Embed Size (px)
Citation preview

aDivision of Emergency Medicine, McMaster University, Hamilton, Ontario, Canada; bHamilton Health Sciences, Centre for Paramedic Education and Research, Hamilton, Ontario, Canada; cDepartment of Critical Care Nursing, Graduate School of Human Health Science, Kyoto University, Kyoto, Japan; dDivision of Neonatalogy, National Center for Child Health and Development, Tokyo, Japan; eNeonatal Services, The Royal Women’s Hospital and University of Melbourne, Melbourne, Australia; fPediatrics and Communicable Diseases, University of Michigan and C. S. Mott Children’s Hospital, Ann Arbor, Michigan; gMedical Sciences Division, Department of Paediatrics, University of Oxford, Oxford, United Kingdom; hNewborn Services, John Radcliffe Hospital, Oxford University Hospitals, National Health Service Foundation Trust, Oxford, United Kingdom; iDivision of Neonatal-Perinatal Medicine, University of Texas Southwestern Medical Center, Dallas, Texas; jDepartment of Pediatrics, University of Calgary, Calgary, Alberta, Canada; and kAlberta Children’s Hospital Research Institute, Calgary, Alberta, Canada
To cite: Welsford M, Nishiyama C, Shortt C, et al. Room Air for Initiating Term Newborn Resuscitation: A Systematic Review With Meta-analysis. Pediatrics. 2019;143(1):e20181825
CONTEXT: The International Liaison Committee on Resuscitation prioritized to rigorously review the initial fraction of inspired oxygen (Fio2) during resuscitation of newborns.OBJECTIVE: This systematic review and meta-analysis provides the scientific summary of initial Fio2 in term and late preterm newborns (≥35 weeks’ gestation) who receive respiratory support at birth.DATA SOURCES: Medline, Embase, Evidence Based Medicine Reviews, and Cumulative Index to Nursing and Allied Health Literature were searched between January 1, 1980 and August 10, 2018.STUDY SELECTION: Studies were selected by pairs of independent reviewers in 2 stages, with a Cohen’s κ of 0.8 and 1.0.DATA EXTRACTION: Pairs of independent reviewers extracted data, appraised risk of bias, and assessed Grading of Recommendations Assessment, Development and Evaluation certainty of evidence.RESULTS: Five randomized controlled trials (RCTs) and 5 quasi RCTs included 2164 patients. Room air (Fio2 0.21) was associated with a statistically significant benefit in short-term mortality compared with 100% oxygen (Fio2 1.0) (7 RCTs; n = 1469; risk ratio [RR] = 0.73; 95% confidence interval [CI]: 0.57 to 0.94). No significant differences were observed in neurodevelopmental impairment (2 RCTs; n = 360; RR = 1.41; 95% CI: 0.77 to 2.60) or hypoxic-ischemic encephalopathy (5 RCTs; n = 1315; RR = 0.89; 95% CI: 0.68 to 1.18).LIMITATIONS: The Grading of Recommendations Assessment, Development and Evaluation certainty of evidence was low for short-term mortality and hypoxic-ischemic encephalopathy and very low for neurodevelopmental impairment.CONCLUSIONS: Room air has a 27% relative reduction in short-term mortality compared with Fio2 1.0 for initiating neonatal resuscitation ≥35 weeks’ gestation.
Room Air for Initiating Term Newborn Resuscitation: A Systematic Review With Meta-analysisMichelle Welsford, BSc, MD, FRCPC, a, b Chika Nishiyama, RN, PhD, c Colleen Shortt, PhD, b Tetsuya Isayama, MD, MSc, PhD, d Jennifer Anne Dawson, RN, PhD, e Gary Weiner, MD, f Charles Christoph Roehr, MD, PhD, g, h Myra H. Wyckoff, MD, i Yacov Rabi, MD, j, k on behalf of the International Liaison Committee on Resuscitation Neonatal Life Support Task Force
abstract
PEDIATRICS Volume 143, number 1, January 2019:e20181825 REVIEW ARTICLE by guest on January 21, 2021www.aappublications.org/newsDownloaded from

Resuscitation guidelines published before 2000 recommended a 100% inspired concentration of oxygen (fraction of inspired oxygen [Fio2] 1.0) for respiratory support of newborns, regardless of gestation.1 However, evidence has emerged over the past decades recognizing that administration of high Fio2 leads to free radical formation and is toxic to the newly born lungs, eyes, brain, and other organs.2 Excess oxygen can be toxic; however, too little oxygen can also lead to harm from hypoxia. The Resair-2 study revealed that using room air (Fio2 0.21) during initial respiratory support in term newborns at birth did not increase mortality or long-term neurodevelopmental impairment (NDI) and resulted in a quicker time to first breath compared with Fio2 1.0.3, 4 A Cochrane systematic review in 2005 confirmed reduction in short-term mortality for newborns initially resuscitated with Fio2 0.21 compared with 1.0.5
The International Liaison Committee on Resuscitation (ILCOR) reviews evidence on important clinical practice questions regarding resuscitation. The review process includes rigorous evaluation of relevant science by a team of multidisciplinary experts culminating in a consensus on the science with treatment recommendations (CoSTRs). In 2010, ILCOR recommended using Fio2 0.21 rather than 1.0 for newborns born at term who received respiratory support at birth; however, this was before the incorporation of Grading of Recommendations Assessment, Development and Evaluation (GRADE) assessment into CoSTRs.6 The 2015 ILCOR guidelines continued to recommend the use of room air during initial resuscitation for term newborns but did not provide an updated review.7 Recently, ILCOR has moved from a 5 year review cycle to a continuous evaluation process, and this provided an opportunity to
perform an updated analysis on this topic by using rigorous methodology including GRADE.
This systematic review and meta-analysis is the core that serves as the “consensus on science” for the ILCOR CoSTRs. This scientific summary was completed in parallel and in collaboration with ILCOR and is published separately from the ILCOR CoSTRs, which will be published in the fall of 2019 and will focus on the treatment recommendations. In cooperation with the ILCOR Neonatal Life Support (NLS) task force, we investigate in this meta-analysis initiating resuscitation with lower compared with higher Fio2 on mortality and morbidity among term and late preterm newborns (≥35 weeks’ gestation) who receive respiratory support at birth. The primary outcome is short-term mortality. Secondary outcomes include long-term mortality, NDI, and the proportion of neonates with hypoxic-ischemic encephalopathy (HIE).
METHODS
Protocol
This systematic review and meta-analysis was conducted in accordance with the Cochrane Handbook for Systematic Reviews of Interventions and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement for meta-analysis in health care interventions.8, 9 The protocol was registered in advance of article selection with the Prospective Register of Systematic Reviews (registered January 8, 2018; CRD42018084902; see Supplemental Information). The protocol included term and preterm newborns as predetermined subgroups, and these were separated into different analyses after initial article selection. Studies were included in this systematic review if >75%
of the newborns were ≥35 weeks’ gestation. The cutoff at 35 weeks’ gestation was chosen on the basis of the experience of our clinical experts that late preterm infants were more similar physiologically to term infants than the population of very premature infants enrolled in the preterm randomized controlled trials (RCTs) and pragmatically based on the knowledge of the enrollment criteria for previous studies.
Outcomes
The selection and importance rating of patient-oriented outcomes for term and late preterm newborns ≥35 weeks’ gestation were determined in advance through discussion and consensus with the ILCOR NLS task force.10 The outcomes centered on all-cause mortality and neurologic impairment.10 When available, we collected all-cause mortality at 2 time intervals: short-term (primary outcome, in-hospital or up to 30 days postnatal) and long-term (1–3 years); and neurologic impairment at 2 time intervals: short-term HIE (Sarnat Stage II–III), and long-term NDI (moderate to severe at 1–3 years).11 NDI is commonly defined as having at least 1 of cerebral palsy, cognitive impairment, visual impairment, or hearing impairment and is categorized by severity. Where available, we extracted data for moderate to severe NDI at 1 to 3 years based on the Gross Motor Function Classification System and Bayley Scales of Infant and Toddler Development, Third Edition.12, 13
Search Strategy
Ovid Medline, Embase, all Evidence Based Medicine Reviews (including Cochrane CENTRAL and others), and EBSCOhost Cumulative Index to Nursing and Allied Health Literature (CINAHL) were searched for relevant neonatal literature between January 1, 1980, and December 11, 2017, without language restrictions. The search was updated from December
WELSFORD et al2 by guest on January 21, 2021www.aappublications.org/newsDownloaded from

1, 2017, to August 10, 2018, before publication (Supplemental Tables 6 and 7). The searches were limited to the last 4 decades because no pertinent studies were expected before this. An iterative approach was used to ensure that key articles (identified by content experts and in previous systematic review articles) were found. Additionally, we searched the first 200 hits on Google Scholar, references of systematic reviews on the topic, references of the ILCOR 2010 and 2015 CoSTRs, and trial registries (clinicaltrials.gov; the International Standard Randomized Controlled Trial Number Registry, isrctn.com; and the EU Clinical Trials Register, clinicaltrialsregister.eu; last searched August 10, 2018).
Study Selection and Data Extraction
Covidence software was used for study selection in 2 steps (Covidence systematic review software; Veritas Health Innovation, Melbourne, Australia; www. covidence. org). Pairs of independent reviewers screened titles and abstracts. In the event of a disagreement at abstract screening, the full text was reviewed. Independent reviewers subsequently completed full-text review for eligibility in duplicate. A third reviewer was involved for disagreements at the full-text stage, and final decisions were determined by consensus. The first reason for exclusion was captured according to a predetermined, ordered list of exclusions. Interrater agreement for article selection was assessed by using Cohen’s κ coefficient at the abstract and full-text stages.
RCTs, quasi randomized controlled trials (qRCTs), and nonrandomized (observational) studies were eligible if they included comparison of low with high initial oxygen concentration for respiratory support at birth. Review articles, editorials, comments, case reports, and small case series (≤10 patients) were
excluded. We excluded studies that were focused on oxygen use beyond the initial stabilization in the delivery room or studies that were focused on oxygen saturation targeting and not initial oxygen concentration. To avoid publication bias, the protocol was amended to include data from conference abstracts (not otherwise published) in a sensitivity analysis if the authors provided enough information to confirm the methods, key patient characteristics, and outcomes.
Data Collection, Bias, and Quality Assessment
For each study, pairs of authors independently extracted predetermined study characteristics and study outcomes and then achieved consensus. Pairs of independent authors evaluated risk of bias (RoB) in individual studies using the Cochrane Risk of Bias Tool for RCTs and the Risk of Bias in Non-Randomized Studies of Interventions tool for observational studies.8, 14 Similarly, 2 authors assessed the certainty of evidence (confidence in the estimate of effect) for each outcome on the basis of the GRADE framework, including calculating the optimal information size to assess imprecision (GRADEpro Guideline Development Tool, McMaster University, Ontario, Canada; available at gradepro.org).15 The RoB and GRADE assessments were then reviewed by ILCOR content experts who are also authors to achieve consistency and consensus.
Data Analysis
Covidence, GRADEpro, and Review Manager software (RevMan 5.3; The Nordic Cochrane Centre, Copenhagen, Denmark) were used to abstract, summarize, and analyze the data, respectively.
Meta-analyses were performed if ≥2 studies were available. Heterogeneity was measured by using the I2 statistic.16 Because multiple small
studies (<250 patients) were anticipated, a random effects model was used for analysis. We report pooled unadjusted risk ratios (RRs) and corresponding 95% confidence intervals (CIs) using the Mantel-Haenszel method for dichotomous variables. Forest plots were used for graphical representation of RRs. To assess for publication bias, we visually inspected funnel plots where >8 studies were available. The absolute risk difference and number needed to treat (NNT) were calculated where the pooled estimate from RCTs revealed a statistically significant benefit by using the method recommended by the Cochrane Collaboration.17
Sensitivity analyses were completed where inclusion of 1 or more studies was uncertain because of a high RoB, incongruent allocation, mixture of adjusted and nonadjusted analyses, or significant heterogeneity.
Prespecified subgroup analyses were planned if >2 studies were available with relevant outcome information related to gestational ages (≥35 and ≥37 weeks’ gestation), specific Fio2 ranges, or oxygen saturation targeting as a cointervention.
RESULTS
Literature Search and Study Selection
Using this search strategy, we identified a total of 2366 records; after removing 967 duplicates, 1399 records were screened by title and abstract. Five additional studies (abstracts) were found via reference searches and added to full-text screening. A total of 59 full-text articles were assessed for eligibility, and 12 publications on term or late preterm newborns were included.2 – 4, 18 – 26 The Cohen’s κ coefficient, a measure of interrater agreement, was 0.81 (excellent) at the abstract stage and 1.0 (full agreement) at the full-text stage.
PEDIATRICS Volume 143, number 1, January 2019 3 by guest on January 21, 2021www.aappublications.org/newsDownloaded from

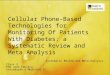
See Fig 1 for the PRISMA study selection diagram including the reasons for article exclusion.
Of the additional studies found via reference searches, 1 study published in Romanian with an English abstract was originally excluded because it did not include outcomes of interest.22 However, the publication included a full description of methods and the first author provided additional relevant outcome data; therefore, the full-text of the study was translated and included. Three additional titles by the same first author were identified but were only published as conference abstracts.23 – 25 The author provided additional information regarding methodology, patient characteristics, and outcomes for all 3 of these studies and thus they were included in sensitivity analysis.
Another article of note included both randomized and observational data for 830 term newborns over a 6-year time period (1994–1999) at a single center.19 Some of the randomly assigned patients overlapped with
other included publications.3, 20 The first author provided additional information and outcomes for a subset of 537 patients who were randomly assigned but not published in other included studies. Thus, the study was included in the systematic review and considered for the meta-analysis.
Lastly, a search of clinical trial registries (www. clinicaltrials. gov, www. isrctn. com, and www. clinicaltrialsreg ister. eu) revealed no additional published or unpublished term or late preterm studies.
Study Characteristics
In Table 1, we summarize the characteristics of the included studies and highlight these differences. Of the 12 included articles, there were 10 original studies and 2 publications of follow-up data. Five were quasi randomized on the basis of alternating days and 5 were RCTs, but only 2 were fully randomized with blinding of allocation and intervention. No eligible
observational cohort studies were identified. Ten studies contained reports of short-term mortality (in hospital or up to 30 days postnatal), 7 contained reports of HIE (Sarnat Stage II–III), 1 contained a report of long-term mortality (1–3 years), and 3 contained reports of NDI (moderate to severe, 1–3 years).
A total of 2164 patients were included in studies ranging from 44 to 609 patients. Most studies were from India and Europe; they were published between 1993 and 2007, with patient recruitment from 1990 to 2007. In 4 of 10 studies, the authors reported multicenter data. The authors of all the included studies compared initiating Fio2 0.21 with Fio2 1.0.
The Resair-2 study was a large, nonblinded, multicenter qRCT (allocated by even and odd days). There were 10 sites, which were predominantly low-resource settings with high event rates.3 The authors of the original study indicated that the researchers enrolled 609 patients but subsequently determined data from 18 neonates had been duplicated.4 The authors reported that the corrected demographics and outcomes revealed no difference. As the specific outcome and demographic data for the corrected numbers was not available, the original data were used. The follow-up data at 18 to 24 months used the corrected numbers, but only some of the original centers were included, and there was significant loss to follow-up such that only 66% had follow-up data.
Although the reporting of mortality was similar, the definition of NDI was different among the 3 studies that contained reports of it. In the Resair-2 follow-up publication, they evaluated whether the neonates had developed normally using an unvalidated simple assessment tool.4 In Bajaj et al, 21 NDI assessment was performed by using the Baroda development screening
WELSFORD et al4
FIGURE 1PRISMA flow diagram of study selection. EBM, evidence-based medicine.
by guest on January 21, 2021www.aappublications.org/newsDownloaded from

test (modified Bayley), and <97% score on the development screening test was defined as neurologically abnormal. In Toma et al, 22 they assessed NDI using the Bayley Scales of Infant and Toddler Development, Third Edition and divided neonates into 3 categories: high, moderate, and low according to a total score. Where available, we extracted information on moderate to high NDI. Additionally, HIE reported in Ramji et al26 required clarification, and the data used in our analysis were confirmed with the authors.
Patient Characteristics
In Table 2, we outline the patient characteristics of the included studies. The intervention and comparator groups were similar in most of the key prognostic variables (although patient characteristics was not available for 1 study).19 Eight of the 10 studies included either term or late preterm newborns (≥35 weeks’ gestation), 1 study included newborns ≥34 weeks’ gestation, and 1 study (including follow-up publication) included some preterm patients but <25% were <35 weeks’ gestation (median 38, interquartile range [IQR] 31–42 weeks’ gestation).3, 4, 22 The gestational age mean and median ranged from 35.3 to 40.5 weeks with well-matched intervention and comparator groups. The birth weight mean and median ranged from 2319 to 3536 g and were also well matched. Researchers did not routinely report sex, but those that did reported a slight male sex predominance (49%–60%). Intubation and mechanical ventilation were not routinely reported but ranged from 10% to 51%. Apgar scores were well matched between the 2 comparators.
RoB
The RoB assessment for each study is summarized in Table 3. Only 2 studies were fully randomized and blinded for participants, personnel, and assessors;
PEDIATRICS Volume 143, number 1, January 2019 5
TABL
E 1
Stud
y Ch
arac
teri
stic
s
Term
(≥
35 w
k) R
ando
miz
ed a
nd q
RCTs
Stud
ySt
udy
Char
acte
rist
ics
Tota
l Pa
tient
sGe
stat
iona
l Age
Patie
nts
by
Oxyg
en L
evel
s,
n
Oxyg
en L
evel
De
finiti
on, %
O 2 Sat
Ta
rget
Outc
omes
Year
s of
Re
crui
tmen
tCo
untr
y of
Re
crui
tmen
tM
ulti-
or
Sing
le
Cent
er
Stud
y De
sign
Blin
ding
of
Gas
<35
wk
≥35
w
kLo
wHi
ghST
MLT
MND
IHI
E
Ram
ji et
al18
1990
–199
1In
dia
Sing
leqR
CT b
y da
teNo
84—
Yes
4242
Low
, 21;
hig
h, 1
00No
Yes
——
Yes
Saug
stad
et a
l319
94–1
996
Mul
tiM
ulti
qRCT
by
date
No60
9<2
5%Ye
s28
832
1Lo
w, 2
1; h
igh,
100
NoYe
s—
—Ye
s
Vent
o et
al19
a19
94–1
999
Spai
nSi
ngle
qRCT
by
date
No53
7—
Yes
300
237
Low
, 21;
hig
h, 1
00No
Yes
——
—
Ram
ji et
al26
1995
–199
7In
dia
Mul
tiqR
CT b
y da
teNo
431
—Ye
s21
022
1Lo
w, 2
1; h
igh,
100
NoYe
s—
—Ye
s
Saug
stad
et a
l419
94–1
996
Mul
tiM
ulti
qRCT
by
date
No41
0<2
5%Ye
s91
122
Low
, 21;
hig
h, 1
00No
——
Yes
—
Vent
o et
al20
2000
–200
1Sp
ain
Sing
leRC
TYe
s10
6—
Yes
5155
Low
, 21;
hig
h, 1
00No
Yes
——
—Ba
jaj e
t al21
2001
–200
2In
dia
Sing
leqR
CT b
y da
teNo
204
—Ye
s10
797
Low
, 21;
hig
h, 1
00No
Yes
—Ye
sYe
s
Vent
o et
al2
1999
–200
2Sp
ain
Sing
leRC
TYe
s39
—Ye
s17
22Lo
w, 2
1; h
igh,
100
NoYe
s—
——
Tom
a et
al22
2006
Rom
ania
Sing
leRC
TNo
44≥
34 w
kYe
s20
24Lo
w, 2
1; h
igh,
100
NoYe
s—
—Ye
sTo
ma
et a
l23a
2005
Rom
ania
Mul
tiRC
TNo
54—
Yes
2727
Low
, 21;
hig
h, 1
00No
Yes
——
Yes
Tom
a et
al25
a20
06–2
007
Rom
ania
Mul
tiRC
TNo
56—
Yes
3026
Low
, 21;
hig
h, 1
00No
Yes
——
Yes
Tom
a et
al24
a20
05Ro
man
iaSi
ngle
RCT
No54
—Ye
s27
27Lo
w, 2
1; h
igh,
100
No—
Yes
Yes
—
LTM
, lon
g-te
rm m
orta
lity;
STM
, sho
rt-te
rm m
orta
lity;
—, n
ot a
pplic
able
.a
Stud
y w
as o
nly
incl
uded
in s
ensi
tivity
ana
lysi
s.
by guest on January 21, 2021www.aappublications.org/newsDownloaded from

WELSFORD et al6
the majority of the studies were determined to have a high RoB.
The 3 articles that were published as conference abstracts were determined to have a critical RoB and thus were included in the sensitivity analysis but not the primary meta-analysis.11, 24, 25 Additionally, although outcome data were provided for the
randomly assigned subset of patients from Vento et al, 20 the demographic information for this subset was not available, and the imbalance in the numbers randomly assigned to each group was unexplained (300 compared with 237). For these reasons, this study was found to have a critical RoB and only included in
the sensitivity analysis and not the primary meta-analysis.
Outcome Analysis
Results of the meta-analysis are detailed below and shown in the Figs 2–5 forest plots.
TABLE 2 Patient Characteristics
Study Oxygen Level Gestational Age, wk
Male Sex, % Birth Wt, g Apgar Score at 5 min
Cesarean Delivery, %
Intubation and Mechanical
Ventilation, %
Chest Compressions, %
Ramji et al18 Low 38.4 (1.9)a N/A 2410 (540)a 8 (7–9)b 24 14 N/AHigh 38.1 (2.6)a N/A 2410 (660)a 7 (6–8)b 21 33 N/A
Saugstad et al3 Low 38 (32–42)b 54 2600 (1320–4078)b 8 (4–9)c 41 25 N/AHigh 38 (31–42)b 59 2560 (1303–3900)b 7 (3–9)c 37 26 N/A
Vento et al19,d Low N/A N/A N/A N/A N/A N/A N/AHigh N/A N/A N/A N/A N/A N/A N/A
Ramji et al26 Low 37.9 (2.9)a N/A 2400 (563)a 7 (3–10)b 83 N/A N/AHigh 38.1 (2.6)a N/A 2529 (629)a 7 (2–10)b 88 N/A N/A
Saugstad et al4 Low 38 (32–42)b 49 2650 (1490–4240)b 8 (4.6–9.0)c N/A N/A N/AHigh 39 (33–42)b 60 2800 (1560–4300)b 8 (4.1–9.0)c N/A N/A N/A
Vento et al20 Low 38.9 (1.6)a N/A 3160 (240)a 6 (5–8)c 69 10 N/AHigh 40.5 (1.1)a N/A 3220 (168)a 6 (4–8)c 75 13 N/A
Bajaj et al21 Low 38.3 (2.8)a 54 2461 (602)a 6.8 (2.0)a 50 51 7High 37.4 (3.5)a 58 2319 (614)a 7.1 (1.6)a 41 35 0
Vento et al2 Low 39.6 (1.6)a N/A 3320 (180)a 5 (3–5)b N/A 41 N/AHigh 39.2 (1.1)a N/A 3110 (90)a 4 (3–5)b N/A 36 N/A
Toma et al22 Low 36.0 (2.69)a N/A 2684 (1013)a N/A N/A N/A N/AHigh 35.3 (2.22)a N/A 2468 (685)a N/A N/A N/A N/A
Toma et al23, 24,d Low 39.1 (1)a N/A 3536 (519)a 8 (3.4–10.0)a N/A N/A N/AHigh 39.2 (0.7)a N/A 3530 (337)a 8 (2.4–10.0)a N/A N/A N/A
Toma et al25d Low 38.8 (0.78)a N/A 3172 (599)a N/A N/A N/A N/AHigh 38.6 (0.58)a N/A 3200 (200)a N/A N/A N/A N/A
N/A, not available (not collected in original study).a Reported as mean (SD).b Reported as median (IQR).c Reported as median (5th–95th percentile).d Study was only included in sensitivity analysis.
TABLE 3 RoB According to Cochrane RCTs Criteria
Cochrane RoB for RCTs
Study Sequence Generation
Allocation Concealment
Blinding of Participants
and Personnel
Blinding of Outcome
Assessors
Incomplete Outcome Data
Selective Outcome Reporting
Other Sources of Bias
Overall Bias
Ramji et al18 High High High High Low Low Unclear HighSaugstad et al3 High High High High Low Low Unclear HighVento et al19a High High High High Unclear High High CriticalRamji et al26 High High High Unclear Unclear Unclear Low HighSaugstad et al4 High High High Unclear High Unclear Unclear HighVento et al20 Low Low Low Unclear Low Unclear Low UnclearBajaj et al21 High High High Low Low Low Low HighVento et al2 Low Low Low Unclear Low Low Unclear UnclearToma et al22 Low High High High Unclear Low High HighToma et al23,a Low High High High Unclear Low High CriticalToma et al24,a Low High High High Unclear Unclear High CriticalToma et al25,a Low High High High Unclear Unclear High Critical
a Denotes articles of critical RoB and only included in sensitivity analysis.
by guest on January 21, 2021www.aappublications.org/newsDownloaded from

Short-term Mortality
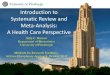
Seven RCTs and qRCTS involving 1469 term and late preterm newborns (≥35 weeks’ gestation) containing reports on short-term mortality (in-hospital or up to 30 days postnatal) were included in the meta-analysis.2, 3, 19, 21– 23 The pooled estimate demonstrated a statistically significant reduction in
mortality for Fio2 0.21 compared with 1.0 (RR = 0.73; 95% CI: 0.57 to 0.94; I2 = 0%). The absolute survival benefit (absolute risk difference) is 4.6% (95% CI: 1.0% to 7.3%) and the relative survival benefit is 27%. Based on an assumed control risk of 17.0% (from the mortality rate of the comparison group), the NNT with room air to have 1 additional survivor (short-term) is
22 (95% CI: 14 to 99). The forest plot is presented in Fig 2A. Heterogeneity was low as evidenced by the low I2 = 0%, visual inspection of the forest plot, and similarities in the included populations. Although the CIs from the included studies crossed the null effect line, all studies trended in the same direction (favoring room air), and the summary estimate from the
PEDIATRICS Volume 143, number 1, January 2019 7
FIGURE 2Summary of results: term newborns receiving respiratory support comparing Fio2 0.21 with 1.0. A, Short-term mortality (in-hospital or up to 30 days).
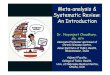
FIGURE 3Summary of results: term newborns receiving respiratory support comparing Fio2 0.21 with 1.0 (continued). B, Short-term mortality (in-hospital or up to 30 days) sensitivity analysis demonstrating studies that are blinded, unblinded, and at critical RoB.
by guest on January 21, 2021www.aappublications.org/newsDownloaded from

meta-analysis provides confirmation that initial room air improves survival.
To explore the reasons for heterogeneity, a sensitivity analysis was conducted for the primary outcome of short-term mortality to compare studies that were blinded, unblinded, and those at a critical RoB (Fig 3B).19, 23, 25 Inclusion of data from the studies at a critical RoB to the meta-analysis (additional 647 neonates from 3 studies) made no appreciable change in the outcome estimate for short-term mortality, favoring an Fio2 0.21 compared with 1.0 (RR = 0.71; 95% CI: 0.56 to 0.91; I2 = 0%).
Long-term Mortality
Long-term mortality (1–3 years) was reported in 1 abstract with a critical RoB, involving a total of 54 patients with no deaths in either group.24
NDI
NDI (moderate to severe, 1–3 years) was reported in 2 qRCTs involving
360 term and late preterm newborns (≥35 weeks’ gestation, Table 2). The summary estimate from meta-analysis revealed no difference in initiating respiratory support with Fio2 0.21 compared with 1.0 (RR = 1.41; 95% CI: 0.77 to 2.60; I2 = 0%).4, 21
The sensitivity analysis for NDI involving 1 additional study that was determined to be at a critical RoB (414 patients from 3 studies), still demonstrated no statistically significant difference (RR = 1.24; 95% CI: 0.73 to 2.10; I2 = 0%) for Fio2 0.21 compared with 1.0.24
HIE
HIE (Sarnat Stage II–III) was reported in 5 RCT and/or qRCTs involving 1315 term and late preterm newborns (≥35 weeks’ gestation) receiving respiratory support at birth included in the meta-analysis and revealed no statistically significant difference in Fio2 0.21 compared with
1.0 (RR = 0.90; 95% CI: 0.71 to 1.14; I2 = 8%) (Fig 5D).3, 18, 21, 22, 26
Sensitivity analysis for HIE (Sarnat Stage II–III) was performed with 3 additional studies that were determined to be at a critical RoB. Data from these 8 studies and 2006 neonates did not change the RR appreciably and still demonstrated no statistically significant difference (RR = 0.89; 95% CI: 0.73 to 1.10; I2 = 0%) for Fio2 0.21 compared with 1.0.19, 23, 25
Subgroup Analyses
The authors of all studies compared Fio2 0.21 with 1.0, and thus subgroup analysis according to different initial oxygen concentrations was not possible. There were no data for the planned subgroups analyses related to different gestational ages and whether oxygen saturation targeting was included as a cointervention.
The GRADE summary of quality evaluation for the primary outcomes is presented in Table 4. RCTs start at high
WELSFORD et al8
FIGURE 4Summary of results: term newborns receiving respiratory support comparing Fio2 0.21 with 1.0 (continued). C, Long-term NDI (1–3 years).
FIGURE 5Summary of results: term newborns receiving respiratory support comparing Fio2 0.21 with 1.0 (continued). D, HIE (Sarnat Stage II–III). df, degrees of freedom; M-H, Mantel-Haenszel method; Random, random effects.
by guest on January 21, 2021www.aappublications.org/newsDownloaded from

certainty. Because of concerns with RoB, inconsistency, and imprecision, the certainty of the results was downgraded. The ILCOR NLS Task Force provided the expert opinion that it was unlikely that there were any additional unpublished studies on this topic given the intense clinical interest in this topic, the international reach and involvement of the committee, and the extensive search including uncovering abstracts and conference proceedings. Therefore, the outcomes were not downgraded for publication bias. The GRADE certainty was determined to be low for short-term mortality and HIE and very low for NDI because of serious concerns with RoB and imprecision. The ratings of the importance of outcomes for the GRADE analysis were all “critical” and ranged from 7 to 9 on the 9-point scale.
DISCUSSION
In this systematic review and meta-analysis involving 2164 neonates ≥35 weeks’ gestation, we demonstrate a 27% relative survival benefit and 4.6% absolute survival benefit (short-term) when initial room air is compared with Fio2 1.0 for neonates receiving respiratory support at birth. This corresponds to an NNT with room air to have 1 additional survivor (short-term) of 22. There were no statistically significant differences for HIE and NDI. The GRADE certainty of evidence was low for short-term mortality and HIE and very low for NDI.
The last ILCOR analysis of initial oxygen use for term neonatal resuscitation was completed in 2010 before the adoption of the GRADE methodology for ILCOR reviews. The ILCOR 2010 NLS CoSTR stated, “In term infants receiving resuscitation at birth with positive pressure ventilation, it is best to begin with air rather than 100% oxygen. If despite effective ventilation there is no increase in heart rate or if oxygenation (guided by oximetry) remains unacceptable, use of a
PEDIATRICS Volume 143, number 1, January 2019 9
TABL
E 4
GRAD
E Su
mm
ary
of F
indi
ngs
Cert
aint
y As
sess
men
tNo
. Pat
ient
sEf
fect
Cert
aint
yIm
port
ance
(R
atin
g Sc
ale)
No.
Stud
ies
Stud
y De
sign
RoB
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nOt
her
Room
Air
Ev
ents
/n (
%)
100%
Ev
ents
/n,
(%)
Rela
tive
(95%
CI)
Abso
lute
(9
5% C
I)
Shor
t-ter
m m
orta
lity
(in-
hosp
ital o
r 30
d
post
nata
l)
7RC
TSe
riou
saNo
t ser
ious
Not s
erio
usSe
riou
sbNo
nec
89/7
14 (
12.5
)12
8/75
5 (1
7.0)
RR 0
.73
(0.5
7 to
0.
94)
−46
of 1
000
(−10
to
−73
)
⨁⨁
◯◯
Lo
wCr
itica
l (9)
NDI (
mod
erat
e-se
vere
, 1–3
y)
2RC
TVe
ry s
erio
usd
Not s
erio
usNo
t ser
ious
Very
se
riou
seNo
nec
20/1
68 (
11.9
)17
/192
(8
.9)
RR 1
.41
(0.7
7 to
2.
60)
36 o
f 100
0 (−
20 to
−
42)
⨁◯
◯◯
Ve
ry L
owCr
itica
l (8)
HIE
(Sar
nat S
tage
II–
III)
5RC
TSe
riou
sfNo
t ser
ious
Not s
erio
usSe
riou
sgNo
nec
117/
661
(17.
7)13
7/69
8 (1
9.6)
RR 0
.90
(0.7
1 to
1.
14)
−20
of 1
000
(27
to
−57
)
⨁⨁
◯◯
Lo
wCr
itica
l (7)
a Fi
ve o
ut o
f 7 s
tudi
es h
ave
a hi
gh r
isk
of “
allo
catio
n se
quen
ce, ”
“allo
catio
n co
ncea
lmen
t, ” a
nd “
blin
ding
.” Th
ese
dom
ains
may
influ
ence
the
outc
ome.
b To
tal n
umbe
r of
pat
ient
s (1
469)
incl
uded
in th
e SR
was
less
than
OIS
(21
46).
c The
ILCO
R NL
S Ta
sk F
orce
pro
vide
d th
e ex
pert
opi
nion
that
it w
as u
nlik
ely
that
ther
e w
ere
any
furt
her
unpu
blis
hed
stud
ies
on th
is to
pic.
The
refo
re, t
he o
utco
mes
wer
e no
t dow
ngra
ded
for
publ
icat
ion
bias
.d
Both
stu
dies
hav
e hi
gh r
isk
of “
allo
catio
n se
quen
ce, ”
“allo
catio
n co
ncea
lmen
t, ” a
nd “
blin
ding
.” ND
I sho
uld
be id
eally
ass
esse
d by
a b
linde
d as
sess
or b
ut “
blin
ding
of d
ata
colle
ctor
s” w
as u
ncle
ar. A
nd t
he fo
llow
-up
rate
(Sa
ugst
ad e
t al
4 ) w
as
extr
emel
y lo
w (
only
app
roxi
mat
ely
two-
thir
ds o
f pat
ient
s).
e Nin
ety-
five
perc
ent C
I of R
R in
clud
ed b
oth
bene
fit a
nd h
arm
(RR
of u
nder
0.7
5 or
ove
r 1.
25 a
s a
roug
h gu
ide)
, dow
ngra
de im
prec
isio
n tw
ice.
f All
stud
ies
have
the
high
ris
k of
“al
loca
tion
conc
ealm
ent”
and
“bl
indi
ng”
affe
ctin
g th
e ou
tcom
e.g
Nine
ty-fi
ve p
erce
nt C
I inc
lude
s 1.
0 (a
bsol
ute
effe
ct)
alth
ough
CI r
elat
ivel
y na
rrow
, dow
ngra
de im
prec
isio
n on
ce.
by guest on January 21, 2021www.aappublications.org/newsDownloaded from

higher concentration of oxygen should be considered.” 6 After the release of this CoSTR, there was widespread adoption of initial room-air resuscitation worldwide. The Neonatal Resuscitation 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations did not update the CoSTR.7
The ILCOR NLS Task Force prioritized this research question in 2017 because of the strong desire to have the existing evidence subjected to a methodologically rigorous review including GRADE analysis of confidence in effect. In Table 5, we compare this analysis to key previously published meta-analyses.5, 27 – 30 The results are fairly consistent across the meta-analyses, with the largest number of patients included in the current publication’s sensitivity analysis and the Saugstad et al27 publication.
There have been no new publications of term studies on this topic since 2007; therefore, we are left with these few older studies from a different era, with their inherent differences to current state-of-the-art neonatal resuscitation to reflect on the evidence for current care. This previous evidence, despite low and very low confidence in the point effect estimates, has low statistical heterogeneity and consistent short-term mortality excess with Fio2 1.0. The findings of the current systematic review and meta-analysis are similar to the 2010 ILCOR review and indicate benefit in short-term mortality by initiating respiratory support at birth for term and late preterm newborns (≥35 weeks’ gestation), with room air compared with Fio2 1.0. There are no identified term or late preterm studies comparing outcomes at any intermediate oxygen concentration between these 2 extremes. However, given that practice has changed to initiating resuscitation
WELSFORD et al10
TABL
E 5
Com
pari
son
of M
eta-
anal
yses
This
stu
dyTh
is s
tudy
aSa
ugst
ad e
t al27
,bRa
bi e
t al28
,cTa
n et
al5,
dSa
ugst
ad e
t al29
,eDa
vis
et a
l30,f
Shor
t-ter
m m
orta
lity
RR 0
.73
RR 0
.71
RR 0
.69
RR 0
.63
RR 0
.71
OR 0
.59
RR 0
.75
(0.5
7–0.
94)
(0.5
6–0.
91)
(0.5
4–0.
88)
(0.4
2–0.
94)
(0.5
4–0.
94)
(0.4
0–0.
87)
(0.5
6–1.
0)n
= 14
69N
= 21
16n
= 21
33n
= 13
76n
= 12
75n
= 15
02n
= 65
9ND
I (1–
3 y)
RR 1
.41
RR 1
.24
——
RR 1
.56
—RR
1.5
6(0
.77–
2.66
)(0
.73–
2.10
)—
—(0
.76–
3.22
)—
(0.7
6–3.
22)
n =
360
n =
414
——
n =
213
—n
= 12
2HI
E (S
arna
t Sta
ge II
–III)
RR 0
.90
RR 0
.89
RR 0
.88
RR 0
.86
RR 0
.84
—RR
0.8
4(0
.71–
1.14
)(0
.74–
1.10
)(0
.72–
1.08
)(0
.65–
1.14
)(0
.65–
1.08
)—
(0.6
5–1.
08)
n =
1359
n =
2006
n =
2133
n =
693
n =
1124
—n
= 58
4
RR <
1 fa
vors
Fio2 0
.21
com
pare
d w
ith 1
.0. —
, not
app
licab
le.
a Se
nsiti
vity
ana
lysi
s in
clud
ing
3 ad
ditio
nal s
tudi
es.
b In
clud
ed V
ento
et a
l19 a
nd 2
Tom
a ab
stra
cts24
, 25.
c Sho
rt-te
rm m
orta
lity
defin
ed a
s m
orta
lity
at 1
mo.
d De
ath
at la
test
follo
w-u
p, a
bnor
mal
dev
elop
men
t at 1
8–24
mo.
e Res
ults
rep
orte
d as
odd
s ra
tio n
ot R
R.f S
hort
-term
mor
talit
y de
fined
as
deat
h in
firs
t wk;
NDI
defi
ned
as a
bnor
mal
dev
elop
men
t.
by guest on January 21, 2021www.aappublications.org/newsDownloaded from

with room air and using oxygen saturation monitoring to adjust oxygen administration, the precise initial Fio2 may have become less important, and it is unlikely that there will be any future studies on this topic.
In this systematic review and meta-analysis, we include a prespecified protocol, broad search strategy, additional unpublished data from authors, unpublished studies (abstracts) included in sensitivity analyses, use of GRADE to describe certainty in effect estimate, a team of expert systematic reviewers coupled with international multidisciplinary experts in neonatology, and adherence to PRISMA reporting.
However, several limitations are worth noting. First, out of 10 trials, all but 2 had high RoB, 5 studies used a quasi-randomized design (alternating days), and 8 did not have allocation concealment or personnel blinding. This serious RoB, as well as imprecision, make the certainty of the evidence low or very low. In addition, the mortality incidence was vastly different between studies. Short-term mortality ranged from 1.5% in Vento et al19 (Spain) to 15% in Ramji et al26 (India), and 18% in Saugstad et al3 (patients were mostly from India, Egypt, and Philippines). Studies with high mortality are more heavily weighted in the meta-analyses, and thus caution is needed to ensure similar results are found in countries with lower newborn mortality. Furthermore, all of the studies were conducted >10 years ago and before continuous oxygen saturation monitoring and oxygen titration during delivery room resuscitation were routine. Therefore, it is not clear whether the same results would be found in the setting of current clinical practice in which the inspired oxygen concentration is titrated to achieve targeted levels of oxygen saturation.7 The evidence in which
long-term NDI was evaluated was limited because of the small sample size included in the 2 eligible trials and 1 abstract. We assessed HIE as a short-term neurologic outcome as oxygen administration was historically investigated as a treatment; however, the pathogenesis of HIE starts in utero and HIE may not accurately predict important long-term neurologic outcomes.31 Lastly, all the trials included in this review compared initial room air with Fio2 1.0; therefore, whether room air is superior to other low or intermediate Fio2 (eg, Fio2 0.30) is not known.
CONCLUSIONS
With this systematic review and meta-analysis, we confirm a statistically significant reduction in short-term mortality (without statistically significant differences in short- and long-term neurologic outcomes) by using initial room air compared with Fio2 1.0 (100% oxygen) for term and late preterm newborns (≥35 weeks’ gestation) receiving respiratory support at birth. The certainty of effect is low (short-term mortality); however, the results are consistent across studies with no evidence of statistical heterogeneity and represent the best available evidence to answer this important question.
ACKNOWLEDGMENTS
The authors would like to express their appreciation to the following for contributing valuable support to improve this review: Laurie J. Morrison (ILCOR Continuous Evidence Evaluation Working Group Liaison), and Carolyn Ziegler (St. Michael’s Hospital Information Specialist) and Andrei Harabor (article translation). The authors would also like to highlight the following researchers who kindly contributed valuable information and data from
their studies to improve this review: Naveen Bajaj, Ola Saugstad, Adrian Toma, and Maximo Vento.
Besides the authors Tetsuya Isayama, Charles Christoph Roehr, Myra H. Wyckoff, and Yacov Rabi, members of the International Liaison Committee on Resuscitation Neonatal Life Support Task Force include: Jonathan Wyllie, Jeffrey M. Perlman, Khalid Aziz, Ruth Guinsburg, Maria Fernanda de Almeida, Vishal Kapadia, Daniele Trevisanuto, Sithembiso Velaphi, Lindsay Mildenhall, Helen Liley, Shigeharu Hosono, Han-Suk Kim, and Edgardo Szyld.
PEDIATRICS Volume 143, number 1, January 2019 11
ABBREVIATIONS
CI: confidence intervalCINAHL: Cumulative Index to
Nursing and Allied Health Literature
CoSTR: consensus on the science with treatment recommendation
Fio2: fraction of inspired oxygen
GRADE: Grading of Recommendations Assessment, Development and Evaluation
HIE: hypoxic-ischemic encephalopathy
ILCOR: International Liaison Committee on Resuscitation
IQR: interquartile rangeNDI: neurodevelopmental
impairmentNLS: Neonatal Life SupportNNT: number needed to treatPRISMA: Preferred Reporting
Items for Systematic Reviews and Meta-Analyses
qRCT: quasi randomized controlled trial
RCT: randomized controlled trial
RoB: risk of biasRR: risk ratio
by guest on January 21, 2021www.aappublications.org/newsDownloaded from

REFERENCES
1. Niermeyer S, Kattwinkel J, Van Reempts P, et al. International guidelines for neonatal resuscitation: an excerpt from the guidelines 2000 for cardiopulmonary resuscitation and emergency cardiovascular care: international consensus on science. Contributors and reviewers for the neonatal resuscitation guidelines. Pediatrics. 2000;106(3). Available at: www. pediatrics. org/ cgi/ content/ full/ 106/ 3/ e29
2. Vento M, Sastre J, Asensi MA, Viña J. Room-air resuscitation causes less damage to heart and kidney than 100% oxygen. Am J Respir Crit Care Med. 2005;172(11):1393–1398
3. Saugstad OD, Rootwelt T, Aalen O. Resuscitation of asphyxiated newborn infants with room air or oxygen: an international controlled trial: the Resair 2 study. Pediatrics. 1998;102(1). Available at: www. pediatrics. org/ cgi/ content/ full/ 102/ 1/ e1
4. Saugstad OD, Ramji S, Irani SF, et al. Resuscitation of newborn infants with 21% or 100% oxygen: follow-up at 18 to 24 months. Pediatrics. 2003;112(2):296–300
5. Tan A, Schulze A, O’Donnell CP, Davis PG. Air versus oxygen for
resuscitation of infants at birth. Cochrane Database Syst Rev. 2005; (2):CD002273
6. Perlman JM, Wyllie J, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Part 11: neonatal resuscitation: 2010 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2010;122(16 suppl 2):S516–S538
7. Perlman JM, Wyllie J, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Part 7: neonatal resuscitation: 2015 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2015;132(16suppl 1):S204–S241
8. Higgins JPT, Altman DG, Gøtzsche PC, et al; Cochrane Bias Methods Group; Cochrane Statistical Methods Group. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928
9. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred Reporting Items for Systematic Reviews and
Meta-Analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097
10. Strand M, Simon W, Wyllie J, Wyckoff M, Weiner G. Consensus outcome rating for international neonatal resuscitation guidelines. In: Pediatric Academic Societies Meeting; May 5–8, 2018; Toronto, Canada
11. Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress. A clinical and electroencephalographic study. Arch Neurol. 1976;33(10):696–705
12. Younge N, Goldstein RF, Bann CM, et al; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Survival and neurodevelopmental outcomes among periviable infants. N Engl J Med. 2017;376(7):617–628
13. Bayley N. Bayley Scales of Infant and Toddler Development. 3rd ed. San Antonio, TX: Harcourt Assessment; 2006
14. Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919
15. Schünemann HB, Guyatt G, Oxman A; The GRADE Working Group. GRADE
WELSFORD et al12
Dr Welsford prepared the protocol, screened studies, abstracted data, completed risk of bias and Grading of Recommendations Assessment, Development and Evaluation (GRADE) evaluations, completed the analysis, and prepared the first draft of the manuscript; Dr Nishiyama reviewed the protocol, screened studies, abstracted data, completed risk of bias and GRADE evaluations, reviewed the analysis, and prepared the first draft of the manuscript; Dr Shortt reviewed the protocol, screened studies, abstracted data, prepared the tables, and was involved in writing and editing the manuscript; Drs Isayama and Dawson reviewed the protocol, completed risk of bias and GRADE evaluations, reviewed the analysis, and were involved in writing and editing the manuscript; Drs Weiner, Roehr, Wyckoff, and Rabi were involved in reviewing the protocol, reviewing the analysis, and writing and editing the manuscript; and all authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
This trial has been registered with PROSPERO (https:// www. crd. york. ac. uk/ PROSPERO) (identifier CRD42018084902).
DOI: https:// doi. org/ 10. 1542/ peds. 2018- 1825
Accepted for publication Sep 11, 2018
Address correspondence to Michelle Welsford, BSc, MD, FRCPC, Division of Emergency Medicine, McMaster University, Centre for Paramedic Education and Research, Hamilton General Hospital, McMaster Clinic, 237 Barton St E., Room 253, Hamilton, ON L8L 2X2, Canada. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2019 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Funded by the American Heart Association on behalf of the International Liaison Committee on Resuscitation. The funder was involved in the International Liaison Committee on Resuscitation process but had no role in this systematic review study design, data collection and analysis, or preparation of the article.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
COMPANION PAPER: Companions to this article can be found online at www. pediatrics. org/ cgi/ doi/ 10. 1542/ peds. 2018- 1828 and www. pediatrics. org/ cgi/ doi/ 10. 1542/ peds. 2018- 3365.
by guest on January 21, 2021www.aappublications.org/newsDownloaded from

handbook. 2013. Available at: www. guidelinedevelopm ent. org/ handbook. Accessed May 27, 2018
16. Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560
17. Higgins J, Green S, eds. Cochrane handbook for systematic reviews of interventions version 5.1.0. In: The Cochrane Collaboration. 2011. Available at: www. handbook. cochrane. org. Accessed May 27, 2018
18. Ramji S, Ahuja S, Thirupuram S, Rootwelt T, Rooth G, Saugstad OD. Resuscitation of asphyxic newborn infants with room air or 100% oxygen. Pediatr Res. 1993;34(6):809–812
19. Vento M, Asensi M, Sastre J, García-Sala F, Viña J. Six years of experience with the use of room air for the resuscitation of asphyxiated newly born term infants. Biol Neonate. 2001;79(3–4):261–267
20. Vento M, Asensi M, Sastre J, Lloret A, García-Sala F, Viña J. Oxidative stress in asphyxiated term infants resuscitated with 100% oxygen [published correction appears in J Pediatr. 2003;142(6):616]. J Pediatr. 2003;142(3):240–246
21. Bajaj N, Udani RH, Nanavati RN. Room air vs. 100 per cent oxygen for neonatal resuscitation: a controlled clinical trial. J Trop Pediatr. 2005;51(4):206–211
22. Toma AI, Nanea M, Scheiner M, Mitu R, Petrescu I, Matu E. Efectele Gazului Folosit Pentru Reanimarea Nou-Nascutului Asupra Hemodinamicii Post-Resuscitare [Effects of the gas used in the resuscitation of the newborn in the post-resuscitation haemodynamics]. Asfixia Perinat. 2006;33–34. Available at: http:// rjp. com. ro/ articles/ 2007. 1/ Pedia_ Nr- 1_ 2007_ Art- 12. pdf. Accessed November 15, 2018
23. Toma A, Sarbu A, Popescu O, Mitu A, Dobrescu M. Room air versus oxygen in the resuscitation of term infants. In: E-PAS 2006 Pediatric Academic Societies Annual Meeting; April 29–May 2, 2006; San Francisco, CA
24. Toma A, Albu D, Mitu R, Matu E. Follow up for 12-15 months of children resuscitated at delivery with 21% or 100% oxygen. In: PAS 2007; May 5–8, 2007; Toronto, Canada
25. Toma A, Albu D, Dambenau I, et al. 21% versus 100% oxygen in the resuscitation of term infants. In: Annual Meeting of the European Society for Paediatric Research;
October 6–8, 2007; Prague, Czech Republic
26. Ramji S, Rasaily R, Mishra PK, et al. Resuscitation of asphyxiated newborns with room air or 100% oxygen at birth: a multicentric clinical trial. Indian Pediatr. 2003;40(6):510–517
27. Saugstad OD, Ramji S, Soll RF, Vento M. Resuscitation of newborn infants with 21% or 100% oxygen: an updated systematic review and meta-analysis. Neonatology. 2008;94(3):176–182
28. Rabi Y, Rabi D, Yee W. Room air resuscitation of the depressed newborn: a systematic review and meta-analysis. Resuscitation. 2007;72(3):353–363
29. Saugstad OD, Ramji S, Vento M. Resuscitation of depressed newborn infants with ambient air or pure oxygen: a meta-analysis. Biol Neonate. 2005;87(1):27–34
30. Davis PG, Tan A, O’Donnell CPF, Schulze A. Resuscitation of newborn infants with 100% oxygen or air: a systematic review and meta-analysis. Lancet. 2004;364(9442):1329–1333
31. Wyatt JS, Gluckman PD, Liu PY, et al; CoolCap Study Group. Determinants of outcomes after head cooling for neonatal encephalopathy. Pediatrics. 2007;119(5):912–921
PEDIATRICS Volume 143, number 1, January 2019 13 by guest on January 21, 2021www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2018-1825 originally published online December 21, 2018; 2019;143;Pediatrics
Support Task Forceon behalf of the International Liaison Committee on Resuscitation Neonatal Life
Dawson, Gary Weiner, Charles Christoph Roehr, Myra H. Wyckoff, Yacov Rabi and Michelle Welsford, Chika Nishiyama, Colleen Shortt, Tetsuya Isayama, Jennifer Anne
With Meta-analysisRoom Air for Initiating Term Newborn Resuscitation: A Systematic Review
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/143/1/e20181825including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/143/1/e20181825#BIBLThis article cites 23 articles, 7 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/neonatology_subNeonatologysubhttp://www.aappublications.org/cgi/collection/fetus:newborn_infant_Fetus/Newborn Infantine_subhttp://www.aappublications.org/cgi/collection/evidence-based_medicEvidence-Based Medicinefollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on January 21, 2021www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2018-1825 originally published online December 21, 2018; 2019;143;Pediatrics
Support Task Forceon behalf of the International Liaison Committee on Resuscitation Neonatal Life
Dawson, Gary Weiner, Charles Christoph Roehr, Myra H. Wyckoff, Yacov Rabi and Michelle Welsford, Chika Nishiyama, Colleen Shortt, Tetsuya Isayama, Jennifer Anne
With Meta-analysisRoom Air for Initiating Term Newborn Resuscitation: A Systematic Review
http://pediatrics.aappublications.org/content/143/1/e20181825located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2018/12/17/peds.2018-1825.DCSupplementalData Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2019has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on January 21, 2021www.aappublications.org/newsDownloaded from