Embed Size (px)
Citation preview

Role of Three-Dimensional Echocardiography inManagement of Acquired Intracardiac Shunts
Tuncay Taskesen, M.D.,* Steven L. Goldberg, M.D.,† and Edward Allen Gill, M.D.†
*Harborview Medical Center, Seattle, Washington; and †Medicine/Cardiology, University of Washington,Seattle, Washington
Gerbode defect and sinus of Valsalva aneurysm fistula are congenital and acquired forms of intracardiacshunt. The increasing prevalence of invasive, recurrent cardiovascular procedures cause tissue damageand has led to more iatrogenic and acquired cases of predominantly congenital shunt over time. Wereport 2 cases of acquired intracardiac fistula precisely defined by Real time three-dimensional trans-esophageal echocardiography (3DTEE). The first case is a 70-year-old male with Gerbode defect aftersecond aortic valve replacement surgery due to prosthetic valve endocarditis and the other case is a 41-year-old male with sinus of Valsalva aneurysm fistula between aorta and right atrium post subclinicalinfective endocarditis. Advanced cardiac imaging techniques such as cardiac computerized tomogra-phy, MRI and Real time three-dimensional (3D) echocardiography help to precisely detect intracardiacfistula and provide detailed anatomic and physiologic information. The relatively low cost, lack of radia-tion exposure, portability and guiding characteristic make real time 3DTEE an imaging technique witharguably the most advantages. Surgical repair is the usual treatment for intracardiac shunt, and percuta-neous catheter-based closure is a less invasive alternative. (Echocardiography 2014;31:E250–E253)
Key words: Gerbode defect, ruptured sinus of valsalva aneurysm, real time three-dimensional echocar-diography
Case Presentation:Case 1:A 79-year-old male with a history of chronickidney failure, coronary artery disease, and aorticvalve replacement (AVR) presented with dyspneaand leg edema. The patient had an AVR and cor-onary bypass surgery for severe aortic stenosisand coronary artery disease 9 months prior topresentation (PTP). Three months PTP herequired reoperation because of prosthetic valveendocarditis and perivalvular regurgitation. Atthat time, he received a permanent pacemakerplacement, secondary to complete AV block. Inthe month PTP the patient began experiencingworsening shortness of breath and leg edema.On physical exam, he was found to have a new3/6 holosystolic murmur appreciable throughoutthe precordium. two-dimensional transesopha-geal echocardiography (2DTEE) using a Philips X-7 2-t transducer (Philips, Andover, MA, USA)revealed preserved LV ejection fraction (EF) of55%, normal bioprosthetic valve motion, withmild aortic perivalvular regurgitation, and addi-
tional flow signal between LV outflow tract andright atrium (RA) (Fig. 1; movie clip S1). Therewas also moderate mitral regurgitation, mildright ventricle (RV), and RA dilatation. Real timethree-dimensional transesophageal echocardiog-raphy (3DTEE) color full-volume images werecropped to demonstrate flow acceleration within
Figure 1. Two-dimensional color Doppler TEE. Mid-esopha-geal four-chamber view at 34° shows intracardiac shunt(arrow) between LV and RA in mid-systole. LA = left atrium;LV = left ventricle; RA = right atrium; RV = right ventricle.
Address for correspondence and reprint requests: TuncayTaskesen, M.D., Medicine/Cardiology, University of Washing-ton, 325 9th Ave, Seattle, Washington 98104. Fax: 206-744-5996;E-mail: [email protected]
E250
© 2014, Wiley Periodicals, Inc.DOI: 10.1111/echo.12682 Echocardiography

the left ventricular outflow tract and extension offlow across the atrioventricular septum superiorto the tricuspid septal leaflet into the right atrium(Fig. 2; movie clip S2). Despite a notableimprovement LV EF since his second surgery(30% to 55%) the patient’s functional capacityhad worsened. The patient was clearly a high risksurgical candidate because of his multiple comor-bidities and his redo AVR surgery. Based on thepatient’s clinical features and information gath-ered from detailed real time 3DTEE, the decisionwas made to perform a percutaneous interven-tion. Percutaneous closure was performed suc-cessfully with a vascular plug insertion withguidance by real time 3DTEE (movie clip S3).
Case 2:A 41-year-old male was referred to our clinic forevaluation after an unusual heart murmur wasdetected by his primary care physician. His onlycardiac symptom was mild exertional dyspnea.He had a history of alcohol and intravenous drugabuse. He had been previously treated with anti-biotics and surgical debridement for a methicillinresistant Staphylococcus aureus abscess on hisback 3 years PTP. Physical exam was notable forobesity and a machine-like continuous murmurheard over the left upper sternal border. 2DTEErevealed mildly dilated LV, RA, and RV; high-velocity continuous flow (3 m/sec) directed intothe RA from aortic root, and mild sclerosis onright coronary aortic leaflet (Fig. 3; movie clipsS4 and S5). Real time 3DTEE showed ananatomic and flow confirmed communicationbetween right coronary sinus of Valsalva to rightatrium and enlargement of heart chambers, pre-dominantly the right atrium and ventricle withincrease QP/QS ratio of 2.0 (Fig. 4; movie clipsS6 and S7). Right and left heart catheterization
confirmed the shunt between the right sinus ofValsalva and right atrium as well as the QP/QSratio; coronary arteries were normal. Based onanatomic and hemodynamic studies patient wasreferred for surgical closure. Right sinus of Val-salva aneurysm rupture was repaired successfullyby primary closure technique with autologouspericardium.
Discussion:Ruptured sinus of Valsalva aneurysm (RSVA) is arare cardiac anomaly (<0.1%) that can be con-genital or acquired. The congenital form is usu-ally associated with other congenital heartdefects. The associated defects include bicuspidaortic valve, ventricular septal defect or in thesetting of Marfan syndrome.1 Acquired formsof RSVA are caused by endocarditis, trauma, orconnective tissue disorders. In our case, thepatient was not known to have recurrent endo-carditis. However, the finding of isolated aorticvalve sclerosis on 2DTEE adjacent to the fistula
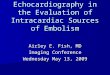
Figure 2. Real time 3D transesophageal echocardiographicmid-esophageal four-chamber image of intracardiac fistula(arrow) at upper interventricular septum between LV and RA.LV = left ventricle; RA = right atrium.
Figure 3. Two-dimensional color Doppler TEE. Midesopha-geal four-chamber view shows intracardiac shunt (arrow)toward the RA from left heart in midsystole. LA = Left atrium;LV = left ventricle; RA = right atrium; RV = right ventricle.
Figure 4. Real time 3D transesophageal color Dopplerimage showing shunt (arrow) between aortic root and RAabove aortic valve at sinus of Valsalva. AO = aorta; AV = aorticvalve; RA = right atrium.
E251
Three-Dimensional Echocardiography Intracardiac Shunt

tract (movie clip S5), as well as his history ofintravenous drug use, antibiotic therapy, thesurgical debridement for methicillin resistantStaphylococcus aureus abscess, and no concomi-tant congenital abnormality prompted us toconclude previous subclinical endocarditis wasthe likely etiology.2
Although the cardiac catheterization is consid-ered to be the accepted “standard” for diagnosisof RSVA, new cardiac imaging techniques such ascardiac computerized tomography (CT), MRI,and real time 3D echocardiography also provideexcellent anatomic and functional assessment.3
Real time 3DTEE is particularly helpful for delin-eating the relational anatomy and as a guide topercutaneous or surgical closure. Although thepatient had minimal symptoms, enlargement ofthe right heart chambers and increasedpulmonary blood flow (QP/QS > 1.5) indicated ahemodynamically important shunt. Surgicalrepair is the usual treatment of choice for RSVA,and percutaneous catheter-based closure is a lessinvasive alternative.4
Left ventricle to right atrium fistula is anuncommon (0.08%) congenital heart disorderand was first classified by Gerbode in 1958.5
Increasing invasive and recurrent cardiovascularprocedures have led to more iatrogenic andacquired cases of what used to be a predominantcongenital heart defect. Acquired causes aresecondary to trauma, infective endocarditis,myocardial infarction, aortic or mitral valve sur-gery, and percutaneous invasive procedures.6–8
Recurrent aortic valve surgery and prostheticvalve endocarditis cause destruction and erosionof supportive tissue leading to acquired fistulasand also conduction abnormality.
In the first case despite normal prostheticvalve function and improved LV EF after valvesurgery, it was noted that the patient symptom-atically was worse, with new appreciableholosystolic murmur and the right atrium andRV were enlarging. In symptomatic patients,surgical or percutaneous intervention is indi-cated. These defects have been closed success-fully with percutaneous approach for at leastthe last decade.9 To date there has been oneother report describing the diagnosis of Ger-bode defect by 3DTEE and a separate one thatutilized 3DTEE to aid percutaneous closure ofsuch a defect.10
Recurrent percutaneous or surgical proce-dures cause tissue damage that may increase riskof intracardiac fistula over time. Advancedcardiac imaging such as cardiac CT, MRI and Realtime 3D echocardiography help to preciselydetect intracardiac fistula and provide detailedanatomic and physiologic information. Therelatively low cost, lack of radiation exposure,
portability, and guiding characteristic make realtime 3DTEE an imaging technique with arguablythe most advantages.
References1. Takach TJ, Reul GJ, Duncan JM, et al: Sinus of Valsalva
aneurysm or fistula: Management and outcome. AnnThorac Surg 1999;68:1573–1577.
2. Palraj BR, Sohail MR: Appropriate use of echocardiogra-phy in managing Staphylococcus aureus bacteremia.Expert Rev Anti Infect Ther 2012;10:501–508.
3. Chandra S, Vijay SK, Dwivedi SK, et al: Delineation ofanatomy of the ruptured sinus of Valsalva with three-dimensional echocardiography: The advantage of theadded dimension. Echocardiography 2012;29:E148–E151.
4. Ott DA: Aneurysm of the sinus of Valsalva. Semin ThoracCardiovasc Surg Pediatr Card Surg Annu 2006;9:165–176.
5. Gerbode F, Hultgren H, Melrose D, et al: Syndrome ofleft ventricular- right atrial shunt: Successful surgicalrepair of defect in five cases with observation of bradycar-dia on closure. Ann Surg 1958;148:433–436.
6. Wasserman SM, Fann JI, Atwood JE, et al: Acquired leftventricular-right atrial communication: Gerbode-typedefect. Echocardiography 2002;19:67–72.
7. Dadkhah R, Friart A, Leclerc JL, et al: Uncommonacquired Gerbode defect (left ventricular to right atrialcommunication) following a tricuspid annuloplasty with-out concomitant mitral surgery. Eur J Echocardiogr2009;10:579–581.
8. Sharma AK, Chander R, Singh JP: AV nodal ablation-induced Gerbode defect (LV-RA Shunt). J Cardiovasc Elec-trophysiol 2011;22:1288–1289.
9. Sinisalo J, Sreeram N, Qureshi SA: Transcatheter closureof acquired left ventricle to right atrium shunts. CatheterCardiovasc Interv 2013;82:E809–E814.
10. Poulin F, Horlick EM, David T, et al: 3-Dimensional trans-esophageal echocardiography-guided closure of a Ger-bode shunt due to CorMatrix patches dehiscence. J AmColl Cardiol 2013;62:e5.
Supporting InformationAdditional Supporting Information may be foundin the online version of this article:
Movie Clip S1. Two-dimensional colorDoppler TEE. Mid-esophageal four-chamber viewshows intracardiac shunt between LV and RA inmid-systole.
Movie Clip S2. Real time 3D transesophagealechocardiographic mid-esophageal four-cham-ber image of intracardiac fistula at upper inter-ventricular septum between LV and RA andpermanent pacemaker lead in RV.
Movie Clip S3. Real time 3D transesophagealechocardiographic mid-esophageal four-cham-ber image after percutaneous closure was donewith vascular plug insertion of intracardiac fistulaat upper interventricular septum between LV andRA.
Movie Clip S4. Two-dimensional colorDoppler TEE. Mid-esophageal four-chamber viewshows intracardiac shunt between upper leftheart and right atrium in mid-systole with unclearorigin.
E252
Taskesen, Goldberg and Gill

Movie Clip S5. Two-dimensional colorDoppler TEE. Upper esophageal 40° short-axisview shows mild sclerosis of right coronary leafletand color Doppler jet flow show fistula betweenaorta and right atrium.
Movie Clip S6. Real time 3D transesophagealechocardiographic. Upper esophageal 40° short-
axis side view shows tissue defect and fistula ofsinus of Valsalva.
Movie Clip S7. Real time 3D transesophagealcolor Doppler image. Upper esophageal 40°short-axis side view shows shunt and color flowjet between aortic root and right atrium.
E253
Three-Dimensional Echocardiography Intracardiac Shunt