Embed Size (px)
Citation preview

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
1
Romanian Journal
of Oral Rehabilitation
Vol. 2, No. 3, July 2010
Editor in Chief
Norina Consuela Forna, Iaşi, România
Vice-Editor
Viorel Păun, Bucharest, România
Senior Associate Editors
Pierre Lafforgue, Paris, France
Sammi Sandhaus, Lausanne, Switzerland
Robert Sader, Germania
Zhimon Jacobson, Boston, USA
Editorial Board
Marcel Agop, Iaşi, România
Corneliu Amariei, Constanţa, România
Vasile Astărăstoae, Iaşi, România
Mihai Augustin, Bucharest, România
Grigore Băciuţ, Cluj-Napoca, România
Constantin Bălăceanu-Stolnici, Bucharest,
România
Marc Bolla, Nice, France
Dorin Bratu, Timişoara, România
Alexandru Bucur, Bucharest, România
Eugen Carasevici, Iaşi, România
Radu Septimiu Câmpean, Cluj-Napoca,
România
Virgil Cârligeriu, Timişoara, România
Costin Cernescu, Bucharest, România
Yves Comissionat, Paris, France
Marysette Folliguet, Paris, France
Cristina Glavce, Bucharest, România
Emilian Hutu, Bucharest, România
Constantin Ionescu-Tîrgoviste, Bucharest,
România
Michel Jourde, Paris, France
Veronica Mercuţ, Craiova, România
Patrick Missika, Paris, France
Ostin Costin Mungiu, Iaşi, România
Ady Palti, Kraichtal, Germany
Mihaela Păuna, Bucharest, România
Phillipe Pirnay, Paris, France
Constantin Popa, Bucharest, România
Sorin Popşor, Tg. Mureş, România
Dorin Ruse, Vancouver, Canada
Valeriu Rusu, Iaşi, România
Adrian Streinu-Cercel, Bucharest, România
Dragoş Stanciu, Bucharest, România
Mircea Suciu, Tg. Mureş, România
Alin Şerbănescu, Cluj-Napoca, România
General Secretary
Magda Ecaterina Antohe, Iaşi, România
Legislation Committee
Delia Barbu, Bucharest, România
Technical Committee
Andrei Istrate, Iaşi, România
Volum realizat în cadrul Casei Editoriale DEMIURG

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
2
CUPRINS
FOREWARD (Prof. Univ. Dr. Norina Forna)
3
POSTTHERAPEUTIC FEEDBACK EVALUATION IN ORAL REHABILITATION
Sami Sandhaus, Norina Forna
4
THE EPIDEMIOLOGY OF THE SAGITTAL DISORDERS AT THE LEVEL OF THE SKELETAL
BASIS CORRELATED WITH THEIR VERTICAL DISORDERS ON A GROUP OF PATIENTS OF
BUCHAREST
R. Stanciu, Anca Temelcea, Ileana Simion, Valentina Dorobăţ
7
ANATOMIC AND ANTHROPOLOGICAL CONSIDERATIONS OF NEUROCRANIUM
Anca Indrei, Gr. D. Mihalache, Gr. Mihalache
11
CHILD PHYSICAL ABUSE FROM THE PERSPECTIVE OF PEDIATRIC DENTISTRY
Savin Carmen, Bălan Adriana, Petcu Ana, Maxim A., Earar K., Bălan Gh.
17
THE MECHANICAL BEHAVIOR OF THE AESTHETIC MATERIALS IN VENEERED PROSTHETIC
CONSTRUCTIONS
Diana Diaconu, Monica Tatarciuc, Anca Viţalariu, St. Panaite
21
THE ROLE AND IMPORTANCE OF THE CARIES DETECTORS DYES IN EARLY DIAGNOSIS
AND TREATMENT OF DENTAL CARIES
Pancu Galina, Stoleriu Simona, Andrian Sorin, Gheorghe Angela, Topoliceanu Claudiu, Pancu Ion,
Lăcătuşu Ştefan
26
PERIODONTAL CHANGES IN CONJUNCT PROSTHESES
Valeria Pendefunda, Arina Ciocan-Pendefunda, Carmen Pîrlia
29
RADIODENSITOMETRIC STUDY REGARDING CONSERVATIVE ENDODONTIC THERAPY IN
PERIAPICAL LESIONS
Sãlceanu Mihaela, Donciu Cristi, Maria Vataman, Radu Vataman
35
PRE-EXTRACTIONAL VALUE OF THE INTERNATIONAL NORMALIZED RATIO IN
IDENTIFICATION OF THE HEMORRHAGIC AND THROMBOEMBOLIC RISK IN PATIENTS
UNDERGOING ORAL ANTICOAGULANT TREATMENT
Oleg Zănoagă, Valentin Topalo, Ion Corcimaru, Dumitru Sîrbu, Ilie Suharschi
40
ASSESSMENT OF ORO-DENTAL HEALTH STATUS USING THE CAO AND EGOHID INDEXES AT
THE YOUNG PEOPLE
Ioan Dănilă, Iulia Saveanu, Carina Balcos
50
THE DAY OF PROPHYLAXY, JUNE, 9, 2010
55

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
3
FOREWORD
The Day of Moldavian Prophylaxy in Dental
Medicine is already a traditional manifestation. This
year the topic is “Evaluation of the Oral Status at Rural
and Monastic Population and Rehabilitation
Possiiities”, which extends the population health
assessment to the villages in the county of Iasi.
The Symposium dedicated to oral pathology
prevention methods reunites both conferences held by
representative personalities in the field and
representative companies which promote prophylaxy products. An important
aspect is the Prophylaxy Caravan organizing special places for the oral health
evaluation as well of information , promotion, and distribution of free samples
of prophylaxy products in the county of Iasi and in the monastic community.
The assessment results is particularly important for the future dissemination of
prophylaxy methods and identification of incipient stages in oral pathology.
Prof. Univ. Dr Norina Forna
The President of Romanian Society ofOral Rehabilitation
Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
4
POSTTHERAPEUTIC FEEDBACK EVALUATION IN ORAL
REHABILITATION Sami Sandhaus
1, Norina Forna
2
1. Forum Odontologicum International, Lausanne, SWITZERLAND
2. ―Gr. T. Popa‖ University of Medicine and Pharmacy Iasi
Faculty of Dental Medicine
Clinic and Therapy of Extended Partial Edentation
Abstract:
Objectives: The goal of this study was to assess the subjective post-therapeutic feedback for a group of patients
in order to evaluate the possibility of including in the analysis structure of expert system psycho-behavioral
parameters.
Methods: 135 patients diagnosed with class I and II Kennedy edentation, aged between 40 and 89 years old,
where clinically examined. All patients filled in structured questionnaires focused on psycho-behavioral
parameters.
Results: Prosthetic treatment in oral rehabilitation improves subjective perception of facial aesthetic (66,86%
total and moderate accord), psychological status (71,14% total and moderate accord) and of the social relations
(77,47% total, moderate and low accord) but it is not subjective associated with the improving of general health
(55,49% disagreement).
Conclusions: We can establish statistical support correlation between psycho-behavioral parameters and
therapeutic solutions applied in oral rehabilitation, correlation that can be later quantified and use in the
development of an expert system.
Key words: psycho-behavioral parameters, posttherapeutic feedback, expert systems.
INTRODUCTION
Establishing a treatment plan in oral
rehabilitation involves particularization of
general information concerning clinic,
paraclinical and technological aspects of
removable partial dentures realization and
also a synthesis of clinical, social and
psychological parameters of the patient.
After this complex evaluation, medical
approach of the case leads to a diagnostic
and choosing optimal therapeutic solution,
choice based on practical and theoretical
background of the practitioner. The chosen
solution will guide all the stages of the
treatment, local and generally, so in the
end the stomatognat system to be able to
sustain the prosthetic device in optimal
conditions.
AIMS AND OBJECTIVES
This study aims to analyze subjective
post-therapeutic feedback of patients
diagnosed with Kennedy class I and II
edentation, treated with three therapeutic
solutions: acrylic prosthesis, composite
prosthesis and implanto-prosthetic
rehabilitation. The final objective is to
analyze the possibility to insert psycho-
behavioral parameters in the analysis
structure of an expert system for oral
rehabilitation.
MATERIAL AND METHOD
Our research analyzed the way in
which therapeutic solutions applied to a
group of patients diagnosed with maxillary
and/or mandibullary partial edentation,
Kennedy class I and II modified the
subjective perception of some personal
psycho-behavioral characteristics.
The study has a descriptive design and
includes 135 patients with ages between
40 and 89 years old which has addressed
to Interdentis Medical Center from Pascani
between 01.11.2007 and 01.11.2008. The
patients were divided in three groups
according to the applied treatment
solutions, respectively classic acrylic
solution, composite prosthetic devices and
implanto-prosthetic rehabilitation. We

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
5
estimated the size of the representative
group in order to have statistically
significant results and the examination
protocol was approved by the Clinic and
Therapy of Extended Partial Edentation
Discipline form Dental Faculty of U.M.F.
"Gr. T. Popa", Iasi. The patients included
in our research were investigated and the
results were statistically analyzed.
Clinical examination allowed an
evaluation of the patients’ subjective
perception regarding the way in which
prosthetic treatment modified their facial
esthetic, psychological status, social
relations and general health.
Statistically research has been realized
by creating a database which was
computer analyzed using SPSS 15.00
software that provided an interpretation of
the statistical analysis.
RESULTS
Fig. 1 - Age distribution of patients Fig. 2 - Sex distribution of patients
Fig. 3 - Living area distribution of patients Fig. 4 - Education distribution of patients
We can see that majority of the
patients from study group are aged
between 40 and 59 years old (68,90%) and
sex distribution is relatively equal between
male and female (55,31% female and
respectively 44,69% male). Living area
show that most of the subjects came urban
area, 57,69% have a city address and only
42,09% are coming from rural areas.
Educational level distribution puts the
majority of the patients in the groups of
high school and university degree (46,55%
and respectively 24,95%)
Fig. 5 - Affirmation "Prosthetic treatment improved my facial esthetic"
44,69%
24,21%
20,67%
10,43% 40-50 years
51-60 years
61-70 years
over 71 years
44,69%
55,31%male
female
57,91%
42,09%
urban
rural
13,97%
14,53%
46,55%
24,95%
primary classes
8 classes
highschool
college
3,17% 4,28%
7,45%
36,69%18,25%
30,17%total disagreement
slight disagreement
moderate disagreement
moderate agreement
slight agreement
total agreement
0
500 80457
7,26%20,86%
27,37%22,53%
12,10%
9,87%total disagreement
slight disagreement
moderate disagreement
moderate agreement
slight agreement
total agreement
0
100
200
300
disagreement agreement
298239

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
6
Fig. 6 - Affirmation "Prosthetic treatment improved my general health"
Fig. 7 - Affirmation "Prosthetic treatment improved my psychological status"
Fig. 8 - Affirmation "Prosthetic treatment improved my social relations"
DISCUSSIONS
Without determining directly the
course of the treatment, psycho-behavioral
parameters influence the choice of the
final therapeutic solution, case
management and medium and long term
prognostic for the case.
Subjective post-therapeutic feedback
may represent an orientation element in
pretreatment psycho-behavioral
assessment of the patient and in the
process of choosing the final prosthetic
solution
CONCLUSIONS
1. 85,10% of patients consider that
prosthetic treatment improved their facial
esthetic (66,86% total and moderate
accord).
2. 87,52% of patients consider that
prosthetic treatment improved their
psychological status (71,14% total and
moderate accord).
3. 77,47% of patients consider that
prosthetic treatment improved their social
relations (total, moderate and low accord).
4. Improvement of the general health is not
associated with prosthetic treatment
(55,49% total, moderate and low
disagreement).
5. We can statistically support the
establishment of correlations between
patient's psycho-behavioral parameters and
applied therapeutic solutions, correlations
that can be later used in development of an
expert system for oral rehabilitation.
REFERENCES 1. N. Forna, Burlui V. - Clinical guidelines and principles in the therapy of partial extended edentation -
editura Apollonia, Iași, 2001
2. Collen M.F. - A vision of health care and informatics - American Journal of Medical Informatic
Association, 2008
3. Reichert A., Sadan B.A., Bengtsson S. - Design of an oral health information system based upon a
computer based dental record - Jerusalem, Israel, 1993.
7,26%
45,81%
16,39%
25,33% 5,21%total disagreement
slight disagreement
moderate disagreement
moderate agreement
slight agreement
total agreement
0
200
400
600
disagreement agreement
67
470
3,17% 7,26%
12,10%
29,05%22,91%
25,51%
total disagreement
slight disagreement
moderate disagreement
moderate agreement
slight agreement
total agreement
0
200
400
600
disagreement agreement
121
416

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
7
THE EPIDEMIOLOGY OF THE SAGITTAL DISORDERS AT THE
LEVEL OF THE SKELETAL BASIS CORRELATED WITH THEIR
VERTICAL DISORDERS ON A GROUP OF PATIENTS OF
BUCHAREST R. Stanciu
1, Anca Temelcea
2, Ileana Simion, Valentina Dorobăţ
3
1 The University of Medicine and Pharmacy „Carol Davila‖ Bucharest, Faculty of Dental Medicine,
Orthodontics and Dento-facial Orthopedics Clinic 2 The University of Medicine and Pharmacy „Carol Davila‖ Bucharest, Faculty of Dental Medicine,
Orthodontics and Dento-facial Orthopedics Clinic 3 The University of Medicine and Pharmacy „Gr. T. Popa‖ Iaşi, Faculty of Dental Medicine
Abstract: The development disorders of the maxillary and mandibular skeletal basis in a sagittal and vertical
plan correlate and create a clinical image with an impressive variability. Even if the proportions on each
development model are less important, their association determines an important treatment necessity.
Key words: class II/2 malocclusion, hyperdivergent development, hypodivergence development
PURPOSE: determining the prevalence of
the epidemiology for Class II/2
malocclusion in a survey.
OBJECTIVES:
- establishing the prevalence of the
modifications occured on the basis in
Class II/2 malocclusion;
- studying the reported phenomenon in
relation to the age and sex group;
- introducing the early therapeutic
measures for the population.
WORK METHOD:
The research is based on the data
collected from a group of 268 patients,
aged between 4 and 16 years, 126 boys
and 142 girls.
The data were registered in the
diagnosis report sheet and in that of the
epidemiological examination, where the
main purposes were:
- the level of the general psycho-somatic
development;
- the clinical facial examination, the
position of the lower cranial floor of the
face compared to the middle one, the facial
typology, normal, hypo-/hyper-divergent,
thus realizing a three-dimensional
analysis;
- the dimensional equilibrium between the
anterior and the posterior floors of the
face;
- thus obtaining enough information in
order to establish the equilibrium existence
or the lack of equilibrium at the level of
the maxilar basis and implicitly the
necessity to continue the investigations in
order to assess the need for an orthodontic
treatment.
The dental analysis focused on the
occlusion of the three dimensions of the
space, a fact which allowed the group’s
division into two, with dental and
maxillary abnormalities, classified in the
three Angle classes (Class I, Class II/1,
Class II/2, Class III) and dental and
maxillary abnormalities.
The gathering of the dental and facial
data allowed us to perform an overall
assessment of the health status of the
population and to establish the needs for
treatment.
The epidemiological sheets were
stored in the information database; the
statistic processing was performed
according to the SPSS 16.0 system.
Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
8
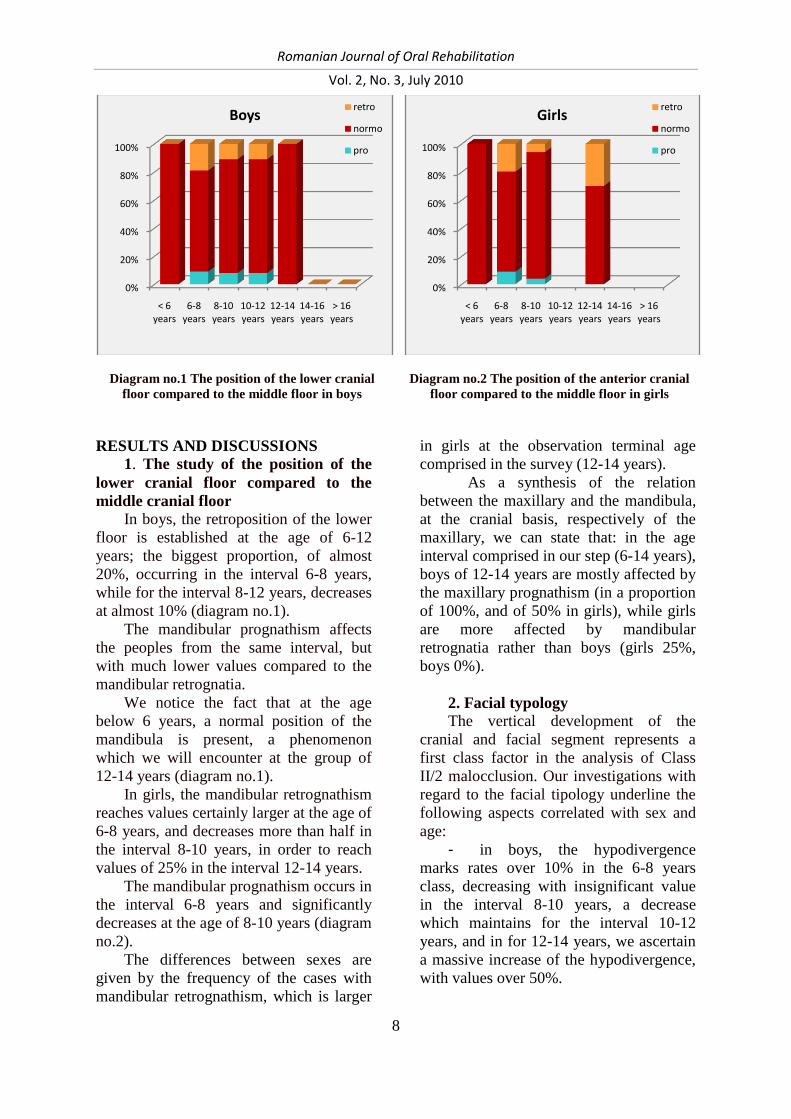
Diagram no.1 The position of the lower cranial
floor compared to the middle floor in boys
Diagram no.2 The position of the anterior cranial
floor compared to the middle floor in girls
RESULTS AND DISCUSSIONS
1. The study of the position of the
lower cranial floor compared to the
middle cranial floor In boys, the retroposition of the lower
floor is established at the age of 6-12
years; the biggest proportion, of almost
20%, occurring in the interval 6-8 years,
while for the interval 8-12 years, decreases
at almost 10% (diagram no.1).
The mandibular prognathism affects
the peoples from the same interval, but
with much lower values compared to the
mandibular retrognatia.
We notice the fact that at the age
below 6 years, a normal position of the
mandibula is present, a phenomenon
which we will encounter at the group of
12-14 years (diagram no.1).
In girls, the mandibular retrognathism
reaches values certainly larger at the age of
6-8 years, and decreases more than half in
the interval 8-10 years, in order to reach
values of 25% in the interval 12-14 years.
The mandibular prognathism occurs in
the interval 6-8 years and significantly
decreases at the age of 8-10 years (diagram
no.2).
The differences between sexes are
given by the frequency of the cases with
mandibular retrognathism, which is larger
in girls at the observation terminal age
comprised in the survey (12-14 years).
As a synthesis of the relation
between the maxillary and the mandibula,
at the cranial basis, respectively of the
maxillary, we can state that: in the age
interval comprised in our step (6-14 years),
boys of 12-14 years are mostly affected by
the maxillary prognathism (in a proportion
of 100%, and of 50% in girls), while girls
are more affected by mandibular
retrognatia rather than boys (girls 25%,
boys 0%).
2. Facial typology
The vertical development of the
cranial and facial segment represents a
first class factor in the analysis of Class
II/2 malocclusion. Our investigations with
regard to the facial tipology underline the
following aspects correlated with sex and
age:
- in boys, the hypodivergence
marks rates over 10% in the 6-8 years
class, decreasing with insignificant value
in the interval 8-10 years, a decrease
which maintains for the interval 10-12
years, and in for 12-14 years, we ascertain
a massive increase of the hypodivergence,
with values over 50%.
0%
20%
40%
60%
80%
100%
< 6 years
6-8 years
8-10 years
10-12 years
12-14 years
14-16 years
> 16 years
Boysretro
normo
pro
0%
20%
40%
60%
80%
100%
< 6 years
6-8 years
8-10 years
10-12 years
12-14 years
14-16 years
> 16 years
Girlsretro
normo
pro
Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
9
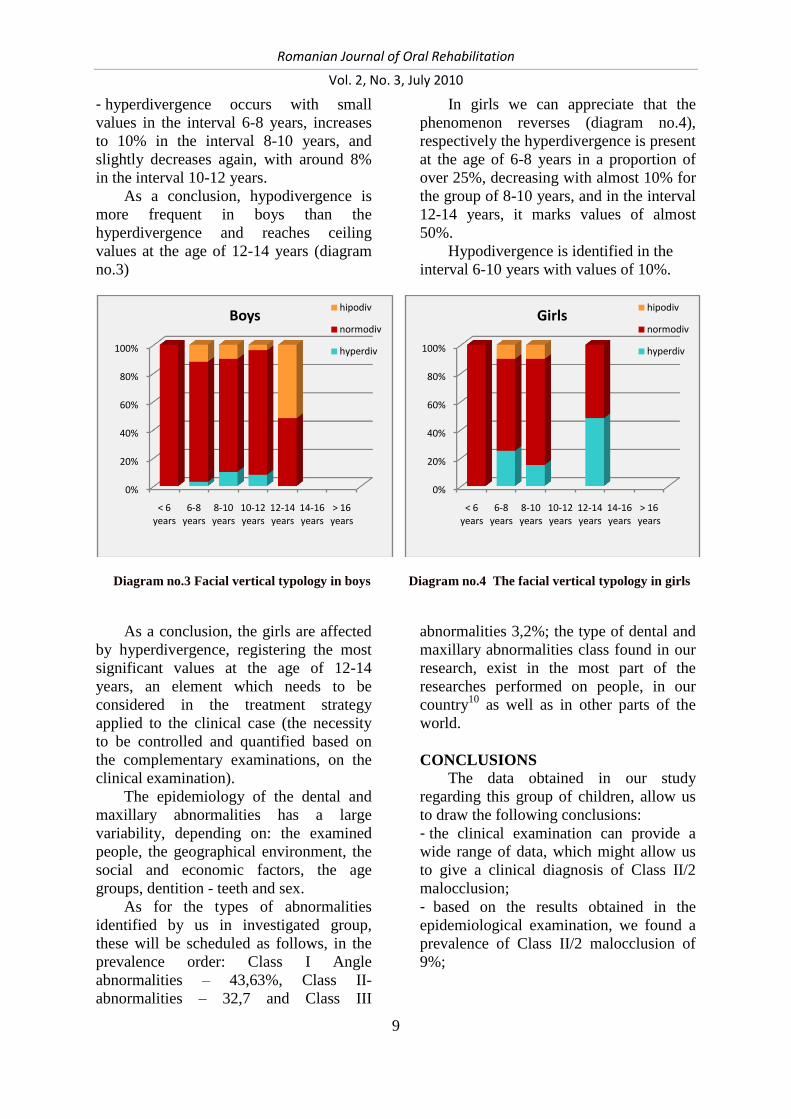
- hyperdivergence occurs with small
values in the interval 6-8 years, increases
to 10% in the interval 8-10 years, and
slightly decreases again, with around 8%
in the interval 10-12 years.
As a conclusion, hypodivergence is
more frequent in boys than the
hyperdivergence and reaches ceiling
values at the age of 12-14 years (diagram
no.3)
In girls we can appreciate that the
phenomenon reverses (diagram no.4),
respectively the hyperdivergence is present
at the age of 6-8 years in a proportion of
over 25%, decreasing with almost 10% for
the group of 8-10 years, and in the interval
12-14 years, it marks values of almost
50%.
Hypodivergence is identified in the
interval 6-10 years with values of 10%.
Diagram no.3 Facial vertical typology in boys
Diagram no.4 The facial vertical typology in girls
As a conclusion, the girls are affected
by hyperdivergence, registering the most
significant values at the age of 12-14
years, an element which needs to be
considered in the treatment strategy
applied to the clinical case (the necessity
to be controlled and quantified based on
the complementary examinations, on the
clinical examination).
The epidemiology of the dental and
maxillary abnormalities has a large
variability, depending on: the examined
people, the geographical environment, the
social and economic factors, the age
groups, dentition - teeth and sex.
As for the types of abnormalities
identified by us in investigated group,
these will be scheduled as follows, in the
prevalence order: Class I Angle
abnormalities – 43,63%, Class II-
abnormalities – 32,7 and Class III
abnormalities 3,2%; the type of dental and
maxillary abnormalities class found in our
research, exist in the most part of the
researches performed on people, in our
country10
as well as in other parts of the
world.
CONCLUSIONS
The data obtained in our study
regarding this group of children, allow us
to draw the following conclusions:
- the clinical examination can provide a
wide range of data, which might allow us
to give a clinical diagnosis of Class II/2
malocclusion;
- based on the results obtained in the
epidemiological examination, we found a
prevalence of Class II/2 malocclusion of
9%;
0%
20%
40%
60%
80%
100%
< 6 years
6-8 years
8-10 years
10-12 years
12-14 years
14-16 years
> 16 years
Boyshipodiv
normodiv
hyperdiv
0%
20%
40%
60%
80%
100%
< 6 years
6-8 years
8-10 years
10-12 years
12-14 years
14-16 years
> 16 years
Girlshipodiv
normodiv
hyperdiv

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
10
- the prevalence of Class II/2 malocclusion
established differences depending on the
sex and age group;
- our research underlines the need for the
trials on people, extended to larger groups
of persons and for a long-term follow-up,
based on the complementary examinations
(trial; models, teleradiographies) of small
groups of subjects, in order to obtain more
clear data;
- the treatment strategies must take into
account the insertion of the early
orthodontic therapy, correlated with sex
and the age group.
REFERENCES 1. DOROBĂŢ, V. şi colab.: Epidemiologia anomaliilor dento-maxilare la vârsta de 7 ani. Rev. Ortod. şi ODF
1(2): 2-7,2000.
2. HEIKINHEIMO, K.: Need of Orthodontic treatment and prevalence of cranio-mandibular dysfunction in
Finnish Children Turku – Finland, 1989.
3. HELM, S.: Malocclusion in Danish Children with adolescent dentition. An epidemiologic study. Am J
Orthod, 54:352-66, 1968.
4. PROFFIT, W.R., FIELDS, H.W. JR, SARVER, D.M.: Contemporary Orthodontics. Mosby, 2007.
5. STANCIU, D., DOROBĂŢ V., BRATU E., ŞERBĂNESCU, A. ŞI COLAB. - Proiect CEEX nr. 87/2006.
6. STANCIU, D., SCÂNTEI-DOROBĂŢ, V.: Ortodonţie. Editura Medicală Bucureşti, 1991.

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
11
ANATOMIC AND ANTHROPOLOGICAL CONSIDERATIONS OF
NEUROCRANIUM Anca Indrei, Gr. D. Mihalache, Gr. Mihalache
―Gr.T.Popa‖ University of Medicine and Pharmacy Iaşi
School of Dental Medicine
Discipline of Anatomy and Embryology Abstract: The neurocranium, the part of the skull enclosing the brain, plays a significant role in the skeleton.
This is the reason for which it has been the subject of many studies, that have not clarified all its anatomic but,
most of all, anthropological aspects. Material and method: Our research is based on the study of 60 skulls from
the collection belonging to ―Ion Iancu‖ Institute of Anatomy and to Iaşi Institute of Anthropology. 30 skulls
dated from the 1st century (15 male skulls and 15 female skulls) and 30 from the 20
th century (also, 15 male
skulls and 15 female skulls). We grouped these skulls by age, resulting thus 12 sub-categories.
We studied the braincase bones of each skull, noticing first of all any potential variations. We also measured the
maximum cranial length and width of each skull, and we determined the cephalic index, and the cranial
capacity. Results: Our study revealed several variations of the neurocranium bones, and the anthropometric
values showed that most of the investigated skulls from the 1st century were dolichocephalic and mesocephalic
in the 20th
century. We should also mention that the skulls from the 20th
century had an increased cranial
capacity than those from the 1st century.
Key words: neurocranium, cephalic index, cranial capacity.
INTRODUCTION
The neurocranium, the part of the
skull enclosing the brain, plays a
significant role in the skeleton. This is the
reason for which it has been the subject of
many studies, that have not clarified all its
anatomic but, most of all, anthropological
aspects.
MATERIAL AND METHOD
Our research is based on the study of
60 skulls from the collection belonging to
―Ion Iancu‖ Institute of Anatomy and to
Iaşi Institute of Anthropology. 30 skulls
dated from the 1st century (15 male skulls
and 15 female skulls) and 30 from the 20th
century (also, 15 male skulls and 15
female skulls). We grouped these skulls by
age (under 30 years age, between 30 and
60 years age and over 60 years age),
resulting thus 12 sub-categories.
We studied the braincase bones of
each skull, noticing first of all any
potential variations (1).
We measured the maximal cranial
length (summit of glabella to furthest
occipital point) and the maximal cranial
breath of each skull (greatest breath, at
right angles to median plane). We
determined the cranial index (breath/
length ratio). After the cranial index, the
skulls may be dolichocephalic (the index
up to 74,9), mesocephalic (the index
between 75 and 79,9) and brachycephalic
(the index over 80).
We measured too, the cranial capacity
using the following formulae:
Males: 0.000337 (L-11) (B-11) (H-11)
+ 406.01cc
Females: 0.000400 (L-11) (B-11) (H-
11) + 206.60 cc
In these formulae L and B are
maximal cranial length and breadth and H
is the auricular height, measured to the
vertex from the external acoustic meatus
(2). All measurements are in millimeters.
RESULTS AND DISCUSSIONS
The bones of the neurocranium
presented numerous variations.
The frontal bone and the parietal bone
were the most constant bones presenting
no major variations from the normal
bones.
The ethmoid bone presented in one
case (skull nr. 17 – figure 1) the presence

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
12
of the accessory nasal concha of Santorini
(3).
The sphenoid bone presented the most
variations (4,5). Three skulls presented
middle clinoid processes. We present in
figure 2 such a case.
We also noted the presence in one
case of the ossified ligament of Civinini
(6). We present in figure 3 the skull 18
with this variation.
The temporal bone presented in one
case (figure 4) the persistence of the suture
between the squamous part and the
mastoid part (7).
A rare case is the presence of a
vermian bone at the level of the occipito-
temporo-parietal suture (8). This case is
presented in figure 5.
Figure 1. The accessory nasal concha of Santorini.
Figure 2. Middle clinoid processes in skull nr. 31.
Figure 3. Ossified ligament of Civinini.

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
13
Figure 4. The persistence of the suture between the squamous part and the mastoid part –
skull 42.
Figure 5. Vermian bone at the level of the occipito-temporo-parietal suture.
The skulls from the first century presented the following dimensions:
The first subcategory – female skulls from the first century (under 30 years old):
Skull Length (mm) Breath (mm) Auricular
height (mm)
Cranial Index Cranial
capacity (cc)
1. 180 148 109 82,2 1129,19
2. 181 137 110 75,6 1054,83
3. 184 136 111 73,9 1071,6
4. 186 138 110 74,1 1086,71
5. 188 139 111 73,9 1112,84
The second subcategory – female skulls from the first century (between 30 and 60 years old):
Skull Length (mm) Breath (mm) Auricular
height (mm)
Cranial Index Cranial
capacity (cc)
6. 185 147 111 79,4 1153,1
7. 186 138 114 74,1 1122,27
8. 184 139 116 75,5 1136,64
9. 187 139 112 74,3 1116,73
10. 189 140 115 74,0 1161,81

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
14
The third subcategory – female skulls from the first century (over 60 years old):
Skull Length (mm) Breath (mm) Auricular
height (mm)
Cranial Index Cranial
capacity (cc)
11. 182 141 112 77,4 1104,69
12. 185 149 115 80,5 1205,49
13. 178 148 114 83,1 1149,21
14. 189 141 113 74,6 1150,71
15. 186 139 111 74,7 1102,61
The fourth subcategory – male skulls from the first century (under 30 years old):
Skull Length (mm) Breath (mm) Auricular
height (mm)
Cranial Index Cranial
capacity (cc)
16. 189 145 115 76,7 1375,38
17. 190 140 113 73,6 1277,46
18. 188 141 114 75,0 1282,92
19. 187 139 115 74,3 1272,88
20. 185 138 116 74,5 1256,34
The fifth subcategory – male skulls from the first century (between 30 and 60 years old):
Skull Length (mm) Breath (mm) Auricular
height (mm)
Cranial Index Cranial
capacity (cc)
21. 191 147 118 76,9 1375,17
22. 194 145 116 74,7 1429,78
23. 188 140 113 74,4 1267,72
24. 189 141 115 74,6 1287,87
25. 186 142 114 76,3 1279,68
The sixth subcategory – male skulls from the first century (over 60 years old):
Skull Length (mm) Breath (mm) Auricular
height (mm)
Cranial Index Cranial
capacity (cc)
26. 188 151 117 80,3 1377,88
27. 182 139 116 76,3 1256,35
28. 186 138 119 74,1 1294,12
29. 185 140 118 75,6 1294,64
30. 189 141 120 74,6 1339,24
The skulls of the 20-th century presented the following results:
The 7-th subcategory – female skulls from the 20-th century (under 30 years old):
Skull Length (mm) Breath (mm) Auricular
height (mm)
Cranial Index Cranial
capacity (cc)
31. 187 148 116 79,1 1219,30
32. 191 147 119 76,9 1404,96
33. 189 143 114 75,6 1206,24
34. 188 146 115 77,6 1200,63
35. 192 146 116 76,0 1232,87

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
15
The 8-th subcategory – female skulls from the 20-th century (between 30 years and 60 years
old):
Skull Length (mm) Breath (mm) Auricular
height (mm)
Cranial Index Cranial
capacity (cc)
36. 188 146 116 77,6 1210,19
37. 193 148 116 76,6 1253,82
38. 197 147 118 74,6 1289,26
39. 195 149 117 76,4 1283,22
40. 199 152 120 76,3 1362,34
The 9-th subcategory – female skulls from the 20-th century (over 60 years old):
Skull Length (mm) Breath (mm) Auricular
height (mm)
Cranial Index Cranial
capacity (cc)
41. 191 150 118 78,5 1277,45
42. 196 151 116 77,0 1294,40
43. 204 152 119 74,5 1382,20
44. 202 154 117 76,2 1473,92
45. 201 149 119 74,1 1339,30
The 10-th subcategory – male skulls from the 20-th century (under 30 years old):
Skull Length (mm) Breath (mm) Auricular
height (mm)
Cranial Index Cranial
capacity (cc)
46. 185 144 118 77,8 1322,20
47. 188 146 120 77,6 1369,69
48. 193 151 121 78,2 1443,04
49. 200 155 122 77,5 1523,77
50. 203 160 121 78,8 1570,35
The 11-th subcategory – male skulls from the 20-th century (between 30 and 60 years old):
Skull Length (mm) Breath (mm) Auricular
height (mm)
Cranial Index Cranial
capacity (cc)
51. 201 148 119 73,6 1446,16
52. 202 143 118 70,7 1404,15
53. 204 154 121 75,4 1529,28
54. 203 155 122 76,3 1541,51
55. 206 156 121 75,7 1556,80
The 12-th subcategory – male skulls from the 20-th century (over 60 years old):
Skull Length (mm) Breath (mm) Auricular
height (mm)
Cranial Index Cranial
capacity (cc)
56. 203 151 122 74,3 1500,02
57. 205 154 121 75,1 1535,10
58. 201 152 122 75,6 1552,60
59. 199 153 119 76,8 1472,78
60. 200 155 120 77,5 1503,63

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
16
CONCLUSIONS
Our study revealed several variations
of the neurocranium bones – the most
variable bone being the sphenoid bone.
The anthropometric values showed
that most of the investigated skulls from
the 1st century were dolichocephalic and
mesocephalic in the 20th
century.
We should also mention that the skulls
from the 20th
century had an increased
cranial capacity than those from the 1st
century.
REFERENCES 1. Rouviere H, Delmas A. Anatomie humaine. Tome 1 - Tete et cou. Paris: Masson, 2002, 39–90.
2. Williams PL, Warwick R. Dyson M, Bannister LH. Gray's Anatomy. 37th
ed. Edinburgh: Churchill
Livingstone, 1989, 371-398.
3. Ashton EH, Moore WJ. Cranial shape in the hominidea - exploratory considerations. J Anat 1980; 131:
744-745.
4. Berry AC. Factors affecting the incidence of non - metrical skeletal variants. J Anat 1975; 120: 519-535.
5. Indrei A, Mihalache GrD. Neurocraniul – elemente de curs. Iaşi: Casa de Editură ―Venus‖, 2002, 25–84.
6. Kinman J. Surgical aspects of the anatomy of the sphenoidal sinuses and the sella turcica. J Anat 1977;
124: 541-553.
7. Solter M, Panjana D. Variations in shape and dimensions of sigmoid groove, venous portion of jugular
foramen, jugular fossa, condylar and mastoid foramina classified by age, sex and body size. Z Anat Entw
Gesch 1973; 140: 319-335.
8. Olivier G. Biometry of the human occipital bone. J Anat 1975; 120: 507-518.

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
17
CHILD PHYSICAL ABUSE FROM THE PERSPECTIVE OF
PEDIATRIC DENTISTRY Savin Carmen
1, Bălan Adriana
1, Petcu Ana
1, Maxim A.
1, Earar K.
2, Bălan Gh.
3
1 Pediatric Dentistry Department, Faculty of Dental Medicine, Iasi „Gr.T. Popa‖ University
of Medicine and Pharmacy 2 Dentist, Iasi „Sara Dent‖ Dental Office
3 Student, Iasi „Gr.T. Popa‖ University of Medicine and Pharmacy
Abstract: Child physical abuse is a complex problem, of great topical interest, a severe social problem, with
direct implications on the dento-somato-facial harmony and on the psycho-mental and intellectual development
of the child.
Aim. To highlight the oro-maxillo-facial signs of physical abuse and the role of the pediatric dentists in
identifying and evaluating this signs of physical abuse.
Material and Method. The study was carried out on a sample of 299 abused subjects (218 boys and 81 girls)
aged between 6-18 y.o. from Iasi rural and urban area. The data were analyzed and statistically processed and
the results were synthesized with the help of a descriptive and correlative study.
Results. The physical abuse has serious consequences in oro-dento-facial area, that consists especially in soft
tissue lesions – 62.11%, dento-periodontal trauma (fractures, luxations, concussions, avulsions) – 19.47%,
mandible fractures – 7.89% facial massif fractures – 7.89% and temporo-mandibular joint lesions - 2.63%.
Conclusion. Pediatric dentist should to be legally qualified and morally entitled to report to report when s/he
suspects any physical abuse against the child.
Key words: child, physical abuse, pediatric dentist.
INTRODUCTION Child physical abuse is a complex
highly topical issue, a serious social
problem that has direct implications on the
dental, somatic and facial harmony and
over the psycho-mental and intellectual
development of the child and the adult he
will become.
Analyzing the data from the
specialized literature regarding the
psychical, mental and behavioral evolution
of the child, from birth to teenage, and the
determining pre-and post-natal
circumstances, it was ascertained that one
of the factors that may disturb variably the
normal development, is child abuse and
neglect [1]. Kempe W. and col. (1962)
introduced in the specialized medical
literature the notion ―syndrome of the
beaten child‖, and Elerstein states that
―child abuse causes more physical and
psychological morbidity than most child
diseases.‖
Health Canada defines child abuse as
any maltreatment enforced by a parent,
guardian, caretaker or any other person
onto a child that results in hitting or
traumatizing emotionally or psychically
the child. Physical abuse is the most
frequent form of abuse and the easiest
form to notice by the dentist, due to the
prevailing location of lesions (over 50%)
[2, 3, 4, 5] on the cephalic extremity, on
the orofacial soft parts, on the facial
massive bone, on the dental and
periodontal units, mandible etc.
Specialized studies show that in Great
Britain, every year at least 1 child out of
1000 (under 4 years old) is a victim of
violence, while in the United States and in
Canada 47 children out of 1000 are
physically abused.
Dentists should be aware that physical
abuse involves in more than half of the
cases (65%) (Becker and col. 1978,
daFonseca and col.1992, Jesse, 1995),
manifestations in the mouth and on the
head (i.e. bleeding of the face skin,
excoriations, dental fractures, dental-
alveolar fractures, lesions of the lip, gum,
mandible fractures) that may provide clues

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
18
as to the time of the abuse, its nature or the
identity of the aggressor.
The aim of this study is to outline the
orofacial manifestations of the physical
abuse of the child and to emphasize the
important part played by the pediatric
dentists in identification and correct
assessment of these signs and in reporting
the various child abuse forms.
MATERIAL AND METHOD
This paper is an integrative part of a
longitudinal study on the medical legal
aspects of oro-facial and dento-periodontal
traumas of the child and the teenager. The
study was conducted on a group of 299
subjects (218 boys, 81 girls), aged between
6 and 18 year old, from the urban and the
rural environment of Iasi county, that were
referred to the Service of Forensic
Medicine in the Polyclinic no.1 of Iasi.
The distribution of subjects per sexes and
environments of origin are shown in fig.1
and fig.2.
Fig. 1 Distribution of subjects per sexes Fig. 2 Distribution of subjects per
and origin environment origin environment
The data (number of traumas, etiology
of the trauma, type of orofacial traumatic
lesion, type of odonto-periodontal lesion
and so on) obtained from all legal medical
certificates were statistically analyzed and
processed and the results were synthesized
by means of a descriptive and correlative
study.
RESULTS AND DISCUSSIONS
It was ascertained an alarming rate of
cases of oro-facial traumas produced via
physical abuse, compared to other cases
(car crashes, rapes) (fig.3), and their
prevalence at the age stage 13 to 18 years
(table 1), which suggests a higher rate of
oro-facial traumatic lesions at this age
stage in comparison to other age stages,
data comparable with those in the
specialized literature [2, 6].
0
50
100
150
200
250 218
81boys
girls
0
20
40
60
80
100
120
140
urban rural
91
127
3645
boys
girls

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
19
Fig. 3 Etiology of orofacial traumas
Age 6-12 years 13-18 years
Etiology Physical abuse Physical abuse
Number of
subjects
15.05% (45 subjects) 84.95% (254 subjects)
Table 1 - Distribution of subjects per age stages
Child abuse has major consequences
in the oro-facial area, which consisted
generally in lesions of soft tissues
(contusions and ecchymoses, bites) -
62.11%, dento-periodontal traumas
(fractures, dislocations, conccusions,
avulsions and so on) – 19.47%, mandible
fractures – 7.89%, fractures of the facial
massive bone – 7.89% and lesions of ATM
– 2.63% (fig5). It was ascertained that in
comparison to other types of lesions,
dental fractures were at a higher rate –
49%, and as to the topography of the
dento-periodontal traumas, they were
prevailingly located at the level of the
central incisors – 74%.
Fig. 5 Distribution of the lesion type on the orofacial area
We may say that it is highly necessary
to make a minute extra and extra oral
examination in all cases that the dentist
suspects or believes are child abuse cases.
Some authors [7] consider the oral cavity
as being a target of the physical abuse
because of its significance and role in
ensuring important functions, such as
communication or nutrition.
All pediatric dentists should know
how to recognize the signs and symptoms
of child abuse and to be aware of the laws
which requires them to report such cases to
the authorities, because the timely
recognition of such a problem leads to
0
10
20
30
40
50
60
70
80
phys.abuse rape car crash
70,3%
11% 18,7%
soft tiss.les.d-per.tr.
dento-parod
fract mas fac ATMles.

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
20
taking effective intervention measures,
beneficial on the short, medium and long
term, if we consider that most of the times
these children are subject both to physical
abuse and to the emotional abuse, as they
live in fear, they lack confidence in
themselves and have no self-respect.
CONCLUSIONS It is required a holistic approach of
child health and social work for the child,
with the true involvement of all the
decision-makers. As most then half the
lesions resulting from physical abuse are
located in the orofacial area, pediatric
dentists have the moral and ethic
obligation to report child abuse that they
see in their dental practices. The pediatric
dentists should be legally habilitated and
morally entitled to report to competent
authorities that they suspect any child
abuse, as this is a complex issue with
multiple legal-medical and psychological-
behavioral implications.
REFERENCES 1. Maxim A., Balan A., Pasareanu M., Nica M., Stomatologie comportamentala pediatrica, Ed. Contact
International, Iasi 1998, pp 91-97.
2. Stavrianos C., Stavrianou I., Kafas P., Mastagas D., The Responsibility of Dentists in Identifying and
Reporting Child Abuse, The Internet Journal of Law, Healthcare and Ethics 2007, volume 5, number 1.
3. Ambrose JB., Orofacial signs of child abuse and neglect: a dental perspective, Pediatrician 1989; 16:188-
92.
4. American Academy of Pediatrics Committee on Child Abuse and Neglect and the American Academy of
Pediatric Dentistry, Guideline on oral and dental aspects of child abuse and neglect, adopted 1999, revised
2005, vol.3, no.7.
5. Balan A., Maxim A., Pedodontie traumaele dento-parodontale, Ed. Junimea Iasi, 2001, pp192-202.
6. Needleman HL. Orofacial trauma in child abuse: Types, prevalence, management, and the dental
profession’s involvement, Pediatr Dent 1986;8(Spec Iss 1):71-80.
7. Wooley E: Significance of skeletal lesions in infants resembling those of traumatic origin. JAMA, 1955;
158:539.
8. Welbury R, Gregg T., Managing dental trauma in practice, Quintessence publishing Co.Ltd. London 2006,
pp 99-109
9. Welbury RR, Macaskill S.G., Murphy JM., Evans DJ., Weightman KE., Jackson MC., Crawford MA.,
General Dental Practitioners’perception of their role within child protection: a qualitative study, European
Journal of Paediatric Dentistry, 2003; 2:1-7.
10. Tsang A., Sweet D. Detecting Child Abuse and Neglect —Are Dentists Doing Enough?, J Can Dent Assoc
1999; 65:387-91
11. Mouden LD, Bross DC. Legal issues affecting dentistry’s role in preventing child abuse and neglect. J Am
Dent Assoc 1995;126:1173-80.
12. Misawa S., Feature: Child Abuse and what Dentists can do. Forensic Odontology Today, J.F.O.C., 2001; 5;
1.
13. Kenney J.P., Spencer E.D., Child Abuse and Neglect. In Bowers CM, Bell GL (ed). Manual of Forensic
Odontology, ASFO, 1995, pp 191-193.
14. Vadiakas G, Roberts MW, Dilley DC. Child abuse and neglect: Ethical issues for dentistry. J Mass Dent
Soc 1991;40:13-5.

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
21
THE MECHANICAL BEHAVIOR OF THE AESTHETIC MATERIALS
IN VENEERED PROSTHETIC CONSTRUCTIONS Diana Diaconu, Monica Tatarciuc, Anca Viţalariu, St. Panaite
Abstract:
Introduction. The researches in dental materials aria improve the mechanical and biological properties of the
veneered prosthetic constructions. The veneered bridges combine the strength of the metallic restorations with
cosmetic effect of the ceramic or polymeric component.
Materials and methods. The aim of our study is to compare the mechanical and technological parameters of
three aesthetic materials: Solidex (Shofu) and SR Adoro (Ivoclar) resins and Vintage Halo (Shofu) ceramic. The
research investigate the characteristics in making the design of the metall frame, the specific conditioning of the
bonding surface and the methods in application of the aesthetic component, varying with the nature of the
material.
Results and discussions. The knowledge of the technological procedures achieves higher mechanical
performance of fixed veneered constructions. The analyse of those three materials demonstrate that ceramic
component has a greater resistance. Making a comparison between the two types of composites, the SR Adoro
resin has higher mechanical performance, because the double cure method determine a compact and
homogenous structure, consequently, superior performance.
Conclusions. The knowledge of the characteristics of the technological steps allowed to choose an adequate
aesthetic material for fixed veneered bridges, with best mechanical resistance and higher longevity.
Key words: veneered bridges, resin composite, ceramic, mechanical behavior.
INTRODUCTION
The main thrust of the development
work on metalo-nonmetalic prosthetic
construction is to find an aesthetic
veneering material that offers optimal
physical properties, excellent
physiognomy and optimal flexibility. The
veneered bridges combine the strength of
the metallic restorations with cosmetic
effect of ceramic or polymeric component.
The nature of the veneering material has a
direct influence to the design of the metal
frameworkl, to the specific conditioning of
the bonding surface and, implicit, to the
mechanical parameters of the bridges.
MATERIAL AND METHODS
In our work we want to demonstrate,
that the technologigal steps have a huge
influence to the biomechanical behavior of
the bridges, with direct impact on their
clinical performance and longevity.
The purpose was to compare and
analyse three aesthetic veneering
materials: composit resins SR Adoro
(Ivoclar) and Solidex (Shofu), and the
ceramic Vintage Halo (Shofu).
After the construction and
conditioning of the metallic framework
and the edification of the physiognomic
component it was analysed the
deformation behaviour and the fracture
resistance of the fixed prosthetic
construction.
SR Adoro is a microfilled composit
veneering system with high loading of
inorganic microfillers, in nanoscale range.
The matrix, based on urethane
dimethacrylate, give more toughness,
endowning the material with excellent
physical properies and a high resistance to
wear.
The framework is realised so the
dimension concede a stable metal
component and a durable relation between
metal and composite. After finishing, the
framework is blasted with Al2O3 particles,
at 2 barr pressure. It tis basically to apply
retention beads, to provide mechanical
retention, in addition to the chemical bond
-with SR Link. (fig.1)

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
22
Fig. 1 Mechanical retentions beads
The individual SR Adoro pastes are
applied according to the layering diagram.
The aesthetic component is build up step
by step and each segment is precure for 20
sec.(fig.2) The final polymerization is in
Lumamat 100 furnace and the material is
light and heat cured.(fig.3)
Fig. 2 Precuring with Targis Quick Fig. 3 Final curing in Lumamat 100
After the last finishing procedures the
bridge has an optimal aesthetic aspect.
The Solidex resin is also a new
composit material with 53% inorganic
component, 21% organic matrix and 1%
catalysts. The metal substructure is
prepared in the same way: finishing,
blasting with Al2O3; the retention of the
aesthetic component is also mechanical
and chemical. After casting, the retention
beads may be reduced by half of theirsize,
to preserve enough retention surface; the
mechanical retention produce an irregular
surface. The chemical retention, with
Solibond (a silan layer) increase the bond
strength between metal and veneering
composite. Each ledge of the resin
component is light cured.(fig.4)
Fig. 4 Light curing of the composite layers

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
23
It is crucial to adhere to the
recomanded curring depths and maximum
layer thickness of the individual materials
when carrying out the layering procedure.
(Park Y.J.1999)
After polymerization, the bridge is
finished and polished with rotative
instruments and is prepared to be fixed in
the oral cavity.
The ceramic Vintage Halo, the third
material in our study, is a felspatic
porcelain, with a high mechanical
resistance, optical properties similar with
the natural teeth and the wear near to the
enamel.
In the constructions of the metallo-
ceramic bridge, the technological steps are
the same: the design and the fabricate of
the framework, the conditioning of the
metal surface and the apply of the aesthetic
component.
The difference is that the metal
substructure, in metallo-ceramic
constructions do not have macroretentions,
because the metallo-nonmetalic bonding is
strictly chemical.(fig.5)
The framework, smooth and clean, is
conditioned by oxidation and the next step
is to build up the ceramic component,
following each technological step.(fig.6)
Fig. 5 The conditioned metall framework Fig. 6 The apply of the ceramic component
RESULTS AND DISCUSSIONS
It is crucial to know the technological
peculiarities of the prosthetic materials.
The specifically design of the metal
framework influence the resistance and the
retention of the aesthetic component.
The conditioning of the metal surface
increases the bonding strength between
metal and the veneering element. The
metallic nonmetallic relation is important
for the longevity of fixed prosthetic
constructions.( Dale B,1993, Waknine S,
2001)
Our mechanical studies reveal that the
nature of the material, the technological
steps in the building up of the
physiognomic component, the strength of
the interface bonding, influence the
mechanical resistance, the clinical
behavior and, of course, the longevity.
Analyzing the two types of composite
resins, we observe that SR Adoro material
has a higher fracture resistance than that of
Solidex resin. The values of the load
failure are not significantly statistic
different, but clinically, SR Adoro
composite has a better mechanical
resistance. (Kynomoto Y 1998).
The double mechanism in
polymerization- heat and light- determine
for the SR Adoro material a more
homogenous, more dense structure and
less wear. (Lutz F 1999)
As concerns ceramics, Vita Hallo
material has a significantly higher fracture
resistance.(fig7)

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
24
Composite resin
Ceramic material
Fig.7 The comparable behavior of the fracture resistance
The behavior in deformation, at a
loading similar with masticator forces, was
also different, comparing the two
categories of materials. (Giezendanner P
1991)
The ceramic modulus of elasticity is
similar to the enamel and the modulus of
elasticity of the composite resin is similar
to the dentine. (tab.I)
TABLE I
Values of the modulus of elasticity
Material Modulus of elasticity(GPa)
Enamel 50-80
Dentine 15-20
Ceramic 50-80
Composite 10-18
After we calculate the minimal and
maximal deformation for ceramic and
composite, at a loading values comparable
with the masticator forces, we observe that
composite resins has a higher deformation
and a smaller loading resistance in
comparing with ceramic material ( tab II)
TABLE II
Comparative values of the minimal and maximal deformation
Material Minimal
deformation
Maximal
deformation
Composite resin 0,200 0,266
Ceramic 0,080 0,050
CONCLUSIONS
Our mechanical studies reveal that the
nature of the material, the technological
steps in the build up of the physiognomic
component, the strength of the interface
bonding, have a huge influence to the
mechanical resistance, the clinical
behavior and, of course, to the longevity.
SR Adoro material has a higher
fracture resistance than that of Solidex

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
25
resin. The double mechanism in
polymerization- heat and light- determine
for the SR Adoro material a more
homogenous, more dense structure and a
less wear.
The ceramic material has a higher
fracture resistance and a reduce
deformation at the masticator loading.
(Esquivel-Upsaw Josephine 2001, Kato H.,
1996). The knowledge of the technological
procedures achieves higher mechanical
performance of fixed veneered
constructions. The analyses of those three
materials demonstrate that ceramic
component has greater resistance. Making
a comparison between the two types of
composites, the Adoro resin has higher
mechanical performance, because the
double cure method determine a compact
and homogenous structure, consequently,
superior performance.
The knowledge of the characteristics
of the technological steps allowed to
choose an adequate aesthetic material for
fixed veneered bridges, with best
mechanical resistance and higher
longevity.
REFERENCES 1. Dale B., A clinical approach to techniques and materials, Esthetic Dentistry, Leo & Febiger, Philadelphia,
1993, 210-292.
2. Esquivel-Upsaw Josephine, Anusavice K, Reig Megan,Yang M., Lee R., Fracture resistance of all ceramic
and metalo-ceramic inlays , The Journal of Prosthodontics, 2001, (14)2, 26-35.
3. Giezendanner P., Die Anfertigung von Kompositinlays aus Klinischer und zahntechnischer Sicht,
Quintesenz Zahntech.,1991, (17), 407-420.
4. Kato H., Matsumura H., Tanaka T., Atsuta M., Bond strength and durability of porcelain bonding system, J
.Prosthet. Dent., 1996, (75 ), 163-168.
5. Kynomoto Y.,Torii M., Fotoelastic analysis of polymerization contraction stress in resin composite
restorations , J. Dent., 1998, (26), 165-172.
6. Lutz F. ,Phillips R.W., Roulet J., F., Setcos J.C., Varying chewing forces versus wear of composite and
opposing enamel, Journal of Dental Resorations, 1999, (4). 35-44.
7. Park Y.J., Chal K.H., Rawls H.R., Development of a new photoinitiation system for dental light cure
composite resines, Dental Material,1999, (15), 120-127.
8. Waknine S., Conqueste D.F., A new universal dental composite restaurative system, Esthetic Dentistry,
Update, (2), 2001, 256-273.

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
26
THE ROLE AND IMPORTANCE OF THE CARIES DETECTORS DYES
IN EARLY DIAGNOSIS AND TREATMENT OF DENTAL CARIES Pancu Galina
1, Stoleriu Simona
2, Andrian Sorin
3, Gheorghe Angela
4, Topoliceanu
Claudiu5, Pancu Ion
6, Lăcătuşu Ştefan
7
1,2,34,5,7 Departament Restorative Dentistry-Cariology ,
Faculty of Dental Medicine 6
Private Dentistry Medilife, Iassy, România.
Abstract: Despite the progresses of the modern dentistry, the carious disease is still affecting a large number of
peoples. The caries detectors would be helpful for diagnosis of early enamel caries as well as dentinal caries.
The study focused on the role of caries detectors on objective criteria of assessment of the caries preparation, the
early diagnosis of the incipient caries as well as monitorisation of the remineralising processes. The study used
product Color-test of the Vladmiva (Rusia): solution and gel. The study was performed on 25 patients age 15-38
with medium and high level of cariogenic status. The statistical results show the practical importance of the
caries detectors for the conservative treatment of the dental caries, with different degree of penetration in dental
tissues. It also allows the monitorisation of the success of the non-invasive or minimal invasive treatment. The
use of the caries detectors allows minimal preparation of the dental issues, accordingly to modern principles of
the actual dentistry.
Key words: incipient caries, caries detectors, remineralisation therapy.
INTRODUCTION
Although many dentists know modern
principles of dental caries therapy, the use
of dental caries indicators is very limited
in current practice. Today is more
important that restorative dentistry to stand
on minimal invasive approach, without
idle sacrifices of healty dental tissues. The
role of the research is to highlight dental
caries in incipient stages, with caries
detectors dyes and to monitor their
evolution after remineralisation therapy.
MATERIALS AND METHODS
The caries detector dyes Color-test
(Vladmiva, Rusia) is used in study. The
diagnostic and monitorisation of the
incipient dental caries were made through
Borovschii-Axamit method. This method
allows us to assess depth and surface of
demineralisation area. In study were
included 36 patients and 65
demineralisation focuses (white-spot).
These demineralisation areas were divided
in 4 lots: lot 1- 18 teeth (10 patients) with
remineralisation therapy by fluor gel; lot
2- 15 teeth (8 patients) with
remineralisation therapy by calcium,
phosphat and fluor; lot 3- 17 teeth (12
patients) with remineralisation therapy by
calcium-phosphat gel; lot 4 (6 patients)- 15
teeth without remineralisation therapy
(witness lot). The patients were
monitorised for 12 months, with
assessment periodes at 6 and 12 months.
RESULTS
The evolutions of the caries detector
dyes intensity and of the demineralisation
surfaces in the four lots are synthesised in
tables I and II.

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
27
TABLE I.
The evolution of the caries detector dyes
LOT 1 –
F
(Average
values)
LOT 2 –
CaFP
(Average
values)
LOT 3 –
CaP
(Average
values)
LOT 4 –
witnes
(Average
values
Initial 6,06 5,87 5,59 6,80
First
application
4,94
Decreasing
18,34%
4,40
Decreasing
24,99%
2,71
Decreasing
51,56%
After 2
weeks
4,72
Decreasing
22,00%
1,20
Decreasing
79,50%
3,06
Decreasing
45,25%
6,80
Increasing
0,00%
After 6
months
3,72
Decreasing
38,50%
3,07
Decreasing
47,70%
3,47
Decreasing
37,88%
7,07
Increasing
3,92%
After 12
months
1,78
Decreasing
70,59%
2,40
Decreasing
59,06%
1,47
Decreasing
73,66%
7,80
Increasing
14,71%
TABLE II.
Total surfaces of the demineralisation areas
LOT 1 – F
Total
values
LOT 2 –
CaFP
Total
values
LOT 3 –
CaP
Total
values
LOT 4
witness
Total
values
Total
surfaces
(mm2)
54.50 48.20 51,80 46,90
Total
surfaces-
6 months
46.90
Decreasing
13.94%
41,70
Decreasing
13,49%
48,90
Decreasing
5,60%
51,70
Increasing
10,23%
Total
surfaces–
after 12
months
42.30
Decreasing
22.39%
37,60
Decreasing
21,99%
43,40
Decreasing
16,22%
58,90
Increasing
25,59%
The results regarding depth of the
demineralisation focuses (colour
intensity) were different related to the four
lots. For lot 1 (F) the results consisted in
significant decreasing of colour intensity
with 17,2% after first application, with
20,8% after 2 weeks, with 28,7% after 1
month and with 70,5% (after 6 months).
For lot 2 (CaPF) the results consisted in
colour intensity decreasing with 27% after
first application, with 81% after 2 weeks,
with 45,6% after 1 month and with 53,7%

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
28
after 6 months. For lot 3 (CaP) the results
consisted in colour intensity decreasing
with 48,7% after first application, with
37,9% after 2 weeks, with 24,3% after 1
month and small increasing after 6 months.
For lot 4 (witness lot) the results consisted
in colour intensity increasing with 3,92%
after 6 months and with 14,71% after 12
months.
The results regarding surfaces of the
demineralisation focuses (colour
intensity) were different related to the four
lots. For lot 1 (F) the results consisted in
significant decreasing from 54,50 mm to
42,30 mm (decreasing with 22,39%), for
lot 2 (CaPF) the results consisted in
decreasing from 48,20 mm to 37,60 mm
(decreasing 21,99%), for lot 3 (CaP) the
results consisted in decreasing from 51,80
mm to 43,40 mm (decreasing with
16,22%), and for lot 4 there is a increasing
with 25,59% of the total demineralisation
surface.
DISCUSSIONS
Caries detector dyes are useful for
early detection of the incipient dental
caries in pits, fissures and smooth dental
surfaces (Lăcătuşu Şt.., Ismail AI). The
retention of the caries detector dyes allows
precise assessment of the depth and
surface for demineralisation areas, through
assessment of the colour intensity and use
of a graph paper (Ржанов Е.А. şi colab.).
The caries detector dyes are an useful
instrument for detection of secondary
dental caries and fissures or microfractures
(Andrian S., Cureachina N.V.). The
scientific progress of the modern dentistry
allows more effective caries detector dyes
that can be visible in special spectrum. In
fact, these caries detector dyes make
possible a less invasive treatment (Andrian
S., Ржанов Е.А.).
CONCLUSIONS
The caries detector dyes are extremely
useful in early detection of incipient dental
caries located in pits, fissures and smooth
dental surfaces.
REFERENCES 1. Andrian Sorin Tratamentul minim invaziv al cariei dentare , Editura, Princeps Edit, Iaşi 2002, pag. 94-95.
2. Andrian Sorin, Lăcătuşu Ştefan., Caria dentară, protocoale şi tehnici. Ed. Apollonia, Iaşi, 1999.
3. Cureachina N.V., Savelieva N. A. Profilaxia stomatologică. Mascva, Izdatelistvo Mediţinscaia cniga,
2005, pag. 35-55,104.
4. Ismail AI. Clinical diagnosis of precavitated carious lesions. Community Dental Oral Epidemiol
1997;25:13-23
5. Lăcătuşu ŞT., Dănilă I, Ghiorghe A, Iovan G, Pendefunda V, Solomon S. Caria fisurală: diagnostic,
aspecte morfopatologice. Rez.Com. Ses. Şt. ―30 de ani de Învăţământ stomatologic ieşean‖, Iaşi, 1.03.1996,
100, 3-4, 193
6. Ржанов Е.А. Минимально-инвазивное лечение кариеса зубов. // Клиническая стоматология. – 2005,
№1 – с. 24-27.

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
29
PERIODONTAL CHANGES IN CONJUNCT PROSTHESES Valeria Pendefunda, Arina Ciocan-Pendefunda, Carmen Pîrlia
E.P.R. Department- Dental prosthesis
Dentistry Medicine Faculty, U.M.F. ―Gr.T. Popa‖ Iasi
Abstract:
Introduction. The treatment of reduced partially edentulous patients with gnatprosthetic bridges, linked to the
organic substructure, determines on the gum’s tissue many adaptive changes, related to the following factors:
previous state of sulcular epithelium, quality of the finishing edges of the microprostheses, material from which
the bridge is made, definitive cementing materials, etc.
The aim of our study is to assess the impact of the fixed prostheses upon the periodontal health.
Material and method. The study includes 112 patients (54 males and 58 females) with ages between 20-60
years. The evaluation was made on 282 conjunct prostheses. The statistical processing was made by the program
STATISTIC (dedicated to medical research) and specific tests as ANOVA, Spjotvol/Stoline, Pearson, CHI –
square (2), Fisher, Spearman, etc.
Results. Periodontal changes appeared in 44.64% of cases. This aspect was correlated with different
particularities of the prosthetic device. These can be taken into consideration as potential risk factors for
periodontal changes. The study of periodontal health, related to the material that was used, showed a low
prevalence in metal ceramic bridges (14.3%) and metal composite bridges (8.9%). Periodontal changes are more
important in case of high amplitude and older bridges, and they are influenced by the material and the quality of
their finishing. Although, there is a correlation between oral hygiene and periodontal changes of the prosthetic
bridges patients.
Conclusions. Results show a close relation between periodontal changes and: the amplitude and age of the
prosthetic bridges, quality of the finishing edges of the microprostheses, surface texture, axial and transversal
adjustment and the materials used for the bridge and final cementation.
Key words: periodontal dieses, dental – periodontal joint, iatrogenic.
INTRODUCTION
The treatment of partially reduced
edentulous patients with gnatprosthetic
bridges, linked to the organic substructure,
determines on the gum’s tissue many
adaptive changes.
A very important observation,
regarding the prosthetic treatment of
partially reduced edentulous patients, is
that there is the highest iatrogenic risk.
Only small mistakes (just a few
millimeters) in the adaptation of prosthetic
field and the manufacturing of the bridges
may lead to dental pulp damages,
pathological functions and periodontotic
teeth, determining further teeth losses.
The aim of our study is to assess the
impact of the fixed prostheses upon the
periodontal health.
MATERIAL AND METHOD
The study includes 112 patients (54
males and 58 females) with ages between
20-60 years. The evaluation was made on
282 conjunct prostheses by clinical and
paraclinical exams, mainly X-rays. The
clinical evaluation of bridges includes the
following parameters: the age and material
of the bridge, the amplitude, axial and
transversal adaptation, prophylactic
modeling and periodontal modifications:
gum retraction, periodontal bags, teeth
mobility, bleeding index and hygiene
status.
The statistical processing was made
by the program STATISTIC (dedicated to
medical research). We used also many
other specific tests, such as: ANOVA,
Scheffé, Spjotvol/Stoline, correlation tests
for quantitative and qualitative data, such
as: Pearson, CHI – square (2), Mantel-
Haenszel, Fisher, Spearman, Kendall tau,
Gamma.
Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
30
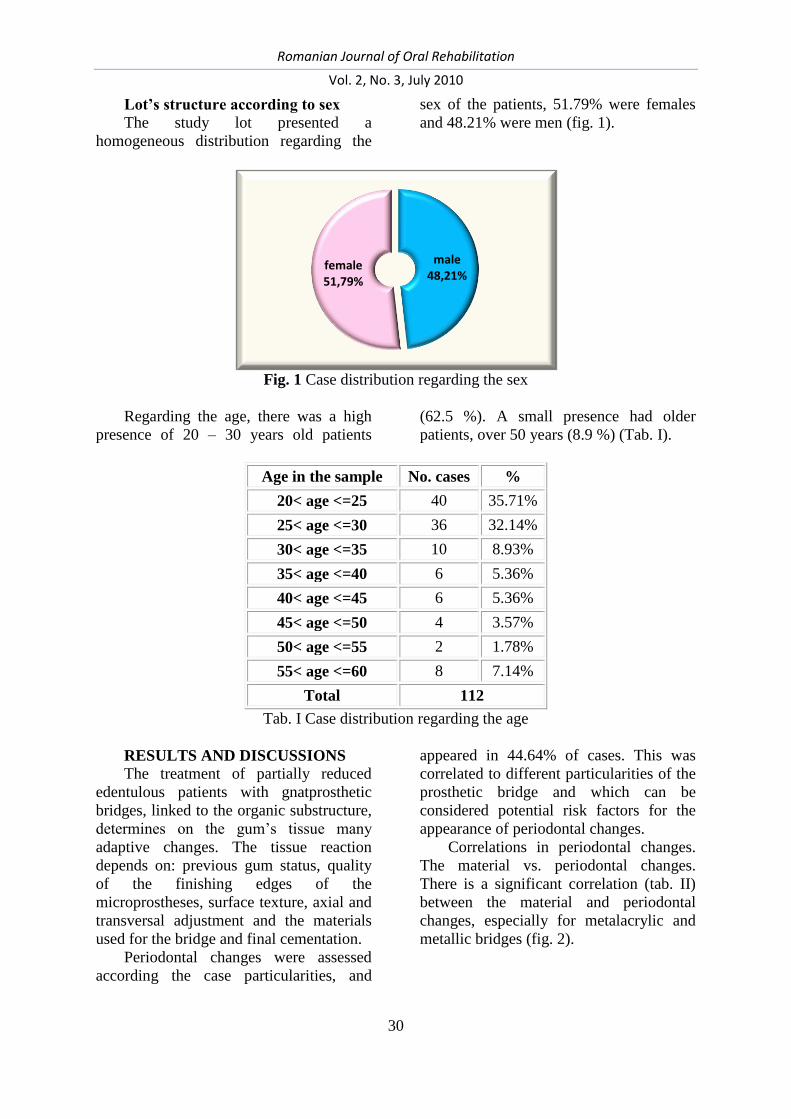
Lot’s structure according to sex
The study lot presented a
homogeneous distribution regarding the
sex of the patients, 51.79% were females
and 48.21% were men (fig. 1).
Fig. 1 Case distribution regarding the sex
Regarding the age, there was a high
presence of 20 – 30 years old patients
(62.5 %). A small presence had older
patients, over 50 years (8.9 %) (Tab. I).
Age in the sample No. cases %
20< age <=25 40 35.71%
25< age <=30 36 32.14%
30< age <=35 10 8.93%
35< age <=40 6 5.36%
40< age <=45 6 5.36%
45< age <=50 4 3.57%
50< age <=55 2 1.78%
55< age <=60 8 7.14%
Total 112
Tab. I Case distribution regarding the age
RESULTS AND DISCUSSIONS
The treatment of partially reduced
edentulous patients with gnatprosthetic
bridges, linked to the organic substructure,
determines on the gum’s tissue many
adaptive changes. The tissue reaction
depends on: previous gum status, quality
of the finishing edges of the
microprostheses, surface texture, axial and
transversal adjustment and the materials
used for the bridge and final cementation.
Periodontal changes were assessed
according the case particularities, and
appeared in 44.64% of cases. This was
correlated to different particularities of the
prosthetic bridge and which can be
considered potential risk factors for the
appearance of periodontal changes.
Correlations in periodontal changes.
The material vs. periodontal changes.
There is a significant correlation (tab. II)
between the material and periodontal
changes, especially for metalacrylic and
metallic bridges (fig. 2).
male48,21%
female51,79%
Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
31
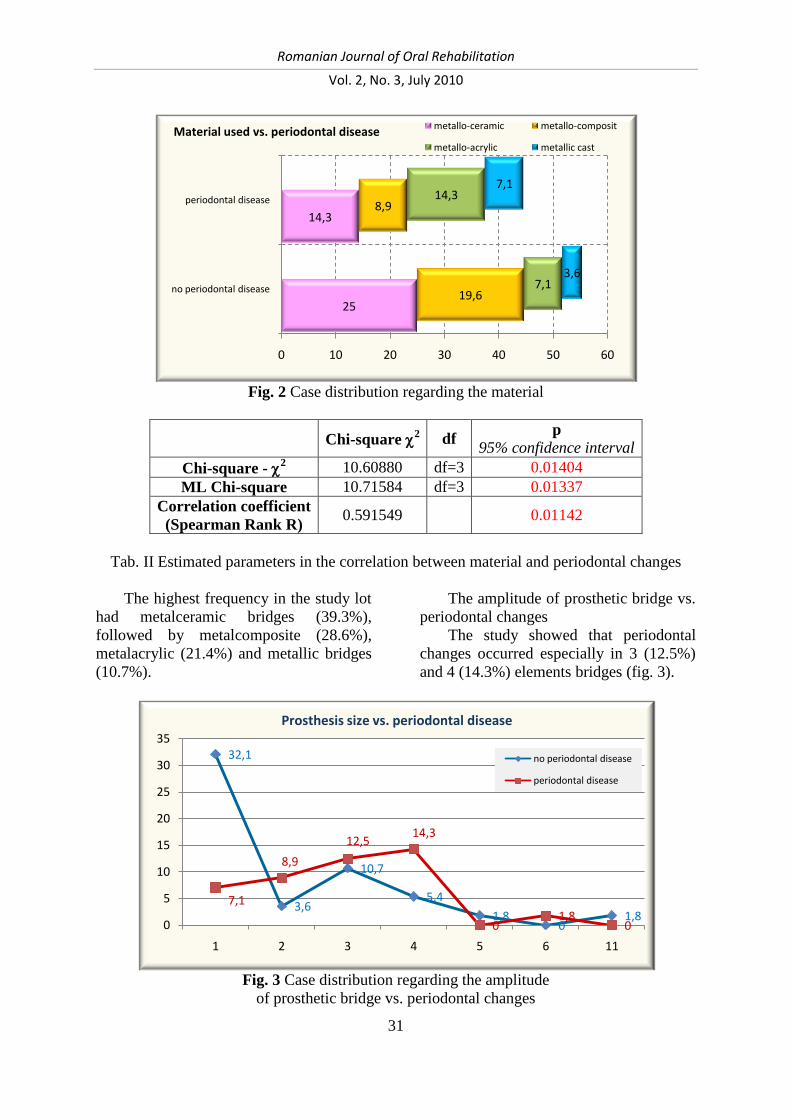
Fig. 2 Case distribution regarding the material
Chi-square 2 df
p
95% confidence interval
Chi-square - 2 10.60880 df=3 0.01404
ML Chi-square 10.71584 df=3 0.01337
Correlation coefficient
(Spearman Rank R) 0.591549 0.01142
Tab. II Estimated parameters in the correlation between material and periodontal changes
The highest frequency in the study lot
had metalceramic bridges (39.3%),
followed by metalcomposite (28.6%),
metalacrylic (21.4%) and metallic bridges
(10.7%).
The amplitude of prosthetic bridge vs.
periodontal changes
The study showed that periodontal
changes occurred especially in 3 (12.5%)
and 4 (14.3%) elements bridges (fig. 3).
Fig. 3 Case distribution regarding the amplitude
of prosthetic bridge vs. periodontal changes
25
14,3
19,6
8,9
7,1
14,3
3,6
7,1
0 10 20 30 40 50 60
no periodontal disease
periodontal disease
Material used vs. periodontal diseasemetallo-ceramic metallo-composit
metallo-acrylic metallic cast
32,1
3,6
10,7
5,4
1,80
1,87,1
8,9
12,514,3
01,8
00
5
10
15
20
25
30
35
1 2 3 4 5 6 11
Prosthesis size vs. periodontal disease
no periodontal disease
periodontal disease

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
32
The study demonstrated a significant
correlation between the prosthetic bridge
amplitude and periodontal changes. In one
element bridges the changes occurred only
in 7.1% of cases. In 3 and 4 elements
bridges the changes increased significantly
(r=0.51, p=0.001, 95%CI).
The age of prosthetic bridge vs.
periodontal changes
The medium values of the age of
prosthetic bridges depending on the
changes were 10.4 months in the cases
without modifications, and 51.5 months in
the cases with periodontal changes (tab.
III).
Periodontal
disease
Mean
Prosthesis age
Mean
Dev.std Er. std Min Max Q25 Median Q75 -95% +95%
Absent 10.4 2.4 18.4 31.4 4.0 0.2 240.0 1.0 3.0 7.0
Present 51.5 30.3 72.8 74.7 10.6 1.5 300.0 12.0 24.0 36.0
Total 28.8 17.8 39.7 58.6 5.5 0.2 300.0 2.0 7.5 24.0
Tab. III The age of prosthetic bridge vs. periodontal changes
Prosthesis age F (95% confidence interval) p
ANOVA test 15.42233 0.000150
Tab. IV Test for comparison of the medium values of the age of prosthetic bridges depending
on the periodontal changes
Results of ANOVA test demonstrate
significant differences between the
medium values of the age of prosthetic
bridges and the presence or absence of
periodontal changes (p=0.00015, 95%CI)
(tab. IV).
The anatomical restoration of
prosthetic bridge vs. periodontal
changes
The anatomical restoration of the
tooth leaded to an absence of periodontal
changes in 67.4% of cases. Contrary,
84.6% of cases without anatomical
restoration presented periodontal
modifications (fig. 4).

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
33
Fig. 4 Case distribution regarding the anatomical restoration of prosthetic
bridge vs. periodontal changes
Estimated value 95% Confidence interval
Minim Maxim
Chance parameters
Odds ratio (OR) 11.39 3.27 43.5
Risk parameters
Relative risk (RR) 2.6 1.84 3.67
STATISTICAL TEST Chi-pătrat
Chi - squared (χ2) 21.89
p – significance level 0.0000029
Correlation coefficient 0.838
Tab. V Estimated chance and risk parameters depending on the
periodontal modifications in the bridges without anatomical restoration
The lack of anatomical restoration of
the teeth was taken into consideration as a
risk factor for the contingent table (tab. V).
Starting from here we calculated the
chance and risk parameters depending on
the periodontal changes. From this study
we can notice that the chance ratio for
periodontal changes is 11.39 (OR=11.39),
which is a high risk for the patients with
prosthetic bridges that do not respect the
tooth anatomy to present periodontal
changes (11.3 times higher then cases with
anatomical restorative bridges). This
parameter can increase up to a highest of
43.5 (OR=43.5).
The results show that any
modification (rough edges of
microprostheses, retentive spaces between
margins and organic substructure) of the
gum, which has a high predisposition to
bacterial plaque, promotes quantitative and
qualitative changes of the plaque. The
modification of the plaque’s ecology
determines a local inflammation and a fast
depth and surface spreading of bacteria.
The presence in the bridges and cements of
toxic and irritating materials will maintain
and amplify the already existing
inflammation.
CONCLUSIONS
The periodontal changes are in close
relationship with: amplitude and age of the
prosthetic bridges, quality of the finishing
32,6
84,6
67,4
15,4
0
10
20
30
40
50
60
70
80
90
doesn't respect the teeth morphology respect the teeth morphology
The teeth's anatomic shape vs. periodontal disease
periodontal disease
no periodontal disease

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
34
edges of the microprostheses, surface
texture axial and transversal adjustment
and the materials used for the bridge and
final cementation. These parameters are
risk factors which will determine
important periodontal modifications.
REFERENCES 1. Carranza F.A., Glickman’s
Clinical Periodontology 7/e, HBJ I.E.Saunders Philadelphia 1990, 403-420.
2. Burlui V., Norina Forna, Gabriela Ifteni., Clinica şi Terapia Edentaţiei Parţiale Intercalate Reduse, Ed.
Appolonia Iaşi 2001, 50-55.
3. Bratu D., Nussbaum R., Bazele clinice şi tehnice ale protezării fixe, Ed.Signata Timişoara 2001, 592-617.
4. Blanchard J.P., Lauverjat Y., Limites prothetiques et environnement gingival. Les Chaier de Prothese
1996, 94, 45-50.
5. Shillingburg H.T., Jacobi R., Brackett S.E., Les préparations en prothèse fixée. Principes et applications
cliniques, Ed.CdP,Paris 1988, 45-57.
6. Silness J., Fixed prosthodontics and periodontal health. Dent. Clin.North Am.1980, 24: 317.
7. Gűnay H., Tschernitschek H., Geurtsen W., Ligne de fintion des préparations et de sante parodontale –
Etude clinique prospective sur 2 ans. Parodontie et. Dentisterie Restauratrice 2000, 20, 173-181.
8. Ayad M.F., Rosensiel S.F., Salama M., Influence of tooth surface roughness and type of cement on
retention of complete cast crowns J.Prosthet Dent 1997,77,116-121.
9. Vataman R., Noţiuni de profilaxie parodontală, I.M.F. Iaşi 1982.
10. Brian S. Everitt, Modern Meddical Statistics, Oxford University Press Inc. New York, 2003.

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
35
RADIODENSITOMETRIC STUDY REGARDING CONSERVATIVE
ENDODONTIC THERAPY IN PERIAPICAL LESIONS 1Sãlceanu Mihaela,
2Donciu Cristi,
3Maria Vataman,
4Radu Vataman
1 Assistent, Discipline of Endodontics, Department of Odontology and Parodontology,
School of Dental Medicine, „Gr.T.Popa‖ University of Medicine and Pharmacy, Iasi,
Romania 2 Tehnical University of Iasi, Romania
3 Professor, Discipline of Endodontics, Department of Odontology and Parodontology,
School of Dental Medicine, „Gr.T.Popa‖ University of Medicine and Pharmacy, Iasi,
Romania
4 Professor, School of Dental Medicine, „Gr.T.Popa‖ University of Medicine and Pharmacy,
Iasi, Romania
Abstract:
Introduction. Our study aimed to assess periapical healing processes using a quantitative method based on
radiodensitometry.
Material and methods. The evolution of periapical lesions in a study group of 10 patients taken in conservative
endodontical therapy was monitorised through radiographs taken at baseline, after 12 months and after 24
months. The radiographs were scanned at 300 dpi resolution with an automated level of bright and contrast.
Modification of bone density and periapical lesion size were assessed using radiodensitometry.
Results and discussions. Radiodensitometry indicated objectively the increase of bone density and decrease of
periapical radiotransparencies size that were correlated with time interval and preoperator diagnostic.
Conclusions. Radiodensitometry can be useful for an objective cuantification of endododontic therapy success
in chronic periapical periodontitis..
Keywords: periapical lesions, endodontic therapy, bone density, size, radiodensitometry
INTRODUCTION
The conventional radiographic
examen is an important tool in
contemporary dentistry related to
diagnostic and monitoring of healing
processes of periapical lesions post-
nonsurgical treatment. Post-treatment
monitoring of healing processess is based
on radiographic criteria of success or
failure. The absence of changes in
periapical radiotransparency diameter or
increase of periapical lesion diameter
represent signs of failure treatment.
However conventional radiographs taken
at different time intervals can present
different contrasts, bright levels and scales
because of the different angles of
incidence and different properties of the
films./1/ To reduce the error possibilities,
dentists use a category of indices, named
PAI (Periapical Index), on a scale that
includes clinical situations from healthy
periapical bone to severe chronic apical
periodontitis. That is why, in some cases
that present discrete healing processes,
conventional radiography can lead to
diagnostic errors. Digital radiovisiography
allows an objective assessment of stages of
periapical healing because of the
reproductibility and possibilities of
objective measurement but this method is
not a routine practice for most dentists
because of the high costs. As alternative
technique to improve diagnostic
performances were proposed optical
densitometry or processing of digitized
serial radiographs /2/ Also images
processing can offer objective indicators
for a number of medical applications/3/
AIM
Our study aimed to present
possibilities of radiodensitometry in
monitorising the evolution of periapical

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
36
status at patients with periapical lesions
treated through conservative endodontic
therapy.
MATERIAL AND METHODS
Study group included 12 patients with
age ranging between 19 and 34 years, with
bicusps and molars with severe periapical
lesions (PAI 4-5) treated endodontically
and monitorised for 24 months. Working
protocol followed conventional stages
used in periapical lesions treatment.
NaOCl 2,5% and EDTA 17% were
solutions used as root canals irrigants,
Rockle’s solutions was used as antiseptic,
and calcium hydroxide was used as
intracanalar medication for 14-30 days.
Radicular obturations were processed
using lateral condensing technique and
Endoflas sealer (Sanlor), a sealer with
powerful antibacterial and remineralising
properties (calcium hydroxide, eugenol,
iodoform). Following endodontic
treatment, periapical lesions presented
visible positive evolution for all teeth
taken in study. Conventional periapical
radiographs were taken baseline, at 12
months and 24 months. The radiographs
were scanned at 300 dpi resolution with an
automated level of bright and contrast. To
avoid subjective analyzing of healing
processes, conventional radiographs were
processed through radiodensitometric
method. The implemented processing
algorithm uses as source the digitized
image of the classic radiographies or the
image obtained in digital format. The main
instrument, in realizing the interpreting
analysis for the bone tissue’s renewal, is
the histogram function. Only those pixels
having a value that falls in this range are
taken into account by the histogram
calculation. In order to objectively
interpret the process of bone tissue’s
renewal, it is defined a global index of
renewal. The global index of renewal (GI)
represents an objective evaluation of the
bone tissue’s renewal, being defined as the
ratio between the global luminous intensity
of a geometric area (ROI –Region of
interest) of affected tissue and the
luminous intensity of the same geometric
area of healthy tissue. The software
instrument is represented by LabView 8.2.
Imaging processing was realized through
virtual instrumentation techniques in order
to calculates and displays the value of the
global index of renewal and the average
value of the gray level, specific to the
healthy bone tissue. Taking into
consideration that the determination of the
ROI area is realized with certain
subjectivism, to calculate the final
evaluation value (GI) it was introduced the
reporting of the ROI to the same area with
the reference gray hue of the healthy
tissue. So, the total number of pixels, as
ROI area, is not a parameter that will
interfere in the calculation of the global
index of renewal. To interpret the
evolution of the bone tissue’s renewal of a
patient it were taken into consideration
three radiographies taken during 24
months interval of monitoring.
RESULTS AND DISCUSSIONS
We selected three representative cases
of chronic periapical lesions with visible
gradual evolution that was quantified
through radiodensitometric methods.
Case 1. Patient B.A, age 31. Patient
presented at 3.5. a periapical granuloma
with PAI 5. Periapical lesion was treated
following conservative endodontic
treatment as described below. Control
radiographs were taken at 12 months and
24 months. Figure 1 presents periapical
status of 3.5. periapical area at baseline.
Figures 2-3 present processed
conventional radiographs and values for
Global index of bone renewal. We see an
increase of GIR from 77% at 12 months
post-treatment to 81% at 24 months post-
treatment.

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
37
Fig.1. Radiographic aspect at baseline (3.5.)
Case 2. Patient C.A, age 28. Patient
presented at 3.6. difuse periapical osteitis
with PAI 5. Periapical lesion was treated
following conservative endodontic
treatment as described below. Control
radiographs were taken at 12 months and
24 months. Figure 4 presents radiographic
aspect of 3.6. periapical area at baseline.
Figures 5-6 present processed
conventional radiographs and values for
Global index of bone renewal. We see an
increase of GIR from 64% (12 months
post-treatment) to 80% at 24 months post-
treatment.
Fig.4. Radiographic aspect at baseline (3.6.)
Fig. 3. Stage 3 of investigation
Fig. 2. Stage 2 of investigation

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
38
Fig.5. Stage 2 of investigation (12 months post-treatment)
Fig.6. Stage 3 of investigation (24 months post-treatment)
Case 3. Patient D.D., age 26. Patient
presented at 3.5. periapical granuloma with
PAI 5. Periapical lesion was treated
following conservative endodontic
treatment as described below. Control
radiographs were taken at 12 months and
24 months. Figure 1 presents processed
conventional radiographs 3.5 and values
for Global index of bone renewal. We see
an increase of GIR from 51% at 12 months
post-treatment to 66% to 24 months post-
treatment.
Fig.7. Radiographic aspect at baseline (3.6.)
Fig. 8 Stage 2 of investigation (12 months post-treatment)

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
39
Fig. 9 Stage 3 of investigation (24 months post-treatment)
For all radiographs sets taken in study
index GIR presented a gradual increase
value indicating the existence of
remineralisation processes of bone tissues.
GIR changes express the periapical healing
processes observed on conventional
radiographs. Our results sustain favourable
conclusions of similar studies focused on
possibilities of improving diagnostic and
monitoring of periapical lesions evolution
through methods of imaging processing
and radiodensitometry /4-8/.
CONCLUSIONS
The evolution of the periapical healing
processes can be objectively quantified
through radiodensitometry. The various
values of bone remineralisation degree,
detected in the selected cases, indicate the
different individual reactions influenced
by systemic status, reactivity of immune
system, phosphate and calcium
metabolism and type and extension of
chronic periapical lesions.
REFERENCES 1. Gordon J.Christensen. Why switch to digital radiography? J Am Dent Assoc, Vol 135, No 10, 1437-1439.
2004
2. Heling I,Bialla-Shenkman S,Turetzky A,Horwitz J,Sela J. The outcome of teeth with periapical
periodontitis treated with nonsurgical endodontic treatment: a computerized morphometric
study.Quintessence Int 2001;32:397-400.
3. Fujimasa, I., Nakazawa, H., Miyasaka, E. Development of an image processing software for medical
thermogram analysis using a commercially available image processing system, Engineering in Medicine and
Biology Society, 1998. Proceedings of the 20th Annual International Conference of the IEEE Volume 2, 29
Oct.-1 Nov. 1998 Page(s):956 – 958
4. Nicopoulou-Karayianni K., Bragger U., Patrikiou A., Stassinakis A., Lang P. Image processing for
enhanced observer agreement in the evaluation of periapical bone changes. Int.Endod J.2002 jul; 35 (7): 615-
622
5. Orstavik D, Farrants G, Wahl T, Kerekes K. Image analysis of endodontic radiographs: digital
subtraction and quantitative densitometry. Endod Dent Traumatol. 1990 Feb;6(1):6-11
6. Orstavik D. Radiographic evaluation of apical periodontitis and endodontic treatment results: a computer
approach. Int Dent J. 1991 Apr;41(2):89-98.
7. Rózyło-Kalinowska I, Czelej-Górski J, Rózyło TK. Radiodensitometric measurements in cases of chronic
periapical changes of endodontically treated teeth. Ann Univ Mariae Curie Sklodowska [Med].
2002;57(1):98-105
8. Narcis M.Marcov, Elena-Cristina Gh.Roman. Digital radiodensitometry monitoring evolution of bone
periapical lesions posttreatment. Journal of Romanian Medical Dentistry 2008; 3 (vol.12): 73-82
Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
40
PRE-EXTRACTIONAL VALUE OF THE INTERNATIONAL
NORMALIZED RATIO IN IDENTIFICATION OF THE
HEMORRHAGIC AND THROMBOEMBOLIC RISK IN PATIENTS
UNDERGOING ORAL ANTICOAGULANT TREATMENT Oleg Zănoagă
1, Valentin Topalo
1, Ion Corcimaru
2, Dumitru Sîrbu
1, Ilie Suharschi
1
State University of Medicine and Pharmacy ―Nicolae Testemiţanu‖ 1 Department of Orthopedic Dentistry, Oro-maxillo-facial Surgery and Oral Implantology
Abstract: The study comprised 38 patients undergoing antithrombotic treatment. Relying on the research which
we have carried out, we can conclude that patients who undergo unsupervised anticoagulant treatment have an
increased both hemorrhagic and thromboembolic risk. The incidence of bleeding after dental extraction in
patients undergoing antithrombotic therapy who have been extracted teeth without any prior withdrawal of these
drugs, is 30,8±10,2%. These hemorrhages, having recorded the values INR<2,4, have an insignificant intensity.
As a prophylaxis of the severe hemorrhagic and thromboembolic events the dose of the anticoagulant drug will
be modified depending on INR.
Key words: tooth extraction, bleeding after dental extraction, thromboembolism, international normalized ratio.
INTRODUCTION
Thrombolitic therapy is known to be
one of the most important 10
achievements of cardiology in the XXth
century (N.J. Mehta and I.A. Khan, 2002).
Nowadays some oral anticoagulants with
coumarinic or inandionic structure are
used. They differ by the time of their
action, active doses, effect duration [1].
Due to its advantageous pharmacological
peculiarities (it is less toxic, it has an
adequate plasmatic T1/2) warfarin has
become in the last years, in the majority of
European countries and USA, the drug of
the first choice in the prolonged therapy
with oral anticoagulants [2]. In Romania,
the only oral anticoagulant registered at
present is acenocoumarol (thrombostop)
[3]. At the same time, of all antithrombotic
drugs, acetylsalicylic acid (aspirin) has a
central place.
In the last years the indications for
treatment with oral anticoagulant drugs
have extended [4]. This is due to an
increase of the angio/and cardiosurgical
assistance rendered to population (cardiac
valve prosthesis, coronary by-pass,
valvuloplasty as well as the number of
people who are carriers of artificial cardiac
valves and valve prosthesis, with
disturbances of the cardiac rhythm etc. [5].
In 1997 there were performed 64000
valvular surgeries in the whole Europe.
Mechanic prostheses were used in 2/3 of
these cases [6]. At present 500
cardiosurgeries are annualy performed in
MSPI Center of Heart Surgery from
Chisinău.
It is known that mechanic valves are
foreign bodies for the organism which
have a high risk of infections and
thromboembolic complications. This fact
requires an anticoagulant therapy and
prophylactic antibiotic therapy during the
whole life [7]. Sometimes these patients
require to be rendered stomatological
assistance including dental extractions.
The latter can lead to hemorrhagic
complications. The hemorrhagic events are
relatively frequent in this group of patients
[1]. They are fostered by a high risk of
overdosage, linked with the individual
variations in the pharmacokinetic
behaviour, as well as interferences
connected with different pathologic
conditions or associated drugs [1,2].
According to data taken from literature,
the incidence of hemorrhages in patients
undergoing a treatment with indirect
anticoagulants varies between 5-10% [2].

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
41
The rate of severe bleedings is 2,4-8,1%,
while the rate of the fatal outcomes is 0–
4,8% [2].
Thrombolitic disease represents a
major complication of the surgical patient.
The importance of this medical problem,
on the one hand is due to the increase of
frequency, on the other hand it is due to
the difficulties of intravital diagnosis and
increased lethality [8]. Anatomo-clinical
statistics of USA shows that massive
embolism is the third cause of sudden
death. About 300 thousand patients are
annualy hospitalized with profound venous
thrombosis (PVT) which causes
approximately 50 thousand deaths from
pulmonary thromboembolism (PTE). The
incidence of PVT in Europe which was
recorded in the last years, reached 160
cases at 100 thousand population. Over 80
thousand of PTE occur annualy in
France,while, at least 20 thousand deaths
are recorded.
In order to prevent occurence of
hemorrhagic and thromboembolic
accidents, patients following anticoagulant
treatment are compelled to monitor their
monthly anticoagulant effect of
coumarinic drugs [1,2,9]. With this
purpose the optimum level of oral
anticoagulant drugs is assessed by
monitoring the time of prothrombin which
is represented by the international
normalized ratio (INR) [2,9]. The
therapeutic level of anticoagulants depends
on the indication for which it was
administered. INR values range within 2,0-
4,0 [9]. The higher this coefficient is the
more marked hypocoagulation is and,
consequently, the hemorrhagic
complications are more frequent and more
dangerous. Conversely, reduction of INR
values below the therapeutic range limits
leads to increase of the risc of
thromboembolitic events occurence [9].
Management of teeth extraction in
patients under antithrombotic therapy is
disputable [10,11]. In order to prevent
hemorrhagic accidents some doctors
recommend their patients to cancel oral
antiplatelet and/or anticoagulant therapy
some days prior to operation (pre-
surgically and pre-extractionally) [12],
others recommend a compulsory
substitution with heparin during the whole
period of treatment, up to oral
anticoagulants return [13]. Other
researchers suggest to perform dental
extractions in patients undergoing
antithrombotic therapy without suspending
these remedies [14]. Thus, the dilemma
widley disputable within the last years in
the medical literature: „Is it necessary to
discontinue anticoagulant treatment in
patients who are sibjected to tooth
extractions?‖ – is still actual and any
gained experience contribute to
elaboration of an optimal treatment
management of these patients.
So, the problem of tooth extraction in
patients undergoing antithrombotic therapy
has a major practical importance and is
insufficiently approached in the medical
literature. Therefore there are
complications which occur in these cases
and varied choice of medical tactics, which
is often groundless.
PURPOSE OF STUDY
To assess the frequency of the post-
operatory hemorrhage, hemorrhagic and
thromboembolic risk in patients
undergoing antithrombotic therapy who
are subjected to dental extractions without
cancelling these drugs.
MATERIALS AND METHODS
The study comprised 38 patients under
antithrombotic therapy. They were
admitted to Oro-maxillo-facial Surgery
Department from the National Scientific
Practical Centre of Emergency Medicine
(NSPCEM) from Chişinău in April 2007 –
November 2009. Men (18) constituted
47,4 ± 8,1%, while women (20) - 52,6 ±
7,6% (p>0,05). Mean age was 54,8 ± 1,7
years (p<0,001). Of 38 patients, 26 (68,4
± 7,5%) were hospitalized in order to be
performed surgical manipulations in the
oral cavity (34 dental extractions were

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
42
carried out). 12patients (31,6 ± 7,9%)
(p<0,01) – complained of hemorrhage in
the oral cavity: 8 (66,7%) had post-
extractional dental hemorrhage (PDH), 3
(25,0%) hemorrhage resulting from
periosteotomy and 1(8,3%) patient with
gingival hemorrhage.
Clinical examination was carried out
according to the traditional methods of
patients examination. The routine
parameters of general and biochemical
blood analyses, urine analysis,
coagulogram indices (prothrombin index,
fibrinogen content, time of partially
activated thromboplastin (TPAT),
thrombin time, ethanol test), panoramic
and retroalveolar radiography,
electrocardiography were examined.
To have an orientative examination of
the haemostatic system, the examined
patients were determined the bleeding time
according to Duke and blood coagulation
time according to Lee-White.
The effect of oral anticoagulants was
assessed at admission and in dynamics
through determination of INR values. Due
to its pharmacological properties, aspirin,
unlike indirect anticoagulants
(thrombostop, warfarin, fenilin) does not
require laboratory monitoring of
coagulations [2]. Despite this fact in 5
patients who were administering aspirin,
the anticoagulant effect was not estimated
through assessment of INR values.
The mathematical processing of the
study results was carried out by means of
the statistical set of programs: EXCELL
and STATISTICA. Obtained results were
presented by the respective tabels.
RESULTS AND DISCUSSIONS
Our studies have reported that of 38
patients ungergoing antithrombotic
therapy, the majority of patients (21
patients or 55,3%) were administered
thrombostop, being followed by those who
were receiving warfarin (9 or 23,7%),
aspirin (5 patients or 13,1%) and fenilin (3
patients or 7,9%). The causes of
administration of antithrombotic therapy
were the following : cardiosurgical
interventions (valve prosthesis) - in 32
cases (84,2%); ischemic cardiopathies – in
4 (10,5%); thromboembolic case history –
in 1 (2,6%); thrombophlebitis of the lower
extremity – in 1 patient (2,6%).
Although multiple guides and
recommendations on thromboprophylaxis
are published, the way these
recommendations are applied into the
medical practice represents only a partially
solved problem. Studies that have
observed this aspect, suggest that
pharmacological thromboprophylaxis is
underutilized in 30-50% of patients with
thromboembolic risk [3]. This fact was
stated in the current study as well. Thus,
after anamnesis taking it was stated that of
33 patients receiving oral anticoagulant
therapy, in 11 (33,3%) patients the effect
of these drugs was not monitored.
Consequently during 2-3 months INR
values were not estimated in 6 patients,
between 4-6 months – in 3 patients and >
12 months in 2 patients.
Moreover, in the medical practice
anticoagulant therapy interruption is
frequently groundless. Thus, after history
taking it was established that of 38 patients
in 7 cases (18,4 ± 6,3%) the oral
anticoagulant therapy was cancelled one
day prior to dental extraction in order to
prevent hemorrhage occurence. In 4
(57,1%) cases the patient himself
discontinued receiving the anticoagulant,
in 2 (28,6%) cases the patients were
recommended by the dentist to discontinue
the therapy; in 1 case (14,3%) – the patient
got the indication from the family doctor.
Despite the fact that the duration of
thrombostop effect after treatment
interruption is 48-72 hours, unlike
warfarin which has a longer effect
duration (5-7 days) [1], we can state that
interruption of these drugs one day prior to
operation hasn't been justified, at least
from the theoretical point of view.
Postoperatory wound bleeding having
continued, patients required specialized
medical assistance. At the same time it

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
43
should be recognized the fact that having
groundlessly interrupted the anticoagulant
therapy, these patients were exposed to a
major thromboembolic risk.
Of those 38 examined patients
positive hemorrhagic anamnesis was
revealed in 33 cases (86,8 ± 5,9%,
p<0,001). It manifested by occurence of
bruises without any marked lesions in 19
(57.6%) patients, post-extractional dental
hemorrhages in 7 (21,2%) patients,
excessive menstrual hemorrhage in 4
(12,1%) cases. Hemorrhagipar syndrome
was less frequent (9,1%), it manifested in
the anamnesis by epistaxis, hemorrhage
after periosteotomy and petechiae
hemorrhages in places where clothes were
tightly adherent to skin. Thus, clinical
manifestations of hemorrhagipar
syndrome, which previously had been
recorded (within anamnesis) in patients
following antithrombotic therapy, were
marked by multiple symptoms of
hemorrhagic character. At the same time,
the most frequent symptom (in 57,6 ±
8,6% cases) recorded in these patients was
occurrence of bruises without any evident
lesions or after insignificant traumatism. It
is necessary to mention the fact that
negative hemorrhagic anamnesis was
established in those 5 patients (13,2 ±
5,5%, p < 0,05) following antiplatelet
(acetylsalicilic acid) therapy. Perhaps, this
fact is due to different patients
sensitiveness to aspirin. In this respect, the
patients are divided into some groups
according to their sensitiveness [15]:
reactive (aspirine in dose of 0.5g
diminishes aggregation by 50-40%);
hyperreactive (aspirin inhibits the
aggregation maximally or up to 80-90%)
and areactive (antiplatelet effect is absent).
According to some sources it was
established that only 20-25% of patients
receiving antiplatelet drugs have abnormal
bleeding time (a prolonged one) [16].
Initial evaluation of the haemostatic
system was carried out through
determination of the bleeding time
according to Duke and the coagulation
time according to Lee-White. Thus, of 38
patients, 36 (94,7 ± 3,6%) patients had
bleeding time according to Duke within
the limits of normal values (2-4 minutes).
Only 2 patients (5,3 ± 3,6%) (p<0,001)
were suspected with alteration of the
primary haemostasis through increase of
the bleeding time (5 and 6 minutes), it
being subsequently confirmed by decrease
of the platelets count (58,0.10
9/l şi
84,0.10
9/l). After having estimated the
coagulation time according to Lee-White,
it was stated that in 3 patients (7,9 ± 4,3%)
the values of this test exceeded the upper
limit of the norm (>12 minutes), INR
being 4,6; 4,7 and 4,8. By means of these
two tests, initially there were suspected,
then confirmed marked disturbances in the
primary vasculo-thrombocyte haemostasis
(severe thrombocytopenia) and in the
secondary haemostasis (overdosage of
indirect anticoagulants).
In patients whose INR (at admission)
was below the therapeutic range limits (<
2), the anticoagulant dose was individually
increased (pre-extractionally as well) to
prevent thromboembolic accidents. It was
increased up to INR adjustment within the
therapeutic limits. The results obtained
from adjustment of dose of the oral
anticoagulant therapy are presented in
Tabel 1.

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
44
INR values At admission At discharge
p n P±ES% n P±ES%
1,0 – 1,9 15 45,5 ± 8,7 - - ****
2,0 – 2,5 10 30,3 ± 7,9 28 84,8 ± 6,2 ****
2,6 – 3,0 3 9,1 ± 5,0 4 12,1 ± 5,7 *
3,1 – 3,5 1 3,0 ± 2,9 1 3,0 ± 2,9 *
3,6 – 4,0 1 3,0 ± 2,9 - - *
4,1 – 4,5 - - - - -
4,6 – 5,0 3 9,1 ± 5,0 - - *
Tabel 1. INR values at admission and discharge in patients receiving oral anticoagulant
therapy (n = 33) (* p > 0,05 **** p < 0,001)
The data from the tabel show that INR
(at admission) ≤ 1,9 was revealed in 15
patients (45,5 ± 8,7%). To reduce the risk
of occurrence of the thromboembolic
events, the anticoagulant dose was
increased up to INR adjustment to the
therapeutic range values (2,0-4,0). In 15
(45,5 ± 8,7%) cases INR was within the
therapeutic range limits and anticoagulants
dose was not modified. It was stated an
overdosage of indirect anticoagulants in 3
patients (9,1 ± 5,0%). INR values at
admission were 4.6-4.8. In patients with
overdosage, the anticoagulant dose was
reduced and subsequently kept within the
therapeutic limits. There was one
exception when the anticoagulant was
cancelled by general physician`s
indication. In the result we have
determined that after having been
administered the individual anticoagulant
dose, all the patients were discharged with
INR within the limits of 2.0-3.5, that is
within the therapeutic range limits. Thus,
thromboembolic complications have been
avoided, especially in patients hospitalized
with INR values below the therapeutic
limits.
Pre-extractional modification
(increase) of the oral anticoagulant dose in
patients with INR (at admission) below the
therapeutic range limits is reflected in the
following clinical case.
Patient C.V., aged 57 years, medical
card nr.21485, was admitted to the
Departament of OMF Surgery on
November 18, 2008 complaining of
presence of the root debris on the mandible
on the left side which periodically caused
painful sensations and discomfort; marked
general weakness. From the anamnesis –
painful dental sensations appeared 10-11
days prior to admission. The respective
teeth were endodontically treated 8 years
ago. As the patient stated and according
to the data from the medical outpatient
card in 2005 the patient had undergone a
cardiosurgical intervention (mitral valve
prosthesis) after which he received
thrombostop (2mg/day). The last check-up
of INR was done on March 15, 2007. Its
values were 2.0. Thus, it was established
that trombostop effect had not been
monitored for one year, although at
patient's discharge from MSPI Center of
Heart Surgery, the patient was
recommended by his physician to monthly
assess INR and to keep it within the limits
of 2,5-3,5. Objective examination:
symmetrical face, pale-rose colour of the

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
45
skin. The regional lymphatic nodes were
not palpable. Mouth opened easily.The
endobuccal examination revealed presence
of the 35th, 36th teeth roots. They were
not tender to percussion in the axis. They
were immobile. Palpation of both slopes of
alveolar apophysis of the 35th, 36th teeth
was painless. The haemodynamic indices
at admission: AP= 110/70 mmHg, puls =
78 b/min. Bleeding time according to
Duke = 3 minutes, while the blood
coagulation time according to Lee-White =
12 minutes. The patient was consulted by
the internist. Orthopantomography
revealed presence of oval, radiotransparent
formations, with a well-defined contour
around the 35th, 36th teeth apices, with a
size of < 0,5 cm.
The diagnosis was established on the
basis of the clinical and paraclinical
examination: „Chronic granulomatous
periodontitis of the 36th, 36th teeth.
Rheumatic valvulopathy. Condition
associated with mitral valve prosthesis
(2005)‖.
Due to absence of monitoring over the
anticoagulant therapy and presence of the
major risk both hemorrhagic and
thromboembolic, venous blood was taken
at admission to assess the indices of
coagulogram. The following results were
obtained: prothrombin index = 93%;
fibrinogen = 2,4 g/l; TTPA = 37 sec.;
thrombin time = 24 sec.; ethanol test was
„negative‖; INR = 1,10. While assessing
respective indices it was observed the
increase of prothrombin index (93%) and
decrease of INR values (1.10) below the
therapeutic limits. This suggested
existence of the major risk of occurrence
of the thromboembolic events. This served
as an indication for increase of
thrombostop dose from 2 mg/day to 3
mg/day under a control in dynamics of
INR.
The results of paraclinical analyses
(general blood analysis) urine analysis,
biochemical blood analysis) were within
the limits of normal values. On November
19, 2008, at the INR level of 1.14, the
extraction of the 35th, 36th teeth roots was
carried out. Immediately the alveoli of the
extracted teeth filled post-extractionally
with blood which flowed on the bottom of
the vestibular and lingual sac. Bleeding
lasted for 30-40 sec. Its intensity was
insignificant. The formation of the blood
clot was post-extractionally assessed in the
3rd
minute after transformation of the
blood from liquid state into gel-like state
(Picture 1.A). At the same time, it was
observed that the newly formed clot was
homogenous. Being at the level of the
alveolus, the clot had a contact with the
alveolus edges. In the 10th post-
extractional minute there was observed the
appearance of a light-red gingival line at
the periphery compared with the dark-red
colour from the clot center. Thus, it was
stated that a scratchy clot had appeared.
This coincided with its „migration‖ under
the alveolar edge (Picture 1.B). Post-
operatory period lasted without any
peculiarities: at inspection of the post-
extractional wound, which was carried out
12 hours after the extraction, it was
determined the presence of retracted blood
clots (Picture 1.C). Restoration of the
gingival integrity was practically recorded
36 hours after the extraction (Picture 1.D).

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
46
Picture 1. Blood clot formation and its appearance after the extraction of 35th, 36th teeth
roots in patient C.V. receiving oral anticoagulant therapy (Thrombostop).
A – Blood clot formation in the 3rd
post-extractional minute; B – Appearance of the scratchy
clot and its position under the alveolar edge; C – Appearance of the post-extractional
wound after 12 hours of extraction; D - Appearance of the post-extractional wound after 36
hours of extraction.
On November 21, 2008, after the
increase of thrombostop dose, it was stated
the restoration of INR within the
therapeutic range limits (2,84). Thus, the
patient was not subjected to risk of
occurrence of the thromboembolic
complications. The patient stated that his
general weaknes had disappeared. Perhaps,
it was due to improvement of rheological
properties of the blood after INR
adjustment to therapeutic values. On
November 22, 2008 the patient was
discharged, his general condition being
satisfactory.
From those mentioned above we can
conclude that when patients receiving oral
anticoagulant therapy have INR values
below the therapeutic range limits, the
dose of these drugs can and must be
increased (including pre-extractionally) to
prevent the thromboembolic
complications. Moreover, after assessment
of the post-extractional dental haemostasis,
the patient was found to have blood
hypercoagulation which was evaluated by:
A B
C D

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
47
short bleeding duration of the post-
extractional dental wound (30-40 seconds)
opposite the mean bleeding duration in
patients with an uncompromised
haemostatic system [17] (1,2 ± 0,2
minutes);
early formation of the blood clot
(in the 3rd
post-extractional minute)
opposite the mean time of the blood clot
formation in patients with an
uncompromised haemostatic system [17]
(in the 5.2 ± 0,1 minutes).
After dental extractions (34)
performed on 26 patients under
antithrombotic therapy it was stated the
absence of BADE in the majority (18) of
cases (69,2 ± 9,1%), Of those 18 patients,
14 (77.8%) received oral anticoagulants
(thrombostop – 9 (64,3%), warfarin – 5
(35,7%)) and 4 patients (22,2%) received
antiplatelet therapy (aspirin). INR values
estimated on the day of dental extractions
in patients receiving oral anticoagulants
without BADE were within the following
limits: INR = 2,0-2,6 was established in 6
(42,9%) cases, while INR < 1,9 – in 8
(57,1%) patients.
At the same time, it was observed
absence of this contact in 30,8 ± 10,2%
patients (8), in whom bleeding continued
after 15-20 minutes. This condition was
appreciated as BADE. This was a
cappilary bleeding. Its intensity was
insignificant. Bleeding continued from the
soft tissues through the space between the
clot and the alveolus edge. Of 8 patients
with BADE, 6(75,0%) received oral
anticoagulant therapy (thrombostop – 4
(66,7%), warfarin –2 (33,3%); one patient
(12,5%) received antiplatelet therapy
(aspirin) and one patient (12,5%) –
received both oral anticoagulant
(thrombostop) and antiplatelet (aspirin)
therapy. In patients with BADE receiving
thrombostop and warfarin (7) INR values
assessed on the day of the dental
extractions were within the following
limits: INR = 2,0-2,4 was established in 5
(71,4%) cases, while INR < 1,9 – in 2
(28.6%) patients. Although it is considered
that blod coagulation increases in patients
who are below the therapeutic range limits
(INR < 2,0) [9], the analysis of the
obtained data has proved that in 2 patients
(28,6%) BADE appeared at INR values of
1,8 and 1,4. This phenomenon can be
explained by the fact that in one clinical
case apprearance of BADE was
conditioned by the simultaneous presence
in the patient of thrombocytopenia
(thrombocyte count was 84,0.10
9/l). In
another clinical case it has been
conditioned by associated antithrombotic
therapy (thrombostop and aspirin) which
significantly increases the risk of
appearance of BADE [18].
Thus the presented data show that
hemorrhagic accidents in patients
receiving oral anticoagulant therapy can
occur at any INR value. The frequency of
this post-operatory complication in
patients under antithrombotic therapy
subjected to dental extractions without
cancellation of these drugs was 30,8 ±
10,2%. It is necesary to mention that
BADE which occured at the level of INR
values <2.4 was a cappilary bleeding. Its
intensity was insignificant. According to
some studies, these hemorrhages are easily
kept under control through local
applications of human thrombin and
aminocaproic acid of 5% [19]. At the same

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
48
time, it is necessary to mention that
BADE occuring in patients who have had
an overdosage of oral anticoagulants are
extremely severe and can jeopardize
people's health [9]. To prevent the severe
hemorrhagic accidents in this group of
patients, our study has proved that
overdosage with indirect anticoagulants
can be pre-extractionally assessed through
determination of both INR values and time
of the blood coagulation according to Lee-
White. Some authors mention that the
optimal value of INR for performing
dental extractions is 2.5, because this limit
reduces the risk of occurrence of both
hemorrhagic accidents and
thromboembolic events [20]. Despite this
we consider that dental extractions can be
successfully performed at the level of
individual INR values recommended to the
patients by the general physician. At the
same time we are aware of the local
haemostatic measures that should be
undertaken and are necessary in order to
control the bleeding.
Taking into consideration the increase
of frequency and high lethality of
thromboembolic complications, we think
that the decision of modifying the
anticoagulant therapy should be
deliberated after a careful consideration of
risk and benefit. In this respect, when INR
value is higher than 4.0, the dental
extraction will be delayed and the dose of
the anticoagulant will be reduced.
Conversely, when INR values are below
the therapeutic range limits, the dose of
these drugs should be increased (including
pre-extractionally) to prevent
thromboembolic complications.
CONCLUSIONS
1. Assessment of INR is a compulsory
method of pre-extractional evaluation of
the effect of oral anticoagulants.
2. Patients under unmonitored
anticoagulant therapy are exposed to an
increased risk both hemorrhagic and
thromboembolic.
3. Frequency of BADE in patients
receiving antithrombotic therapy who
undergo dental extraction without
cancellation of these drugs constitutes 30,8
± 10,2%. These hemorrhages, at INR
values < 2,4, have an insignificant
intensity.
4. As a prophylactic measure in
prevention of severe thromboembolic and
hemorrhagic accidents the dose of the
anticoagulant will be modified depending
on INR.
5. Dental extraction in these patients
can be performed without interruption of
the anticoagulant therapy by maintaining
INR within the limits of individual
therapeutic values.
REFERENCES 1. Cojocaru V., Dereglări hemostazice în stări patologice critice, Chişinău, Art-Grup Brivet, 2006.
2. Grosu A., Profilaxia accidentului vascular cerebral ischemic şi a altor complicaţii tromboembolice în
fibrilaţia atrială, Buletinul Academiei de Ştiinţe a Moldovei, Ştiinţe medicale, vol. 1, no. 5, p. 189-202,
2006.
3. Antonescu D., Gherasim L., Tulbure D., Jurcuţ R., Ghid de prevenţie a tromboembolismului venos,
Medicina Internă, vol. 5, no. 5, p. 23-39, 2007.
4. Gohlke-Bärwolf C., Zentrum H., Krozingen B., Anticoagulation in valvar heart disease: new aspects and
management during non-cardiac surgery, Heart, vol. 84, p. 567-572, 2000.
5. Ciubotaru A., Manolache Gh., Chişlaru L., Istoricul şi prezentul chirurgiei cardiovasculare în Republica
Moldova, Buletinul Academiei de Ştiinţe a Moldovei, Ştiinţe medicale, vol. 5, no. 9, p. 8-13, 2006.

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
49
6. British Society of Haematology, British committee for standards in haematology guidelines on oral
anticoagulation, 3rd ed, Br J Haematol, vol. 101, p. 374-387, 1998.
7. Bucur A., Cioacă R., Urgenţe şi afecţiuni medicale în cabinetul stomatologic, note de curs, Bucureşti,
Editura Etna, p. 23, 2004.
8. Hotineanu V., Jovmir V., Ciubotaru A., Chirurgie, curs selectiv, Chişinău, Medicina, p. 214, 2008.
9. Момот А.П., Патология гемостаза, Принципы и алгоритмы клинико-лабораторной диагностики,
Санкт-Петербург, ФормаТ, с. 101-107, 2006.
10. Dunn A.S., Turpie A.G., Perioperative management of patients receiving oral anticoagulants, a systematic
review, Ar Intern Med, vol. 163, no. 8, p. 901-908, 2003.
11. Ferrieri G.B., et al., Oral surgery in patients on anticoagulant treatment without therapy interruption, J
Oral Maxillofac Surg, vol. 65, no. 6, p. 1149-1154, 2007.
12. Scher K.S., Unplanned reoperation for bleeding, Am Surg, vol. 62, no. 1, p. 52-55, 1996.
13. Hirsh J., Raschke R., Heparin and low-molecular-weight heparin, the Seventh ACCP Conference on
Antithrombotic and Thrombolytic Therapy, Chest, vol. 126, suppl. 3, p. 188S-203S, 2004.
14. Napeñas J.J. The frequency of bleeding complications after invasive dental treatment in patients receiving
single and dual antiplatelet therapy, J Am Dent Assoc, vol. 140, no. 6, p. 690-695, 2009.
15. Ghicavîi V., Sârbu S., Bacinschi N., Şcerbatiuc D. Farmacoterapia afecţiunilor stomatologice, ediţia a II-
a, revăzută şi completată, Chişinău, Tipar, p. 161-162, 2002.
16. Owens C.D., Belkin M., Thrombosis and coagulation: operative management of the anticoagulated
patient, Surg Clin North Am, vol. 85, no. 6, p. 1179-1189, 2005.
17. Zănoagă O., Evaluarea hemostazei postextracţionale dentare la pacienţii cu un sistem hemostatic
necompromis, Curierul medical, vol. 4, no. 310, p. 12-14, 2009.
18. Flaker G.C., et al., Risks and benefits of combining aspirin with anticoagulant therapy in patients with
atrial fibrillation: an exploratory analysis of stroke prevention using an oral thrombin inhibitor in atrial
fibrillation (SPORTIF) trials, Am Heart J., vol. 152, no. 5, p. 967-973, 2006.
19. Zănoagă O., Topalo V., Sîrbu D., Suharschi I., Procopenco O., Conduita în extracţia dentară la pacienţii
aflaţi sub medicaţie anticoagulantă orală, Revista medico-chirurgicală a Societăţii de Medici şi Naturalişti
din Iaşi, vol. 113, no. 2, supliment no. 2, p. 75-79, 2009.
20. Pototski M., Amenábar J.M., Dental management of patients receiving anticoagulation or antiplatelet
treatment, J Oral Sci, vol. 49, no. 4, p. 253-258, 2007.

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
50
ASSESSMENT OF ORO-DENTAL HEALTH STATUS USING
THE CAO AND EGOHID INDEXES AT THE YOUNG
PEOPLE Ioan Dănilă, Iulia Saveanu, Carina Balcos
Faculty of Dentistry, ―Gr.T.Popa‖ University of Medicine and Pharmacy Iasi
Abstract: CAO and CAOS epidemiological indices provide significant information for an overview assessment
of dental health but can not make a nuanced type of carious lesions and involvement of the need for treatment.
EGOHID system of clinical assessment and restoration of carious lesions provide evidence on lesion topography
guided us on the degree of dental damage in motivating action supporting our dental health. The purpose of this
study was to evaluate the comparative in terms of dental health indices CAO, CAOS and EGOHID system.
Materials and methods: The study was conducted on a sample of 122 subjects with a mean age 23.53 years in
which data were collected on the type of carious lesion and the type of restoration. Data were collected by
clinical examination and observation files recorded according to codes. All patients in the study were informed
verbally about the purpose of the study noting their consent. Statistical data processing was performed with
SPSS 14.00 for Windows fixing the threshold of statistical significance of p ≤ 0.05. Results and discussion:
Comparative analysis of two systems of assessment revealed that significant differences p ≤ 0.05 for the system
of assessment of dental status in the system component EGOHID carious lesions, lesion assessment is
accomplished underestimated component CS of CAOS index showing an average of 4.42 (± 4.132) compared
with EGOHID-C is the index of the cavity showing an average of 10.38 (± 7.484). Conclusion: Data obtained
through evaluation of dental caries is higher, providing a concrete image of the orientation dentistry, early
diagnosis of dental caries, treatment and hence the technicallity and restorative treatments.
Key words: CAO, EGOHID, dental status.
INTRODUCTION
World Health Organization has
formulated a definition that dental caries,
prevention and prevention methods shall
constitute an integral part of restorative
treatment, clinical caries as an
evolutionary stage that grows from a
microscopic lesion that can not be
diagnosed with certainty in current clinical
means [1,2]. Switching from an early
lesion, non-cavitary, cavitary lesion to
reverse, irreversible, develops slowly, by
disrupting the balance between
demineralization and remineralization
processes in favor of demineralization [3].
Therefore diagnosis dental decay,
apparently simple, it seems practically a
difficult decision, therefore, recommended
the combination of clinical examination
with additional tests. However the
assessment of epidemiological indicators
is mostly based on clinical examinations
which induce more bias in the assessment
of early carious lesions that may be an
overestimation or underestimation of the
presence of injury for the purposes of
giving or another function code the
examiner. Therefore, refinement of codes
carious lesion should be a mandatory step
since and conduct therapeutic purposes is
different in primary, secundary and tertiary
prevention measures. CAO and CAOS
epidemiological indices provide significant
information for an overview assessment of
dental health but can not achieve a
nuanced type of carious lesions and
involvement of the need for treatment. Nor
shall a targeted, individualized treatment
strategy on prevention schemes of primary
or secondary prevention of treatment
patterns.
As the evaluation indices CAO index
of caries in all those early carious lesions
showing noncavitation remineralization
potential and non-invasive treatment we
intend to achieve a differentiated based
monitoring injury from minor changes in
tooth surfaces following with obvious
changes of enamel structure, with loss of

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
51
substance or not located in dental enamel
or dentin.
EGOHID system of clinical
assessment and restoration of carious
lesions was designed to support the
collection of global oral health indicators
(EGOHID - European Global Oral Health
Index Development). This system provides
evidence on lesion topography guided us
on the degree of dental damage and costs
arising from default on it. Data provided
by EGOHID system contribute to a
strategy of primary prevention and
secondary motivating with local, national
and European decision makers [4].
EGOHID is a comprehensive
evaluation of oral health status, which
consists of several sections, namely:
identification data and background
information of subjects; Questionnaire on
dental health, dental fluorosis
questionnaires, survey on periodontal
health, determination of the presence of
oral cancer, orthodontic treatment,
prosthetic treatment.
In this study we considered part of the
questionnaire on dental health codes for
attributed type of restoration present, the
type of carious lesions developed. Codes
are assigned according to Table 1.
Table 1.
Codes for restoration and sealing Codes for tooth decay
0= without sealing and restoration 0= surface without lesion
1= partial sealing 1= slight modification of the surface, the inspection
2= sealing 2= obvious change of surface
3 = discoloration restoration 3= cavity in the enamel, dentin without evidence
4 = amalgam restoration 4= damage to the enamel-dentin junction
5 = steel crown 5= dentin cavity
6= crown , facet ceramics, gold or composite 6= extended cavity dentin
7= restoration fractured or missing
8= temporary restoration
Missing teeth
97 = the extracted teeth cause tooth decay
98 = teeth absent from other causes
99= teeth that have erupted
P = implant
MATERIAL AND METHOD
In designing and running clinical trials
have formulated the following hypotheses:
the null hypothesis was that there is no
difference between the results of dental
health evaluation by epidemiologists
indices CAO, CAOS and EGOHID
system, testable hypothesis tested was that
the systems differ them, this translated by
statistically significant differences
obtained from analysis codes on the
questionnaire on dental health.
Patient selection was done among
students of III, Faculty of Dentistry, UMF
―Gr.T.Popa‖ Iasi. Following clinical
examination were selected a number of
122 subjects with a mean age of 23.53
years, 45 male and 77 female.
Inclusion criteria of patients in the
study followed the patients: to provide
carious lesions and restorative treatment to
highlight the value index and filling
cavities. The exclusion criteria were
followed: patients who had no carious
lesions or dental restorations.

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
52
Following clinical examination data
were collected on the type of carious
lesion and the type of restoration, data
were collected through clinical
examination and preparation of charts. The
study was clinical type.
All patients in the study were
informed verbally about the purpose of the
study noting the consent form. The
examination was performed in the office
of dispensary patients nr.1, outpatient
dentistry. Patients were placed in the
database according to certain codes.
Statistical data processing was done with
software for Windows SPSS14.00 settling
a threshold of statistical significance of p ≤
0.05.
RESULTS AND DISCUSSIONS
Assessment component of the system
decay index EGOHID namely EGOHID-C
was performed on a tooth surface because
can exist at different codes of carious
lesions.
The results of comparative analysis of
two systems of assessment revealed that
the differences statistically significant p ≤
0.05 (Table 4) for dental status assessment
system through the component EGOHID
carious lesions, lesion assessment can be
done in CS underestimated component of
the index showing an average of 4.42
CAOS (± 4.132) (Fig. 1, Table 2)
compared with EGOHID-C (the decay
index) an average 10,38 (±7,484) (Table
3).
Fig. 1. CS component analysis (mean scores obtained).
20151050
CS
40
30
20
10
0
Fre
qu
en
cy
Mean =4.42Std. Dev. =4.132
N =122
CS

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
53
Table 2. Analysis of CaO and descriptive indices CAOS
N Minimum Maximum Mean Std. Deviation
CAO 122 1 29 10,11 5,507
CD 122 0 20 3,76 3,507
AD 122 0 9 ,97 1,443
OD 121 0 19 5,49 3,608
CAOs 122 2 62 17,46 11,825
CS 122 0 20 4,42 4,132
AS 122 0 45 4,85 7,110
OS 122 0 40 8,37 7,039
Valid N (listwise) 121
Differences fall mainly in providing
code 01 which represents a slight
modification of the surface with an
average of 3.72 (± 4.005) and the award
code 02 which represents a clear change of
the surface with an average of 2.89 (±
2.785).
Component analysis OD 5.49 (±
3.608) (Table 2) compared with
EGOHID-R 5.48 (± 3.793) (Table 3)
reveals no significant differences
statistically however there is a difference
in assessment of present sealing part code
10 with an average of 0.07 (± 0.421) and
sealing all present, that code 20 with an
average of 0.24 (± 0.882) (Table 3).
Table 3. Descriptive statistical analysis of system components EGOHID
N Minimum Maximum Mean Std. Deviation
EGOHID-C 122 0 37 10,38 7,484
EGOHID-R 122 0 17 5,48 3,793
cod 01 122 0 23 3,72 4,005
cod 02 122 0 18 2,89 2,785
cod 03 122 0 13 2,39 2,671
cod 04 122 0 11 ,70 1,520
cod 05 122 0 10 ,45 1,234
cod 06 122 0 6 ,23 ,758
cod 10 122 0 4 ,07 ,421
cod 20 122 0 6 ,24 ,882
cod 30 122 0 12 4,24 3,330
cod 40 122 0 10 ,57 1,548
cod 50 122 0 5 ,07 ,477
cod 60 122 0 6 ,18 ,693
cod 70 122 0 3 ,20 ,492
cod 80 122 0 3 ,13 ,444
cod 99 122 0 4 ,48 ,938
cod98 122 ,00 3,00 ,2705 ,76100
Valid N (listwise) 122
EGOHID-C -carious lesions,
EGOHID- R-dental restorations 01 - now partly sealed, code 02 - sealed, code 03 - filling, code 04
- amalgam fillings, code 05 - crown, ceramic side, code 07 - fractured fillings or missing, code 08 -
filling temporary, code 10 - slight modification of the surface, the inspection, code 20 - obvious
change of surface, code 30 -cavity in the enamel, without dentin evidence, code 40 - lesion-enamel-
dentin junction, code 50 - dentin cavity, code 60 - extended cavity dentin
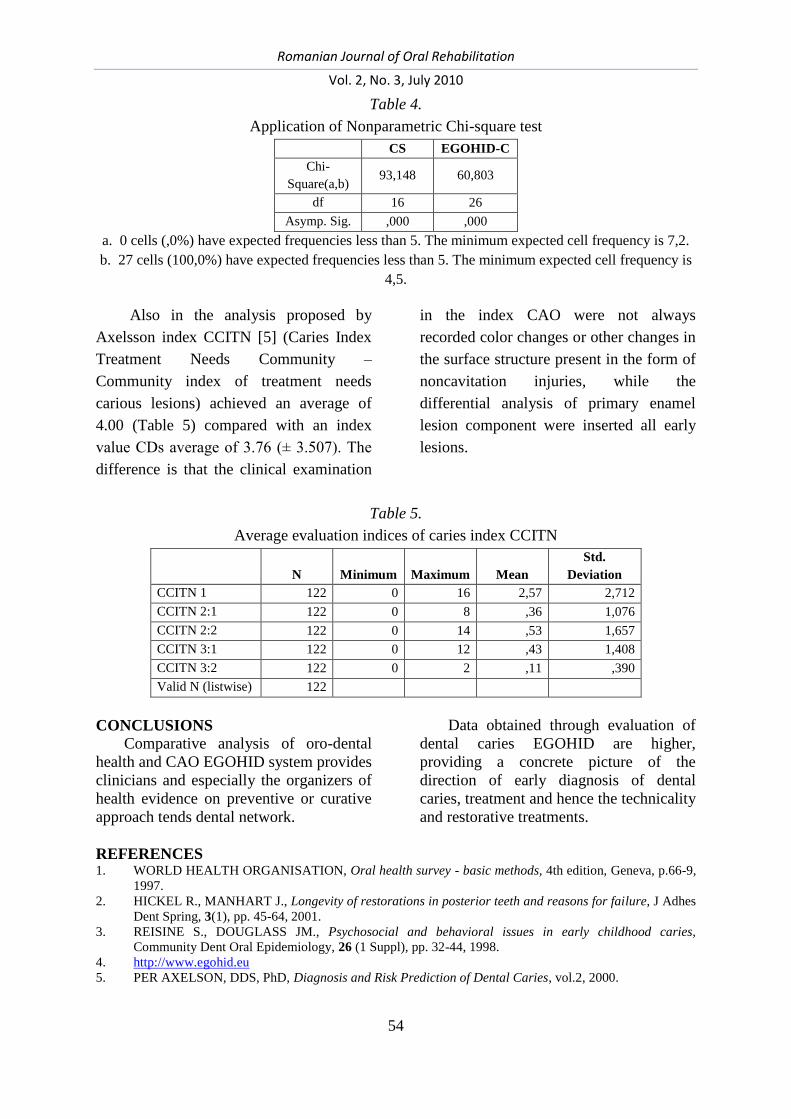
Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
54
Table 4.
Application of Nonparametric Chi-square test
CS EGOHID-C
Chi-
Square(a,b) 93,148 60,803
df 16 26
Asymp. Sig. ,000 ,000
a. 0 cells (,0%) have expected frequencies less than 5. The minimum expected cell frequency is 7,2.
b. 27 cells (100,0%) have expected frequencies less than 5. The minimum expected cell frequency is
4,5.
Also in the analysis proposed by
Axelsson index CCITN [5] (Caries Index
Treatment Needs Community –
Community index of treatment needs
carious lesions) achieved an average of
4.00 (Table 5) compared with an index
value CDs average of 3.76 (± 3.507). The
difference is that the clinical examination
in the index CAO were not always
recorded color changes or other changes in
the surface structure present in the form of
noncavitation injuries, while the
differential analysis of primary enamel
lesion component were inserted all early
lesions.
Table 5.
Average evaluation indices of caries index CCITN
N Minimum Maximum Mean
Std.
Deviation
CCITN 1 122 0 16 2,57 2,712
CCITN 2:1 122 0 8 ,36 1,076
CCITN 2:2 122 0 14 ,53 1,657
CCITN 3:1 122 0 12 ,43 1,408
CCITN 3:2 122 0 2 ,11 ,390
Valid N (listwise) 122
CONCLUSIONS
Comparative analysis of oro-dental
health and CAO EGOHID system provides
clinicians and especially the organizers of
health evidence on preventive or curative
approach tends dental network.
Data obtained through evaluation of
dental caries EGOHID are higher,
providing a concrete picture of the
direction of early diagnosis of dental
caries, treatment and hence the technicality
and restorative treatments.
REFERENCES 1. WORLD HEALTH ORGANISATION, Oral health survey - basic methods, 4th edition, Geneva, p.66-9,
1997.
2. HICKEL R., MANHART J., Longevity of restorations in posterior teeth and reasons for failure, J Adhes
Dent Spring, 3(1), pp. 45-64, 2001.
3. REISINE S., DOUGLASS JM., Psychosocial and behavioral issues in early childhood caries,
Community Dent Oral Epidemiology, 26 (1 Suppl), pp. 32-44, 1998.
4. http://www.egohid.eu
5. PER AXELSON, DDS, PhD, Diagnosis and Risk Prediction of Dental Caries, vol.2, 2000.

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
55
THE DAY OF PROPHYLAXY, JUNE, 9, 2010
The Day of Moldavian Prophylaxy in Dental Medicine, organized by the Romanian
Dental Association for Education, The Faculty of Dental Medicine, UMF, Gr. T. Popa, Iasi,
in partnership with companies dealing with prophylaxy products used in preventing oral
pathology and its complications in Moldavia focuses on the topic ―The Evaluation of the Oral
Status of the population from rural areas and monasticism‖. There is to be assessed the
population from villages in the Iasi county with no residing dentist –Popesti, Braesti, Dagita,
Dobrovat, Gropnita and as well as from those having a dentist doctor-Rediu, Miroslava. An
important role in such events s held by the local authorities-both from the villages involved in
the study and from Iasi, as ell as by the Metropolitan Bishopric of Moldavia and Bucovina.
The event will take place on June, 9, 2010 and it focuses on two main aspects: the former
is the Symposium dedicated to oral pathology prevention methods where outstanding
specialists in the field are expected to hold conferences and representatives of the companies
promoting prophylaxy products in Moldavia are invited to participate. The Symposium is
scheduled for 9.00AM in the G E Palade auditorium of The University of Medicine and
Pharmacy Gr. T. Popa, Iasi. The Latter manifestation is the Prophylaxy Caravan (9.00am-
9.00pm) evaluating and distributing free samples of prophylaxy products in the county of Iasi
(The Theatre Park, V Alecsandri). The other places for evaluation and product distribution
are in rural and monastic communities: Neamt, Agapia, Varatec, Secu, Sihastria. The
participant companies –Colgate, Glaxo, Johnson and Johnson, Oral B will deliver free
samples and informative brochures.
The participants will come in touch with prevention methods in oral pathology and the
new products on the market used in this respect, leading to an increase in their life quality.
Univ Prof Dr Norina Forna
Dean of the Faculty of Dental Medicine Iasi

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
56

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
57

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
58
Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
59

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
60

Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
61
Romanian Journal of Oral Rehabilitation
Vol. 2, No. 3, July 2010
62





























