Embed Size (px)
Citation preview
Roles of OT, PT, ST in the Long Term Acute Care Setting
By Juhi Gupta
Objectives
● Introduction to purpose of Long Term Acute Care (LTAC) facilities ● Introduction to rehabilitation team at LTAC● Roles of OT, PT, & ST● Discuss understanding of Skilled vs. Non-skilled services ● Determine importance of recommendations provided by OT/PT/ST to enhance
patients safety with mobility and ADLs.
What are Long Term Acute Care Facilities? ● Most patients who need immediate medical
attention are admitted to an “acute-care” hospital for an relatively short stay.
● However, some patients need longer hospital stay to receive an extensive medical attention due to more than one serious condition such as respiratory failure, heart conditions, kidney failure etc.
● Long Term Acute Care Hospital such as our facility are certified as acute-care hospitals, however, LTACs focus on patients who, on average, stay more than 25 days.
Rehabilitation Department at LTAC
“Rehabilitation services are for the recovery or improvement of function and when possible to restore function to previous level.”
Rehabilitation services personnel includes:
● Occupational therapist ○ Occupational therapy assistant
● Physical therapist ○ Physical therapy assistant
● Speech pathologist (speech therapist)● Rehabilitation aide
What does a therapist (OT/PT/ST) do?
● Performs initial evaluation when patient is admitted to LTAC● Device a Plan of Care
○ Establishes a rehabilitation diagnosis○ Individualized plan for each patient based on how he/she performs during evaluation/reassessments
○ Establishes a treatment program which includes specific interventions such as functional training, adaptive devices etc.
○ Establishes anticipated goals, expected outcomes, any predicted level of improvement■ Short term goals ■ Long term goals ■ Frequency, intensity & duration for care
○ Plan of care includes the anticipated discharge plans
Occupational Therapy
● “Occupational therapy plays an important role in facilitating early mobilization, restoring function, preventing further decline, and coordinating care including transition and discharge planning.”
● Occupational therapist provides a systematic process of client-centered evaluation, intervention and task modification to facilitate progress towards ADLs based goals such as dressing, eating, bathing, & grooming.
● Occupational therapist analyses patient’s prior level of function and their likelihood of resuming them after being discharged from the hospital.
Occupational Therapy
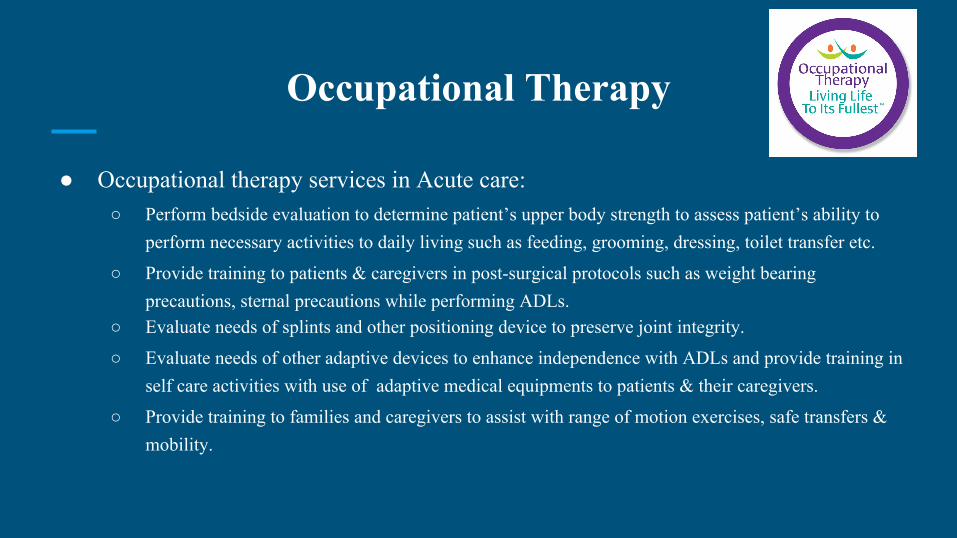
● Occupational therapy services in Acute care: ○ Perform bedside evaluation to determine patient’s upper body strength to assess patient’s ability to
perform necessary activities to daily living such as feeding, grooming, dressing, toilet transfer etc.
○ Provide training to patients & caregivers in post-surgical protocols such as weight bearing precautions, sternal precautions while performing ADLs.
○ Evaluate needs of splints and other positioning device to preserve joint integrity.
○ Evaluate needs of other adaptive devices to enhance independence with ADLs and provide training in self care activities with use of adaptive medical equipments to patients & their caregivers.
○ Provide training to families and caregivers to assist with range of motion exercises, safe transfers & mobility.

Occupational therapy
Adaptive equipment to perform ADLs
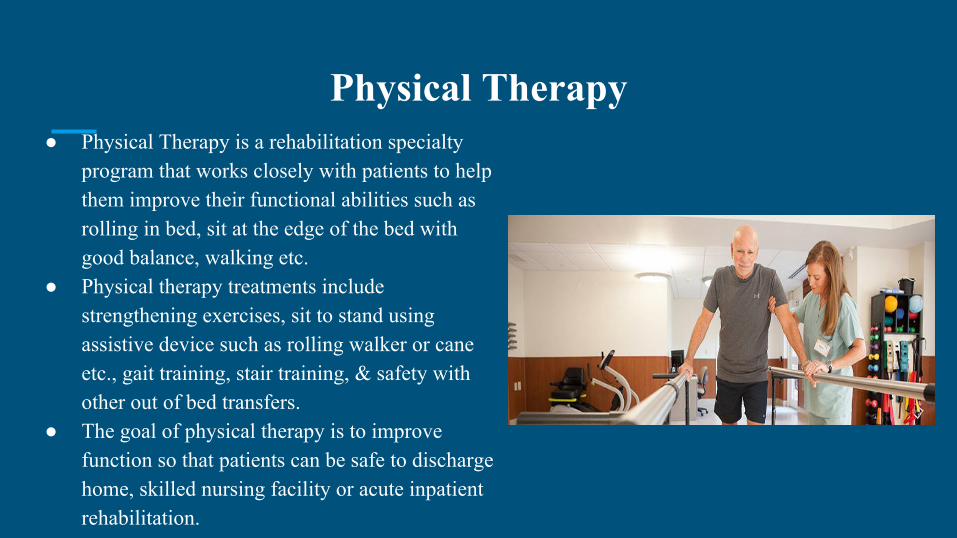
Physical Therapy ● Physical Therapy is a rehabilitation specialty
program that works closely with patients to help them improve their functional abilities such as rolling in bed, sit at the edge of the bed with good balance, walking etc.
● Physical therapy treatments include strengthening exercises, sit to stand using assistive device such as rolling walker or cane etc., gait training, stair training, & safety with other out of bed transfers.
● The goal of physical therapy is to improve function so that patients can be safe to discharge home, skilled nursing facility or acute inpatient rehabilitation.

Physical therapy
Speech therapy/ Speech-language pathologist
● Speech-language pathologist are referred to “speech therapists (ST)” provides a wide-range of services to patients in the Long Term Acute Care.
● Many patients in the LTAC have trach and/or are ventilator-dependent, ST performs bedside swallowing evaluation to determine swallowing impairments and possible risk of aspiration.
● STs works with patients on improving swallowing abilities, tolerance for voice prostheses (PMV value), and optimize patient’s communication.
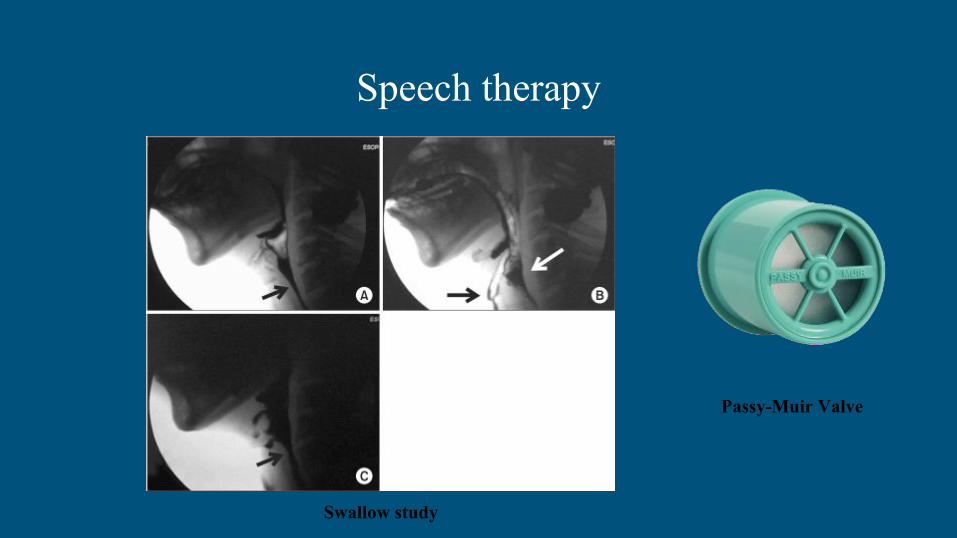
Passy-Muir Valve
Swallow study
Speech therapy
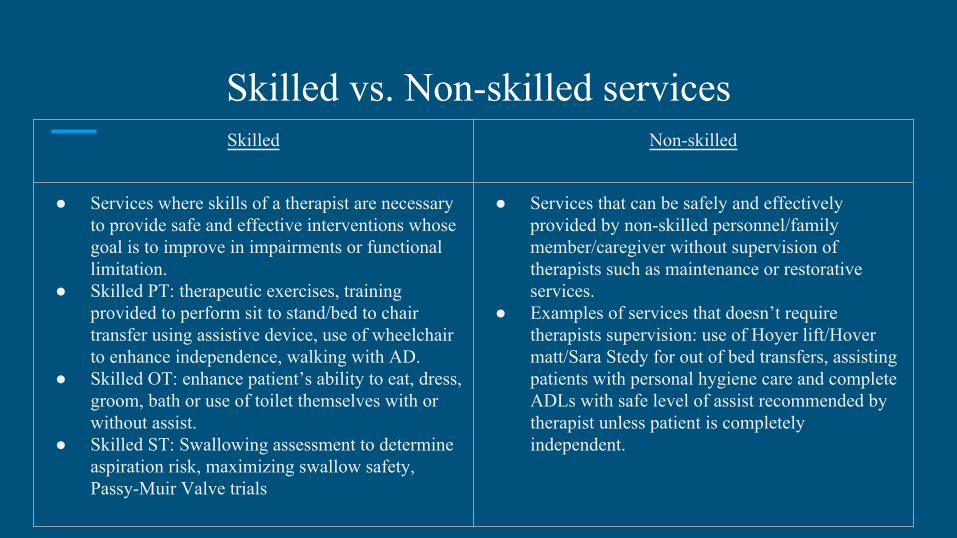
Skilled vs. Non-skilled servicesSkilled Non-skilled
● Services where skills of a therapist are necessary to provide safe and effective interventions whose goal is to improve in impairments or functional limitation.
● Skilled PT: therapeutic exercises, training provided to perform sit to stand/bed to chair transfer using assistive device, use of wheelchair to enhance independence, walking with AD.
● Skilled OT: enhance patient’s ability to eat, dress, groom, bath or use of toilet themselves with or without assist.
● Skilled ST: Swallowing assessment to determine aspiration risk, maximizing swallow safety, Passy-Muir Valve trials
● Services that can be safely and effectively provided by non-skilled personnel/family member/caregiver without supervision of therapists such as maintenance or restorative services.
● Examples of services that doesn’t require therapists supervision: use of Hoyer lift/Hover matt/Sara Stedy for out of bed transfers, assisting patients with personal hygiene care and complete ADLs with safe level of assist recommended by therapist unless patient is completely independent.
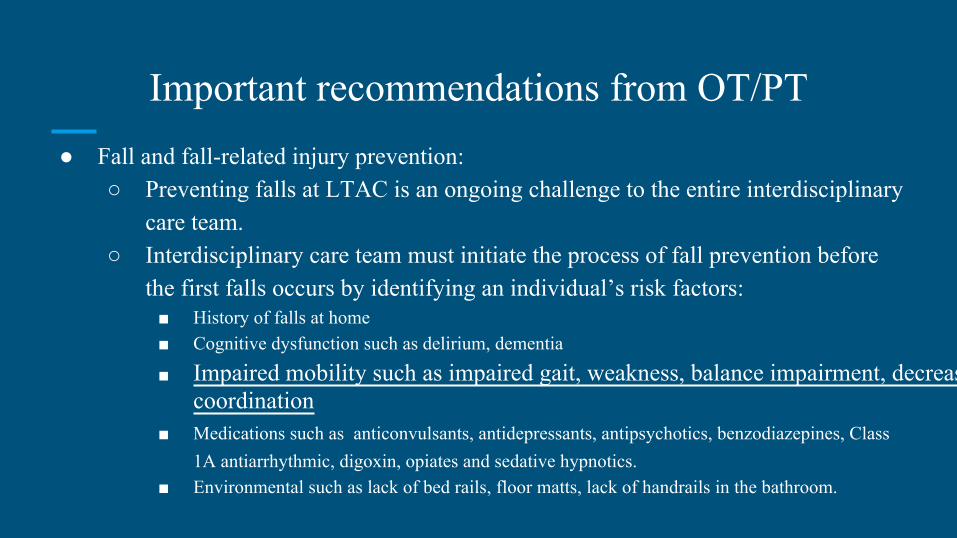
Important recommendations from OT/PT● Fall and fall-related injury prevention:
○ Preventing falls at LTAC is an ongoing challenge to the entire interdisciplinary care team.
○ Interdisciplinary care team must initiate the process of fall prevention before the first falls occurs by identifying an individual’s risk factors:■ History of falls at home■ Cognitive dysfunction such as delirium, dementia
■ Impaired mobility such as impaired gait, weakness, balance impairment, decreased coordination
■ Medications such as anticonvulsants, antidepressants, antipsychotics, benzodiazepines, Class 1A antiarrhythmic, digoxin, opiates and sedative hypnotics.
■ Environmental such as lack of bed rails, floor matts, lack of handrails in the bathroom.
Helping Hands for fall prevention
● Helping Hands is a fall prevention program initiated at the LTAC by the Rehab team members.
● Therapists evaluate patients (using all the points mentioned on the previous slide) and place a purple hand at the patient’s door and main patient board across from the nurses station.
● When the alarm light is on, it is crucial to remember that if the patient is assigned a purple helping hand then he/she is at high risk for falling, and need immediate attention from the staff to prevent fall.
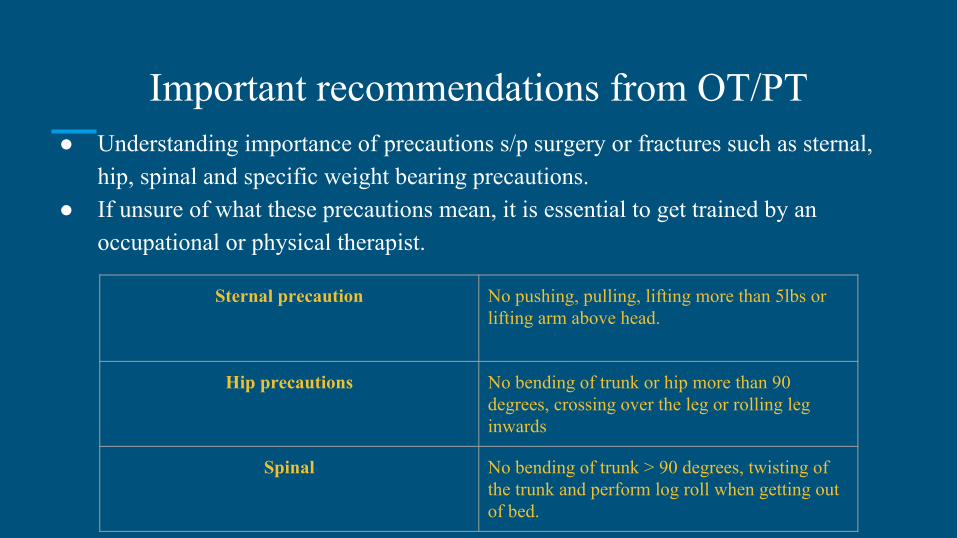
Important recommendations from OT/PT● Understanding importance of precautions s/p surgery or fractures such as sternal,
hip, spinal and specific weight bearing precautions. ● If unsure of what these precautions mean, it is essential to get trained by an
occupational or physical therapist.
Sternal precaution No pushing, pulling, lifting more than 5lbs or lifting arm above head.
Hip precautions No bending of trunk or hip more than 90 degrees, crossing over the leg or rolling leg inwards
Spinal No bending of trunk > 90 degrees, twisting of the trunk and perform log roll when getting out of bed.
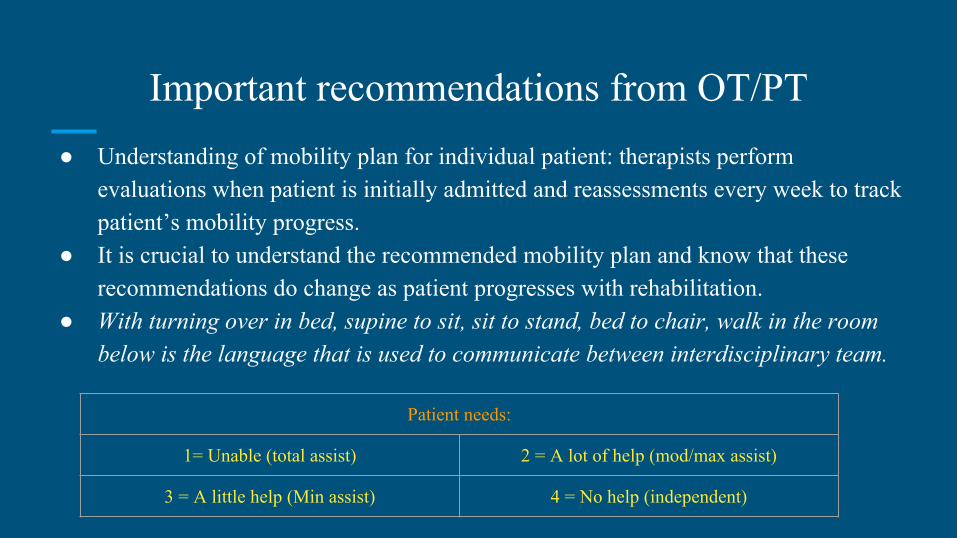
Important recommendations from OT/PT● Understanding of mobility plan for individual patient: therapists perform
evaluations when patient is initially admitted and reassessments every week to track patient’s mobility progress.
● It is crucial to understand the recommended mobility plan and know that these recommendations do change as patient progresses with rehabilitation.
● With turning over in bed, supine to sit, sit to stand, bed to chair, walk in the room below is the language that is used to communicate between interdisciplinary team.
Patient needs:
1= Unable (total assist) 2 = A lot of help (mod/max assist)
3 = A little help (Min assist) 4 = No help (independent)
Important recommendations from ST
● Understanding of patient’s nutritional and hydration needs as well as compensatory swallowing strategies is critical: speech therapist rely on the nursing/nursing tech’s observations in terms of dietary consistency tolerance, nutritional pattern changes in patients, and changes in aspiration risk behaviors.
● Communication between nursing staff and speech therapist is critical to track patient’s oral intake needs as their recommendations has an impact on nutrition and hydration which is beyond assessing aspiration risk.
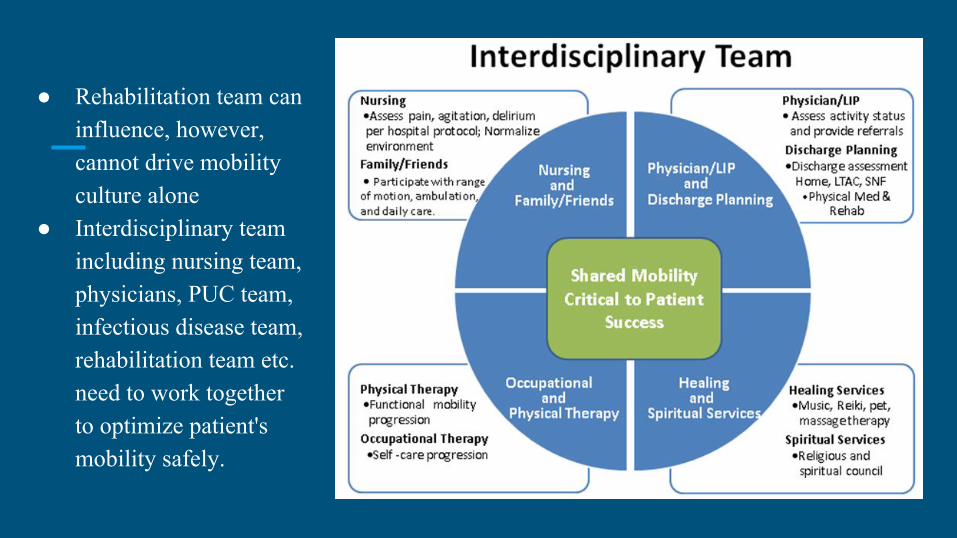
● Rehabilitation team can influence, however, cannot drive mobility culture alone
● Interdisciplinary team including nursing team, physicians, PUC team, infectious disease team, rehabilitation team etc. need to work together to optimize patient's mobility safely.
References
1) What are Long Term Care Hospitals? Centers for Medicare and Medicaid Services. https://www.medicare.gov/Pubs/pdf/11347.pdf. Revised on September, 2015. 2) Physical, Occupational, Speech Therapy Services. Centers for Medicare and Medicaid Services. https://www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/Medical-Review/Downloads/TherapyCapSlidesv10_09052012.pdf. Published on September, 2012. 3) Available at: http://www.aota.org/about-occupational-therapy/professionals/rdp/acutecare.aspx#sthash.Ozhef1Tm.dpuf. Accessed July 11, 2016. 4) Sponholz, M. The difference between Physical, Speech and Occupational Therapy. Aging Care. https://www.agingcare.com/Articles/geriatric-rehabilitation-services-what-is-physical-therapy-143151.htm. Accessed on July, 2016.5) Available at: http://www.lakewoodcare.org/Services/Physical-Therapy.aspx. Accessed July 11, 2016.
6) Available at: http://www.apta.org/PTCareers/RoleofaPT/. Accessed July 11, 2016.
7) Available at: http://www.asha.org/uploadedFiles/SLP-Medical-Review-Guidelines. Accessed July 11, 2016.
8) Available at: http://www.asha.org/slp/healthcare/LTAC/. Accessed July 11, 2016.
References
9) Available at: http://www.asha.org/Practice/reimbursement/medicare/Examples-of-Documentation-of-Skilled-and-Unskilled-Care-for-Medicare-Beneficiaries/. Accessed July 11, 2016.
10) Available at: http://www.ascseniorcare.com/physical-therapy-for-seniors/. Accessed July 11, 2016.
11) Available at: https://www.icsi.org/_asset/dcn15z/Falls-Interactive0412.pdf. Accessed July 11, 2016.
12) Hausdorff JM. Gait variability and fall risk in community-living older adults: A 1-year prospective study. Arch Phys Med Rehabil. 2001;82(8):1050–6.
13) Cahalin LP, Lapier TK, Shaw DK. Sternal Precautions: Is It Time for Change? Precautions versus Restrictions - A Review of Literature and Recommendations for Revision. Cardiopulm Phys Ther J. 2011;22(1):5-15.
14) Available at: http://www.dukehealth.org/repository/dukehealth/2010/10/28/09/36/28/6495/Posterior Hip Precautions. Accessed July 11, 2016.
15) Available at: https://ahc.aurorahealthcare.org/fywb/x15161.pdf. Accessed July 11, 2016.
16) Friedman M, Stilphen M. ESTABLISHING A CULTURE OF MOBILITY IN THE HOSPITAL SETTING. John Hopkins Medicine and Cleveland Clinic.
17) Available at: http://www.amyspeechlanguagetherapy.com/blognews/swallow-assessment-in-the-long-term-acute-care-hospital-more-than-just-an-evaluation-for-aspiration-guest-blog-by-eric-blicker. Accessed July 11, 2016.








![· Web viewsyndrome*[ot] OR motor development disorder*[ot] OR Stereotypic Movement Disorder*[ot] OR Body Rocking[ot] OR Body-Focused Repetitive Behavio*[ot] OR Head Banging[ot]](https://img.pdfslide.us/doc/110x75/5b0593dc7f8b9ad1768b921d/viewsyndromeot-or-motor-development-disorderot-or-stereotypic-movement-disorderot.jpg)