Embed Size (px)
Citation preview

1
ROOTCANALTREATMENT:ACLINICALGUIDEFORDENTALSTUDENTS,
GENERALDENTISTSWHOLIKEDOINGRCTSANDGENERALDENTISTSWHOHATEDOINGRCTS©2016
GregY.Kim,DDSDiplomate,AmericanBoardofEndodontics
Thisdocumentisintendedtobeaneasy-to-readguidefordentalstudentsandgeneralpractitionersofdifferent
clinicalcapacitywhoseektoimprovetheirrootcanaltreatmentskillsandobtainamoreconsistentlypredictable
outcomeintheireverydaypractice.Doingarootcanaltreatment(RCT),forthemostpart,isnotacomplicated
taskandtheprocedureshouldbecomeeasierandmoresystematicasthecliniciangainsmoreexperience.There
are,however,differentcomponentsofdevelopmentinbecomingamoreskilledclinician,andbecoming
technicallygoodisonlyoneaspectofit.Inordertobetrulyproficientinthisfield,aclinicianmustalsoimprove
his/herdiagnosticskillsandunderstandingofitsbiologicalprinciples.Thisguideisdividedintodifferenttopicsand
subtopicswhicharedeemedimportantforunderstandingofthosefundamentalendodonticprinciples.
DIAGNOSIS
Gooddiagnosticskillsareundeniablyimportantforbettermanagementofendodonticcases.Dayinanddayout,
weseeawholeslewoferrorsassociatedpoordiagnosis,whetheritbeprescribingwrongmedicationsor
treatment-planningforawrongprocedure.Theimportanceofthisfirststepoftreatmentcan’tbestressed
enough.Startingoutwithagooddiagnosisattheonsetcanreallysparethedentistofunnecessaryheadaches
duringfollow-upphase.Forthepurposeofthisguide,differentpulpalandperiapicaldiagnosesarenotgoingtobe
discussedcomprehensively,butsomeofthemostcommonerrorsassociatedwitheitherdoinganerroneous
diagnosisorNOdiagnosisdeserveadiscussionhere.
o PrescribingAntibioticsforPulpitis
Pulpitisbydefinitionisaninflammationofthepulptissueandcouldbeexceedinglypainfulunderacute
inflammatoryconditions.Forpainrelief,eitherthisinflamedpulptissueneedstoberemovedorthe
toothneedstoberemoved.Whenthepulpisstillvitalandinflamed(note:blooduponaccessopening),
takingantibioticsactuallydoesnothingforpainreliefandonlyaddsthehassleofhavingtotake
medicationsformultipledaysforanalreadydistressedpatient.Inmyoffice,Ihaveseenapatientgiven
antibioticsforpulpitis,andwhensymptomsdidnotimprove,shewasadministeredtotheERandgiven
evenhigherdosageofIVantibiotics.Thiswouldbeahard-to-defendcaseifshedecidedtoseeyouatthe
court.Forantibioticstobeeffectiveatreducingsymptoms,thepulpmustbenecroticandinfectedfor
themostpart(note:absenceofblooduponenteringpulpspace).Now,itshouldbenotedthat

2
percussionsensitivitycouldpresentwithbothvitalandnon-vitalpulp.But,ingeneral,thecaseswhere
antibioticscanworkforpainreliefdonotrespondtothermalstimuli(endoice,hotcoffee,etc.)but
insteaddisplaymarkedpercussionsensitivitythatcanbelocalizedwellbythepatient.Tendernessofsoft
tissueinthevestibuleneartheapicesoftheassociatedtoothmaybepresentaswell.Ontheotherhand,
ifapatient’schiefcomplaintisexperiencingseverepainupondrinkingsomethingcoldorhot,donotgive
thatpatientantibioticsforthepurposeofaddressingthatchiefcomplaint.Atleastdoapulpotomyifyou
havetime,orfindanendodontistwhocanprovideanemergencytreatmentforyou.Anotherkey
indicationofpulpitis,otherthanpainonthermalstimulus,isatypeofpainthatseemstojumparound
andcannotbelocalizedwellbythepatient.Pulpitiscannotbelocalizedwellbythepatientbecause
therearenosignificantproprioceptivenervefibersinthepulp.Besuretodoathoroughdiagnosisas
manypatientswillpresentwithatooththatisnecroticandinfectedbutwillalsocomplainofthermal
sensitivityfromadjacentvitalteethaswell.Thekeyistoaddressthetooththatisthemaincauseof
acutesymptoms(targetingthechiefcomplaint).
o NotInstrumentingtheCanalsforaNecroticToothwithInfectedRootCanals
Thisisanothererrorcommonlyencountered.Whenpulpalinflammationprogressesandthepulp
becomesnecrotic,fullinstrumentationofthecanalsisrequiredtoeliminatetheinfectionandreduce
symptoms.Anecrotictoothhasinfectioninthecanals,themostcommoncauseofwhichisbacterial
insultfromcaries.Thesepatientscanpresentwithswollengumsand/orface.Instrumentingtoatleast
size30/04withagoodamountofsodiumhypochloriteirrigationisrecommended.Otherwise,givethe
patientantibiotics(oryoucandoboth)andthepatientwilltypicallyseereliefofsymptomswithinaday
ortwo.
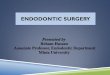
Beforeinitiatingthistreatment,Iaskedmyselfthefollowingquestions—whyistherealesiononmid-distalpartoftheroot?Istherearootfracture?Istherealocalizeddeepprobingdepthinthisarea?Ifarootcanalprocedureiscarriedout,thenwillithelpresolvethispathology?Thepost-opPAshowsthatthereisalateralcanalinthispartoftheroot,confirmingtheendodonticoriginofthelesion.

3
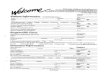
DIAGNOSISDICTATESTREATMENT.An8-year-oldboypresentedwithapinpointexposureof#9fromtrauma.Patient’shistoryofchiefcomplaintanddiagnostictestsindicatedthatthepulpwasstillinareversiblestateofinflammation.Thetoothstructureimmediatelyadjacenttothesiteofexposurewascleanedoutwithasmallroundburanddisinfectedwithsodiumhypochlorite.ThisareawascappedwithBioceramicPuttymaterialandthepatientwasreferredbacktothegeneraldentistforacompositerestoration.A9-monthfollow-upshowed(despiteforeshorteninginthefirsttwox-rays)thatthetoothmaintaineditsvitalityandcontinueditsnormaldevelopment.IfRCThadbeendonewithoutproperlydiagnosingthestateofthepulpandtheperiapex,thetoothwouldhavestoppeditsnormaldevelopmentandwouldhaveresultedinaclinicallymorecomplicatedsituation.(1stPA:Pre-op,2ndPA:ImmediatePost-op,3rdPA:9-MonthFollow-Up)
ANTIBIOTICS
o Thego-tomedicationforanodontogenicinfectionisPenVK500mg(bactericidal,narrowerspectrumof
actionthanamoxicillin,taken4timesperday).Forpatientswithamoxicillin/penicillinallergy,
Clindamycinshouldfirstbeconsidered.
o Forpatientswithalarge,noticeableswelling:Refertoanoralsurgeonifyouarenottotallycomfortable
dealingwiththesituation.Ifyougive2differentantibioticstogether,themosteffectivecombinationmay
be2bactericidalantibiotics,suchasPenVKandmetronidazole.Acombinationofbactericidaland
bacteriostaticantibiotics(suchaspenicillinwithclindamycin)mightpotentiallycounteractthe
effectivenessofeachotherandmaynotbeashelpful.
THETREATMENT:STEPBYSTEP
Beforeinitiatinganytreatment,takealong,closelookatthex-rays.Mostoftheworstexperiencesassociated
withrootcanalprocedures,byyouandbythepatient,canbeavoidedbychoosingNOTtodothemost
complicatedcases.Olderpatientshaveahigherlikelihoodofpresentingwithcalcifiedcanalsandmaynotbeable
totoleratelongertreatmentsessionsatthesametime.Ifyouhavedifficultydiscerningthecanalsdueto
calcification,itmaybeadvisabletorefertoaspecialist.Lookingatbitewingx-raysaswellasperiapicalscanalso
giveyouadditionalinformationastowhatkindofdifficultyleveltoexpect.
o Access
Agoodaccesscanfacilitatetherestoftheprocedure.Apooraccess,bythesametoken,canmakethe
proceduremoredifficultthanneeded.Studythebitewingx-raybeforepickingupahigh-speedmotorto
gaugehowmuchyouneedtogodowntobeinthepulpchamber.Itshouldalwaysberememberedthat

4
thecoronalpulptissuevolumeislargestontopofthebiggercanals,meaningthatitwouldbeeasierto
exposethispartofthechamberfirstandthenpeelawayfromhere(Note:Thisisnotnecessarilythe
highestpointofthepulpchamber.Mandibularmolarshavehighmesialpulphornsbutthemesial
canalsaresmallerthandistalcanals).Foruppermolars,it’seasiesttoexposethepalatalcanalfirst
becauseit’sthelargestcanalwiththemostamountofcoronalpulpchamberspaceontopofit.Thisis
especiallyhelpfultorememberifyouareworkingonacalcifiedtoothwithareducedpulpspace.Asyou
peelawaytheroofofthepulpchamber,adarkpulpalfloorrevealsitselfandtheothercanalsarefoundat
theouteredgesofthisdarkerfloor.Italsohelpstorememberthatthepulpchamberiscenteredand
concentricwiththetoothoutlineattheleveloftheCEJ.MakeahabitoflookingattheCEJoutlineand
envisioningthepulpchamberatthecenterofthiscrosssection.Doingthisoccasionallywhileaccess-
preppingcanhelpyougetreorientedifyouaredrillinginawrongdirection.Caution:Thisinformation
regardingtheCEJanditsrelationtopulpchambermaybedistortedincrownedteeth.
o MeasuringWorkingLength
Theveryfirstfilesplacedinacanalmustalwaysbepre-curvedwiththesmallestpossibleradius.That
is,allK10andK15fileshavetobecurved(thereareinstrumentsspecificallyusedforthispurposebutif
youdon’thavethose,acollegeplierwilldo)atthetipinordertonegotiatearoundthecurvatureofthe
canalandtopreservethatnaturalcurvaturewiththeleastamountoftransportation.Thiscurvingofthe
tipofasmallfileisutterly,criticallyimportant.Oncethetipofasmallfileiscurved,itisplacedinthe
canalandgentlyworkedwithacircumferentialwatch-windingmotionuntilitisabletoreachtheapex.It
isimportanttorememberthat,inyourendeavortogettotheapex,thecircumferentialwatch-winding
motionmayprovetobemuchmoreeffectivethanastraightup-and-downfilingmotion.Fornarrower
canals,youmaynotbeabletoreachtheapeximmediately.Thegoalistoworkyourselfdown
incrementallywithoutdistortingthecanalanatomy.Whenyouaresuccessfullyworkingyourselfdown
toreachtheapex,thecanalfeelsstickyandthisisagoodindicationthatyoucancontinuetocarefully
workyourselfdowntoestablishthelength.Acanalthatnolongerfeelsstickybutfeelslikeahardwall
indicatesthatyoucouldbetransportingthecanaloutofitsnaturalanatomy.Thismeansthatyouare
makingyourowncanal,andsuccessratetypicallynosedivesinthosecaseswithaman-made-canal.Ifyou
nolongerfeelthestickinessofthecanal,backstepforonesecond,takeadeepbreath,anddothe
followingthreethings:openupthecoronalpartofthecanal(moreonthislater),irrigatecopiously,and
pickupthesmallestfilethatyouhaveavailable(K6orK8)andagaingiveitasmallcurveatthetip.Place
thesmallfileinthecanalwhilekeepinganeyeonitasK6andK8filesareverydelicateandwillcrimple
easilyifyouhitanyotherhardsurfacewhiletryingtoplacetheminthecanal.Onceitisinthecanal,
gentlykeeprotatingthembackandforthtoseeifyoucanfindthestickyspotagain.Virtuallynoapical
pressureisneededwhiledoingthis.Onceastickyspotisfound,youmayhavetokeepworkinginthe

5
samemannerwhilefrequentlyirrigating.Again,thesmallfilescanseparateeasilyinanarrowcanalif
handledcarelessly,anditmaybewisetoinspectthemfrequentlyandtogothroughafewofthem
insteadofusingoneuntilitseparates.
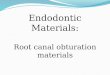
AK15filecurvedwithasmallradiusofcurveatthetipandwithalargeradiusofcurveatthetip.ALLsmallfiles(6,8,10,15)mustbepre-curvedwithasmallradiuscurveatthetip.Afileshouldnotbebentwithalargeradiuscurveliketheoneshownontherightbecausecurvingafilethiswayhasonlylimitedbenefits.
o Coronal/OrificeWidening
Howweachievethiscoronalwideningofthecanalhaschangedsomewhatovertheyears.First,the
rationaleforcoronalcanalwidening:Insmallercanals,openingupthecoronalportionofthecanal
allowsyoutoreachtheapexmoreeasily,againwithlesstransportationinthecriticalapical1/3ofthe
canal.Inotherwords,youaremorelikelytopreservethenaturalcanalanatomywhenthecoronal
portionofthecanalhasbeenopenedupfirst.Inlargercanalswhereyouareabletoreachtheapex
easily,orifice/coronalcanalwideningisactuallynotthatimportant.Itmustbepointedoutthatthegates
gliddenisnolongerroutinelyusedforthispurpose,atleastbytoday’seducators’standards.Therearea
fewstudiesintheliteraturethatshowedremovingexcessivetoothstructurefromthecoronalpartofthe
canalcanreducetheresistanceofthetoothtorootfracture.Obviously,thereisnogoodreasonto
removemoretoothstructurethannecessaryespeciallywhenit’smorelikelytoleadtoamoreadverse
outcome.Personally,Iseldomusethegatesglidden,andIonlyuse04taperrotaryfiles,evenforcoronal
flaring.
• AdvancedTip:Incorporatingsomedegreeof“crown-down”techniquemaygiveyoubetterresultsin
manycases.Iusuallypickupabiggerrotaryfile,suchasa40/04ora35/04file,toinitiatecrown
downformostofmycases.ThisisactuallydoneevenbeforeImeasuremyworkinglength.Knowing
thatthemajorityofrootcanalworkinglengthsfallunder19mms–22mmsrange,Iwillusetherotary
inacrown-downfashion,startingwitha40/04andthenusinga35/04anda30/04toabout14mms–
16mms.Imeasuremylengthatthispoint,hand-filealittlebitandthenbegintherotary
instrumentationatfullworkinglength.Thisislistedasanadvancedtipbecauseyouhavetobe

6
proficientatdoingRCTsbeforeyoucaneffectivelytakeadvantageofthistechnique.Choosingthe
rightsizerotaryfiletoinitiateyourcrown-downisajudgmentcallasyourinitialfilesizemaybe
differentfordifferentcases.Youmusthavebuiltsomespeedintoyourtreatments,andyoualso
mustbeabletoperceivewhentochangetherotaryfiletoasmalleronewhilegoingdownapically
whencertainamountofresistanceismet.
#19WITHSEVERELYCALCIFIEDMESIALCANALS.Thesecasescantake2-3timeslongerthanastraightforwardcase,andpatientsshouldbeinformedofthatbeforeinitiationoftreatment.
#19WITHLONGROOTS.Workinglength(26mms)wasmeasuredafteratleastcoronalhalfofthecanalshavebeenopenedupwithrotaryfiles.Managementofcurveintheapical1/3wouldhavebeenmuchmoredifficultwithoutfirstinstrumentingthecoronalportionsofthecanals.
o Instrumentation
Thegeneralruleistohand-instrumenttosizeK15beforeswitchingtorotaryfiles.Oneofthemost
disturbingexperiencesapractitionerdoingaRCTcanhaveistohaveafileseparation.Topreventthis
mishapandotheriatrogenicerrors,itisimportanttorememberafewthings.First,alwayshavesome
formoflubricationsuchassodiumhypochloriteorRCPrepinsidethecanal.Continuousinstrumentation
insideadebris-filleddrycanalcanbeamaincauseofallsortsoftroubles.Second,justlikethehandfiles,
ifyouarenotgettingtothemeasuredlengthinoneattemptwitharotaryfile,thenthelengthshouldbe
attainedincrementally.Thismeansremovingthefilewhenresistanceismet,irrigating,andwipingthe
fileswithanalcohol-soakedgauzetoremovethedebrisstuckintheflutesofthefile.Sometimes
irrationalitycouldtakeoverandwecanpushalittletoohard(It’sFridayafternoon,4:30PMandyouhad
alatestartwiththelastcaseofday)inanattempttoreachtheworkinglengthquickly,butdoingsocan
inevitablyresultinaseparatedfileatsomepoint.

7
• Oneofthesignificantbutlesstalkedaboutbenefitsofamodernendodonticrotaryinstrumentis
thatitremovesdebrisfromthecanalasitrotatesclockwise.Observethefiletoseeifitis
accumulatingtoomuchdebrisintheflutesandwipethemofftopreventgeneratingexcessive
torqueandstress.
• Theeffectofalarge-taperinstrumentisnotawellunderstoodconcept.Wetypicallyassociate
increasedstiffnessanddecreasedflexibilityofarotaryfilewiththeincreaseintipsizeonly.That
is,wesaythatsize30isstifferandlessflexiblethansize25becauseitisbigger,andsize40isless
flexiblethansize35,andsoon.Butincreasingthetaperoftheinstrumentcanalsohavea
dramaticnegativeeffectontheoverallflexibilityoftheinstrument.Thus,an06-taperfileis
muchstifferandlessflexiblethanan04-taperfile,andbecauseofthatinflexibilityitmaynotbe
abletobypassacurvedpartofthecanalthatan04-taperfileofthesametipsizecan.
CHALLENGINGINSTRUMENTATION.ForMBandDcanals,workinglengthcouldnotbereachedwithapre-curvedK10handfile.Instrumentationwasdoneusingthefollowingsequence:40/04toopenuptheverycoronalportionofthecanal,then35/04,30/04,and25/04toresistance(advancingfurtherapicallyusingincrementallysmallerrotaryfiles),thenK8,andthenC6handfilestomeasurelength.Then,incrementallybiggerinstrumentswereusedatworkinglengthforcompleteinstrumentation:K8again,K10,15/04,20/04,25/04,30/04,andfinally35/04.ItmayhavebeenimpossibletoinstrumenttheMBcanaltothesametipsize35usinganytaperlargerthan04.
• OnEfficientInstrumentation,RPM,andContactTime:Anargumentcouldbemadethatusinga
rotaryfileatahighRPM(>500)isdangerousforlessexperiencedclinicians.Anargumentcould
bemadethatusingarotaryfileatalowRPM(<300)isalsodangerousforlessexperienced
clinicians(whichprobablyindicatesthatwhat’sdangerousistheperson).Itisoftenoverlooked
howusingahigherRPMcandramaticallyincreasethecontacttimeoftheinstrumentwiththe
wallsofthecanal,butthisisanotherimportantconcepttounderstand.Astraightfileinserted
intothecanalwantstostraightenitselfinsideacanal.Thisishowtransportationofthecanal
occurs.Therefore,inordertominimizetransportation,afile’scontacttimewiththewallsof
thecanalshouldbekeptasminimalaspracticallypossible.Thus,whenafilehasdoneitsjobof
reachingtheapex,thecanalshouldbeirrigatedtoremovedebris,andthenextlargerfilesize
mustbeused.Thereisatendencyforlessexperiencedclinicianstorepeatedlyinstrumentthe

8
canals,overandover.Thishabitisespeciallydeadlywhentherepeatedinstrumentationisdone
underahighRPM,asthemostcommonundesirableoutcomewouldbeeitheraseverely
transportedcanalorablown-outapex.
o InstrumentationSize
Thisisanareaoffiercecontroversyandtherearevaryingopinionsabouthowbigacanalneedstobe
instrumentedto(IoncehadarepfromthelargestdentalproductcompanyintheUSaskmewhyI
instrumentthecanalstocertainsizes).Onethingthatmostendodontistsdoagreeon,however,isthat
theirrigatingsolutionmustbeabletoreachtheapextoremovedebrisanddisinfectthecanals.Asmall
canal(instrumentedtosize25/04orsmaller)maynothavetheirrigatingsolutionreachthecriticalapical
1/3ofthecanalandalsomaybedifficulttofillproperlyinsomecases.Conversely,inaheavilyinfected
rootcanalsystemitmaybenecessarytoinstrumentthecanalstoabiggersizethanwhenthepulpisstill
vital(vitalmeanssterile).Thefollowingisalistofmyusualinstrumentationsizesasofthiswriting:
• UpperCentrals:45/04or50/04
• UpperLaterals:35/04or40/04(Thistoothhasanapicaldistolingualcurvethatisoftentimes
mismanaged,leadingtomanyfailedtreatments.)
• LowerIncisors:30/04,35/04,or40/04(Consideredthemostdifficulttoothbysomespecialists)
• AllCanines:40/04or45/04
• SingleCanalPremolars:Atleastsize40
• TwoCanalPremolars:30/04or35/04
• MesialCanalsofLowerMolars:30/04or35/04
• DistalCanalsofLowerMolars:40/04or45/04
• MBandDBofUpperMolars:30/04or35/04
• PalatalofUpperMolars:40/04or45/04
• Thisis,ofcourse,alooseguideline.Afinaldecisiononthesizeofinstrumentationismadewhile
thecanalsarebeinginstrumented.Insomerarecases,averylargecanalwithalongstanding
infectionandaresorbedrootendmayhavetobeinstrumentedtoevenhigherthansize50.
Somecanalswithwickedcurvesmaynotbeabletobeinstrumentedtoanythingbiggerthansize
25.Atanyrate,itisimportanttorememberthatthediscussionofapicalsizeshouldbecarried
outalongwithaconsiderationfortheinstrument’staper.Afilewithasize25tipand08taper
wouldbemoreaggressiveinremovingrootdentinthanafilewithasize35tipand04taper.It
mustagainbenotedthatlargetaperinstruments(06orgreater)removemoredentinfromthe
coronalhalfoftheroot,whichunnecessarilyweakenstheroot.

9
o RootFilling/Obturation
Verticalcompactionofguttaperchausingaheatedpluggerandbackfillingwiththermoplasticgutta
perchahasbecomemoreorlessthestandardobturationtechniqueovertheyears.Thebasicpremiseof
thistechniqueisbasedoncreatinga“smallapex”andacontinuouslytapered,flaringcanalusingalarge
taperedinstrument.Thosetwoprinciplesaboutcreatinganapexassmallaspossibleandinstrumenting
thecanalwithacontinuouslytaperedinstrumentrepresentthe“inborn”characteristicsofthisvertical
compactiontechniqueatitsorigin.However,inpastandpresent,thisparticularobturationtechniquehas
hadasomewhatunfortunateinfluenceontheoveralldesignofrotaryinstruments(smalltip,
larger/progressivetaper)inthemarket.Itmustbepointedoutthatthisisprobablytheoppositeofwhat
weshouldbethinking,becauseourfirstpriorityindoingarootcanaltreatmentshouldbeproper
debridinganddisinfectionofthecanals,notfillingtherootsaccordingtothemandatesofaspecific
obturationtechnique.Obturationtechniqueswillevolveandgetmodifiedovertime.Moreover,some
cliniciansmaytakeastandthatitisnotpossibletocreatea“continuouslytaperingfunnel”inallthe
canals.Asstatedbefore,thesizeofinstrumentationremainsanareaofopendiscussion,butwhat
everybodyagreesonisthefactthatbyinstrumentingthecanalswemustcreateastoporaboxjustshort
oftheapicalconstriction.Let’slookatsomeofthetechniquesthatmayfacilitatetherootfillingprocess.
• Indiscriminatelyusingalargequantityofthesealercanmakethingsmoredifficult.Itshouldbe
rememberedthatexcesssealerjustcomesbackoutduringbackfillingwithguttapercha,making
thingsmessier,especiallywhenlargeamountofthesealerisallmuddledupwiththermoplastic
guttapercha.
• Thesealercanalsobeplacedinthecanalbeforeconeplacementeitherwithafileorwitha
smallersizeguttapercha,butthisisnotmandatory.Then,asmallamountofsealercouldbe
placedonthe3-4mmtipoftheguttaperchaconeandplacedinthecanal.
• Anypastetypematerial,suchasthesealerorcalciumhydroxidepasteusedasinter-appointment
medicament,canbeplacedinthecanalbyrotatingafileinacounterclockwisemotion.
Rememberthatthedefaultclockwiserotationofarotaryfileremovesdebrisupandoutofthe
canal.
• Treattheguttaperchaconewithcarewhileplacingitinthecanalwithacollegepliertomake
surethatthetipdoesn’tgetfoldedover.Keepaneyeonthetipuntilitdisappearsintothe
orifice.Then,usingyourfingers,gentlyrotatetheconebackandforthuntilitadvancesallthe
waytoworkinglength.Strictlyusingaverticallydirectedmotionwithoutanyrotationmay
preventtheguttaperchaconefromseatingallthewayinsomecanals.

10
• Twocanalsthatjoin:Inthismorphology,separatelyplacingaguttaperchaconeineachcanal
willallowittoadvancetoworkinglength,butwhenplacedtogether,thefirstconewillprevent
thesecondconefromgettingtolength.Thishappensfrequentlyinthetwomesiobuccalsof
maxillarymolars,thetwomesialsofthemandibularsecondmolars,upperpremolars,andlower
incisors.Youmayalsogetahintofthisparticularanatomyifyouarelookingattheorificeswith
ahigh-poweredmagnificationwhiledryingthecanals,asyoumaybeabletonoticethe
fluctuationofirrigantinthe2ndcanalwhilethe1stcanalisbeingdriedwithapaperpoint.Place
thefirstconeinthecanalthatisassumedtobelargerorstraighter(e.g.,inMB1beforeMB2in
uppermolars,inthepalatalbeforethebuccalinupperpremolars,inthemesiolingualbeforethe
mesiobuccalinmandibularmolars),andthenplacethe2ndguttaperchaconetothepointof
joining.Now,searoffthe2ndconethatisnotreachingtheapexattheorificelevel,thenburnoff
the1stconethatwasinitiallyplacedtolength.Insummary,thestepsareasfollows:Placethe1st
conetolength,placethe2ndconetojoininglevel,burnoffthe2ndcone,thenburnoffthe1st
cone.
• Oneofthemorefrequentlyaskedquestionsregardingobturationtechniqueisaboutfillingthe
canalsthatbranchinto2ormorecanalsfurtherapically.Forallintentsandpurposes,strongly
considerreferringthesecasestoaspecialist.Thelevelofdifficultyisexceedinglyhighinsome
cases,especiallywhenonecanalbranchesoutatasharpangle,andpropermanagementmay
onlybepossiblewiththeuseofamicroscope.
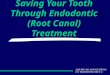
MANDIBULARPREMOLARSWITHTHREECANALS.Thesecasesaretypicallymuchmoredifficultthanmaxillarypremolarswiththreecanals.Propermanagementofatri-furcatingmandibularpremolarmayrequiretheuseofamicroscope.Eachguttaperchaconeneedstobesearedoffatthelevelofbranching,andthiscanonlybedoneifthereisclearvisualizationofallthreeorifices.(1stPA:Pre-op,2ndPA:2guttaperchaconeshavebeensearedoffanda3rdconehasbeenplacedtolength,3rdPA:Post-op)

11
• Help!Myguttaperchadoesn’tgotomyworkinglength!Sometimeswerealizethatdespite
havingfullycompletedtheinstrumentation,theguttaperchaconedoesn’tfitallthewayto
workinglength.Thereareanumberofpossibleexplanationsforthis,butwhateveryoudo,resist
thetemptationtofillit3mmsshortandmaketheall-too-commondefensivestatement—Well,
myapexlocatortoldmethatthatwastheworkinglength.Itneedstobepointedoutthatthe
canalconstrictionisshortoftheradiographicapexandinsomecasestherootfillingcouldlooka
littleshort.Yet,iftheapexlocatorinitiallyindicatedthattheworkinglengthwas20mms,andifI
filleditto18mms,thenthemachinemostcertainlydidnottellmethat18mmswasthelength.
What’sresponsibleforthatdiscrepancyisthehumanerrorinproperexecution.Let’slookat
someofthereasonswhyaguttaperchaconemaynotgofullytoworkinglength:
o Debrisinthecanal:Afilemaystillgotoworkinglengthinpresenceofsomedebris
becauseitismetal,butasoftguttaperchaconemaynot.Hittheapexonemoretime
withthelargestrotaryfileyouused(wipethefilecleanbeforeyoudothis)andthen
irrigatethecanalonemoretime.
o Discrepancyinmanufacturing:Ifyoutook5differentbrandsofguttaperchaand
comparedtheexacttipsizeusingagauge,thenitwouldshowusthatsomebrandsof
guttaperchaarebiggerorsmallerthantheothers.Now,ifyouopenedupapacketof
guttaperchafromonebrandandthencomparedtheguttaperchaconesinthatpacket,
youarestilllikelytogetsomediscrepancyinsizedespitetheconesbeingmadebythe
samemanufacturer.Atanyrate,ifoneconedoesnotfittoyourdesiredlength,try
anotheroneofthesameorsmallersize(whichmayhavetobemodifiedtocreatetug-
back).
o Usingastrictlyverticalmotiontoplacethecone:Asexplainedbefore,incorporatea
rotatingmotionwhenplacingtheguttaperchatomoreeasilygetitdowntotheapexof
acurvedcanal.
FINALTHOUGHTS
BackinthedayswhenIwasadentalstudent,arespectableperiodontistwhowastheheadoftheperiodontics
departmenthadsaidsomethingthatIremembertothisday—thathedidn’tlearntoSRPuntil2yearsafterhe
becameaperiodontist.ThisstatementwassostrikingtomethatIstillrememberthetoneoftheprofessor’s
voicewhenhesaidit.Not2yearsafterhegraduateddentalschool,but2yearsafterhebecameaspecialist.
Myperspectiveabouttheendodonticspecialtyissimilar.AndIsaythisnottomakeitseemlikelearning
aboutrootcanalsisadauntingtask,butasareminderthatcontinuouslylearningtoimproveyourselfand

12
puttingintheeffortcanresultinalevelofproficiencythataddslayersofsatisfactiontoyourpracticeof
dentistry.IfyoucontinuetodoRCTsinyourpractice,youareboundtohavedifficultandfrustratingcasesat
somepoint.Butgettingbetteratanythingworthwhileisahumblingexperiencebecauseitgoeshandinhand
withfailure.Itisonlyhumantobediscouragedbytheseexperiences,butthemostimportantthingistosee
whatcouldbelearnedfromthesechallengingcases.Standup,dustyourselfoff,anddon’tstopdoingyour
carefullyselectedcases.Iwishyouthebestofluck!