Embed Size (px)
Citation preview
PCOS – Where does it come from, where does it go to?
Roy Homburg
2
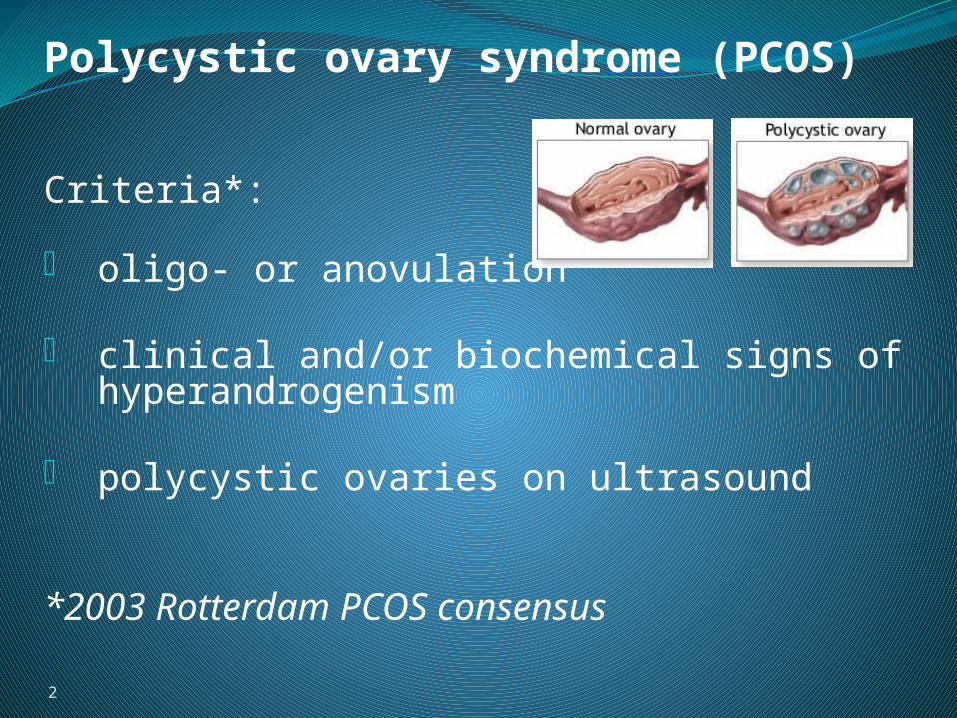
Polycystic ovary syndrome (PCOS)
Criteria*:
• oligo- or anovulation
• clinical and/or biochemical signs of hyperandrogenism
• polycystic ovaries on ultrasound
*2003 Rotterdam PCOS consensus

Barker hypothesis‘developmental origin of adult disease’
‘The womb may be more important than the home’

PCOS - Candidate Genes
PCOS is strongly familial
Genetically defined basis not found – almost all initial candidates failed to maintain linkage with PCOS phenotype
? inheritance is modified by environmental factors
? Re-programming of genes in utero.

Excess androgens in utero- defeminization of sexual functionPrenatal maternal testosterone levels –
dose-related link with gender role behaviour in pre-school girls (Hines et al, 2002)
Girls exposed to high levels of T pre-natally (CAH) show distinct masculine-type behavioral traits (Berenbaum & Hines, 1992)
Traits also correlate with T levels in amniotic fluid (Grimshaw et al, 1995)

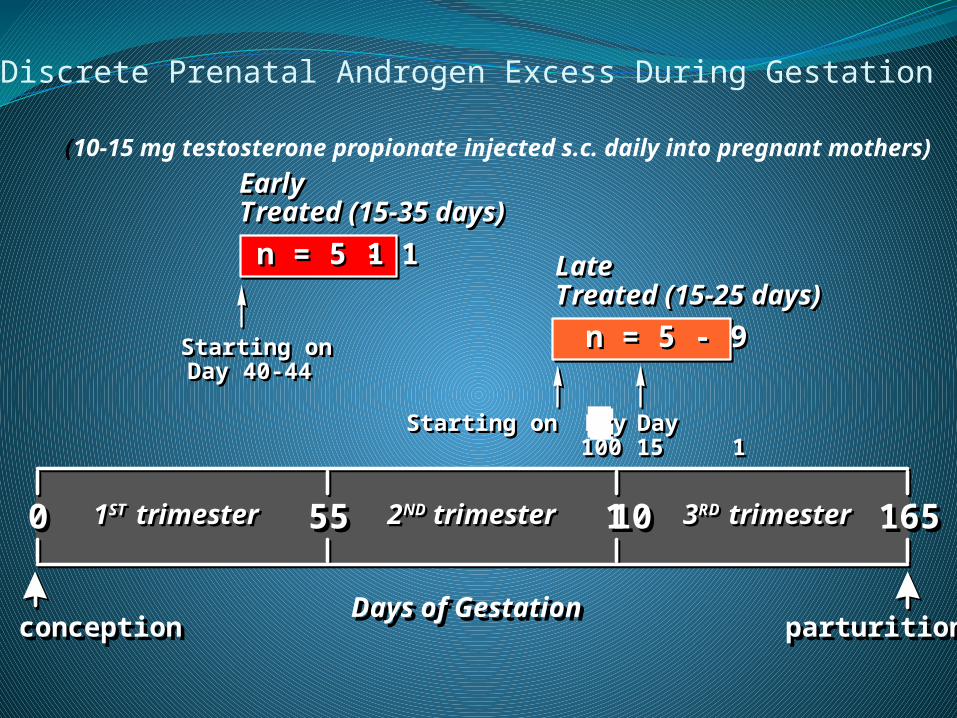
Discrete Prenatal Androgen Excess During Gestation
(10-15 mg testosterone propionate injected s.c. daily into pregnant mothers)
Early Treated (15-35 days)Early Treated (15-35 days)
Days of GestationDays of Gestation
165165 110 110555500
n = 5 - 11 n = 5 - 11
n = 5 - 9n = 5 - 9
Late Treated (15-25 days)Late Treated (15-25 days)
Starting on Day 40-44
Starting on Day 40-44
Starting on Day or Day 100 115
Starting on Day or Day 100 115
conceptionconception parturitionparturition
1ST trimester1ST trimester 2ND trimester2ND trimester 3RD trimester3RD trimester
0
0.1
0.2
0.3
0.4
0.5
40 60 80 100 120 140
Gestation days
0
4
8
12
16
20
24
28
32
36
ng
/ml
40 60 80 100 120 140
Gestation days
0
0.1
0.2
0.3
0.4
0.5
0 10 20 30
Postnatal days
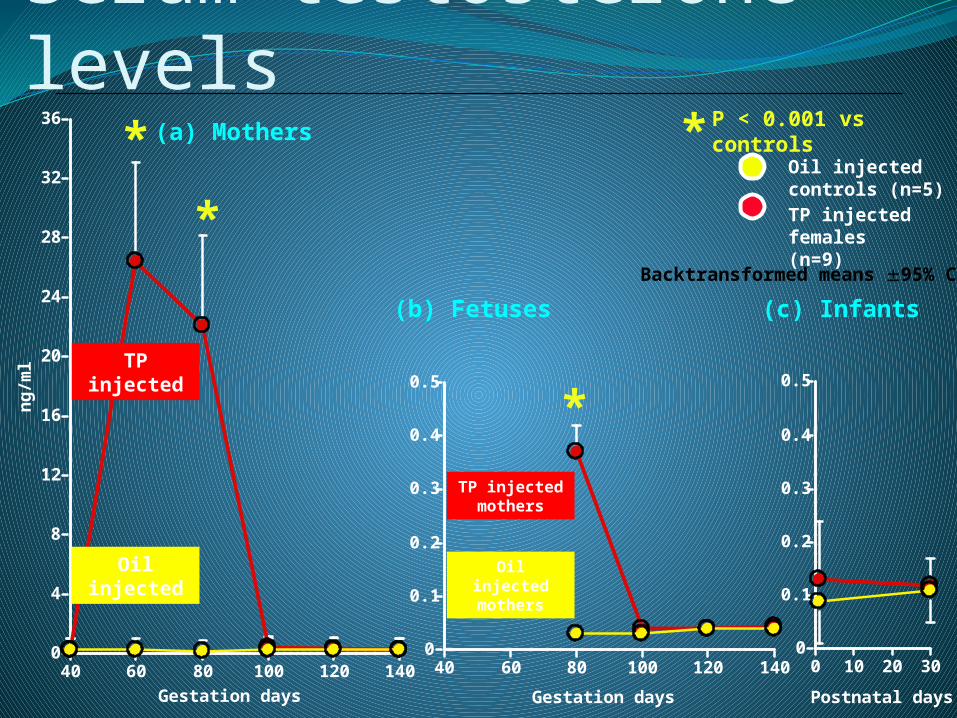
Serum testosterone levels
TP injected females (n=9)
Oil injected controls (n=5)
* P < 0.001 vs controls
TP injected
Oil injected
Backtransformed means 95% CI
(a) Mothers
(b) Fetuses (c) Infants
TP injected mothers
Oil injected mothers
*
*
*

Ovulatory menstrual cycles in control and prenatally androgenized females over a 6-month period
7 *†
p < 0.02 vs. controls
p < 0.03 vs. controls
Control females( n = 6)
Early PA females ( n = 6 )
Late PA females( n = 5 )
0
1
2
3
4
5
6
*†
Number of cycles per six month period
Late-treated(n = 3)
0
5
10
15
20
25
30
35
ng/ml
Controlfemales(n = 24)
Early-treated(n = 10)
prenatally androgenizedfemales
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
ng/ml
Controlfemales(n = 5)
Early-treated(n = 4)
Late-treated(n = 5)
prenatally androgenizedfemales
Late-treated(n = 3)
0
5
10
15
20
25
30
35
ng/ml
Controlfemales(n = 24)
Early-treated(n = 10)
prenatally androgenizedfemales
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
ng/ml
Controlfemales(n = 5)
Early-treated(n = 4)
Late-treated(n = 5)
prenatally androgenizedfemales
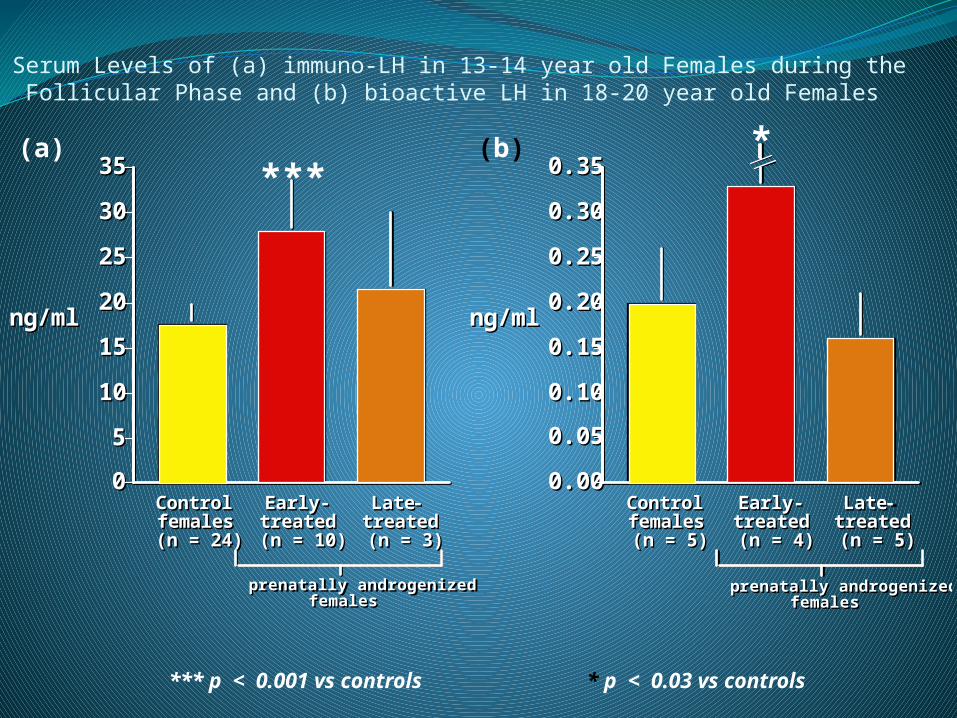
Serum Levels of (a) immuno-LH in 13-14 year old Females during the Follicular Phase and (b) bioactive LH in 18-20 year old Females
***
*** p < 0.001 vs controls
*
* p < 0.03 vs controls
(a) (b)

In the beginning…. A excess in utero Programming of
PCOS
Insulin + LH Pre/small antral Thecal follicle number enzymesserine phosphorylation
Androgen excess

Hypothesis for Prenatal Androgen Programming of Females for PCOS
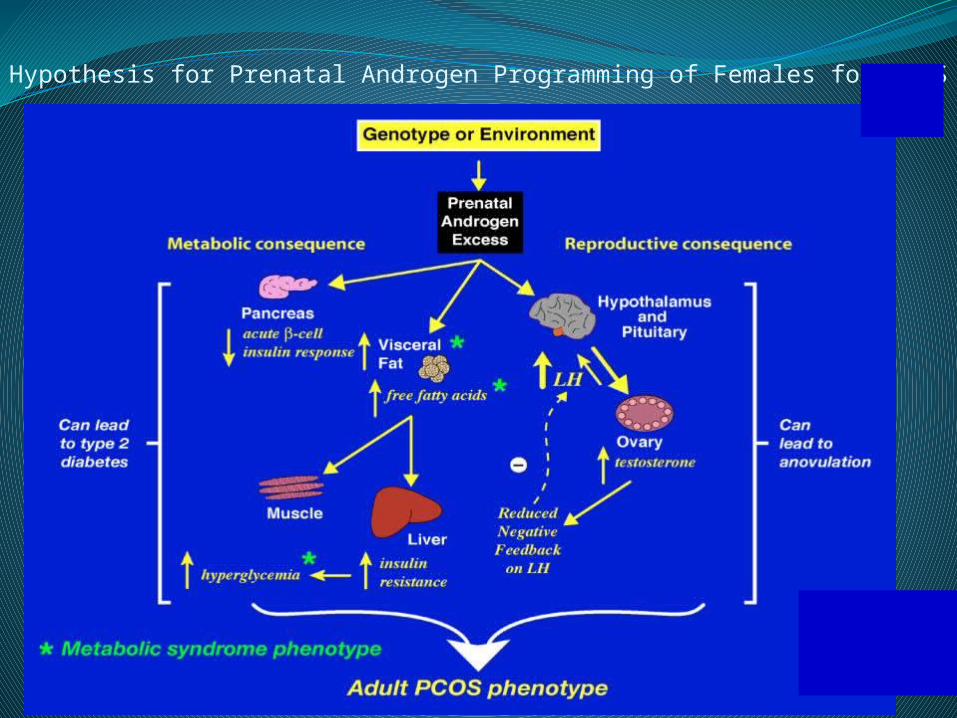
Hypothesis for Prenatal Androgen Programming of Females for PCOS
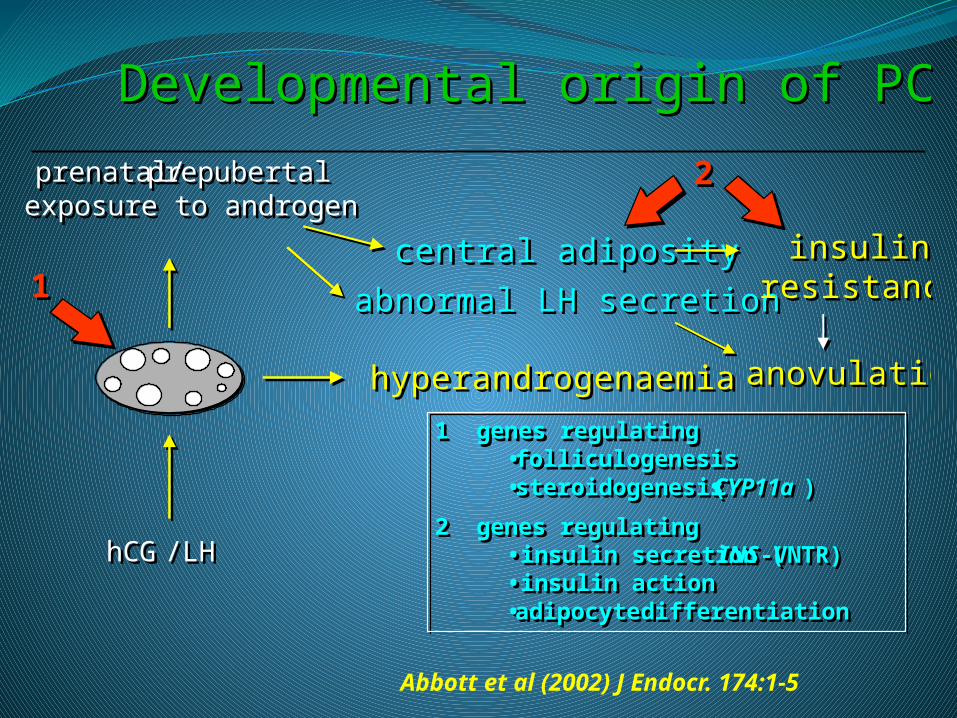
Developmental origin of PCOS
prenatal/prepubertalexposure to androgen
hCG/LH
hyperandrogenaemia
central adiposity
abnormal LH secretion
insulinresistance
2
1
1 genes regulating•folliculogenesis•steroidogenesis (CYP11a )
2 genes regulating•insulin secretion ( INS-VNTR)•insulin action•adipocyte differentiation
anovulation
Developmental origin of PCOS
prenatal/prepubertalexposure to androgen
hCG/LH
hyperandrogenaemia
central adiposity
abnormal LH secretion
insulinresistance
2
1
1 genes regulating•folliculogenesis•steroidogenesis (CYP11a )
2 genes regulating•insulin secretion ( INS-VNTR)•insulin action•adipocyte differentiation
anovulation
Abbott et al (2002) J Endocr. 174:1-5
16
Androgens in girls with PCOS mothers
Does prenatal exposure to androgens cause PCOS?
Origin of androgens in PCOS women:
• Maternal origin placental passage during gestation
• Fetal origin is the fetus making the androgens?
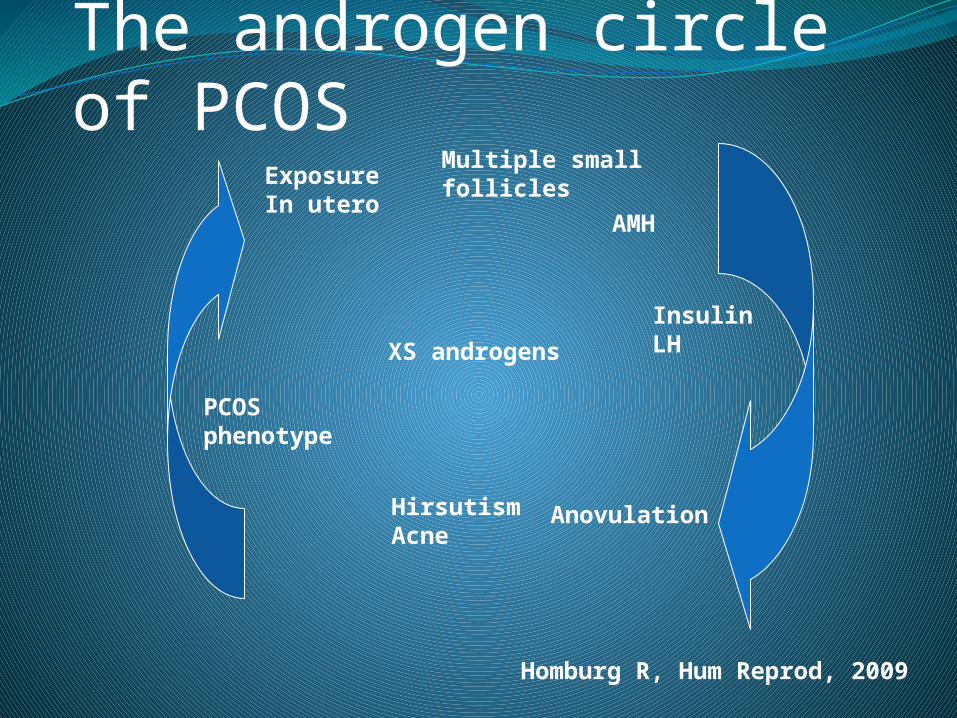
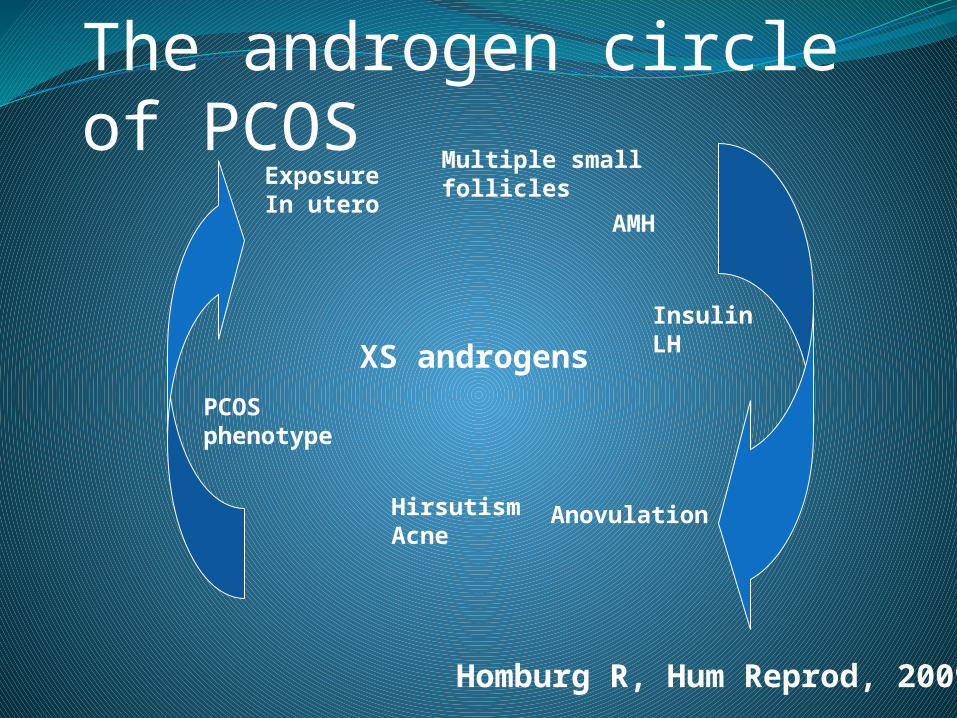
The androgen circle of PCOS
XS androgens
Exposure In utero
Multiple smallfollicles
InsulinLH
AMH
AnovulationHirsutismAcne
PCOSphenotype
Homburg R, Hum Reprod, 2009
One in every five women
has polycysticovaries.
Polycystic Ovary Syndrome(PCOS)About 20% of the female population have polycystic ovaries.
5-10% of the female population suffer from symptoms.
Manifestations of PCOSMenstrual
disturbance Hirsutism
Acne Infertility
Obesity
High LH
High Testosterone
Hyperinsulinemia
Ultrasound appearance

Manifestations of PCOSMenstrual
disturbance (66%)Hirsutism (66%)
Acne (35%)Infertility (75%)
Obesity (38%)
LH up (40%)T up (30%)
Insulin up - in obese 80%
- in slim 30-40%
RANGE OF PCOS
I_______________________________I
NORMAL OVULATORYCYCLES, MILD HIRSUTISM
AMENORRHEAHIRSUTISM/ACNEINFERTILITYOBESITY

* The fundamental disturbance of PCOS involves a primary lesionin the ovary.
* The expression of the lesion is determined in part by extra-ovarian factors.
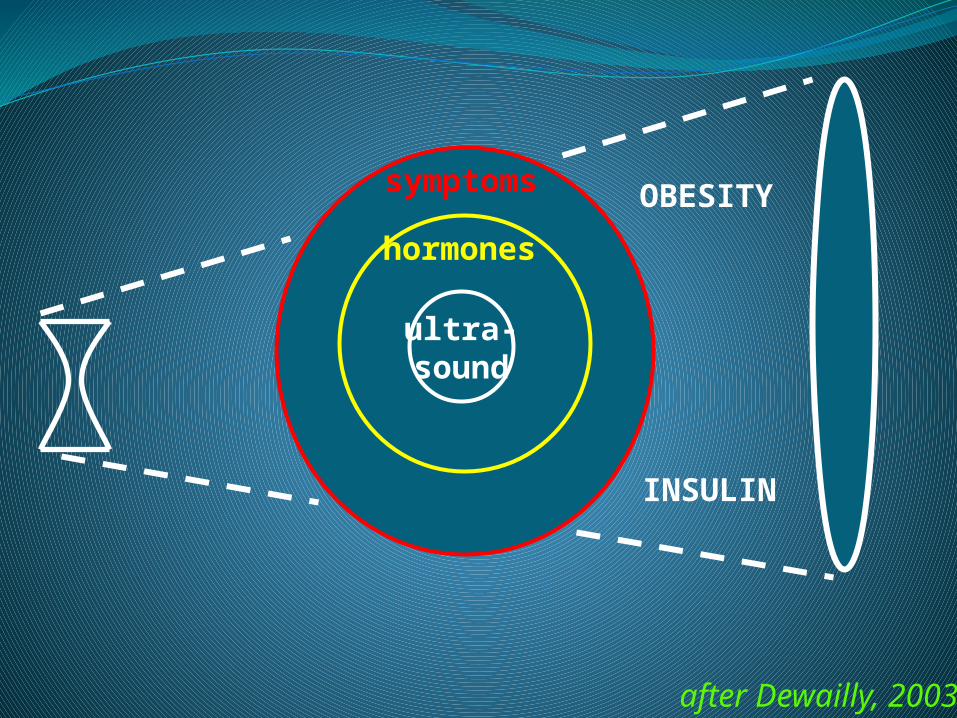
ultra-sound
hormones
symptoms OBESITY
INSULIN
after Dewailly, 2003
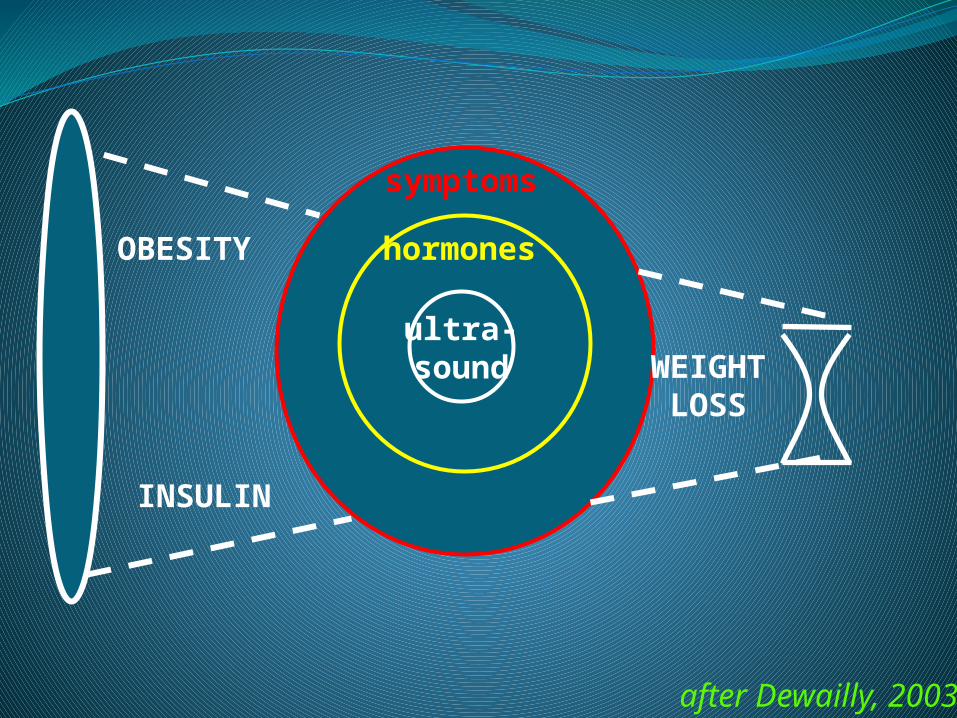
ultra-sound
hormones
symptoms
OBESITY
INSULIN
WEIGHTLOSS
after Dewailly, 2003

Main disturbances in PCOS Abnormal steroidogenesisIncreased ovarian production of:
Androgens
Progesterone Estradiol
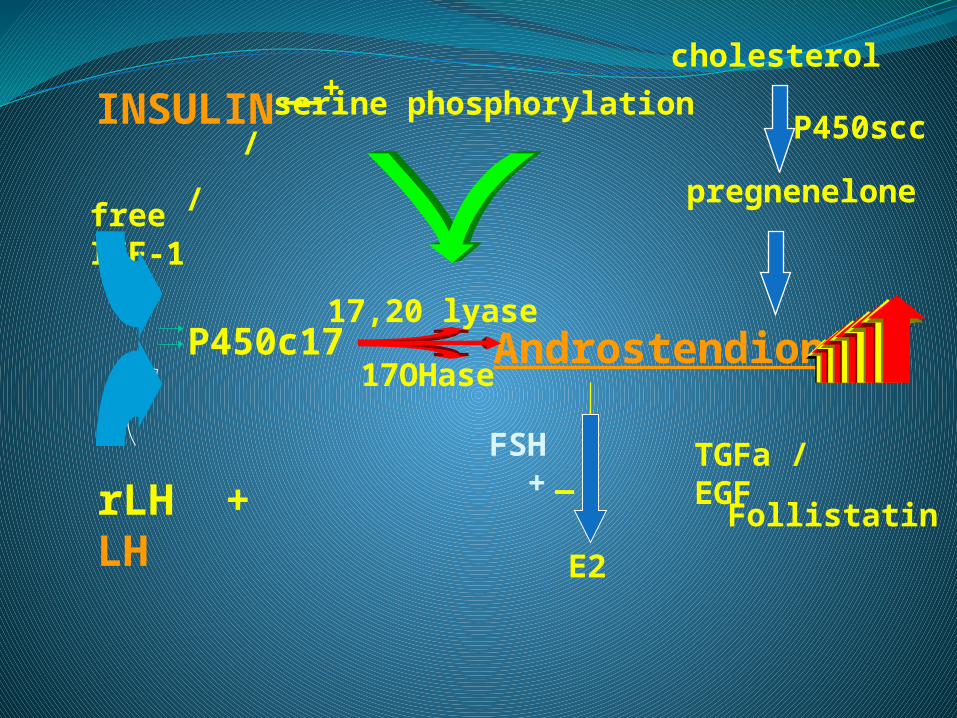
Androstendione17,20 lyase
17OHaseP450c17
INSULIN
rLH + LH
free IGF-1
serine phosphorylation
E2
TGFa / EGF
/ /
__+
_ Follistatin
cholesterol
P450scc
pregnenelone
FSH +
PCOS morphologyx6 the density of pre-antral follicles compared with normal ovary .
(Webber et al, 2003)
Large cohort of small follicles arrest in development but capable of responding to exogenous FSH.

Human Follicle Growth
(Gou
geon
, E
ndoc
r R
ev 1
996)
Primary follicle1 layer cuboidal GCs )46 µm, 570(
Secondary follicle 2 layers of GCs )77 µm, 480(
Pre-antral follicleclass 1 )theca cells & arterioles( )120 µm, 350(
Early antral follicleclass 2 )180-250 µm, 170(
Small antral follicleclass 4 )2 mm, 25(
Primordial follicle1 layer flat granulosa cells )36µm, 570(
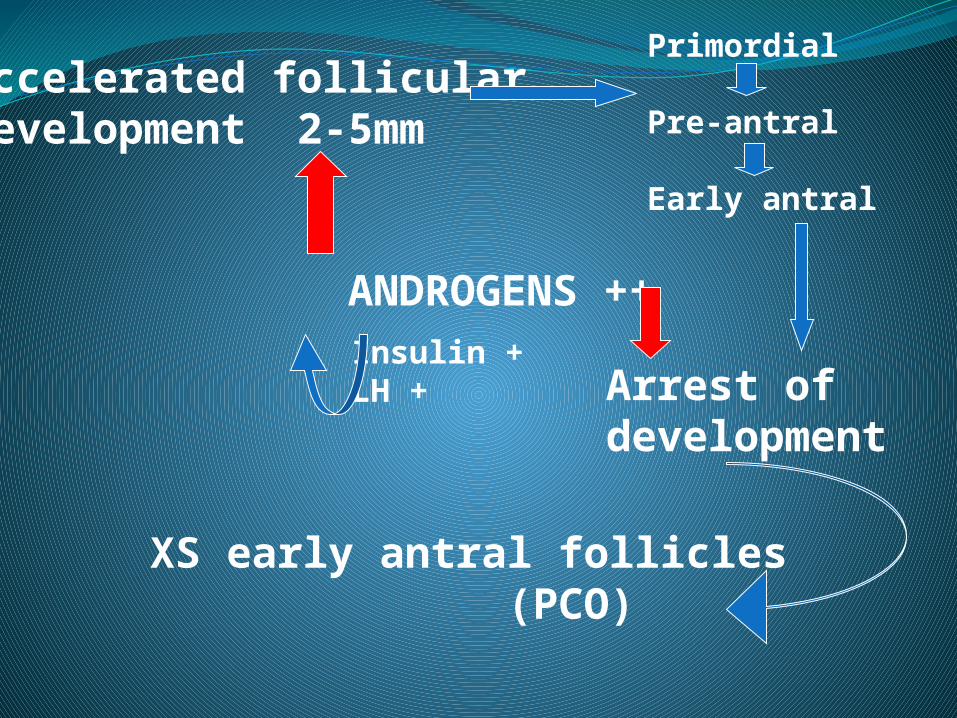
ANDROGENS ++
Accelerated follicular development 2-5mm
Primordial
Pre-antral
Early antral
Arrest of development
XS early antral follicles (PCO)
Insulin +LH +
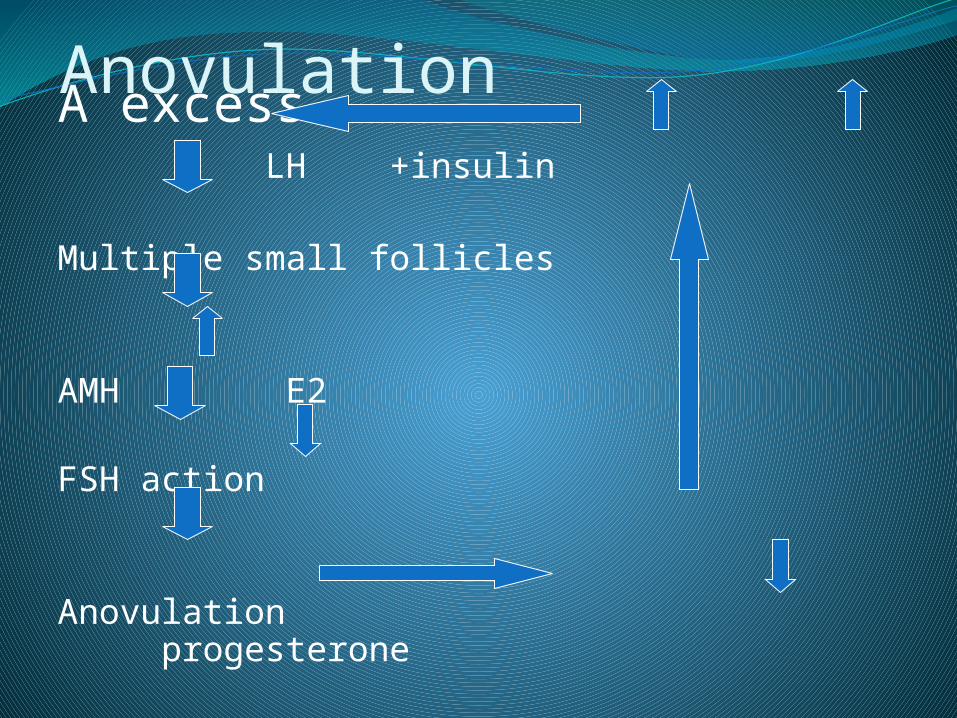
AnovulationA excess LH +insulin
Multiple small follicles
AMH E2
FSH action
Anovulation progesterone


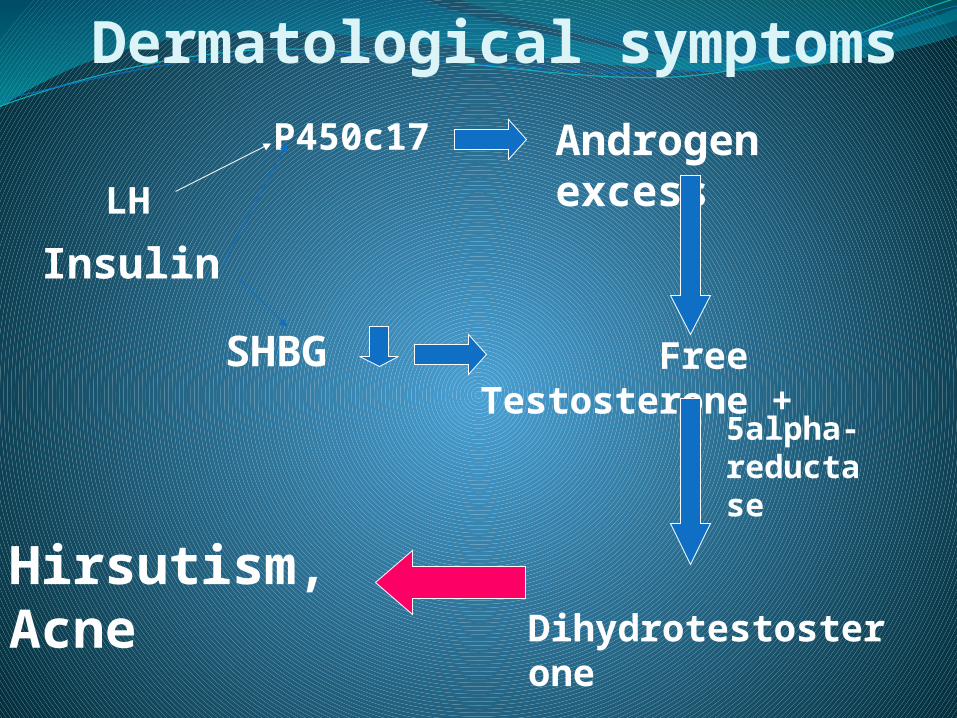
Insulin
LH
P450c17 Androgen excess
Free Testosterone +
Dihydrotestosterone
5alpha-reductase
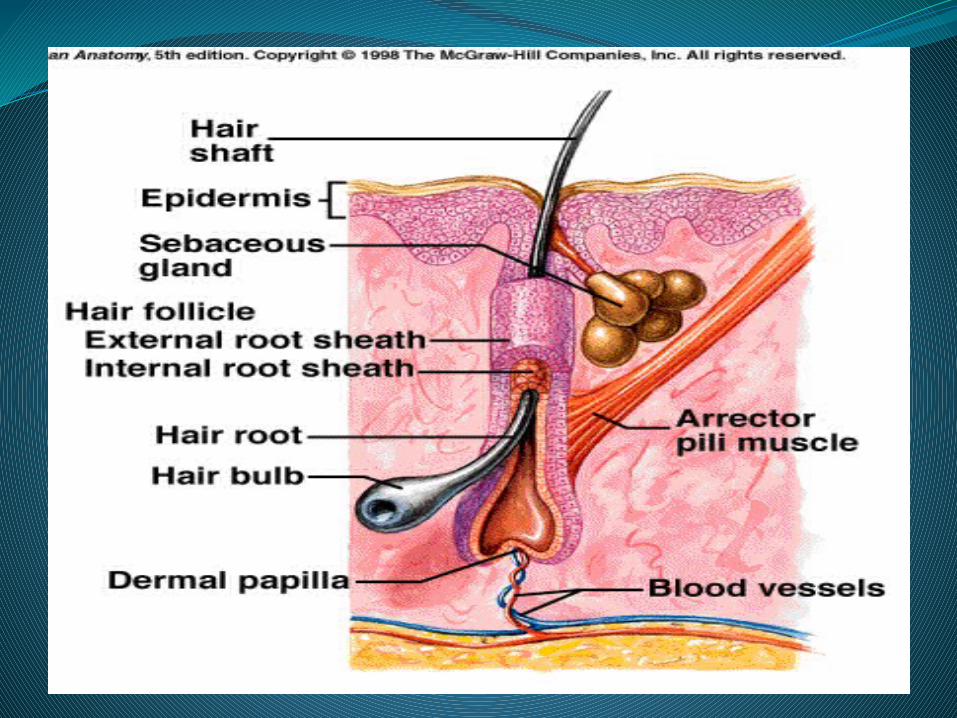
Hirsutism,Acne
SHBG
Dermatological symptoms

PCOS - Late sequelaeHyperinsulinemia / hyperandrogenism / obesity
• Diabetes mellitus x7
• Hypertension x4
• Low HDL/high LDL
*All are risk factors for cardiovascular disease and CVA
Main disturbances in PCOS Insulin resistance
80% of obese PCOS
30-40% of lean PCO
Genetic post-receptor defect unique to PCO
• Exaggerated by obesity

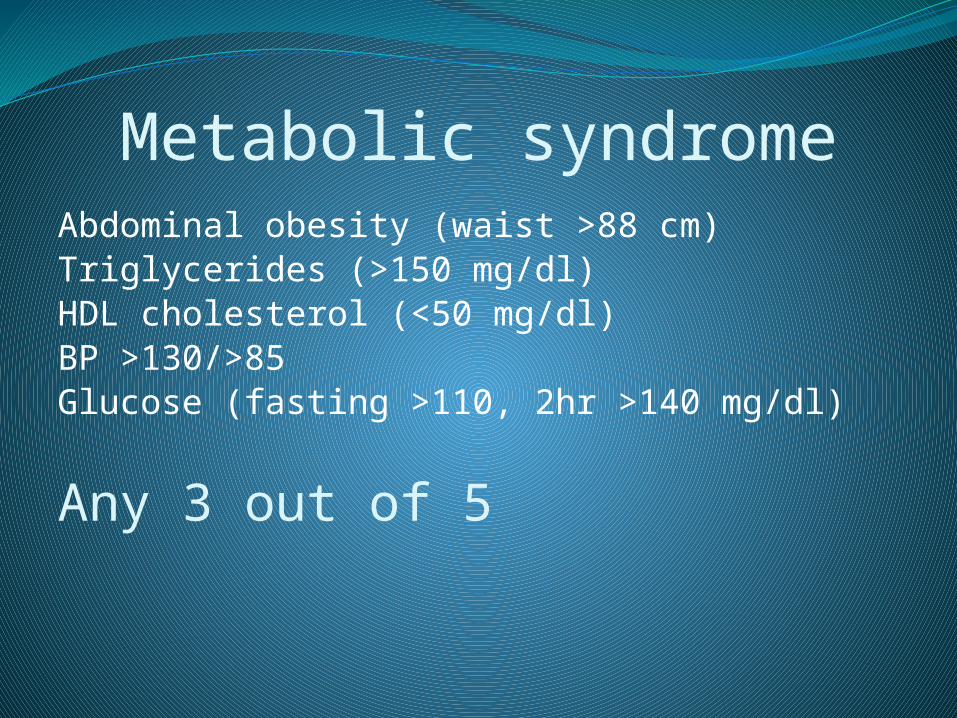
Metabolic syndromeAbdominal obesity (waist >88 cm)Triglycerides (>150 mg/dl)HDL cholesterol (<50 mg/dl)BP >130/>85Glucose (fasting >110, 2hr >140 mg/dl)
Any 3 out of 5
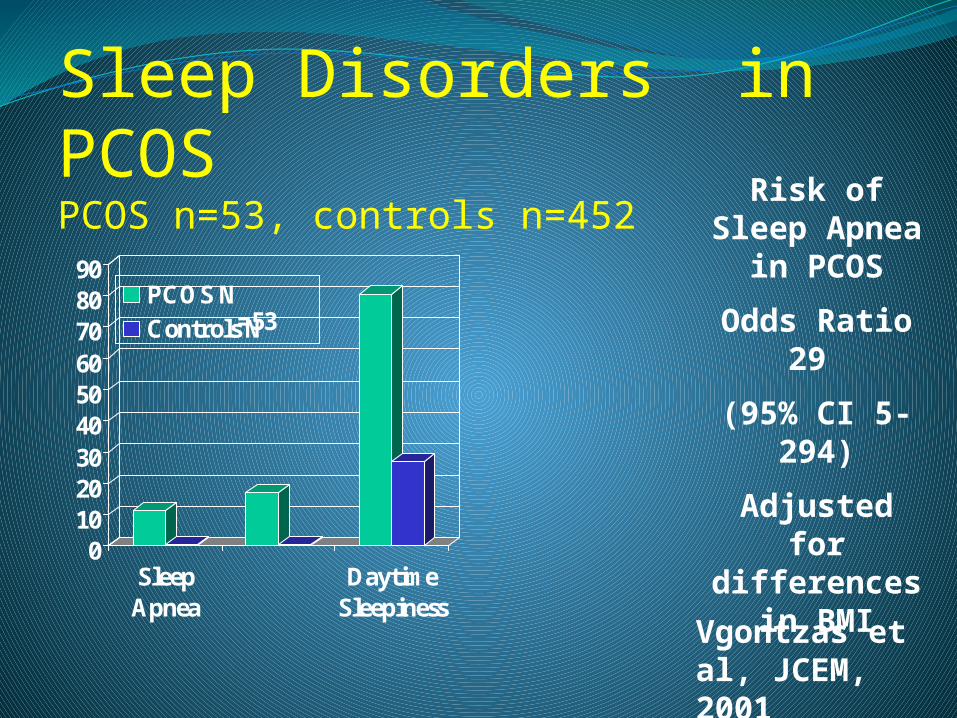
Sleep Disorders in PCOSPCOS n=53, controls n=452
0102030405060708090
SleepApnea
DaytimeSleepiness
PCOS N=53Controls N
=452
Risk of Sleep Apnea in PCOS
Odds Ratio 29
(95% CI 5-294)
Adjusted for differences in
BMI
Vgontzas et al, JCEM, 2001
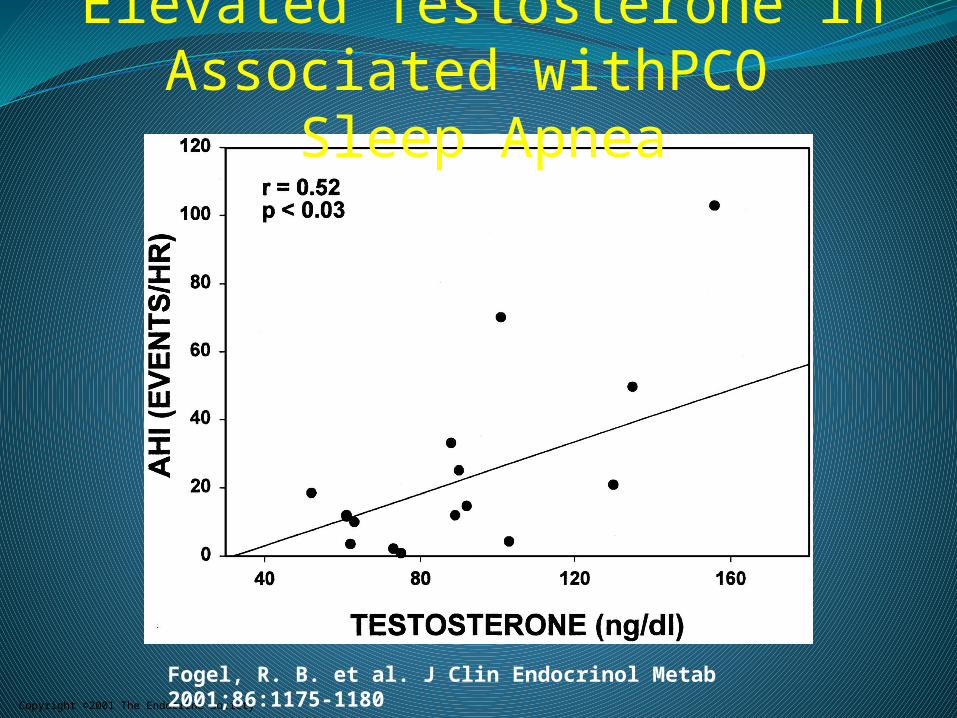
Copyright ©2001 The Endocrine Society
Fogel, R. B. et al. J Clin Endocrinol Metab 2001;86:1175-1180
Elevated Testosterone in PCO Associated with Sleep Apnea
The androgen circle of PCOS
XS androgens
Exposure In utero
Multiple smallfollicles
InsulinLH
AMH
AnovulationHirsutismAcne
PCOSphenotype
Homburg R, Hum Reprod, 2009