ROLE OF OPTICAL COHERENCE TOMOGRAPHY IN MANAGEMENT OF MACULAR
DISEASES.
A JOURNAL REVIEW ON
What is Optical coherence tomography ? Devised by Tanno et al in
1990 & Introduced by
Huang et al 1991, Optical coherence tomography (OCT) is a new,
non-contact, non-invasive, transpupillary technique for high
resolution, crosssectional imaging of tissue. It is analogous to :
computed tomography - which uses X rays, magnetic resonance - which
uses spin resonance, and, ultrasound B scan - which uses sound
waves. The operation of OCT is similar to that of ultrasound B-scan
imaging except it utilizes near infra-red light (830nm) waves
rather than acoustic sound waves. Because of this difference, the
axial resolution of OCT is as high as 10 m, compared with 150 m of
that of a conventional 10-MHz Bscan ultrasound.
Techniques of oct : TIME DOMAIN OCT (STRATUS OCT) has an
axial resolution of 10 microns and a transverse resolution of 20
microns. SPECTRAL/FOURIER DOMAIN OCT is capable of higher
resolutions of 57microns(axial) & 10-20 microns(transverse) and
acquires 512 vertical
scans. An experimental ultra high resolution OCT system has been
developed using Ti-laser that provides an improved axial resolution
of 2 to 3microns.
Scanning Tips1. 2. 3. 4. 5. Have a clear idea regarding the size
and location of the pathology of interest. Refer to other images of
the pathology, e.g. color photos and FA. Review past OCT exams and
repeat scan types used before. Dilate the eye well. The patient
must keep the forehead against the bar and the chin in the
chinrest, with teeth together. Use the marker on the headrest to
align the patient vertically. The outer canthus should be even
with
6.Use the two buttons near the joystick for freezing and saving
scans. This saves you from having to juggle the joystick and the
mouse.
7.Minimize patient fatigue by keeping scan time to a minimum.
Never scan an eye for more than 10 minutes (FDA regulation). 8.Keep
the cornea lubricated. Use artificial tears and have the patient
blink when you are not saving a scan pass. 9.Move the instrument on
the x and y axis
Principle :low coherence interferometry.
MICHELSON INTERFEROMETER
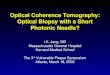
OCT Image of Normal Fovea
The OCT image above can be compared to what we know about
retinal anatomy from conventional microscopic sections. The
vitreous is the black space on the top of the image. We can
identify the fovea by the normal depression. The nerve fiber layer
(NFL) and the retinal pigment epithelium (RPE) are easily
identifiable. These layers are more highly reflective than the
other layers of the retina. This higher reflectivity is represented
by the "hotter" colors (red, yellow, orange, white) in the false
color representation of the OCT . The
Applications (a) Follow up of the clinical
course, understanding the pathogenesis of the disease, (b) For
assessing the response to medical/surgical/ laser therapy, (c) For
documentation and explaining the prognosis of a particular
disease.
RegionsFor purposes of analysis, the OCT image of the retina can
be subdivided vertically into four regions: the pre-retina the
epi-retina the intra-retina and the sub-retina
ProfilesOCT retinal morphology (form and structure) can be
subdivided into four "profiles": Each profile has it's own set of
deformations and anomalous structures.
1. 2. 3. 4.
pre-retinal profile overall retinal profile foveal profile
macular profile
The pre-retinal profile A normal pre-retinal profile is black
space, as
pictured below, because the normal vitreous space is
translucent, meaning it has minimal reflective properties. The
small, faint, bluish dots in the preretinal space is "noise". This
is an electronic aberration created by increasing the sensitivity
of the instrument to better visualize low reflective
structures.
Anomalous structures that have been observed in the preretinal
profile include the following: 1. pre-retinal membrane 2.
epi-retinal membrane 3. vitreo-retinal strands 4. vitreo-retinal
traction 5. pre-retinal neovascular membrane 6. pre-papillary
neovascular membrane A pre-retinal membrane with traction on the
fovea is pictured below.
The over-all retinal profileThe normal over-all retinal profile
has a slightly concave curvature that you would expect from
observing the surface of a globe. Abnormal profiles would include
exaggerated concavity and convexity. Retinal folds would also
result in an abnormal over-all profile.
The following OCT image demonstrates an abnormal convexity in
the over-all retinal profile. In this case, a pigment epithelial
detachment is causing the convexity.
The image below demonstrates an abnormal concavity to the
over-all retinal profile. Aside from the retinal detachment, notice
the underlying concave curvature of the retina, suggesting the long
eye of a significant myope.
The foveal profileThe normal foveal profile is a slight
depression in the surface of the retina, as pictured below.
Deformations that have been observed in the foveal profile
include the following: 1. macular pucker 2. macular pseudo-hole 3.
macular lamellar hole 4. macular cyst 5. macular hole, stage 1 (no
depression, cyst present) 6. macular hole, stage 2 (partial rupture
of retina, increased thickness) 7. macular hole, stage 3 (hole
extends to RPE, increased thickness, some fluid) 8. macular hole,
stage 4 (complete
macular cyst
The macular profileThe macular profile can, and often does,
include the fovea as it's center. Therefore, a common OCT scan
length of 6 mm would include 3 mm of the macula on each side of the
fovea.
Deformations that have been observed in the macular profile
include the following: 1. serous retinal detachment (RD) 2. serous
retinal pigment epithelial detachment (PED) 3. hemorrhagic pigment
epithelial detachment A serous PED is pictured below. We know that
it is a PED because the fluid (black space around the arrow) is
pushing up underneath the retinal pigment epithelium, identified by
the relatively highly reflective (red and orange) line (arrow).
Intra-retinal anomalies that have been identified in the macular
profile include: 1. choroidal neovascular membrane(I & II) 2.
diffuse intra-retinal edema 3. cystoid macular edema 4. drusen 5.
hard exudates 6. scar tissue 7. atrophic degeneration 8.
sub-retinal fibrosis
Cystoid Macular Edema
OCT is capable of detecting small, fluid-filled, cystic spaces
within the macula.
Central Serous Chorioretinopathy
Central serous chorioretinopathy is characterized by the
presence of fluid between the RPE and neurosensory retina.
Diabetic Retinopathy
Exudates appear as accumulation of dense material within the
neurosensory retina.
Artifacts Artifacts in the OCT scan are anomalies in the scan
that are
not accurate images of actual physical structures, but are
rather the result of an external agent or action. Notice the large
gap in the middle of the scan below. This is
an artifact caused by a blink during scan acquisition. This was
a high resolution scan, which takes about a second for the scan
pass, which is plenty of time to record a blink.
The scan below has waves in the retinal contour. These are not
retinal folds, but rather movement of the eye during the scan
pass.
Various studies have been published in different journals to
study ROLE OF OCT IN MANAGEMENT OF MACULAR DISEASES. A few of them
are mentioned below. 1. The following study was conducted for
Alberta Heritage Foundation for Medical Research (2003) Canada To
evaluate the evidence on the use of OCT to diagnose retinal disease
From 1995July/August 2003 Cystoid macular oedema diagnosis:1 study
compared OCT with FFA in patients with uveitis. 1 study compared
OCT with FFA + slit-lamp biomicroscopy in patients with diabetic
retinopathy.
Likelihood ratios indicate that OCT provided strong to
convincing diagnostic evidence for detecting cystoid macular oedema
and retinal blood vessel leakage. Resul ts: Accuracy for diagnosis
of macular oedemaOCT in patients with uveitis (FFA as reference
standard) (1 study): Sensitivity = 89%; specificity = 100% OCT in
patients with diabetic retinopathy (FFA as reference standard) (1
study): Foveal retinal thickness: Sensitivity = 81.5%; specificity
= 94.1% (FFA as reference standard) Average retinal thickness:
Sensitivity = 73.1%; specificity = 100% (FFA as reference standard)
Foveal retinal thickness: Sensitivity = 88.8%; specificity = 96.0%
(slit-lamp biomicroscopy as reference standard) Average retinal
thickness: Sensitivity = 80.2%; specificity = 100% (slit-lamp
biomicroscopy as reference standard)
2.Optical coherence tomography to detect and manage retinal
disease and glaucoma. Jaffe GJ, Caprioli J.2004,USA.PURPOSE: To
review basic principles of optical coherence tomography, and to
describe its use in the diagnosis and management of retinal
diseases and glaucoma. DESIGN: Perspective. METHODS: Literature
review. RESULTS: Optical coherence tomography is a noninvasive
imaging technique that has been used increasingly to diagnose and
manage a variety of retinal diseases and glaucoma. Optical
coherence tomography (OCT) is based on the principal of Michelson
interferometry. Interference patterns produced by low coherence
light reflected from retinal tissues and a reference mirror are
processed into an "A-scan" signal. Multiple A-scan signals are
aligned to produce a two-dimensional image that can be thought of
as a form of "in vivo histology." Optical coherence tomography has
been used to identify macular holes, to differentiate macular holes
from simulating lesions, to identify lamellar macular holes,
macular cysts, vitreomacular traction, subretinal fluid, pigment
epithelial detachment, and choroidal neovascularization. It can be
used to identify and quantify macular edema, and to measure retinal
thickness changes in response to therapy. Macular thickness
measurements determined by OCT correlate well with visual acuity
and with leakage observed by fluorescein angiography. Optical
coherence tomography is an accurate and reproducible method to
measure retinal nerve fiber layer thickness. Particularly, when
used in combination with other optic nerve
Optical coherence tomography equipment is expensive, and not all
insurance companies reimburse this procedure. Image quality is
dependent on operator technique & degraded in the presence
of
media opacity. Change analysis software for glaucoma
applications is not fully developed, and there is a scarcity of
age, gender, and racespecific normative data upon which to compare
eyes with retinal disease and glaucoma. In the next few years, it
is likely that the role of OCT as a method to diagnose and manage
retinal disease and glaucoma will be further defined, and many of
the current limitations will be overcome. CONCLUSIONS: Optical
coherence tomography is a useful imaging technique to diagnose and
manage a variety of retinal diseases and
Diabetic macular edema assessed with optical coherence
tomography and stereo fundus photography. Strm C, Sander B, Larsen
N, Larsen M, Lund-Andersen H. Department of Ophthalmology, Herlev
Hospital, University of Copenhagen, Copenhagen, Denmark. JAN 2002.
compare retinal thickening in PURPOSE: To
diabetic macular edema assessed subjectively by evaluation of
stereo fundus photographs with that assessed objectively by optical
coherence tomography (OCT). CONCLUSIONS: The degree of agreement
between subjectively and objectively assessed retinal thickening
was very good, implying that
Optical Coherence Tomography versus Stereoscopic Fundus
Photography or Biomicroscopy for Diagnosing Diabetic Macular Edema:
A Systematic ReviewGianni Virgili, Francesca Menchini, Andrea F.
Dimastrogiovanni, Emilio Rapizzi, Ugo Menchini, Francesco Bandello,
and Raffaella Gortana Chiodini
Rome, Italy in 2000. PURPOSE.
To review systematically the sensitivity and
specificity of optical coherence tomography (OCT) for diagnosing
macular edema attributable to diabetic retinopathy compared with
well-established gold standard tests such as fundus
stereophotography or
RESULTS. Fifteen studies were considered eligible. These studies
were of good quality for most items of the QUADAS checklist, but
most studies did not report masking of examiners and did not
describe how withdrawals and undetermined results were treated.
Seven studies included healthy control subjects, which could have
artificially enhanced OCT diagnostic performance. All but one study
included both eyes of the patients without taking into account the
withinsubject correlation in statistical analyses. Sensitivity and
specificity data could be extracted from only 6 of 15 studies,
because appropriate cross tabulations of index and reference tests
were not reported by the others. In five of these studies, central
retinal thickness cutoffs between 230 and 300 m were adopted to
define abnormal OCT results and considered the central type of CSME
only, whereas in one study a complex algorithm accounting for
extrafoveal CSME was used. The design of one study was casecontrol
and was excluded from the meta-analysis. The expected operating
point on the summary ROC, a pooled estimate of all studies,
corresponded to a sensitivity of 0.79 (95% CI: 0.710.86), a
specificity of 0.88 (95% CI: 0.800.93), a positive likelihood ratio
of 6.5 (95% CI: 4.010.7), and a negative likelihood ratio of 0.24
(95% CI: 0.170.32). These values suggest a good overall performance
of OCT for diagnosing CSME.
Purpose: To investigate the quantitative assessment of macular
edema secondary to central or branch retinal vein occlusion with
foveal thickness measurements by optical coherence tomography
(OCT). Material and methods: Thirty eight eyes of 38 cases examined
between October 2000-May 2002, with central or branch retinal vein
occlusion were included in the study. At initial examination and
during follow-up examinations at 3-6 month intervals, complete
ophthalmic examination was done, color fundus photographs were
taken and fluorescein angiography was performed. Foveal thickness
measurements were taken in macular crosssection images obtained
with optical coherence tomography. Control group included
thirty-nine eyes of 33 healthy objects without eye pathology.
Foveal thickness measurements were obtained from macular OCT images
and compared with the values of study group.
Results: At initial examination, there was sponge-like retinal
swelling in 34 %, cystoid macular edema in 34 %, serous macular
edema in 19.2 % and mixed edema in 12.8 % of 38 cases (11 of them
had central, 27 of them had branch retinal vein occlusion). In the
study group, the mean foveal thickness at initial examination
(590.2 45 m) was significantly higher than the mean value at last
visit (403.1 53 m). These values were also significantly higher
than the mean foveal thickness in control group (177.1 19.4 m).
There was negative correlation between mean foveal thickness
measurements and visual acuities at initial and final
examinations.
Conclusion: Optical coherence tomography is a useful technique
for noninvasive, objective and quantitative assessment of macular
edema secondary to retinal vein occlusions with foveal
Purpose : To evaluate central serous chorioretinopathy (CSCR)
with optical coherence tomography (OCT) during the acute and
resolution phase. Method : 12 patients (8 men and 4 women) who were
examined between October 2000 and May 2001 and diagnosed as CSCR
were included in the study. Complete ophthalmologic examination was
performed, color fundus photographs were taken and optical
coherence tomography was performed. Fundus fluorescein angiography
was performed in all cases except two pregnant women during initial
examination. FA and OCT were repeated during the control
examinations. The difference between the retinal thickness and
serous
Results :14eyesof12patientshadonacutephaseofCSCR
accordingtofundusexaminationandfluoresceinangiography.2patients
werepregnantandoneofthemhadbilateralinvolvement.Fluoresceinangiography
wasnotperformedinthesecases.Fluoresceinangiograhyrevealedoneormore
leakagepointsin10eyes,multiplepigmentepithelialdetachments(FED)inoneeye.
OCTscansshowedneurosensoryretinaldetachmentandincreasedretinalthickness
in13eyes,andPED'sinoneeye.FEDinapregnantwomanwasdetectedbyOCT.
Duringfollow-upperiod,intheeyeswithoutactiveleakagepointinfluorescein
angiography,theneurosensorydetachmentsresolvedandretinalthicknessdecreased
In OCT scans.
Conclusion:OCTisausefulandobjectivediagnostictechnique in
evaluating FED, neurosensory retinal detachment and retinal
thickness in CSCR. It may be an alternative diagnostic tool in
pregnantwomen.
Virgili et al. (2007) Italy : systematically the sensitivity and
specificity To reviewof OCT for diagnosing macular oedema
attributable to diabetic retinopathy compared with fundus
stereophotography or contact and non-contact fundus biomicroscopy.
OCT can be used to diagnose CSME, particularly its central type or
CDME, and decide on laser photocoagulation in patients with
intermediate suspicion of disease The strength of this conclusion
is limited by the fact that data could be extracted from only a
fraction of the published literature due to limitations in
reporting. The precision of estimates is inflated by the
within-patient correlation between Results : Sensitivity = 0.79
(95% CI: 0.710.86); specificity = 0.88 (95% CI: 0.800.93)
Comparison between optical coherence tomography and fundus
fluorescein angiography for the detection of cystoid macular edema
in patients with uveitis.ANTCLIFFR. J. ; STANFORDM. R. ; CHAUHAND.
S. ; GRAHAME. M. ; SPALTOND. J. ; SHILLINGJ. S. ; FFYTCHET. J. ;
MARSHALLJ. Department of Ophthalmology, Rayne Institute, St.
Thomas'Hospital, London. Purpose: To compare optical coherence
tomography (OCT) with fundus fluorescein angiography (FFA) for the
detection of cystoid macular edema (CME) in patients with uveitis.
Main Outcome Measures: Detection and distribution of macular edema.
Results: One hundred eight eyes had similar results on both OCT and
FFA in that 67 eyes had CME and 41 eyes had no CME. In 10 eyes
subretinal fluid was detected on OCT but not FFA. Five of these
eyes had CME on FFA but not OCT. Three other eyes had CME that was
detected by FFA but not by OCT. Compared with FFA, the OCT
sensitivity for detecting CME was 96% (including the eyes with
subretinal fluid), and the OCT specificity was 100%.
Conclusions: OCT is as effective at detecting CME as is FFA but
is superior in demonstrating axial
Conclusion :1) OCT can detect very early macular disease
changes. 2) It can be used to study, diagnose, monitoring &
guiding retreatment decisions. 3) It is reproducible, accurate,
sensitive and specific. Limitations: 1) Clear media needed, 2)
Pupillary dimeter of approx. 4 mm, 3) Costly.
THANK YOU!