Embed Size (px)
Citation preview

Editorial
Rotaviruses and Rotavirus Vaccines
Rotaviruses were first described in 1963 when theywere observed during electron microscopy of faecalsamples from monkeys and mice. Some 10 yearslater, similar viruses with the characteristic sphericalstructure resembling the spokes of a wheel wereobserved in faecal samples from children withdiarrhoea (Fig. 1).The capsid, a protein coat that surrounds the
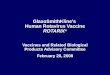
genome, has three layers each constructed from adifferent viral protein (VP). The inner and middlelayers, constructed from VP2 and VP6, respectively,are perforated by channels. The middle layercontains the ‘spokes’ of the wheel and is a majorconstituent of the virion. The outer layer isconstructed from another protein, VP7, which is aglycoprotein. Three other proteins are found in thevirion, VP1 and VP3 in the core, and VP4 whichforms 60 spikes on the surface (Fig. 2). Both VP7 andVP4 have a role in protective immunity.The proteins are numbered in order of their size,
the largest being towards the centre of the virion.Associated with the genome within the inner capsidlayer are copies of VP1 and VP3 which are enzymes(Fig. 3).The genome comprises 11 double stranded RNA
segments. Each segment encodes one protein exceptone segment which encodes two proteins. Thus in all12 proteins are encoded—six structural and six non-structural proteins.The two structural proteins that comprise the outer
viral capsid are the neutralization antigens VP7(or G for glycoprotein) and VP4 (or P for proteasesensitive). They define the serotypes [1]. There are23 P and 15G serotypes. Five G–P combinationsG1P8, G2P4, G3P8, G4P8 and G9P8 constitute 90%of human rotavirus strains worldwide. G1P8 strainsare most prevalent but large regional differences existand strain types can change with time [2]. This hasimplication in the development of vaccine.Change in serotypes occurs because of:
(i) Point mutation (or ‘drift’).(ii) Genomic reassortment caused by exchange
of RNA segments between strains (or ‘shift’).Overall most reassortment occurs in the genesencoding VP7 and VP4.
(iii) Duplication and deletion of sequences within asegment.
(iv) Introduction of animal rotaviruses into thehuman population.
Reassortment and crossing of species barrierresults in a large number of G types besides just theG1 and G4 in some regions. Thus serotypes G5,G8 and G9 have been described as importantserotypes encountered in Brazil, Malawi, India andBangladesh, respectively [2, 3].The virion utilizes sites on the spike proteins
initially to bind to the host cell, followed by siteson the glycoprotein (VP7) on the capsid surface.On entry into the host cell the virus elaborates potentexotoxin that can cause diarrhoea, and then goes onto destroy the cell causing blunting of villi, extensivedamage and shedding of large quantities of virus.The faeces of the infected individual may containup to 109–1010 per gram. A small infectious dose(<100 virus particles) is needed which facilitatestransmission.In developing countries rotavirus diarrhoea is the
third most common cause of death in infants withan estimated 5% of all deaths in children <5 yearsold [4, 5]. First infections after the neonatal periodare generally symptomatic, some 1–2% developingsevere or moderately severe disease. Repeat disease isuncommon after the second infection.Antibody response mounted by the host is targeted
at two proteins of the outer capsid namely VP7 (a Gprotein) and VP4 (a P protein). Vaccine developmenthas aimed at promoting antibody response to thesecapsid proteins of the commonly occurring strains.Animal strains from monkeys (rhesus RRV) [6], cows(WC 3) [7, 8] and lambs [9], that are not infective forhumans have been cultured with human strains toproduce reassortants. Those reassortants selected forvaccine production contain 10 genes from animalstrains to maintain non-infectivity and one gene-encoding proteins of outer capsid common to thecirculating serotype.A candidate oral vaccine derived from bovine
strain of rotavirus (RIT4237) underwent a trial in1983 with disappointing results [10]. The efficacy ofmonovalent vaccine was improved by reassortantsstrains that were non-infective tetravalent rhesusstrains as well as individual genes encoding outercapsid proteins of common human strains [11].The vaccine (Rotashield, Wyeth-Lederle, PearlRiver, NY, USA) was found highly effective inclinical trials. But an unexpected complication,intussusception, was reported to occur in the firsttwo weeks after administration of the first doseresulting in the vaccine being withdrawn [12].
� The Author [2008]. Published by Oxford University Press. All rights reserved. For Permissions, please email: [email protected] 79doi:10.1093/tropej/fmn015 Advance Access Published on 16 February 2008
at Aston U
niversity on January 7, 2014http://tropej.oxfordjournals.org/
Dow
nloaded from

Two next generation vaccines based on differentprinciples have recently undergone clinical trials.Rotarix (GlaxoSmithKline, Belgium) is derived froman individual human strain that replicates well in thegut and is shed in the stools. The strain was at firstattenuated by passaging 43 times, then clonedand renamed RIX4414 and further passaged [13].The vaccine is in the form of a lyophilized powderwhich must be reconstituted with 1ml of citratebicarbonate buffer and is administered orally.Following initial trials in Finland that showedsafety, immunogenicity and efficacy [14], the vaccinewas tested in middle-income countries of LatinAmerica (Brazil, Mexico and Venezuela) [15] and inSingapore [16]. The vaccine showed an efficacy of70–85% against rotavirus diarrhoea and 85–93%against severe disease. A large multicentre trial thatenrolled 63 000 infants in 12 countries of LatinAmerica and Finland was next undertaken. Theeffectiveness of the vaccine was 85% against severerotavirus diarrhoea, and reduced admission for
diarrhoea of any cause by 41%. Six vaccinatedsubjects and seven placebo administered ones devel-oped intussusception during 1 month of observationconfirming lack of causal association.Rota Teq (Merck) is prepared from a bovine strain
of rotavirus (WC3) that had shown variable effec-tiveness in clinical trials in USA, China and Africa.To improve its effectiveness reassortant strains wereprepared containing 10 genes from the parent bovinestrain and an individual capsid gene from the mostcommon human serotypes. Five single gene reassor-tants each containing a gene for a capsid protein forhuman serotypes G1–G4 and PIA were combined ina pentavalent vaccine [17]. The vaccine is formulatedas liquid containing 12� 107 infectious units perdose, and is administered in three oral dosescommencing at 6 weeks of age. Efficacy of 96%against admission for rotavirus diarrhoea wasdemonstrable. The vaccine also protects against arange of rotavirus serotypes in circulation [18].
Other Candidate Vaccines
Regional diversity of rotaviruses requires thatvaccines evolved from locally prevalent genotypesare likely to be more efficient. Several vaccines basedon this principle are at present in experimental stage.In China, a strain of rotavirus obtained from lamband grown in calf kidney cells has been the startingpoint of a vaccine licensed in that country. In India,two candidate rotavirus strains obtained duringnosocomial outbreaks in asymptomatic newborns,strain 116E and 1321 are likely source of a vaccine.Both strains do not cause disease in infants. They arenatural human bovine reassortants that grow wellin the infant gut, and can resist neutralizationby maternally derived antibodies [19, 20]. Anothernaturally occurring asymptomatic neonatal rotavirus
FIG. 2. (a) On electron microscopy and (b) schematic representation.
FIG. 1. Electron microscope appearance of rotavirus.
EDITORIAL
80 Journal of Tropical Pediatrics Vol. 54, No. 2
at Aston U
niversity on January 7, 2014http://tropej.oxfordjournals.org/
Dow
nloaded from

strain in Australia, RV3, is also under considerationas a potential source of vaccine [21].Since vaccines are licensed on the basis of safety,
immunogenicity and efficacy candidate vaccines willneed to be tested in clinical trials in a number of low-income countries to check their effectiveness whereexclusive breastfeeding is the norm, malnutritionis prevalent and frequent transmission of entericmicroorganisms occur in a generally unhygienicenvironment. A robust vaccine to protect infants insuch an environment is the overall aim.
G. J. EBRAHIM
References
1. Hoshimo Y, Kapikian AZ. Rotavirus serotypes: classi-fication and importance in epidemiology, immunity,and vaccine development. J Health Popul Nutr2000;18:5–14.
2. Gentsch JR, Woods PA, Ramachandran M, et al.Review of G and P typing results from a globalcollection of rotavirus strains: implications for vaccinedevelopment. J Infect Dis 1996;174:S30–6.
3. Koshimura Y, Nakagomi T, Nakagomi O. Therelative frequencies of G serotypes of rotavirusesrecovered from hospitalized children with diarrhoea:a 10 year survey (1987–1996) in Japan with a reviewof globally collected data. Microbiol Immunol2000;44:499–510.
4. Kosek M, Bern C, Guerrant RL. The global burden ofdiarrhoeal disease as estimated from studies publishedbetween 1992 and 2000. Bull World Health Organ2003;81:197–294.
5. Parashar U, Gibson CJ, Bresee JS, et al. Rotavirus andsevere childhood diarrhoea. Emerg Infect Dis 2005;12:304–6.
6. Kapikian AZ, Hoshino Y, Chanock RM, et al. Efficacyof a quadrivalent rhesus rotavirus-based human rota-virus vaccine aimed at preventing severe rotavirusdiarrhoea in infants and young children. J Infect Dis1996;174(Suppl 1):S65–72.
7. Clark HF, Offit PA, Ellis RW, et al. WC3 reassortantvaccine in children in children. Arch Virol 1996;12(Suppl):187–98.
8. Clement-Mann ML, Makhene MK, Mrukowicz J, et al.Safety and immunogenicity of live attenuated human-bovine (UK) reassortant rotavirus vaccine withVP7-specificity for serotype 1,2,3, or 4 in adults,children and infants. Vaccine 1999;17:2715–25.
9. WHO. Report of the Meeting on Future Directions forRotavirus Vaccine Research in Developing Countries.Geneva: World Health Organization, 2000;1–56.
10. Vesikari T, Isolauri E, D’Hondt E. Protection of infantsagainst rotavirus rotavirus diarrhoea by RIT4237attenuated bovine rotavirus strain vaccine. Lancet1984;1:977–81.
11. Kapikian AZ, Hoshino Y, Channock RM,Perez-Schael I. Efficacy of a quadrivalent rhesusrotavirus-based human rotavirus vaccine aimed atpreventing severe rotavirus diarrhoea in infants andyoung children. J Infect Dis 1996;174(Suppl 1):S65–72.
12. Centres for Disease Control and Prevention.Withdrawal of rotavirus vaccine recommendation.MMWR Morb Mortal Wkly Rep 1990;48:1007.
13. Bernstein DI, Sack DA, Rothstein E, et al. Efficacyof live attenuated human rotavirus vaccine 89–12 ininfants: a randomised placebo controlled trial. Lancet1999;354:287–90.
14. de Vos B, Vesikari T, Linhares AC, et al. A rotavirusvaccine for prophylaxis of infants against rotavirusgastroenteritis. Pediatr Infect Dis J 2004;23(Suppl 10):S179–82.
15. Salimas B, Perez-Shael I, Linhares AC, et al.Evaluation of safety, immunogenicity and efficacy ofattenuated rotavirus vaccine, RIX4414; a randomizedplacebo controlled trial in Latin American infants.Pediatr Infect Dis J 2005;24:807–16.
16. Phua KB, Quak SH, Lee BW, et al. Evaluation ofRIX4414, a live attenuated rotavirus vaccine in arandomized double-blind placebo controlled Phase 2trial involving 2464 Singaporean infants. J Infect Dis2005;192(Suppl 1):S6–16.
17. Heaton PM, Goveia MC, Miller JM, et al.Development of a pentavalent rotavirus vaccine against
FIG. 3. Virus proteins on electrophoresis.
EDITORIAL
Journal of Tropical Pediatrics Vol. 54, No. 2 81
at Aston U
niversity on January 7, 2014http://tropej.oxfordjournals.org/
Dow
nloaded from

prevalent serotypes of rotavirus gastroenteritis. J InfectDis 2005;192(Suppl 1):S17–21.
18. Vesikari T, Metson DO, Dennehy P, et al. Safetyand efficacy of a pentavalent human-bovine (WC£)reassortants rotavirus vaccine. N Eng J Med2006;354:23–33.
19. Das BK, Gentscha JR, Hoshino Y, et al.Characterisation of the G serotype and genogroup of
New Delhi newborn rotavirus strain 116E. Virology1993;197:99–107.
20. Glass RI, Bhan MK, Ray P, et al. Development ofcandidate rotavirus vaccines derived from neonatalstrains in India. J Infect Dis 2005;192(Suppl 1):S30–5.
21. Barnes GL, Lund JS, Mitchell SV, et al. Early phase IItrial of human rotavirus vaccine candidate RV3.Vaccine 2002;20:2950–6.
EDITORIAL
82 Journal of Tropical Pediatrics Vol. 54, No. 2
at Aston U
niversity on January 7, 2014http://tropej.oxfordjournals.org/
Dow
nloaded from