Embed Size (px)
Citation preview

Rural PsychiatrySpecial Issues and Models of Service Delivery
Fiona Judd,1,2 Caitlin Fraser,1 Margaret Grigg,1,3 Joseph Scopelliti,1,2 Gene Hodgins,1,4
Adrian Donoghue1,4 and John Humphreys5
1 Centre For Rural Mental Health, Bendigo Health Care Group, Bendigo, Victoria, Australia2 School of Psychiatry, Psychology and Psychological Medicine, Monash University, Victoria, Australia3 School of Health and Environment, LaTrobe University, Bendigo, Victoria, Australia4 Department of Psychology, University of Melbourne, Melbourne, Victoria, Australia5 School of Rural Health, Monash University, Victoria, Australia
Contents
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7711. Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7722. Characteristics of the Rural Location and Community . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 772
2.1 Cultural Characteristics of Rural Communities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7723. Demands Upon, and Availability of, Mental Health Clinicians . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7744. The Changing Role and Focus of Mental Health Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 775
4.1 Community-Based Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7754.2 A Broadening of the Aim of Mental Health Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7764.3 Evidence-Based Medicine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 776
5. Models of Mental Health Service Delivery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7776. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 778
Abstract The commonly occurring psychiatric disorders, anxiety and depression, have a combined community prev-alence rate of 15–30% and are associated with significant clinical and economic cost. Although a number ofeffective pharmacological and psychological treatments are available for the management of these disorders,many people do not have access to, or do not receive, these treatments. An important factor associated with thelower rates of use of specialist services is rural, particularly remote, residence.
This review discusses the problems of delivery of services to rural areas in countries with formal mentalhealth services, and where the availability of psychiatrists and specialist mental health practitioners approxi-mates that recommended by the World Health Organization. Relevant data were collected via a literature searchusing Medline and PsychLit and supplemented by material from key textbooks and by articles recommendedby local experts in the field.
A variety of special issues in rural areas, which make mental health service provision problematic, wereidentified. These relate to the characteristics of the rural location and community, demands upon and availabilityof mental health clinicians, and the changing role and focus of mental health services.
These features, together with limited access to services by patients, necessitate models of service deliverydifferent from those provided in urban areas. Important features include a shift from the ‘specialist as directprovider of care’ role to one of consultation, education, and indirect service provision and the use of a varietyof outreach arrangements to enable patient access to essential specialist services.
REVIEW ARTICLE Dis Manage Health Outcomes 2002; 10 (12): 771-7811173-8790/02/0012-0771/$25.00/0
© Adis International Limited. All rights reserved.

1. Background
The common psychiatric disorders, anxiety and depression,have a combined community prevalence rate of between 15 and30%.[1-3] The clinical and economic costs of these disorders can-not be underestimated. They account for a large percentage ofdays lost from work due to illness[2,3] and are associated withimpairments in physical and social role functioning at least assevere as those associated with chronic physical illness.[4] Thesefindings have been supported by those of the Global Burden ofDisease Study, which found that of the ten leading causes of dis-ability worldwide in 1990, measured in years lived with a disabil-ity, five were psychiatric conditions: unipolar depression, alcoholuse, bipolar affective disorder, schizophrenia, and obsessive-compulsive disorder. Furthermore, unipolar depression is pre-dicted to be the second largest cause of disease burden in the year2020, second only to ischemic heart disease.[5]
A variety of pharmacological and psychological treatmentshave been shown to be effective in these disorders.[6] However,many people do not have access to, or do not receive, these treat-ments.[1,3] An important factor associated with the lower rates ofuse of specialist services is rural, particularly remote, resi-dence.[7] Given the effects of these disorders on the individualand the family and the related social and economic consequences,methods must be found to ensure that mental health services inrural areas are readily available and effective.
The provision of psychiatric services in rural and remoteareas poses significant challenges to those involved in the plan-ning and delivery of these services. These challenges vary con-siderably between Western and nonWestern countries. The lattergenerally have a lack of sustained public investment in mentalhealth services and, as a consequence, limited development ofsuch services.
In this paper we confine our discussion to the problems ofdelivery of services to rural areas in those countries with formalmental health services, and where the availability of psychiatristsand specialist mental health practitioners approximates that rec-ommended by the World Health Organization (e.g. Canada,North America, Britain, Australia and New Zealand). A literaturesearch was conducted for this review on Medline and PsychLit,using the key words rural, remote, psychiatry, psychology andmental, in order to identify relevant literature published since1980. These data were supplemented by material from key text-books and by articles recommended by local experts in the field.
Worldwide, rural residents comprise a very substantial pro-portion of the population (e.g. 30% in Australia, 25% in the USA,and 16% in Canada). Rural residents inhabit a wide range of com-munities from major regional centers, through small communitytowns, to isolated small communities. These communities are
highly diverse and dynamic, differing in employment patterns,land use, socioeconomic status, culture, ethnic diversity, andphysical environment.[8]
Until recently, it has been assumed by many that the commonpsychiatric disorders occur less frequently in rural than in urbanresidents.[9,10] However, overall studies show no urban-rural dif-ferences in prevalence.[11] Rather, it appears that a variety of fac-tors, which vary within and between rural (and urban) communi-ties, such as poverty, unemployment,[12] poor social networks,[13]
mental status and gender,[12,14] most influence prevalence.There are a variety of special issues that impact on mental
health service provision in rural areas. Broadly, these fall intothree distinct areas: characteristics of the rural location and com-munity, demands upon, and availability of, mental health clini-cians, and the changing role and focus of mental health services(table I).
2. Characteristics of the RuralLocation and Community
Whilst rural communities vary considerably, there are sim-ilar characteristics between those in developed nations such asthe US, Canada and Australia. Rural populations tend to be older,sicker, poorer, have less education and are more likely to beuninsured than urban residents.[15,16] Complex global economic,social, political and technological changes have had a profoundimpact on these communities. The main mechanism throughwhich regional populations have adjusted to these changing cir-cumstances is via migration,[17] with the end result of the migra-tion of young people to urban areas and an aging rural popula-tion.[18]
The structure of rural life has also changed, with the role offarming being increasingly less profitable. The last two decadeshave seen a dramatic decline in the number of people employedin the agricultural sector,[19] which has impacted upon both theeconomic viability and cultural identity of small country towns.For those who remain in agriculture there has been a decline inreal incomes throughout the 1980s and 1990s, with many produc-ers regularly returning no profit.[20] Poverty is also a commonfeature of many rural areas, with high numbers of people depend-ent upon welfare payments.[21] In the US and Australia there isalso the relatively recent trend of counter-urbanization, which hasseen the rural drift of low-income urban families to nonmetro-politan communities often in search of low-cost housing.[22]
2.1 Cultural Characteristics of Rural Communities
Generally, the larger proportion of the population in rural andremote areas are indigenous peoples. This population group
772 Judd et al.
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 2002; 10 (12)

experiences disadvantages in all the socioeconomic indicators,thus having for example high unemployment rates, overcrowdedhousing conditions, and an over-representation in the criminaljustice system.[23] Due to the diversity of indigenous populations,and the relative paucity of research into indigenous mental health,it is difficult to estimate the prevalence of psychiatric disordersin these peoples.[24] However, given the violence, discriminationand trauma experienced by many indigenous groups we can as-sume that there are high rates of neuropsychiatric and behavioralproblems among them.[25] For example, mental health issues suchas depression, suicide, and substance abuse are a major problemin Australian Aboriginal communities.[26]
When seeking and obtaining treatment, indigenous peopleface a mix of barriers including those of language, how symptomsare manifested or communicated, the stigma of psychiatric dis-ease, and the racial intolerance of their practitioners which canlead to inappropriate or inadequate treatment.[27] Furthermore,the treatment of indigenous peoples may be complicated by is-sues of diagnostic validity, with many diagnostic categories be-ing culturally constructed and lacking the clinical manifestationsseen in nonWestern populations.[28]
There are very clear disadvantages for rural residents whoexperience psychiatric disorders. Rurality has been associated
with individuals failing to seek help for mental health problemsand a tendency for individuals to rely on their family and friendsfor support.[1,29] Certain communities are typified by stereotypicvalues that affect how individuals deal with mental illness. Forexample, rural Appalachians in the US have been described ashighly individualistic, antiauthoritarian, opinionated and stub-born.[30] It is suggested that the ‘frontier ideology’ in the westernstates in the US advocates an independent approach to livingwhich can lead to isolation and limit access to medical, includingmental health, care.[31] The cultural barriers to seeking help arecompounded by the limited services available in rural and remotecommunities. In rural areas there continues to be an undersupplyof primary care physicians, and an even greater shortage of spe-cialist and mental health professionals.[32,33]
The limited number of mental health professionals alsoplaces an increased burden upon the caregivers of people withmental illness. Since deinstitutionalization began in the 1950s inthe US, Australia, New Zealand, the UK, Canada and other sim-ilar countries, families have become the primary caregivers ofpeople with mental health problems, and in rural areas this hasoften meant that a major role of the caregiver is to compensatefor the lack of mental health services.[34] In a recent Australianstudy[34] families cited difficulty in accessing treatment, highturnover of mental health staff, early discharge from inpatientcare and limited follow-up as major difficulties in caring for theirfriend or family member.
Given the relatively small populations in rural areas, mostresidents in these areas are well known to each other. Rural peo-ple are usually aware of the affairs of neighbors, including whenneighbors are in receipt of care for mental health problems.[35]
Further, attitudes toward mental illness within the rural commu-nity are generally more negative[36] and this can present signifi-cant problems for people seeking help in small communitieswhere there is a lessened sense of confidentiality and anonym-ity.[37-40]
It is also argued that there has been limited involvement ofconsumers in the planning of mental health service provision,leading to services that are less responsive to both consumers andrural contexts.[41] Whilst the consumer movement that began toflourish in the 1970s is now playing a significant role in the de-livery of urban mental health service, little impact has been madein rural communities. It has been suggested that the stigma asso-ciated with mental illness is a disincentive to form advocacygroups and that rural areas lack the critical mass of population tosupport and sustain such groups.[41]
For those who do experience mental health problems thecultural characteristics of rural communities have advantages anddisadvantages. Studies of mental health, culture and stigma have
Table I. Special issues involved in the provision of mental health servicedelivery in rural areas
Characteristics of the rural location and communityDemographics, e.g. ageing population, out-migration from ruralcommunities
Socioeconomic factors, e.g. high rates of unemployment/poverty
Large indigenous population
Attitudes and behaviors to illness/health and mental health
Access, travel time, distance, and costs related to mental health services
Local availability of healthcare services
Informal mental healthcare
Limited consumer involvement in service planning
Limited supports for caregivers
Demands upon, and availability of, mental health cliniciansLimited supply of specialist mental health clinicians
Professional isolation and limited peer support
Dual, multiple or overlapping relationships (i.e. people with whom mentalhealth professionals may have had a previous or current personal orother type of relationship)
Complex confidentiality issues
Multiple role requirements
Changing role and focus of mental health servicesInstitution to community-based care
Broadening of the aim of mental health services
Availability of evidence-based medicine
Rural Psychiatry 773
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 2002; 10 (12)

focused largely upon urban areas.[42] This research has focusedon deinstitutionalization and has documented the exclusionarypractices of local communities (and society generally), designedto physically exclude those with serious mental illness, the con-centration of former inpatients in inner city areas and the emer-gence of ‘service-dependent ghettos’.[43]
The few studies that have concentrated on rural areas haveshown contrasting results. Burvill and colleagues[44] found intheir study in Western Australia that the high visibility withinsmall towns results in individuals with mental illness being so-cially excluded from the community. These findings were rein-forced by Milligan[45] in her study of rural Scotland in whichparticipants with mental illness not only felt excluded within theirown communities but also had few alternative options for em-ployment or social interaction, thus further contributing to theirsense of isolation. Other authors have identified positive aspectsof rural culture for those experiencing mental ill health. Reed[46]
believes that churches provide a substitute for the social welfareagencies that exist within urban areas, providing services forthe social and physical needs of isolated individuals. This roleof the church has been highlighted for particular populations(e.g. African-American populations).[39] Community organiza-tions and people in key interactive roles (e.g. postmen, hairdress-ers) also play a role in the rural community’s informal system ofcare.[39] A number of authors have also found that there is agreater sense of community in rural areas and a willingness toensure that those affected by psychiatric illness have the oppor-tunity to participate and contribute to community life;[47,48] othersdismiss this as succumbing to romantic idealism.[49] The positiveaspects of rural communities may, in part, account for the find-ings of a number of studies which have identified lower levels ofco-morbidity[1] and better long-term outcomes for rural resi-dents[50] who experience mental illness.
3. Demands Upon, and Availability of,Mental Health Clinicians
The poor availability of specialized mental health personnelat a global level has recently been highlighted in an internationalinvestigation of mental health resources.[51] This short supply ofspecialists is particularly striking in rural areas where their dis-tribution tends to be markedly lower than that found in urbanlocations.[52,53] Similar problems exist with primary care provid-ers, notably general medical practitioners, who have a greaterrole in providing mental healthcare in rural communities than inurban ones.[54] Indeed, the problem of inadequate staffing is con-sistently identified as the largest obstacle confronting rural men-tal health services.[46]
Difficulties in the recruitment and retention of a rural mentalhealth workforce can be attributed to a number of factors. Pro-fessional isolation and limited peer support because of low staffnumbers, along with reduced opportunities for further trainingand professional development have been identified as disincen-tives to rural work in mental health.[55-57] The multiple role re-quirements of clinicians in areas with limited resources may placeunrealistic expectations on available providers, requiring themto function as ‘Jack and Jill of all trades’.[58] As a consequence,it may be necessary at times for care to be provided in areasthat are outside of the practitioners’ areas of competence andexpertise.[59]
Preparation for rural mental health work is also an issue.Not only are most mental health professionals trained in urbanlocations as specialists, but also the content of training pro-grams tends to prepare them for work specifically in an urbansetting.[60-62] Rural workforce issues impact significantly on theways that services can be delivered and are likely to present con-tinuing challenges to mental health planners and policy makers.
The characteristics of rural settings, with limited healthcareand other resources, place increased demands on the providers ofmental health services to ensure ethical conduct. Thus, guidelinesfor ethical practice, which determine professional codes of con-duct or ethics, may not be directly applicable to the practice de-mands faced by rural clinicians. Providers of mental healthcareare challenged to develop and apply guidelines for ethical prac-tice that respect the principles of patient welfare while takingaccount of those broader issues within the community that pro-vide a context for the delivery of care.
The obligation of professionals to respect confidentiality ofinformation from service users is a complex and critical issue inrural areas. The nature of smaller communities is such that con-fidentiality is more difficult to ensure in practice with the poten-tial for greater harm where breaches occur. In cases where thereis multiagency involvement, the practice of exchanging informa-tion between service agencies may be problematic, particularlygiven the heightened social stigma about mental health prob-lems.[63] Strict adherence to confidentiality and the withholdingof information, on the other hand, may impact adversely on thevital collaborative relationships between service agencies andproviders that exist in rural communities.[59]
Greater demands on mental health professionals to provideservices to people with whom they may have a previous or currentpersonal or other type of relationship is also characteristic ofsmaller communities.[64] Referred to as dual, multiple or overlap-ping relationships,[65] these situations have been highlighted forthe potential problems that they may give rise to in terms ofconflict of interest, loss of objectivity and exploitation of service
774 Judd et al.
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 2002; 10 (12)

users.[66] In rural areas, the possible benefits of overlapping rela-tionships, such as the opportunity for a mental health professionalto observe patients in a wider environment, have also been notedby some authors.[67,68] Similarly, rural mental health cliniciansmay experience problems in maintaining their own sense of pri-vacy. The rural clinician will frequently see current and past pa-tients outside the clinical situation when attending social events,going shopping etc. Appropriate boundaries must be set in thesesituations, and this may challenge the clinician’s flexibility andadaptability.[31]
4. The Changing Role and Focus ofMental Health Services
The challenges and opportunities involved in the provisionof services to meet the mental health needs of rural residents havechanged considerably over the past several decades. Three majorfactors account for this: (i) the move from institution-based tocommunity-based care; (ii) a broadening of the aim of mentalhealth services reflecting adoption of a public health approach;and (iii) the recent explosion of interest in evidence-based med-icine.
4.1 Community-Based Care
The practice of psychiatry over the past half-century, andparticularly the past decade, has changed fundamentally. Com-munity psychiatry, now the dominant model, is described as com-prising ‘the principles and practices needed to provide mentalhealth services for a local population by: establishing population-based needs for treatment and care; providing a service systemlinking a wide range of resources of adequate capacity; operatingin accessible locations; and delivering evidence-based treatmentsto people with mental disorders’.[69] Of note, implicit in this def-inition is the idea that mental health services are a type of wide-area network including both health and social care, and formaland informal government-funded and voluntary services.
Tansella and Thornicroft[70] have outlined the essential ele-ments for any system of care. These include outpatient and com-munity services, day services, acute in-patient services, longer-term residential services and interfaces with other services. Thelatter include other health services (e.g. primary care, aged care,drug and alcohol services etc.), social services/welfare, housingagencies, other government agencies (e.g. police), and non-government organizations such as religious groups, voluntaryand for-profit private organizations. It is immediately evident thatwhilst all these elements can reasonably be expected in an urbansetting, this will frequently not be possible in smaller, more dis-persed rural communities.
The concept of sectorization has been used to describe theorganizational framework of community psychiatric services.Sectorized services usually provide services to a particular geo-graphic area and are responsible for the provision of care to thetotal population within the catchment area. Of relevance for ourconsideration of rural services, sectorized services can be cate-gorized into a variety of models:[71]
• the hospital core model: the hospital is the center of the sys-tem with coordinated services, such as community clinics,placed in strategic parts of the catchment area
• the community mental health center model: a communitybase for both acute and continuing services provides both alocation for services and a base for outreach services, andlinks to other local services outside the mental health service
• the integrated primary care model: first contact sites (e.g.general practitioner [GP]) are the base and location for as-sessment and treatment. Mental health services staff have aspecific liaison role with these services for both short termand continuing care
• the assertive outreach or home-based model: used for a coreclient group with severe needs who are unable or unwillingto attend the regular services.Most mental health services are delivered by generic com-
munity teams. Although multidisciplinary in nature, psychiatristsand mental health nurses are key participants. In general, serviceshave different generic teams for the different age groups of pa-tients – child and adolescent teams caring, respectively, for indi-viduals up to 16 or 18 years of age, and elderly teams for indi-viduals over 65 years of age. In addition, many services havespecialist teams with defined target groups based on diagnosis orspecific need. These include, for example, mother and baby units,eating disorder services and forensic services.
Over the past 30 years two organizational mechanisms, casemanagement and assertive community treatment, have evolvedto deliver, integrate and coordinate care in the community.
Case management seeks to access most or all of the neededservices from other community agencies. Whilst there are variousmodels of case management, all include at least five core func-tions: assessment, planning, advocacy, linkage and monitor-ing.[72] Different models (e.g. brokered models, intensive casemanagement models) combine these functions in different ways.In rural settings, three weaknesses – inconsistent and inappropri-ate training, restrictions from role as direct service provider (i.e.it is often difficult in rural areas to adequately perform the roleof direct service provider so another model has to be used) andlimited service availability – have been found to diminish thepracticality of the broker model.[73] Thus, it is not surprising thatrural dwellers with serious mental illness have been found to beless likely to receive case management than non-rural persons.[74]
Rural Psychiatry 775
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 2002; 10 (12)

In stark contrast to case management, assertive communitytreatment brings together a multidisciplinary treatment team thatcan provide most or all of the needed services directly. Clearly,this is a more intensive intervention and one that is unlikely to beeasily provided in rural areas. However, rural adaptations of theassertive community treatment model have been described,[75,76]
albeit in areas large enough to support a community mental healthclinic as the service base.
The challenge in small and dispersed rural communities ishow to maintain a comprehensive program in the absence of acommunity-based mental health team. Successful programs arethose that have been able to creatively use the resources of ruralareas.[77] Key factors which can be utilized include: (i) commu-nity members knowing each other well and being willing to getinvolved in the problems of others; (ii) use of neighbors as asource of volunteers; (iii) professionals knowing consumers per-sonally so problems are easier to identify; and (iv) lower rate ofcommunication problems than in urban settings.[78]
4.2 A Broadening of the Aim of Mental Health Services
Over the past decade the demonstration of high levels ofpsychiatric morbidity[1] and high levels of unmet needs, and therecognition that the burden (years lived with a disability) of men-tal disorders is growing[5] has led to a rethinking of how thechallenge of mental health problems can best be met. This has ledto a greater focus on a public health approach, one that identifiesproblems experienced by whole populations and provides inter-ventions to mitigate them for the whole population.[79] Adoptionof a public health approach has broadened the aim of mentalhealth services from that of improving the mental health of pop-ulations they service to also include an interest in disease preven-tion and health promotion. This has led to an expectation thatservices will provide a mental health intervention spectrum thatincludes a focus on prevention, treatment and maintenance.[80]
The lack of clear understanding of the causal risk factors forpsychiatric disorders means primary prevention is not at presenta realistic goal. By contrast, secondary prevention is achievable.In particular, preventive measures[80] have increasingly becomea focus of attention. These measures are targeted at individualswho have an identified individual ‘risk factor’ for the future de-velopment of psychiatric disease. Other secondary preventionstrategies include early case detection and shortening of delaysin accessing treatment, optimizing and intensifying treatmentstrategies to minimize duration of illness per episode, and relapseprevention strategies. These approaches require integration be-tween inpatient and community-based services and between spe-cialist mental healthcare and primary healthcare, both of which
are difficult to achieve when workforce is limited and servicesites and target populations are dispersed.
4.3 Evidence-Based Medicine
The past decade has witnessed an increasing focus on theneed to ensure that clinical decision making is based upon themost appropriate, accurate and up-to-date information, i.e. thepractice of evidence-based medicine. Evidence-based medicineis ‘the conscientious, explicit and judicious use of currently avail-able best evidence in making decisions about the care of individ-ual patients’.[81] Evidence-based practices are interventions forwhich there is scientific evidence consistently showing that theyimprove client outcomes.
Whilst in many circumstances variation in diagnostic andtherapeutic practice is justified, the diversity of rural environ-ments has inevitably resulted in greater variability and inconsis-tency of service systems.[82] Historical neglect of rural mentalhealth by both researchers and policy makers has limited the de-velopment of coordinated and empirically-based services,[83] andeconomic constraints have limited implementation of theory-driven service delivery systems. Thus, the necessary globalmovement toward evidence-based healthcare practice[84] is par-ticularly timely in rural mental health systems.
There is a strong role for evidence-based practice within theframework of mental health service delivery, and there is muchevidence available on which to base mental health interventions.Although often difficult to find, this is gradually being systemat-ically reviewed by organizations such as the Cochrane Collabo-ration.[85] Unfortunately, despite the extensive evidence andagreement on effective mental health practices for persons withsevere psychiatric illness, research shows that routine mentalhealth programs do not provide evidence-based practices to thegreat majority of their clients with these illnesses.[86] A varietyof factors may account for this. These include clinicians’ lack ofawareness of how to use the evidence,[85] poor communicationbetween employers, educators, practitioners and communitymembers,[84] and the influence of political values rather than ev-idence on mental health policy.[85]
There are added barriers to delivering evidence-based prac-tice to rural areas. Firstly, there is very little research on evidence-based interventions in rural regions. Existing urban-based ap-proaches to evidence-based practice can disadvantage ruralpractitioners because they do not recognize and accommodate theinherent differences in rural and urban healthcare cultures. It istherefore recognized that there is a need to seek approaches toresearch-based practices that arise from the specific needs of ru-ral settings.[87] However, it is difficult to conduct research in rural
776 Judd et al.
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 2002; 10 (12)
areas that meets the standard requirements and has the method-ology expected of present day clinical trials. This can be attrib-uted to the fact that there is not a well developed ‘research cul-ture’ that can support a rigorous statistical research methodologyin rural regions. In addition, it can be difficult to measure and tocontrol for the number of variables that are important in ruralmental health research.
Secondly, there are basic differences between urban and ru-ral practitioners access to information. For example, rural prac-titioners’ can experience difficulties accessing the Internet or li-braries, as well as problems accessing training and supervisionin order to implement evidence-based treatments. These occurparticularly because of the isolation and a lack of skilled scien-tist-practitioners in rural services.
Thirdly, in order to provide a foundation for evidence-basedpractice that will demonstrate quality, efficiency, effectiveness,and community acceptability, there must be support from em-ployers to address both the infrastructure and educational needsof their employees.[84] Therefore, mental health service employ-ers need to see evidence-based practice as important, if staff areexpected to seek and utilize such practices.
5. Models of Mental Health Service Delivery
The key defining characteristic of rural mental health serviceprovision is access to services. Variations in the size, density anddegree of isolation of rural populations result in significant dif-ferences in the need for and the abilities of rural communities tosustain a range of health services.[88] When determining the wayin which health services can be delivered, service threshold andrange are important.[89] The threshold of a service refers to theminimum market (number of people) needed for its existence andto sustain the service over time. Services requiring many peopleto sustain their existence (i.e. with high thresholds) providehigher order functions (e.g. generic mental health services). Thehighest order services (e.g. specialist mental health services suchas forensic services, mother-baby unit, eating disorders service)may require the whole state to support them.
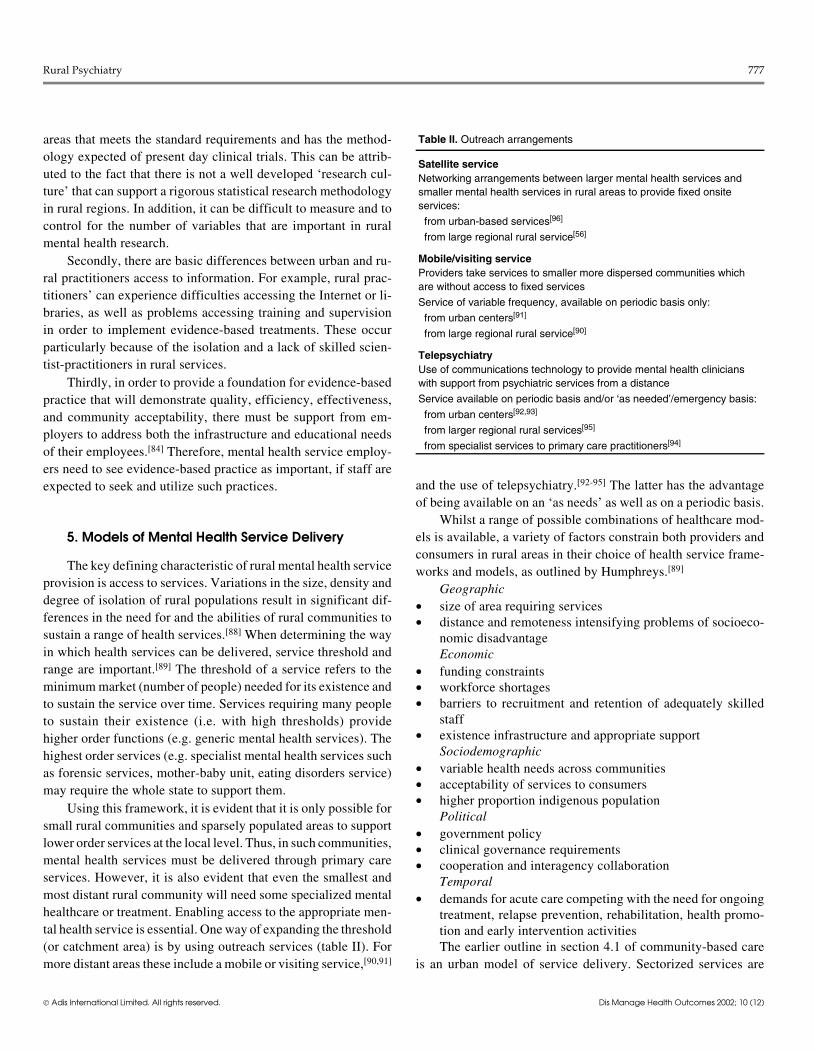
Using this framework, it is evident that it is only possible forsmall rural communities and sparsely populated areas to supportlower order services at the local level. Thus, in such communities,mental health services must be delivered through primary careservices. However, it is also evident that even the smallest andmost distant rural community will need some specialized mentalhealthcare or treatment. Enabling access to the appropriate men-tal health service is essential. One way of expanding the threshold(or catchment area) is by using outreach services (table II). Formore distant areas these include a mobile or visiting service,[90,91]
and the use of telepsychiatry.[92-95] The latter has the advantageof being available on an ‘as needs’ as well as on a periodic basis.
Whilst a range of possible combinations of healthcare mod-els is available, a variety of factors constrain both providers andconsumers in rural areas in their choice of health service frame-works and models, as outlined by Humphreys.[89]
Geographic• size of area requiring services• distance and remoteness intensifying problems of socioeco-
nomic disadvantageEconomic
• funding constraints• workforce shortages• barriers to recruitment and retention of adequately skilled
staff• existence infrastructure and appropriate support
Sociodemographic• variable health needs across communities• acceptability of services to consumers• higher proportion indigenous population
Political• government policy• clinical governance requirements• cooperation and interagency collaboration
Temporal• demands for acute care competing with the need for ongoing
treatment, relapse prevention, rehabilitation, health promo-tion and early intervention activitiesThe earlier outline in section 4.1 of community-based care
is an urban model of service delivery. Sectorized services are
Table II. Outreach arrangements
Satellite serviceNetworking arrangements between larger mental health services andsmaller mental health services in rural areas to provide fixed onsiteservices:
from urban-based services[96]
from large regional rural service[56]
Mobile/visiting serviceProviders take services to smaller more dispersed communities whichare without access to fixed services
Service of variable frequency, available on periodic basis only:
from urban centers[91]
from large regional rural service[90]
TelepsychiatryUse of communications technology to provide mental health clinicianswith support from psychiatric services from a distance
Service available on periodic basis and/or ‘as needed’/emergency basis:
from urban centers[92,93]
from larger regional rural services[95]
from specialist services to primary care practitioners[94]
Rural Psychiatry 777
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 2002; 10 (12)

delivered by general and specialist teams to a large, closely set-tled population. A combination of the hospital core model andthe community mental health center model is used and there is astrong emphasis on specialist mental health workers as the directproviders of care. Moving beyond urban centers requires modi-fication of the service delivery model to account for the size ofthe population and the degree to which the population is dispersedover the catchment area.
In large regional centers (i.e. medium-sized but closely set-tled population) the focus on specialist mental health workers asdirect providers of care is generally maintained. Specialist pro-viders may be resident or attend on an outreach basis.[97] Facili-ties are decentralized and represent extensions of a main facility.Models of care within the regional center resemble those of urbanservices and are often structured on the hospital core model. Mostdo not have resident subspecialist services but may access theseas an outreach service.[98]
Commonly, large regional services have been developed asthe hub of a sectorized service covering a large geographic area,which also includes a number of smaller, moderately closely set-tled communities and/or smaller and more dispersed communi-ties. These ‘hub and spoke’ or networking/satellite models arenot without problems. The structure of such services assumes thatrural people have ties to the larger population center (the hub).However, rural dwellers typically do not have strong integrativeties to nearby regional hubs and are less likely to utilize regionalservices.[99] Furthermore, rural populations are less likely tomake use of facility-based services, especially when facilities areat significant distances and providers are less cognizant of theculture and beliefs of rural persons.[52]
Provision of satellite services outside the hub to smaller pop-ulation centers requires a change in focus from that of the urbansetting. The most common model of service provision involvesreliance on an enhanced role for GPs (primary care physicians)and the establishment of rural clinics[56] (i.e. a combination ofthe community mental health center model and the integratedprimary care model). Generic multidisciplinary mental healthcommunity teams usually staff these clinics with a psychiatristproviding input on an outreach basis. This may be done by ‘inperson’ visits[100] or by telepsychiatry.[95]
The model used for the provision of rural healthcare servicesis more the consultation or indirect service model with a focuson utilizing and mobilizing existing resources and structuresthrough consultation and education.[101] Links are establishedwith GPs and other healthcare providers enabling local arrange-ments for collaborative care,[102] sometimes including local ar-rangements for inpatient care using general hospital facili-ties.[100,103] Often from these centers mental health teams provide
outreach services to smaller communities, either as a lone mentalhealth worker based on site or visiting on a regular basis.[90]
The reliance on GPs for providing healthcare services inrural communities is opportunistic, using their proximity to thepatients. However, this is not without problems. Many GPs arenot skilled in the detection and treatment of psychiatric disor-ders.[104,105] In addition, problems may be encountered in inte-grating professionals who are trained in diverse ways and havedifferent ideologies.[106,107]
The predominant model of service delivery in smaller andmore dispersed communities is the primary healthcare model inwhich primary healthcare workers from various backgrounds andexpertise are trained to recognize and manage psychosocial dis-orders.[79] In addition, mental healthcare workers may be inte-grated into the local health service. In addition to improving ac-cessibility and reducing the primary care provider’s burden ofproviding mental health services, this model has the advantageof reducing the stigma associated with psychiatric disorders insmall communities where consumers of mental health servicesare more easily visible.[88,108] A key disadvantage is the potentialfor isolation of mental health staff working in these settings.[106]
In such models, outreach services provide consultation, educa-tion, training and support to a wide range of professionals includ-ing nurses, GPs, indigenous health workers, ambulance officers,police, and teachers.[90,91]
These different models of service delivery in rural areas havegenerally evolved or been designed to provide practical, localsolutions to the limited access to services. Evaluation of suchservices is generally lacking, with most of the services identifiedhere being descriptive (i.e. people have reported what they havedone but no systematic evaluation of outcomes or impact is avail-able). There is an urgent need to evaluate the models of servicedelivery that have evolved. Therapies which have been shown tobe effective have generally been delivered in specialist settingsor in settings with the substantial support of specialist care pro-viders.[6] An important question to be examined during the eval-uation of these models is whether reliance on primary care pro-viders may compromise the quality of care to patients, or whatamount of specialist service input is needed for effective treat-ment.[109] The answer to this question is essential in order to de-termine what outcomes (individual, social, and economical) canbe achieved with the use of such rural mental health services.
6. Conclusions
The provision of mental health services in rural areas posesboth challenges and opportunities. The challenges are obvious.Key issues include improving coverage of mental healthcare in
778 Judd et al.
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 2002; 10 (12)

rural areas, recruitment and retention of an appropriately trainedspecialist mental health workforce, adaptation of clinical practiceto meet the needs and constraints of rural communities, and thedevelopment and evaluation of models of service delivery de-signed to overcome problems of access in more distant and iso-lated areas.
Alongside the challenges there are significant opportunities.These include the chance to work flexibly outside the traditional‘specialist as direct service provider’ role, better potential forcollaboration between local health and associated service pro-viders, productive use of the culture of informal care and senseof community, and scope to develop innovative services whichcreatively use those resources which are available.
The task for all stakeholders, including clinicians and policymakers, is to meet the challenges and maximize the opportunities.This will require both short- and long-term strategies which linkresearch, service evaluation, education, training and support, andservice delivery with policy formulation and implementation.
Acknowledgements
No sources of funding were used and the authors have no conflicts ofinterest directly relevant to the content of this review.
References1. Kessler, McGongale KA, Zhao S, et al. Lifetime and 12-month prevalence of
DSM-II-R psychiatric disorders in the United States. Arch Gen Psychiatry 1994;51 (1): 8-19
2. Jenkins R, Lewis G, Bebbington P, et al. The National Psychiatric Morbidity sur-veys of Great Britain: initial findings from the household survey. Psychol Med1997; 27 (4): 775-89
3. Andrews G, Henderson S, Hall W. Prevalence, comorbidity, disability and serviceutilisation: overview of the Australian National Mental Health Survey [publish-ed erratum appears in Br J Psychiatry 2001; 179: 561-2]. Br J Psychiatry 2001;178: 145-53
4. Wells KB, Golding JM, Burnam MA. Psychiatric disorder and limitations in phys-ical functioning in a sample of the Los Angeles general population. Am J Psy-chiatry 1988; 145 (6): 712-7
5. Murray CJL, Lopez AD. The global burden of disease: a comprehensive assessmentof mortality and disability from diseases, injuries and risk factors in 1990 andprojected to 2020. Cambridge (MA): World Health Organisation, World Bank,Harvard School of Public Health, 1996
6. Nathan P, Gorman J. Guide to treatments that work. New York (NY): OxfordUniversity Press, 1998
7. Parslow RA, Jorm AF. Who uses mental health services in Australia? An analysisof data from the National Survey of Mental Health and Wellbeing. Aust N Z JPsychiatry 2000; 34 (6): 997-1008
8. Hugo G. What is really happening in regional and rural populations. In: RogersMF, Collins YMJ, editors. The future of Australia’s country towns. Bendigo:La Trobe University, 2001: 57-71
9. Dohrenwend BP, Dohrenwend BS. Psychiatric disorders in urban settings. In:Caplan G, editor. Child and adolescent psychiatry: sociocultural and communitypsychiatry. New York (NY): Basic Books Inc, 1974: 424-49
10. Webb SD. Rural-urban differences in mental health. In: Freeman H, editor. Mentalhealth and the environment. New York (NY): Churchill-Livingstone, 1984:226-49
11. Judd F K, Jackson H, Komiti A, et al. High prevalence disorders in urban and rural
communities. Aust N Z J Psychiatry 2002; 36 (1): 104-13
12. Parikh SV, Wasylenki D, Goering P, et al. Mood disorders: rural/urban differences
in prevalence, health care utilization, and disability in Ontario. J Affect Disord
1996; 38 (1): 57-65
13. Romans-Clarkson SE, Walton VA, Herbison GP, et al. Psychiatric morbidity
among women in urban and rural New Zealand: psycho-social correlates. Br J
Psychiatry 1990; 156: 84-91
14. Paykel ES, Abbott R, Jenkins R, et al. Urban-rural mental health differences in
Great Britain: findings from the National Morbidity Survey. Psychol Med 2000;
30 (2): 269-8015. Braden J, Beauregard K. Health status and access to care of rural and urban popu-
lations. Rockville (MD): Agency for Health Care Policy and Research, 1994
16. Trickett P, Titulaer I, Bhatia K. Rural, remote and metropolitan health differentials:
a summary of preliminary findings. Aust Health Rev 1997; 20 (4): 128-37
17. Bryant C, Joseph A. Canada’s rural population: trends in space and implications in
place. Can Geographer 2001; 45 (1): 132-7
18. Joseph A, Martin-Matthews A. Growing old in aging communities. J Can Studies
1993; 28: 14-2919. Booth NJ, Lloyd K. Stress in farmers. Int J Soc Psychiatry 2000; 46 (1): 67-73
20. Tonts M. Some recent trends in Australian regional economic development policy.
Reg Stud 1999; 33: 581-6
21. Dalakar J, Proctor B. Poverty in the United States. Washington, DC. US Census
Bureau, 1999
22. Fitchen JM. Spatial redistribution of poverty through migration of poor people to
depressed rural communities. Rural Sociol 1995; 60 (2): 181-202
23. McKendrick J, Cutter T, Mackenzie A, et al. The pattern of psychiatric morbidity
in a Victorian urban aboriginal general practice population. Aust N Z J Psychi-
atry 1992 Mar; 26 (1): 40-7
24. Cohen A. The mental health of indigenous peoples. Geneva: Department of Mental
Health, World Health Organization, 2001
25. Fullilove MT. Psychiatric implications of displacement: contributions from psy-
chology of place. Am J Psychiatry 1996; 153 (12): 1516-23
26. Swan P, Raphael B. ‘Ways forward’: national consultancy report on Aboriginal
and Torres Strait Islander mental health. Canberra (ACT): Australian Govern-
ment Publishing Service, 1995
27. McCarthy M. US mental-health system fails to serve minorities, says US Surgeon
General [letter]. Lancet 2001; 358 (9283): 733
28. Kleinman A. Rethinking psychiatry: cultural category to personal experience. New
York (NY): The Free Press, 1998
29. Regier DA, Hirschfeld RMA, Goodwin FK, et al. The NIMH depression awareness,
recognition, and treatment program: structure, aims, and scientific basis. Am J
Psychiatry 1988; 145 (11): 1351-7
30. Weller J. Yesterday’s people: life in contemporary Appalachia. Lexington (KY):
University of Kentucky Press, 1966
31. Reed D, Merrell A. Practice styles in rural psychiatry. In: Vaccaro JV, Clark Jr GH,
editors. Practising psychiatry in the community: a manual. Washington, DC:
American Psychiatric Press, 1996: 417-31
32. American Medical Association. Physician characteristics and distribution in the
US, 1999. Chicago (IL): American Medical Association, 1999
33. Australian Institute of Health and Welfare. Health in rural and remote Australia.
Canberra (ACT): Australian Government Publishing, 1998. Report no.: CAT
No. PHE6
34. Mathews-Cowey S. Too much responsibility, too little help: family carers and the
rural mental health care system. J Fam Stud 2000; 6 (2): 267-71
35. Loschen EL. The challenge of providing quality psychiatric services in a rural
setting. QRB Qual Rev Bull 1986; 12 (11): 376-9
36. Bachrach LL. Deinstitutionalization of mental health services in rural areas. Hosp
Community Psychiatry 1977; 28 (9): 669-72
37. Hill CE. Folk beliefs and practices. New York (NY): Brunner & Mazel, 1985
Rural Psychiatry 779
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 2002; 10 (12)

38. American Psychological Association. Caring for the rural community: an inter-disciplinary curriculum. Washington, DC. American Psychological Associa-tion, Office of Rural Health, 1995
39. Fox J, Merwin E, Blank M. De facto mental health services in the rural south. JHealth Care Poor Underserved 1995; 6 (4): 434-68
40. Hill CE, Fraser GJ. Local knowledge and rural mental health reform. CommunityMent Health J 1995; 31 (6): 553-68
41. Bjorklund RW, Pippard JL. The mental health consumer movement: implicationsfor rural practice. Community Ment Health J 1999; 35 (4): 347-59
42. Wolch J, Philo C. From distributions of deviance to definitions of difference: pastand future mental health geographies. Health Place 2000; 6 (3): 137-57
43. Dear M, Wolch J. Landscapes of despair: from deinstitutionalization to homeless-ness. Princeton (NJ): Princeton University Press, 1987
44. Burvill PW, Stampfer H, Reymond J. Rural psychiatric services in western Aus-tralia. Soc Sci Med 1984; 18 (11): 991-6
45. Milligan C. Without these walls: a geography of mental ill-health in a rural envi-ronment. In: Butler R, Parr H, editors. Mind and body spaces: geographies ofillness, impairment and disability. London: Routledge, 1999: 221-39
46. Reed DA. Adaptation: the key to community psychiatric practice in the ruralsetting. Community Ment Health J 1992 Apr; 28 (2): 141-50
47. Voss SL. The church as an agent in rural mental health. J Psychol Theol 1996; 24(2): 114-23
48. Kane CF, Ennis JM. Health care reform and rural mental health: severe mentalillness. Community Ment Health J 1996; 32 (5): 445-62
49. Murray JD, Kelleher K. Psychology and rural America: current status and futuredirections. Am Psychol 1991; 46 (3): 220-31
50. McGlashan TH. A selective review of recent North American long-term followup studies of schizophrenia. Schizophr Bull 1988; 14 (4): 515-42
51. World Health Organization Atlas. Mental health resources in the world 2001.Geneva: World Health Organization, 2001
52. Human J, Wasem C. Rural mental health in America. Am Psychol 1991; 46 (3):232-9
53. Sheehan MP, Loschen EL, D’Elia GM. Psychiatrists’ perceptions of mental healthmanpower needs in various population areas. Hosp Commun Psychiatry 1985;36 (10): 1111-3
54. Hall G. Monitoring and predicting community mental health centre utilisation inAuckland, New Zealand. Soc Sci Med 1988; 26 (1): 55-70
55. Harvey D, Hodgson J. New directions for research and practice in rural areas. AustPsychol 1995; 30 (3): 196-9
56. Tobin MJ. Rural psychiatric services. Aust N Z J Psychiatry 1996; 30 (1): 114-2357. Wolfenden K, Blanchard P, Probst S. Recruitment and retention: perceptions of
rural mental health workers. Aust J Rural Health 1996 May; 4 (2): 89-95
58. Gething L. Providing services in remote and rural Australian communities. J Com-munity Psychology 1997; 25 (2): 209-26
59. Hargrove DS. Ethical issues in rural mental health practice. Prof Psychol Res Pract1986; 17 (1): 20-3
60. Hargrove DS, Breazeale RL. Psychologists and rural services: addressing a newagenda. Prof Psychol Res Pract 1993; 24 (3): 319-24
61. Kenardy J, Griffiths R. Education and training for rural psychologists. WaggaWagga (NSW): Australian Rural Health Research Institute, 1996
62. Merwin EI, Goldsmith HF, Manderscheid RW. Human resource issues in ruralmental health services. Community Ment Health J 1995 Dec; 31 (6): 525-37
63. Roberts LW, Battaglia J, Epstein RS. Frontier ethics: mental health care needs andethical dilemmas in rural communities. Psychiatr Serv 1999; 50 (4): 497-503
64. Schank JA, Skovholt TM. Dual-relationship dilemmas of rural and small commu-nities. Prof Psychol Res Pract 1997; 28 (1): 44-9
65. Brownlee K. Ethics in community mental health care: the ethics of non-sexualdual relationships: a dilemma for the rural mental health profession. Commu-nity Ment Health J 1996; 32 (5): 497-503
66. Glosoff H, Corey G, Herlihy B. Dual relationships. In: Herlihy B, Corey G, edi-tors. ACA ethical standards casebook. 5th ed. Alexandria (VA): AmericanCounseling Association, 1996: 251-66
67. Gates KP, Speare KH. Overlapping relationships in rural communities. In: LermanH, Porter N, editors. Feminist ethics in psychotherapy. New York (NY):Springer, 1990: 97-101
68. Jennings FL. Ethics in rural practice. Psychother Priv Pract 1992; 10 (3): 85-104
69. Szmukler G, Thornicroft G. What is community psychiatry? In: Szmukler G,Thornicroft G, editors. Textbook of community psychiatry. Oxford: OxfordUniversity Press, 2001: 1-12
70. Tansella M, Thornicroft G. The mental health matrix: a manual to improve ser-vices. New York (NY): Cambridge University Press, 1999
71. Strathdee G, Thornicroft G. Community sectors for needs-led mental health ser-vices. In: Thornicroft G, Brewin CR, Wing J, editors. Measuring mental healthneeds. London: Gaskell, 1992: 140-62
72. Scott JE, Dixon LB. Assertive community treatment and case management forschizophrenia. Schizophr Bull 1995; 21 (4): 657-88
73. Rohland BM, Rohrer JE. Capacity of rural community mental health centers totreat serious mental illness. Community Ment Health J 1998 Jun; 34 (3): 261-73
74. Sullivan G, Jackson CA, Spritzer KL. Characteristics and service use of seriouslymentally ill persons living in rural areas. Psychiatr Serv 1996; 47 (1): 57-61
75. Santos AB, Deci PA, Lachance KR, et al. Providing assertive community treat-ment for severely mentally ill patients in a rural area. Hosp Community Psy-chiatry 1993; 44 (1): 34-9
76. McDonel EC, Bond GR, Salyers M, et al. Implementing assertive communitytreatment programs in rural settings. Adm Policy Ment Health 1997; 25 (2):153-73
77. Huessy HR. Deinstitutionalisation in a rural state: the Vermont experience. In:Wagenfeld MO, editor. Perspectives on rural mental health. San Franciso (CA):Jossey-Bass, 1981: 33-8
78. Diamond RJ, VanDyke D. Rural community support programs: the experience inthree Wisconsin counties. New Direct Ment Health Serv 1985; 26: 49-58
79. Desjarlais R, Ivanberg L, Good B, et al. World Mental Health: problems andpriorities in low income countries. Oxford: Oxford University Press, 1995
80. Mrazek PJ, Haggerty RJ. Reducing risk of mental disorders: frontiers for preven-tive intervention research. Washington, DC: National Academy Press, 1994
81. Sackett DL, Rosenberg WM, Gray JA, et al. Evidence based medicine: what it isand what it isn’t. BMJ 1996 Jan; 312 (7023): 71-2
82. Blank MB, Fox JC, Hargrove DS, et al. Critical issues in reforming rural mentalhealth service delivery. Community Ment Health J 1995 Dec; 31 (6): 511-24
83. Fox JC, Blank MB, Kane DF, et al. Balance theory as a model for coordinatingdelivery of rural mental health services. Appl Prevent Psychol 1994; 3 (2):121-9
84. McMurray A. Undertaking research for the benefit of the rural community. AustJ Rural Health 1998; 6 (2): 89-95
85. Geddes J, Reynolds S, Streiner D, et al. Evidence based practice in mental health.BMJ 1997; 315 (7121): 1483-4
86. Drake RE, Goldman HH, Leff HS, et al. Implementing evidence-based practicesin routine mental health service settings. Psychiatr Serv 2001; 52 (2): 179-82
87. McCarthy A, Hegney D. Evidence-based practice and rural nursing: a literaturereview. Aust J Rural Health 1998; 6 (2): 96-9
88. Reid M, Solomon S. National health strategy: improving Australia’s rural healthand aged care services. Melbourne (VI): National Health Strategy Unit, 1992
89. Humphreys J. Health service models in rural and remote Australia. In: WilkinsonD, Blue I, editors. The new rural health: an Australian text. Melbourne: OxfordUniversity Press, 2002: 273-96
90. Yellowlees P. Bush psychiatric services. Aust N Z J Psychiatry 1992; 26 (2): 191-691. Owen C, Tennant C, Jessie D, et al. A model for clinical and educational psychi-
atric service delivery in remote communities. Aust N Z J Psychiatry 1999; 33(3): 372-8
92. Hawker F, Kavanagh S, Yellowlees P, et al. Telepsychiatry in South Australia. JTelemed Telecare 1998; 4 (4): 187-94
93. Dossetor DR, Nunn KP, Fairley M, et al. A child and adolescent psychiatricoutreach service for rural New South Wales: a telemedicine pilot study. JPaediatr Child Health 1999; 35 (6): 525-9
780 Judd et al.
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 2002; 10 (12)

94. Hilty DM, Servis ME, Nesbitt TS, et al. The use of telemedicine to provide con-sultation-liaison service to the primary care setting. Psychiatr Ann 1999; 29:421-7
95. Buist A, Coman G, Silvas A, et al. An evaluation of the telepsychiatry programmein Victoria, Australia. J Telemed Telecare 2000; 6: 216-21
96. Henderson C, Vanier C, Noel P. A Canadian model for developing mental healthservices in rural communities through linkages with urban centres. J MentHealth Adm 1991; 18 (2): 135-42
97. Large M, Paton M, Wright M, et al. Current approaches to enhancing non-metro-politan psychiatrist services. Aust Psychiatry 2000; 8: 249-52
98. Judd F K, Jackson H, Davis J, et al. Improving access for rural Australians totreatment for anxiety an depression: the University of Melbourne Depressionand Anxiety research and treatment group. Bendigo Health Care Group initia-tive. Aust J Rural Health 2001; 9 (2): 91-6
99. Hill CE. Community health systems in the rural American south: linking peopleand policy. Boulder (CO): Westview Press, 1988
100. Samuels AH, Owen C. A day in the country: a perspective on rural psychiatry. AustPsychiatry 1998; 6: 283-6
101. Wodarski JS. Rural community mental health practice. Baltimore (MD): UniversityPark Press, 1983
102. Katon W, Von Korff M, Lin E, et al. Collaborative management to achieve treat-ment guidelines. JAMA 1995; 273: 1026-31
103. Richardson ME. Rooming in: an alternative to involuntary detention. Aust N Z JPsychiatry 1996; 30 (2): 263-9
104. Ormel J, Oldehinkel T, Brilman E, et al. Outcome of depression and anxiety inprimary care: a three-wave 3 1/2-year study of psychopathology and disability.Arch Gen Psychiatry 1993; 50 (10): 759-66
105. Goldberg DP, Bridges A. Screening for psychiatric illness in general practice: the
GP versus the screening questionnaire. J R Coll Gen Pract 1987; 37 (15): 18
106. Van Hook MP, Ford ME. The linkage model for delivering mental health services
in rural communities: benefits and challenges. Health Soc Work 1998; 23 (1):
53-60
107. Munetz M, Bimbaum A, Wyzik P. An integrative ideology to guide community-
based multidisciplinary care of severely mentally ill patients. Hosp Community
Psychiatry 1993; 44 (6): 551-5
108. Burns BJ, Wagner HR, Taube JE, et al. Mental health service use by the elderly in
nursing homes. Am J Public Health 1993; 83 (3): 331-7
109. Gregoire A. Needs assessment for rural mental health services. In: Thornicroft G,
editor. Measuring mental health needs. 2nd ed. London: Royal College of Psy-
chiatrists, 2001: 435-53
About the Author: Fiona Judd is Professor of Rural Mental Health atMonash University in Victoria, and is Director of the Centre for Rural MentalHealth in Bendigo, Victoria, Australia. Her clinical and research interestsinclude anxiety and depression, effects of place in mental well being andmental disorders, development and evaluation of models of mental healthservice delivery to suit diverse rural locations.Correspondence and offprints: Fiona Judd, Centre for Rural Mental Health,Bendigo Health Care Group, Australia, PO Box 126, Bendigo, Victoria, Aus-tralia.E-mail: [email protected]
Rural Psychiatry 781
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 2002; 10 (12)