Embed Size (px)
Citation preview

Copyright 1986 by The Journal of Bone and Joint Surgery, Incorporated
Rupture and Displacement of theUlnar Collateral Ligament of the
Metacarpophalangeal Joint of the ThumbPREOPERATIVE DIAGNOSIS*’~
BY DEAN S. LOUIS, M.D.S, JULIUS J. HUEBNER, JR., M.D.-~, AND FRED M. HANKIN, M.D.-~,
ANN ARBOR, MICHIGAN
From the Orthopaedic Hand Service, University of Michigan Hospitals, Ann Arbor
ABSTRACT: The evaluation and treatment of injuriesof the ulnar collateral ligament of the metacarpopha.langeal joint of the thumb remain controversial. In aretrospective study that was done to assess our abilityto determine whether displacement of the ligament (aStener lesion) was present, we reviewed our accumulated[experience with patients who had an injury of this lig..ament who were treated surgically between 1972 and1984. Since our method of evaluation changed in 1977,we compared the preoperative and operative diagnosesin the twenty patients who were treated surgically from1972 through 1976 with those in the twenty patients whowere so treated from 1977 through 1984.
Considering all forty patients who were treated op-eratively, sixteen (40 per cent) had a typical Stener le-sion, and in two others (5 per cent) the ulnar collateralligament was rolled up ~on itself and lying beneath theadductor aponeurosis. From 1972 through 1976, stabil-ity was tested with the metacarpophalangeal joint incomplete extension or in varying amounts of flexion. Ofthe twenty thumbs that were evaluated by this techniqueand.were treated surgically, 20 per cent had a Stenerlesion. From 1977 through 1984, stability was tested withthe joint in full flexion because of the findings in ana-tomical stfidies that were completed in 1977; the inci-dence of a Stener lesion in the twenty thumbs that weretreated by repair or reattachment of the ligament duringthis time was 70 per cent.
We believe that when no fracture is present, aproper physical examination of an injured thumb is suf-ficient to determine the degree of instability of the ulnarcollateral ligament, and that a five-stage grading systemof injuries that appear to involve the ulnar side of themetacarpophalangeal joint of the thumb is helpful inseparating them into operative and non-operativegroups.
* No benefits in any form have been received or Will be received froma commercial party related directly or indirectly to the subject of this article.No funds were received in support of this study. "
~" Read at the Annual Meeting of the American Orthopaedic Asso-ciation Residents’ Conference, Los Angeles, California, May 1, 1986.
~: 2912 Taubman, Box 0328, University of Michigan Hospitals, AnnArbor, Michigan 48109.
Despite numerous recent reports on injuries of the ulnarcollateral ligament of the metacarpophalangeal joint of thetJhumb~22, controversy persists regarding management. Thisconcerns what constitutes an appropriate evaluation of sta-bility, the relationship between the extent of the specificanatomical injury and the resultant laxity of the joint, andthe indications for surgical or non-surgical treatment of acuteinjuries.
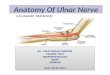
There is general agreement that all patients who havea displaced fracture that involves the attachment of the ulnarcollateral ligament should be treated surgically to restorethe integrity of this ligament, as well as to restore the normalarchitecture of the joint when the articular surface is in-wglved. The controversy about management has largely cen-tered on injuries in which no fracture is present and themetacarpophalangeal joint is unstable during stress-testing.Irt 1962, Stener described the interposition of the adductoraponeurosis between the distal site of attachment of theruptured ulnar collateral ligament and the detached ligament(Fig. 1). Since then, some authors have maintained thatbecause of the possibility that this lesion may be present,all[ thumbs that have such an injury should be explored toensure that the ligament is reattached at the propersiteI’3’1°’11’14A7’~°. Others, however, have concluded thatclosed treatment is satisfactory for all of these injuries, andhave reported excellent results~. Bowers and Hurst, on theother hand, in a review of the literature that was publishedin 1977, found a rate of failure of 50 per cent after treatmentby closed means.
Irl 1977, Palmer and Louis~6 described their findingsfrom an anatomical study of twenty-five fresh cadaverthumbs and a clinical study of 750 normal thuml~s. The twostudies complemented each other, delineating the range andva~:iability of motion in the normal human thumb and thedegree to which the various supporting soft tissues are re-sponsible for the stability of the metacarpophalangeal joint.The anatomical study demonstrated that the ulnar collateralligament is the major stabilizing element on the ulnar sideof the thumb. In full extension (zero degrees) of the meta-carpophalangeal joint of the intact thumb, the average radialdeviation was 4 degrees when the metacarpal of the thumbwas stabilized and a radial-deviation force was applied to
1320THE JOURNAL OF BONE AND JOINT SURGERY

RUPTURE AND DISPLACEMENT OF THE ULNAR COLLATERAL LIGAMENT 1321
E.P.L. C.L. A.A.
FIG. 1Diagram of a Stener lesion, showing the collateral ligament excluded
from its normal site of attachment on the proximal phalanx by interpositionof the adductor aponeurosis. E.P.L. = extensor pollicis longus, C.L. =collateral ligament, A.A. = adductor aponeurosis, A.T. = adductor ten-don, and Add. = adductor muscle. (Reproduced with permission fromPalmer, A. K., and Louis, D. S.: Assessing Ulnar Instability of the Meta-carpophalangeal Joint of the Thumb. J. Hand SUN., 3: 544, 1978.)
the proximal phalanx. When the thumb was similarlystressed while the metacarpophalangeal joint was in fullflexion, no radial displacement could be demonstrated. Itwas also found that when the adductor aponeurosis, thedorsal part of the capsule, and the ulnar collateral ligamentwere cut, at least 35 degrees of radial deviation was possiblein all specimens during stress-testing with the metacarpo-phalangeal joint in full flexion. However, when the samespecimens were tested with the joint in full extension or 15degrees of flexion, the joint was more stable. The greaterstability under these circumstances (full extension or 15degrees of flexion) was thought to be due to the normaltautnes..s of the volar plate when the joint was extended ascompared with its laxity during full flexion. When both thevolar plate an.d the ulnar collateral ligament were cut, thejoint could be angulated more than 90 degrees by radialstress in any :position of flexion or extension.
The study of 750 normal thumbs demonstrated con-siderable variation in the amounts of flexion and extensionof the metacarpophalangeal joint. The average total arc ofmotion of the metacarpophalangeal joint was 45 degrees inthese thumbs. The curve of distribution for the total arc ofmotion was bimodal, reflecting the hypermobility of indi-viduals with so-called double-jointed metacarpophalangealjoints in the thumb. More importantly, however, Palmerand Louis ~6A7 demonstrated that when the metacarpophalan-geal joint of these normal thumbs was stressed radially infull flexion, the average radial displacement that was pos-sible was only 1 degree, as compared with an average of 6degrees when the joint was in full extension and an averageof 12 degrees when it was in 15 degrees of flexion. Basedon these studies and on observations of patients who hadan injury of the metacarpophalangeal joint of the thumb, anew classification of injuries to the ulnar side of this joint
and a new method for their evaluation were developed andapplied to all patients who had this injury who were seenduring 1977 and thereafter.
In 1977, Palmer and Louis published a classificationof these injuries in which there were four types~6. Louislater came to the conclusion, from his accumulated exper-ience, that there are five distinct patterns of injury thatappear to involve the ulnar side of the metacarpophalangealjoint of the thumb. In Type I, there is an undisplaced fractureon the ulnar side of the base of the proximal phalanx (Fig.2) and in Type II, there is a displaced fracture in the samelocation in the proximal phalanx (Fig. 3). In Type III, thereis no fracture and the joint is stable (angulates tess than 35degrees) when it is stressed radially in full flexion. In TypeIV, there is no fracture but the joint angulates more than35 degrees when it is stressed radially in full flexion, im-plying complete disruption of the ulnar collateral ligament,as demonstrated by the anatomical studies of Palmer andLouis 16’17. Type V, which is easily confused with Types Iand Ill and must be differentiated from them by a carefulphysical examination, is, in fact, an avulsion of a portionof the volar plate with an attached piece of the proximalphalanx, and not an avulsion of the ulnar collateral ligament.This ]:esion is identified clinically by the presence of ten-derne:ss and swelling located volarty in the area of the at-tachment of the volar plate to the proximal phalanx and bythe position of the fragment on the volar rather than on theulnar aspect of the phalanx, as seen on the lateral radiograph(Fig. 4). In addition, after a regional anesthetic block, therrletacarpophalangeal joint of a thumb with a Type-V injuryis stable when it is stressed in full flexion.
The purpose of this retrospective review of our exper-ie, nce was to determine the frequency of the Stener lesionin thumbs that were treated surgically for a fracture or in-stability after injury to the ulnar side of the metacarpo-phalangeal joint and to compare the frequency of this lesionin the thumbs that were operated on before 1977 with itsfrequency in the thumbs that were treated operatively afteradoption of the new classification and new method of eval-uation in 1977.
Materials and Methods
From 1972 to 1984, forty patients were treated sur-gically at the University of Michigan Hospitals for an acuteinjury to’ the ulnar aspect of the metacarpophalangeal jointof the thumb. We reviewed the medical records, operativenotes, and pertinent radiographs of these forty patients. Suf-ficient data were available to fulfill the aforementioned lim-ited objectives of this study. Assessment of the results ofsurgical and non-surgical management after the twelveweeks or more that these patients were followed was notpossible because so many of the patients had been studentswiho could not be located at the time of this study.
Thirteen male and seven female patients were operatedon for instability of the metacarpophalangeal joint or a dis-placed fracture before 1977. The average age was 22.5 years(range, fourteen to twenty-nine years). The right thumb was
VOL. 68-A, NO. 9, DECEMBER 1986

1322 D. S. LOUIS, J. J. HUEBNER, JR., AND F. M. HANKIN
FIG. 2 F~G. 3 FIG. 4Fig. 2: A Type-I lesion. Note the undisplaced fracture at the base of the proximal phalanx on the ulnar side of the metacarpophalangeal joint. Injuriesof this nature, we believe, can be treated by closed means.
Fig. 3: A Type-II lesion. Note the displaced fracture at the base of the proximal phalanx. Obviously, open reduction is required to re-establish thecongruity of the joint and the integrity of the ligament.
Fig. 4: A Type-V lesion, not a Type-II injury. Note the avulsion of the phalangeal attachment of the volar plate. The joint is lax in extension butstable in full flexion, a finding that differentiates a lesion of the volar plate from a tear of the ulnar collateral ligament.
injured in fourteen patients and the left, in six. The pre-operatiye evaluation included plain radiographs to determinewhether there were any fractures and clinical stress tests todemonstrate a..ny complete tears of the ulnar collateral lig-ament. The radiographs sho’~ed no fracture in eight thumbsand a fracture of the base of the proximal phalanx in twelve.Of the twelve patients who had a fracture, eight had a smallchip fracture that appeared to be an avulsion of the insertionof the ulnar collateral ligament with an attached piece ofbone. The other four fractures involved more than one-thirdof the articular surface of the proximal phalanx, and all butone of these patients were less than seventeen years old.All twelve fractures were displaced, corresponding to theType-I! injury in the classification that was used in the latergroup.
To perform the stress tests from which a preoperativediagnosis of a complete tear of the ligament was made inthis group, radial stress was applied to the thumb with the
metacarpophalangeal joint in full extension and in varyingdegrees of flexion, with no attempt to control axial rotationof the metacarpal during testing. A diagnosis of a completetear was made when the laxity of the injured joint wasconsidered to be significantly more than the laxity of the
joint :in the opposite thumb, but no consistent criteria orspecified amount of radial deviation was used to judge-thepresence or absence of a complete tear. In addition, sixpatients were evaluated by radiographic stress examinationswith the metacarpophalangeal joint in full extension, andan abnormal radiograph was the primary indication for sur-gical treatment. For two of these patients stress radiographsweremade despite the fact that a displaced fracture wasvisible: on plain radiographs.
The .literature at that time provided no guide to theappropriate method for clinical evaluation when rupture ofthe ulnar collateral ligament of the metacarpophalangealjoint of the thumb was suspected. Our aggressive surgicalapproach was based on our knowledge of Stener’s work in1962 and on the presumption that the displaced ulnar col-lateral ligament would not function effectively unless thenormal anatomy was restored surgically. However, whenwe compared the incidence of a Stener lesion of 20 per centin .our patients who were seen from 1972 through 1976 withthe incidence of 64 per cent that Stener reported, we wereconcerned that we were not differentiating lesions thatshould be treated surgically from those that should be treatednon-surgically, and that we were operating on thumbs that

RUPTURE AND DISPLACEMENT OF THE ULNAR COLLATERAL LIGAMENT
might have done just as well with non-operative tkeatmentbecause the ligaments were disrupted but not displaced. Itwas then that we changed our management of these injuries,based on the previously described findings of Palmer andLouis16,~7.
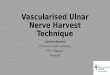
Beginning in 1977, all patients who had an acute injuryto the ulnar aspect of the metacarpophalangeal joint of thethumb were treated according to the following protocol,which we continue to use. For all patients who give a historyof such an injury prior to any clinical examination, plainanteroposterior and lateral radiographs are made. If there isa non-displaced fracture (Type I), the thumb is immobilizedwith the metacarpophalangeal joint in full extension for fourweeks. If there is a displaced fracture on the ulnar aspectof the base of the proximal phalanx (Type II), operativereduction or excision of the fragment with reattachment ofthe ligament is performed. If there is no evidence of fracture,the median and radial nerves are anesthetized at the wrist.Then, while the metacarpal head is grasped between thethumb and index finger of the examiner’s non-dominanthand, the metacarpophalangeal joint is flexed completelyand passive radial deviation is attempted while the examinerholds the proximal phalanx with his or her dominant hand(Fig. 5). If resistance is felt as radial deviation of the thumb(to less than 35 degrees) is attempted, it is assumed that thepatient has a so-called strain of the ligament (Type III),rather than a complete tear, and a spica cast is applied tothe thumb with the metacarpophalangeal joint in extension.This is worn for three weeks to allow the ligament to heal.
1323
If the., joint angulates without resistance and to more than35 degrees as it is stressed, a diagnosis of a complete avul-sion or tear of the ulnar collateral ligament (Type IV) established. We believe that this lesion should be treatedsurgically, since the presence of a Stener lesion cannot beruled out preoperatively. In our experience, when there isno evidence of a fracture after this injury, the results of theclinical test are usually not equivocal, since the metacar-pophalangeal joint either opens widely or does not open atall.
Frora 1977 through 1984, twenty patients were treatedsurgically according to the aforementioned protocol. Therewere thirteen men and seven women, and the average agewas 32.5 years (range, twenty-one to fifty-eight years). Theright thumb was injured in nine patients and the left, inelew~n. There were seven Type-II, one Type-HI, and twelveType-IV injuries, as determined by our preoperative eval-uation. The one Type-III injury that was treated surgicallyoccurred in the dominant thumb of a surgical resident whorequested surgical treatment even though only 25 degreesof radial deviation was possible when the metacarpopha-langeal joint was stressed in full flexion. In none of theType-II injuries did the fracture involve more than one-thirdof the surface of the proximal phalanx ..No stress radiographswere made for these twenty patients, but a positive arthro-gram of the metacarpophalangeal joint of one patient witha Type-IV injury supported the findings by clinical stress-testing. Five other patients (who were not treated surgicallyand not included in the series) were evaluated under regional
FIG. 5
d to test for instabilit of the ulnar coliateral ligament of the |humb~. With the carpometacarpal joint initially in a position ofThe proper metho . Y .............. ,a..~ ~,f the metacam 1 head The oroximal l~halanx is then grasped asc al Is stabilized b ras lng it just proxlmat to the cut~uytco ~. ............. ra - - - ,,extension, the meta arp Y g P ...... : ...... the collateral li ament is intact,
shown, and the stability of the metacarpophalangeal joint ~s tested first w~th the joint ~n full flexion. In this posmon, ffg
the joint will not open. However, if the joint is held in a position of less than the maximum obtainable passive flexion, there may be some laxitynormally. In the fully extended position, there is normally some laxity of the ulnar collateral ligament, the average excursion being 6 degreestT. If thefully extended joint is tested for laxity, and there is only an injury of the volar plate, there will’be marked laxity of as much as 30 degrees. However,when the same joint is tested in flexion, it will be stable, since the ulnar collateral ligament is intact. (Reproduced with permission from Palmer, A.K., and Louis, D. S.: Assessing Ulnar Instability of the Metacarpophalangeal Joint of the Thumb. J. Hand Surg., 3: 545, 1978.)

1324 D. S. LOUIS, J. J. HUEBNER, JR., AND F. M. HANKIN
anesthesia in the operating room and examined by one ofus (D. S. L.). They were found to have a Type-III injuryand were therefore not treated surgically. Unfortunately, noadditional data are available regarding the remaining pa-tients who were seen between 1977 and 1984 and who wereconsidered to have a Type-I, III, or V injury. All of thepatients in the later group who were treated non-operativelyhad a stable thumb when they were last seen.
Results
Of the twenty patients who had an injury of the ulnarcollateral ligament that was treated surgically between 1972and 1976, eight did not have an associated fracture. Twoof these had a rapture of the distal part of the ulnar collateralligament with a classic Stener lesion, while the other sixhad complete disruption of the ulnar collateral ligament butno displacement. Of the six ligaments that did not show aStener lesion, four were torn from the attachment to theproximal phalanx and two were a mid-substance rupture.
Of the twelve patients who had a fracture that wastreated surgically before 1977, eight had a chip-type avul-sion fragment that was displaced from its original position,and four had a fragment that involved more than one-thirdof the joint surface. Of the eight chip-type fragments, onewas associated with a Stener lesion. In the other seventhumbs, the ulnar collateral ligament was detached from itsattachment to the proximal phalanx in all seven, the frag-ment of bone remained attached to the ulnar collateral lig-ament in six, and the fragment was attached only to synovialtissue in one. Of the four patients who were treated sur-gically and had a significant articular fragment, one hadassociated displacement of the ligament as described byStener and in three the fragment was displaced sufficientlyto distort the normal architecture of the joint, but none ofthe ligaments was rolled back on itself.
~The eight patients who did not have an associated frac-ture and the eight patients who had a small avulsion fracturewere treated by primary repair or reattachment of the lig-ament to the proximal phalanx; depending on the locationof the injury. The other four patients, all of whom had amajor articular fragment, were treated with open reductionand internal fixation using Kirschner wires. This restoredthe integrity of the ulnar collateral ligament, which wasattached to the fragment of the fracture. All twenty thumbswere immobilized in a spica cast with the metacarpopha-langeal joint in extension for six to seven weeks. There wereno complications. When these patients were last seen, threeto four months postoperatively, all of the thumbs were stableon examination and were free of pain, but four of the patientshad mild complaints of stiffness.
of the twenty injuries that were treated surgically from1977 through 1984, seven were classified as Type II; one,as Type HI; and twelve, as Type IV, based on the preop-erative evaluations. Of the twelve Type-IV injuries, elevenwere a complete disruption of the ulnar collateral ligamentand one was not a complete disruption, but at operation theulnar collateral ligament and capsule of the joint were found
to be attenuated and redundant. In the eleven thumbs thathad a complete disruption there were six typical Stenerles:ions, two ligaments that were rolled up and lying underthe adductor aponeurosis, two ligaments that were torn com-pletely from their attachment to the proximal phalanx butwe:re not displaced, and one mid-substance rupture.
In the patient with a Type-III injury who requestedope.rative treatment, a 50 per cent rupture of the mid-portionof the ulnar collateral ligament was found and was treatedby primary repair. Immobilization alone probably wouldhave been adequate for this patient.
Of the seven Type-II fractures (with a displaced chip-type avulsion fragment), none involved a significant portionof the articular surface. Six of these fractures were asso-ciated with a typical Stener lesion. The seventh, which wasnot associated with a Stener lesion, was operated on threeweeks after injury because the fragment was displaced. Atoperation, the fragment was noted to be healing well to the
¯ proximal phalanx and there was no significant laxity, despitethe abnormal position. This patient was treated simply bysurgical exploration and subsequent immobilization, whilethe patient with the redundant ulnar collateral ligament andcapsule was treated by reefing of these structures, followedby immobilization. The other eighteen patients were treatedby repair or reattachment of the ligament, followed by im-mobilization in a thumb-spica cast with the metacarpo-pha]tangeal joint held in extension for four to six weeks.
Postoperatively, one patient in this group had persistentanesthesia on the ulnar aspect of the thumb, presumablydue to accidental injury of the ulnar digital nerve at the timeof c,peration..When these twenty patients were last seen,three to twelve months after repair, none had any evidenceof instability of the metacarpophalangeal joint and all werefree of symptoms. Two patients had mild stiffness of thethumb.
Discussion
When a patient who has an acute injury to the ulnaraspect of the metacarpophalangeal joint of the thumb is firstseen, the surgeon must decide if the joint is unstable andwhether surgical repair is required to restore stability. Whenthe ulnar collateral ligament is torn and displaced, with
interpo.sition of the adductor aponeurosis as described byStener, stability can be restored only by surgical repair.Stener described this lesion in twenty-five of thirty-nine.patients, or 64 per cent of the patients whom he operated,on..In some, but not all, of these patients there was anassociated avulsion fracture. He concluded that displace-ment of the ruptured ligament cannot be ruled out beforeoperation, and this key point is supported by the evidencein our study. Stener did not specify the indications for sur-gical treatment, and no additional details concerning theiinjuries in his patients are available. Several authors havesubsequently reported incidences of surgically proved Stenerlesions that have ranged from 15 to 52 per cent, and theyused a variety of indications for surgical treatment3,13,1~,~9.
]in our patients, in whom the status of the ulnar collateral

RUPTURE AND DISPLACEMENT OF THE ULNAR COLLATERAL LIGAMENT
ligament was proved by operative exposure, we attemptedto determine whether an appropriate physical examinationand radiographs provide an accurate and reliable way ofdetermining whether surgical treatment is indicated.
Based on the anatomical studies of Palmer andLouis16’17 and on our clinical experience, presented here, webelieve that acute injuries of the ulnar collateral ligamentcan be divided into four types that can be identified byclinical and radiographic examination, and that the appro-priate treatment can be selected according to the type. Afifth type of injury is included because avulsion of the volar
TABLE I
SuggestedInjury Examination Treatment
Type I Undisplaced fracture No stress Cast for 4 wks.
Type II Displaced fracture Unknown Operative reduction
Type III No fracture Stable in Cast for 3 wks.flexion
Type IV No fracture Unstable in Operative repairflexion
Type V Avulsion fracture of Stable in Castfor 4 wks.the volar plate flexion
plane with an attached piece of bone may easily be mistakenfor a Type-II injury on the basis of radiographs. This is not,however, an injury of the ulnar collateral ligament, and theimplications for treatment are different. Table I lists the fivetypes of injury and the treatment that we prefer for eachtype at the time of writing.
As shown by the findings in this study, our ability todiagnose the Stener lesion improved by 50 per cent after1977, when we began to follow the protocol that we have
1325
described. Two questions remain, however. First, since allpatients who did not have a fracture and were treated sur-gically from 1972 through 1976 had complete disruptionsof ~the ulnar collateral ligament, and presumably would havebeen classified as having a Type-IV injury if they had beenexamined according to our present protocol, why was theirincidence of a Stener lesion only 25 per cent (two of eight),whereas in the later group the incidence was 70 per cent?Once possible explanation is that these joints were so unstablethat displacement of a previously disrupted but undisplacedligament occurred during the type of stability testing thatwas performed in the later group. Second, why did theincidence of a Stener lesion in thumbs that had a displacedchip-type avulsion fracture increase from 13 per cent (oneof eight) to 86 per cent (six of seven) between the earlierand later groups? There is no obvious explanation for this.
We cannot yet establish the validity of our presentmanagement protocol because we do not have documenteddata on the results in the thumbs of all patients who weretreated according to the protocol for each type of injury,and then were followed for long enough to establish theresult. However, the incidence of a Stener lesion amongType-II lesions of 86 per cent (six of seven) and the inci-dence among Type-IV lesions of 66 per cent (eight oftwelve) suggest strongly that all patients who have this typeof injury should undergo repair of the ligament. We antic-ipate that appropriate treatment for all injuries to the ulnaraspect of the metacarpophalangeat joint of the thumb canbe. determined by using this simple protocol and the clas-sification that we have described. In order to establish thevalidity of this suggestion, we are now beginning both aprospective and a retrospective study of patients who weretreated according to this protocol.
References
1. ~ALLDRED, A. J.: Rupture of the Collateral Ligament of the Metacarpo-Phalang~al Joint of the Thumb. J. Bone and Joint Surg., 37.B(3):_4~43-445,1955.. ’
2. BADLY; .R.A.J.: Some Closed Injuries of the Metacarpo-Phalangeal Joint of the Thumb. In Proceedings of the South-West Orthopaedic Club. J.Bone and Joint Surg., 45-B(2): 428-429, 1963.
3. BOWERS, W. H., and HURST, L. C.: Gamekeeper’s Thumb. Evaluation by Arthrography and Stress Roentgenography. J. Bone and Joint Surg.,59-A: 519-524, June 1977.
4. CAMPI~ELL, G. S.: Gamekeeper’s Thumb. J. Bone and Joint Surg., 37-B(D: 148-149, 1955.5. COOr~R~, R. W., and GOLDNER, J. L.: A Study of the Pathological Findings and Treatment in Soft-Tissue Injury of the Thumb Metacarpophalangeal
Joint. With a Clinical Study of the Normal Range of Motion in One Thousand Thumbs and a Study of Post Mortem Findings in LigamentousStructures in Relation to Function. J. Bone and Joint Surg., 50-A: 439-451, April 1968.EATON, R. G., and DR~¥, G. J Dislocations and Ligament Injuries in t]he Digits. In Operative Hand Surgery, edited by D. P. Green. Vol. 1,p. 659. New York, Churchill Livingstone, 1982.FR~, W. E., and DO~¥NS, JAMES: Surgical Pathology of Collateral Ligamentous Injuries of the Thumb. Clin. Orthop., 83:102-114, 1972.FRYKMAN, G., and JOaA~SSOr~, O.: Surgical Repair of Rupture of the; Ulnar Collateral Ligament of the Metacarpo-Phalangeal Joint of the Thumb.Acta Chir. Scandinavica, 112: 58-64, 1956.KA~’LAN, E. B.: Lateral Subluxation of the Metacarpophalangeal Joint of the Thumb. Experimental Study. Bull. Hosp. Joint Di~., 21: 217-228,1960. "KESSLER, I.: Complete Avulsion of the Ulnar Collateral Ligament of the Metacarpophalangeal Joint of the Thumb. Clin.. Orthop., 29: 196-200,1963.K~SSLER, I., and HELLER, J.: Complete Avulsion of the Ligamentous Apparatus of the Metacarpophalangeal Joint of the Thumb. Surg., Gynec.and Obstet., 116: 95-98, 1963.MOBERG, E., and ST~ER, B.: Injuries to the Ligaments of the Thumb and Fingers. Diagnosis, Treatment and Prognosis. Acta Chit. Scandinavica,106: 166-186, 1953. "MOGENSEN, B. A., and MATTSSON, H. S.:. Post-Traumatic Instability of the Metacarpophalangeal Joint of the Thumb. Hand, 12: 85-90, 1980.NEVIASER, R. J. ; WILSON, J. N. ; and LIEVA~O, ALVARO: Rupture of the Ulnar Collateral Ligament of the Thumb (Gamekeeper’ s Thumb). Correctionby Dynamic Repair. J. Bone and Joint Surg., 53-A: 1357-1364, Oct. 1971. .Os’rERIVlAN, A. L.; HAYNES, G. D.; and BORh, F. W., JR.: A Quantitative Evaluation of Thumb Function after Ulnar Collateral Repair andReconstruction. J. Trauma, 21: 854-861, 1981.PALMER, A. K., and Louis, D. S.: Gamekeeper’s Thumb. When is Surgery Necessary? Orthop. Trans., 1: 14-15, 1977.PALMER, A. K., and Louis, D. S.: Assessing Ulnar Instability of the Met~carpophalangeal Joint of the Thumb. J. Hand Surg., 3: 542-546, 1978.SMITH,’R. J.: Lateral Instability of the Metacarpophalangeal Joint of the Thumb. In Proceedings of the American Society for Surgery of the Hand.J. Bone and Joint Surg., 57-A: 729-730, July 1975.
7.8.
9.
11.
12.
13.14.
15.
16.17.18.
VOI. 6~-A. NO O, DECEMBER 1996

1326 D.S. LOUIS, J. J. HUEBNER, JR., AND F. M. HANKIN
19. SMITH, R. J.: Post-Traumatic Instability of the Metacarpoohalangeal Jc.int of "20. SrENER, BER’rIL: Displacement of the Ruptured Ulnar Collateral Ligament the Thumb. J. Bone and Joint Surg., S9-A: 14-21, Jan. 1977.
Anatomical Study. J. Bone and Joint Surg., 44-B(4): 869-879, 1962. of the Metacarpo-Phalangeal Joint of the Thumb. A Clinical and21. S’rRANDELL, Gt~NNAR: Total Rupture of the Ulnar Collateral Ligament of the Metacarpophalangeal Joint of the Thumb. Results of Surgery in 35
Cases. Acta Chir. Scandinavica, 118: 72-80, 1959.22. ZILBERMAN, Zwv; ROTSCHILD, ELIEZER; and KRAUSS, LUDWIG: Rupture of the Ulnar Collateral Ligament of the Thumb. J. Trauma, 5: 477-481,
1965.
Copyright 1986 by The Journal of Bone and Joint Surgery, Incorporated
Adolescent Idiopathic ScoliosisTreated by Harrington-Rod Distraction and Fusion* :
BY JEFFREY L. LOVALLO, M.D.~f, JOHN V. BANTA, M.D. I , AND THOMAS S. RENSHAW, M.D.S’, NEWINGTON, CONNECTICUT
From the Department of Orthopaedic Surgery., Newington Children’s Hospital, Newington
ABSTRACT: One hundred and thirty-three patientswho had adolescent idiopathic scoliosis were treated byinsertion of a single Harrington distraction rod andspinal fusion. Postoperative immobilization consisted ofsix months in a below-the-shoulder cast. The mean pre..operative curve was 50 degrees, with a range of 30 to.110 degrees. The mean final curve was 35 degrees, witha range of 19 to 63 degrees. There were no neurologicalinjuries and no deep wound infections. Twelve patientsrequired further surgery for complications, all of whichwere treated successfully. The duration of follow-upranged from twenty-four to seventy-two months. At finalfollow-up, all patients had resumed their normal pre-operative activities without limitations.
For more than twenty years, posterior spinal fusionwith HalTington-rod instrumentation has been the surgicaltreatment of choice for adolescent idiopathic scoliosis inmany centers. Since Harrington reported the early results,the popularity of this procedure has increased~a2. Its ad-vantages compared with .other methods are low rates ofmorbidity: and mortalityT,9.’oaz and few long-term compli-cations. However, in patients who have had a fusion thatextended to the lower part of the lumbar spine or the pelvis,there have been problems such as iatrogenic fiat back andlow-back pain~,8.
Since 1976, more complex procedures, such as seg-mental spinal instrumentation with sublaminar wiring, havebecome increasingly popular in the treatment of certain pa-tients who have scoliosis, including those who have ado-lescent idiopathic scoliosis. We therefore reviewed ourrecent experience with spinal fusion using Harrington-rodinstrumentation in patients who were treated at Newington
* No benefits in any form have been received or will be received froma commercial party related directly or indirectly to the subject of this article.No funds were received in support of this study.
~" Department of Orthopaedic Surgery, Newington Children’s Hos-pital, 181 East Cedar Street, Newington, Connecticut 06111. Please ad-dress requests for reprints to Dr. Renshaw.
Children’s Hospital for idiopathic scoliosis. The purpose oftl~e study was to compare our results with this techniquewith those reported in the literature for the more complicatedprocedures that are used to treat adolescent idiopathic sco-liosis (excluding severe curves).
Materials and MethodsIn a retrospective study, the cases of patients who had
adolescent idiopathic scoliosis and were treated by instru-mentation with a single Harrington distraction rod and au-togenous bone-grafting at Newington Children’s Hospitalfrom October 1, 1978, to December 31, 1982, were re-viewed. The chart and radiographs of each patient werestud.ied. Only patients who had a minimum follow-up oftwo years were included. A total of 179 patients who hadadolescent idiopathic scoliosis were treated by surgery dur-¯
,~ this period of time. One hundred and sixty-eight p_~tientsln~were treated with Harrington-rod instrumentation andeleven, with Luque-rod instrumentation that was attachedto the spine by sublaminar wiring.
Thirty-five patients, all with Harrington-rod instru-mentation, were lost to follow-up~ Sixty-five patients werefollowed for less than three years, fifty-five were followedfor three to five years, and thirteen were followed for morethan five years. The mean length of follow-up was forty-four rfionths (range, twenty-four to seventy-two months).The operations were performed by six different surgeons.
Of the 133 patients who were treated by Harringtoninstrumentation, in 130 the indication for surgery was pro-gressive idiopathic scoliosis of more than 40 degrees andan age of at least ten years. The other three patients had arapidly progressing curve that had not yet reached 40 de-gree.s. In the eleven patients who were treated with Luque-rod instrumentation and sublaminar wiring, this strongersystem:6 "was thought to be preferable to the Harringtoninstrumentation for several reasons¯ Seven patients had pro-four, td or morbid obesity, and therefore a system with greaterstrength of internal fixation was indicated; three patients hadsevere psychiatric problems, and it was believed that they