price and the quality of care undereach health plan, to facilitate competition basedon those two factors.
o Health plans would have substantially nonover-lapping networks of affiliated providers, tofacilitate each plan's ability to induce providersto adopt more cost-effective practice patterns.
o Payments from HPPCs to health plans would beadjusted for risk (while maintaining community-rated premiums for enrollees), to reduce plans'incentives to seek lower-cost enrollees ratherthan lower-cost means of providing high-qualitycare.
o The amount of tax-sheltered health insurancepremiums would be limited to the level of theleast expensive plan offered through the HPPCin each region, to make consumers more con-scious of costs.
This chapter discusses the extent to which theManaged Competition Act incorporates each ofthese key features. In brief, the proposal lacks one(the assurance of universal coverage), but it has partor all of the other seven. The chapter concludes

8 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
with a description of the Congressional BudgetOffice's (CBO's) assumptions regarding the degreeto which the growth of health care costs would berestrained by the managed competition features ofthe proposal.
For the most part, the discussion in this chapterassumes that the standard benefit package would becomprehensive, covering most health care needs. If,instead, the standard package was so limited thatmany people purchased supplementary insurance,then a substantial portion of health care spendingwould take place outside the system of managedcompetition. Consequently, the effects of managedcompetition would also be limited, and many of theproblems evident in the insurance market nowwould be present in the market for supplementaryinsurance.
Regional Health PlanPurchasing Cooperatives
Conceptually, regional health plan purchasing coop-eratives are a key element to the success of man-aged competition. HPPCs are intended to integratethe market for health insurance sold to individualsand small employers, which is currently segmentedby risk. By organizing the demand side of themarket and enforcing open access to health insur-ance, the HPPC would create countervailing powerfor purchasers in their relationships with insurers.In addition, the HPPC would restructure competitionwithin insurance markets by providing clearer infor-mation about the differences among insurers' net-works of providers, reducing incentives for insurersto engage in nonprice competition based on enroll-ing low-risk members, and increasing incentives forinsurers to reduce premiums by delivering high-quality care to their enrollees in more cost-effectiveways.
The proposal would establish a single HPPC ineach region to coordinate all offerings by account-able health plans (AHPs) to individuals and smallemployers. The HPPC would provide informationon each plan's price and quality of care; it wouldalso collect premiums from enrollees and make risk-adjusted payments to the plans.
Under this proposal, however, the role of theHPPC would be more limited than might be neces-sary to achieve fully the objectives of managedcompetition. A significant proportion of the insuredpopulation in each state would be outside theauthority of the HPPC because large employerscould not obtain insurance through it. The proposaldefines a large employer as one with more than 100employees, but it would allow states to raise thisthreshold as long as no more than half of all em-ployees in the state would then be eligible to obtaininsurance through a HPPC. Because the HPPC'spool of insured people would exclude those in plansoffered by large employers, it would be smaller andhigher in risk than a pool that included all AHPs inthe region.
Even for HPPC-sponsored health plans, theHPPC would not be permitted to bargain or other-wise influence plans' premiums or the rates paid toproviders. In addition, the HPPC would have noauthority to approve or disapprove health plansseeking to offer insurance in the region—this author-ity would reside, instead, in the new federal HealthCare Standards Commission.
Universal Access toInsurance
The proposal would ensure universal access tohealth insurance, and it would provide subsidies tolow-income people to help them pay the costs ofthat insurance. All HPPC-sponsored AHPs wouldhave to hold open-enrollment periods and chargecommunity-rated premiums. Plans could not denycoverage on the basis of health status, and theycould restrict coverage for preexisting conditionsonly for the first six months of a new policy.
The proposal would not, however, guaranteeuniversal coverage. In the absence of a requirementfor such coverage, people who anticipated relativelyhigh costs for health care would be more likely topurchase insurance than people who expected rela-tively low costs. With a portion of the populationremaining uninsured, per capita insurance costs forthe insured population would be higher, comparedwith universal coverage, for two reasons. First, the

CHAPTER TWO THE PROPOSAL'S ADHERENCE TO THE KEY FEATURES 9
average level of risk among those who purchasedcoverage would be higher than the level amongthose who did not. Second, when uninsured peoplerequired care, providers would probably shift anyuncompensated costs for that care to the insuredpopulation through higher charges that would bereflected in higher insurance premiums.
Standard Benefit Packagesand ComparativeInformation
In addition to the tax cap discussed in a later sec-tion, two other features of the proposal would en-courage price consciousness in health insurance andhealth care markets. First, all AHPs (both the openplans offered through the HPPC and the closedplans offered by large employers) would have tooffer a standard benefit package, which would facil-itate meaningful price comparisons among plansbecause the product would be uniform. Second, theHPPC would be required to compile comparableinformation-not only about price but also aboutquality of care~for all its AHPs to help purchasersbalance quality against costs when choosing a plan.
Both open and closed AHPs would have to meetsimilar requirements with regard to the standardbenefit package, which would include a standardcost-sharing requirement. The proposal's provisionfor a standard benefit package would override cur-rent laws in some states that require insurers tocover specific services.
Plans could offer benefits beyond the standardpackage subject to two conditions: the extra bene-fits could not reduce cost-sharing requirements onthe standard benefits, and the extra benefits wouldhave to be offered and priced separately from thestandard package. Anyone eligible to purchaseinsurance through the HPPC could purchase an openAHP's supplemental policy, whether or not theypurchased that plan's standard policy. The lattercondition would help to ensure that insurers' supple-mental benefits would not become a means for theirachieving favorable risk selection in their standardhealth plans.
Nonoverlapping Networksof Providers
To realize fully the potential savings from managedcompetition, insurers would have to compete vigor-ously with respect to price and quality of care.Effective competition would probably require thatinsurers have nonoverlapping networks of providers.If, instead, most providers were affiliated with sev-eral insurance networks, price differences among theplans would mostly reflect differences in discountsthat the plans had negotiated. Providers' incentivesto adopt the cost-effective patterns of treatmentencouraged by any one of the networks they servedwould be weakened in direct proportion to the per-centage of their patients whose insurers were associ-ated with other networks.
The proposal would override laws that in somestates require managed care plans to enroll all pro-viders in the service area who wish to serve theplan's membership. Thus, the proposal would per-mit insurers to form nonoverlapping networks ofaffiliated providers, but to what extent insurerswould actually do so is unclear. Competitive pres-sures might be sufficient to induce insurers to de-velop such networks, but the incentives would beeven stronger if insurers were held accountable forthe quality of care provided under their plans.
Effective accountability for the quality of careprovided under their health plans would substan-tially change the incentives insurers now face. Itwould encourage much closer scrutiny of the pro-viders they enrolled and closer involvement in theday-to-day practice of those providers. A degree ofaccountability would be achieved through the disci-pline of a market in which consumers were well in-formed about differences in the quality of careprovided through each network; under the proposalthe HPPC would provide such information to indi-vidual consumers and small employers. Another,more certain way to achieve accountability wouldbe to hold insurers liable, along with their affiliatedproviders, under current standards for malpractice,but the proposal has no such provision.

10 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
Risk-Adjusted Paymentsto Health PlansIn any system that required open enrollment withcommunity-rated premiums but that had no mecha-nism to neutralize the financial effects of risk selec-tion, the main factor determining profitability forinsurers would be how successfully they couldattract relatively healthy enrollees. Under the man-aged competition approach, even if the benefit pack-age was uniform and enrollment in plans was con-trolled by the HPPCs, plans might nevertheless findways to achieve favorable risk selection. For exam-ple, plans might target their marketing to moreactive (and presumably healthier) people, or theymight limit the number of affiliated physicians instrategic specialties. Plans with limited access tocardiologists, for instance, would be unlikely toattract many people with heart disease.2 Withoutcompensating payments, plans that enrolled a rela-tively large proportion of high-cost members mightbe unable to compete because of the characteristicsof their membership, even if they provided carevery efficiently.
In principle, the proposal would establish asystem of payments to compensate plans for differ-ences in risk, but no accurate mechanism currentlyexists to calculate such payments. Also unclear ishow quickly risk-adjustment mechanisms could bedeveloped or how accurate they would have to be toeliminate incentives for plans to compete based onrisk selection rather than price and quality. What iscertain is that without a mechanism that was "goodenough," efficient plans would not necessarily berewarded appropriately.
Limits on the Amountof Tax-ShelteredInsurance PremiumsOne of the key elements of managed competition islimiting the amount of tax-sheltered health insurance
premiums to the cost of the least expensive planavailable to each enrollee. Because the additionalcost of purchasing a more expensive plan would notbe subsidized through the tax system, consumerswould be more conscious of the cost of healthinsurance. This awareness, in turn, would make in-surers more conscious of the costs they incurred toprovide benefits.
Under the proposal, only premiums for plansthat met the requirements established by the HealthCare Standards Commission-accountable healthplans—would be deductible, and for these plans thetax preference would be limited. The proposalwould cap the currently unlimited tax subsidy foremployment-based health insurance by imposing anexcise tax on employers' contributions that wereabove the premium for the lowest-cost plan in theHPPC—the reference premium. (If an employercontributed less than the amount of the referencepremium, the difference between the reference pre-mium—or the actual premium, if less—and theemployer's contribution could be deducted fromtaxable income by the worker.) The proposal wouldalso allow self-employed people and individualenrollees to deduct premium payments, up to theamount of the reference premium, from their in-come. That provision would expand the tax subsidyfor these people because most premiums paid byindividuals do not qualify for tax subsidies undercurrent law.3
The Effect of the CurrentUnlimited Tax Subsidy onSpending for Health Care
Health care costs are high in part because healthinsurance premiums are subsidized through the taxcode. Employers' contributions toward the cost ofemployees' health insurance are not taxable com-pensation. Unlike cash wages, they are not subjectto income or Social Security payroll taxes. As aresult, saving a dollar's worth of employment-based
2. See J.P. Newhouse, "Patients at Risk: Health Reform and RiskAdjustment," Health Affairs, vol. 13, no. 1 (Spring (I) 1994).
For self-employed people and other individual purchasers, insur-ance premiums up to the cap would be a deductible expense forincome tax purposes but not for calculating liability under theSocial Security payroll tax.

CHAPTER TWO THE PROPOSAL'S ADHERENCE TO THE KEY FEATURES 11
health insurance gains the typical employee in 1994only 74 cents in take-home pay.4
The tax subsidy for employment-based healthinsurance has encouraged employers to sponsorhealth insurance coverage for their employees.About 75 percent of workers and their families arecovered by such insurance. But the subsidy hasalso discouraged workers and employers from seek-ing less expensive forms of health insurance be-cause the tax subsidy is unlimited. Because thesubsidy is more valuable for comprehensive healthinsurance with few controls on costs than for moreeconomical health insurance coverage, employersexert less pressure on insurers to control costs thanthey otherwise would.
The subsidy adds to health spending in twoways. First, people tend to buy more of anything,including insurance, when its price is reduced.Second, the additional spending on insurance indi-rectly translates into additional spending on healthcare. People with health insurance pay little ornone of the cost of care when they get sick; instead,insurance pays the cost for them. As a result, theyand their doctors have little incentive to pay atten-tion to the costs of diagnostic and treatment options.
The Effect of the Tax Capin the Proposal
Limiting the tax subsidy by imposing a tax cap ofsome form would encourage employees and em-ployers to choose more cost-effective health insur-ance. One type of cap would require employees toinclude in their taxable income the portion of theiremployer's payments for health insurance premiumsthat exceeds the cost of the lowest-cost plan avail-able to them—the cap amount. Another optionwould prohibit employers from claiming as a busi-ness income tax deduction any health insurancepayments in excess of the cap amount. A third op-tion, which is the approach taken in the proposal,would apply an excise tax to employers' contribu-
4. See Congressional Budget Office, The Tax Treatment of Employ-ment-Based Health Insurance (March 1994).
tions in excess of the cap. (Like other excise taxes,the 35 percent excise tax in this proposal would bea deductible business expense.)
Effect on Employers' Contributions for HealthInsurance. Under the proposed tax cap, an em-ployer that contributed more than the amount of thereference premium would have to pay a 35 percentexcise tax on the excess contribution. That taxwould be passed on to employees in the form oflower cash wages. Thus, employees would ulti-mately pay the tax even if the employer chose tocontribute more than the cap amount. If, instead,the employer limited its contribution to the amountof the cap, employees could select a more expensiveplan, but they would pay the additional cost out ofafter-tax, rather than pretax, income. In otherwords, if the excise tax caused employers to limittheir contributions to the reference premium, the taxwould have the same effect as a limit on the amountof health insurance premiums that could be ex-cluded from employees' taxable income.
The excise tax would create a strong incentivefor employers to limit their contributions to the ref-erence premium, but the cap in the proposal wouldconstrain the choices of some employbrs and theiremployees more than others. For small employers,who would have to obtain coverage through theHPPC, the cap would-by definition-equal the costof the lowest-cost AHP available to their employees.Thus, any additional expenditures for health insur-ance would either be subject to an excise tax, if theemployer paid the additional premium, or incomeand payroll taxes, if the employee paid it.
Because a large employer—generally, one withmore than 100 employees—that wanted to pay forinsurance for its employees would be required topurchase insurance outside the HPPC, the premiumfor its lowest-cost plan would not necessarily equalthe reference premium. Plans sponsored by em-ployers whose workers were less healthy than theaverage participant in the HPPC areas in which thefirm operated would typically cost more than thereference premium. Those employers would beleast likely to pay more than the premium for theleast expensive plan available to them. Moreover, ifthey limited their contributions to the cap amount,employees who wanted health insurance would have

12 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
to pay the amount in excess of the reference pre-mium out of after-tax wages.
But some other large firms would be less con-strained by the cap in the proposal. Their premiumfor a plan that covered the standard benefits wouldbe less than the reference premium because theirworkers would be healthier than average.5 Thesefirms would still have a strong incentive to limittheir contribution to the cap, but that contributionmight pay for basic insurance that cost more thanthe reference premium or for supplemental healthinsurance policies offered through an AHP. Thus,the cap would constrain the behavior of those largefirms less than the behavior of small firms under theproposal.6
The adjustment of employers' contributions tothe cap levels might take several years. Over theshort run, employers might continue to make contri-butions that exceeded the reference premium-because of multiyear labor contracts, for example.7
But over time, most would have a strong incentiveto limit their contributions to the amount of the capand increase employees' wages. An employer whocontributed more than the cap would have to payexcise taxes on its excess contributions for all em-ployees—even for those employees who would havebeen satisfied with a plan that could be purchasedfor the reference premium. Thus, the employerwould be paying a tax (plus the additional premi-ums) to provide a benefit that was valuable only tosome employees. By limiting contributions to theamount of the cap, the employer could make
5. The proposal would also allow large employers that maintained aclosed AHP to elect to use simplified rules for computing thereference premium. For example, an employer with younger-than-average employees would have a higher tax cap if it elected to usea "community rate" reference premium rather than one based onthe age composition of its work force. That election might allowthe employer to avoid the excise tax or to offer additional healthbenefits without exceeding the tax cap.
6. Some self-insured firms might also be able to circumvent the capsby recharacterizing insurance costs as company overhead or byartificially reallocating costs from enterprises with low insurancecosts to those with high costs. For a discussion of this issue, seeChapter 6 of Congressional Budget Office, The Tax Treatment ofEmployment-Based Health Insurance.
7. The proposal provides a temporary exception from the excise taxfor health insurance contributions made by employers as part of acollective bargaining agreement ratified before the date of enact-ment of the proposal, or January 1, 1998, whichever is earlier.
employees who chose the low-cost plan better off;employees who preferred the high-cost plan couldstill pay the extra premiums out of after-tax income.
Over the long run, firms would be likely to paymore than the cap amount for their employees'health insurance only if almost all employees agreedthat they wanted a health insurance plan with a pre-mium that exceeded the cap. Those employeeswould pay less for their insurance if their employerpaid the 35 percent excise tax and passed on the taxin the form of lower wages than if they had to paythe extra premiums out of after-tax wages.8 Theless comprehensive the standard benefit package, themore likely it would be that employees would agreeon additional health benefits. Thus, more firmswould elect to offer health insurance that exceededthe reference premium (and would thus incur theexcise tax) under a limited standard benefit packagethan under a more comprehensive one.
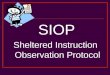
Effect of a Tax Cap on the Choice of Health In-surance Plans. An example illustrates how a taxcap, such as the one in the proposal, would providea stronger incentive than exists at present to selectlow-cost health insurance. Suppose that the low-cost health insurance plan in an area costs $4,000for family coverage and that the high-cost healthplan costs $5,000. Under current law, if the em-ployer is willing to contribute the entire premium(in exchange for paying lower cash wages), everydollar of health insurance costs the employee a dol-lar of cash wages minus the income and payrolltaxes that would be paid on those wages. An em-ployee subject to a marginal tax rate of 30 percentwho was covered by the low-cost health insuranceplan for $4,000 would save $1,200 in taxes com-pared with receiving the $4,000 in cash wages (seeTable 2-1).9 If the employee was covered by the
8. Because the reduction in wages as a result of the excise tax wouldreduce employees' income and payroll tax liability, the effectivetax rate on the excess premiums paid by the employer wouldrange from 20 percent to 25 percent for employees with taxableincome. Those rates are lower than the combined income andpayroll tax rates for most employees, so employees who preferreda more expensive health insurance plan would rather have theiremployer pay for it-and pay the excise tax-than receive the addi-tional compensation as taxable wages.
9. The 30 percent tax rate corresponds roughly to the combinedincome and payroll tax rates (both the employer and employee

CHAPTER TWO THE PROPOSAL'S ADHERENCE TO THE KEY FEATURES 13
Table 2-1.Employees' Incentive to Purchase More Expensive Health Insurance UnderPresent Law, a Tax Cap, and No Tax Exclusion (In dollars)
Low-CostInsurance Plan
Present Law(Full exclusion)
Tax Cap of $4,000
Before-TaxCost
4,000
4,000
AmountExcluded
fromTaxes
4,000
4,000
TaxSavings
1,200
1,200
After-Tax
Cost*
2,800
2,800
Before-TaxCost
5,000
5,000
High-CostInsurance Plan
AmountExcluded
fromTaxes
5,000
4,000
TaxSavings8
1,500
1,200
After-TaxCost
3,500
3,800
AdditionalCost of
High-CostPlan After
Taxes
700
1,000
No TaxExclusion 4,000 0 4,000 5,000 5,000 1,000
SOURCE: Congressional Budget Office.
a. Based on a marginal tax rate of 30 percent.
high-cost plan for $5,000, the tax savings from theexclusion would increase to $1,500. Thus, the addi-tional cost of the more expensive plan after taxes isonly $700. When the additional services or reducedcost sharing in the more expensive plan are worthmore than $700, under current law an employeewould choose the more expensive plan, even thoughthe additional premiums cost $1,000 before consid-ering the tax savings.
Suppose that under the proposal the employerchose to contribute only $4,000. The cost to theemployee of the low-cost health insurance planwould not change because the employer's contribu-tion would continue to be fully excluded from taxa-tion. If the employee paid the additional $1,000 inpremiums for the high-cost health insurance, the taxsavings would not change because of the cap. As aresult, the after-tax cost of insurance would increasefrom $2,800 to $3,800. The additional cost wouldbe the same as if no tax exclusion had existed at all(see Table 2-1). Thus, if the cap was in place, theemployee would choose the more expensive plan
shares) for a taxpayer in the 15 percent income tax bracket. Notethat eventually the immediate savings in payroll taxes are offset inpart by lower Social Security benefits than would be paid if allcompensation had been in the form of wages.
only if it was worth its full additional cost. Forexample, if the additional services covered under thehigh-cost plan were worth only $850 to the em-ployee, the cheaper plan would be chosen under thetax cap. But under present law, the employeewould choose the more expensive plan.
Assumed Effects of theProposal on the Growthof Health Care Costs
If the standard benefit package was a comprehen-sive one, the Managed Competition Act would putin place, to some degree, all of the features impor-tant to the success of managed competition exceptuniversal coverage, but it would be unlikely to real-ize the full potential of that approach to containinghealth care costs. Its potential would be enhanced ifthe HPPCs had more power to negotiate with AHPsand if everyone purchased health insurance throughthese cooperatives (which would mean that an effec-tive tax cap would apply to them all). Achievingthe full potential of managed competition wouldalso depend on developing an adequate mechanismfor adjusting payments to plans to compensate for

14 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
risk selection; this problem, however, is one thatwould affect all managed competition proposals.
CBO assumes that the proposal would restrainthe growth of health care costs through two mainavenues. First, the incentives created by the man-aged competition environment would accelerate theshift in insurance enrollment that is already underway toward effectively managed plans. CBO as-sumes that this effect would slow the growth incosts of AHPs by 0.6 percentage point per year forthe first five years, compared with the rate ofgrowth that would result under current law. Be-cause of this effect, national health expenditures bythe year 2000 would be about 1 percent lower thanthey would be otherwise.
Second, CBO assumes that the competitivepressures fostered by the proposal would cause allinsurers to intensify their efforts to control costs.How successful they would be, and the resultingeffect on the growth of overall health care spending,are uncertain. There are no credible estimates ofthe potential savings under managed competition,largely because this approach is untried. Althoughsome features of managed competition exist inCalifornia, Minnesota, Wisconsin, and perhaps afew other states in which large purchasing coopera-
tives have been formed in recent years, the broadercontext in which these cooperatives operate differsfrom the environment that would exist under currentmanaged competition proposals. For the cost esti-mates provided in the next chapter, CBO assumesthat the competitive pressures created by the pro-posal would dampen the rate of growth of costs ofAHPs by increasing amounts over a 10-year period,until the restraint amounted to a 1 percentage-pointreduction in the rate of growth of these costs foreach year after 2004.
These assumptions are used for both of thealternatives examined in the next chapter—one basedon a comprehensive standard benefit package andone based on a more limited package. Growth innational health expenditures would be more con-strained under the comprehensive package thanunder the limited one, though, because a largerportion of that spending would flow through themanaged competition system if the package wascomprehensive. Thus, in 2004 the estimated rate ofgrowth in national health expenditures would be 7.6percent under the alternative with a comprehensivestandard benefit package, 7.8 percent under thealternative with a more limited package, and 8.2percent under current law. However, a great deal ofuncertainty surrounds these estimates.

Chapter Three
Financial Impact of the Proposal
T he Managed Competition Act aims to slowthe growth of national health expendituresand increase the number of people with
health insurance. In the Congressional BudgetOffice's (CBO's) estimation, the proposal wouldlead to a slight increase in national health expendi-tures in the near term but would reduce healthspending in the long run. Under the proposal, morethan 15 million additional people would be coveredby health insurance, and the number of uninsuredwould fall to less than 10 percent of the population.
The Managed Competition Act would achievethese outcomes by fundamentally transforming thenation's health insurance markets and its health caredelivery system. The effects of these changes,however, are difficult to predict. Like the estimatesof other proposals for comprehensive reform, suchas the Administration's proposal or the single-payerplans, CBO's estimates of the effects of the Man-aged Competition Act are unavoidably uncertain.1
Despite their lack of precision, however, estimatesof the effect of different approaches to health re-form provide useful comparative information ontheir relative costs or savings.
CBO's estimates of the effects of the ManagedCompetition Act on national health expenditures andthe federal budget use CBO's baseline projectionsas their starting point. The Economic and BudgetOutlook: Fiscal Years 1995-1999 (January 1994)
CBO has released estimates of the costs of the Administration'sproposal (H.R. 3600) and two single-payer plans (H.R. 1200 andS. 491) and will soon be providing estimates for other pendingproposals. See Congressional Budget Office, An Analysis of theAdministration's Health Proposal (February 1994).
describes CBO's current economic assumptions andbaseline budget projections. A CBO Memorandum,"Projections of National Health Expenditures: 1993Update" (October 1993), sets out CBO's baselineprojections of national health expenditures.
Determining the StandardBenefit Package
The Managed Competition Act poses a major prob-lem for estimation because it does not specify oneof the most crucial elements of the new system~thestandard benefit package that would be offered byaccountable health plans (AHPs). Over the 10 yearscovered by CBO's estimate, a more comprehensivepackage would add to budgetary costs and nationalhealth expenditures. With a comprehensive standardbenefit package, people would have little need topurchase supplementary health insurance coverage,but the demand for such supplementary coveragecould be considerable if the standard package wasvery limited.
Under the proposal, the Health Care StandardsCommission would specify the standard benefitpackage. This package would go into effect unlessdisapproved by a joint resolution of the Congress,which would have to be signed by the President.The commission could change the benefit packageannually under the same procedure.
One can only speculate about the comprehen-siveness of the benefit package that the commissionmight choose. As a politically appointed body, the

16 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
commission would be subject to many pressures,including the need to obtain Congressional andPresidential approval for its recommendations. Itmight find it difficult to limit the services thatwould be covered under the standard package. Ifso, the benefits could be fairly comprehensive-forexample, somewhat more generous than the averageof existing private health insurance policies—and thepackage would be relatively costly. Alternatively,the commission could try to design a benefit pack-age whose cost did not exceed the savings generatedby the proposal. Such a limited package, however,would be far less comprehensive than the benefitsnow enjoyed by the vast majority of people withhealth insurance.
Because of the uncertainty regarding the benefitpackage, CBO has estimated the financial impactsof the proposal using two illustrative alternatives-acomprehensive benefit package, which is identical tothat proposed by the Administration, and a limitedbenefit package, which is 20 percent less costly.For differing reasons, however, neither of these twoalternatives is likely to be workable without furtheradjustments to the proposal.
Alternative 1: A ComprehensiveBenefit Package
The first benefit package—a relatively comprehen-sive one—would cover the same services in the firstyear as the package specified in the Administra-tion's health proposal. This package is roughly 5percent more generous than the average privatehealth insurance plan, but a bit less generous thanthe average plan provided by large firms.
The explicit limits on the growth of health in-surance premiums included in the Administration'sproposal but absent in the Managed CompetitionAct complicate the comparison of the benefit pack-ages in the two proposals after the first year. Ulti-mately, the Administration's proposal would limitthe growth of premiums to roughly the rate ofgrowth of the economy. The rate of growth ofpremiums under the Managed Competition Act,which would rely primarily on market forces toconstrain costs, would be higher. Whether theAdministration's proposal could actually provide the
same level of health benefits and services as theManaged Competition Act with a much lower levelof spending is not clear. To some extent, theAdministration's proposal might constrain costs byreducing inefficiencies or limiting payments toproviders of health care. But it is also possible thatthe Administration's proposal would result in alower amount or quality of health care services thanthe Managed Competition Act, even if the benefitpackages in the two proposals were nominally thesame.
Under the comprehensive alternative, the subsi-dies and other costs to the federal governmentwould far exceed the savings generated by the pro-posal. Because the proposal would largely precludeincreases in the deficit, other steps would have to betaken to make up the shortfall. If the Congress didnot adopt additional spending cuts or tax increases,the commission would be required to reduce thepremium subsidies provided to accountable healthplans for low-income participants. In that case,AHPs would have to accept the reduced subsidies asfull payment and would have to find ways to dealwith the shortfall. As Chapter 5 describes in detail,however, CBO believes that the uncertainty andinstability inherent in this process could seriouslycompromise the orderly functioning of the marketfor accountable health plans.
Alternative 2: A LimitedBenefit Package
The second illustrative option is a much morelimited standard benefit package. This package is20 percent less expensive than the comprehensiveone and would roughly balance the savings andcosts of the proposal over its first five years ofoperation. Equating the costs and savings each yearwould require annual changes in the benefit pack-age, both up and down, and would create seriousadministrative problems for consumers, health plans,and health plan purchasing cooperatives (HPPCs).The benefit package that could be obtained for thislower premium would be less generous than that en-joyed by 90 percent of people with private healthinsurance coverage. Such a benefit package wouldnot cover mental health services, prescription drugs,preventive health services, or dental care and would

CHAPTER THREE FINANCIAL IMPACT OF THE PROPOSAL 17
severely limit coverage of hospitalization. In addi-tion, CBO has assumed that this alternative wouldnot provide cost-sharing subsidies to people withincomes above 100 percent of the poverty level.
The second alternative is as problematic as thefirst, although for different reasons. First, thelimited benefit package assumed by CBO may notbe consistent with the proposal's requirement thatthe benefit package cover all medically appropriatetreatments and a full range of preventive and diag-nostic services. Second, in order to make the pro-posal fit within the available funds, CBO has elimi-nated the cost-sharing subsidies that the proposalspecified for persons with incomes between thepoverty level and twice the poverty level.
Under the limited alternative, those with incomebelow 100 percent of poverty would continue tohave rather generous coverage: the wraparoundbenefit would cover the excluded services, and theywould be required to pay only nominal cost sharing.Those with incomes not far above the poverty level,however, would have less comprehensive benefitsand would have to pay significant amounts of costsharing from after-tax income. Under the proposal,they could not obtain supplementary policies thatcovered this cost sharing. Among upper-incomepeople, supplementary insurance covering the ex-cluded services and bought with after-tax dollarscould become widespread. Thus, under this alterna-tive, health insurance coverage would probably bemore limited for middle-income people than for therich or poor.
Estimating Health InsurancePremiums
A second critical element in assessing the impact ofthe Managed Competition Act is estimating thepremiums that would be charged for accountablehealth plans inside and outside the HPPCs. Thissection describes how CBO estimated the initiallevel of premiums for the comprehensive benefitpackage and their subsequent rate of growth. Thepremiums for the limited benefit package wereassumed to be 20 percent lower across the board.
Initial Level of Premiums
The premiums to be paid to health insurance plansand the extent of health insurance coverage underthe proposal must be estimated jointly. For a givenset of benefits, the level of the premium, net of anygovernment subsidy or employer contribution, af-fects the number of people who buy insurance, andthe number of people who buy insurance affects thepremium.
The estimate proceeds in three steps: calculatethe amount of health spending under the proposalfor people who would be eligible to participate inthe HPPC and for those who would have to pur-chase their AHP through their employer, estimatethe proportion of people in various demographiccategories who would decide to purchase healthinsurance, and compute the average premiums insideand outside the HPPC based on the amount ofhealth spending for those who would choose toparticipate in the program.
The estimate of premiums relies on demo-graphic and income data from the March 1993Current Population Survey (CPS) and data on theuse of health care services from the 1987 NationalMedical Expenditure Survey. The population wassubdivided into categories based on the proposedpremium classes (individual, individual and spouse,individual and one child, and individual and family),current insurance coverage (employer-sponsoredinsurance, individually purchased insurance, Medic-aid, or no insurance), level of income, size of theprimary worker's firm, and whether or not the em-ployer now contributes to the cost of insurance.The data on use of health care services were used toallocate national health expenditures among eachcategory of people. The expenditure figures wereboosted to reflect the higher use of services ex-pected for those becoming newly insured, the gener-osity of the comprehensive benefit package, and anincrease in rates of payment for services previouslypaid by Medicaid.
All people who currently receive cash welfarebenefits, purchase individual health insurance, orwork for large employers that provide health insur-ance were assumed to purchase health insurancecoverage under the new system. As discussed in

18 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
Chapter 4, however, enacting the proposal is likelyto cause some employers to reduce their contribu-tions to their employees' health insurance and allowthe government to assume the cost of covering theirlow-income workers. The estimate assumes that 10percent of workers with employer-sponsored insur-ance in small firms would lose their employer'scontribution and that half of these workers wouldstill decide to purchase insurance. In addition, forworkers with incomes below the poverty level, theaverage payment by contributing employers wasassumed to fall from about 85 percent of the costinitially to about 75 percent over 10 years, sincesome employers would cease making contributionsfor low-income workers. For the rest of the popula-tion-primarily the uninsured and Medicaid recipi-ents who do not receive cash welfare benefits—thedecision to purchase or not purchase health insur-ance was assumed to hinge on its net price.2 Theparticipation rates for low-income people, whowould see large reductions in the net price of insur-ance, was assumed to depend on the ratio of priceto household income.3
The estimated average premiums in 1994 for thecomprehensive benefit package for the four types ofpolicies specified in the proposal are as follows:
IndividualIndividual and SpouseIndividual and One ChildIndividual and Family
InsideHPPC
$2,500$5,000$3,976$6,796
OutsideHPPC
$2,345$4,690$3,560$6,153
Based on data on the distribution of insurance pre-miums, the estimate assumes that the reference pre-mium-the premium for the least expensive plan inthe HPPC with substantial enrollment-would be 90percent of the premium of the average plan.
2. Congressional Budget Office, "Behavioral Assumptions for Esti-mating the Effects of Health Care Proposals," CBO Memorandum(November 1993), pp. 4-5.
3. Lewin-ICF, Inc., "Insurance Coverage and Health ExpendituresUnder the Bush and Clinton Health Reform Plans" (October1992), p. 12.
The premiums inside the HPPCs would exceedthose outside the HPPCs by about 10 percent be-cause of differences in the use of health care ser-vices by the insured population. In particular, theHPPCs would cover most current recipients of Med-icaid as well as many early retirees, both of whomare relatively heavy users of health care. Congress-man Jim Cooper has informed CBO that he intendsto modify his proposal by placing disabled Medicaidbeneficiaries in a separate risk pool. This changecould reduce the difference in premiums betweenplans in HPPCs and those outside by as much asone-half.
Although the comprehensive benefit package inthe Managed Competition Act is assumed to be thesame as the standard package in the Administra-tion's proposal, the cost of the package would dif-fer. For example, the 1994 premium for a singleperson would be an estimated $2,100 under theAdministration's proposal and almost $2,400 for allAHPs (both inside and outside HPPCs) under theManaged Competition Act. About $50 of this dif-ference stems from treatment of Medicaid beneficia-ries, whose costs would be largely excluded fromthe premium calculation for the Administration'splan. The generous cost-sharing subsidies—whichwould increase the use of health care services bylow-income enrollees—and the assumed increase inMedicaid's payment rates add another $100 to thepremium for the Managed Competition Act. Theremaining difference is largely attributable to ad-verse selection; the Administration's proposal wouldrequire universal participation, but low-risk individ-uals could opt to go without insurance under theManaged Competition Act.
Rate of Growth of Premiums
The estimate assumes that the proposal would slowthe rate of growth of health expenditures and healthinsurance premiums for two reasons. First, theproposal would encourage more people to enroll inhealth maintenance organizations (HMOs). Second,the competitive pressures created by managed com-petition would cause all insurers to intensify theirefforts to control costs.

CHAPTER THREE FINANCIAL IMPACT OF THE PROPOSAL 19
Because group- or staff-model HMOs can pro-vide health care more efficiently than other organi-zational forms, they would probably be the lowestbidders in most HPPC areas. Thus, the proposalwould increase the difference in effective pricesbetween fee-for-service plans and HMOs becausepeople would have to pay the higher cost of fee-for-service plans out of after-tax rather than before-taxincome. Based on the experience of California,Minnesota, and Wisconsin-states whose healthinsurance programs for public employees embodyaspects of managed competition-CBO assumes thatthree-quarters of the nonpoor, urban populationwould ultimately choose HMOs instead of moreexpensive fee-for-service plans. Based on its reviewof the available evidence, CBO finds that the mosteffective HMOs reduce the use of health care ser-vices by about 9 percent compared with the fee-for-service sector and that the average reduction isabout 4 percent.4 All in all, the estimate assumesthat the shift to managed care would slow thegrowth in costs for private health plans by 0.6 per-centage point per year for the first five years of theproposal. This assumption presumes that HMOswould find some way to cope with the difficultiescreated for them by the cost-sharing requirementsand the limited benefit package (see Chapter 5).
As detailed in Chapter 2, the proposal incorpo-rates, to some degree, all of the features importantto the success of managed competition in control-ling health care costs, except universal health insur-ance coverage. Because managed competition is anuntried concept, however, no data exist that wouldallow one to estimate its effect on the growth ofhealth expenditures. In the absence of any data, thisestimate assumes that the system of managed com-petition established by the proposal would dampenthe rate of growth of private health insurance costsby an amount reaching 1 percentage point a yearafter 2004. The same assumption about the effectof managed competition is used for both alterna-tives—the comprehensive and the limited benefitpackages-although managed competition would af-fect a smaller share of health spending if the stan-dard package was limited in its scope.
4. Congressional Budget Office, "Effects of Managed Care: AnUpdate," CBO Memorandum (March 1994).
How the Proposal WouldAffect Health InsuranceCoverage and NationalHealth Expenditures
The Managed Competition Act would encouragemore people to obtain health insurance coverage bysubsidizing its purchase. People with very low in-comes would receive direct government subsidies,and people with higher incomes would be allowedto deduct the cost of health insurance from theirtaxable income. At first, the expansion of healthinsurance coverage would increase the demand forhealth care services and would add to nationalhealth expenditures. In the longer run, however, thesystem of managed competition would slow thegrowth of health spending and bring national healthexpenditures below the baseline level.
The estimates of health insurance coverage andnational health expenditures assume that the pre-mium assistance specified in the proposal is fullyfunded, either through additional spending cuts, taxincreases, or borrowing. Failure to fund the subsi-dies could result in an upward spiral of health insur-ance premiums, declines in health insurance cover-age, and, potentially, the collapse of the HPPC sys-tem (see Chapter 5).
Health Insurance Coverage
The low-income assistance and tax subsidies con-tained in the proposal would induce 18 million ofthe uninsured in 1996 to purchase health insurance.More than 2 million people who would be eligiblefor Medicaid under current law, however, wouldhave their health insurance only partly subsidizedand would choose not to obtain coverage. Another1 million people now covered by small employerswould drop coverage after their employer ceased tocontribute to the cost of their plan. The net increasein health insurance coverage would be 15 millionpeople (see Table 3-1). Most of the increase incoverage-11 million people—would occur for peo-ple in poor families, whose purchase of insurancewould be fully subsidized.

20 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
The proposal would leave 24 million peopleuninsured. About 4 million poor people are as-sumed not to participate in the program despite theavailability of a full subsidy—a rate similar to thatfor other public benefit programs. In addition, thecost of insurance would continue to deter some 16million people with family incomes between 100percent and 300 percent of the poverty level fromparticipating. For nonelderly people with incomesover 300 percent of poverty, the rate of coveragewould exceed 96 percent. In all, the proportion of
the population without coverage would drop froman estimated 15 percent in 1995 to 9 percent in1996 and remain roughly the same thereafter.
Insurance coverage would be similar with boththe comprehensive and the limited benefit packages.Although the premiums for the limited packagewould be 20 percent lower than for the comprehen-sive package, the benefits would be 20 percent less,and the effective price of insurance would be littlechanged.
Table 3-1.Health Insurance Coverage Under the Managed Competition Act (By calendar year, in millions of people)
1996 1997 1998 1999 2000 2001 2002 2003 2004
Baseline
Insured 222 224 226 228 229 230 232 233 234Uninsured 39 40 40 40 41 42 43 43 44
Total 261 264 266 268 270 272 274 276 278
Uninsured as Percentage of Total 15 15 15 15 15 15 16 16 16
Alternative 1: Comprehensive Benefit Package
Insured 237 239 242 243 245 247 249 251 253Uninsured 24 24 24 25 25 25 25 26 26
Total 261 264 266 268 270 272 274 276 278
Increase in Insured 15 15 16 16 16 17 17 18 18
Uninsured a s Percentage o f Total 9 9 9 9 9 9 9 9 9
Alternative 2: Limited Benefit Package
InsuredUninsured
Total
Increase in Insured
Uninsured as Percentage of Total
23724
261
15
9
24024
264
16
9
24224
266
16
9
24424
268
16
9
24625
270
16
9
24725
272
17
9
24925
274
18
9
25125
276
18
9
25325
278
19
9
SOURCE: Congressional Budget Office.
NOTE: The estimates assume full funding of the subsidies.

CHAPTER THREE FINANCIAL IMPACT OF THE PROPOSAL 21
Table 3-2.Projections of National Health Expenditures Under the Managed Competition Act(By calendar year, in billions of dollars)
1996 1997 1998 1999 2000 2001 2002 2003 2004
Baseline
Total 1,163 1,263 1,372 1,488 1,613 1,748 1,894 2,052 2,220
Alternative 1: Comprehensive Benefit Package
1,196 1,288 1,392 1,495 1,610 1,750 1,888 2,035 2,190
33 25 20 7 -3 2 -6 -17 -30
Alternative 2: Limited Benefit Package
1,178 1,271 1,375 1,480 1,597 1,726 1,865 2,013 2,171
15 8 4 - 8 - 1 6 - 2 3 -30 -39 -50
Total
Change from Baseline
Total
Change from Baseline
SOURCE: Congressional Budget Office.
NOTE: The estimates assume full funding of the subsidies.
National Health Expenditures
The proposal would make health insurance availableto a much larger group than is currently covered,which would initially increase national health ex-penditures. The estimate assumes that the newlyinsured would increase their use of covered healthservices by 57 percent.5 It also assumes that thecomprehensive benefit package would initially beabout 5 percent more expensive than the averagebenefit of privately insured people in the baseline.In 1996, the increase in national health expenditureswould amount to some $30 billion for the compre-hensive benefit package and half that amount for thelimited benefit package (see Table 3-2).
The institution of managed competition, theshift to HMOs, and the cuts in Medicare wouldslow the growth of health spending and would even-
5. CBO, "Behavioral Assumptions," p. 21.
tually bring national health expenditures below thebaseline. With the comprehensive benefit package,CBO projects that total spending on health in 2004would be $30 billion below what it would be if cur-rent policies and trends continued. With the limitedbenefit package, health spending in 2004 would be$50 billion—or 2 percent—below the baseline.
How the Proposal WouldAffect the Budget
The Managed Competition Act would create a pro-gram of federal subsidies to help low-income peoplepurchase health insurance and meet its cost-sharingrequirements. It would also allow taxpayers to de-duct in full spending for health insurance premiums(up to the reference premium rate) from income fortax purposes. These new federal costs would be fi-nanced primarily by repealing Medicaid and achiev-ing savings in Medicare. In addition, by reducing

22 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
Table 3-3.Estimated Budgetary Effects of the Managed Competition Act (By fiscal year, in billions of dollars)
1996 1997 1998 1999 2000 2001 2002 2003 2004
Alternative 1:
Premium AssistanceNon-MedicareMedicare
SubtotalCost-Sharing Assistance'
Non-MedicareMedicare
SubtotalRepeal of MedicaidMedicare SavingsAssistance for Long-Term CareMedical EducationPostal Service RetirementFederal Administrative CostsOther Spending
Total, Outlays
683
71
299
38-81-11a
-28
_b
35
Comprehensive
Outlays
974
101
411556
-121-613
-210_L
42
1055
109
451761
-135-913
-310_b
38
Benefit
1135
118
481867
-151-13
b3
-311_b
32
Package
1225
127
522072
-168-17
03
-311_b
26
1346
139
572380
-186-18
03
-311_b
26
1456
151
622587
-206-19
03
-312_b
24
1576
163
672894
-227-21
03
-312_b
21
1686
175
7131
102-250-23
03
-312_b
16
RevenuesDeduction of Health
Insurance PremiumsIncrease in Medicare Premium
for High-Income IndividualsIncome and Payroll Taxes
on Additional IncomeAssessment for Medical EducationExcise Tax and Other
Total, Revenues
Deficit with Full Amount of SubsidiesShortfall in SubsidiesNet Deficit Effect
-6
1
34
_b
1
35-30
5
-15
1
55
^1
-4
46-42
4
-16
2
55
_b
-4
Deficit
42-38
4
-17
2
66jl
-4
36-33
3
-18
2
66
_!
-4
30-28
3
-20
3
67
^1
-6
32-39-8
-23
4
67
_j[
-7
31-50-19
-24
5
68
_J.
-6
27-59-32
-25
7
69
_J.
-6
22-68-46
SOURCES: Congressional Budget Office; Joint Committee on Taxation.
NOTES: The figures in the table include changes in authorizations of appropriations and in Social Security that would not be counted for pay-as-you-go scoring under the Budget Enforcement Act of 1990. The table excludes the effects of sections 1421 and 1422, whichrelate to rural emergency access care hospitals.

CHAPTER THREE FINANCIAL IMPACT OF THE PROPOSAL 23
Table 3-3.Continued
1996 1997 1998 1999 2000 2001 2002 2003 2004
Alternative 2: Limited Benefit Package
OutlaysPremium Assistance
Non-MedicareMedicare
SubtotalCost-Sharing Assistance*
Non-MedicareMedicare
SubtotalRepeal of MedicaidMedicare SavingsAssistance for Long-Term CareMedical EducationPostal Service RetirementFederal Administrative CostsOther Spending
Total, Outlays
543
57
309
39-81-11a
-28
_b
22
774
81
421557
-121-613
-210_L
23
835
88
451762
-135-913
-310_b
17
905
95
491167
-151-13
b3
-311_b
10
975
102
532073
-168-17
03
-311_b
2
1056
111
572380
-186-18
03
-311_b
-3
1136
119
612587
-206-19
03
-312_b
-8
1226
128
662894
-227-21
03
-312_b
-14
1316
138
7131
102-250-23
03
-312_b
-21
RevenuesDeduction of Health
Insurance PremiumsIncrease in Medicare Premium
for High-Income IndividualsIncome and Payroll Taxes
on Additional IncomeAssessment for Medical EducationExcise Tax and Other
Total, Revenues
Deficit with Full Amount of SubsidiesShortfall in SubsidiesNet Deficit Effect
-3
1
53
_3
8
14-86
-7
1
74
_5
10
14-85
-8
2
74
_6
11
Deficit
6-15
-9
2
85
_7
12
-30
-3
-9
2
85
_7
14
-110
-11
-11
3
85
_7
13
-160
-16
-13
4
86
_8
13
-210
-21
-13
5
86
_8
15
-29-1
-31
-14
7
97
_9
17
-39-6
-45
a. Includes wraparound benefit.
b. Less than $500 million.

24 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
the growth of health spending, the proposal wouldreduce spending by employers for health insurance,raise earnings or other taxable income by a similaramount, and increase collection of income and pay-roll taxes. With the limited benefit package, thesavings in the proposal would nearly equal its costsin the early years, and the savings would exceed thecosts in 1999 and beyond. With the comprehensivebenefit package, however, the savings would fall farshort of covering the costs, and the proposal wouldrequire scaling back premium subsidies for the non-Medicare population by amounts ranging up to 45percent.
Budgetary Treatment
The Managed Competition Act raises no knotty is-sues of budgetary treatment or classification. Un-like the Administration's health proposal, the Man-aged Competition Act would create no universalfederal entitlement to health insurance. Participationwould be voluntary. Also, unlike the health alli-ances in the Administration's plan, the HPPCswould have no authority to assess mandatory premi-ums. Therefore, although the HPPCs would be es-tablished under the terms of a federal statute, theywould not exercise sovereign power, and their trans-actions should not be included in the accounts ofthe federal government. The budget would include,however, the taxes and spending items that wouldflow through the Treasury—for example, premiumand cost-sharing assistance, federal administrativecosts, and the changes to existing programs. De-pending on how the system was structured, the re-distribution of shortfalls in subsidies might also beconsidered a federal activity.
Subsidies
By far the largest cost of the proposal would be thepremium and cost-sharing assistance for low-incomepeople. Under the proposal, nonelderly personswith incomes up to 200 percent of the poverty levelwould be eligible for both types of subsidy. ForMedicare beneficiaries, the premium assistancewould extend to 120 percent of poverty, and cost-sharing subsidies would be provided to those withincomes below 100 percent of the poverty level.
CBO based its estimate of subsidies for non-elderly people on the March 1993 Current Popula-tion Survey. Using data from the CPS and the rulesspecified in the proposal, CBO assigned people toinsurance units and categorized these units accord-ing to their premium class, demographic characteris-tics, and income bracket. The estimated amount ofpremium assistance for each category of unit de-pends on the reference premium for the class, thenumber of units, their average income, and theestimated rate of purchase of health insurance.Cost-sharing subsidies were assumed to equal 21percent of the premium for the standard benefitpackage—a figure derived from the 1987 NationalMedical Expenditure Survey. The wraparoundbenefit was assumed to cost 9 percent of the stan-dard premium. The estimated premium and cost-sharing assistance for Medicare beneficiaries arebased on data for 1990 from the Health Care Fi-nancing Administration's Continuous MedicareHistory Sample.
With the comprehensive benefit package, pre-mium assistance would total $101 billion in fiscalyear 1997-the first full year of the proposal-and$175 billion in 2004 (see Table 3-3). Cost-sharingassistance (including both cost-sharing subsidies andthe wraparound benefit) would grow from $56 bil-lion to $102 billion over the same period. Over 60percent of families insured through HPPCs andabout 20 percent of families insured through otherAHPs would receive some subsidy.
Premium assistance would be about 20 percentsmaller with the limited benefit package than withthe comprehensive one, but cost-sharing assistancewould be about the same. To make the proposalroughly deficit neutral, the estimate eliminates cost-sharing subsidies for people with incomes above thepoverty level. The additional cost of the wrap-around benefit for people in poverty, however,would use up the savings generated by this change,so the total amount of cost-sharing assistance wouldbe roughly the same for the two alternatives.
Other Outlays
The federal government would incur significantadministrative costs to determine eligibility for

CHAPTER THREE FINANCIAL IMPACT OF THE PROPOSAL 25
premium and cost-sharing assistance and to overseethe AHPs and HPPCs. In its first year of full oper-ation, the Health Care Standards Commission wouldobligate almost $10 billion and have outlays ofmore than $8 billion. Processing applications forsubsidies would require $8.6 billion, assuming 43million applications for assistance at a cost of $200per application. By comparison, it currently costsabout $160 to process an elderly person's claim forSupplemental Security Income and $620 to processan application for Aid to Families with DependentChildren. The commission's other activities, pri-marily oversight of the health plans and HPPCs,would cost another $1 billion.
Repeal of Medicaid would provide most of thefunding for the proposal, totaling $121 billion in1997 and $250 billion in 2004. In addition, theproposal would cut Medicare spending, primarily byslowing the growth of payments to hospitals andphysicians, phasing out payments to disproportion-ate share hospitals, and changing the method ofpaying for medical education. CBO's estimates ofthe savings from these changes are consistent withthe baseline projections of spending for the affecteditems.
The proposal would also make several smallerchanges in federal spending. It would establish atemporary program of assistance for states thatspend a very large share of their Medicaid funds onlong-term care, create a new system for financingmedical education, require the Postal Service toprefund health benefits for retirees, and expandseveral public health programs.
Revenues
The Joint Committee on Taxation (JCT) has esti-mated the impact of the provisions of the proposalthat would affect income and payroll taxes. Themajor revenue-losing item is allowing full deduct-ibility of health insurance premiums (up to thereference premium rate) from income for tax pur-poses. The revenue loss would reach $25 billion in2004 with the comprehensive benefit package, butonly $14 billion with the limited benefit packagebecause the maximum allowable deduction wouldbe less.
For the comprehensive benefit package, CBOand JCT assume that firms would largely avoidpaying the 35 percent excise tax on excess healthinsurance premiums by limiting their contributionsto the reference premium amount and returning theexcess to workers primarily in the form of higherwages. Federal revenues would then rise becausemore compensation would be subject to both per-sonal income and payroll taxation. If the commis-sion adopted the limited benefit package, the tax capwould be lower, but many employees would want toobtain supplementary health insurance coverage. Inthis case, as explained in Chapter 2, workers couldfind it advantageous to have their employer pay fortheir supplementary policy—and pay the excise tax--rather than to receive that portion of their compen-sation as taxable earnings. Not all employers wouldtake this tack, however, and the increase in incomeand payroll taxes would be slightly higher as aresult of the lower tax cap.
Two other provisions of the proposal would alsoincrease federal revenues. High-income individualswould be subject to an increase in their premiumsfor Medicare's Supplementary Medical Insurance.Also, each accountable health plan would be subjectto an assessment of 1 percent of gross premiumreceipts to finance medical residency training.
Shortfall in Subsidies
The proposal would create a process to scale backpremium assistance for low-income people notreceiving Medicare if the proposed savings failed tocover the additional costs. With the comprehensivebenefit package, the shortfall in subsidies wouldamount to about $35 billion a year over the firstfive years. The required reduction in premiumassistance for the non-Medicare population wouldrange from almost 45 percent in 1996 to 23 percentin 2000. With the limited benefit package, theshortfall would amount to 15 percent in 1996, 10percent in 1997, and little or nothing thereafter.
Despite the provision for limiting the amount ofpremium assistance, the proposal would add slightlyto the deficit in the first few years, largely becausethe formula for computing the shortfall excludesfederal administrative costs. With the limited bene-

26 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
fit package, the proposal would reduce the deficit in of gross domestic product, even though the actuallater years. The proposal could also reduce the savings would increase at a more rapid rate. If alldeficit with the comprehensive benefit, but only the savings were made available to fund the subsi-because after 1999 it would not permit all the dies, there would be no net deficit reduction, andspending reductions to be counted against the cost the shortfall in funding the subsidies would beof the subsidies. It would limit the growth of the smaller,countable savings in spending to the rate of growth

Chapter Four
The Economic Effects ofthe Managed Competition Act
L ike the current system, the Managed Com-petition Act of 1993 would not require thatemployers purchase insurance for their
employees, nor would it mandate that individualspurchase insurance on their own. Nevertheless, theproposal would affect the economy because of thechanges it would make to the cost-effectiveness andaffordability of the nation's health insurance system.Since most people currently receive insurancethrough their employer, changes in the financing ofthat insurance would inevitably affect the nation'sjob market.
The Effect of InsuranceReforms on the LaborMarket
without insurance typically receive roughly one-third less health care than fully insured people whoare otherwise similar.1 Moreover, many familiescan afford insurance only by having someone in thefamily work at a company that offers it. Over thepast decade, soaring premiums have made individ-ual policies for nonworkers prohibitively expensive,especially for those with significant health problemsor risk factors.2 As a result, some people have hadto work just because they need insurance.
The proposal would change this situation byguaranteeing universal access to insurance coverage.Because fear of becoming uninsured would no lon-ger be a significant factor in decisions about work,some people would stop working. Some olderworkers, for instance, might seek an early retire-ment; others might choose to devote more of theirenergies to raising their families.
The proposal would significantly alter the nation'sinsurance markets in several ways that would affectthe functioning of labor markets. Health insuranceconsiderations would be less likely to lock workersinto their current jobs. As a result, workers wouldbe more likely to choose the jobs in which theywould be the most productive and from which theywould derive the most satisfaction.
People Would No Longer Haveto Work Just for the Insurance
Given the high cost of care in the current system,timely and complete access to modern medicinedepends in large part on having insurance. People
Fewer People Would Be Lockedinto Their Jobs
The proposal would also reduce a related problemwith the current system: job lock. Currently, somepeople may be reluctant to leave the safety of alarge corporation to work in a small company, starta small business, or even change jobs because they
Congressional Budget Office, "Behavioral Assumptions for Esti-mating the Effects of Health Care Proposals," CBO Memorandum(November 1993).
The majority of the uninsured work full time at firms that do notoffer insurance; see Congressional Budget Office, Economic Impli-cations of Rising Health Care Costs (October 1992).

28 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
fear losing their health insurance or being deniedcoverage for a preexisting health condition.
The proposal would reduce these concerns.Insurance would always be available at a reasonableprice because all workers would be able to purchasecoverage at no more than the reference premium—that is, the cost of the least expensive plan in theirarea with more than a minimum number of enroll-ees. Moreover, the proposal would prohibit insurersfrom denying insurance to people with preexistingconditions, although health plans would be permit-ted to exclude coverage (except for services tonewborns and pregnant women) of most preexistingconditions for six months after enrollment. Thosefeatures of the proposal would reduce distortionscreated by the current health system in the decisionsof workers about where to work.
The quantitative importance of job lock, how-ever, in reducing economic efficiency in the currentsystem is unclear. Public opinion surveys suggestthat 10 percent to 30 percent of people feel lockedinto their current jobs because they fear losinghealth insurance.3 But statistical studies of the ex-tent to which this fear actually reduces job mobilityhave reached mixed conclusions.4 Overall, the evi-dence suggests that job lock probably hinders theoperation of the labor market to some degree, butthe magnitude of that effect is uncertain.
Benefits of Subsidies toLow-Income People
The proposal would significantly improve the well-being of the poor and near-poor by subsidizing theirpurchase of health insurance. It would significantly
3. Erik Eckholm, "Health Benefits Found to Deter Switches in Jobs,"The New York Times, September 26, 1991, p. 1; ChristopherConte, "Labor Letter," The Wall Street Journal, June 15, 1993,p. Al.
4. Douglas Holtz-Eakin, "Job-Lock: An Impediment to LaborMobility?" Jerome Levy Economics Institute of Bard College Pub-lic Policy Brief, vol. 10 (1993); Brigitte Madrian, "Employment-Based Health Insurance and Job Mobility: Is There Evidence ofJob Lock?" Working Paper 4476 (National Bureau of EconomicResearch, Cambridge, Mass., September 1993).
Table 4-1.Projected Poverty Guidelines, U.S. Average,by Family Type, 1995 (In dollars)
Number ofFamily Members8
12345678b
100 Percentof Poverty
7,52010,08012,64015,20017,76020,32022,88025,440
200 Percentof Poverty
15,04020,16025,28030,40035,52040,64045,76050,880
SOURCE: Congressional Budget Office.
NOTE: The U.S. average excludes Hawaii and Alaska.
a. Includes adults.
b. For families with more than eight members, the poverty levelincreases by $2,560 for each additional member.
reduce the number of poor people who were unin-sured and could slightly reduce the tendency of thecurrent system to lock people into welfare.
Factors That Would Reducethe Average Cost of Insurancefor Low-Income People
The proposal would provide free insurance to every-one whose family income was below the povertylevel and who chose a health plan that cost no morethan the reference plan.5 Subsidies would also beavailable to people under 65 with family incomesbetween 100 percent and 200 percent of poverty,although they would be phased out over this incomerange (see Table 4-1 for poverty levels). In addi-tion, families with incomes less than 200 percent ofthe poverty level would receive assistance in payingthe cost-sharing requirements of their health plan.
5. In addition, those with incomes below 200 percent of povertywould be able to purchase plans that were more expensive thanthe reference plan for only a fraction of the additional cost.

CHAPTER FOUR THE ECONOMIC EFFECTS OF THE MANAGED COMPETITION ACT 29
Those with incomes below poverty would also re-ceive help in purchasing certain services and itemsthat were not covered by the standard benefit pack-age—the so-called wraparound benefits.
A considerable fraction of the population wouldbe eligible for some subsidy. For example, in 1993roughly 46 million people under 65 had family in-comes below poverty, and 84 million people-almost40 percent of the nonaged population—had incomesbelow 200 percent of poverty.
The proposal could make insurance somewhatmore affordable in other ways-and not just for peo-ple with low incomes. The health plan purchasingcooperatives (HPPCs) would reduce administrativecosts of insurance available to small employers andindividuals by creating large insurance pools, andseveral features of the plan would strengthen com-
petition in the health care sector and reduce thegrowth of premiums. For the poorest families, how-ever, the subsidies would be the most important fac-tor in reducing the cost of their insurance.
Effect on Insurance Coverage
Combined with other cost-saving features of theproposal, the subsidies for low-income familieswould significantly reduce the number of uninsuredpoor people (see Table 4-2). The CongressionalBudget Office (CBO) estimates that, if the proposalwere enacted, the total number of uninsured at allincome levels would decline by 15 million—or al-most 40 percent—by 1996. Most of the reductionwould be among uninsured people with incomesbelow the poverty line: their number would drop by11 million.
Table 4-2.The Effect of the Managed Competition Act on the Number of Uninsured,by Income Category, 1996 (In millions of people)
Income Category(As a percentage of the poverty level)
Under CurrentPolicy Under MCA
Decrease in theNumber of Uninsured
Under 100 Percent
100 Percent to 150 Percent
150 Percent to 200 Percent
200 Percent to 300 Percent
300 Percent to 400 Percent
400 Percent to 500 Percent
500 Percent and Above
Total
15
7
5
6
3
1
39
4
6
4
6
2
1
24
11
2
a
1
a
a
15
SOURCE: Congressional Budget Office.
NOTE: MCA = Managed Competition Act of 1993.
a. Less than 500,000.

30 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
By contrast, the number of uninsured between100 percent and 200 percent of poverty would de-cline much less because the cost of insurance formany of these people, even after subsidies, wouldstill amount to a significant expenditure. (For ex-ample, the premium costs, net of subsidies and taxbenefits, for the comprehensive benefit packagewould be about $2,100, or about 9 percent of in-come, for a four-person family with income equal to150 percent of the poverty threshold.) In total, theproposal would leave some 24 million without in-surance in 1996. Reducing the generosity of thebenefit package, as discussed in Chapter 3, wouldhave little effect on the number—and distribution—ofuninsured people.
Effect on Welfare Beneficiaries
The subsidies in the proposal would also reduce anincentive in the current system for beneficiaries ofAid to Families with Dependent Children (AFDC)to remain on welfare. Under current rules, when awelfare beneficiary goes to work and earns incomeabove certain thresholds, the beneficiary loses eligi-bility both for cash assistance and for Medicaid.6
(Children of working mothers, however, remain eli-gible for Medicaid coverage in families with higherincomes, even if the mother loses eligibility for herown coverage.) Unless such workers find employ-ment at a firm that offers insurance, they lose someaccess to affordable health benefits. Moreover,even if their firm offers insurance, employers passthe cost of that insurance to workers in the form oflower wages. In both cases, welfare beneficiarieslose the value of free insurance if they take a job.
Under the proposal, by contrast, welfare benefi-ciaries would not risk losing insurance coverage ifthey worked. They would be able to earn up to 100percent of the poverty level—considerably higherthan the income thresholds for AFDC beneficiaries—and still have free insurance with nominal costsharing.
6. Different thresholds apply for AFDC eligibility and Medicaideligibility. Medicaid coverage may be maintained for a transitionperiod of up to 12 months after starting work. Pregnant womencan retain Medicaid coverage at higher income levels.
Empirical evidence suggests that, under currentrules, AFDC and Medicaid have discouraged partici-pation in the labor force, but the evidence is notdirectly applicable to the proposal. Nevertheless,the responses found in the literature suggest that theManaged Competition Act could slightly increasethe participation of AFDC beneficiaries in the laborforce.
Incentives Inherent inthe Subsidy System
The subsidy scheme in the Managed CompetitionAct is designed to encourage low-income people toobtain health insurance. However, it would createcertain other incentives and disincentives that couldaffect employers' willingness to pay for theiremployees' insurance and the work effort of certainlow-income people.
The Subsidy System and Employers'Health Insurance Contributions
Under the proposal, employer-paid health insurancefor low-income workers would be costly to firms,but would have little or no value to poor workers.This situation would occur because the subsidies forpremiums for low-income workers would be re-duced dollar for dollar by the amount that theiremployers contributed to the workers' health insur-ance.
Thus, excluding other considerations, neither theemployer nor its low-income employees would seeany advantage in having the employer pay for thehealth insurance of its low-income workers. If theemployer paid none of the premium, the insurancewould be free for workers whose incomes were ator below the poverty level. By contrast, if theemployer paid some or all of the premium, the costswould be shifted back onto the workers in the formof reduced wages. The loss of the subsidy couldcost each poor worker thousands of dollars. Be-cause of this, AFDC beneficiaries and other low-income workers eligible for subsidies would have astrong incentive to work for employers that did not

CHAPTER FOUR THE ECONOMIC EFFECTS OF THE MANAGED COMPETITION ACT 31
contribute to insurance and instead paid higherwages.
This incentive could create a number of re-sponses among low-income workers and firms.First, firms could "outsource" or contract out theirlow-income jobs. By outsourcing these jobs tocompanies that did not pay for insurance, firmscould reduce their labor costs and the affectedworkers would become eligible to receive full subsi-dies. Second, companies that currently pay forinsurance could stop paying for it, thereby allowinglow-income workers to claim federal subsidies. Thenet cost of insurance for higher-income workers inthese firms would increase, however, because theirinsurance premiums would no longer be excludedfrom the payroll tax. Thus, some high-incomeworkers might seek employment elsewhere.
Both of these responses would be costly anddisruptive to employers and employees. Someworkers would have to find new employers, andsome firms would have to reorganize their produc-tion. This reshuffling would reduce the efficiencyof the economy because labor would be allocatedpartly with regard to the availability of subsidies,and not solely with regard to efficiency and produc-tivity.
A third response is that companies could expandtheir use of certain types of "cafeteria" plans. Incafeteria plans, each employee chooses the desiredmix of cash wages and certain fringe benefits (suchas health insurance, life insurance, and dependentcare assistance programs), subject to some restric-tions. If a low-income worker did not want theemployer to pay for insurance, the worker couldreceive higher wages or a more generous package ofother benefits instead. High-income workers wouldstill have the option of having the employer pay fortheir insurance.
Under the proposal, every firm-even those thatdid not pay any of the premium—would have tooffer insurance to its workers and would be requiredto set up a payroll deduction scheme for them.Given this requirement, the additional administrativecost of establishing a cafeteria plan could be smallrelative to those in the current system.
However, three factors would limit the interestof some employers in establishing a cafeteria plan.First and foremost, companies with more than 100employees could face adverse selection if some oftheir healthiest employees decided not to take theinsurance. As some healthy workers dropped out ofthe insurance pool, the company's insurance premi-ums would rise, causing more people to withdrawfrom the pool.7 Second, some companies mightface resistance to establishing a cafeteria plan if itcaused a redistribution of wage income amongsingle and family workers. (Such a redistributioncould occur, for instance, if firms currently reduceeach worker's wages by the average cost of insur-ance for both single workers and those with fami-lies, instead of reducing each worker's wages by theactual cost of insurance.) Third, some firms mightbe concerned that their cafeteria plans would notmeet certain legal provisions that prohibit discrimi-nation in favor of highly compensated and certain"key" employees, such as officers of the company.For example, cafeteria plans cannot provide morethan 25 percent of their qualified benefits to keyemployees. Although these provisions might notinfluence decisions in a large number of firms, theycould affect some firms' decisions about setting upcafeteria plans.
All of those behavioral responses would in-crease the cost of the subsidy program to the federalgovernment because they would expand the pool ofpeople who would receive subsidies. But the use ofcafeteria plans would probably be the least costly toeconomic efficiency. Cafeteria plans would allowworkers and firms to adjust to the proposal withoutinducing an inefficient reshuffling of workersamong firms in an effort to find employers that pro-vided a better mix of benefits.
Work Disincentives ofthe Subsidy Scheme
Although the subsidies would reduce the averagecost of insurance for low-income people and im-
Adverse selection would not affect decisions to establish a cafete-ria plan for firms with 100 or fewer employees. These companieswould purchase insurance through the HPPC at community-ratedpremiums, which would be unaffected by their employees* deci-sions to take insurance as a fringe benefit.

32 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
prove their circumstances as a result, the subsidysystem would also discourage certain low-incomepeople from working more hours or, in some cases,from working at all. This work disincentive wouldarise from phasing out the subsidies as family in-come rose between 100 percent and 200 percent ofthe poverty guidelines. Workers who earned moremoney within this income range would have to paymore for health insurance, thereby cutting into theincrease in their take-home wage. In essence, phas-ing out the subsidies would implicitly tax theirincome from work.
Once a family's income (net of premium)reached 200 percent or more of poverty, the pro-posal would not affect decisions about work. Andlower-income families—with incomes below thepoverty level—would not be affected by the phase-out either. But for families with incomes between100 percent and 200 percent of poverty, the impactcould be rather large.
Families in this income range already pay—andwill continue to pay under current law—relativelyhigh marginal tax rates on their earnings. For ex-ample, in 1995, some workers in this range willhave to give up more than 45 cents in federal taxesfor each additional dollar of compensation. Thislarge bite reflects the 15 percent federal income taxrate, the 15.3 percent federal payroll tax, and thephaseout of the earned income tax credit (EITC).8
For a husband and wife with two children, thephaseout of the EITC will impose about a 20 per-cent tax on 1995 earned incomes between $11,290and $26,691. In addition, many of these workerspay state and local income taxes and some receivefood stamp benefits that are phased out as incomerises. Both of these factors increase their marginaltax rates even more.
The proposal would further increase the implicitmarginal tax on the incomes of those families earn-ing between 100 percent and 200 percent of pov-erty. Although estimating the precise effects re-
8. Although the employer legally pays half of the federal payroll tax,economic analysis indicates that employers shift these costs toworkers in the form of lower wages. For this reason, the employ-er* s share is counted as a tax on the employee. See CongressionalBudget Office, Economic Implications of Rising Health CareCosts.
quires detailed information that is not available, asimple example can illustrate the economic effectsof the proposal in broad brush. Consider a hypo-thetical two-parent family with two children, withone member of the family working 35 hours perweek for total annual compensation of $24,000 (seeTable 4-3). For such a family, the least expensivehealth plan would cost about $6,650 in 1995, as-suming the comprehensive benefit package de-scribed in Chapter 3.
If the worker worked an additional five hoursper week, his or her total annual compensationwould increase by $3,429. But federal payroll taxwould take an additional $487, and federal incometaxes (before the EITC) would claim another $332.The family would lose $644 of benefits from theearned income tax credit and $968 in low-incomesubsidies for health insurance. (The example as-sumes that the employer does not pay for insur-ance).
The net increase in the family's income fromfive hours more work per week would be only $996per year assuming the premiums associated with thecomprehensive benefit package; federal taxes andincreased insurance premiums would claim about 70percent of the worker's added compensation. Inother words, the marginal return from working theadditional hours would be only about 30 percent ofthe increase in gross compensation—an estimate thatdoes not even include the additional costs of stateand local income taxes.
The marginal tax on work would be smaller ifthe premiums used in the example were those asso-ciated with the limited benefit package described inChapter 3 (see Table 4-4). In that case, the value ofthe full subsidy would be lower and the phaseoutrate would be smaller. Nevertheless, the marginaltax on work would still be high—about 67 percent.
Phaseout rates would vary among workers indifferent types of families because the maximumsubsidy and poverty level would depend on familysize (see Figures 4-1 and 4-2). Nevertheless, thephaseout of these subsidies would impose heftymarginal levies on workers from all types of fami-lies over certain income ranges. The ManagedCompetition Act would increase the implicit mar-

CHAPTER FOUR THE ECONOMIC EFFECTS OF THE MANAGED COMPETITION ACT 33
ginal tax as much as 20 percentage points on theincomes of single workers, 25 percentage points onheads of households, and 30 percentage points onmarried workers if the premiums were those associ-ated with the comprehensive benefit package.Under the premiums of the limited benefit package,the marginal levies would increase from about 15percentage points to 25 percentage points.
Besides the phaseout of subsidies for premiums,the loss of assistance for cost sharing would occurabruptly when a family's income hit 200 percent ofpoverty and it became ineligible for this assistance.For example, in 1995 a married couple with twochildren would lose cost-sharing subsidies worthabout $1,400 under the comprehensive benefit pack-age when its income rose from $30,399 to $30,400,which would be 200 percent of the poverty guide-line for a family of four.
Another "cliff would occur at 100 percent ofpoverty, where workers would lose subsidies for thewraparound benefits. Assuming the comprehensivebenefit package, the loss of wraparound benefitswould cost such a family $600 in 1995 at this cliff.Under the limited benefit package, CBO assumesthat workers would not only lose the wraparoundbenefits at poverty, but also assistance for costsharing. Under this less generous package, thecombined loss of both benefits would be huge-amounting to $2,900 for such a family in 1995. (Asdiscussed in Chapter 3, the wraparound benefitswould be worth much more under the limited bene-fit package than under the comprehensive one.)These estimates reflect the average amount of assis-tance for cost sharing and wraparound benefits. Buthigh health costs are extremely concentrated amongcertain families. As a result, the majority of eligiblefamilies would receive levels of assistance that wereless than average. Still, even for the median family,the loss of assistance for cost sharing and wrap-around benefits would probably result in a signifi-cant cliff at certain income levels.
Faced with these incentives, some low-incomeworkers could decide that earning additional incomeby working longer hours was not worth the trouble.These incentives could also discourage them from
moonlighting at a second job or working harder attheir existing job in order to secure a raise or apromotion.
Workers could respond in ways that wouldreduce these high marginal levies on work: theycould become uninsured, for instance. (The pro-posal would not mandate insurance.) Certainly,becoming uninsured would increase take-home payand might reduce the disincentive to work, but itwould not eliminate it. As long as workers valuehealth insurance, they would lose a valued benefit(insurance) if they earned more than the povertylevel and took this option. Thus, the subsidieswould improve the well-being of the poor by ex-panding insurance coverage, but the phaseout of thesubsidies would reduce the marginal return fromworking and thereby discourage additional workeffort.
The incentives created by the subsidy systemwould also lead some workers to drop out of thelabor force or not enter in the first place. Althoughmost workers' decisions about participating in thelabor force are generally not sensitive to changes innet returns, one group is relatively responsive:second workers in households in which one personis already employed. These so-called secondaryworkers are more responsive to changes in net re-turns from work because they can rely on theirspouse's income. They will participate in the labormarket when the net returns from work exceed theircosts of working, including the value of the timethat would otherwise be available for leisure orother activities.
The proposal would reduce the willingness ofsecondary workers in some low-income householdsto take a job. If the family's income was between100 percent and 200 percent of the poverty leveland the second worker's income did not raise thefamily's income beyond the 200 percent level, thereward from the second worker's efforts would beonly about 30 percent of the gross compensation ifthe premiums were those for the comprehensivebenefit package, and only slightly higher if thelower premiums for the limited benefit packagewere charged. (Again, this assumes that the

34 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
Table 4-3.Take-Home Pay for Additional Hours of Work:A Comprehensive Standard Benefit Package
Compensationminus
Employer's Share of Payroll Taxequals
Base Wageminus
Net Insurance Cost (After subsidy)8
equalsAdjusted Gross Income
minusPersonal Exemptions and Standard Deduction
equalsTaxable Income
Federal Tax Before Creditminus
Earned Income Tax Creditequals
Net Federal Income Taxplus
Employee's Share of Payroll Taxequals
Total Federal Tax Paid Directly by Employee
Under the Managed
35-HourWork Week
In Dollars
24,000
1,706
22,294
2,157
20,137
16,550
3,587
538
889
-351
1,706
1,355
Competition Act
40-HourWork Week
27,429
1,949
25,479
3,126
22,354
16,550
5,804
871
245
626
1,949
2,575
Change
3,429
244
3,185
968
2,217
0
2,217
332
-644
976
244
1,220
Net Income After Tax and Insurance 18,783 19,779 996
As a Percentage of Additional Wages
Net Income from Working Five Additional Hours n.a.
Marginal Levy on Wages from WorkingFive Additional Hours n.a.
n.a.
n.a.
29
71
SOURCE: Congressional Budget Office.
NOTE: Table assumes a hypothetical two-parent, two-child family in 1995; n.a. = not applicable.
a. Assumes that employers pay nothing for insurance and that the family chooses the least expensive health plan, which would cost $6,641before subsidies.

CHAPTER FOUR THE ECONOMIC EFFECTS OF THE MANAGED COMPETITION ACT 35
Table 4-4.Take-Home Pay for Additional Hours of Work:A Limited Standard Benefit Package Under the
Compensationminus
Employer's Share of Payroll Taxequals
Base Wageminus
Net Insurance Cost (After subsidy)8
equalsAdjusted Gross Income
minusPersonal Exemptions and Standard Deduction
equalsTaxable Income
Federal Tax Before Creditminus
Earned Income Tax Creditequals
Net Federal Income Taxplus
Employee's Share of Payroll Taxequals
Total Federal Tax Paid Directly by Employee
Managed Competition
35-HourWork Week
In Dollars
24,000
1,706
22,294
1,838
20,457
16,550
3,907
586
889
-303
1,706
1,403
Act
40-HourWork Week
27,429
1,949
25,479
2,662
22,817
16,550
6,267
940
245
695
1,949
2,644
Change
3,429
244
3,185
825
2,360
0
2,360
354
-644
998
244
1,242
Net Income After Tax and Insurance 19,054 20,173 1,118
As a Percentage of Additional Wages
Net Income from Working Five Additional Hours n.a.
Marginal Levy on Wages from WorkingFive Additional Hours n.a.
n.a.
n.a.
33
67
SOURCE: Congressional Budget Office.
NOTE: Table assumes a hypothetical two-parent, two-child family in 1995; n.a. = not applicable.
a. Assumes that employers pay nothing for insurance and that the family chooses the least expensive health plan, which would cost $5,313before subsidies.

36 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
Figure 4-1.Effective Marginal Tax Rates on Compensation in 1995: A ComprehensiveStandard Benefit Package Under the Managed Competition Act
too
80
60
40
20
Married Couple with Two ChildrenPercent
-20
: SubsidyPhaseoutRange
Single Parent with One Child
100
80
60
40
20
Percent
-20
SubsidyPhaseout
Range
10,000 20,000 30,000 40,000 10,000 20,000 30,000 40,000
Married Couple with No Children
100
80
60
40
20
Percent
-20
SubsidyPhaseoutRange
10,000 20,000 30,000 40,000
Current Law
SOURCE: Congressional Budget Office.
100
80
60
40
20
Percent
-20
Single Individual
SubsidyPhaseout
Range
0 10,000 20,000 30,000 40,000
Under the Managed Competition Act
NOTE: The effective marginal tax rate includes the individual income tax, the earned income credit, both the employee's and the employer'sshare of the payroll tax, and the phaseout of the premium subsidy in H.R. 3222. It does not include the loss of cost-sharing subsidiesor wraparound benefits.

CHAPTER FOUR THE ECONOMIC EFFECTS OF THE MANAGED COMPETITION ACT 37
Figure 4-2.Effective Marginal Tax Rates on Compensation in 1995: A LimitedStandard Benefit Package Under the Managed Competition Act
100
80
60
40
20
Married Couple with Two ChildrenPercent
-20
: Subsidy' Phaseout
Range
Single Parent with One Child
100
80
60
40
20
Percent
-20
SubsidyPhaseoutRange
10,000 20,000 30,000 40,000 10,000 20,000 30,000 40,000
100
80
60
40
20
Married Couple with No ChildrenPercent
-20
SubsidyPhaseout
Range
10,000 20,000 30,000 40,000
Current Law
SOURCE: Congressional Budget Office.
Single Individual
100
80
60
40
20
Percent
-20
SubsidyPhaseout
Range
0 10,000 20,000 30,000 40,000
Under the Managed Competition Act
NOTE: The effective marginal tax rate includes the individual income tax, the earned income credit, both the employee's and the employer'sshare of the payroll tax, and the phaseout of the premium subsidy in H.R. 3222. It does not include the loss of cost-sharing subsidiesor wraparound benefits.

38 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
worker's employer does not pay for insurance.) Ineither case, the returns from work would be low,and the second earner's net income might not beenough even to cover the costs of transportation andchild care. Moreover, by going to work, the secondearner would lose time that could be spent onhomemaking, childrearing, or other pursuits.
Of course, the work disincentive would besmaller if the second worker's income increased thefamily's income well above 200 percent of poverty.Moreover, if the primary worker earned 200 percentor more of the poverty level, the phaseout of thesubsidies would have no effect on the secondearner's decision to take a job.
Inherent Trade-Offs inDesigning Subsidies
The work disincentives under the Managed Compe-tition Act are an inherent element in all health plansthat target subsidies toward low-income people be-cause those benefits must be phased out as incomerises. Although changing the design of the subsidysystem could reduce the marginal levy on the in-come of low-income people, doing so would intro-duce other problems.
One way to reduce the subsidy phaseout ratewould be to provide a smaller subsidy to peopleearning income at (or below) the poverty level.
With a smaller subsidy to start—something less than100 percent of the premium-less of it would haveto be taken away as income rose. But this changewould make it more difficult for low-income peopleto afford insurance and would undercut one of themajor goals of the proposal. In addition, such achange would do less to reduce Medicaid "lock."As long as Medicaid offered free care-but peoplewho worked had to pay for a significant fraction oftheir care—welfare beneficiaries would face someincentive to stay out of the job market.
A second way to reduce the marginal levywould be to phase out the subsidies over a broaderincome range—in other words, to raise the incomethreshold at which subsidies were terminated to,say, two and one-half or three times the povertylevel. This approach, however, would dramaticallyraise the overall cost of the subsidies, since it wouldgreatly increase the number of eligible families.
Moreover, these additional subsidies would haveto be financed-and that financing could also distortdecisions about work. Inevitably, such a policywould spread the work disincentives to a largerfraction of the population than would be true underthe proposal. Thus, although a slower phaseoutwould significantly improve the work incentives forpeople earning between 100 and 200 percent ofpoverty, it would increase the work disincentives forothers. The net effect of these changes on eco-nomic efficiency is uncertain.

Chapter Five
Other Considerations
T he Managed Competition Act of 1993 pro-poses to restructure the health care systemusing market reforms, competitive forces,
and subsidies for low-income families to expandhealth care coverage and slow the rate of growth ofhealth spending. Changes in the tax system wouldmake people with employment-based coverage moresensitive to its price, as well as provide incentivesfor uninsured people to purchase coverage. Theproposal would not require people to obtain healthinsurance, but under it the number of uninsuredpeople would drop significantly.
To strengthen the demand side of the insurancemarketplace, employees of small firms and peoplewithout ties to the labor force would purchasehealth care coverage through regional health planpurchasing cooperatives (HPPCs), which wouldoffer a choice of accountable health plans (AHPs).All AHPs would provide coverage for a standardpackage of benefits that would be specified by afederal Health Care Standards Commission. Conse-quently, purchasers would base their choices onprice, quality, and convenience. Within the HPPC,a modified form of community rating would prevailthat would ensure that a plan's premiums wouldvary only by type of enrollment (individual, individ-ual and spouse, individual and one child, and indi-vidual and family) and the age of the principalenrollee. All people, regardless of their actuarialrisk status, would be assured that they could obtaincoverage.
All employers would have to offer their employ-ees health insurance coverage through an AHP, butthey would be under no obligation to contribute tothe cost of that coverage. Small employers could
meet this requirement only by contracting with aHPPC. Large employers would have more flexibil-ity; they could self-insure by establishing an AHPfor their employees or purchase coverage in themarketplace from an insurance carrier offeringAHPs, but they would be prohibited from purchas-ing coverage through the HPPC. Large employerswould, however, have to ensure that their employeeswere at no financial disadvantage from being out-side the HPPC; generally, one of the plans that theyoffered would have to provide coverage at a cost totheir employees that was no higher than the refer-ence premium for their area (that is, the premiumfor the lowest-cost plan in the HPPC that enrolled aspecified proportion of the eligible population).
The proposal would terminate the Medicaidprogram and provide federal subsidies to low-income families to enable them to purchase healthcare coverage from plans of their choice, eitherthrough the HPPC or, in the case of low-incomefamilies with a worker employed by a large firm,from their employer. The subsidy program wouldnot be open ended; federal expenditures for subsi-dies would be limited to the savings and increasedreceipts generated by the proposal. Although thefederal liability for subsidies would be effectivelycapped, the Congressional Budget Office (CBO)believes that if the shortfall in subsidies was sub-stantial, the mechanism for limiting the federalsubsidies would seriously disrupt the insurancemarketplace and could render it unworkable.
Even with subsidies for low-income people, thisvoluntary system of health care coverage would stillleave a significant number of people uninsured.Although premiums would be community rated,

40 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
they might still represent a considerable bite (tat ofthe budgets of those low- and moderate-incomefamilies who were eligible for, at most, a partialsubsidy. Nevertheless, proponents of the managedcompetition approach believe that the market systemshould be given an opportunity to work peforemandates on individuals are considered.
As with other proposals that would fundamentally restructure the health care system, estimates ofthe cost and other consequences of the ManagedCompetition Act are highly uncertain. One reasonfor this is that managed competition remains alargely untried system, and there is little analyticalevidence to indicate how effective it might be.Although a few large purchasers of health insurancehave implemented components of the managedcompetition approach, and voluntary purchasingcooperatives exist in some markets, these e tperi-
in aimifi-
ments offer little insight because they operatlarger environment that is unmanaged. The rcations of the proposal are also uncertain bdcauseimportant features—including the standard benefitpackage and many operational details-are not speci-fied and would be left for the Health Care StandardsCommission, the Congress, or later regulations toresolve.
In preparing its cost estimates, therefore, CBOhad to make a number of assumptions about boththe effectiveness of managed competition and theunspecified dimensions of the proposal. Several ofthe underlying assumptions were difficult to developand, together with other uncertainties about theproposal, gave rise to fundamental questions abouthow the system would actually work. This chapterdiscusses several of these issues.
Determining Eligibilityfor Subsidies
As described in Chapter 1, the Managed Coihpeti-tion Act would establish a complex system of subsi-dies that would be a challenge for the Health CareStandards Commission to administer and for benefi-ciaries to cope with. Subsidies for premiums andcost sharing would be available for non-Medicareenrollees with family income below 200 percent of
the poverty level. Medicare beneficiaries with in-come below 120 percent of the poverty level wouldbe eligible for premium subsidies; those with in-come below 100 percent of poverty would also beeligible for cost-sharing subsidies. People withincome below the poverty level would also be enti-tled to federally financed wraparound benefits--services that are now covered by Medicaid butwould not be included in the standard benefit pack-age promulgated by the commission. All thosereceiving Aid to Families with Dependent Children(AFDC) or Supplemental Security Income (SSI)would be eligible for full premium and cost-sharingsubsidies as well as the wraparound benefits, regard-less of whether their family income was below thepoverty line. Although, in principle, the eligibilitycriteria are straightforward, several questions ariseabout the feasibility and possible consequences ofthe system for establishing eligibility.
State-Adjusted Measures of Poverty
The proposal does not adopt the usual approach tomeans-tested programs, which is to employ a na-tional poverty standard. Rather, it would use state-specific measures in an attempt to adjust the eligi-bility criteria for the wide variations in the cost ofliving across the country. The goal of this approachis to target subsidies more effectively toward theneediest people. Although this goal has obviousappeal, it is not clear whether it could be accom-plished. Cost-of-living indices for states do notexist, and the Departments of Labor and Commercewould have to undertake a major statistical effort togenerate reliable indices. Consequently, CBO wasunable to take such adjustments into account in itscost estimates.
Even if reliable indices could be developed,using state-specific measures of poverty could createconsiderable confusion in the many multistate urbanmarkets in which eligibility for a subsidy wouldvary according to the jurisdiction in which one lived(assuming that eligibility was based on one's stateof residence rather than place of employment). Thevariation in eligibility criteria could cause low-income families to cluster in certain border jurisdic-tions. In addition, the commission's job would bemade more difficult if it had to calculate subsidies

CHAPTER FIVE OTHER CONSIDERATIONS 41
based on more than 50 separate poverty levels. Inthe end, switching to state-specific measures mightresult in only modest improvements in the targetingof subsidies, because variation in the cost of livingwithin states could be as great as that betweenstates.
The Eligibility Process and Accessto Care
With the exception of AFDC and SSI beneficiaries,who would automatically be eligible for subsidies,low-income people might find the process of obtain-ing subsidies rather daunting. They would have toapply to a federal agency—the Health Care Stan-dards Commission—submitting proper informationabout their family circumstances, income, employer,and the AHP in which they were enrolled or wishedto enroll. Those receiving subsidies would have toreapply for them each year in October to be eligiblefor subsidies for the following year; if their incomefell during the year, they could apply for largersubsidies at quarterly intervals. If they failed to filean annual income reconciliation statement in April,they would lose their eligibility for future subsidies.
How accessible would this system of subsidiesbe to low-income people, particularly those withlimited education, complex family circumstances,unstable income, and a high degree of residentialmobility? The proposal provides some assistancefor local organizations to help people apply forsubsidies, but the appropriation for these activitieswould be small. State and local governments wouldhave no explicit role in this process, although theyprobably would facilitate enrollment in order toavoid costs they would otherwise incur for uncom-pensated care. If adequate outreach and assistancewere not provided, many low-income families mightremain uninsured and not seek to enroll in healthplans until they needed medical care. Yet many ofthese uninsured people might find that they couldnot enroll in AHPs at the particular time theyneeded care because, unlike enrollment in the Med-icaid program, which is year-round, enrollment inAHPs would be restricted to an annual 30-day open-enrollment period. (Special enrollment periodswould be available for people who experiencedchanges in family or employment status.)
Thus, although the proposal would allow manylow-income families to purchase health insurance ina systematic or planned way, it would also removethe ready—or "as needed"-access to coverage thatMedicaid affords to eligible populations. Thischange could leave the providers of last resort thatserve the low-income population—hospital emer-gency rooms, outpatient departments, and publicclinics—in difficult circumstances. Some could expe-rience an increase in uncompensated care.
The Potential for OverpayingSubsidies
The methods that the proposal specifies for deter-mining eligibility for subsidies and distributingsubsidies to AHPs also raise the possibility thatsubsidies might be misdirected or overpaid. TheHealth Care Standards Commission would establishthe eligibility of individuals and then send premiumand cost-sharing subsidies directly to their chosenplan. Thus, AHPs enrolling low-income peoplewould receive subsidy payments from the federalgovernment with relatively little ongoing federalmonitoring of the process. Verification would beperformed for only a sample of those receivingsubsidies.
The proposal specifies an annual process forreconciling the premium subsidies by comparingactual with expected income using data from the taxsystem, although many of those eligible for subsi-dies would not be required to file tax returns andwould therefore have to file a separate income state-ment with the commission. There would be noreconciliation for the cost-sharing subsidies or thewraparound benefits for low-income people. Appar-ently, AHPs would have no liability for repayingany excess subsidy payments that they might re-ceive.
Because of the constant movement of people inand out of HPPC areas, their changing eligibility forsubsidies, and the fact that some people wouldprobably be dropped from health plans if they didnot pay their share of the premium, it would bedifficult for the commission to avoid misdirectingsome subsidy payments. To minimize the extent ofthat problem, it would need to track the enrollmentand disenrollment records of low-income individu-

42 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
als and their eligibility for subsidies very closely—probably on a quarterly basis. The commissionwould also have to make the subsidy payments thatfrequently; the probability of overpayment wouldincrease considerably if subsidies were paid annu-ally or even semiannually.
The Consequences ofShortfalls in Payments forLow-Income EnrolleesThe complex subsidy mechanism that would becreated by the Managed Competition Act and thecontrols that would be established to ensure that thesubsidies did not add to the federal deficit couldpresent AHPs with shortfalls in payments for low-income enrollees and considerable amounts of un-certainty that could undermine the effective func-tioning of the HPPC marketplace.
Shortfalls in premiums for low-income enrolleescould arise from the limits that the proposal wouldplace on federal subsidies. The annual amountavailable for subsidies would be limited to the sumof any additional revenues generated by the taxchanges in the proposal and the savings from elimi-nating the Medicaid program, reducing spending forMedicare, and prefunding retiree health benefits inthe Postal Service. This pool of resources wouldfinance premium and cost-sharing subsidies, wrap-around benefits for low-income people, transitionassistance for the states (between 1995 and 1998) asthey took over the long-term care portion of theMedicaid program, and other grants and expendi-tures included in the proposal.
The premium subsidies for non-Medicare enroll-ees, however, would be paid only after all of theother required payments had been made; hence,these subsidies would bear the brunt of any short-fall. If the available funding was insufficient, AHPswould have to accept reduced premiums for theirlow-income enrollees. Moreover, even with fullfunding of the subsidies, some AHPs could experi-ence shortfalls in premiums and cost-sharing pay-ments for low-income enrollees.
If shortfalls in payments for low-income enroll-ees occurred-for whatever reason—AHPs would
probably have to raise their premiums for all enroll-ees. Although the proposal includes provisions todistribute the burden of premium and cost-sharingshortfalls across all health plans (including closedAHPs) and across HPPCs, it would be extremelydifficult to develop and implement an accurate andeffective distribution mechanism. Consequently, theapproach to subsidizing the health care coverage oflow-income people—which is an explicit form ofcost shifting—could introduce considerable uncer-tainty and instability into HPPC markets. More-over, if shortfalls were substantial, the amount ofcost shifting that would be necessary to cover themmight be untenable.
Shortfalls in Premiums
In general, AHPs enrolling low-income peoplewould experience shortfalls in premiums if federalsubsidies were not fully funded. In that case,AHPs would be required to cut their premiums forlow-income people and absorb the difference them-selves (see the appendix). Because any subsidywould be inversely related to a family's income-reaching zero for those at 200 percent of the pov-erty level—the corresponding premium shortfallwould decline as income rose above poverty. Evenif the unspecified mechanism for distributing theshortfalls among health plans worked perfectly,AHPs would have to raise premiums for all enroll-ees to cover the average systemwide shortfall. Ifthe distribution mechanism was not perfect, AHPswould have to raise their premiums by differentialamounts to cover their particular shortfalls. Thatresponse could change AHP premium rankingswithin a HPPC, possibly changing which AHP wasthe reference plan (the lowest-cost plan enrolling aspecified proportion of the eligible enrollees).
The only situation in which an AHP might notexperience a shortfall with partial funding of federalsubsidies would be if a low-income person receivedan employer's contribution for the entire premium.Although the proposal is silent on what would hap-pen if an employer contributed more than the maxi-mum premium that an AHP could charge a low-income person, it would be illogical to ask a plan toaccept a lower payment in those circumstances. Ingeneral, however, the primary beneficiary of em-ployers' contributions would be the federal govern-ment, which would reduce its premium subsidy

CHAPTER FIVE OTHER CONSIDERATIONS 43
accordingly. Given that employees "pay" for theiremployers' contributions to health insurance throughlower wages, every dollar from an employer thatsubstituted for a federal subsidy dollar would makelow-income workers worse off.
Even with full funding of the subsidies, AHPswith premiums higher than the reference premiumwould have to lower them for low-income enrollees.The amount of the reduction would be a function ofthe family's income and the degree to which aplan's premium exceeded the reference premium.For example, a poor family participating in ahigher-cost plan would be required to pay only 10percent of the difference between the referencepremium and the plan's actual premium. Therewould be no federal subsidy to cover this shortfallbecause the maximum subsidy could not exceed thereference premium. If, in addition, the federalsubsidies were only partially funded, the plan wouldface a higher premium reduction—reflecting botheffects.
It is not at all clear how many low-incomefamilies would choose to enroll in plans thatcharged more than the reference premium. Muchwould depend on the distribution of premiumsamong AHPs in the HPPC area, the availability andaccessibility of plans that cost no more than thereference premium, the perceived quality of care insuch plans, total out-of-pocket premium costs, andthe additional out-of-pocket premium costs associ-ated with the higher-cost plans. Families with in-come around the poverty level, particularly thosewith health problems, might find the higher-costplans an attractive option because at that level ofincome they would be required to pay little out ofpocket to enroll. By contrast, families with incomein the declining-subsidy range might be discouragedfrom purchasing any insurance (either at the level ofthe reference premium or higher) because of thesubstantial individual obligation they would face.
Shortfalls in Cost-Sharing Subsidies
All AHPs would be required to lower cost-sharingamounts to "nominal" levels for non-Medicare bene-ficiaries with income less than 200 percent of thepoverty level. Under the proposal, plans would
receive cost-sharing subsidies that would not be tiedto the actual health care expenditures of their low-income enrollees. Rather, the cost-sharing subsidieswould be lump-sum payments that would vary onlyby the type of enrollment and the age of the princi-pal enrollee.
These payments would be uniform nationwideand consequently could vary widely as a percentageof total costs in different markets. Some planscould gain and others lose under such an arrange-ment, depending on the utilization patterns of theirenrollees. Moreover, there is no guarantee thatreductions in cost sharing would be fully subsidizedin the aggregate, since the Health Care StandardsCommission would allocate the annual funds forcost sharing in advance based on estimates thatcould be far off the mark, especially in the initialyears of implementation.
The Interplan Reconciliation Process
To ensure that AHPs enrolling large numbers oflow-income people would not be disproportionatelyaffected by shortfalls in subsidies or premiums, allAHPs-including self-insured firms-would be re-quired to participate in a nationwide system thatwould distribute reductions in premiums and costsharing equitably among plans. Developing a na-tional transfer system involving the thousands ofAHPs in the country would be an extremely diffi-cult task, and whether it could be implementedeffectively is doubtful.
The proposal does not spell out the principleson which the transfers would be based. Would, forexample, plans with higher premiums be entitled toreceive larger interplan transfer amounts for subsi-dized enrollees than plans with lower premiums inmarkets with the same reference premium? Cer-tainly, the shortfalls in premiums would be greaterfor the higher-cost plans, but requiring other plansto contribute more in consequence raises the possi-bility that unsubsidized enrollees in low-cost healthplans would have to pay higher premiums to helpsubsidize low-income enrollees in higher-cost plans.
A further complexity for the transfer system isthat reference premiums could vary greatly among

44 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
HPPCs, reflecting differences in input costs, practicepatterns, quality of care, competitiveness of themarketplace, and the efficiency with which healthcare was delivered. Because federal subsidies inany HPPC area would be tied to the reference pre-mium, plans in markets with high reference premi-ums would receive larger subsidies than plans inmarkets with low reference premiums. Questionswould inevitably arise about whether such discrep-ancies could be justified or whether they were un-fair to health plans in highly competitive markets.
Conceptual questions such as these are difficultto address and would be politically charged. Theyalso evoke concerns about equity among individu-als, plans, and geographic areas and may not beappropriate issues for an appointed commission toresolve.
The Effects of Shortfalls onInsurance Markets
The proposal's complex subsidy mechanisms wouldintroduce a good deal of uncertainty and instabilityinto HPPC and non-HPPC insurance markets.AHPs would have to estimate their potential short-falls under a number of circumstances in order toset their premiums. These calculations would beextremely complex because each plan's expectedshortfall would be related to a number of factorsthat would be difficult to predict, including:
o The federal premium subsidy percentage for theyear;
o The relationship of the plan's premium to thereference premium and to the premiums of otherplans in the market;
o The number of low-income families who mightenroll in the plan by type of enrollment, age ofprincipal enrollee, and family income as a per-centage of the poverty level;
o The amount to be received for cost-sharingsubsidies relative to the use of services by eli-gible enrollees;
o The effectiveness of the mechanism for adjust-ing premiums for risk within the HPPC; and
o The amount that the plan might receive throughthe interplan reconciliation process.
The estimating process would have to be adynamic one because a plan's anticipated shortfallwould be related to the level of its premium. Ahigher premium would probably change the relation-ship of the plan's premium to the reference pre-mium, which would itself depend on the final deci-sions made by all the plans. A higher premiumwould also cause some enrollees to drop their cov-erage or switch plans. Those that dropped coveragemight be healthier than average, causing the averagelevel of risk of the plan's enrollees to rise and plac-ing further pressure on premiums. Thus, whensetting premiums, plans would find themselvesdealing with many unknown and interdependentvariables.
Determining premiums would not become lesscomplex or more certain over time. The federalsubsidy percentage could vary from year to year;the reference premium in the HPPC would probablychange annually, as might the plan or plans offeringthat rate; and considerable numbers of people—par-ticularly low-income people—could switch planseach year to minimize their out-of-pocket premiumpayments. In short, the premiums of health plans inHPPCs with a high percentage of low-income en-rollees could be unstable and unpredictable.
In the absence of an effective distribution pro-cess, AHPs might respond in a variety of ways toshortfalls in payments. The responses and theirimpacts would generally be greater within the HPPCthan outside it because low-income people wouldconstitute a much higher proportion of the HPPCpopulation. Once a plan had set its premiums forthe year, it presumably could not change them untilthe following year. Consequently, if the projectionof the shortfall in payments for low-income enroll-ees on which the premium was based turned out tobe too low, a plan could not adjust its premiums tocompensate in the short run. Small shortfalls wouldprobably pose little problem. Large shortfalls, how-ever, might produce various interim responses, such

CHAPTER FIVE OTHER CONSIDERATIONS 45
as lowering payments to providers and reducing thequality or quantity of care provided.
In the longer term, plans faced with significantreductions in payments would almost certainly raisetheir premiums; some might even withdraw fromthe market. If people chose to drop their coveragewhen premiums rose, the consequences would notbe confined to the plans immediately affected.Because enrollment in AHPs would be voluntary,some healthier people might drop out of the HPPCmarket altogether rather than just switch plans. Thisresponse would cause the average risk level of allenrollees in the HPPC to rise, potentially resultingin an upward spiral of premiums in the HPPC.Very large shortfalls in premiums could cause theHPPC system to collapse entirely because theamount that AHPs would have to pass on in higherpremiums would be unacceptable. CBO believesthat to avoid such consequences, the subsidieswould have to be close to or fully funded.
The Tension BetweenCovered Benefits and theProposed System of Subsidies
CBO's analysis suggests that it would not be possi-ble to implement the proposed system of subsidiesin conjunction with a relatively generous benefitpackage, full funding of the federal subsidies, andno increase in the federal budget deficit. The avail-able funding for the proposed subsidy pool wouldbe insufficient.
If the commission established a standard pack-age of benefits that was similar to that required bythe Administration's proposal-which is about 5percent more generous than the average employer-sponsored plan—the annual shortfalls for premiumsubsidies for the non-Medicare population wouldaverage over 30 percent between 1996 and 2000. Ifsuch shortfalls were reflected in reduced premiumsubsidies, they could well jeopardize the orderlyfunctioning of insurance markets. If so, policy-makers would have only three ways to respond.First, they could fund the subsidies by allowing thedeficit to increase. Second, they could approve
additional spending cuts and tax increases to aug-ment the pool of resources available to fund thesubsidies. Finally, they could scale back the pro-gram either by changing the standard benefit pack-age to reduce premiums or by trimming the gener-osity of the subsidies.
This third approach, which may appear to be theobvious response, could be problematic; it providesa good illustration of the problems and difficultiesthat one encounters when modifications are made incomprehensive health proposals. Often, ad hocadjustments designed to reduce costs in one areainteract with other components to raise costs else-where in the proposal. For example, if the com-mission increased the cost-sharing requirements forthe standard benefit package in an effort to reducepremiums and, hence, premium subsidies, it wouldfind that net federal costs would be reduced littlebecause there would be a concomitant increase inthe spending for the cost-sharing subsidies that arepaid for people with income below 200 percent ofpoverty. Alternatively, if the commission tried toreduce premiums by narrowing the range of Servicescovered in the standard benefit package, it wouldsoon discover that much of the savings achievedfrom lower premium and cost-sharing subsidies wasoffset by increased federal costs for the wraparoundbenefits available to people below the poverty level.Thus, under the proposal, lowering federal subsidycosts by reducing premiums is, at best, a "two stepsforward, one step back" process.
In formulating an alternative that permitted fullfunding of subsidies from the pool of resourcesgenerated by the proposal, CBO found that it had toalter the proposal's subsidy structure in addition toscaling back premiums by limiting the benefit pack-age. This route was taken because CBO concluded,after discussions with health insurance actuaries,that the level of premiums consistent with fullyfunding the subsidies using the pool of resourcesspecified in the proposal would be insufficient topurchase what most would regard as a minimallyadequate package of benefits. Accordingly, thepremium constraint was achieved with a fairly Spar-tan benefit package and the elimination of the cost-sharing subsidies called for in the proposal for peo-ple with income between 100 percent and 200 per-cent of the poverty level.

46 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
There would be many ramifications for thehealth care system and the people it serves if cov-ered benefits and subsidies were reduced to thisdegree. More people-mostly in income rangesbetween 100 percent and 200 percent of the povertylevel-might purchase health insurance in responseto lower premiums. But some others might bediscouraged from purchasing because the benefitpackage would be lean and they would have nocost-sharing assistance. (People with income belowpoverty would not be affected at all because theywould make up in wraparound benefits what theylost in standard coverage.) Others who could affordto do so would probably purchase supplementaryinsurance for benefits not covered by the standardpackage; they would generally have to pay for addi-tional coverage out of after-tax income, whichwould enhance their cost-consciousness. The result-ing health care system might provide quite compre-hensive coverage for both poor and relatively well-to-do families, and rather meager benefits for thosewith moderate income.
Effects of the Proposal onEmployers and Employees inCertain Firms
Although employers would only be required tooffer-not to pay for—health insurance coverage fortheir employees, many could find their circum-stances altered considerably under this proposal andnot always for the better. Ultimately, however,those faced with higher costs for health care wouldpass them on to their employees through lowerwages.
Depending on the standard benefit packagespecified by the Health Care Standards Commission,some small firms that currently offer health insur-ance to their employees might face considerablyhigher premiums under the proposed system. If thebenefit package resembled CBO's more comprehen-sive option, voluntary participation and communityrating in the HPPC could cause premiums to besignificantly higher for those firms that currentlyhave healthy employees and low, experience-ratedpremiums. They would also tend to be higher for
firms whose current benefits were less generousthan those in the standard benefit package. Bycontrast, with a less comprehensive benefit package,experience-rated firms with healthy employeesmight face similar or higher premiums for lessgenerous coverage than they currently have. More-over, if AHPs in the HPPC experienced significantshortfalls in premiums and subsidies for low-incomepeople, all small firms might face increases in pre-miums the next year. To the extent that healthierworkers chose to drop their coverage in the face ofrising premiums, adverse risk selection in the HPPCpool would become more severe.
Some large employers—who would have toobtain their plans outside the HPPC-might alsoconsider themselves to be "losers" under the pro-posed system in the short run. In particular, thosethat did not intend to pay for their employees'health care coverage might, nonetheless, find them-selves involuntarily contributing to such coverage.This situation could occur because some large firmsmight not be able to obtain insurance coverage inthe non-HPPC market for a price equal to or belowthe reference premium although they would berequired to offer their employees a plan that was nomore expensive than that amount.1
The firms most likely to be confronting thisproblem would be those just slightly larger than thesize cutoff for mandatory participation in the HPPC(generally 100 employees) that did not contribute tothe cost of their employees' coverage. With manyworkers in these firms choosing coverage through aspouse who worked for a firm that contributed toemployees' insurance costs, the firm's actual insur-ance pool could be well under 100. Such firmsmight face relatively high premiums if they hadeven a few participants in their plan with healthproblems. Thus, although in theory firms wouldonly be required to offer, not to pay for, coverage,some firms might have to make some contributionto satisfy the requirement that the premium be nohigher than the reference premium in the HPPC. In
This provision, which would generally apply for each type ofenrollment and age group of the principal enrollee, would bemodified for closed AHPs that elected to use community ratingacross types of enrollment or HPPC areas.

CHAPTER FIVE OTHER CONSIDERATIONS 47
the end, those payments would be passed on toworkers in the form of lower wages.
Under the circumstances just described, an ineq-uitable anomaly would occur. Although the firmwould be contracting to obtain the cheapest possibleAHP for its workers, the workers would have to paytaxes on a portion of their contributions for healthinsurance. This situation, which would never facean individual who chose the cheapest available planin a HPPC, would arise because the tax-exemptamount of premiums paid by both the employer andenrollee could not exceed the HPPC's reference pre-mium.
Effect of Cost-SharingProvisions and AlternativeBenefit Packages on AHPs ofDifferent Types
Advocates of the managed competition approachassume that one of the consequences of a morecompetitive marketplace would be that more peoplewould enroll in health maintenance organizations(HMOs). Some of the provisions of the proposalwould have major consequences for HMOs andmight affect in unforeseen ways their ability tocompete.
Cost-Sharing Provisions
The basic tenet of the managed competition ap-proach is that all health plans should offer a stan-dard benefit package. Opinions differ, however, onwhether that package should encompass standard-ized cost-sharing amounts. Advocates for standard-izing cost sharing, which is the approach adopted inthe proposal, maintain that such standardization isnecessary if consumers are to be able to comparepremiums among plans and make informed choices.2
2. The proposal actually requires uniform cost sharing for all typesof plans, with one exception. Network plans would be required toimplement higher levels of cost sharing than the standard amountsfor out-of-network use.
Other observers, however, contend that evenunder managed competition, two cost-sharing op-tions—one lower and one higher—should be permit-ted. Their reasoning is that cost sharing plays verydifferent roles in plans of different types. Effectivehealth maintenance organizations, for example, typi-cally have low cost sharing and limit their patients'use of services through careful management. Fee-for-service plans, in contrast, rely on higher costsharing to control utilization, imposing much lessrestrictive management on patients. Consumers un-derstand the alternatives they face when selecting aparticular type of plan: lower out-of-pocket spend-ing and more restrictions on choice in HMOs versushigher out-of-pocket spending and fewer restrictionson choice in fee-for-service plans.
Given the different functions of cost sharing indifferent kinds of plans, proposals that would stan-dardize cost sharing across all plans could have verydisruptive effects on the health care system, at leastfor the first few years. If, for example, the standardbenefit package required cost-sharing amounts forall plans that were similar to those charged byHMOs today, fee-for-service plans might experiencelarge increases in use of services. The only way forthem to compensate for that increased use would beto increase their premiums significantly, whichcould eventually drive them out of the market.
Conversely, if the standardized cost-sharingamounts reflected current fee-for-service patterns,HMOs could find themselves at a competitive disad-vantage, since low cost sharing is the major attrac-tion of HMOs for many of their enrollees. Al-though HMOs could probably lower their premiumsin those circumstances, their ability to do so mightbe limited by the additional administrative costsimposed by the new cost-sharing provisions. More-over, it is unclear how consumers would respond toHMOs with lower premiums and higher cost shar-ing. As a result, the overall effects of the pro-posal's cost-sharing provisions on the market sharesof HMOs and fee-for-service plans are uncertain.
In both of the situations just described, competi-tive forces would drive those plans that could notsurvive out of the market, but the transition to anew market structure could be difficult for healthplans, providers, and patients alike. To avoid some

48 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
of the potentially disruptive consequences of stan-dardized cost sharing, the proposal includes a re-quirement that cost sharing be set so that utilizationrates would not change from their current averagelevel.
Although the appeal of that idea is understand-able, how the cost-sharing requirements would bedetermined in practice and what their effects wouldbe are unclear. Because the majority of the insuredpopulation is still in fee-for-service plans, however,the resulting cost-sharing provisions would probablybe closer to those of current fee-for-service plansthan to those of HMOs. Thus, although all types ofplans would have to adjust to the new cost-sharingstructure, the consequences might be more far-reaching for HMOs. The extent to which theycould regain their competitive position throughlower premiums would depend on the form that theadditional cost sharing took, the effects on adminis-trative costs, and the response of consumers to thenew payment requirements. There appears to be noguarantee that the proposal's provision of a constantrate of utilization would ensure a smooth transitionto a new market structure.
Alternative Benefit Packages
Another important characteristic of HMOs is theirrelatively comprehensive benefits, which generallyemphasize preventive health care. A meager stan-dard benefit package could, therefore, limit theeffective functioning of HMOs. The impact woulddepend on the particular benefits that were or werenot covered and the extent to which people pur-chased supplementary policies for uncovered bene-fits.
From an HMO's perspective, the most seriousdeficit in coverage would probably result fromlimits on preventive health services. Although theless comprehensive package used in CBO's costestimate does not include coverage of those ser-vices, the commission would face tremendous pres-sure to include them. To cover preventive healthcare and not allow the subsidies to rise, however,would require even stiffer reductions elsewhere thatcould erode the typical HMO benefit package inother ways.
Role of the Health CareStandards Commission
The proposal would create a new federal agency,the Health Care Standards Commission, whichwould have major responsibilities for almost everycomponent of the health care system, eclipsing therole of the states and in some cases that of otherfederal agencies. As described in Chapter 1, thoseresponsibilities would be exceptionally broad, rang-ing from setting national program standards to im-plementing nationwide subsidy programs. Could asingle centralized federal agency perform all of thediverse functions of the commission effectively, andcould an appointed body withstand the many politi-cal pressures the commission would face?
The tasks that might be fitting responsibilitiesfor a single centralized agency are those that relateto the design and establishment of the proposed newhealth care system. Examples include specifyingthe benefit package (including the cost-sharingrequirements), developing the factors for adjustingpremiums for risk, setting standards for AHPs andHPPCs, establishing information standards, anddetermining annual federal expenditures for pre-mium and cost-sharing subsidies.3
Yet the decisions made in some of those areaswould affect the future viability of the health caresystem and could be highly controversial and politi-cally sensitive. Designing the benefit package is animportant case in point. Under the proposal, thecommission would basically be faced with aHobson's choice. It would be told the maximumamount that would be available for subsidies andcould design a benefit package that was consistentwith that amount. But to ensure full funding of thesubsidies, the benefit package would have to be solean that it would probably be unacceptable to manypeople. Because the commission would have to ob-
3. Two additional federal boards responsible to the commissionwould assist in some of those activities. The Benefits, Evalua-tions, and Data Standards Board would provide advice on benefits,information standards, and the evaluation of health care services.The Health Plan Standards Board would advise the commission onstandards for AHPs and HPPCs.

CHAPTER FIVE OTHER CONSIDERATIONS 49
tain Congressional and Presidential approval for itsrecommendations, limiting the benefit packagemight be extremely difficult. If it adopted agenerous benefit package, however, the subsidyshortfall could cause major disruptions to the healthcare system.
The commission would also have major respon-sibilities for the day-to-day operations of the healthcare system-activities that it might be less capableof undertaking. The commission's functions wouldinclude monitoring the HPPCs and the reinsurancemarket for health plans, determining the eligibilityof low-income families for premium and cost-shar-ing subsidies, distributing those subsidies to healthplans, and developing and implementing the systemof transfer payments among HPPCs to ensure thatpremium and cost-sharing adjustments for low-income families were distributed equitably. Thecommission would also be required to register andoversee all AHPs in the country, including the plansof self-insured firms. (State certification would notbe a requirement for registration, which raises thepossibility that plans would not have to be licensedin the states in which they operated.)
In addition, the commission would have toensure that states had established satisfactory protec-tions regarding solvency for enrollees in insuredhealth plans and would itself have to establish sol-vency protections for enrollees in other plans. Tobe appropriately responsive to needs and problemsat the local level, a federal agency performing thesefunctions would probably need to have regional,state, and local offices across the country. Theproposal, however, makes no explicit provisions forsuch a structure.
Conclusion
Several features of the Managed Competition Actthat might otherwise produce unintended conse-quences, lengthen the time needed for implementa-tion, or limit the effectiveness of the approach couldbe modified quite simply. One could, for example,allow two alternative cost-sharing structures forAHPs, use a single poverty standard nationwide toset the eligibility criteria for subsidies, and allowlow-income people to establish their eligibility forsubsidies at local offices (possibly using localoffices of the Social Security Administration, orstate and local welfare agencies).
Changing other aspects of the proposal thatmight affect its feasibility could prove more contro-versial because some of them are inherent elementsof the underlying philosophy of the approach. Asdescribed in this chapter, for example, allowingvoluntary enrollment in AHPs and permitting onlythose firms with no more than 100 employees toparticipate in the HPPC would have the potential toproduce unstable premiums, especially if federalsubsidies were not fully funded. Moreover, withoutadditional revenues or spending cuts, deficit neutral-ity would be difficult to reconcile with a compre-hensive benefit package and full funding of thesubsidies.
These problems present difficult choices andtrade-offs. The most immediate question, however,concerns the issues that should be resolved now aspart of the proposal versus those that should be leftto the commission, other government agencies, orthe Congress to decide in the future.


Appendix
Illustrative Effects of Shortfalls inFederal Subsidies and Premiums
Under the Managed Competition Act
T he examples in this appendix illustrate sev-eral important characteristics of the Man-aged Competition Act's premium subsidy
system. First, if the federal subsidies were not fullyfunded, premium shortfalls could be substantial foraccountable health plans (AHPs) charging the refer-ence premium as well as for higher-cost plans.Second, AHPs charging more than the referencepremium could experience significant shortfalls ifthey attracted large numbers of low-income enroll-ees—regardless of whether the subsidies were fullyfunded. Third, poor families would face rathersmall out-of-pocket costs if they chose to enroll inhigher-cost plans. Finally, the cost of insurancecould be substantial for those with income between100 percent and 200 percent of the poverty level—the income range in which the subsidies would bephased out.
The effects of a shortfall in federal subsidies areillustrated in Table A-l for an AHP charging thereference premium (assumed to be $2,300 for anindividual). Case 1, the simplest situation, assumesthat the subsidies are fully funded and that individu-als receive no contributions from employers. Be-cause the plan charges the reference premium, it isallowed to charge low-income people the fullamount. Individuals with income up to 100 percentof the poverty level receive full subsidies. Forindividuals with income above the poverty level, thesubsidy falls 1 percentage point for every percent-age point that their income exceeds the povertylevel, reaching zero at 200 percent of the povertylevel.
In Case 2, which assumes a federal subsidypercentage of only 70 percent, the amount that planscan charge all low-income people drops, with thereduction being proportional to the amount of theoriginal federal subsidy. In other words, the reduc-tion in the total premium paid to the plan is 30percent of the full subsidy at each level of income.The enrollee's payment remains the same, and theplan absorbs the shortfall.
Cases 3 and 4 show the effects of contributionsfrom employers, which are assumed to be 80 per-cent of the reference premium. In both cases, thefederal subsidy drops dramatically. In Case 3,which assumes that the subsidies are fully funded,the subsidy becomes zero for individuals with in-come at 120 percent of the poverty level. Withpartial funding of the subsidies, the subsidy be-comes zero at a lower level of income. In the par-ticular example shown in Case 4, which assumes afederal subsidy percentage of 70 percent and anemployer's contribution of 80 percent of the refer-ence premium, there is no subsidy at any incomelevel. (Case 4 also assumes that plans can acceptall of an employer's contribution, so that the short-fall in premiums is reduced for low-income enroll-ees up to the income level at which that contribu-tion equals the premium the plan can charge-whichis at 133 percent of the poverty threshold in thisexample.)
Under the proposal, plans charging more thanthe reference premium would have to lower theirpremiums for low-income people, regardless of

52 AN ANALYSIS OF THE MANAGED COMPETITION ACT April 1994
Table A-1.Shortfalls in Federal Subsidies for an AHP Charging the Reference Premium (In dollars)
Payment (By income, as a percentage of the poverty level)
Actual PremiumPremium AHP Could ChargeEmployer's PaymentFederal Subsidy PaymentEnrollee's PaymentPremium Shortfall
Actual PremiumPremium AHP Could ChargeEmployer's PaymentFederal Subsidy PaymentEnrollee's PaymentPremium Shortfall
Actual PremiumPremium AHP Could ChargeEmployer's PaymentFederal Subsidy PaymentEnrollee's PaymentPremium Shortfall
Actual PremiumPremium AHP Could ChargeEmployer's PaymentFederal Subsidy PaymentEnrollee's PaymentPremium Shortfall
100 120
Case 1: Federal Subsidy Percentage = 100Employer's Contribution = 0
2,300 2,3002,300 2,300
0 02,300 1,840
0 4600 0
Case 2: Federal Subsidy Percentage = 70Employer's Contribution = 0
2,300 2,3001,610 1,748
0 01,610 1,288
0 460690 552
Case 3: Federal Subsidy Percentage = 100Employer's Contribution = 0.8 x 2,300 = 1,840
2,300 2,3002,300 2,3001,840 1,840
460 00 4600 0
Case 4: Federal Subsidy Percentage = 70Employer's Contribution = 0.8 x 2,300 = 1 ,840
2,300 2,3001,610 1,7481,840" 1,840s
0 00 0
460 a 460 a
150
2,3002,300
01,1501.150
0
2,3001,955
0805
1.150345
2,3002,3001,840
0460
0
2,3001,9551,840
0115345
175
2,3002,300
0575
1.7250
2,3002,128
0403
1.725173
2,3002,3001,840
0460
0
2,3002,1281,840
0288173
SOURCE: Congressional Budget Office.
NOTES: The reference premium is assumed to be $2,300 for a single individual.
AHP = accountable health plan.
a. The proposal does not address the situation in which an employer's contribution is greater than the amount that the AHP is allowed tocharge. In this example, CBO assumes that the employer pays, and the plan can keep, the employer's full contribution.

APPENDIX ILLUSTRATIVE EFFECTS OF SHORTFALLS IN FEDERAL SUBSIDIES AND PREMIUMS 53
whether the subsidies were fully funded. The ef- In Case 2, the premium shortfalls are the result offects of this provision are shown in Table A-2 for a the combined effects of a 70 percent federal subsidyplan charging $2,500 for an individual policy with a and the plan's premium being above the referencereference premium of $2,300. In Case 1, which premium. Consequently, in this example, whichassumes full funding of the subsidies, the shortfall assumes no contributions from employers, the short-in premiums reflects only the consequences of the falls in Case 2 are more than four times as large asplan's premium being above the reference premium. the shortfalls in Case 1.
Table A-2.Shortfalls in Premiums and Federal Subsidies for an AHP Charging More Than the Reference Premium
Payment (By income, as a percentage of the poverty level)100 120 150 175
Case 1: Federal Subsidy Percentage = 100Employer's Contribution = 0
Actual Premium 2,500 2,500Premium AHP Could Charge 2,320 2,340Employer's Payment 0 0Federal Subsidy Payment 2,300 1,840Enrollee's Payment 20 500Premium Shortfall 180 160
Case 2: Federal Subsidy Percentage = 70Employer's Contribution = 0
Actual PremiumPremium AHP Could ChargeEmployer's PaymentFederal Subsidy PaymentEnrollee's PaymentPremium Shortfall
2,5001,630
01,610
20870
2,5001,788
01,288
500712
2,5002,055
0805
1.250445
2,5002,278
0403
1.875223
SOURCE: Congressional Budget Office.
NOTES: The reference premium is assumed to be $2,300 for a single individual; the actual premium is assumed to be $2,500.
AHP = accountable health plan.
# TJ.S. GOVERNMENT PRINTING OFFICE: 1994 - 301-967 - 814/17258



CONGRESSIONALBUDGET OFFICESecond and D Streets, S.W.
Washington, D.C. 20515
OFFICIAL BUSINESS
PENALTY FOR PRIVATE USE, $300
POSTAGE & FEES PAIDC.B.O.
WASHINGTON, D.C.PERMIT No. G-70