Embed Size (px)
Citation preview

Division Of Cancer Epidemiology And GeneticsRadiation Epidemiology Branch
Non Malignant Thyroid DiseasesNon-Malignant Thyroid Diseases Following a Wide Range of
Radiation Exposures
Elaine RonAlina BrennerAlina Brenner
Late Health Effects of Ionizing Radiation:Late Health Effects of Ionizing Radiation: Bridging the Experimental and Epidemiologic Divide
May 4-6, 2009

OutlineOutline
• A little thyroid gland biologyA little thyroid gland biology• Radiation effects
– Nodules– Hyperthyroidism
H th idi– Hypothyroidism– Autoimmune thyroiditis or elevated levels of
antibodiesantibodies
• Conclusions

Thyroid GlandThyroid Gland
• Makes and storesMakes and stores thyroid hormones
• Thyroid hormonesThyroid hormones instrumental in regulating growth, g g g ,metabolism, reproduction, tissue f ifunction

Thyroid Gland20
30
ve ri
sk Thyroid Gland0 1 2 3 4 5
0
10
Dose (Gy)
Rel
ativ
Age at exposure: < 15: >= 15:
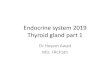
• Radiation effects first reported in 1920s• 1950s clinical observations of association
between external radiation and thyroid cancer
• One of the most radiosensitive organs• Strong linear radiation dose response for g p
cancer especially after childhood exposure• Limited information on radiation and otherLimited information on radiation and other
thyroid diseases

Th id DiThyroid Diseases
Structural Functional• Tumors
– Malignant• Hyperthyroidism• Hypothyroidism
– Benign
• NodulesHyperplastic*
• Autoimmune thyroiditis• Elevated levels of – Hyperplastic
– Cyst
• Thyroid enlargement
antibodies
* Includes nodular goiter

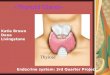
Thyroid Nodule Diagnosis in T itiTransition
• Cancer is a very smallCancer is a very small proportion of nodules
• In past, follicular adenomas defined as benign tumors and most other nodules not considered neoplasticconsidered neoplastic
• Recently, definition of benign nodules reconsidered based on clonal origin
• Difficult to make differential di i t di
Eszlinger et al. JCEM, 2008diagnosis, so many studies combine all benign nodules

Data Sources• Medical
– Children treated with radiation for– Children treated with radiation for benign diseases
– Children and adults treated with radiation for cancer
• Environmental– Chernobyl– Nevada and Kazakhstan test sites
Hanford and Mayak nuclear weapons– Hanford and Mayak nuclear weapons facilities
– Marshall Islanders
• Atomic bomb survivors (AHS)

Thyroid Nodules

Lower Risks for Follicular Adenoma Versus Thyroid Cancer
Ti C iti P ti t Uk i NCI Ch b l
Tumor ERRG
Tinea Capitis PatientsIsrael
Tumor ERRG
Ukraine-NCI Chernobyl Screening Study
Tumor type Cases ERRGy
(95% CI)
Malignant 159 20(12 32)
Tumor type Cases ERRGy
(95% CI)
Malignant 45 5.25(1 7 27)a g a t 59 (12,32)
Follicular adenoma* 42 8
(7,10)
a g a t 5 (1.7, 27)Follicular adenoma* 23 2.07
(0.3, 10)( )
Ratio: malignant/benign = 2.5
( )
Ratio: malignant/benign = 2.5
*b d th l i f t ti
Sadetzki et al. JECM, 2006Ron et al. Rad Res, 1989
Tronko et al. JNCI, 2006Zablotska et al. AJE, 2008
*based on pathology review of tumor tissue

But, for total nodules less clear
Michael Reese Hospital C h t St d
Atomic Bomb
Tumor type Cases ERRGy
(95% CI)
Cohort StudyTumor type Cases EORSv
(95% CI)
Survivors (AHS)
type (95% CI)
Malignant 309 3.0(0.1, 4.0)
type (95% CI)
Malignant 70 1.95(0.67, 4.9)
Benign nodules* 549 8.0
(0.3, 3.7)Benign nodules* 156 1.53
(0.76, 2.7)
Ratio: malignant/benign =0.38
*includes follicular adenoma and other nodules
Ratio: malignant/benign =1.28
Imaizumi et al. JAMA, 2006
*includes follicular adenoma and other nodules
Schneider et al. JECM, 1993

Nodules Associated with High-gDose Radiotherapy for Childhood
Hodgkin DiseaseHodgkin Disease• Thyroid doses ten’s of Gy (Mantle
field)field)• 20-40% risk of developing thyroid
nodulesMantle
• Based on small numbers– Risk of radiation-related benign nodule
slightl lo er than for malignant
field
slightly lower than for malignant– Age, gender and follow-up patterns
similar to cancer patterns
Von der Weid. Support Care Cancer, 2008Acharya et al. Cancer, 2003

Nodules Associated with High-Dose Radiotherapy for Childhood
Hodgkin Diseaseodg sease• Study population
– 146 patients who developed nodules among 1,791 members of CCSS
– 79% had radiotherapy79% had radiotherapy – median thyroid dose, 35 Gy; maximum 55 Gy
• Relative Risks – compared to siblings = 27 (P <0.001) – at >25 Gy = 2.9 (1.4, 6.9)
Sklar et al. JECM, 2000

Thyroid Nodules and Radioactive yIodine Exposure from Fallout
N d S i l ti kNevada Weapons Test Site
• 2500 study subjects
SemipalatinskWeapons Test Site
• 3000 study subjects• Mean dose 120 mGy• Benign tumors (n=15)
y j
• Mean dose: 40 mGy
external; 300 mGy internalERRGy not estimated, Ptrend
<0.001 • Total nodules (n=54)
; y• Total nodules (n=916)
increased with dose, Ptrend• Total nodules (n=54)ERRGy = 4.65; (CI 1.1, 12.3)
<0.001• EORGy = 0.74 (CI 0.22, 1.24)
Lyon et al. Epidemiol, 2006 Land et al. Radiat Res, 2008

Benign Nodules and En ironmental I 131Environmental I-131
• Marshall Islands fallout– High doses on Rongelap, Ailinginae and Utrik
• Clear increase of nodules Low doses on other islands– Low doses on other islands
• Results inconsistent and not well quantified• Inverse relationship - nodules and distance from test site
(Hamilton et al 1987)(Hamilton et al 1987)• Positive relationship - nodules and distance from test site
(Takahashi et al 2001)
• Ozyorsk (Mushkacheva et al 2006)Ozyorsk (Mushkacheva et al 2006)
– Nodules (n=165); RR= 1.4 (CI 1.0, 1.9)• Hanford Nuclear Site (Davis et al 2004)Hanford Nuclear Site (Davis et al 2004)
– Nodules (n=249); ERRGy= -0.008 (CI <-0.02, 0.04)

Functional Thyroid T3Functional Thyroid Diseases
• Excess or deficit of blood levels of thyroid hormones (T4 T3 TSH) alonethyroid hormones (T4, T3, TSH) alone or in combinationC i i ti ith th id• Can occur in association with thyroid nodules
T4

Hyperthyroidism FollowingHyperthyroidism Following High-Dose Radiotherapy
• Overactive thyroid– Thyroid produces too much thyroxine (T4)– Pituitary produces too little TSH
• Relatively rare• Reported infrequently following
radiotherapy for Hodgkin disease in adults, adolescents and children
• Most studies small and do not have individual doses

Hyperthyroidismyp yAtomic Bomb Survivors CCSS
P b bilit f d l i(AHS) Probability of developing hyperthyroidism by dose
4091 i
1791 survivors 2808 siblingsP =0 1010-
4091 survivors51 cases
1791 survivors, 2808 siblings82 cases; 13 control casesRR = 8.0 (4.6, 15)
ds R
atio
P =0.108-6-4-2-
Od
0-
Sklar et al. JCEM, 2000Imaizumi et al. JAMA, 2006
Thyroid Dose, Sv

Hypothyroidismyp y• Underactive thyroid
– Thyroid doesn't produce enough thyroxine (T4) – Pituitary produces too much TSH in an attempt to
compensatep
• Most common thyroid disease– Overt (low T4, normal TSH) - requires treatmentOvert (low T4, normal TSH) requires treatment– Subclinical (high TSH, normal T4) - sometimes treated
• A known late effect of high-dose exposureg p• Effects after low or moderate doses less clear
– Lack of individual doses– Lack of individual doses– Study design

Hypothyroidism following High-Dose R di th i Childh dRadiotherapy in Childhood
• 1,791 members of CCSS; 2808 ;siblings
• 456 CCSS cases;• 456 CCSS cases; 39 control cases
• RR = 17.1 (12, 24), p<0.0001
Probability of developing
Sklar et al. JCEM, 2000
Probability of developing hypothyroidism by thyroid dose

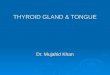
Mild Hypothyroidism and I-131 Dose from Chernobyl Accident
Ukraine-NCI Thyroid
3 0
3.5Category specific ORsFitted ORs based on linear EOR mo
EORGy = 0.10 (95%CI: 0.03; 0.21)
• Category specific ORFitted ORs based on linear model
Ukraine-NCI Thyroid Screening Study
• 11,853 people <18 yrs at accident
2.0
2.5
3.0
OR
__ Fitted ORs based on linear model
OR
• Individual thyroid measurements;– mean thyroid dose = 0.79 Gy; range, 0-
40.7
1.0
1.5
2.0O O • Clinical exam including lab tests• 719 cases with hypothyroidism
– TSH > 4 mIU/L
0.50.0 1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0 9.0 10.0 11.0
Thyroid dose, GyThyroid Dose
– TSH > 4 mIU/L
• Significant relation between prevalence of hypothyroidism and 131I dose from environmental
Ostroumova et al. EHP, in press
I dose from environmental exposure
See Poster by M. Hatch

HypothyroidismHypothyroidismDefinite Effect Possible Effect
• Irradiated cancer patients
• Chernobyl residents• Nevada Test Site
• I-131 treated hyperthyroid
Nevada Test Site• Atomic bomb
survivors (AHS)patients
• Marshall Islanders
survivors (AHS)
No EffectH f d• Hanford

Autoimmune Thyroiditis (AIT)Autoimmune Thyroiditis (AIT)• Relatively common
E k l ti hi ith I 131 lt i• Even a weak relationship with I-131 may result in significant morbidity – hormone replacement to treat thyroid failure or preventhormone replacement to treat thyroid failure or prevent
cardiovascular complications– could increase risk of thyroid cancer
• Various clinical manifestations and degree of thyroid• Various clinical manifestations and degree of thyroid dysfunction
• No internationally accepted classificationNo internationally accepted classification– High thyroid antibodies, ATPO ≥ 250 U/ml– High thyrotropin, TSH ≥ 10.0 mIU/L– Ultrasound, heterogeneous and hypoechoic

Prevalence of AIT and I-131 DoseUkraine-NCI Screening Study
Thyroid dose GyAIT Thyroid dose, Gy<0.14 0.14- 0.34- 0.66- 0.96- 1.5- 3+
Cases 65 50 41 14 10 15 9Cases 65 50 41 14 10 15 9
Non-cases 3,938 2,776 1,906 812 727 998 530
OR*95% CI
1.0 1.10.8,1.7
1.30.8,1.9
1.20.7,2.2
1.10.6,2.0
0.70.4,1.5
0.90.4,1.9
Ptrend = 0.25
*Adjusted for family history of thyroid disease, smoking, thyroid volume, presence of nodules, serum Tg, sex and age
Tronko et al. JCEM, 2006

Anti-Thyroid AntibodiesStudy (reference) Subjects End points ResultsUtah, Nevada, Arizona
Kerber et al, 1993Lyon et al, 2005
2,4732,497
AMA, ATG, TSHAMA, ATG, TSH
Null Positive
A-bomb survivors (AHS)A-bomb survivors (AHS) Nagataki et al, 1994Imaizumi et al, 2006
2,5874,091
AMA, ATG, TSHATPO, ATG, TSH
PositiveNull
Marshall IslandsTakashi et al, 1999* 4,766 AMA, ATG, TSH Null
HanfordHanfordDavis et al, 2004 3,440 AMA or ATPO, Null
Western PomeraniaV lt k t l 2005* 4,299 ATPO, US PositiveVoltzke et al, 2005* , ,
*No individual doses

Prevalence of ATPO and I-131 DoseUkraine-NCI Screening Study
ATPO iti l l t dATPO positively related to dose
D i t t2.02.12.22.3
OR=dose0.08
OR=(1+0.68*dose*e-0.60*dose)
– Dose response consistent with linear-exponential or power model
1 11.21.31.41.51.61.71.81.9
OR
, 95%
CI
– Dose response not driven solely by people with high ATPO levels
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.00.70.80.91.01.1
Thyroid dose, Gy
– ATPO dose response not due to other thyroid disordersdisorders
Tronko et al. JCEM, 2006

Mechanisms for Radiation-InducedMechanisms for Radiation-Induced Thyroid Nodules
• Thyroid cancer – Papillary: chromosomal rearrangementsp y g– Follicular: point mutations
• Benign Nodulesg– Mechanism unknown– Speculation: nodules often have a p
follicular component, so possibly point mutations involved

Mechanisms for Radiation-InducedMechanisms for Radiation-Induced Thyroid Dysfunction
• Direct thyroid cell injury or death• Prevention of cell division• Immune-mediated damageImmune mediated damage• Inflammatory reaction• Damage to small thyroid vessels and• Damage to small thyroid vessels and
gland capsule

ConclusionsConclusions
Si ifi t d fSignificant dose-response for benign nodules – Dose-response appears to be linear– May be somewhat weaker than for
li t tmalignant tumors– Age and latency patterns similar

Conclusions• Data on hyperthyroidism sparse, but
suggestion of an elevated risk in a few high-dose radiotherapy studieshigh-dose radiotherapy studies
• Overt hypothyroidism observed after high-dose radiotherapy; dose-response g py; prelation
• Subclinical hypothyroidism, autoimmune th roiditis and/or ele ated ATPO mathyroiditis and/or elevated ATPO may occur at lower doses, but– Results are inconsistent– Shape of the dose response is unclear – Some of the effects may be transient
• Data not sufficient to describe effect ata ot su c e t to desc be e ectmodification for any outcome